Simulating Arbitrary Electrode Reversals in Standard 12-Lead ECG



Abstract
1. Introduction
- Reversals between limb electrodes are reported to provoke deep QS complexes and inverted T waves in leads (II, III, aVF) that could be misdiagnosed as old myocardial infarctions (MI) involving the inferior heart wall [5]. Right arm (RA) and left arm (LA) interchange is associated with inverted T waves in leads (I, aVL) suggestive of lateral wall MI [6] as well as indicative of ECG features of dextrocardia [7]. RA and right leg (RL) swap results in low-amplitude QRS complexes in lead II [7,8] and all other frontal leads resembling scaled variations of lead III and changed QRS axes in the frontal plane [8]. LA and left leg (LL) reversal creates suspicions of inferior-wall MI [7]. RA and LL swap could be confused for the combined features of lateral wall MI and low atrial rhythm [7].
- Reversals between chest electrodes have been found to provoke erroneous diagnosis in 17% to 24% of cases involving wrongly placed C1 electrodes [9]. Generally, when another precordial lead is substituted for V1, the result is a tall R wave in V1, which could be taken as a sign of right bundle branch block, left ventricular ectopy, right ventricular hypertrophy, acute right ventricular dilation, Type A Wolff-Parkinson-White syndrome, posterior MI, hypertrophic cardiomyopathy, progressive muscular dystrophy or dextrocardia [10].
- Reversals between limb and chest electrodes are a possible scenario due to the matching colors of the two ECG cables [11] or the incorrect attachment of the cable connectors to the junction box of the ECG machine [12]. C2/LA (yellow) cable interchange is described in two case reports [13,14] to have produced right axis deviation and Q waves in (III, aVF), accompanied by an inverted T wave in both leads, together with a quick transition in V2 with qR complex and an inverted T wave. The ECGs are interpreted as an inferior MI with residual ischemia in [13] or recent inferior and a posterior MI [14]. Limb/precordial cable interchange has been observed to result in tall R waves in aVR, negative QRS complexes in the other five limb leads and inverted ST elevation/depression in some of the leads. Thus, inferior, anterior, and lateral MI could be erroneously diagnosed [12]. In another study [15], the authors suspect the same interchange to have resulted in ST-segment elevation in the inferior leads; however, their thesis has been impugned by [16], who have explained the wandering ST elevation with medical reasons.
- Limb leads: LA and LL reversal is indicated by P wave amplitude [25] and QRS, P-axes [26]; RA and RL interchange is detected when lead II presents as a flat line [27] or with peak-to-peak amplitude less than 185 µV [8]; LA-RA and RA-LL swaps are recognized by analysis of P and QRS frontal axes and clockwise vector loop rotation direction, R and T wave amplitudes in leads (I, II) [28]; various LA/RA/LL/RL combinations are detected by a number of analytical approaches based on the assessment of the QRS axis [29,30], together with P wave amplitudes [31], direction of P-loop inscription and/or frontal P-axis [32]; lead reconstruction using redundancy of information in eight independent leads [33]; morphological measurements of QRS, P-wave amplitudes, frontal axis and clockwise vector loop rotation, combined with redundancy features [34]; maximal and minimal QRS, T-wave amplitudes in leads (I, II, III) [35]; correlation coefficients of limb leads vs. V6 [36,37]; combining the features described in [26] and [33] for a more robust and accurate performance [36].
- Chest leads: Different reversal sets have been examined, such as five reversals of adjacent leads (V1/V2, V2/V3, V3/V4, V4/V5, V5/V6), analyzed by P, QRS and ST-T measurements [26] and PQ-RS amplitude distances [31]; nine reversals (five adjacent leads, V1/V3, V4/V6, V4/V5/V6/V1/V2/V3, V6/V5/V4/V3/V2/V1) are evaluated via correlations between measured and reconstructed leads [33]; seven reversals (five adjacent leads, V1/V3, V4/V6) are handled by processing of both morphology and redundancy features [34]; 15 reversals, including all possible pairwise V1–V6 swaps, have been tested in our previous study by applying analysis of inter-lead correlation coefficients [38].
- Limb and chest leads: Interchanges between limb and C2 precordial electrodes specific for a telemonitoring system are detected by correlation to a previously recorded ECG [39]. This early work, together with our recent publication on the unicolor electrode interchange detection [11], are the only studies dealing with recognition of reversals between limb and precordial leads.
2. Methods
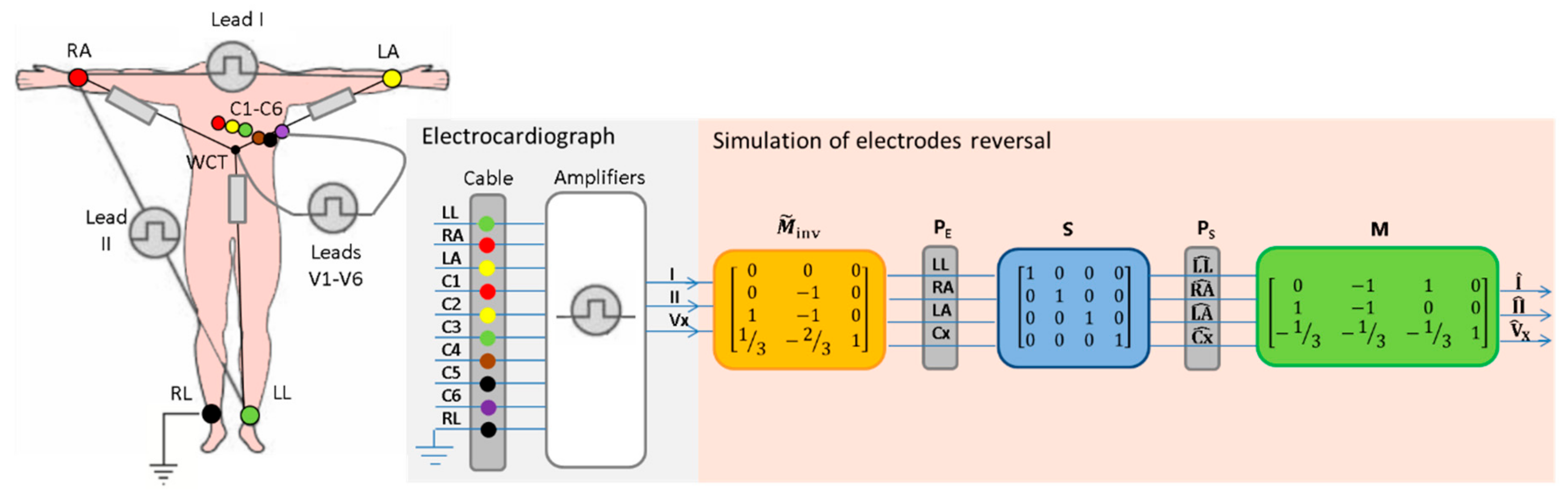
2.1. Derivation of the Transformation Formula
- denotes the electrical potential of the respective electrodes, also referred to as the raw electrode biopotential.
- are the bipolar leads measuring the potential differences between limbs (LA-RA, LL-RA), forming the Einthoven’s triangle.
- represents any of the unipolar chest leads (V1-V6) measuring the potential of the chest electrodes against the reference WCT potential (, which is defined to be the average of the RA, LA and LL electrodes.
- Note that the ground electrode placed on the RL is used for technical reasons (driven right leg) and does not have direct influence on any ECG leads.
2.2. Verification of ‘MSMinv’ Transformation
- ECG electrode reversals with known lead transforms are theoretically studied. For this purpose, the formula for computation of the reordered leads (, ) is directly compared to the published lead transformations. This simple approach is applicable only to reversals between peripheral electrodes, widely analyzed in the literature [5,7,12,21,24,36,37,38,43].
- ECG electrode reversals with unknown lead transformations (such as reversals between limb and chest electrodes) are experimentally studied with a dedicated database (described in Section 3). For this purpose, the 8 independent leads of 2 recordings from the same person (RC, taken with correct electrode position; RS, taken with real electrode swap) are compared in three different scenarios:
- ◦
- (: No transformation is applied to study the lead-specific differences between recordings with correct vs. swapped electrodes.
- ◦
- (: Forward ‘MSMinv’ transformation is applied on the recording with correct lead set to simulate lead swap and to study the lead-specific differences of simulated vs. recorded electrode reversals (.
- ◦
- (: Inverse ‘MSMinv’ transformation is applied on the recording with reversed lead set to simulate correct electrode positions ( and to study the lead-specific differences of simulated vs. recorded, correctly placed electrodes (.
- ◦
- Root-mean-square error:where Fs denotes the sampling frequency of the average beat.
- ◦
- Peak error:
- ◦
- Correlation coefficient:
3. Database
- Correct positions of the electrodes (no electrode is swapped);
- Swap of red electrodes (RA-C1);
- Swap of yellow electrodes (LA-C2);
- Swap of green electrodes (LL-C3);
- Swap of black electrodes (RL-C5);
- Swap of all unicolor electrodes (RA-C1, LA-C2, LL-C3, RL-C5).
4. Results and Discussion
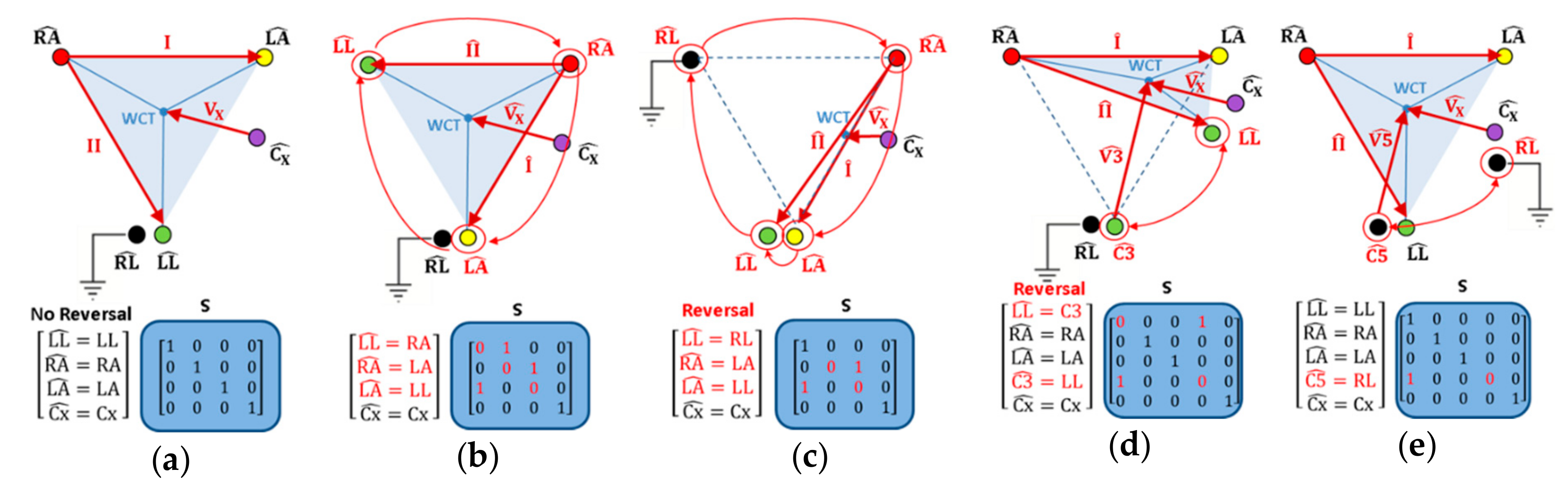
4.1. Theoretical Simulations of Electrode Reversals
4.1.1. Reversals of Peripheral Electrodes Not Involving RL
4.1.2. Reversals of Peripheral Electrodes Involving RL
- RL is in the position of RA:
- RL is in the position of LA:
- RL is in the position of LL: , where is equal to the correct electrode placement.
4.1.3. Reversals of Chest and Peripheral Electrodes
- for the precordial electrodes , which keep their position unchanged on the chest;
- for the precordial electrodes , where n = 1,2,3,5 is substituting the chest electrode number, which changes its position to some of the limbs.
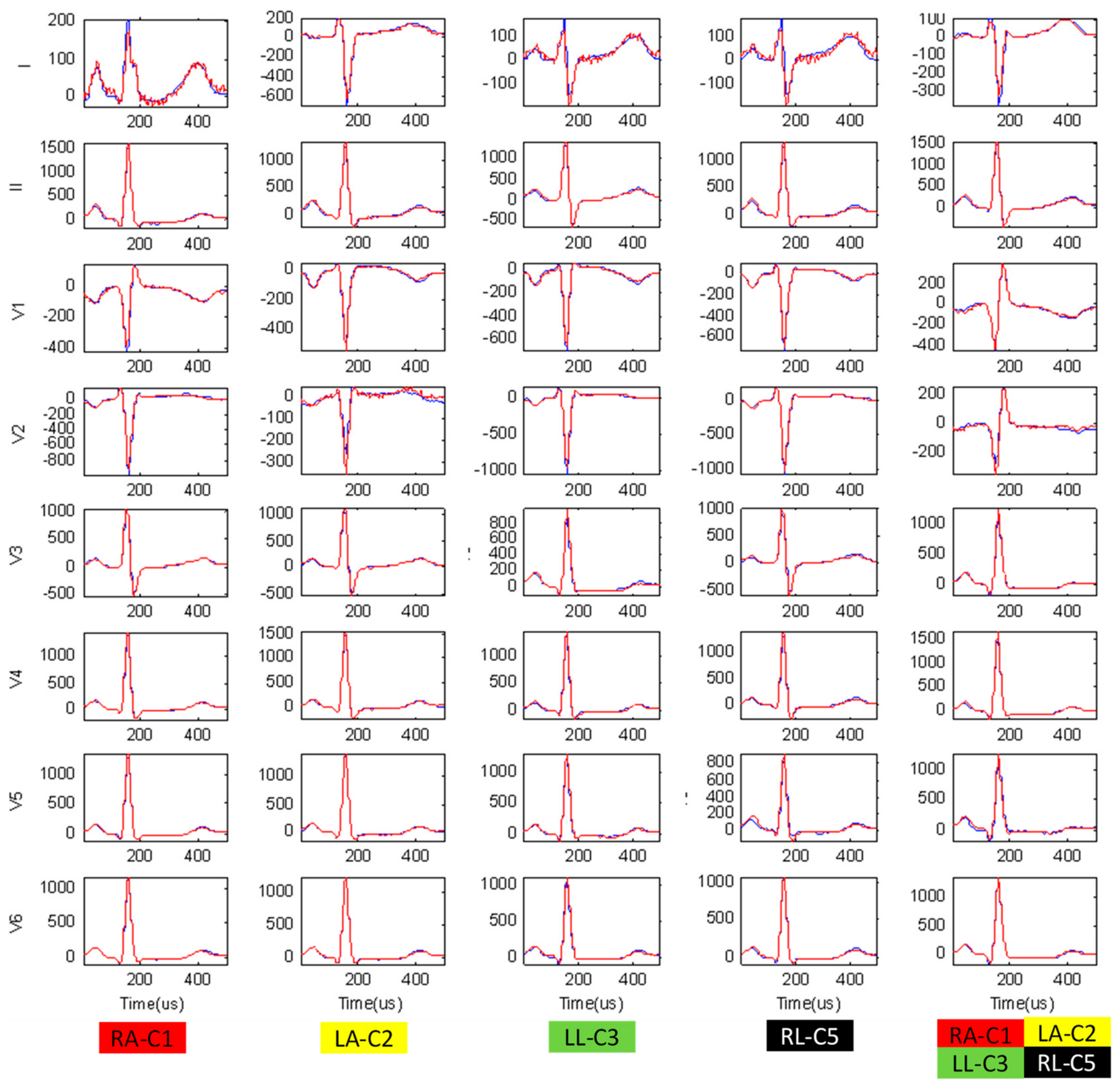
4.2. Experimental Verification of Simulated Swaps Between Unicolor Chest and Peripheral Electrodes
- No transformation, showing the largest differences between correct vs. swapped electrode recordings for all leads because WCT is considerably displaced in most chest-limb reversals (except RL-C5). We note the greatest mean value differences for the unipolar lead with a chest electrode placed on the limbs:
- ◦
- V1 (120 μV, 529 μV, 0.832) for RA-C1,
- ◦
- V2 (246 μV, 1121 μV, 0.456) for LA-C2,
- ◦
- V3 (206 μV, 868 μV, 0.512) for LL-C3,
- ◦
- V5 (131 μV, 639 μV, 0.785) for RL-C5,
- ◦
- V1-V3 (225-289 μV, 967-1235 μV, 0.365-0.652) for all unicolor pairs.
- Forward ‘MSMinv’ transformation, simulating electrode reversals which have significantly reduced differences when compared to the recordings with really swapped electrodes (p < 0.05). We measure mean values (RMS Error, Peak Error, CorCoef) in the range (<20 μV, <60 μV, ≥0.995), assuming they represent negligible average beat differences mainly due to rhythm variation and signal acquisition noises in the compared recordings. We have noticed one exception for both reversals involving RL (RL-C5, all unicolor pairs), where the Forward ‘MSMinv’ transformation introduces a slight error in the calculation of the swapped lead V5 (≤26 μV, ≤104 μV, ≥0.986), assuming the C5 potential to be equal to LL, while C5 is placed on the RL (approximation error from the equipotential legs).
- Inverse ‘MSMinv’ transformation, recovering the correct electrode order, which has significantly reduced differences when compared to the recordings with really correct electrodes (p < 0.05), estimated within the above outlined range of negligible errors (<20 μV, <60 μV, ≥0.995). We have again found an exception for both reversals involving RL (RL-C5, all unicolor pairs), where the Inverse ‘MSMinv’ transformation fails to reconstruct the correct lead V5 (<142 μV, <660 μV, ≥0.792) from a recording with RL electrode in the position of C5 electrode. As soon as RL stops being an input to the ECG device, the potential of V5 electrode is lost and not reproduced by any active electrode in the swap matrix (Table 4, all entries are equal to ‘0’ for the column, corresponding to C5).
4.3. Application of the ‘MSMinv’ Transformation for Automatic Detection of the Exact ECG Electrode Reversals
- All 25 patients are considered, comparing the available pairs of recordings ( ) per patient, where is the recording without electrode reversals, and represents one of the recorded 3 lead swaps (RA-C1, LA-C2, LL-C3), not involving the RL.
- The minimal difference rule (17) is applied on the average beat of each recording.
- The minimal difference rule (17) is evaluated with 3 distance metrics – min(RMS Error) (Equation (13)), min(Peak Error) (Equation (14)), max(CorCoef) (Equation (15)).
- The accuracy for detection of the TLS is evaluated as the true positive (TP) rate, considering the tested population of N subjects:
5. Conclusions
- Limb–chest electrode swaps with WCT potential change which, to the best of our knowledge, have never been simulated in the literature (Table 4). The formulas are exhibited for the most probable reversals of unicolor electrode pairs in the peripheral and precordial ECG cables.
- The ‘Forward’ application computing the reordered lead set from an ECG recorded with correctly placed electrodes is important for educational purposes of both humans and machines to reliably recognize and warn of electrode swaps before potentially erroneous diagnostic interpretation has been made. In this respect, ‘MSMinv’ transformation is applicable to the available immense databases of correctly recorded ECGs (from normal and abnormal heart conditions) for reproducing the vast diversity of distorted ECG leads that can be observed in arbitrary swaps within the limb and precordial electrode set (such as the examples in Figure 3). This is an indispensable tool for the comprehensive training platforms to visualize and study the effects of electrode swaps (e.g. online cardiology courses for physicians, researchers, and instructors) or software design platforms (training the automatic detection algorithms) on abundant ECG electrode reversals.
- The ‘Inverse’ application reconstructing the correct lead set from an ECG recorded with known electrode reversals can save time and the cost of having to repeat ECG recordings in case of follow-up detection of electrode reversals and error-screening of clinical databases. The possibility for straightforward visualization of the correct lead set and its interpretation can easily uncover diagnostic errors or answer dilemmas for suspected or mistrusted electrode swaps (such as the dispute between [15] and [16]). In the general case when the electrode reversal is unknown but a prior correct ECG recording of the same patient is available, the Inverse ‘MSMinv’ transformation is able to solve the non-trivial task of detecting which electrodes have been exactly swapped. For this purpose, all possible swapped reconstructions can be simulated to ultimately determine the one which yields the minimal RMS difference or the highest correlation with the known recording. We have achieved a detection accuracy of 96% to 100% for this simple criterion, which has been tested with available recordings of three electrode swaps (RA-C1, LA-C2, LL-C3, not involving the RL) from 25 healthy persons. One should consider, however, the limitations for the validation of such an application which should be tested against the functional and physiological ECG instability between the two ECG sessions (e.g., the criterion validated on a specific population with “normal” ECG during rest could fail on cardiac patients or patients under environmental stress with lead-wise ECG morphology change). As this work is focused only on the problem of simulating all possible ECG cable reversals, the design and validation of criteria for a self-consistency check for detection of the ECG cable reversals is an extensive problem for a future study.
Author Contributions
Funding
Conflicts of Interest
References
- Kligfield, P.; Gettes, L.S.; Bailey, J.J.; Childers, R.; Deal, B.J.; Hancock, E.W.; van Herpen, G.; Kors, J.A.; Macfarlane, P.; Mirvis, D.M.; et al. Recommendations for the standardization and interpretation of the electrocardiogram: part I: The electrocardiogram and its technology: a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society: endorsed by the International Society for Computerized Electrocardiology. J. Am. ColL. Cardiol. 2007, 115, 1306–1324. [Google Scholar] [CrossRef]
- Rajaganeshan, R.; Ludlam, C.L.; Francis, D.P.; Parasramka, S.V.; Sutton, R. Accuracy in ECG lead placement among technicians, nurses, general physicians and cardiologists. Int. J. Clin. Pract. 2008, 62, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Salvi, V.; Karnad, D.R.; Panicker, G.K.; Kothari, S.; Hingorani, P.; Natekar, M.; Mahajan, V.; Narula, D. Limb lead interchange in thorough QT/QTc studies. J. Clin. Pharmacol. 2011, 51, 1468–1473. [Google Scholar] [CrossRef] [PubMed]
- Rudiger, A.; Hellermann, J.; Mukherjee, R.; Follath, F.; Turina, J. Electrocardiographic artifacts due to electrode misplacement and their frequency in different clinical settings. Am. J. Emer. Med. 2007, 25, 174–178. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.; Chowdhury, A.; Ahmed, M.; Sabah, K.; Haque, H.; Kabir, S.; Islam, K.N.; Saleh, M.A.D. Lead-Reversal ECG Simulating Myocardial Infarction—A Case Report and Literature Review. Bangladesh Heart J. 2016, 31, 104–108. [Google Scholar] [CrossRef]
- Raut, M.; Maheshwari, A. Know the errors in ECG recording. Curr. Med. Res. Pract. 2015, 5, 81–91. [Google Scholar] [CrossRef]
- Vardan, S.; Mookherjee, D.; Sarkar, T.; Mehrotra, K.; Fruehan, T.; Mookherjee, S. Guidelines for the Detection of ECG Limb Lead Misplacements. Resid. Staff 2008, 54. Available online: https://www.mdmag.com/journals/resident-and-staff/2008/2008-01/2008-01_05 (accessed on 24 February 2019).
- Haisty, W.K.; Pahlm, O.; Edenbrandt, L.; Newman, K. Recognition of Electrocardiographic Electrode Misplacements Involving the Ground (Right Leg) Electrode. Am. J. Cardiol. 1993, 71, 1490–1495. [Google Scholar] [CrossRef]
- Bond, R.; Finlay, D.; Nugent, C.; Breen, C.; Guldenring, D.; Daly, M. The effects of electrode misplacement on clinicians’ interpretation of the standard 12-lead electrocardiogram. Eur. J. Int. Med. 2012, 23, 610–615. [Google Scholar] [CrossRef]
- Mattu, A.; Brady, W.; Perron, A.; Robinson, D. Prominent R Wave in Lead V1: Electrocardiographic Differential Diagnosis. Am. J. Emerg. Med. 2001, 19, 504–513. [Google Scholar] [CrossRef]
- Jekova, I.; Leber, R.; Krasteva, V.; Schmid, R. Detection of Unicolor ECG Electrode Reversals in Standard 12-Lead ECG. Comput. Cardiol. 2018, 45. [Google Scholar] [CrossRef]
- Lynch, R. ECG lead misplacement: A brief review of limb lead misplacement. African J. Emerg. Med. 2014, 4, 130–139. [Google Scholar] [CrossRef][Green Version]
- García-Niebla, J.; García, P.L. An unusual case of electrode misplacement: left arm and V2 electrode reversal. J. Electrocardiol. 2008, 41, 380–381. [Google Scholar] [CrossRef] [PubMed]
- Vanninen, S.U.; Nikus, K.C. Electrocardiogram Acquisition Errors or Myocardial Infarct. Case Rep. Cardiol. 2011, 2011, 605874. [Google Scholar] [CrossRef] [PubMed]
- Joshi, K.R.; Morris, D.L.; Figueredo, V.M. Wandering acute myocardial infarction. Am. J. Med. 2014, 127, e5–e6. [Google Scholar] [CrossRef]
- Givens, P.M.; Goldonowicz, J.M.; Littmann, L. The electrocardiogram of chest and limb lead reversal. Am. J. Med. 2014, 127, e29–e30. [Google Scholar] [CrossRef] [PubMed]
- Medani, S.A.; Hensey, M.; Caples, N.; Owens, P. Accuracy in precordial ECG lead placement: Improving performance through a peer-led educational intervention. J. Electrocardiol. 2018, 51, 50–54. [Google Scholar] [CrossRef]
- Thaler, T.; Tempelmann, V.; Maggiorini, M.; Rudiger, A. The frequency of electrocardiographic errors due to electrode cable switches: A before and after study. J. Electrocardiol. 2010, 43, 676–681. [Google Scholar] [CrossRef]
- Mond, H.G.; Garcia, J.; Visagathilagar, T. Twisted Leads: The Footprints of Malpositioned Electrocardiographic Leads. Heart Lung Circ. 2016, 25, 61–67. [Google Scholar] [CrossRef]
- Baranchuk, A.; Shaw, C.; Alanazi, H.; Campbell, D.; Bally, K.; Redfearn, D.P.; Simpson, C.S.; Abdollah, H. Electrocardiography Pitfalls and Artifacts: The 10 Commandments. Crit. Care Nurse 2009, 29, 67–73. [Google Scholar] [CrossRef]
- Batchvarov, V.N.; Malik, M.; Camm, A.J. Incorrect electrode cable connection during electrocardiographic recording. Europace 2007, 9, 1081–1090. [Google Scholar] [CrossRef] [PubMed]
- Rosen, A.V.; Koppikar, S.; Shaw, C.; Baranchuk, A. Common ECG Lead Placement Errors. Part I: Limb lead Reversals. Int. J. Med. Stud. 2014, 2, 92–98. [Google Scholar]
- Rosen, A.V.; Koppikar, S.; Shaw, C.; Baranchuk, A. Common ECG Lead Placement Errors. Part II: Precordial Misplacements. Int. J. Med. Stud. 2014, 2, 99–103. [Google Scholar]
- Sakaguchi, S.; Sandberg, J.; Benditt, D. ECG Electrode Reversals: An Opportunity to Learn from Mistakes. J. Cardiovasc. Electrophysiol. 2018, 29, 806–815. [Google Scholar] [CrossRef] [PubMed]
- Abdollah, H.; Milliken, J.A. Recognition of electrocardiographic left arm/left leg lead reversal. Am. J. Cardiol. 1997, 80, 1247–1249. [Google Scholar] [CrossRef]
- Hedén, B.; Ohlsson, M.; Holst, H.; Mjöman, M.; Rittner, R.; Pahlm, O.; Peterson, C.; Edenbrandt, L. Detection of frequently overlooked electrocardiographic lead reversals using artificial neural networks. Am. J. Cardiol. 1996, 78, 600–604. [Google Scholar] [CrossRef]
- Hoffman, I. A flatline electrocardiogram in lead II is a marker for right arm/right leg electrode switch. J. Electrocardiol. 2007, 40, 226–227. [Google Scholar] [CrossRef] [PubMed]
- Han, C.; Gregg, R.; Babaeizadeh, S. Automatic Detection of ECG Lead-wire Interchange for Conventional and Mason-Likar Lead Systems. Comput. Cardiol. 2014, 41, 145–148. [Google Scholar]
- Krishnan, R.; Ramesh, M. QRS axis based classification of electrode interchange in wearable ECG devices. EAI Endorsed Trans. Future Intell. Educ. Env. 2015, 2. [Google Scholar] [CrossRef]
- Ho, R.T.; Mukherji, L.; Evans, G.T.Jr. Simple diagnosis of limb-lead reversals by predictable changes in QRS axis. Pacing Clin. Electrophysiol. 2006, 29, 272–277. [Google Scholar] [CrossRef]
- De Bie, J.; Mortara, D.W.; Clark, T.F. The development and validation of an early warning system to prevent the acquisition of 12-lead resting ECGs with interchanged electrode positions. J. Electrocardiol. 2014, 47, 794–797. [Google Scholar] [CrossRef] [PubMed]
- Ho, K.K.L.; Ho, S.K. Use of the sinus P wave in diagnosing electrocardiographic limb lead misplacement not involving the right leg (ground) lead. J. Electrocardiol. 2001, 34, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Kors, J.A.; van Herpen, G. Accurate automatic detection of electrode interchange in the electrocardiogram. Am. J. Cardiol. 2001, 88, 396–399. [Google Scholar] [CrossRef]
- Han, C.; Gregg, R.E.; Field, D.Q.; Babaeizadeh, S. Automatic detection of ECG cable interchange by analyzing both morphology and interlead relations. J. Electrocardiol. 2014, 47, 781–787. [Google Scholar] [CrossRef] [PubMed]
- Gregg, R.; Hancock, E.W.; Babaeizadeh, S. Detecting ECG limb lead-wire interchanges involving the right leg lead-wire. Comput. Cardiol. 2017, 44. [Google Scholar] [CrossRef]
- Xia, H.; Garcia, G.A.; Zhao, X. Automatic detection of ECG electrode misplacement: A tale of two algorithms. Physiol. Meas. 2012, 33, 1549–1561. [Google Scholar] [CrossRef] [PubMed]
- Dotsinsky, I.; Daskalov, I.; Iliev, I. Detection of peripheral ECG electrodes misplacement. Proc. 7th Int. Conf. Electronics ET’98, Sozopol, Bulgaria 1998, S2, 21–26. Available online: http://ecad.tu-sofia.bg/et/1998/Statii%20ET98-II/Detection%20of%20Peripheral%20ECG%20Electrodes%20Misplacement.pdf (accessed on 24 February 2019).
- Jekova, I.; Krasteva, V.; Leber, R.; Schmid, R.; Twerenbold, R.; Müller, C.; Reichlin, T.; Abächerli, R. Inter-lead correlation analysis for automated detection of cable reversals in 12/16-lead ECG. Comput. Methods Programs Biomed. 2016, 134, 31–41. [Google Scholar] [CrossRef]
- Végső, B.; Balázs, G.; Gaál, B.; Kozmann, G. Electrode reversal detection in ECG remote monitoring. Meas. Sci. Rev. 2005, 5, 45–48. Available online: http://www.measurement.sk/2005/S2/Vegso.pdf (accessed on 24 February 2019).
- Cooper, C.; Clark, E.; Macfarlane, P.W. Enhanced Detection of Electrode Placement/Connection Errors. Comput. Cardiol. 2008, 35, 89–92. [Google Scholar] [CrossRef]
- Bond, R.; Finlay, D.; Nugent, C.; Moore, G.; Guldenring, D. A simulation tool for visualizing and studying the effects of electrode misplacement on the 12-lead electrocardiogram. J. Electrocardiol. 2011, 44, 439–444. [Google Scholar] [CrossRef]
- Macfarlane, P.W.; Van Oosterom, A.; Pahlm, O.; Kligfield, P.; Janse, M.; Camm, J. Comprehensive Electrocardiography, 2nd ed.; Springer-Verlag: London, UK, 2010; ISBN 978-1-84882-047-0. [Google Scholar]
- Gargiulo, G.D. True Unipolar ECG Machine for Wilson Central Terminal Measurements. BioMed Res. Int. 2015, 586397, 1–7. [Google Scholar] [CrossRef] [PubMed]
- IEC 60601-2-25 International Standard. Medical electrical equipment—Part 2–25: Particular requirements for the basic safety and essential performance of electrocardiographs, 2nd ed.; International Electrotechnical Commission: Geneva, Switzerland, 2011. [Google Scholar]
- Kligfield, P.; Badilini, F.; Denjoy, I.; Babaeizadeh, S.; Clark, E.M.A.; de Bie, J.; Devine, B.; Extramiana, F.; Generali, G.; Gregg, R.; et al. Comparison of automated interval measurements by widely used algorithms in digital electrocardiographs. Am. Heart J. 2018, 200, 1–10. [Google Scholar] [CrossRef]
- Krasteva, V.; Jekova, I.; Schmid, R. Perspectives of human verification via binary QRS template matching of single-lead and 12-lead electrocardiogram. Plos ONE 2018, 13, e0197240. [Google Scholar] [CrossRef] [PubMed]
- Gargiulo, G.D.; Bifulco, P.; Cesarelli, M.; McEwan, A.; Moeinzadeh, H.; O’Loughlin, A.; Shugman, I.M.; Tapson, J.C.; Thiagalingam, A. On the Zero of Potential of the Electric Field Produced by the Heart Beat. A Machine Capable of Estimating this Underlying Persistent Error in Electrocardiography. Machines 2016, 4, 18. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Reversed Electrodes | ΔPWCT | |
|---|---|---|
| Reversals of peripheral electrodes not involving RL | ↔ | * |
| ↔ | * | |
| ↔ | * | |
| CW rotation →→→ | * | |
| CCW rotation →→→ | * | |
| Reversals of peripheral electrodes involving RL | ↔ | |
| ↔ | ||
| ↔ | 0 * | |
| CW rotation with RL →→→→ | ||
| CCW rotation with RL →→→→ | 0 * | |
| Bilateral arm–leg rotation ↔, ↔ | ||
| Cross rotation →→→→ | ||
| Reversals of unicolor peripheral and chest electrodes | Red electrodes ↔ | |
| Yellow electrodes ↔ | ||
| Green electrodes ↔ | ||
| Black electrodes ↔ | * | |
| All unicolor electrodes ↔, ↔, ↔, ↔ |
| Reversed Electrodes | Reordered Leads | ||
|---|---|---|---|
| ↔ | |||
| ↔ | |||
| ↔ | |||
| CW rotation →→→ | |||
| CCWrotation →→→ | |||
| Reversed Electrodes | Reordered Leads | ||
|---|---|---|---|
| ↔ | |||
| ↔ | |||
| ↔ | |||
| CW rotation with RL →→→→ | |||
| CCW rotation with RL →→→→ | |||
| Bilateral arm–leg rotation ↔, ↔ | |||
| Cross rotation →→→→ | |||
| Reversed Electrodes | Reordered Leads | ||
|---|---|---|---|
| Red electrodes ↔ | |||
| Yellow electrodes ↔ | |||
| Green electrodes ↔ | |||
| Black electrodes ↔ | |||
| All unicolor electrode pairs ↔, ↔, ↔, ↔ | |||
| Unicolor Reversals | RMS Error (µV) | Peak Error (µV) | Cor. Coef. (0–1) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Transf. None | Transf. MSMinv Forward | Transf. MSMinv Inverse | Transf. None | Transf. MSMinv Forward | Transf. MSMinv Inverse | Transf. None | Transf. MSMinv Forward | Transf. MSMinv Inverse | ||
| RA-C1 | I | 81 ± 40 | 14 ± 5 * | 15 ± 5 * | 351 ± 162 | 48 ± 19 * | 53 ± 20 * | 0.921 ± 0.093 | 0.997 ± 0.004 * | 0.995 ± 0.006 * |
| II | 81 ± 38 | 13 ± 5 * | 13 ± 4 * | 356 ± 163 | 48 ± 19 * | 46 ± 16 * | 0.909 ± 0.172 | 0.998 ± 0.002 * | 0.996 ± 0.005 * | |
| V1 | 120 ± 52 | 11 ± 4 * | 11 ± 4 * | 529 ± 227 | 38 ± 15 * | 38 ± 13 * | 0.832 ± 0.136 | 0.996 ± 0.002 * | 0.998 ± 0.002 * | |
| Vx | 27 ± 13 | 11 ± 5 * | 12 ± 5 * | 116 ± 61 | 44 ± 9 * | 42 ± 18 * | 0.989 ± 0.029 | 0.998 ± 0.003 * | 0.998 ± 0.003 * | |
| LA-C2 | I | 197 ± 80 | 16 ± 5 * | 15 ± 5 * | 924 ± 336 | 55 ± 20 * | 54 ± 20 * | 0.746 ± 0.144 | 0.997 ± 0.004 * | 0.995 ± 0.005 * |
| II | 18 ± 5 | 13 ± 3 * | 13 ± 3 * | 78 ± 37 | 44 ± 12 * | 46 ± 13 * | 0.994 ± 0.013 | 0.995 ± 0.011 * | 0.995 ± 0.009 * | |
| V2 | 246 ± 102 | 13 ± 6 * | 13 ± 5 * | 1121 ± 396 | 50 ± 25 * | 54 ± 26 * | 0.456 ± 0.180 | 0.990 ± 0.010 * | 0.998 ± 0.002 * | |
| Vx | 58 ± 5 | 12 ± 4 * | 12 ± 5 * | 264 ± 103 | 41 ± 16 * | 47 ± 19 * | 0.956 ± 0.073 | 0.998 ± 0.003 * | 0.997 ± 0.003 * | |
| LL-C3 | I | 15 ± 5 | 15 ± 5 | 15 ± 6 | 56 ± 27 | 54 ± 23 | 56 ± 26 | 0.996 ± 0.006 | 0.995 ± 0.006 * | 0.995 ± 0.006 * |
| II | 154 ± 50 | 18 ± 5* | 15 ± 4 * | 644 ± 228 | 59 ± 22 * | 53 ± 20 * | 0.869 ± 0.146 | 0.998 ± 0.001 * | 0.995 ± 0.008 * | |
| V3 | 206 ± 65 | 12 ± 5 * | 14 ± 5 * | 868 ± 296 | 47 ± 25 * | 53 ± 21 * | 0.512 ± 0.197 | 0.988 ± 0.012 * | 0.997 ± 0.004 * | |
| Vx | 52 ± 18 | 12 ± 5 * | 13 ± 5 * | 219 ± 80 | 45 ± 23 * | 46 ± 20 * | 0.970 ± 0.051 | 0.997 ± 0.004 * | 0.997 ± 0.003* | |
| RL-C5 | I | 16 ± 5 | 15 ± 5 | 15 ± 5 | 57 ± 24 | 54 ± 20 | 54 ± 20 | 0.995 ± 0.008 | 0.995 ± 0.008 | 0.995 ± 0.009 |
| II | 14 ± 4 | 14 ± 4 | 14 ± 4 | 47 ± 15 | 48 ± 18 | 48 ± 17 | 0.995 ± 0.009 | 0.995 ± 0.009 | 0.995 ± 0.010 | |
| V5 | 131 ± 60 | 24 ± 12 *$ | 136 ± 54 # | 639 ± 287 | 102 ± 54 *$ | 660 ± 268 # | 0.785 ± 0.210 | 0.957 ± 0.047 *$ | 0.792 ± 0.144 # | |
| Vx | 14 ± 5 | 14 ± 5 * | 14 ± 5 * | 51 ± 25 | 51 ± 25 | 51 ± 25 | 0.998 ± 0.002 | 0.998 ± 0.002 | 0.997 ± 0.002 | |
| I | 143 ± 72 | 17 ± 9 * | 18 ± 8 * | 726 ± 361 | 59 ± 33 * | 69 ± 35 * | 0.836 ± 0.100 | 0.994 ± 0.006 * | 0.994 ± 0.005 * | |
| II | 138 ± 45 | 19 ± 5 * | 18 ± 9 * | 631 ± 275 | 71 ± 26 * | 60 ± 27 * | 0.925 ± 0.062 | 0.997 ± 0.002 * | 0.993 ± 0.009 * | |
| V1 | 225 ± 97 | 16 ± 5 * | 14 ± 5 * | 967 ± 445 | 50 ± 17 * | 57 ± 18 * | 0.652 ± 0.195 | 0.996 ± 0.003 * | 0.997 ± 0.003 * | |
| V2 | 289 ± 125 | 16 ± 7 * | 18 ± 8 * | 1235 ± 487 | 62 ± 35 * | 69 ± 30 * | 0.365 ± 0.133 | 0.993 ± 0.007 * | 0.996 ± 0.004 * | |
| V3 | 248 ± 92 | 15 ± 5 * | 16 ± 4 * | 1003 ± 378 | 55 ± 19 * | 58 ± 23 * | 0.494 ± 0.184 | 0.994 ± 0.010 * | 0.997 ± 0.003* | |
| V4 | 110 ± 56 | 14 ± 4 * | 16 ± 4 * | 443 ± 258 | 54 ± 20 * | 58 ± 25 * | 0.835 ± 0.204 | 0.997 ± 0.003 * | 0.997 ± 0.002 * | |
| V5 | 161 ± 63 | 26 ± 10 *$ | 142 ± 75 # | 615 ± 285 | 104 ± 50*$ | 659 ± 368 # | 0.705 ± 0.230 | 0.986 ± 0.019 *$ | 0.859 ± 0.106 # | |
| V6 | 113 ± 53 | 13 ± 5 * | 13 ± 5 * | 472 ± 231 | 50 ± 23 * | 45 ± 16 * | 0.886 ± 0.135 | 0.998 ± 0.002 * | 0.996 ± 0.005 * | |
| Accuracy | |||
|---|---|---|---|
| Unicolor Lead Swaps | RMS Error (%) | Peak Error (%) | Cor Coef (%) |
| 100 | 96 * | 100 | |
| 96 * | 88 # | 96 * | |
| 100 | 88 # | 100 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krasteva, V.; Jekova, I.; Schmid, R. Simulating Arbitrary Electrode Reversals in Standard 12-Lead ECG. Sensors 2019, 19, 2920. https://doi.org/10.3390/s19132920
Krasteva V, Jekova I, Schmid R. Simulating Arbitrary Electrode Reversals in Standard 12-Lead ECG. Sensors. 2019; 19(13):2920. https://doi.org/10.3390/s19132920
Chicago/Turabian StyleKrasteva, Vessela, Irena Jekova, and Ramun Schmid. 2019. "Simulating Arbitrary Electrode Reversals in Standard 12-Lead ECG" Sensors 19, no. 13: 2920. https://doi.org/10.3390/s19132920
APA StyleKrasteva, V., Jekova, I., & Schmid, R. (2019). Simulating Arbitrary Electrode Reversals in Standard 12-Lead ECG. Sensors, 19(13), 2920. https://doi.org/10.3390/s19132920