Mapping of Back Muscle Stiffness along Spine during Standing and Lying in Young Adults: A Pilot Study on Spinal Stiffness Quantification with Ultrasound Imaging



Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Instruments for Measuring Back Muscle Stiffness
2.2.1. Wireless Hand-Held Tissue Ultrasound Palpation System (TUPS)
2.2.2. Ultrasonic Scanner with Shear-Wave Elastography (SWE)
2.3. Experimental Procedure
2.4. Reliability Test
2.5. Data and Statistical Analysis
3. Results
3.1. Intra-/Inter-Rater Reliability of Measurements
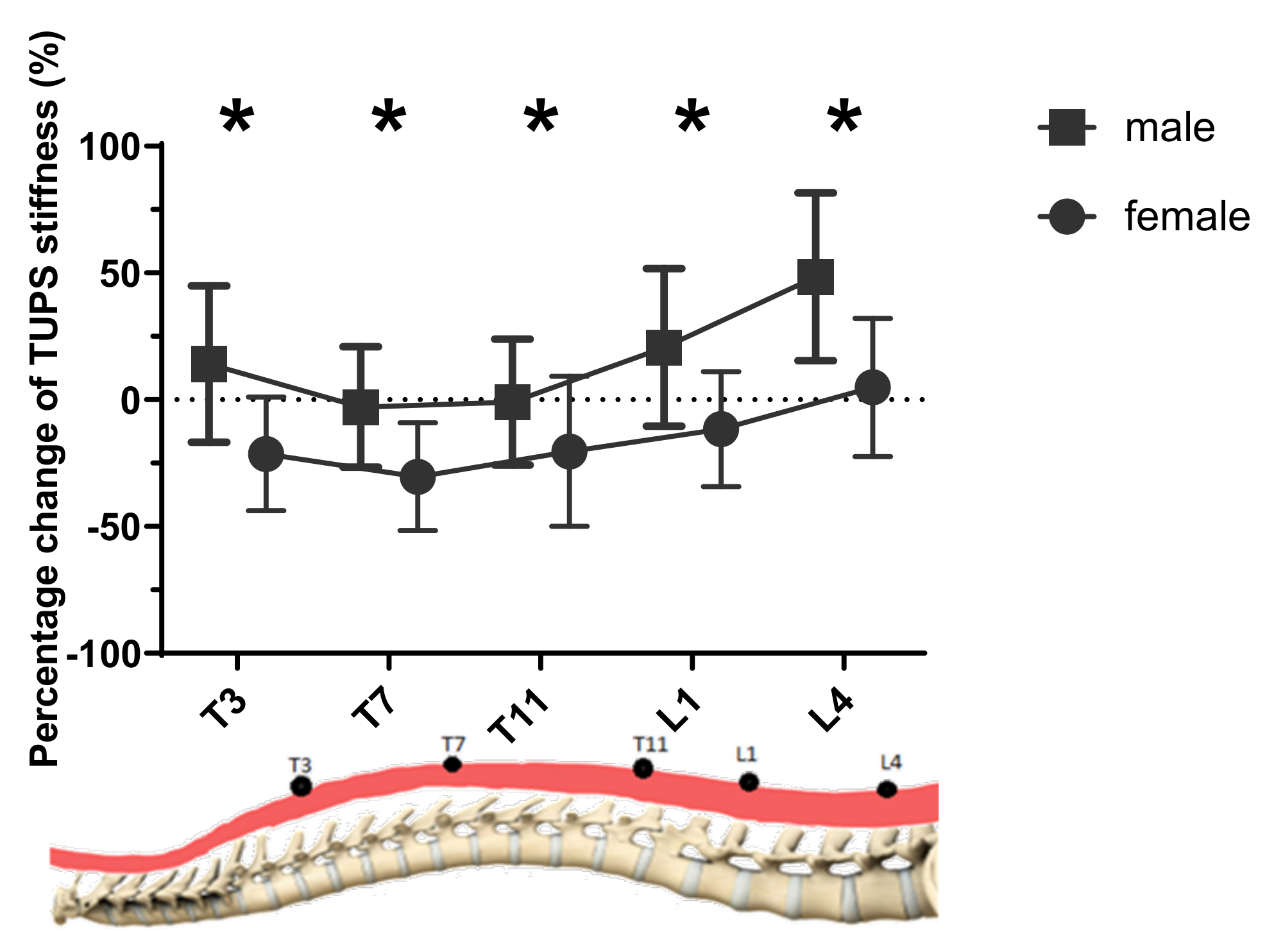
3.2. Muscle Stiffness Measured by TUPS
3.2.1. Effect of Gender
3.2.2. Effect of Level
3.2.3. Effect of Posture
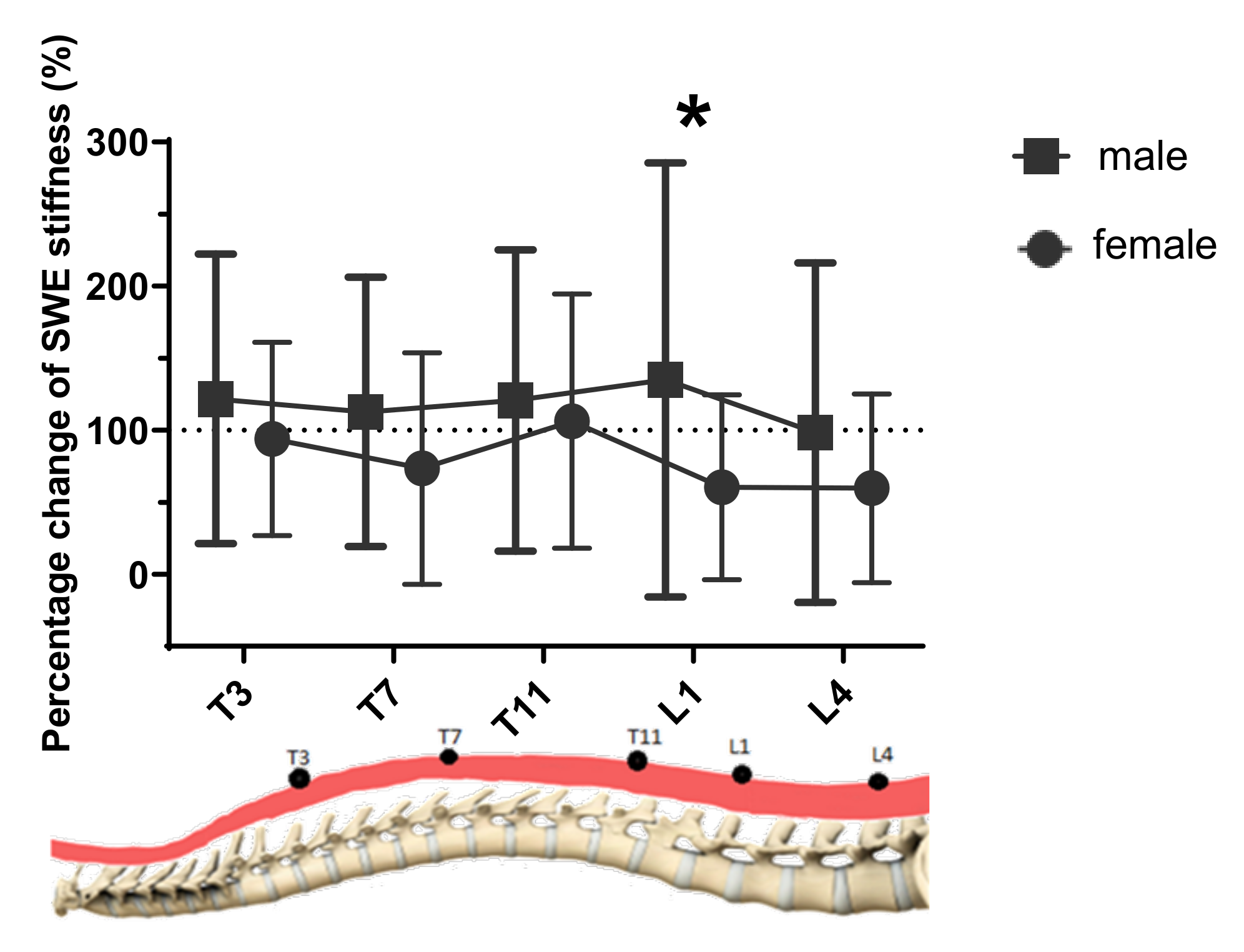
3.3. Muscle Stiffness Measured by SWE
3.3.1. Effect of Gender
3.3.2. Effect of Posture
3.3.3. Effect of Level
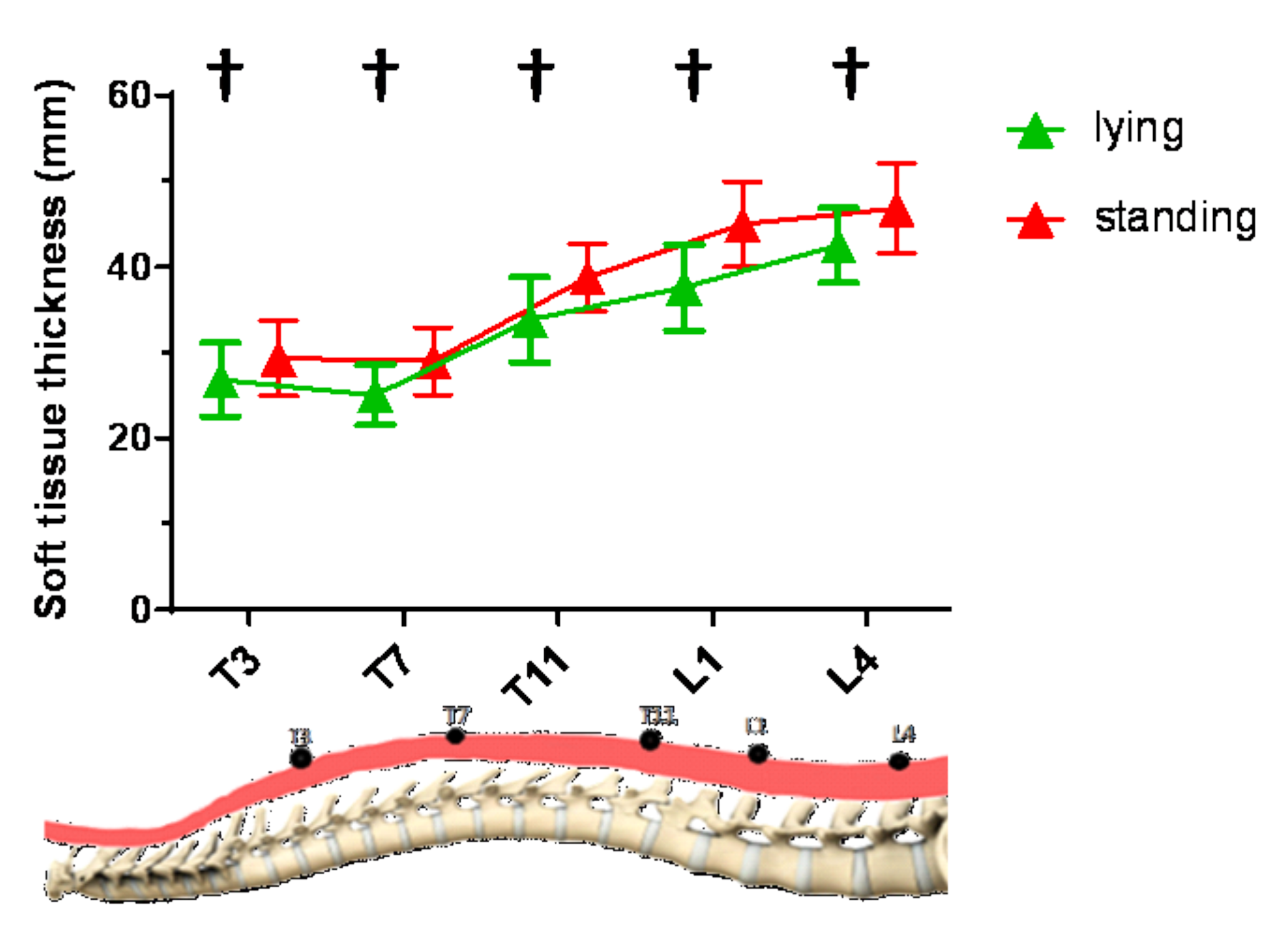
3.4. Change of Soft Tissue Thickness from Lying to Standing Posture
3.5. Relationship between the SWE and TUPS Measurement Techniques
4. Discussions
4.1. Intra-/Inter-Rater Reliability of Measurements
4.2. Effect of Level (T3, T7, T11, L1 vs. L4)
4.3. Effect of Gender (Female vs. Male)
4.4. Effect of Posture (Lying vs. Standing)
4.5. Relationship between the SWE and TUPS Measurement Techniques
4.6. Implications and Outlook
4.7. Best Practice Recommendations for the SWE and TUPS Measurement Techniques
4.8. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Weinstein, S.L.; Dolan, L.A.; Cheng, J.C.; Danielsson, A.; Morcuende, J.A. Adolescent idiopathic scoliosis. Lancet 2008, 371, 1527–1537. [Google Scholar] [CrossRef]
- Ganesan, S.; Acharya, A.S.; Chauhan, R.; Acharya, S. Prevalence and risk factors for low back pain in 1355 young adults: A cross-sectional study. Asian Spine J. 2017, 11, 610–617. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Lenke, L.G.; Bridwell, K.H.; Cheh, G.; Whorton, J.; Sides, B. Prospective pulmonary function comparison following posterior segmental spinal instrumentation and fusion of adolescent idiopathic scoliosis: Is there a relationship between major thoracic curve correction and pulmonary function test improvement? Spine 2007, 32, 2685–2693. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Llorens, J.; Ramirez, M.; Colomina, M.J.; Bago, J.; Molina, A.; Caceres, E.; Gea, J. Muscle dysfunction and exercise limitation in adolescent idiopathic scoliosis. Eur. Respir. J. 2010, 36, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.Y.; Parent, E.C.; Funabashi, M.; Kawchuk, G.N. Do changes in transversus abdominis and lumbar multifidus during conservative treatment explain changes in clinical outcomes related to nonspecific low back pain? A systematic review. J. Pain 2014, 15, 377.e1-35. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Meng, Y.; Jin, X.; Zhang, C.; Zhao, J.; Wang, C.; Gao, R.; Zhou, X. Volumetric and fatty infiltration imbalance of deep paravertebral muscles in adolescent idiopathic scoliosis. Med. Sci. Monit. 2017, 23, 2089–2095. [Google Scholar] [CrossRef]
- Liu, Y.; Pan, A.; Hai, Y.; Li, W.; Yin, L.; Guo, R. Asymmetric biomechanical characteristics of the paravertebral muscle in adolescent idiopathic scoliosis. Clin. Biomech. 2019, 65, 81–86. [Google Scholar] [CrossRef]
- Hides, J.A.; Lambrecht, G.; Stanton, W.R.; Damann, V. Changes in multifidus and abdominal muscle size in response to microgravity: Possible implications for low back pain research. Eur. Spine J. 2015, 25, 175–182. [Google Scholar] [CrossRef]
- Streisfeld, G.M.; Bartoszek, C.; Creran, E.; Inge, B.; McShane, M.D.; Johnston, T. Relationship between body positioning, muscle activity, and spinal kinematics in cyclists with and without low back pain: A systematic review. Sports Health 2017, 9, 75–79. [Google Scholar] [CrossRef]
- Fouré, A.; Nordez, A.; McNair, P.; Cornu, C. Effects of plyometric training on both active and passive parts of the plantarflexors series elastic component stiffness of muscle–tendon complex. Eur. J. Appl. Physiol. 2011, 111, 539–548. [Google Scholar] [CrossRef]
- Liew, B.X.; Netto, K.; Morris, S. Increase in leg stiffness reduces joint work during backpack carriage running at slow velocities. J. Appl. Biomech. 2017, 33, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Tisha, A.L.; Armstrong, A.A.; Johnson, A.W.; López-Ortiz, C. Skeletal muscle adaptations and passive muscle stiffness in cerebral palsy: A literature review and conceptual model. J. Appl. Biomech. 2019, 35, 68–79. [Google Scholar] [CrossRef] [PubMed]
- Lacraz, G.; Rouleau, A.-J.; Couture, V.; Söllrald, T.; Drouin, G.; Veillette, N.; Grandbois, M.; Grenier, G. Increased stiffness in aged skeletal muscle impairs muscle progenitor cell proliferative activity. PLoS ONE 2015, 10, e0136217. [Google Scholar] [CrossRef] [PubMed]
- Eby, S.F.; Cloud, B.A.; Brandenburg, J.E.; Giambini, H.; Song, P.; Chen, S.; Lebrasseur, N.K.; An, K.-N. Shear wave elastography of passive skeletal muscle stiffness: Influences of sex and age throughout adulthood. Clin. Biomech. 2015, 30, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Bailey, J.F.; Miller, S.L.; Khieu, K.; O’Neill, C.W.; Healey, R.M.; Coughlin, D.G.; Sayson, J.V.; Chang, D.G.; Hargens, A.R.; Lotz, J.C. From the international space station to the clinic: How prolonged unloading may disrupt lumbar spine stability. Spine J. 2018, 18, 7–14. [Google Scholar] [CrossRef]
- Chan, S.-T.; Fung, P.-K.; Ng, N.-Y.; Ngan, T.-L.; Chong, M.-Y.; Tang, C.-N.; He, J.-F.; Zheng, Y.-P. Dynamic changes of elasticity, cross-sectional area, and fat infiltration of multifidus at different postures in men with chronic low back pain. Spine J. 2012, 12, 381–388. [Google Scholar] [CrossRef]
- Mahaudens, P.; Detrembleur, C. Increase of passive stiffness in adolescent idiopathic scoliosis. Comput. Methods Biomech. Biomed. Eng. 2015, 18, 1992–1993. [Google Scholar] [CrossRef]
- Linek, P.; Wolny, T.; Sikora, D.; Klepek, A. Intrarater reliability of shear wave elastography for the quantification of lateral abdominal muscle elasticity in idiopathic scoliosis patients. J. Manip. Physiol. Ther. 2020, 43, 303–310. [Google Scholar] [CrossRef]
- Yamauchi, T.; Hasegawa, S.; Nakamura, M.; Nishishita, S.; Yanase, K.; Fujita, K.; Umehara, J.; Ji, X.; Ibuki, S.; Ichihashi, N. Effects of two stretching methods on shoulder range of motion and muscle stiffness in baseball players with posterior shoulder tightness: A randomized controlled trial. J. Shoulder Elb. Surg. 2016, 25, 1395–1403. [Google Scholar] [CrossRef]
- Beach, T.A.; Parkinson, R.J.; Stothart, J.P.; Callaghan, J.P. Effects of prolonged sitting on the passive flexion stiffness of the in vivo lumbar spine. Spine J. 2005, 5, 145–154. [Google Scholar] [CrossRef]
- Aslan, H.; Analan, P. Is there a correlation between Reimers’ hip migration percentage and stiffness of hip muscles measured by shear wave elastography in children with cerebral palsy? Ann. Phys. Rehabil. Med. 2018, 61, e304. [Google Scholar] [CrossRef]
- Ikezoe, T.; Asakawa, Y.; Fukumoto, Y.; Tsukagoshi, R.; Ichihashi, N. Associations of muscle stiffness and thickness with muscle strength and muscle power in elderly women. Geriatr. Gerontol. Int. 2012, 12, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, K.; Shinohara, M.; Nozaki, S.; Katayose, M. Acute decrease in the stiffness of resting muscle belly due to static stretching. Scand. J. Med. Sci. Sports 2015, 25, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Raiteri, B.J.; Hug, F.; Cresswell, A.G.; Lichtwark, G.A. Quantification of muscle co-contraction using supersonic shear wave imaging. J. Biomech. 2016, 49, 493–495. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Nordez, A.; Hug, F. Muscle shear elastic modulus measured using supersonic shear imaging is highly related to muscle activity level. J. Appl. Physiol. 2010, 108, 1389–1394. [Google Scholar] [CrossRef] [PubMed]
- Ling, Y.T.; Ma, C.Z.-H.; Shea, Q.T.K.; Zheng, Y.-P. Sonomechanomyography (SMMG): Mapping of skeletal muscle motion onset during contraction using ultrafast ultrasound imaging and multiple motion sensors. Sensors 2020, 20, 5513. [Google Scholar] [CrossRef]
- Creze, M.; Nyangoh Timoh, K.; Gagey, O.; Rocher, L.; Bellin, M.F. Soubeyrand, M. Feasibility assessment of shear wave elastography to lumbar back muscles: A radioanatomic study. Clin. Anat 2017, 30, 774–780. [Google Scholar] [CrossRef]
- Masaki, M.; Aoyama, T.; Murakami, T.; Yanase, K.; Ji, X.; Tateuchi, H.; Ichihashi, N. Association of low back pain with muscle stiffness and muscle mass of the lumbar back muscles, and sagittal spinal alignment in young and middle-aged medical workers. Clin. Biomech. 2017, 49, 128–133. [Google Scholar] [CrossRef]
- Ren, L.J.; Wang, L.K.; Ma, C.Z.-H.; Yang, Y.X.; Zheng, Y.P. Effect of conventional physiotherapy on pain and muscle stiffness in patients with low back pain assessed by a wireless hand-held tissue ultrasound palpation system (TUPS). Int. J. Phys. Med. Rehabil. 2019, 7, 1–5. [Google Scholar]
- Chao, C.Y.; Zheng, Y.-P.; Huang, Y.; Cheing, G.L.Y. Biomechanical properties of the forefoot plantar soft tissue as measured by an optical coherence tomography-based air-jet indentation system and tissue ultrasound palpation system. Clin. Biomech. 2010, 25, 594–600. [Google Scholar] [CrossRef]
- Lau, J.C.; Li-Tsang, C.W.; Zheng, Y. Application of tissue ultrasound palpation system (TUPS) in objective scar evaluation. Burns 2005, 31, 445–452. [Google Scholar] [CrossRef] [PubMed]
- Teraguchi, M.; Yoshimura, N.; Hashizume, H.; Muraki, S.; Yamada, H.; Minamide, A.; Oka, H.; Ishimoto, Y.; Nagata, K.; Kagotani, R.; et al. Prevalence and distribution of intervertebral disc degeneration over the entire spine in a population-based cohort: The Wakayama Spine Study. Osteoarthr. Cartil. 2014, 22, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; De Vito, G.; Ditroilo, M.; Delahunt, E. Effect of sex and fatigue on muscle stiffness and musculoarticular stiffness of the knee joint in a young active population. J. Sports Sci. 2017, 35, 1582–1591. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.-P.; Mak, A. An ultrasound indentation system for biomechanical properties assessment of soft tissues in-vivo. IEEE Trans. Biomed. Eng. 1996, 43, 912–918. [Google Scholar] [CrossRef]
- Zhang, M.; Zheng, Y.P.; Mak, A.F.T. Estimating the effective Young’s modulus of soft tissues from indentation tests–Nonlinear finite element analysis of effects of friction and large deformation. Med. Eng. Phys. 1997, 19, 512–517. [Google Scholar] [CrossRef]
- Zheng, Y.; Mak, A.F.; Lue, B. Objective assessment of limb tissue elasticity: Development of a manual indentation procedure. J. Rehabil. Res. Dev. 1999, 36, 71–85. [Google Scholar]
- Moreau, B.; Vergari, C.; Gad, H.; Sandoz, B.; Skalli, W.; Laporte, S. Non-invasive assessment of human multifidus muscle stiffness using ultrasound shear wave elastography: A feasibility study. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2016, 230, 809–814. [Google Scholar] [CrossRef]
- Hu, X.; Lei, D.; Li, L.; Leng, Y.; Yu, Q.; Wei, X.; Lo, W.L.A. Quantifying paraspinal muscle tone and stiffness in young adults with chronic low back pain: A reliability study. Sci. Rep. 2018, 8, 14343. [Google Scholar] [CrossRef]
- Hatta, T.; Giambini, H.; Uehara, K.; Okamoto, S.; Chen, S.; Sperling, J.W.; Itoi, E.; An, K.-N. Quantitative assessment of rotator cuff muscle elasticity: Reliability and feasibility of shear wave elastography. J. Biomech. 2015, 48, 3853–3858. [Google Scholar] [CrossRef]
- Ma, C.Z.-H.; Ling, Y.T.; Shea, Q.T.K.; Wang, L.-K.; Wang, X.-Y.; Zheng, Y.-P. Towards wearable comprehensive capture and analysis of skeletal muscle activity during human locomotion. Sensors 2019, 19, 195. [Google Scholar] [CrossRef]
- Ward, S.R.; Tomiya, A.; Regev, G.J.; Thacker, B.E.; Benzl, R.C.; Kim, C.W.; Lieber, R.L. Passive mechanical properties of the lumbar multifidus muscle support its role as a stabilizer. J. Biomech. 2009, 42, 1384–1389. [Google Scholar] [CrossRef] [PubMed]
- Young, B.A.; Koppenhaver, S.L.; Timo-Dondoyano, R.M.; Baumann, K.; Scheirer, V.F.; Wolff, A.; Sutlive, T.G.; Elliott, J.M. Ultrasound shear wave elastography measurement of the deep posterior cervical muscles: Reliability and ability to differentiate between muscle contraction states. J. Electromyogr. Kinesiol. 2020, 56, 102488. [Google Scholar] [CrossRef] [PubMed]
- Koppenhaver, S.L.; Scutella, D.; Sorrell, B.A.; Yahalom, J.; Fernández-de-las-Peñas, C.; Childs, J.D.; Shaffer, S.W.; Shinohara, M.J.C.B. Normative parameters and anthropometric variability of lumbar muscle stiffness using ultrasound shear-wave elastography. Clin. Biomech. 2019, 62, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; De Vito, G.; Ditroilo, M.; Fong, D.T.P.; Delahunt, E. A comparison of muscle stiffness and musculoarticular stiffness of the knee joint in young athletic males and females. J. Electromyogr. Kinesiol. 2015, 25, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Blackburn, J.T.; Riemann, B.L.; Padua, D.A.; Guskiewicz, K.M. Sex comparison of extensibility, passive, and active stiffness of the knee flexors. Clin. Biomech. 2004, 19, 36–43. [Google Scholar] [CrossRef]
- Bawadi, H.; Hassan, S.; Zadeh, A.S.; Sarv, H.; Kerkadi, A.; Tur, J.A.; Shi, Z. Age and gender specific cut-off points for body fat parameters among adults in Qatar. Nutr. J. 2020, 19, 1–5. [Google Scholar] [CrossRef]
- Eby, S.F.; Song, P.; Chen, S.; Chen, Q.; Greenleaf, J.F.; An, K.-N. Validation of shear wave elastography in skeletal muscle. J. Biomech. 2013, 46, 2381–2387. [Google Scholar] [CrossRef]
- Marras, W.S.; Davis, K.G.; Heaney, C.A.; Maronitis, A.B.; Allread, W.G. The influence of psychosocial stress, gender, and personality on mechanical loading of the lumbar spine. Spine 2000, 25, 3045–3054. [Google Scholar] [CrossRef]
- Marras, W.S.; Jorgensen, M.; Granata, K.; Wiand, B. Female and male trunk geometry: Size and prediction of the spine loading trunk muscles derived from MRI. Clin. Biomech. 2001, 16, 38–46. [Google Scholar] [CrossRef]
- Sichting, F.; Kram, N.C. Phantom material testing indicates that the mechanical properties, geometrical dimensions, and tensional state of tendons affect oscillation-based measurements. Physiol. Meas. 2020, 41, 095010. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lying | Standing | |||||
|---|---|---|---|---|---|---|
| Level | Male (n = 32) | Female (n = 32) | Male (n = 32) | Female (n = 32) | p-Value | Partial Eta Squared, ηp2 |
| T3 | 172.0 ± 42.8 † | 166.5 ± 46.4 † | 192.3 ± 55.7 *† | 122.7 ± 27.8 *† | Main effect: | |
| Gender: <0.001 | 0.292 | |||||
| T7 | 157.8 ± 32.5 | 155.8 ± 45.2 † | 150.8 ± 36.9 * | 104.9 ± 26.7 *† | Posture: 0.707 | 0.002 |
| Level: <0.001 | 0.601 | |||||
| T11 | 153.3 ± 27.0 | 144.4 ± 36.1 | 148.3 ± 32.0 * | 111.3 ± 37.6 * | Interaction effect: | |
| Gender * level:<0.001 | 0.111 | |||||
| L1 | 162.1 ± 29.0 † | 168.3 ± 48.4 † | 194.7 ± 55.7 *† | 137.5 ± 36.0 *† | Gender * posture: <0.001 | 0.481 |
| Posture * level: <0.001 | 0.355 | |||||
| L4 | 205.5 ± 36.2 † | 182.7 ± 45.2 † | 303.3 ± 80.6 *† | 180.5 ± 46.7 *† | Gender * level * posture: <0.001 | 0.069 |
| Lying | Standing | |||||
|---|---|---|---|---|---|---|
| Level | Male (n = 32) | Female (n = 32) | Male (n = 32) | Female (n = 32) | p-Value | Partial Eta Squared, ηp2 |
| T3 | 21.8 ± 8.3 *† | 17.8 ± 6.8 *† | 45.5 ± 20.0 *† | 33.7 ± 17.4 *† | Main effect: | |
| Gender: 0.030 | 0.074 | |||||
| T7 | 23.8 ± 5.3 † | 23.1 ± 5.2 † | 47.0 ± 16.2 *† | 37.9 ± 13.6 *† | Posture: <0.001 | 0.772 |
| Level: 0.120 | 0.029 | |||||
| T11 | 22.5 ± 8.4 † | 23.3 ± 7.1 † | 43.7 ± 14.7 † | 44.5 ± 15.1 † | Interaction effect: | |
| Gender * level: 0.080 | 0.033 | |||||
| L1 | 21.1 ± 6.0 † | 24.3 ± 7.9 † | 45.2 ± 21.6 † | 38.3 ± 18.8 † | Gender * posture: 0.016 | 0.090 |
| Posture * level: 0.171 | 0.025 | |||||
| L4 | 24.1 ± 9.3 † | 23.3 ± 7.5 † | 42.0 ± 18.9 † | 35.2 ± 13.7 † | Gender * level * posture: 0.360 | 0.017 |
| Pearson’s Correlation Coefficient (r) | ||
|---|---|---|
| Level | Lying | Standing |
| T3 | −0.294 * | 0.111 |
| T7 | 0.196 | 0.232 |
| T11 | −0.141 | 0.166 |
| L1 | 0.020 | 0.390 * |
| L4 | −0.233 | 0.358 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, C.Z.-H.; Ren, L.-J.; Cheng, C.L.-K.; Zheng, Y.-P. Mapping of Back Muscle Stiffness along Spine during Standing and Lying in Young Adults: A Pilot Study on Spinal Stiffness Quantification with Ultrasound Imaging. Sensors 2020, 20, 7317. https://doi.org/10.3390/s20247317
Ma CZ-H, Ren L-J, Cheng CL-K, Zheng Y-P. Mapping of Back Muscle Stiffness along Spine during Standing and Lying in Young Adults: A Pilot Study on Spinal Stiffness Quantification with Ultrasound Imaging. Sensors. 2020; 20(24):7317. https://doi.org/10.3390/s20247317
Chicago/Turabian StyleMa, Christina Zong-Hao, Long-Jun Ren, Connie Lok-Kan Cheng, and Yong-Ping Zheng. 2020. "Mapping of Back Muscle Stiffness along Spine during Standing and Lying in Young Adults: A Pilot Study on Spinal Stiffness Quantification with Ultrasound Imaging" Sensors 20, no. 24: 7317. https://doi.org/10.3390/s20247317
APA StyleMa, C. Z.-H., Ren, L.-J., Cheng, C. L.-K., & Zheng, Y.-P. (2020). Mapping of Back Muscle Stiffness along Spine during Standing and Lying in Young Adults: A Pilot Study on Spinal Stiffness Quantification with Ultrasound Imaging. Sensors, 20(24), 7317. https://doi.org/10.3390/s20247317