On-Chip Selective Capture and Detection of Magnetic Fingerprints of Malaria

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
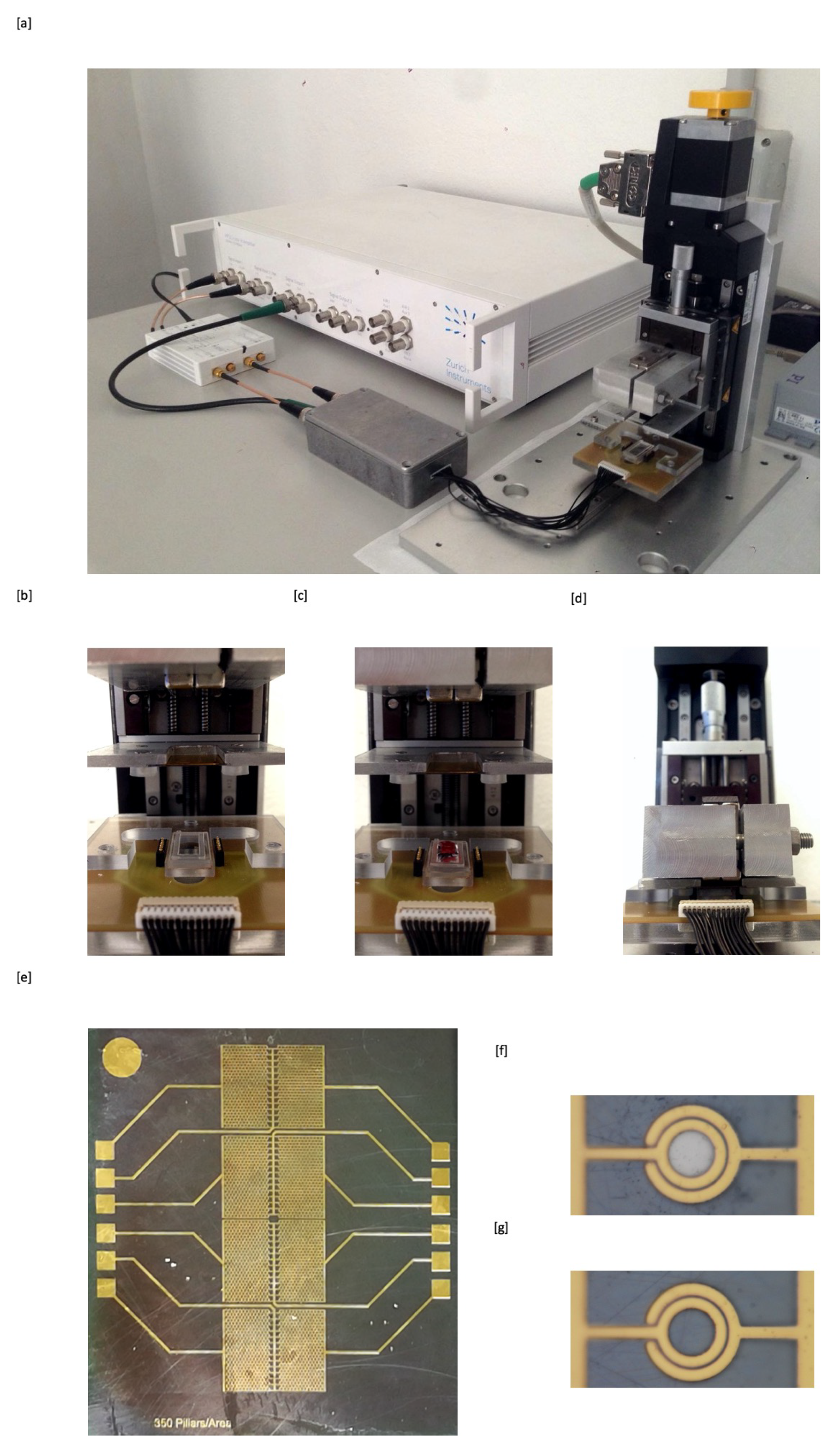
2.1. Measurement Setup
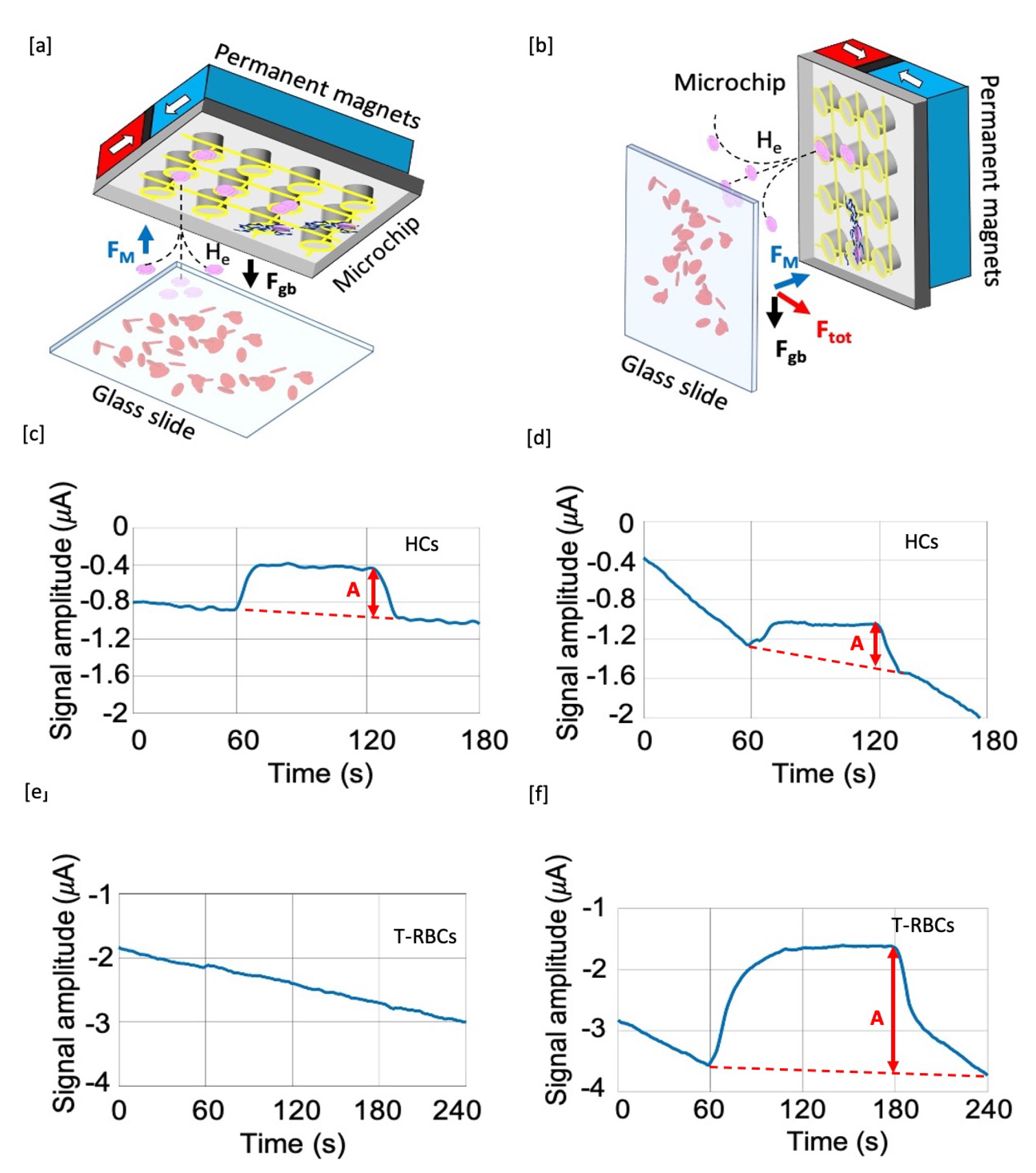
2.2. Experimental Configurations
2.3. Estimation of the Magnetic Field Gradient Needed for Magnetophoretic Separation of Blood Corpuscles
2.4. Red Blood Cells Treatment Protocol
3. Results and Discussion
3.1. Test Selectivity
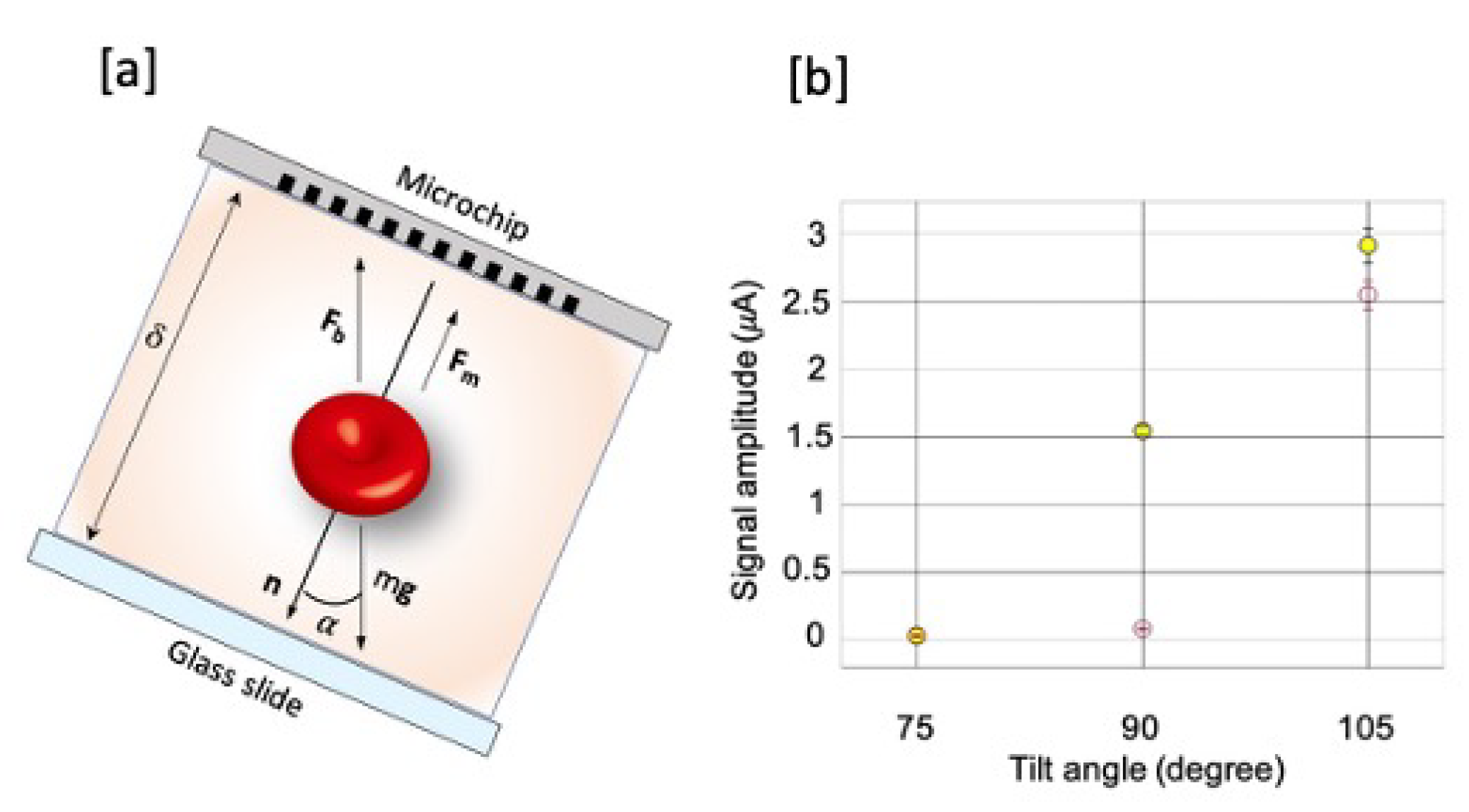
3.2. Detection Efficiency versus the Angle between the Chip Normal and Gravity
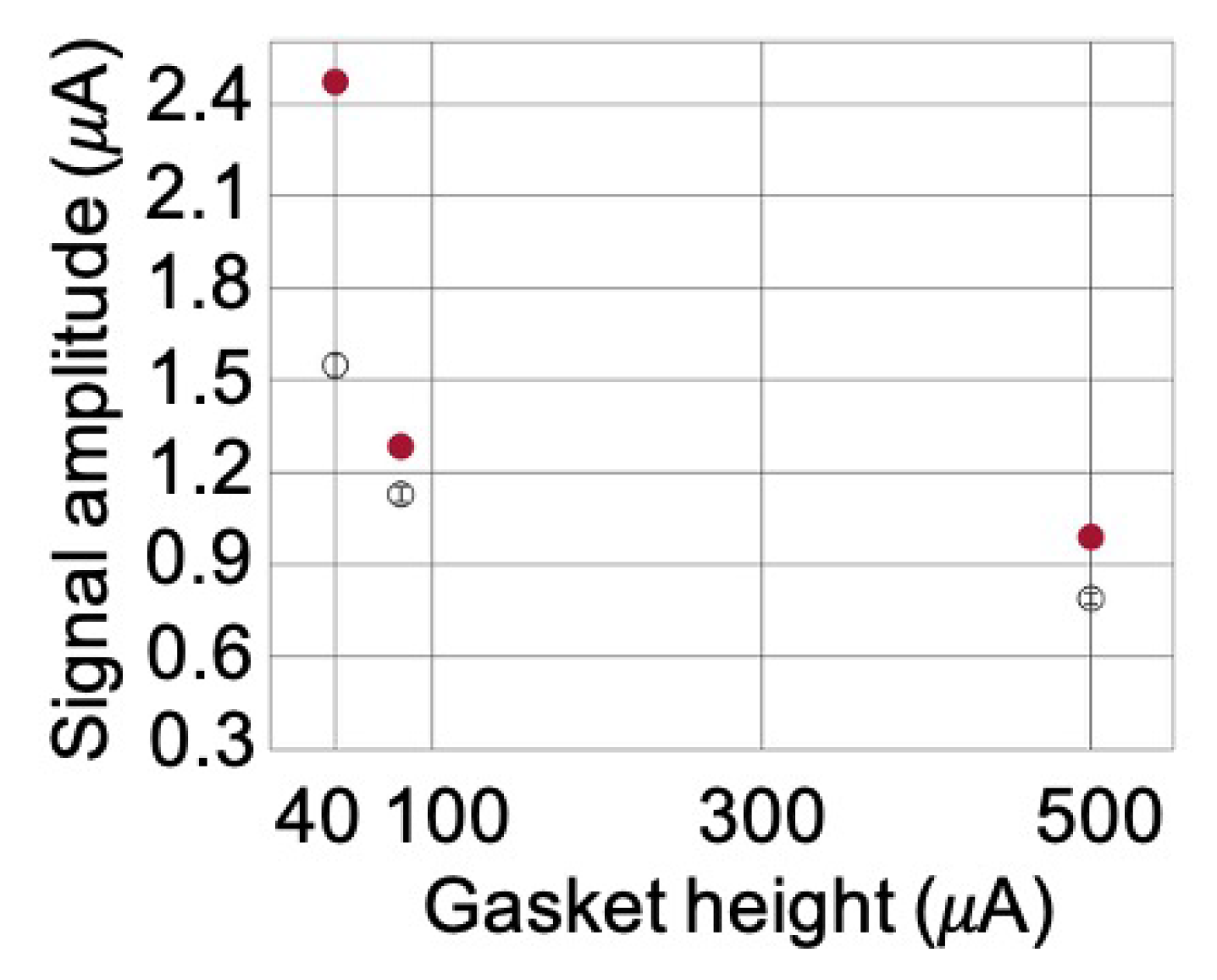
3.3. Optimization of the Microfluidic Chamber Thickness
4. Conclusions
5. Patents
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Malaria Report 2018—World Health Organisation; World Health Organization: Geneva, Switzerland, 2018.
- Adepoju, P. RTS, S malaria vaccine pilots in three African countries. Lancet 2019, 393, 1685. [Google Scholar] [CrossRef]
- World Health Organization. WHO Malaria Policy Advisory Committee MPAC Meeting: Meeting Report. April 2019. Available online: https://apps.who.int/iris/handle/10665/312198 (accessed on 31 August 2020).
- Yerlikaya, S.; Campillo, A.; Gonzalez, J. A systematic review: Performance of rapid diagnostic tests for the detection of Plasmodium knowlesi, Plasmodium malariae, and Plasmodium ovale monoinfections in human blood. J. Infect. Dis. 2018, 218, 265–276. [Google Scholar] [CrossRef]
- Lucchi, N.W.; Gaye, M.; Diallo, M.A.; Goldman, I.F.; Ljolje, D.; Deme, A.B.; Badiane, A.; Ndiaye, Y.D.; Barnwell, J.W.; Udhayakumar, V.; et al. Evaluation of the Illumigene Malaria LAMP: A Robust Molecular Diagnostic Tool for Malaria Parasites. Sci. Rep. 2016, 6, 36808. [Google Scholar] [CrossRef] [PubMed]
- Giacometti, M.; Rinaldi, C.; Monticelli, M.; Callegari, L.; Collovini, A.N.; Petti, D.; Ferrari, G.; Bertacco, R. Electrical and magnetic properties of hemozoin nanocrystals. Appl. Phys. Lett. 2018, 113, 203703. [Google Scholar] [CrossRef]
- Rosenthal, P.J.; Meshnick, S.R. Hemoglobin catabolism and iron utilization by malaria parasites. Mol. Biochem. Parasitol. 1996, 83, 131–139. [Google Scholar] [CrossRef]
- Esposito, A.; Tiffert, T.; Mauritz, J.M.; Schlachter, S.; Bannister, L.H.; Kaminski, C.F.; Lew, V.L. FRET imaging of hemoglobin concentration in Plasmodium falciparum-infected red cells. PLoS ONE 2008, 11, e3780. [Google Scholar] [CrossRef] [PubMed]
- Fitch, C.D.; Chevli, R.; Kanjananggulpan, P.; Dutta, P.; Chevli, K.; Chou, A.C. Intracellular ferriprotopor-phyrin IX is a lytic agent. Blood 1983, 62, 1165–1168. [Google Scholar] [CrossRef]
- Fitch, C.D.; Kanjananggulpan, P. The state of ferriprotoporphyrin IX in malaria pigment. J. Biol. Chem. 1987, 262, 15552–15555. [Google Scholar]
- Pagola, S.; Stephens, P.W.; Bohle, D.S.; Kosar, A.D.; Madsen, S.K. The structure of malaria pigment ß-haematin. Nature 2000, 6775, 307–310. [Google Scholar] [CrossRef]
- Hempelmann, E. Hemozoin biocrystallization in Plasmodium falciparum and the antimalarial activity of crystallization inhibitors. Parasitol. Res. 2007, 100, 671–676. [Google Scholar] [CrossRef]
- Sullivan, D.J. Theories on malarial pigment formation and quinoline action. Int. J. Parasitol. 2002, 32, 1645–1653. [Google Scholar] [CrossRef]
- Inyushin, M.; Kucheryavih, Y.; Kucheryavih, L.; Rojas, L.; Khmelinskii, I.; Makarov, V. Superparamagnetic Properties of Hemozoin. Sci. Rep. 2016, 6, 26212. [Google Scholar] [CrossRef] [PubMed]
- Moore, L.R.; Fujioka, H.; Williams, P.S.; Chalmers, J.J.; Grimberg, B.; Zimmerman, P.A.; Zborowski, M. Hemoglobin degradation in malaria-infected erythrocytes determined from live cell magnetophoresis. FASEB J. 2006, 20, 747–749. [Google Scholar] [CrossRef] [PubMed]
- Berendt, A.R.; Ferguson, D.J.; Newbold, C.I. Sequestration in Plasmodium falciparum malaria: Sticky cells and sticky problems. Parasitol. Today 1990, 6, 247–254. [Google Scholar] [CrossRef]
- Hackett, S.; Hamzah, J.; Davis, T.M.; St Pierre, T.G. Magnetic susceptibility of iron in malaria-infected red blood cells. Biochim. Biophys. Acta Mol. Basis Dis. 2009, 1792, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Coronado, L.M.; Nadovich, C.T.; Spadafora, C. Malarial hemozoin: From target to tool. Biochim. Biophys. Acta Gen. Subj. 2014, 1840, 2032–2041. [Google Scholar] [CrossRef]
- Butykai, A.; Orbán, A.; Kocsis, V.; Szaller, D.; Bordács, S.; Tátrai-Szekeres, E.; Kiss, L.F.; Bóta, A.; Vértessy, B.G.; Zelles, T.; et al. Malaria pigment crystals as magnetic micro-rotors: Key for high-sensitivity diagnosis. Sci. Rep. 2013, 3, 1431. [Google Scholar] [CrossRef]
- Orbán, Á.; Rebelo, M.; Molnár, P.; Albuquerque, I.S.; Butykai, A.; Kézsmárki, I. Efficient monitoring of the blood-stage infection in a malaria rodent model by the rotating-crystal magneto-optical method. Sci. Rep. 2016, 6, 23218. [Google Scholar] [CrossRef]
- Newman, D.M.; Matelon, R.J.; Wears, M.L.; Savage, L.B. The in vivo diagnosis of malaria: Feasibility study into a magneto-optic fingertip probe. IEEE J. Sel. Top. Quantum Electron. 2010, 16, 573–580. [Google Scholar] [CrossRef]
- Lukianova-Hleb, E.Y.; Campbell, K.M.; Constantinou, P.E.; Braam, J.; Olson, J.S.; Ware, R.E.; Sullivan, D.J.; Lapotko, D.O. Hemozoin-generated vapor nanobubbles for transdermal reagent- and needle-free detection of malaria. Proc. Natl. Acad. Sci. USA 2014, 111, 900–905. [Google Scholar] [CrossRef]
- Scholl, P.F.; Kongkasuriyachai, D.; Demirev, P.A.; Feldman, A.B.; Lin, J.S.; Sullivan, D.J., Jr.; Kumar, N. Rapid detection of malaria infection in vivo by laser desorption mass spectrometry. Am. J. Trop. Med. Hyg. 2004, 71, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Campuzano-Zuluaga, G.; Hänscheid, T.; Grobusch, M.P. Automated haematology analysis to diagnose malaria. Malar. J. 2010, 9, 346. [Google Scholar] [CrossRef] [PubMed]
- Rifaie-Graham, O.; Pollard, J.; Raccio, S.; Balog, S.; Rusch, S.; Hernández-Castañeda, M.A.; Mantel, P.Y.; Beck, H.P.; Bruns, N. Hemozoin-catalyzed precipitation polymerization as an assay for malaria diagnosis. Nat. Commun. 2019, 10, 1369. [Google Scholar] [CrossRef] [PubMed]
- Furlani, E.P. Analysis of particle transport in a magnetophoretic microsystem. J. Appl. Phys. 2006, 99, 024912. [Google Scholar] [CrossRef]
- Einstein, A. Uber die von der molekularkinetischen Theorie der Wärme geforderte Bewegung von in ruhenden Flüssigkeiten suspendierten Teilchen. Ann. Der Phys. 1905, 322, 549–560. Available online: https://onlinelibrary.wiley.com/doi/pdf/10.1002/andp.19053220806 (accessed on 31 August 2020). [CrossRef]
- Nam, J.; Huang, H.; Lim, H.; Lim, C.; Shin, S. Magnetic separation of malaria-infected red blood cells in various developmental stages. Anal. Chem. 2013, 15, 7316–7323. [Google Scholar] [CrossRef]
- Han, K.H.; Frazier, A.B. Paramagnetic capture mode magnetophoretic microseparator for high efficiency blood cell separations. Lab Chip 2006, 6, 265–273. [Google Scholar] [CrossRef]
- Han, K.H.; Bruno Frazier, A. Continuous magnetophoretic separation of blood cells in microdevice format. J. Appl. Phys. 2004, 96, 5797–5802. [Google Scholar] [CrossRef]
- Kasetsirikul, S.; Jirayut, B.; Werayut, S.; Morakot, K.; Alongkorn, P. The Development of Malaria Diagnostic Techniques: A Review of the Approaches with Focus on Dielectrophoretic and Magnetophoretic Methods. Malar. J. 2016, 15, 348. [Google Scholar] [CrossRef]
- Dilanian, R.A.; Streltsov, V.; Coughlan, H.D.; Quiney, H.M.; Martin, A.V.; Klonis, N.; Dogovski, C.; Boutet, S.; Messerschmidt, M.; Williams, G.J.; et al. Nanocrystallography measurements of early stage synthetic malaria pigment. J. Appl. Crystallogr. 2017, 50, 1533–1540. [Google Scholar] [CrossRef]
- Candido, R.R.; St Pierre, T.G.; Morassutti, A.L.; Graeff-Teixeira, C.; Jones, M.K. Eggs and magnetism: New approaches for Schistosomiasis diagnosis. Trends Parasitol. 2018, 34, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Xiao, S.H.; Sun, J. Schistosoma hemozoin and its possible roles. Int. J. Parasitol. 2017, 47, 171–183. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Milesi, F.; Giacometti, M.; Coppadoro, L.P.; Ferrari, G.; Fiore, G.B.; Bertacco, R. On-Chip Selective Capture and Detection of Magnetic Fingerprints of Malaria. Sensors 2020, 20, 4972. https://doi.org/10.3390/s20174972
Milesi F, Giacometti M, Coppadoro LP, Ferrari G, Fiore GB, Bertacco R. On-Chip Selective Capture and Detection of Magnetic Fingerprints of Malaria. Sensors. 2020; 20(17):4972. https://doi.org/10.3390/s20174972
Chicago/Turabian StyleMilesi, Francesca, Marco Giacometti, Lorenzo Pietro Coppadoro, Giorgio Ferrari, Gianfranco Beniamino Fiore, and Riccardo Bertacco. 2020. "On-Chip Selective Capture and Detection of Magnetic Fingerprints of Malaria" Sensors 20, no. 17: 4972. https://doi.org/10.3390/s20174972
APA StyleMilesi, F., Giacometti, M., Coppadoro, L. P., Ferrari, G., Fiore, G. B., & Bertacco, R. (2020). On-Chip Selective Capture and Detection of Magnetic Fingerprints of Malaria. Sensors, 20(17), 4972. https://doi.org/10.3390/s20174972