Analyzing Facial and Eye Movements to Screen for Alzheimer’s Disease


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Ethical Considerations
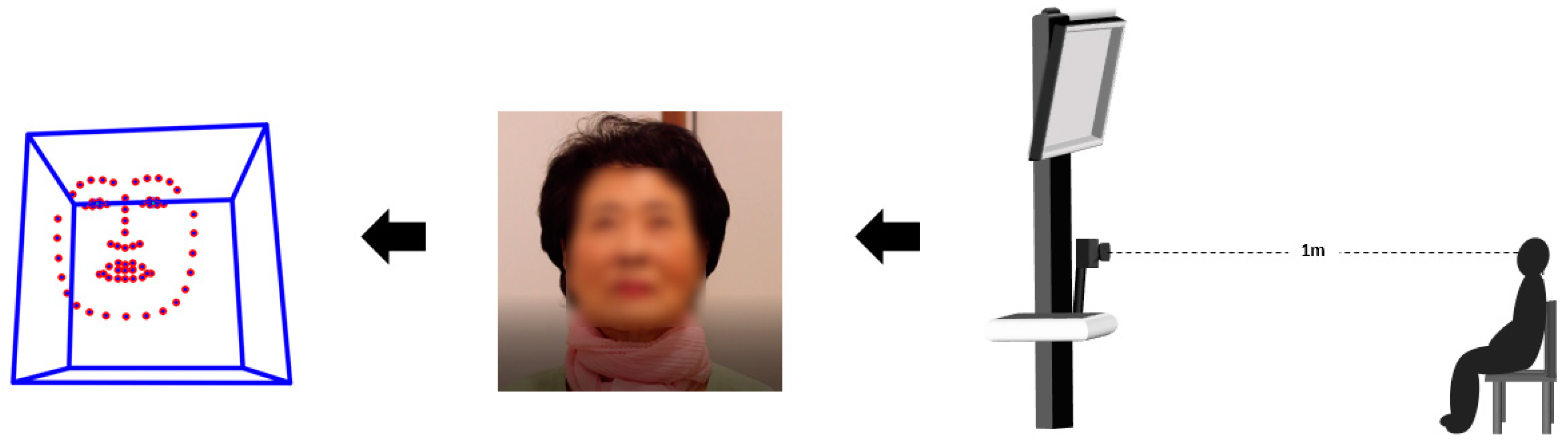
2.3. Experimental Configuration
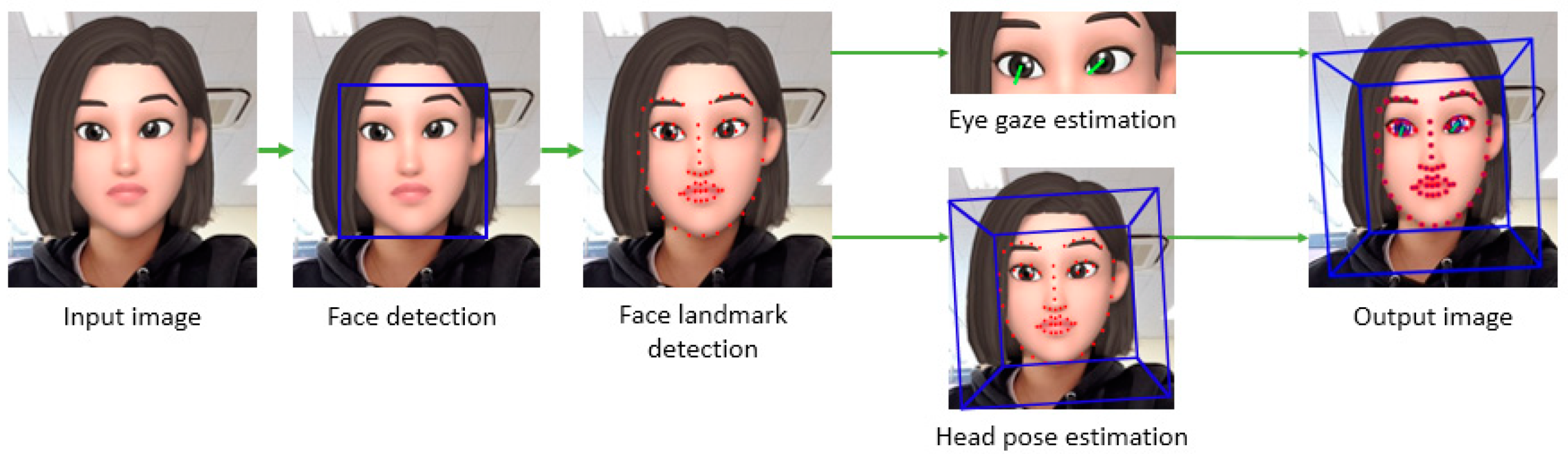
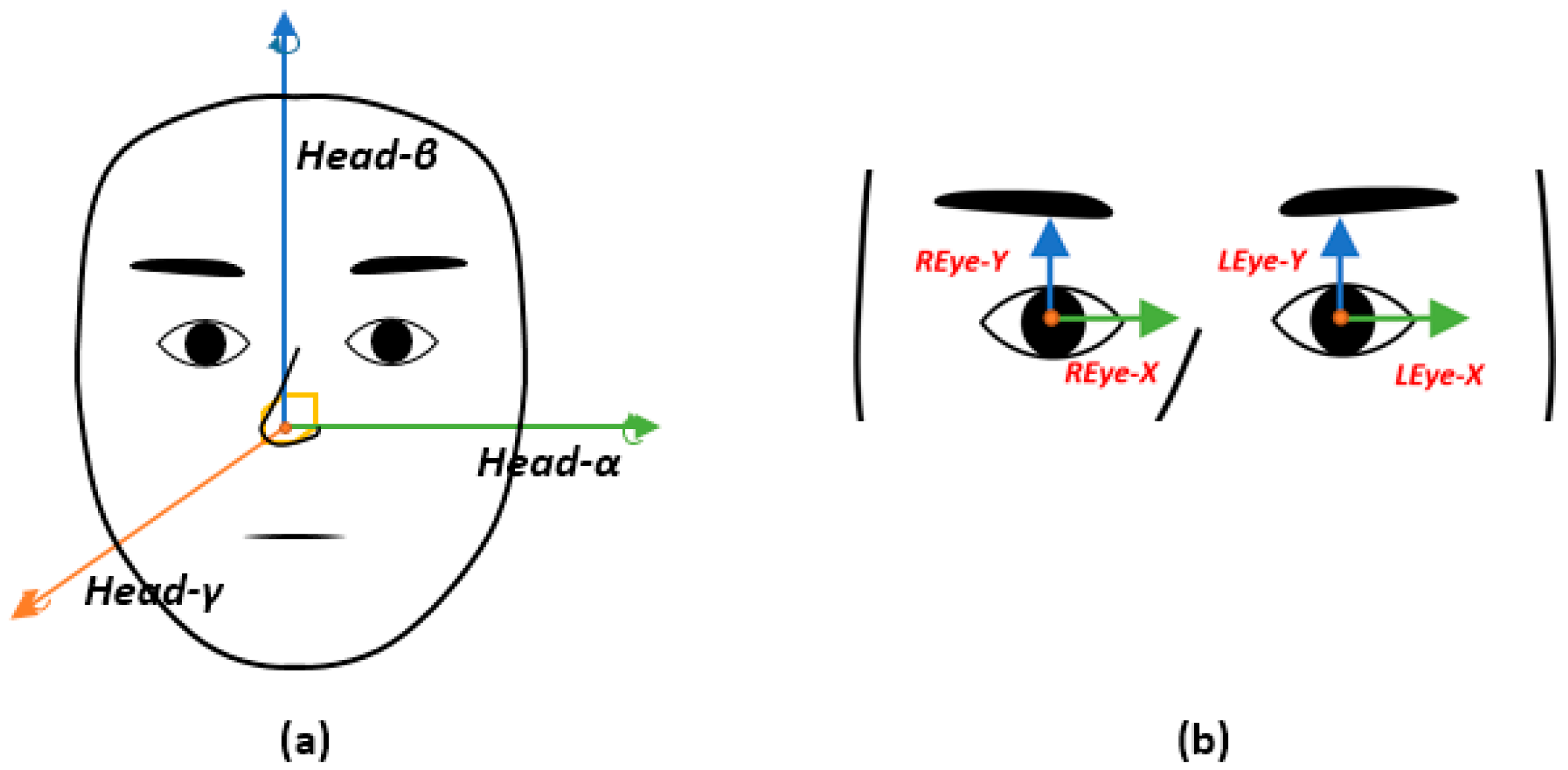
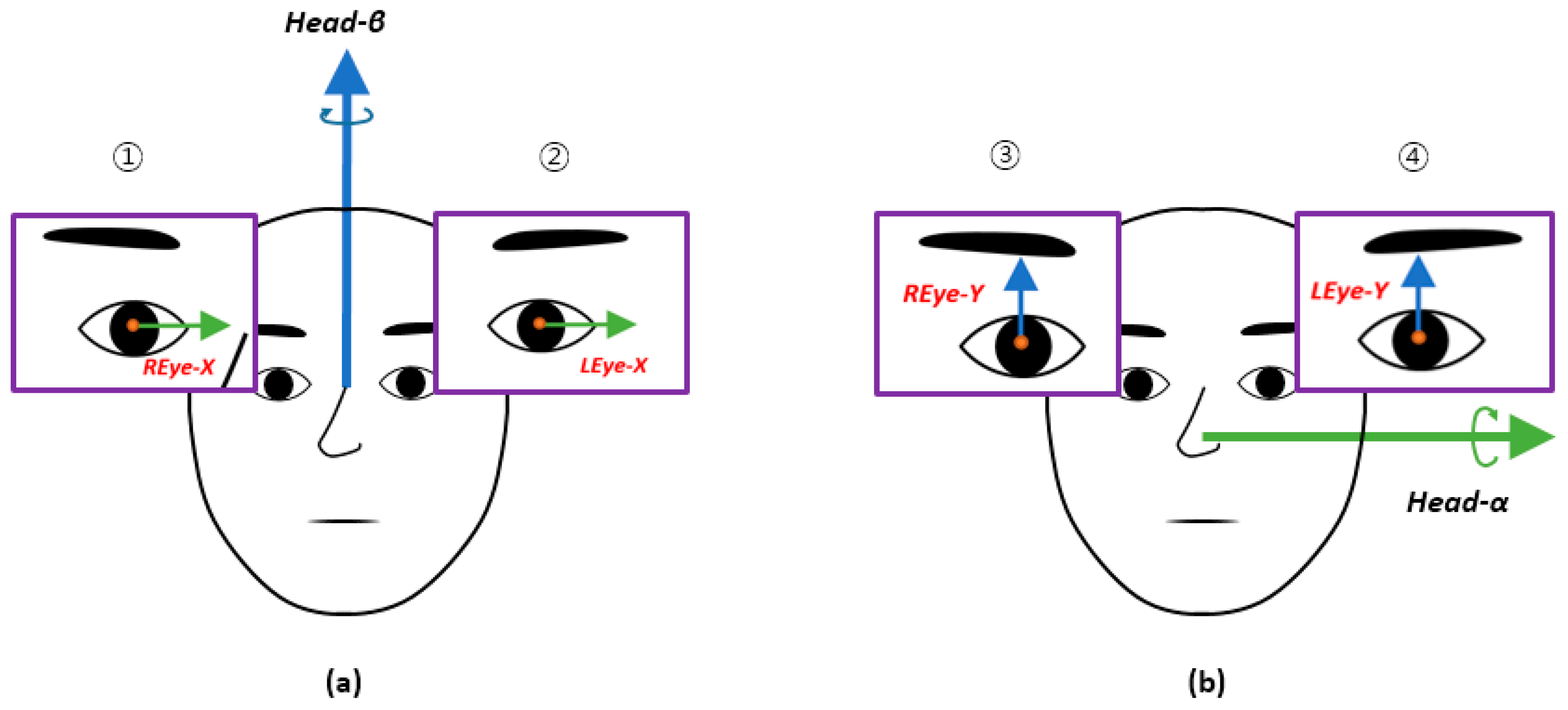
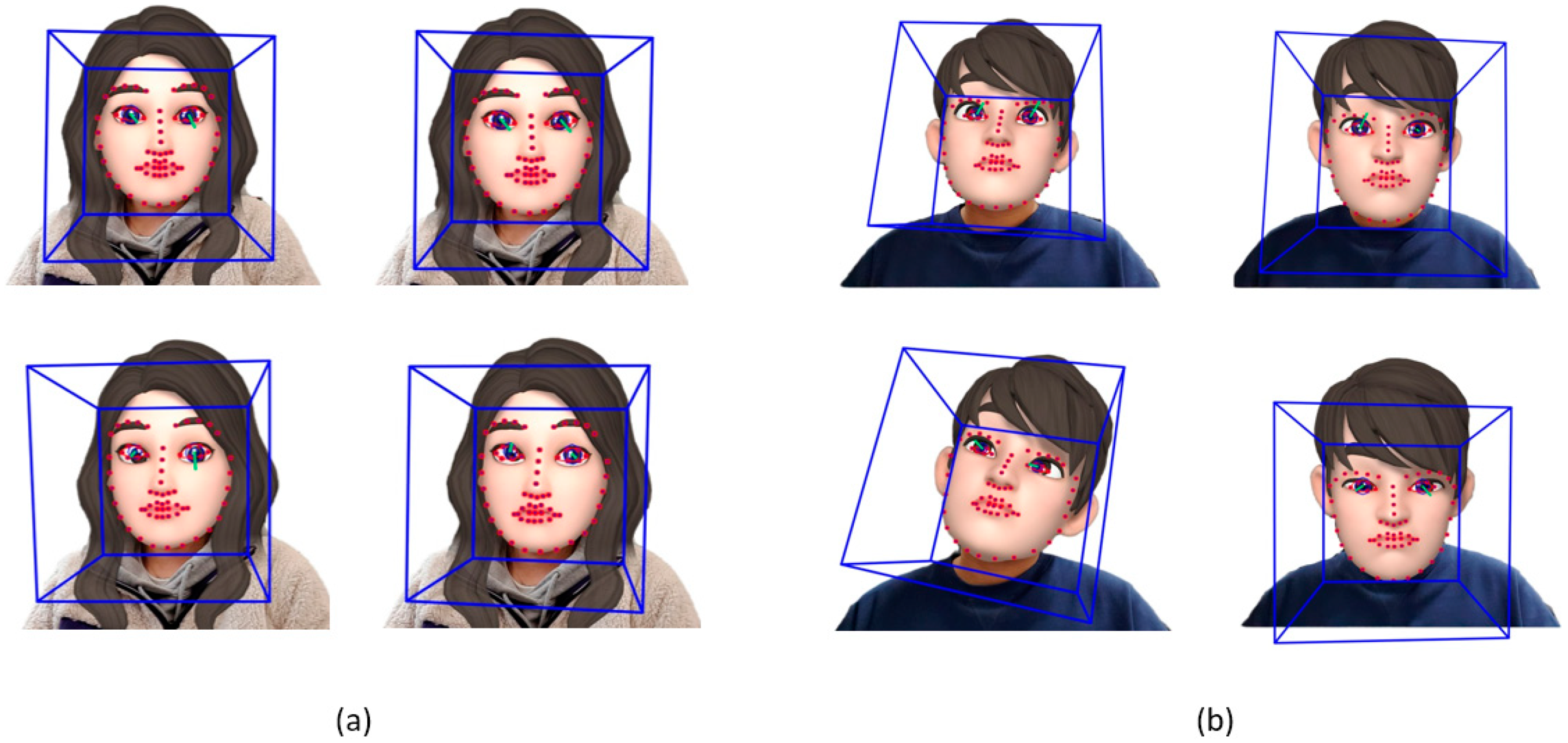
2.4. Image Analysis
2.5. Statistical Analysis
2.5.1. Spearman’s Correlation Coefficients of Facial and Eye Movements
2.5.2. Mann–Whitney–Wilcoxon Test of the Spearman’s Correlation Coefficient
3. Results
4. Discussion and Conclusions
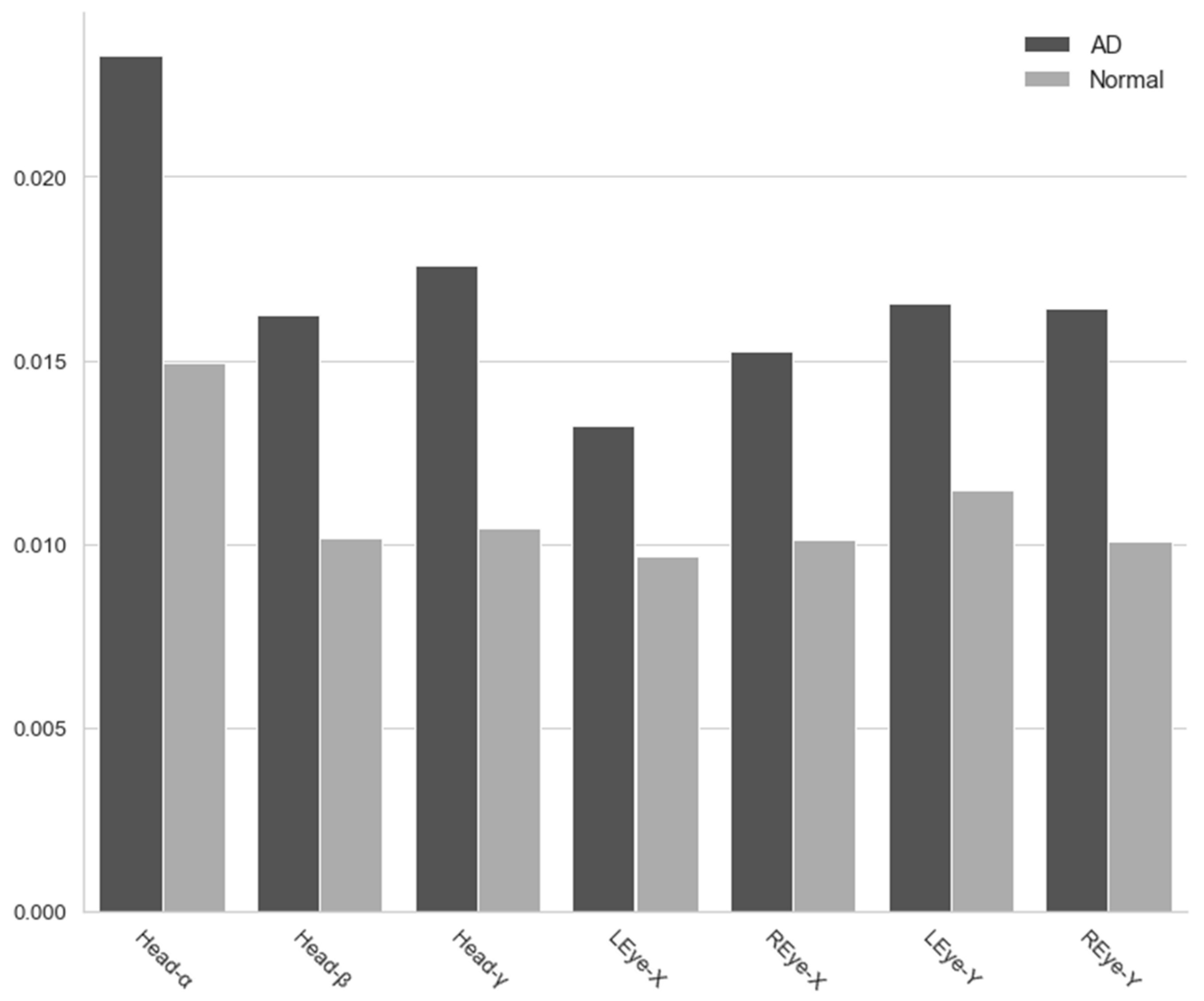
4.1. Variance for Movement in All Directions
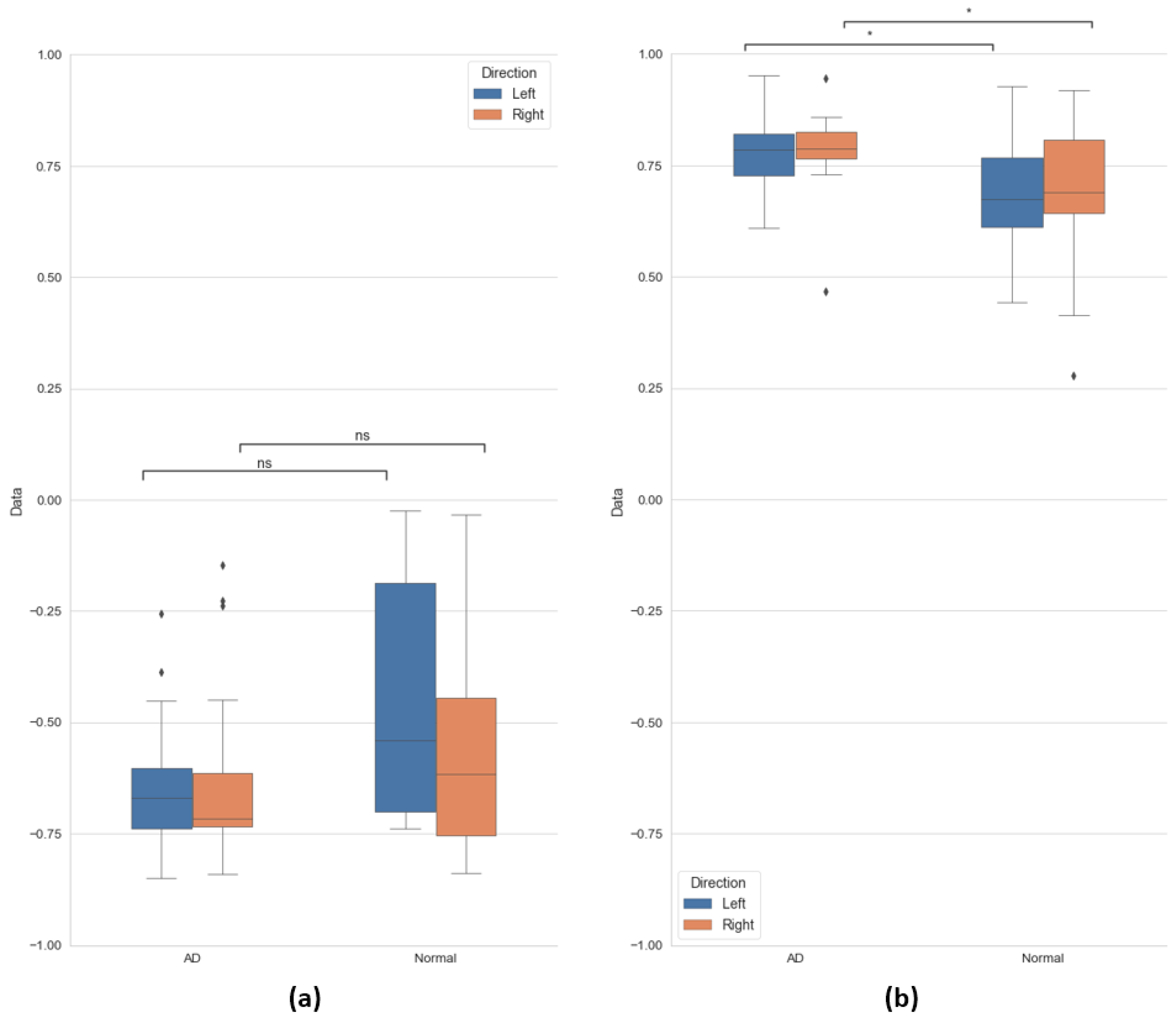
4.2. Correlation in Vertical Direction between Face and Eye Movements
4.3. Limitations and Future Directions
4.4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Powell, J.L. The power of global aging. Ageing Int. 2010, 35, 1–14. [Google Scholar] [CrossRef]
- Wimo, A.; Guerchet, M.; Ali, G.C.; Wu, Y.T.; Prina, A.M.; Winblad, B.; Jönsson, L.; Liu, Z.; Prince, M. The worldwide costs of dementia 2015 and comparisons with 2010. Alzheimer’s Dement. 2017, 13, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Mansfield, J.; Golander, H.; Arnheim, G. Self-identity in older persons suffering from dementia: Preliminary results. Soc. Sci. Med. 2000, 51, 381–394. [Google Scholar] [CrossRef]
- Lu, Y.; Zheng, W.L.; Li, B.; Lu, B.L. Combining Eye Movements and EEG to Enhance Emotion Recognition. In Proceedings of the Twenty-Fourth International Joint Conference on Artificial Intelligence, Buenos Aires, Argentina, 25–31 July 2015. [Google Scholar]
- Schurgin, M.W.; Nelson, J.; Iida, S.; Ohira, H.; Chiao, J.Y.; Franconeri, S.L. Eye movements during emotion recognition in faces. J. Vis. 2014, 14, 14. [Google Scholar] [CrossRef]
- Kojima, T.; Matsushima, E.; Ohta, K.; Toru, M.; Han, Y.H.; Shen, Y.C.; Moussaoui, D.; David, I.; Sato, K.; Kathmann, N.; et al. Stability of exploratory eye movements as a marker of schizophrenia—A WHO multi-center study. Schizophr. Res. 2001, 52, 203–213. [Google Scholar] [CrossRef]
- Rosen, H.J.; Gorno-Tempini, M.L.; Goldman, W.P.; Perry, R.J.; Schuff, N.; Weiner, M.; Feiwell, R.; Karmer, J.H.; Miller, B.L. Patterns of brain atrophy in frontotemporal dementia and semantic dementia. Neurology 2002, 58, 198–208. [Google Scholar] [CrossRef]
- Aarsland, D. Cognitive impairment in Parkinson’s disease and dementia with Lewy bodies. Parkinsonism Relat. Disord. 2016, 22, S144–S148. [Google Scholar] [CrossRef]
- Brahm, K.D.; Wilgenburg, H.M.; Kirby, J.; Ingalla, S.; Chang, C.Y.; Goodrich, G.L. Visual impairment and dysfunction in combat-injured servicemembers with traumatic brain injury. Optom. Vis. Sci. 2009, 86, 817–825. [Google Scholar] [CrossRef]
- Downs, M.G. The role of general practice and the primary care team in dementia diagnosis and management. Int. J. Geriatr. Psychiatry 1996, 11, 937–942. [Google Scholar] [CrossRef]
- Hess, E.H.; Polt, J.M. Pupil size in relation to mental activity during simple problem-solving. Science 1964, 143, 1190–1192. [Google Scholar] [CrossRef]
- Iqbal, S.T.; Zheng, X.S.; Bailey, B.P. Task-Evoked Pupillary Response to Mental Workload in Human-Computer Interaction. In Proceedings of the CHI ‘04 Extended Abstracts on Human Factors in Computing Systems, Vienna, Austria, 24–29 April 2004; pp. 1477–1480. [Google Scholar]
- Marshall, S.P. Identifying cognitive state from eye metrics. Aviat. Space Environ. Med. 2007, 78, B165–B175. [Google Scholar] [PubMed]
- Adoni, A.; McNett, M. The pupillary response in traumatic brain injury: A guide for trauma nurses. J. Trauma Nurs. 2007, 14, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Kuchinke, L.; Trapp, S.; Jacobs, A.M.; Leder, H. Pupillary responses in art appreciation: Effects of aesthetic emotions. Psychol. Aesthet. Creat. Arts 2009, 3, 156. [Google Scholar] [CrossRef]
- Kimble, M.O.; Fleming, K.; Bandy, C.; Kim, J.; Zambetti, A. Eye tracking and visual attention to threatening stimuli in veterans of the Iraq war. J. Anxiety Disord. 2010, 24, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Granholm, E.L.; Panizzon, M.S.; Elman, J.A.; Jak, A.J.; Hauger, R.L.; Bondi, M.W.; Lyons, M.J.; Franz, C.E.; Kremen, W.S. Pupillary responses as a biomarker of early risk for Alzheimer’s disease. J. Alzheimer’s Dis. 2017, 56, 1419–1428. [Google Scholar] [CrossRef]
- Weeks, J.W.; Howell, A.N.; Srivastav, A.; Goldin, P.R. “Fear guides the eyes of the beholder”: Assessing gaze avoidance in social anxiety disorder via covert eye tracking of dynamic social stimuli. J. Anxiety Disord. 2019, 65, 56–63. [Google Scholar] [CrossRef]
- Zhang, Y.; Wilcockson, T.; Kim, K.I.; Crawford, T.; Gellersen, H.; Sawyer, P. Monitoring dementia with automatic eye movements analysis. Intell. Decis. Technol. 2016, 57, 299–309. [Google Scholar]
- Dham, S.; Sharma, A.; Dhall, A. Depression scale recognition from audio, visual and text analysis. arXiv 2017, arXiv:1709.05865. [Google Scholar]
- McKhann, G.; Drachman, D.; Folstein, M.; Katzman, R.; Price, D.; Stadlan, E.M. Clinical diagnosis of Alzheimer’s disease: Report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology 1984, 34, 939–944. [Google Scholar] [CrossRef]
- Morris, J.C. The Clinical Dementia Rating (CDR): Current version and scoring rules. Neurology 1993, 43, 2412–2414. [Google Scholar] [CrossRef]
- Baltrušaitis, T.; Zadeh, A.; Lim, Y.C.; Morency, L.P. OpenFace 2.0: Facial Behavior Analysis Toolkit. In Proceedings of the 13th IEEE International Conference on Automatic Face & Gesture Recognition (FG 2018), Xi’an, China, 15–19 May 2018. [Google Scholar]
- Cao, Z.; Simon, T.; Wei, S.E.; Sheikh, Y. Realtime Multi-Person 2d Pose Estimation Using Part Affinity Fields. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR 2017), San Juan, Puerto Rico, 22–25 July 2017; pp. 7291–7299. [Google Scholar]
- Zadeh, A.; Lim, Y.C.; Baltrušaitis, T.; Morency, L.P. Convolutional Experts Constrained Local Model for 3D Facial Landmark Detection. In Proceedings of the IEEE International Conference on Computer Vision Workshops (ICCVW), Venice, Italy, 22–29 October 2017; pp. 2519–2528. [Google Scholar]
- Baltrusaitis, T.; Robinson, P.; Morency, L.P. Constrained Local Neural Fields for Robust Facial Landmark Detection in the Wild. In Proceedings of the IEEE International Conference on Computer Vision Workshops (ICCVW), Sydney, Australia, 1–8 December 2013; pp. 354–361. [Google Scholar]
- Wood, E.; Baltrusaitis, T.; Zhang, X.; Sugano, Y.; Robinson, P.; Bulling, A. Rendering of Eyes for Eye-Shape Registration and Gaze Estimation. In Proceedings of the IEEE International Conference on Computer Vision (ICCV), Santiago, Chile, 7–13 December 201; pp. 3756–3764.
- Mashiko, T.; Umeda, T.; Nakaji, S.; Sugawara, K. Position related analysis of the appearance of and relationship between post-match physical and mental fatigue in university rugby football players. Br. J. Sports Med. 2004, 38, 617–621. [Google Scholar] [CrossRef] [PubMed]
- Xiao, C.; Ye, J.; Esteves, R.M.; Rong, C. Using Spearman’s correlation coefficients for exploratory data analysis on big dataset. Concurr. Comput. Pract. Exp. 2016, 28, 3866–3878. [Google Scholar] [CrossRef]
- Martínez-Murcia, F.J.; Górriz, J.M.; Ramirez, J.; Puntonet, C.G.; Salas-Gonzalez, D. Alzheimer’s Disease Neuroimaging Initiative. Computer aided diagnosis tool for Alzheimer’s disease based on Mann–Whitney–Wilcoxon U-test. Expert Syst. Appl. 2012, 39, 9676–9685. [Google Scholar] [CrossRef]
- Lilliefors, H.W. On the Kolmogorov-Smirnov test for normality with mean and variance unknown. J. Am. Stat. Assoc. 1967, 62, 399–402. [Google Scholar] [CrossRef]
- Jin, Z.; Reeves, A. Attentional release in the saccadic gap effect. Vis. Res. 2009, 49, 2045–2055. [Google Scholar] [CrossRef]
- Moser, A.; Kömpf, D.; Olschinka, J. Eye movement dysfunction in dementia of the Alzheimer type. Dementia 1995, 6, 264–268. [Google Scholar] [CrossRef]
- Garbutt, S.; Matlin, A.; Hellmuth, J.; Schenk, A.K.; Johnson, J.K.; Rosen, H.; Dean, D.; Kramer, J.; Neuhaus, J.; Miller, B.L.; et al. Oculomotor function in frontotemporal lobar degeneration, related disorders and Alzheimer’s disease. Brain 2008, 131, 1268–1281. [Google Scholar] [CrossRef]
- Antoniades, C.A.; Kennard, C. Ocular motor abnormalities in neurodegenerative disorders. Eye 2015, 29, 200–207. [Google Scholar] [CrossRef]
- Scinto, L.F.; Daffner, K.R.; Castro, L.; Weintraub, S.; Vavrik, M.; Mesulam, M.M. Impairment of spatially directed attention in patients with probable Alzheimer’s disease as measured by eye movements. Arch. Neurol. 1994, 51, 682–688. [Google Scholar] [CrossRef]
- Mosimann, U.P.; Müri, R.M.; Burn, D.J.; Felblinger, J.; O’Brien, J.T.; McKeith, I.G. Saccadic eye movement changes in Parkinson’s disease dementia and dementia with Lewy bodies. Brain 2005, 128, 1267–1276. [Google Scholar] [CrossRef]
- Williams, D.R.; Lees, A.J. Progressive supranuclear palsy: Clinicopathological concepts and diagnostic challenges. Lancet Neurol. 2009, 8, 270–279. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | AD (n = 17) | Normal (n = 17) | ||||
|---|---|---|---|---|---|---|
| Mean | SD | % | Mean | SD | % | |
| Age | 77.23 | 6.79 | - | 74 | 6.53 | - |
| Education 1 | 9.7 | 3.94 | - | 10.94 | 5.06 | - |
| Gender 2 | - | - | 47/53 | - | - | 41/59 |
| MMSE | 20.12 | 5.28 | 27 | 2.85 | ||
| Horizontal (a) | Vertical (b) | |||||||
|---|---|---|---|---|---|---|---|---|
| Direction | Left | Right | Left | Right | ||||
| Group | AD | Normal | AD | Normal | AD | Normal | AD | Normal |
| Median | −0.669 | −0.54 | −0.716 | −0.616 | 0.785 | 0.673 | 0.788 | 0.69 |
| IQR | 0.135 | 0.515 | 0.118 | 0.309 | 0.092 | 0.156 | 0.06 | 0.163 |
| Mean SD | −0.639 0.162 | −0.467 0.219 | −0.62 0.25 | −0.557 0.223 | 0.787 0.08 | 0.681 0.132 | 0.783 0.157 | 0.68 0.096 |
| MWW | U | Sig | U | Sig | U | Sig | U | Sig |
| 91 | 0.067 | 120 | 0.408 | 213 | 0.019 (*) | 210 | 0.025 (*) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nam, U.; Lee, K.; Ko, H.; Lee, J.-Y.; Lee, E.C. Analyzing Facial and Eye Movements to Screen for Alzheimer’s Disease. Sensors 2020, 20, 5349. https://doi.org/10.3390/s20185349
Nam U, Lee K, Ko H, Lee J-Y, Lee EC. Analyzing Facial and Eye Movements to Screen for Alzheimer’s Disease. Sensors. 2020; 20(18):5349. https://doi.org/10.3390/s20185349
Chicago/Turabian StyleNam, Uiseo, Kunyoung Lee, Hyunwoong Ko, Jun-Young Lee, and Eui Chul Lee. 2020. "Analyzing Facial and Eye Movements to Screen for Alzheimer’s Disease" Sensors 20, no. 18: 5349. https://doi.org/10.3390/s20185349
APA StyleNam, U., Lee, K., Ko, H., Lee, J.-Y., & Lee, E. C. (2020). Analyzing Facial and Eye Movements to Screen for Alzheimer’s Disease. Sensors, 20(18), 5349. https://doi.org/10.3390/s20185349