Machine Learning Classification for Assessing the Degree of Stenosis and Blood Flow Volume at Arteriovenous Fistulas of Hemodialysis Patients Using a New Photoplethysmography Sensor Device

 , , and
, , and
Abstract
1. Introduction
2. Theories and Principles
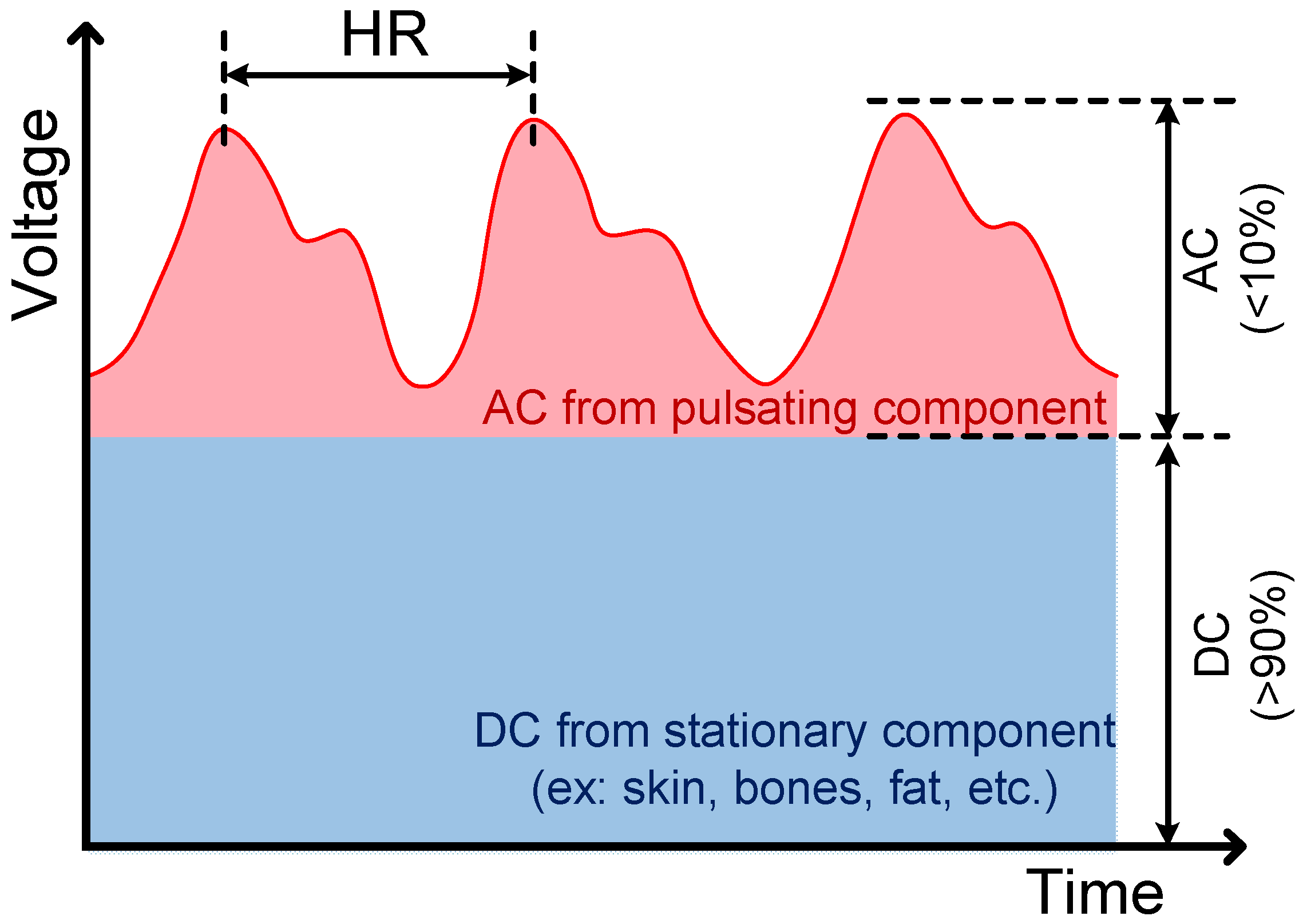
2.1. Beer–Lambert’s Law
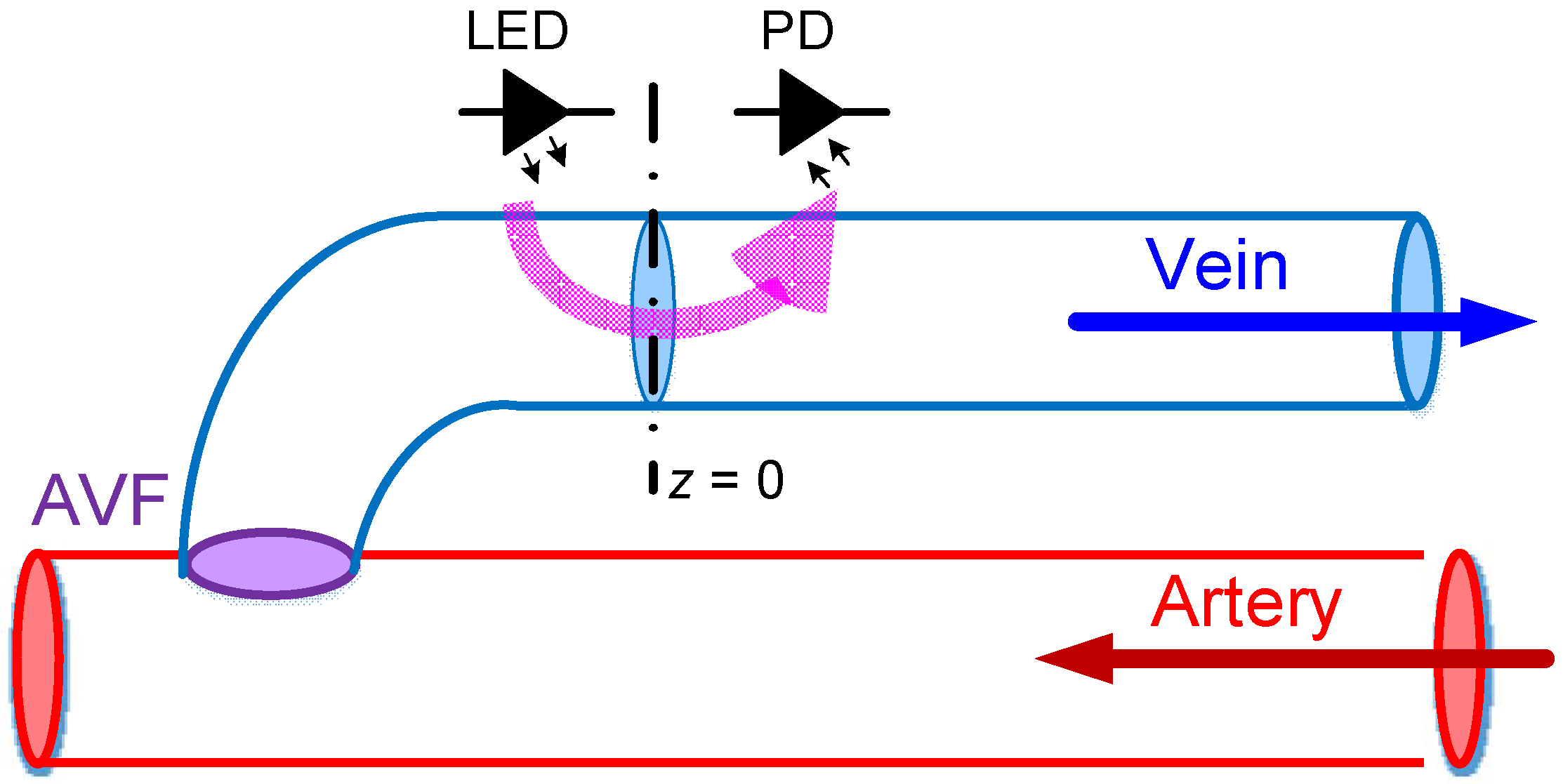
2.2. Hemodynamic Models
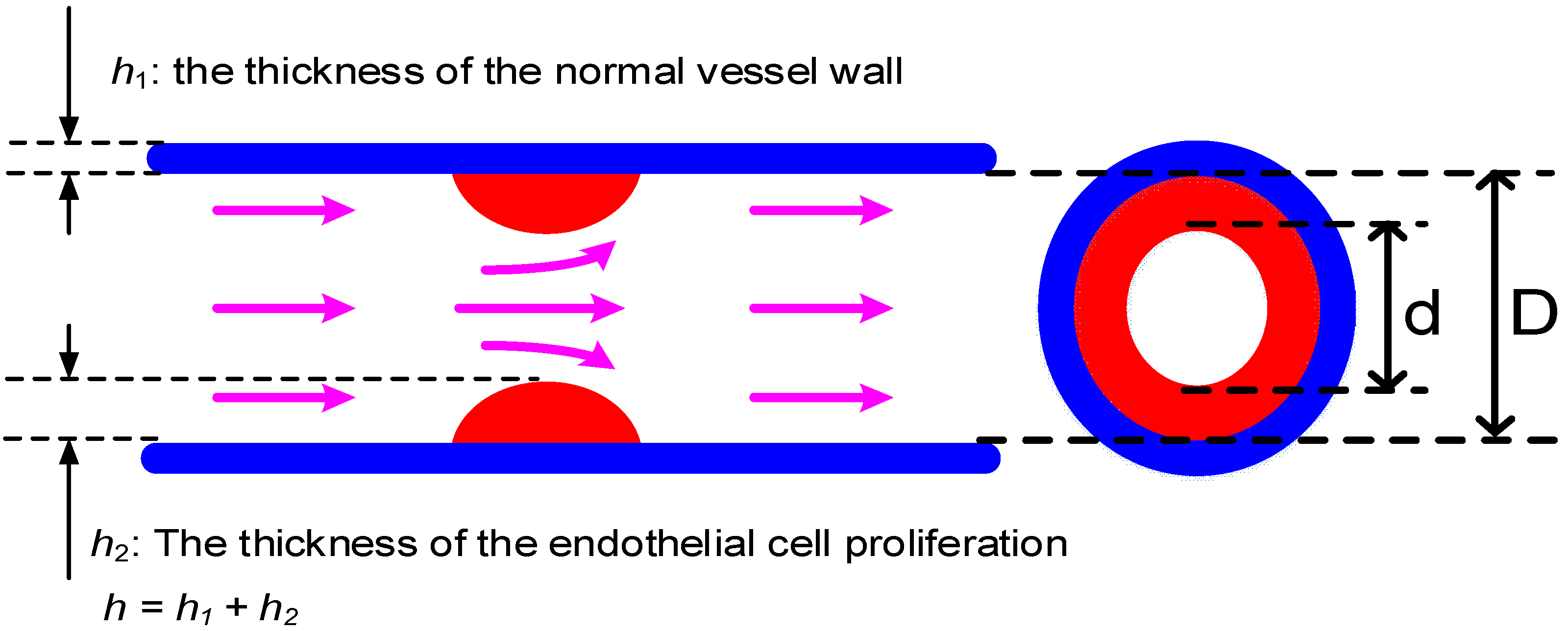
2.3. Degree of Stenosis (DOS)
2.4. Blood Flow Volume (BFV)
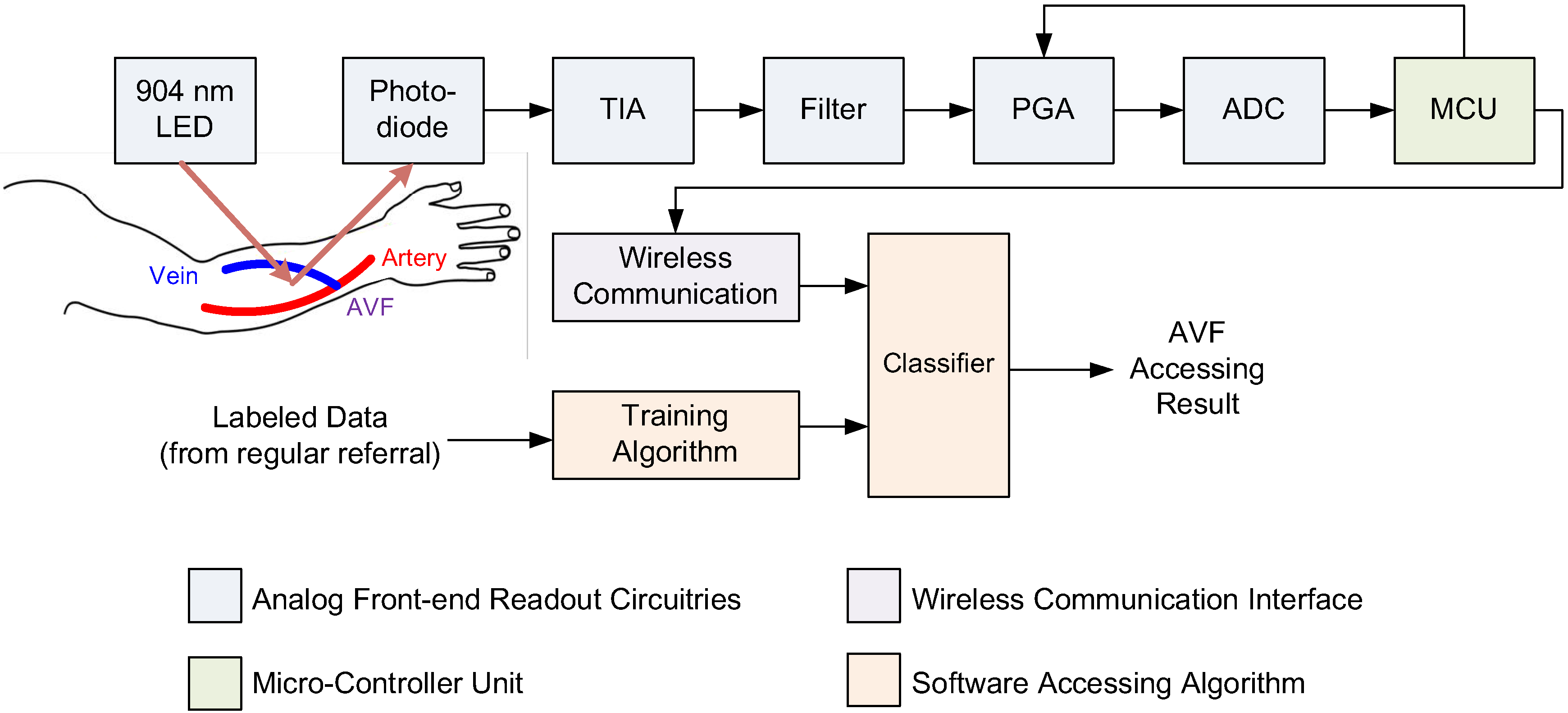
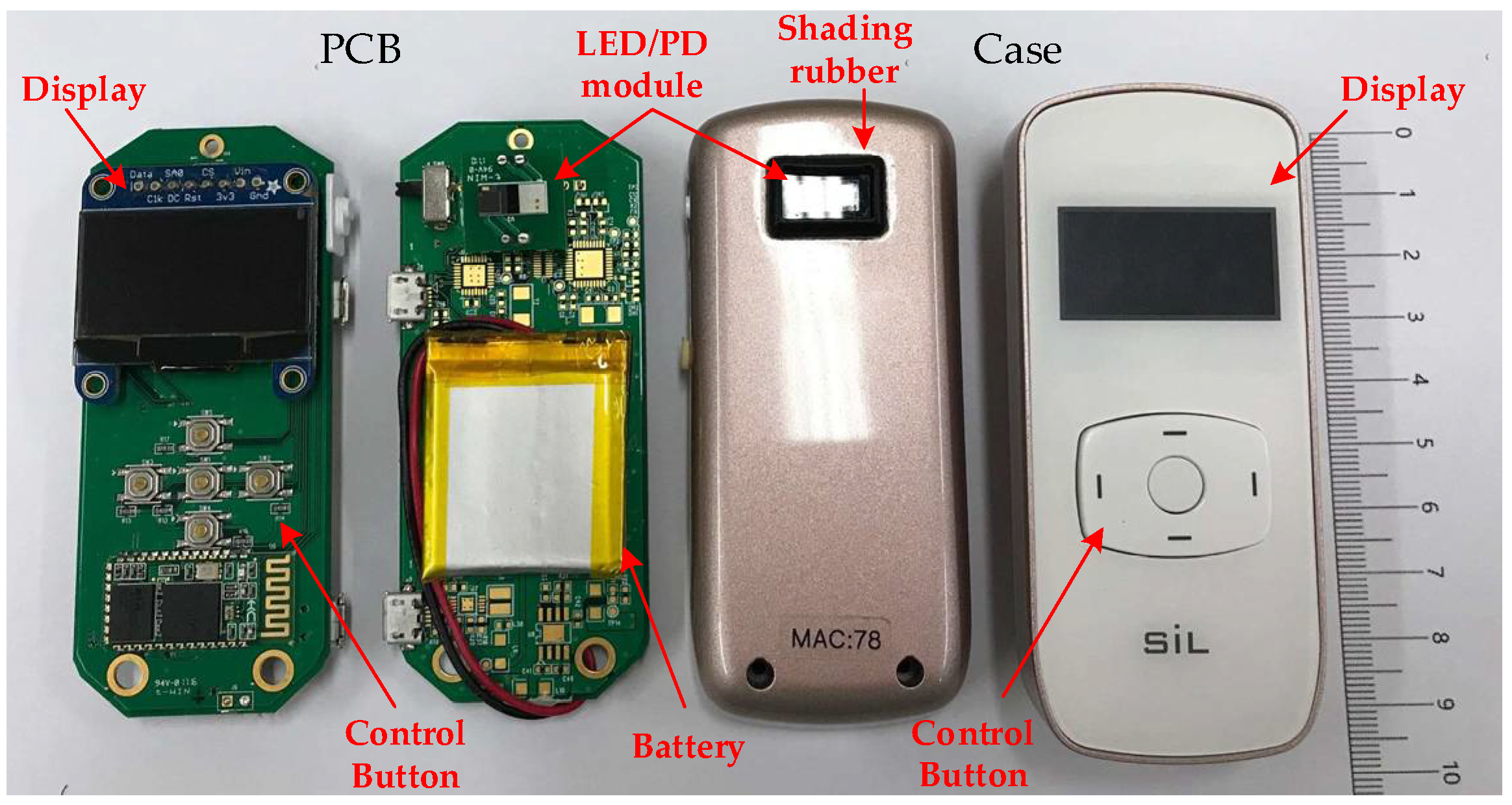
3. Sensor System Design
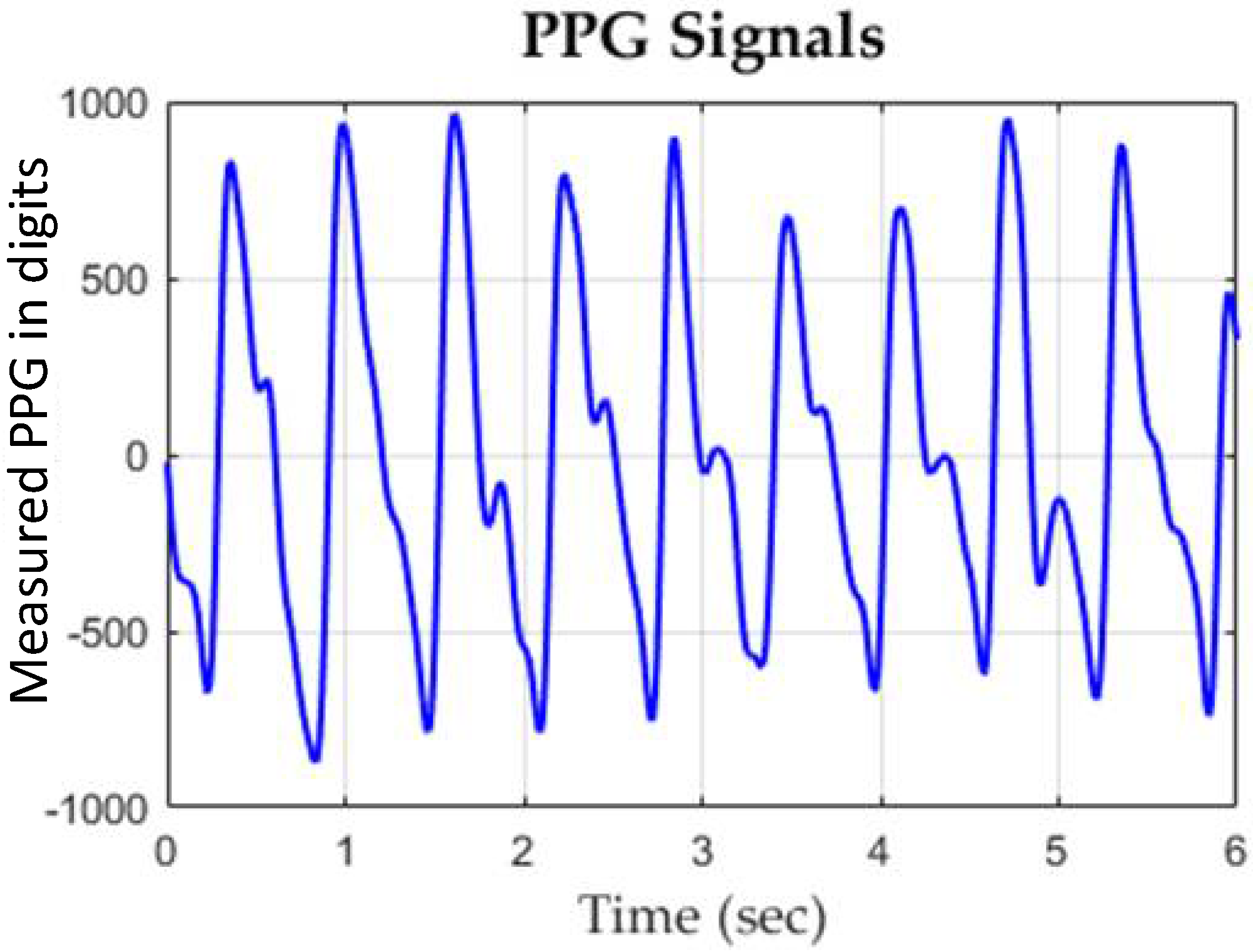
3.1. Readout Circuitry
3.2. Assessing Algorithms
3.2.1. k-Nearest Neighbors (kNN)
3.2.2. Naive Bayes Classifier (NBC)
3.2.3. Support Vector Machine (SVM)
3.2.4. Input Features
- Step (1): randomly divide subjects into 10 subsets.
- Step (2): take only one subset for testing and leave the other for training.
- Step (3): repeat Step (2) 10 times.
- Step (4): calculate the average accuracy and analyze the results.
4. Clinical Validation
4.1. Experiment Setup
4.2. Experiment Results
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
Ethical Statements
Appendix A
References
- National Kidney Foundation. KDOQI clinical practice guidelines and clinical practice recommendations for 2006 updates: Hemodialysis adequacy, peritoneal dialysis adequacy and vascular access. Am. J. Kidney Dis. 2006, 48, S1–S322. [Google Scholar]
- Wang, H.Y.; Wu, C.H.; Chen, C.Y.; Lin, B.S. Novel noninvasive approach for detecting arteriovenous fistula stenosis. IEEE Trans. Biomed. Eng. 2014, 61, 1851–1857. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.L.; Kan, C.H.; Lin, C.H. Arteriovenous shunt stenosis evaluation using a fractional-order fuzzy petri net based screening system for long-term hemodialysis patients. J. Biomed. Sci. Eng. 2014, 7, 258–275. [Google Scholar] [CrossRef][Green Version]
- Yeih, D.F.; Wang, Y.S.; Huang, Y.C.; Chen, M.F.; Lu, S.S. Physiology-based diagnosis algorithm for arteriovenous fistula stenosis detection. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 4619–4622. [Google Scholar] [CrossRef]
- Durand, L.G.; Pibarot, P. Digital signal processing of the phonocardiogram: Review of the most recent advances. Crit. Rev. Biomed. Eng. 1995, 23, 163–219. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.X.; Lin, C.H.; Wu, M.J.; Li, C.M.; Lim, B.Y.; Du, Y.C. Bilateral photoplethysmography analysis for arteriovenous fistula dysfunction screening with fractional-order feature and cooperative game-based embedded detector. Healthc. Technol. Lett. 2015, 2, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.C.; Stephanus, A. A Novel Classification Technique of Arteriovenous Fistula Stenosis Evaluation Using Bilateral PPG Analysis. Micromachines 2016, 7, 147. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.C.; Stephanus, A. Levenberg-Marquardt Neural Network Algorithm for Degree of Arteriovenous Fistula Stenosis Classification Using a Dual Optical Photoplethysmography Sensor. Sensors 2018, 18, 2322. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.X.; Lin, C.H.; Du, Y.C.; Chen, P.J.; Shih, C.C.; Chen, T. Estimation of arteriovenous fistula stenosis by FPGA based Doppler flow imaging system. In Proceedings of the 2015 IEEE International Ultrasonics Symposium (IUS), Taipei, Taiwan, 21–24 October 2015; pp. 1–4. [Google Scholar] [CrossRef]
- Chiang, P.Y.; Chao, P.C.P.; Tarng, D.C.; Yang, C.Y. A Novel Wireless Photoplethysmography Blood-Flow Volume Sensor for Assessing Arteriovenous Fistula of Hemodialysis Patients. IEEE Trans. Ind. Electron. 2017, 64, 9626–9635. [Google Scholar] [CrossRef]
- Webb, R.C.; Ma, Y.; Krishnan, S.; Li, Y.; Yoon, S.; Guo, X.; Feng, X.; Shi, Y.; Seidel, M.; Cho, N.H.; et al. Epidermal devices for noninvasive, precise and continuous mapping of macrovascular and microvascular blood flow. Sci. Adv. 2015, 1, 30. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.J.; Lee, C.K.; Kang, M.; Kang, S.J.; Kim, K.N.; Kim, K.; Kim, K.S.; Lee, J.W. Magneto-Plethysmographic Sensor for Peripheral Blood Flow Velocity. IEEE Sens. J. 2014, 14, 1341–1342. [Google Scholar] [CrossRef]
- Zhu, F.; Williams, S.; Putnam, H.; Campos, I.; Ma, J.; Johnson, C.; Kappel, F.; Kotanko, P. Estimation of arterio-venous access blood flow in hemodialysis patients using video image processing technique. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 207–210. [Google Scholar] [CrossRef]
- Chuang, C.T.; Chang, T.; Chiang, Y.T.; Chang, F.R. Adaptive filtering for heart rate estimation using cepstrum technique. In Proceedings of the 2016 International Conference on System Science and Engineering (ICSSE), Puli, Taiwan, 7–9 July 2016; pp. 1–3. [Google Scholar] [CrossRef]
- Hsiao, C.C.; Hsu, F.W.; Lee, R.G.; Lin, R. Correlation analysis of heart rate variability between PPG and ECG for wearable devices in different postures. In Proceedings of the 2017 IEEE International Conference on Systems, Man, and Cybernetics (SMC), Banff, AB, Canada, 5–8 October 2017; pp. 2957–2962. [Google Scholar] [CrossRef]
- Huang, S.C.; Hung, P.H.; Hong, C.H.; Wang, H.M. A New Image Blood Pressure Sensor Based on PPG, RRT, BPTT, and Harmonic Balancing. IEEE Sens. J. 2014, 14, 3685–3692. [Google Scholar] [CrossRef]
- Yang, Y.H.; Tang, K.T. A pulse oximetry system with motion artifact reduction based on Fourier analysis. In Proceedings of the 2014 IEEE International Symposium on Bioelectronics and Bioinformatics (IEEE ISBB 2014), Chung Li, Taiwan, 11–14 April 2014; pp. 1–4. [Google Scholar] [CrossRef]
- Venema, B.; Gehring, H.; Michelsen, I.; Blanik, N.; Blazek, V.; Leonhardt, S. Robustness, Specificity, and Reliability of an In-Ear Pulse Oximetric Sensor in Surgical Patients. IEEE J. Biomed. Health Inform. 2014, 18, 1178–1185. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Shin, H.S.; Park, J.; Lee, M. The Optimal Attachment Position for a Fingertip Photoplethysmographic Sensor with Low DC. IEEE Sens. J. 2012, 12, 1253–1254. [Google Scholar] [CrossRef]
- Nitzan, M.; Romem, A.; Koppel, R. Pulse oximetry: Fundamentals and technology update. Med. Devices Evid. Res. (Auckland, N.Z.) 2014, 7, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Bessems, D.; Rutten, M.; Vosse, F.V.D. A wave propagation model of blood flow in large vessels using an approximate velocity profile function. J. Fluid Mech. 2007, 580, 145–168. [Google Scholar] [CrossRef]
- Chiang, P.Y.; Chao, P.C.P.; Yang, C.Y.; Tarng, D.C. Theoretical Developments and Clinical Experiments of Measuring Blood Flow Volume (BFV) at Arteriovenous Fistula (AVF) Using a Photoplethysmography (PPG) Sensor. Microsyst. Technol. 2018, 24, 4587–4603. [Google Scholar] [CrossRef]
- Womersley, J.R. Method for the calculation of velocity, rate of flow and viscous drag in arteries when the pressure gradient is known. J. Physiol. 1995, 127, 553–563. [Google Scholar] [CrossRef] [PubMed]
- Akhter, N.; Tharewal, S.; Gite, H.; Kale, K.V. Microcontroller based RR-Interval measurement using PPG signals for Heart Rate Variability based biometric application. In Proceedings of the 2015 International Conference on Advances in Computing, Communications and Informatics (ICACCI), Kochi, India, 10–13 August 2015; pp. 588–593. [Google Scholar] [CrossRef]
- Bozkurt, F.; Uçar, M.K.; Mehmet, R.B.; Tuna, S.; Bílgín, C. Respiratory scoring using photoplethysmography signal and nearest neighbor algorithm. In Proceedings of the 2018 26th Signal Processing and Communications Applications Conference (SIU), Izmir, Turkey, 2–5 May 2018; pp. 1–3. [Google Scholar] [CrossRef]
- Nadzri, N.I.M.; Sidek, K.A.; Nor, R.M. Biometric Identification for Twins Using Photoplethysmogram Signals. In Proceedings of the 2016 6th International Conference on Information and Communication Technology for The Muslim World (ICT4M), Jakarta, Indonesia, 22–24 November 2016; pp. 320–324. [Google Scholar] [CrossRef]
- Venema, B.; Blazek, V.; Leonhardt, S. In-ear photoplethysmography for mobile cardiorespiratory monitoring and alarming. In Proceedings of the 2015 IEEE 12th International Conference on Wearable and Implantable Body Sensor Networks (BSN), Cambridge, MA, USA, 9–12 June 2015; pp. 1–5. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Symbol | Features for Assessing DOS | Features for Assessing BFV | Measurement | Description |
|---|---|---|---|---|
| The max of peak to peak interval (PImax) | O | O | The perfusion index (AC/DC) by the PPG sensors | The normalized maximum length of light transmission path in blood |
| The min of peak to peak interval (PImin) | O | O | The perfusion index (AC/DC) by the PPG sensors | The normalized minimum length of light transmission path in blood |
| sphygmomanometer. Oxyhemoglobin saturation by pulse oximetry (SpO2) | O | O | Oximeter | The blood oxygen saturation level |
| Systolic Blood Pressure (SBP) | O | O | Electronic sphygmomanometer | The systolic blood pressure |
| Diastolic Blood Pressure (DBP) | O | O | Electronic sphygmomanometer | The diastolic blood pressure |
| Heart rate (ω) | X | O | The proposed PPG sensors | The heart rate |
| Samples Number = 74 | Ground Truth (Actual Class) | ||
|---|---|---|---|
| Positive | Negative | ||
| Classification Results of k-Nearest Neighbors (kNN) (Predicted Class) | Positive | TP = 32 (43.24%) | FP = 5 (6.76%) |
| Negative | FN = 13 (17.57%) | TN = 24 (32.43%) | |
| Classification Results of Naive Bayes Classifier (NBC) (Predicted Class) | Positive | TP = 41 (55.41%) | FP = 8 (10.81%) |
| Negative | FN = 4 (5.41%) | TN = 21 (28.38%) | |
| Classification Results of Support Vector Machine (SVM) (Predicted Class) | Positive | TP = 42 (56.76%) | FP = 6 (8.11%) |
| Negative | FN = 3 (4.05%) | TN = 23 (31.08%) | |
| Samples Number = 79 | Ground Truth (Actual Class) | ||
|---|---|---|---|
| Positive | Negative | ||
| Classification Results of kNN (Predicted Class) | Positive | TP = 51 (64.56%) | FP = 6 (7.59%) |
| Negative | FN = 10 (12.66%) | TN = 12 (15.19%) | |
| Classification Results of NBC (Predicted Class) | Positive | TP = 59 (74.68%) | FP = 8 (10.13%) |
| Negative | FN = 2 (2.53%%) | TN = 10 (12.66%) | |
| Classification Results of SVM (Predicted Class) | Positive | TP = 59 (74.68%) | FP = 7 (8.86%) |
| Negative | FN = 2 (2.53%) | TN = 11 (13.92%) | |
| H. Y. Wang et al. (2014) [2] | Du Y.-C. et al. (2018) [8] | D. F. Yeih et al. (2014) [4] | J. X. Wu et al. (2015) [9] | P. Y. Chiang et al. (2017) [10] | F. Zhu et al. (2016) [13] | This Work | |
|---|---|---|---|---|---|---|---|
| Sensor | Stethoscope Auscultation | Bilateral PPG | Stethoscope Auscultation | Ultrasound | Single PPG | Camera | Single PPG |
| Assessing Index | DOS | DOS | DOS | DOS | BFV | BFV | DOS and BFV |
| Principle | Acoustic | Optical | Acoustic | Doppler | Optical | Optical | Optical |
| Communication | Wireless | Wired | Wireless | Wired | Wireless | Wired | Wireless |
| Assessing Algorithm | Neural Network | Neural Network | Support Vector Machine | Color Relation Analysis | Neural Network | Optic Flow Methods | Support Vector Machine |
| Size | 9 cm × 4 cm × 2 cm | Large | - | Large | 9 cm × 8 cm × 4 cm | Large | 9 cm × 3.5 cm × 1.5 cm |
| Number of Subjects | 479 | 11 | 22 | 50 | 40 | 40 | DOS: 74 BFV: 79 |
| Accuracy | 87.8% | 94.82% | 84.3% | 83% | R2 = 0.7176 * | R2 = 0.71 * (with 32.5% outlier subjects) | DOS: 87.84% BFV: 88.61% |
| Type II Error | 10.75% | - | 16.7% | - | >50% | - | DOS: 6.67% BFV: 3.28% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiang, P.-Y.; Chao, P.C.-P.; Tu, T.-Y.; Kao, Y.-H.; Yang, C.-Y.; Tarng, D.-C.; Wey, C.-L. Machine Learning Classification for Assessing the Degree of Stenosis and Blood Flow Volume at Arteriovenous Fistulas of Hemodialysis Patients Using a New Photoplethysmography Sensor Device. Sensors 2019, 19, 3422. https://doi.org/10.3390/s19153422
Chiang P-Y, Chao PC-P, Tu T-Y, Kao Y-H, Yang C-Y, Tarng D-C, Wey C-L. Machine Learning Classification for Assessing the Degree of Stenosis and Blood Flow Volume at Arteriovenous Fistulas of Hemodialysis Patients Using a New Photoplethysmography Sensor Device. Sensors. 2019; 19(15):3422. https://doi.org/10.3390/s19153422
Chicago/Turabian StyleChiang, Pei-Yu, Paul C. -P. Chao, Tse-Yi Tu, Yung-Hua Kao, Chih-Yu Yang, Der-Cherng Tarng, and Chin-Long Wey. 2019. "Machine Learning Classification for Assessing the Degree of Stenosis and Blood Flow Volume at Arteriovenous Fistulas of Hemodialysis Patients Using a New Photoplethysmography Sensor Device" Sensors 19, no. 15: 3422. https://doi.org/10.3390/s19153422
APA StyleChiang, P.-Y., Chao, P. C.-P., Tu, T.-Y., Kao, Y.-H., Yang, C.-Y., Tarng, D.-C., & Wey, C.-L. (2019). Machine Learning Classification for Assessing the Degree of Stenosis and Blood Flow Volume at Arteriovenous Fistulas of Hemodialysis Patients Using a New Photoplethysmography Sensor Device. Sensors, 19(15), 3422. https://doi.org/10.3390/s19153422