Validation of a Body-Conducted Sound Sensor for Respiratory Sound Monitoring and a Comparison with Several Sensors


Abstract
1. Introduction
2. Materials and Methods
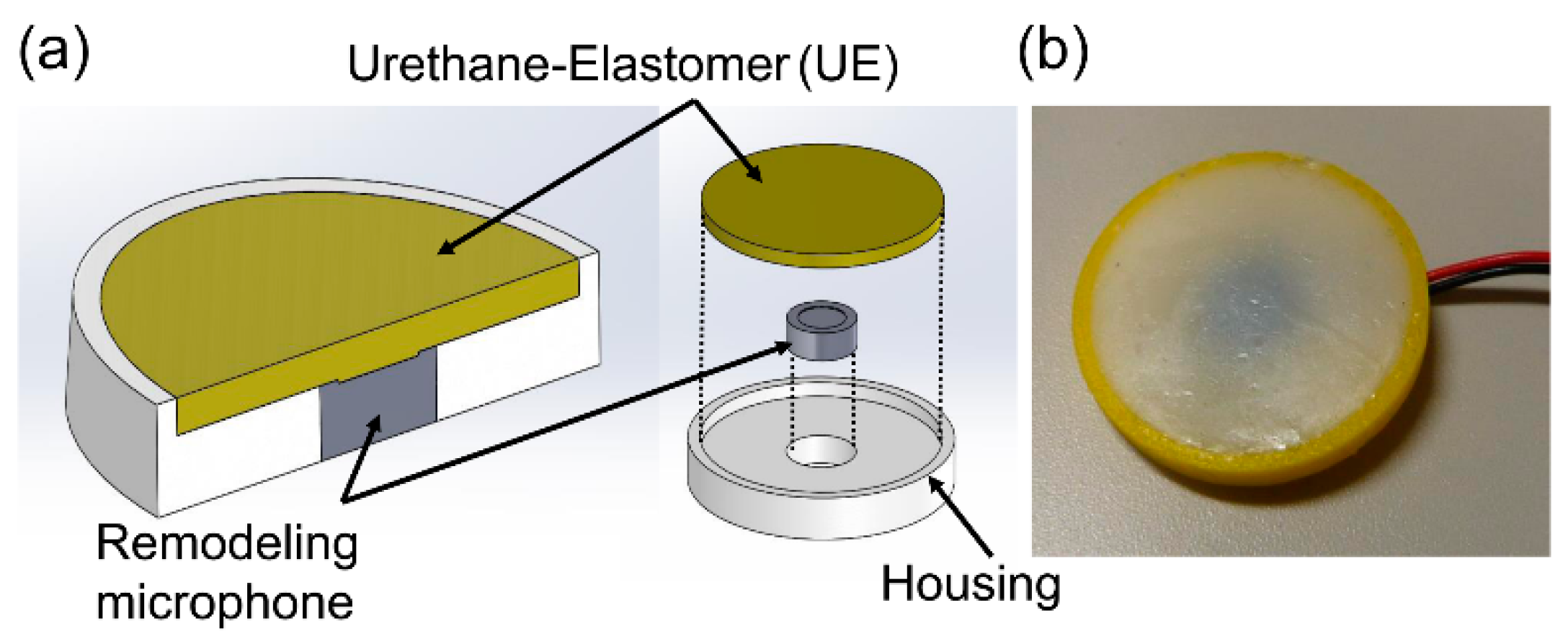
2.1. Sensors of Interst
2.2. Estimation of Frequency Characteristics and Measurements for Sensors on Soft Tissue
2.2.1. Estimation Model for the Frequency Characteristics of Sensors
2.2.2. Measurements for the Sensors
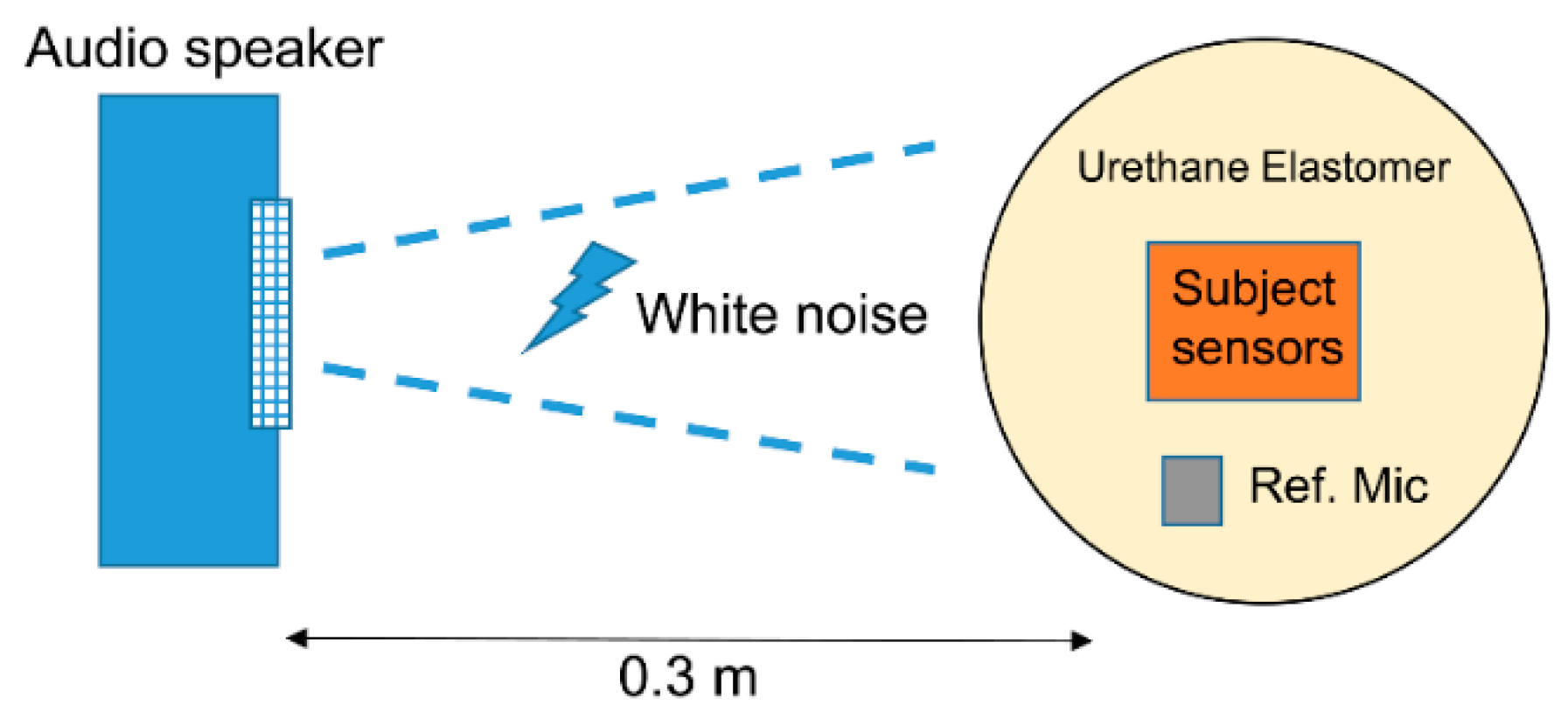
2.3. Tissue-Borne Sensitivity-to-Air Noise Ratio (SRTA)
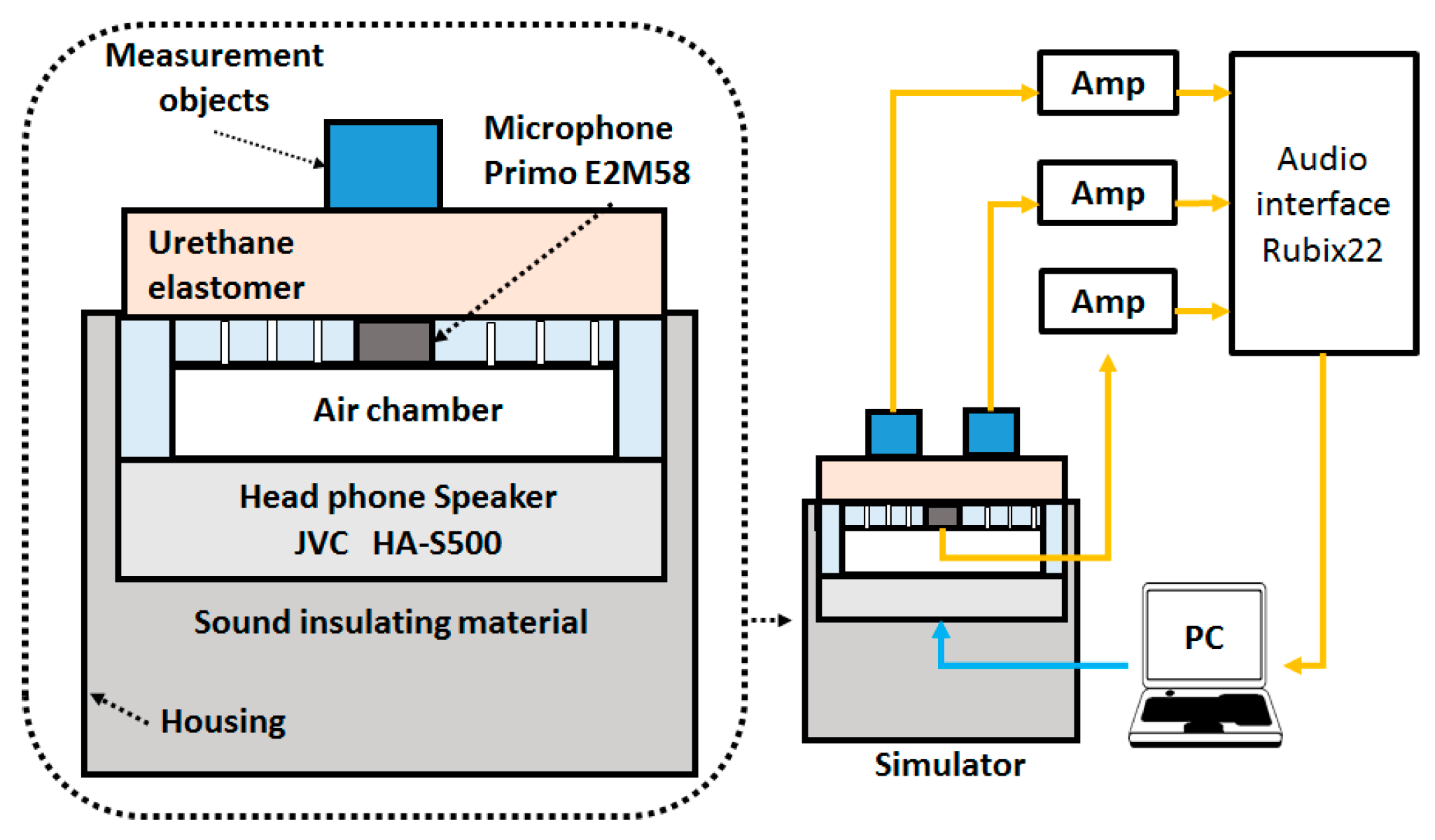
2.4. Evaluation of Sensors in the Respiratory Sound Simulator
2.5. Actual Respiratory Sound Measurements
3. Results
3.1. Simulation and Measurement of Frequency Characteristics of Sensors
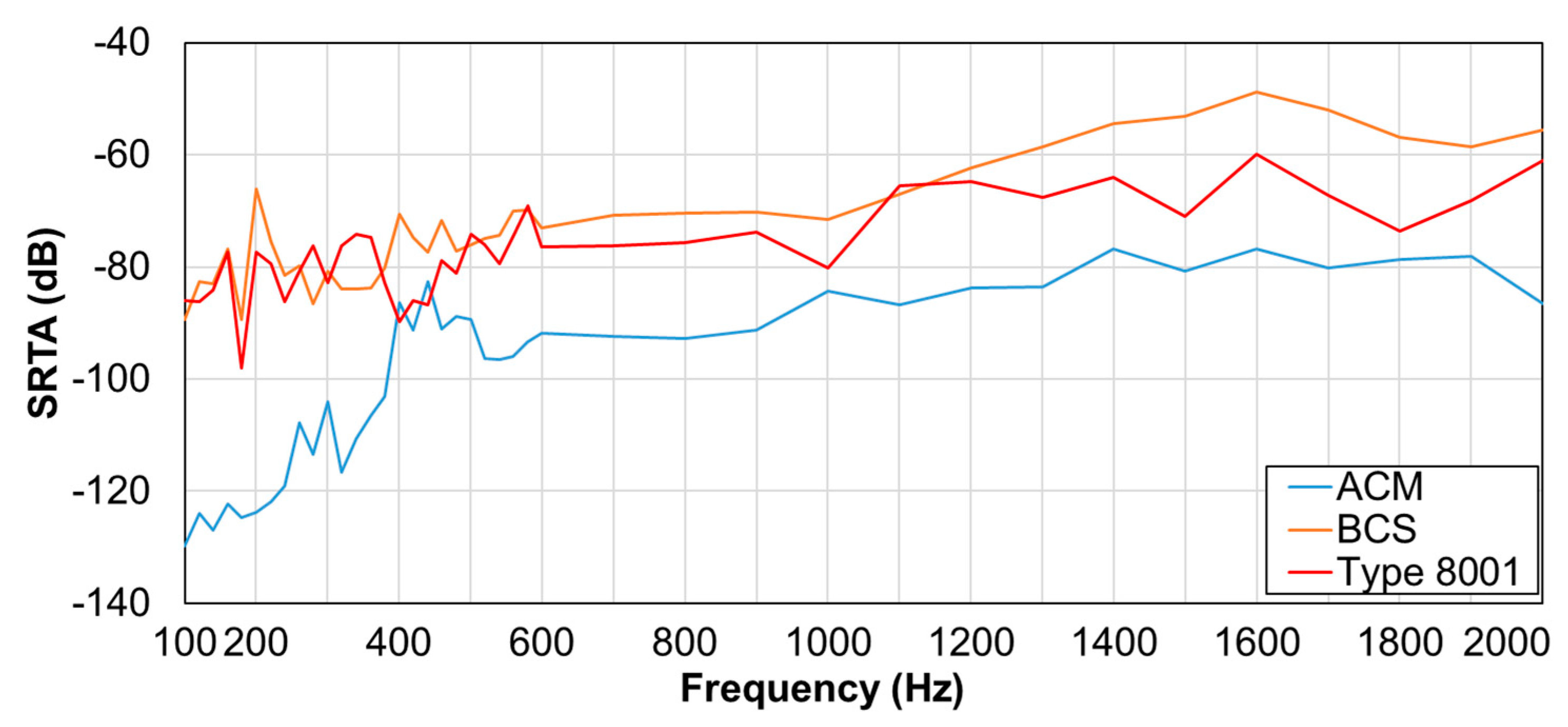
3.2. SRTA Results
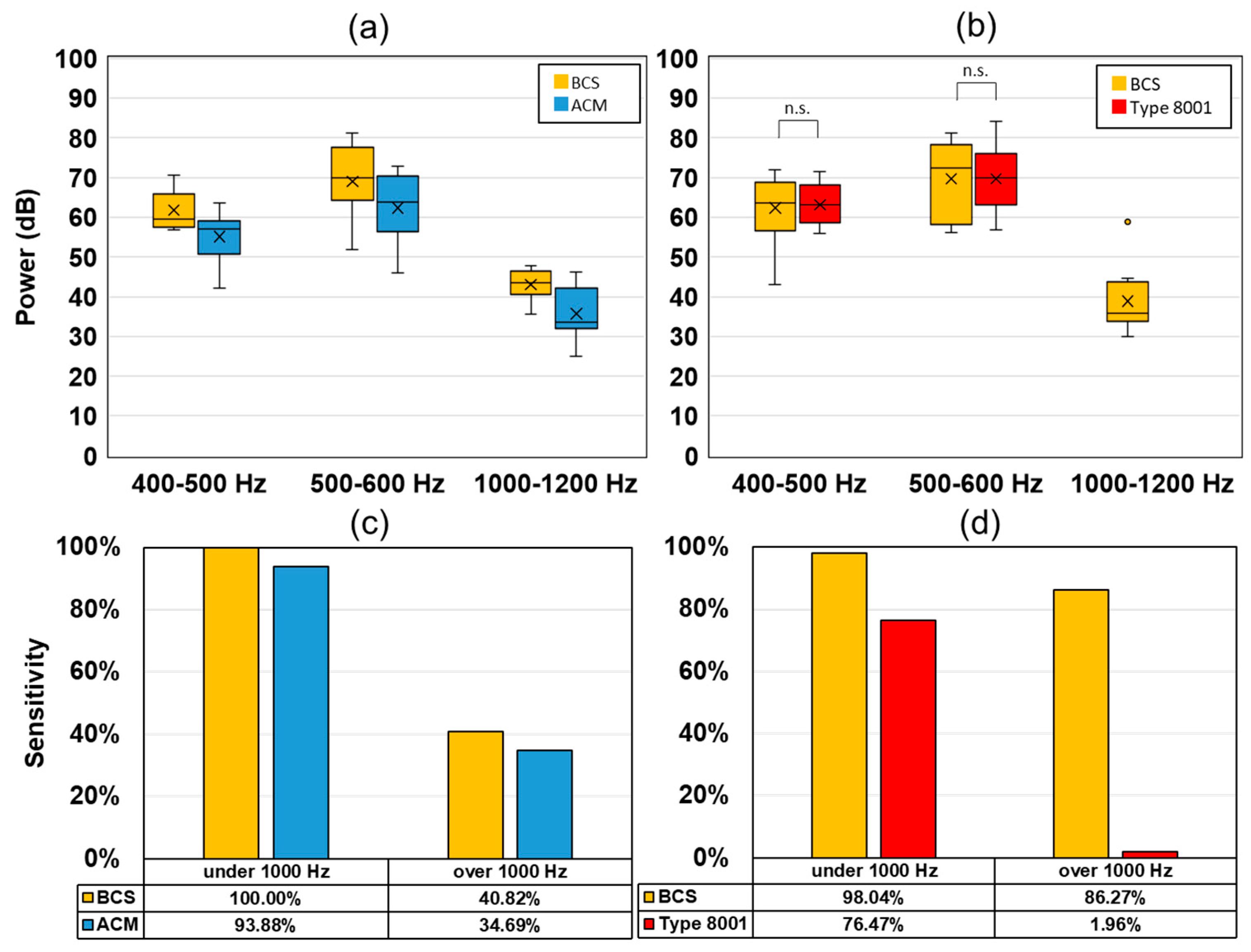
3.3. Observation Experiment using a Respiratory Sound Simulator
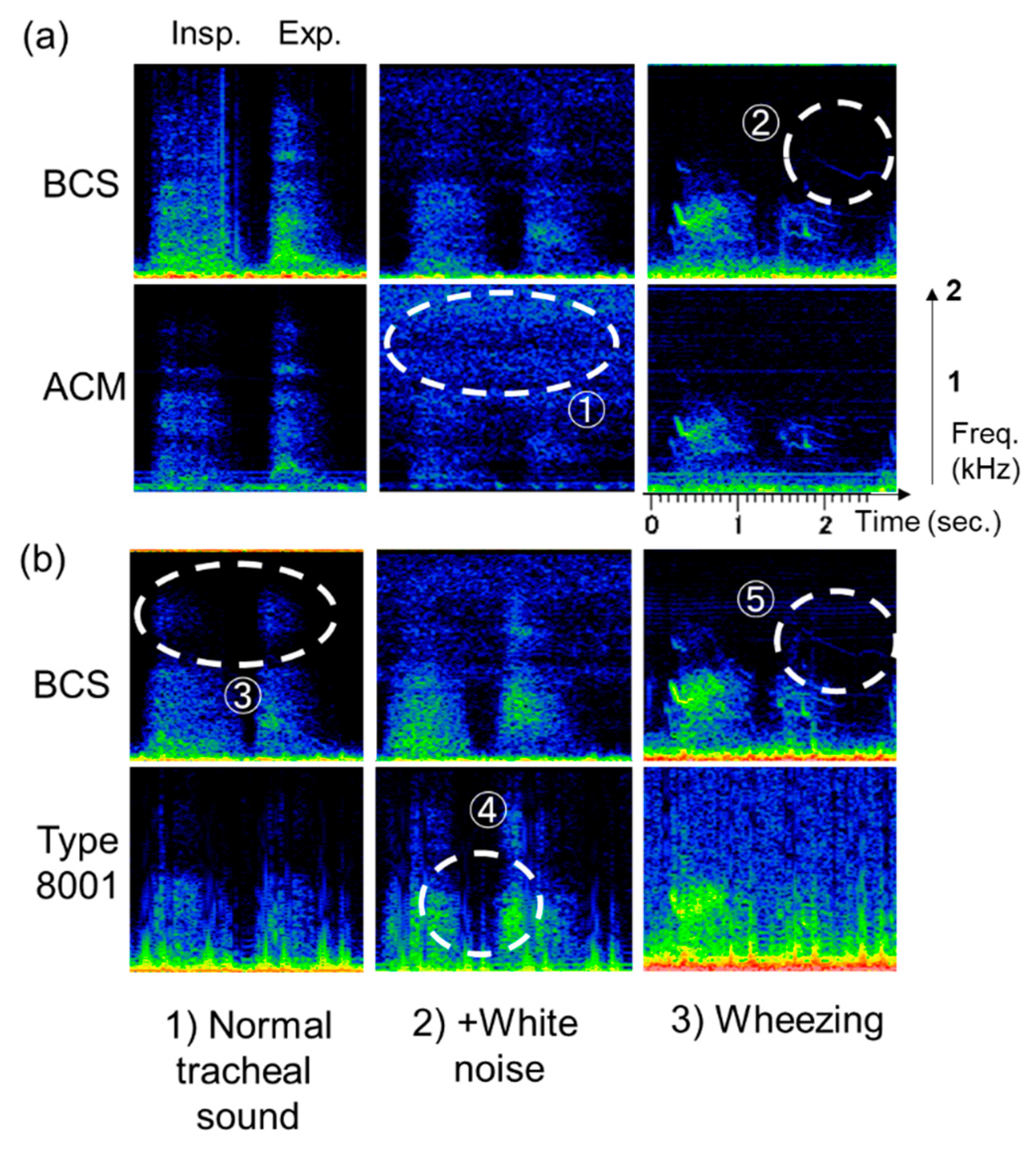
3.4. Actual Respiratory Sound Observation
4. Discussion
4.1. Frequency Characteristic Results of Sensors
4.2. Evaluation of SRTA Results
4.3. Simulator-Observed Respiratory Sounds
4.4. Observation of Actual Respiratory Sound and Usefulness in Clinical Applications
5. Conclusions
- (1)
- Given the same acoustic propagation layer shape, BCS had sensitivity higher than ACM. BCS showed high sensitivity in the high-frequency segments when compared with the acceleration sensors similar to type 8001.
- (2)
- BCS showed high SRTA in the high-frequency segments of 600–1000 and 1200–2000 Hz compared with the other sensors.
- (3)
- The simulator results demonstrated characteristics close to those of the acceleration response. BCS was advantageous for characteristic signal detection in the high-frequency segments.
- (4)
- In the tracheal sound observation experiment, the spectrogram for each sensor showed the same results as those of the simulator, which indicated the advantages of characteristic respiratory sound detection at high frequencies.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Loudon, R.; Murphy, R.L.H. Lung sounds. Am. Rev. Respir. Dis. 1984, 130, 663–673. [Google Scholar]
- Murphy, R.L.; Vyshedskiy, A.; Power-Charnitsky, V.A.; Bana, D.S.; Marinelli, P.M.; Wong-Tse, A.; Paciej, R. Automated lung sound analysis in patients with pneumonia. Respir. Care 2004, 49, 1490–1497. [Google Scholar]
- Shimoda, T.; Obase, Y.; Nagasaka, Y.; Nakano, H.; Kishikawa, R.; Iwanaga, T. Lung sound analysis can be an index of the control of bronchial asthma. Allergol. Int. 2017, 66, 64–69. [Google Scholar] [CrossRef]
- Nakano, H.; Hayashi, M.; Ohshima, E.; Nishikata, N.; Shinohara, T. Validation of a new system of tracheal sound analysis for the diagnosis of sleep apnea-hypopnea syndrome. Sleep 2004, 27, 951–957. [Google Scholar] [CrossRef]
- Ishimatsu, A.; Nakano, H.; Nogami, H.; Yoshida, M.; Iwanaga, T.; Hoshino, T. Breath sound intensity during tidal breathing in COPD patients. Int. Med. 2015, 54, 1183–1191. [Google Scholar] [CrossRef]
- Fernandez-Granero, M.A.; Sanchez-Morillo, D.; Leon-Jimenez, A. Computerised analysis of telemonitored respiratory sounds for predicting acute exacerbations of COPD. Sensors 2015, 15, 26978–26996. [Google Scholar] [CrossRef]
- Yadollahi, A.; Moussavi, Z.M.K. A robust method for estimating respiratory flow using tracheal sounds entropy. IEEE Trans. Biomed. Eng. 2006, 53, 662–668. [Google Scholar] [CrossRef]
- Azarbarzin, A.; Moussavi, Z.M.K. Automatic and unsupervised snore sound extraction from respiratory sound signals. IEEE Trans. Biomed. Eng. 2011, 58, 1156–1162. [Google Scholar] [CrossRef]
- Yu, L.; Ting, C.-K.; Hill, B.E.; Orr, J.A.; Brewer, L.M.; Johnson, K.B.; Egan, T.D.; Westenskow, D.R. Using the entropy of tracheal sounds to detect apnea during sedation in healthy nonobese volunteers. Anesthesiology. J. Am. Soc. Anesthesiol. 2013, 118, 1341–1349. [Google Scholar] [CrossRef]
- Mimoz, O.; Benard, T.; Gaucher, A.; Frasca, D.; Debaene, B. Accuracy of respiratory rate monitoring using a non-invasive acoustic method after general anaesthesia. Br. J. Anaesth 2012, 108, 872–875. [Google Scholar] [CrossRef]
- Ohshima, Y.; Nakayama, H.; Matsuyama, N.; Hokari, S.; Sakagami, T.; Sato, T.; Koya, T.; Takahashi, T.; Kikuchi, T.; Nishizawa, M.; et al. Natural course and potential prognostic factors for sleep-disordered breathing in multiple system atrophy. Sleep Med. 2017, 34, 13–17. [Google Scholar] [CrossRef]
- Pasterkamp, H.; Kraman, S.S.; DeFrain, P.D.; Wodicka, G.R. Measurement of respiratory acoustical signals. Comparison of sensors. Chest 1993, 104, 1518–1525. [Google Scholar] [CrossRef]
- Kraman, S.S.; Wodicka, G.R.; Pressler, G.A.; Pasterkamp, H. Comparison of lung sound transducers using a bioacoustic transducer testing system. J. Appl. Physiol. 1985 2006, 101, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Zanartu, M.; Ho, J.C.; Kraman, S.S.; Pasterkamp, H.; Huber, J.E.; Wodicka, G.R. Air-borne and tissue-borne sensitivities of bioacoustic sensors used on the skin surface. IEEE Trans. Biomed. Eng. 2009, 56, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, A.; Nakayama, K. Characteristics of lung-sound transducers on chest wall(in Japanese). Med. Electron. Biol. Eng. 2000, 38, 298–308. [Google Scholar] [CrossRef]
- Li, S.H.; Lin, B.S.; Tsai, C.H.; Yang, C.T.; Lin, B.S. Design of wearable breathing sound monitoring system for real-time wheeze detection. Sensors 2017, 17, 1–15. [Google Scholar] [CrossRef]
- Morillo, D.S.; Ojeda, J.L.R.; Foix, L.F.C.; Rendon, D.B.; Leon, A. Monitoring and analysis of cardio respiratory and snoring signals by using an accelerometer. In Proceedings of the 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 22–26 August 2007. [Google Scholar]
- Hirahara, T.; Otani, M.; Shimizu, S.; Toda, T.; Nakamura, K.; Nakajima, Y.; Shikano, K. Silent-speech enhancement using body-conducted vocal-tract resonance signals. Speech Commun. 2010, 52, 301–313. [Google Scholar] [CrossRef]
- Nakajima, Y.; Kashioka, H.; Campbell, N.; Shikano, K. Non-Audible Murmur (NAM) recognition. IEICE Trans. Inf. Syst. 2006, E89-D, 1–8. [Google Scholar]
- Toda, T.; Nakagiri, M.; Shikano, K. Statistical voice conversion techniques for body-conducted unvoiced speech enhancement. IEEE Trans. Aud. Speech Lang. Process. 2012, 20, 2505–2517. [Google Scholar] [CrossRef]
- Heracleous, P.; Ishi, C.T.; Miyashita, T.; Ishiguro, H.; Hagita, N. Using body-conducted acoustic sensors for human–robot communication in noisy environments. Int. J. Adv. Robot. Syst. 2013, 10. [Google Scholar] [CrossRef]
- Hirahara, T.; Ooya, T. In High-sensitivity body-conducted sound sensor, International Conference on Natural Polymers(ICNP2010), Kottayam, India. In Kottayam, India; 2010; Vol. 2010, pp. IL141-1–IL141-4. Available online: http://auris.pu-toyama.ac.jp/PDF/ICNP2010_Hirahara.pdf (accessed on 5 August 2012).
- Joyashiki, T.; Wada, C. Estimation of the frequency Response of Body-conducted sound sensors via the equivalent circuit model (in Japanese). Med. Biol. Eng. 2018, 56, 44–51. [Google Scholar] [CrossRef]
- Brüel & Kjær.; Product Data Impedance Heads–Types 8000 and 8001. Available online: https://www.bksv.com/-/media/literature/Product-Data/bp0244.ashx (accessed on 24 December 2019).
- Primo.; Technical Data Electret Condenser Microphone EM258 (In Japanese). Available online: https://www.primocorp.co.jp/product-corp/fileview/5/EM258.pdf, (accessed on 24 December 2019).
- Suzuki, A.; Nakayama, K. Mechanical impedance of soft living tissue based on the model of an oscillating disc on a semi-infinite viscoelastic medium (in Japanese). Med. Electron. Biol. Eng. 1999, 37, 243–249. [Google Scholar] [CrossRef]
- Pasterkamp, H.; Powell, R.E.; Sanchez, I. Lung sound spectra at standardized air flow in normal infants, children, and adults. Am. J. Respir. Crit. Care Med. 1996, 154, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Kraman, S.S.; Pressler, G.A.; Pasterkamp, H.; Wodicka, G.R. Design, construction, and evaluation of a bioacoustic transducer testing (BATT) system for respiratory sounds. IEEE Trans. Biomed. Eng. 2006, 53, 1711–1715. [Google Scholar] [CrossRef] [PubMed]
- Nakano, H. Lung auscultation expert (in Japanese). Available online: http://www.libroscience.com/lung/sonogram (accessed on 1 April 2019).
- Gross, V.; Dittmar, A.; Penzel, T.; Schüttler, F.; Wichert, P. The relationship between normal lung sounds, age, and gender. Am. J. Respir. Crit. Care Med. 2000, 162, 905–909. [Google Scholar] [CrossRef] [PubMed]
- Gavriely, N.; Nissan, M.; Rubin, A.H.; Cugell, D.W. Spectral characteristics of chest wall breath sounds in normal subjects. Thorax 1995, 50, 1292–1300. [Google Scholar] [CrossRef] [PubMed]
- Kraman, S.S. Does the vesicular lung sound come only from the lungs? Am. Rev. Respir. Dis. 1983, 128, 622–626. [Google Scholar]
- Patel, S.; Lu, S.; Doerschuk, P.C.; Wodicka, G.R. Sonic phase delay from trachea to chest wall: Spatial and inhaled gas dependency. Med. Biol. Eng. Comput. 1995, 33, 571–574. [Google Scholar] [CrossRef]
- Bergstresser, T.; Ofengeim, D.; Vyshedskiy, A.; Shane, J.; Murphy, R. Sound transmission in the lung as a function of lung volume. J. Appl. Physiol. (1985) 2002, 93, 667–674. [Google Scholar] [CrossRef]
- Pasterkamp, H.; Sanchez, I. Effect of gas density on respiratory sounds. Am. J. Respir. Crit. Care Med. 1996, 153, 1087–1092. [Google Scholar] [CrossRef]
- Schreur, H.J.W.; Vanderschoot, J.; Zwinderman, A.H.; Dijkman, J.H.; Sterk, P.J. Abnormal lung sounds in patients with asthma during episodes with normal lung function. Chest 1994, 106, 91–99. [Google Scholar] [CrossRef]
- Pasterkamp, H.; Consunji-Araneta, R.; Oh, Y.; Holbrow, J. Chest surface mapping of lung sounds during methacholine challenge. Pediatr. Pulmonol. 1997, 23, 21–30. [Google Scholar] [CrossRef]
- Ward, J.J.; Wattier, B.A. Technology for enhancing chest auscultation in clinical simulation. Respir. Care 2011, 56, 834–845. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, S.; Otani, M.; Hirahara, T. Frequency characteristics of several non-audible murmur (NAM) microphones. Acoust. Sci. Tech. 2009, 30, 139–142. [Google Scholar] [CrossRef]
- Toda, M.; Thompson, M.L. Contact-type vibration sensors using curved clamped PVDF film. IEEE Sens. J. 2006, 6, 1170–1177. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BCS | ACM | Type 8001 | |
|---|---|---|---|
| Diameter (mm) | 20 *1 | 20 *1 | 15 |
| Mass (g) | 1.49 | 1.50 | 30.89 |
| Sensitivity (dB) | −32 (V/Pa) *2 | −32 (V/Pa) | 0 (V/m/s2) *3 |
| Sensor type | Microphone | Microphone | Accelerometer |
| Housing materials | ABS resin | ABS resin | - |
| BCS | ACM | Type 8001 | |
|---|---|---|---|
| Acceleration Response Model | |||
| Pressure Response Model |
| Female/Male | 3/12 |
|---|---|
| Age (Mean ± SD) | 24.6 ± 3.6 |
| Height (cm) (Mean ± SD) | 170.7 ± 10.0 |
| Weight (kg) (Median (min–max)) | 66.0 (47.0–152.0) |
| Tracheal Sound | |||||
| 100–200 | 200–400 | 400–800 | 800–1600 | ||
| BCS | Insp. | 78.5 (75.0–80.0) | 76.0 (71.0–79.0) | 75.0 (68.3–78.8) | 62.5 (62.0–63.0) |
| Exp. | 72.0 (71.3–73.5) | 75.5 (74.3–77.0) | 77.5 (74.0–78.8) | 67.0 (63.3–69.0) | |
| ACM | Insp. | 70.5 (68.0–74.0) | 64.0 (60.3–69.0) | 63.0 (56.5–67.0) | 48.0 (46.0–5 1.3) |
| Exp. | 67.5 (66.0–68.0) | 64.5 (63.0–65.0) | 66.0 (62.0–67.8) | 57.0 (51.0–58.8) | |
| Type 8001 | Insp. | 87.5 (84.8–89.8) | 83.5 (82.3–86.8) | 72.5 (69.0–74.8) | 57.0 (56.3–58.0) |
| Exp. | 82.5 (79.5–83.0) | 84.0 (81.3–84.8) | 74.0 (70.8–75.8) | 62.0 (60.0–65.0) | |
| Polyphonic Wheezes | |||||
| 100–200 | 200–400 | 400–800 | 800–1600 | ||
| BCS | Insp. | 87.0 (83.3–89.8) | 84.5 (80.5–88.8) | 82.0 (79.5–87.0) | 72.5 (68.5–73.0) |
| Exp. | 80.5 (76.0–84.8) | 74.0 (70.3–77.8) | 70.5 (65.0–73.8) | 63.5 (63.0–64.0) | |
| ACM | Insp. | 71.5 (69.3–75.0) | 76.5 (72.0–80.5) | 75.0 (73.3–81.0) | 67.0 (61.3–68.0) |
| Exp. | 66.0 (65.0–70.0) | 60.0 (56.5–61.0) | 56.5 (52.3–59.8) | 52.0 (51.3–52.8) | |
| Type 8001 | Insp. | 85.5 (84.0–91.0) | 91.5 (87.5–93.0) | 81.0 (80.0–86.5) | 67.0 (65.3–68.0) |
| Exp. | 80.0 (76.0–84.0) | 78.5 (73.5–81.3) | 69.5 (58.0–74.0) | 58.5 (58.0–59.0) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Joyashiki, T.; Wada, C. Validation of a Body-Conducted Sound Sensor for Respiratory Sound Monitoring and a Comparison with Several Sensors. Sensors 2020, 20, 942. https://doi.org/10.3390/s20030942
Joyashiki T, Wada C. Validation of a Body-Conducted Sound Sensor for Respiratory Sound Monitoring and a Comparison with Several Sensors. Sensors. 2020; 20(3):942. https://doi.org/10.3390/s20030942
Chicago/Turabian StyleJoyashiki, Takeshi, and Chikamune Wada. 2020. "Validation of a Body-Conducted Sound Sensor for Respiratory Sound Monitoring and a Comparison with Several Sensors" Sensors 20, no. 3: 942. https://doi.org/10.3390/s20030942
APA StyleJoyashiki, T., & Wada, C. (2020). Validation of a Body-Conducted Sound Sensor for Respiratory Sound Monitoring and a Comparison with Several Sensors. Sensors, 20(3), 942. https://doi.org/10.3390/s20030942