Optimal Lead Position in Patch-Type Monitoring Sensors for Reconstructing 12-Lead ECG Signals with Universal Transformation Coefficient


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Protocol
2.3. Data Processing
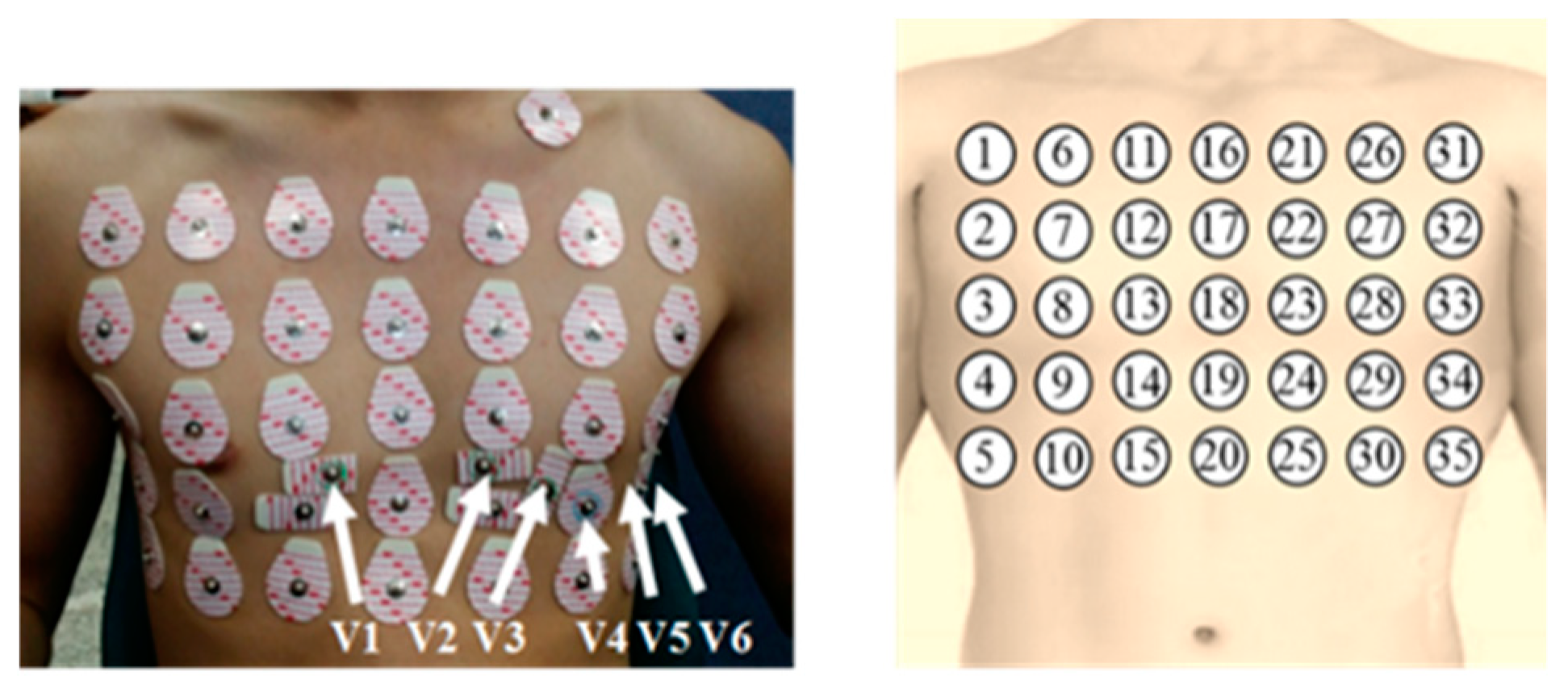
2.3.1. Data Preparation
2.3.2. Chest Leads
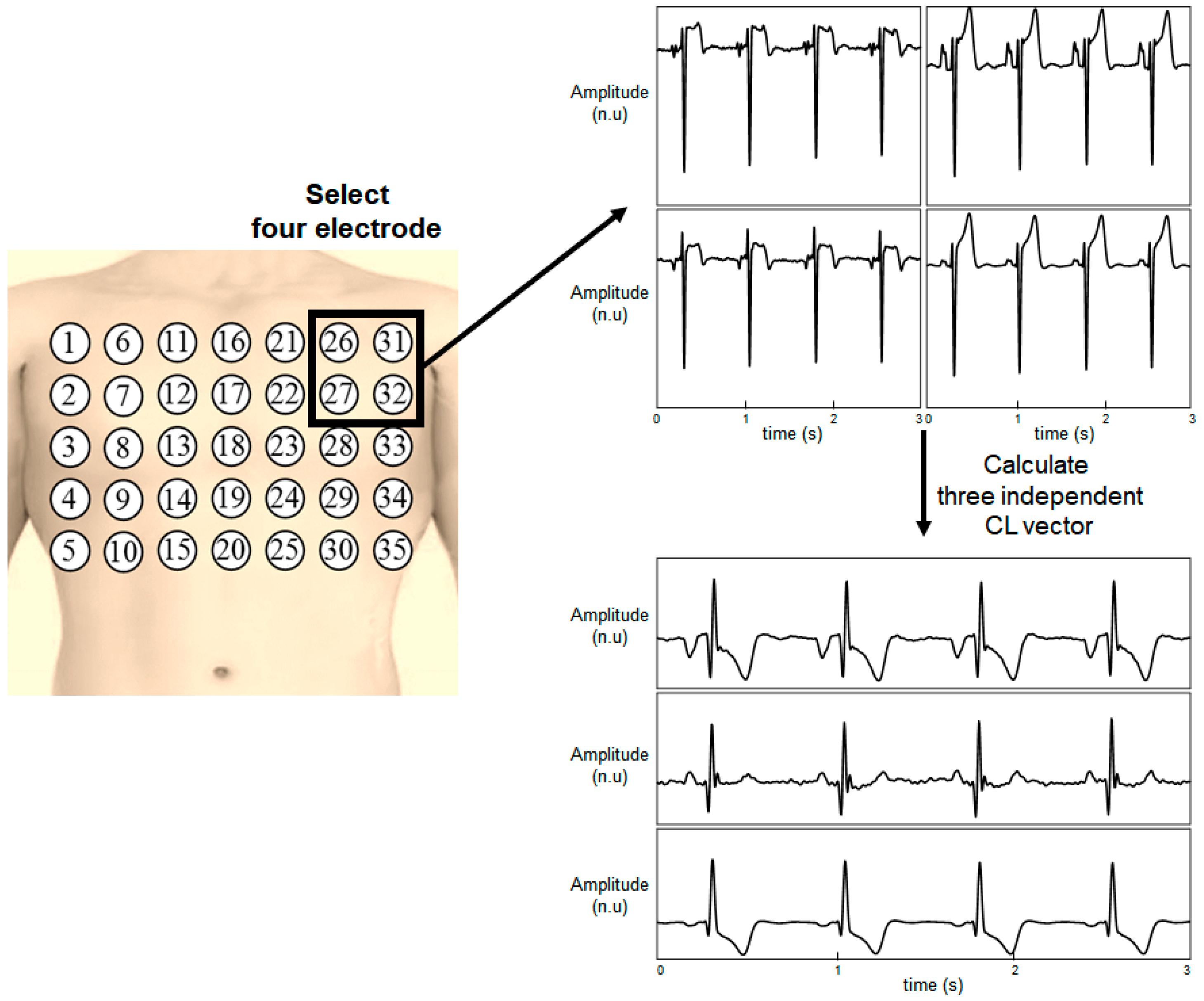
- A 5 cm × 5 cm square (e.g., electrode combination (1, 2, 6, and 7)). The number of combinations for this shape was 6 × 4 = 24.
- A broader 10 cm × 10 cm square (e.g., electrode combination (1, 3, 11, and 13)): The number of combinations for this shape was 5 × 3 = 15.
- A right-angled triangle shape in a 10 cm × 10 cm square area (e.g., electrode combination (1,7,11, and 13): Four orientations were considered. The right-angled triangle shape has four orientations, so the number of combinations for this shape was 5 × 3 × 4 = 60.
2.4. ECG Reconstruction Model
2.4.1. MLR Model
2.4.2. ANN Model
2.5. Evaluation Metrics
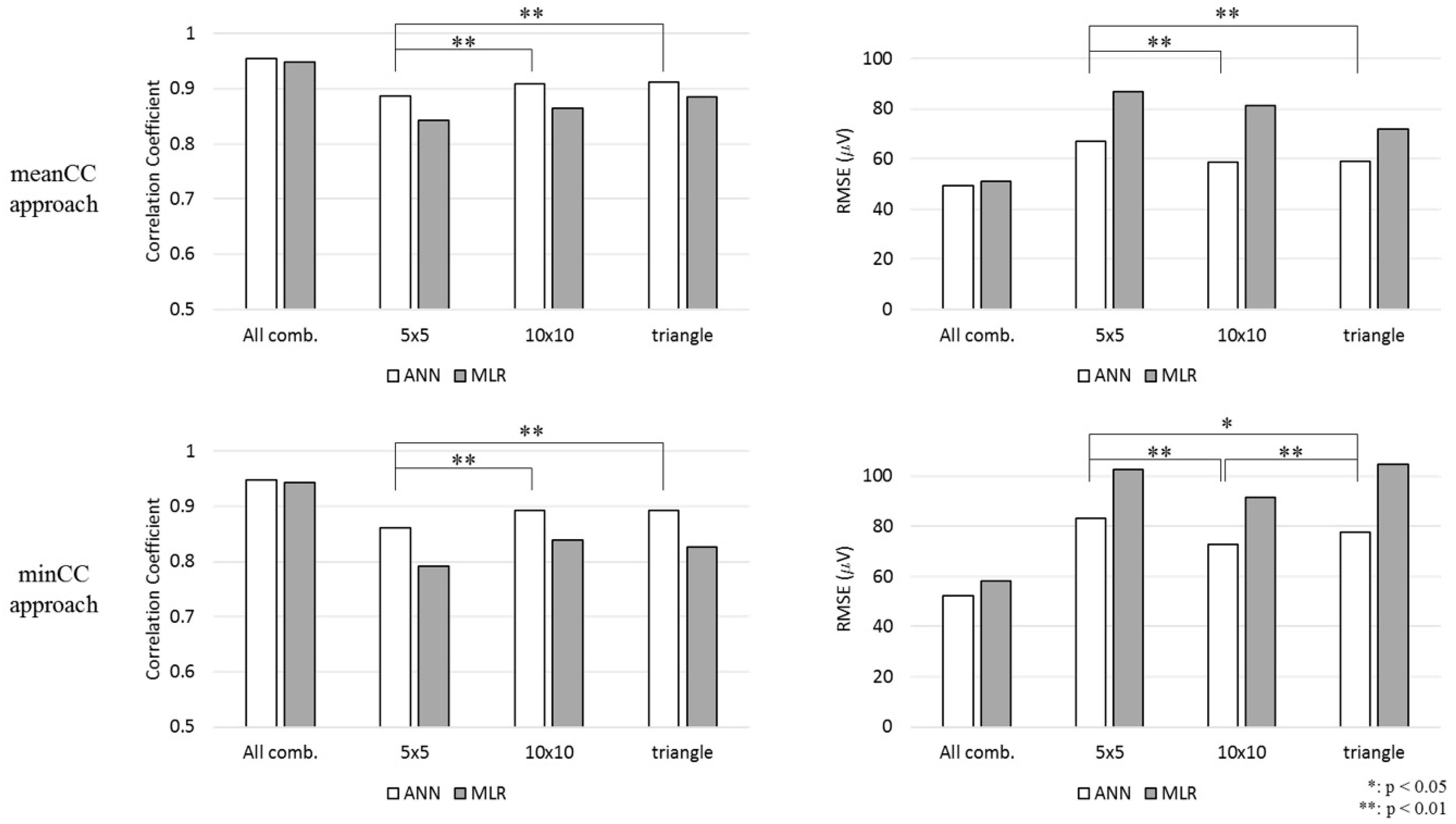
3. Results
4. Discussion
4.1. Reconstruction Quality of Each Lead
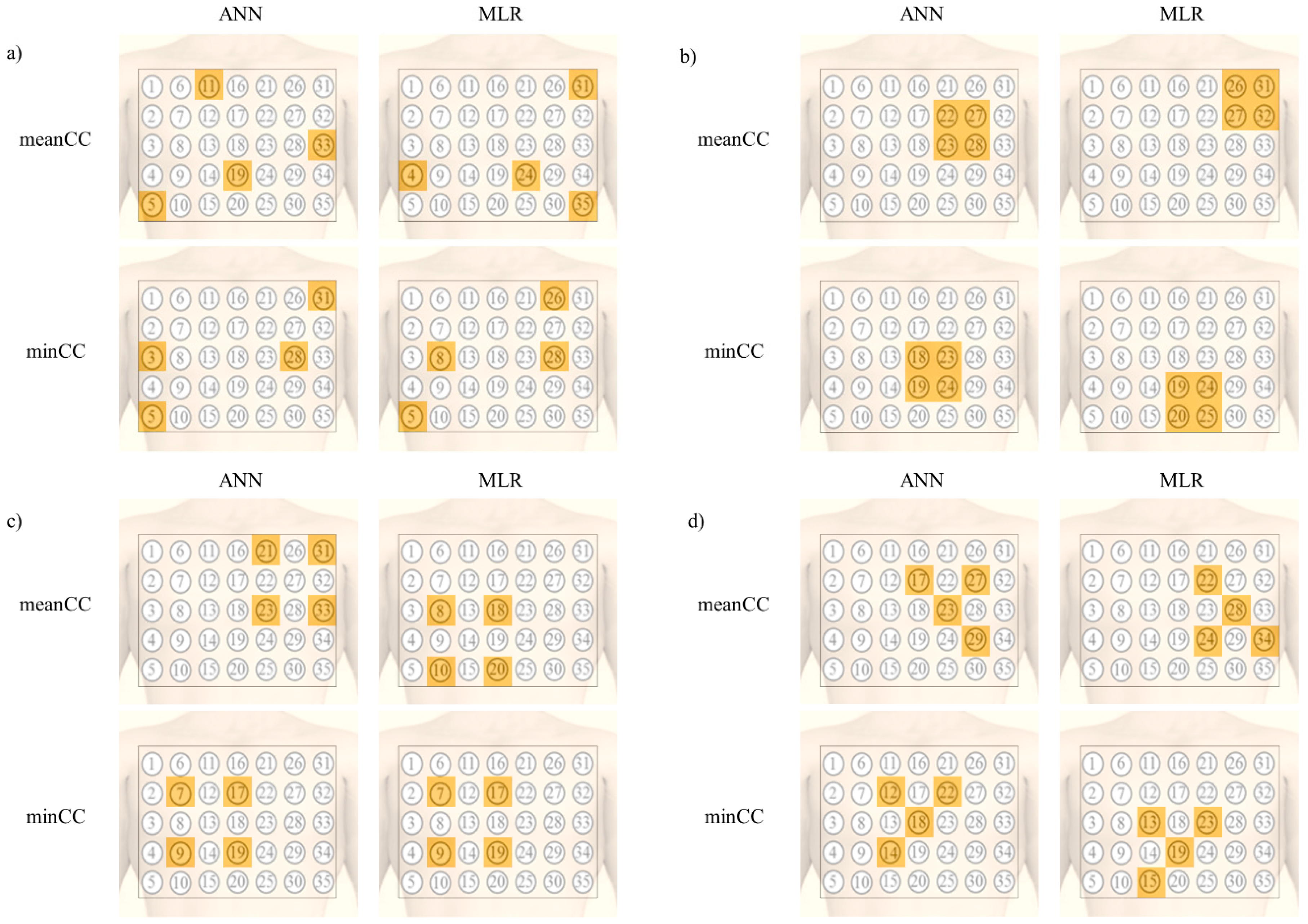
4.2. Robustness of the Position
4.3. Comparison to Previous Reconstruction Algorithms
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Malmivuo, J.; Plonsey, R. 12-lead ECG system. In Bioelectromagnetism; Oxford University Press: Oxford, UK, 1995. [Google Scholar]
- Nelwan, S.P.; Kors, J.A.; Meij, S.H. Minimal lead sets for reconstruction of 12-lead electrocardiograms. J. Electrocardiol. 2000, 33, 163–166. [Google Scholar] [CrossRef] [PubMed]
- Drew, B.J.; Pelter, M.M.; Brodnick, D.E.; Yadav, A.V.; Dempel, D.; Adams, M.G. Comparison of a new reduced lead set ECG with the standard ECG for diagnosing cardiac arrhythmias and myocardial ischemia. J. Electrocardiol. 2002, 35, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Nelwan, S.P.; Kors, J.A.; Meij, S.H.; van Bemmel, J.H.; Simoons, M.L. Reconstruction of the 12-lead electrocardiogram from reduced lead sets. J. Electrocardiol. 2004, 37, 11–18. [Google Scholar] [PubMed]
- Lee, J.; Kim, M.; Kim, J. Reconstruction of Precordial Lead Electrocardiogram from Limb Leads Using the State-Space Model. IEEE J. Biomed. Health 2016, 20, 818–828. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.D.; Zhou, W.; Xing, Y.; Liu, N.; Movahedipour, M.; Zhou, X.G. A novel method based on convolutional neural networks for deriving standard 12-lead ECG from serial 3-lead ECG. Front. Inf. Technol. Eng. 2019, 20, 405–413. [Google Scholar] [CrossRef]
- Dawson, D.; Yang, H.; Malshe, M.; Bukkapatnam, S.T.; Benjamin, B.; Komanduri, R. Linear affine transformations between 3-lead (Frank XYZ leads) vectorcardiogram and 12-lead electrocardiogram signals. J. Electrocardiol. 2009, 42, 622–630. [Google Scholar] [CrossRef]
- Willems, J.L.; Lesaffre, E.; Pardaens, J. Comparison of the classification ability of the electrocardiogram and vectorcardiogram. Am. J. Cardiol. 1987, 59, 119–124. [Google Scholar] [CrossRef]
- Frank, E. An accurate, clinically practical system for spatial vectorcardiography. Circulation 1956, 13, 737–749. [Google Scholar] [CrossRef]
- Dower, G.E.; Yakush, A.; Nazzal, S.B.; Jutzy, R.V.; Ruiz, C.E. Deriving the 12-lead electrocardiogram from four (EASI) electrodes. J. Electrocardiol. 1988, 21, S182–S187. [Google Scholar] [CrossRef]
- Drew, B.J.; Pelter, M.M.; Wung, S.F.; Adams, M.G.; Taylor, C.; Evans, G.T., Jr.; Foster, E. Accuracy of the EASI 12-lead electrocardiogram compared to the standard 12-lead electrocardiogram for diagnosing multiple cardiac abnormalities. J. Electrocardiol. 1999, 32, 38–47. [Google Scholar] [CrossRef]
- Sejersten, M.; Wagner, G.S.; Pahlm, O.; Warren, J.W.; Feldman, C.L.; Horacek, B.M. Detection of acute ischemia from the EASI-derived 12-lead electrocardiogram and from the 12-lead electrocardiogram acquired in clinical practice. J. Electrocardiol. 2007, 40, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Finlay, D.D.; Nugent, C.D.; Donnelly, M.P.; Lux, R.L. Eigenleads: ECG leads for maximizing information capture and improving SNR. IEEE Trans. Inf. Technol. Biomed. 2010, 14, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Trobec, R.; Tomasic, I. Synthesis of the 12-lead electrocardiogram from differential leads. IEEE Trans. Inf. Technol. Biomed. 2011, 15, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Hadzievski, L.; Bojovic, B.; Vukcevic, V.; Belicev, P.; Pavlovic, S.; Vasiljevic-Pokrajcic, Z.; Ostojic, M. A novel mobile transtelephonic system with synthesized 12-lead ECG. IEEE Trans. Inf. Technol. Biomed. 2004, 8, 428–438. [Google Scholar] [CrossRef] [PubMed]
- Dos Reis, J.E.; Soullie, P.; Oster, J.; Soler, E.P.; Petitmangin, G.; Felblinger, J.; Odille, F. Reconstruction of the 12-lead ECG using a novel MR-compatible ECG sensor network. Magn. Reson. Med. 2019, 82, 1929–1945. [Google Scholar] [CrossRef] [PubMed]
- Kew, H.-P.; Jeong, D.-U. Wearable Patch-Type ECG Using Ubiquitous Wireless Sensor Network for Healthcare Monitoring Application. In Proceedings of the 2nd International Conference on Interaction Sciences: Information Technology, Culture and Human, Seoul, Korea, 24–26 November 2009; pp. 624–630. [Google Scholar]
- Yan, L.; Yoo, J.; Kim, B.; Yoo, H.-J. A 0.5-μ Vrms 12-μW wirelessly powered patch-type healthcare sensor for wearable body sensor network. IEEE J. Solid State Circuits 2010, 45, 2356–2365. [Google Scholar]
- Lobodzinski, S.S. ECG patch monitors for assessment of cardiac rhythm abnormalities. Prog. Cardiovasc. Dis. 2013, 56, 224–229. [Google Scholar] [CrossRef]
- Kim, M.S.; Cho, Y.C.; Seo, S.-T.; Son, C.-S.; Kim, Y.-N. Auto-detection of R wave in ECG (electrocardiography) for patch-type ECG remote monitoring system. Biomed. Eng. Lett. 2011, 1, 180. [Google Scholar] [CrossRef]
- Bifulco, P.; Gargiulo, G.; Romano, M.; Fratini, A.; Cesarelli, M. Bluetooth Portable Device for Continuous ECG and Patient Motion Monitoring during Daily Life. In Proceedings of the 11th Mediterranean Conference on Medical and Biomedical Engineering and Computing 2007, Ljubljana, Slovenia, 26–30 June 2007; pp. 369–372. [Google Scholar]
- Lee, H.J.; Lee, D.S.; Kwon, H.B.; Kim, D.Y.; Park, K.S. Reconstruction of 12-lead ECG Using a Single-patch Device. Methods Inf. Med. 2017, 56, 319–327. [Google Scholar] [CrossRef]
- Tomasic, I.; Frljak, S.; Trobec, R. Estimating the Universal Positions of Wireless Body Electrodes for Measuring Cardiac Electrical Activity. IEEE Trans. Biomed. Eng. 2013, 60, 3368–3374. [Google Scholar] [CrossRef]
- Tomasic, I.; Trobec, R. Electrocardiographic systems with reduced numbers of leads-synthesis of the 12-lead ECG. IEEE Rev. Biomed. Eng. 2014, 7, 126–142. [Google Scholar] [CrossRef] [PubMed]
- Puurtinen, M.; Viik, J.; Hyttinen, J. Best electrode locations for a small bipolar ECG device: Signal strength analysis of clinical data. Ann. Biomed. Eng. 2009, 37, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Bailey, J.J.; Berson, A.S.; Garson, A., Jr.; Horan, L.G.; Macfarlane, P.W.; Mortara, D.W.; Zywietz, C. Recommendations for standardization and specifications in automated electrocardiography: Bandwidth and digital signal processing. A report for health professionals by an ad hoc writing group of the Committee on Electrocardiography and Cardiac Electrophysiology of the Council on Clinical Cardiology, American Heart Association. Circulation 1990, 81, 730–739. [Google Scholar] [CrossRef] [PubMed]
- Baumert, M.; Schmidt, M.; Zaunseder, S.; Porta, A. Effects of ECG sampling rate on QT interval variability measurement. Biomed. Signal Process. Control 2016, 25, 159–164. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | N | Method | CC |
|---|---|---|---|
| Nelwan [4] | 234 | Reduced lead sets | 0.912 (median) |
| Lee [5] | 290 | Reduced lead sets | 0.900 (mean) |
| Finlay [13] | 744 | Eigenleads | 0.907 (median) |
| Trobec [14] | 30 | Differntial leads | 0.979 (median) |
| Hadzievski [15] | 192 | Transtelephonic system | - |
| Age (Year) | Chest (cm) | Mean Heart Rate (beat/min) |
|---|---|---|
| 27.4 ± 3.9 | 93.0 ± 6.5 | 72.9 ± 8.2 |
| Approach | Shape | MLR | ANN | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean CC (SD) | Median CC | RMSE (μV) | Mean R2 | Mean ICC | Mean CC (SD) | Median CC | RMSE (μV) | Mean R2 | Mean ICC | ||
| meanCC approach | All comb. | 0.948 | 0.967 | 51.1 | 0.87 | 0.93 | 0.954 | 0.970 | 49.3 | 0.91 | 0.95 |
| (0.07) | (0.05) | ||||||||||
| 5 × 5 | 0.842 | 0.915 | 86.8 | 0.65 | 0.77 | 0.887 | 0.924 | 67.1 | 0.78 | 0.85 | |
| (0.23) | (0.13) | ||||||||||
| 10 × 10 | 0.864 | 0.916 | 81.2 | 0.70 | 0.81 | 0.909 | 0.946 | 58.5 | 0.82 | 0.89 | |
| (0.17) | (0.13) | ||||||||||
| triangle | 0.886 | 0.936 | 72.0 | 0.75 | 0.85 | 0.912 | 0.942 | 58.9 | 0.83 | 0.90 | |
| (0.14) | (0.11) | ||||||||||
| minCC approach | All comb. | 0.943 | 0.958 | 58.1 | 0.84 | 0.91 | 0.947 | 0.961 | 52.3 | 0.90 | 0.95 |
| (0.06) | (0.06) | ||||||||||
| 5 × 5 | 0.792 | 0.858 | 103.0 | 0.58 | 0.72 | 0.860 | 0.892 | 83.2 | 0.70 | 0.84 | |
| (0.19) | (0.10) | ||||||||||
| 10 × 10 | 0.839 | 0.874 | 91.7 | 0.60 | 0.74 | 0.893 | 0.923 | 72.7 | 0.75 | 0.85 | |
| (0.14) | (0.09) | ||||||||||
| triangle | 0.827 | 0.894 | 105.0 | 0.66 | 0.79 | 0.893 | 0.920 | 77.6 | 0.79 | 0.89 | |
| (0.18) | (0.08) | ||||||||||
| I | II | III | V1 | V2 | V3 | V4 | V5 | V6 | aVR | aVL | aVF | Mean | SD | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean CC | 5 × 5 | 0.89 | 0.90 | 0.82 | 0.92 | 0.96 | 0.95 | 0.93 | 0.94 | 0.94 | 0.91 | 0.65 | 0.83 | 0.89 | 0.08 |
| 10 × 10 | 0.91 | 0.93 | 0.84 | 0.93 | 0.98 | 0.97 | 0.95 | 0.96 | 0.96 | 0.95 | 0.66 | 0.87 | 0.91 | 0.08 | |
| Tri. | 0.92 | 0.92 | 0.85 | 0.93 | 0.97 | 0.96 | 0.95 | 0.96 | 0.96 | 0.94 | 0.71 | 0.86 | 0.91 | 0.07 | |
| RMSE (μV) | 5 × 5 | 49.4 | 73.6 | 71.1 | 64.6 | 84.3 | 79.6 | 88.3 | 65.9 | 56.7 | 52.6 | 51.7 | 66.9 | 67.1 | 12.4 |
| 10 × 10 | 43.4 | 63.1 | 68.4 | 56.5 | 63.6 | 71.4 | 83.1 | 56.2 | 46.4 | 41.7 | 47.5 | 61.1 | 58.5 | 11.9 | |
| Tri. | 41.6 | 63.2 | 64.4 | 61.1 | 73.4 | 73.4 | 75.2 | 57.4 | 48.4 | 42.2 | 45.9 | 60.4 | 58.9 | 11.5 | |
| R2 | 5 × 5 | 0.81 | 0.76 | 0.45 | 0.76 | 0.94 | 0.92 | 0.88 | 0.92 | 0.89 | 0.84 | 0.56 | 0.62 | 0.78 | 0.15 |
| 10 × 10 | 0.87 | 0.83 | 0.47 | 0.83 | 0.97 | 0.95 | 0.91 | 0.93 | 0.93 | 0.91 | 0.58 | 0.68 | 0.82 | 0.15 | |
| Tri. | 0.87 | 0.84 | 0.53 | 0.79 | 0.95 | 0.94 | 0.93 | 0.95 | 0.94 | 0.91 | 0.64 | 0.71 | 0.83 | 0.13 |
| I | II | III | V1 | V2 | V3 | V4 | V5 | V6 | aVR | aVL | aVF | mean | SD | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean CC | 5 × 5 | 0.89 | 0.83 | 0.82 | 0.81 | 0.89 | 0.92 | 0.90 | 0.91 | 0.89 | 0.86 | 0.81 | 0.79 | 0.86 | 0.04 |
| 10 × 10 | 0.83 | 0.93 | 0.89 | 0.89 | 0.97 | 0.93 | 0.87 | 0.88 | 0.89 | 0.90 | 0.82 | 0.90 | 0.89 | 0.04 | |
| Tri. | 0.88 | 0.90 | 0.87 | 0.92 | 0.97 | 0.94 | 0.88 | 0.88 | 0.87 | 0.90 | 0.85 | 0.86 | 0.89 | 0.03 | |
| RMSE (μV) | 5 × 5 | 45.5 | 89.9 | 69.9 | 84.2 | 134.7 | 108.6 | 114.5 | 92.7 | 78.6 | 62.2 | 41.1 | 76.3 | 83.2 | 26.3 |
| 10 × 10 | 57.6 | 61.1 | 48.7 | 65.4 | 75.8 | 106.0 | 128.3 | 102.0 | 82.4 | 54.7 | 42.8 | 47.0 | 72.7 | 25.9 | |
| Tri. | 46.7 | 74.8 | 62.0 | 64.9 | 92.5 | 106.7 | 128.3 | 108.2 | 89.3 | 54.4 | 38.5 | 64.7 | 77.6 | 26.3 | |
| R2 | 5 × 5 | 0.77 | 0.65 | 0.51 | 0.59 | 0.81 | 0.86 | 0.82 | 0.78 | 0.74 | 0.73 | 0.63 | 0.56 | 0.70 | 0.11 |
| 10 × 10 | 0.64 | 0.83 | 0.72 | 0.71 | 0.93 | 0.84 | 0.73 | 0.71 | 0.70 | 0.76 | 0.54 | 0.84 | 0.75 | 0.10 | |
| Tri. | 0.84 | 0.80 | 0.63 | 0.79 | 0.93 | 0.87 | 0.78 | 0.80 | 0.78 | 0.84 | 0.70 | 0.74 | 0.79 | 0.07 |
| Electrode Combination | p < 0.05 | p < 0.01 |
|---|---|---|
| (13, 15, 19, 23) | - | - |
| (13, 19, 23, 25) | V6 | - |
| (13, 15, 19, 25) | II | - |
| (15, 19, 23, 25) | V4, V6 | V5 |
| Study | Subjects | Median CC (Interquartile Range) | Method | Algorithm |
|---|---|---|---|---|
| Nelwan [4] | N=234 (patients) | 0.912 (0.858, 0.950) | MLR | Reduced lead set 3 lead sets (I, II, V2)—4 electrodes Universal transformation matrix |
| Finlay [13] | N=744 (normal + MI + LVHs) | 0.907 (0.867, 0.933) | MLR | PCA Eigenleads with BSPM 3 vectors—6 electrodes Universal transformation matrix |
| Tomašić [23] | N=40 (normal + patients) | - | MLR | 35 channel ECG 3 vectors—4 electrodes Universal position Personalized transformation matrix median CC for lead III: 0.84 |
| Our work | N=14 (normal) | 0.920 (0.855, 0.943) | ANN | 35 channel ECG 3 vectors—4 electrodes median CC for lead III: 0.87 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, D.; Kwon, H.; Lee, H.; Seo, C.; Park, K. Optimal Lead Position in Patch-Type Monitoring Sensors for Reconstructing 12-Lead ECG Signals with Universal Transformation Coefficient. Sensors 2020, 20, 963. https://doi.org/10.3390/s20040963
Lee D, Kwon H, Lee H, Seo C, Park K. Optimal Lead Position in Patch-Type Monitoring Sensors for Reconstructing 12-Lead ECG Signals with Universal Transformation Coefficient. Sensors. 2020; 20(4):963. https://doi.org/10.3390/s20040963
Chicago/Turabian StyleLee, Dongseok, Hyunbin Kwon, Hongji Lee, Chulhun Seo, and Kwangsuk Park. 2020. "Optimal Lead Position in Patch-Type Monitoring Sensors for Reconstructing 12-Lead ECG Signals with Universal Transformation Coefficient" Sensors 20, no. 4: 963. https://doi.org/10.3390/s20040963
APA StyleLee, D., Kwon, H., Lee, H., Seo, C., & Park, K. (2020). Optimal Lead Position in Patch-Type Monitoring Sensors for Reconstructing 12-Lead ECG Signals with Universal Transformation Coefficient. Sensors, 20(4), 963. https://doi.org/10.3390/s20040963