1. Introduction
Throughout our lives, practically everyone will experience an incident that will affect our musculoskeletal (MSK) or neuromuscular system. At these issues, the effects can take the form of acute injuries, such as fractures, breaks or muscle tears, sprains, tendinitis, cerebrovascular accidents with peripheral muscular paralysis, etc. In addition, they can evolve as subacute or chronic processes such as degenerative processes, rheumatological diseases or neuropathies with muscular involvement.
The impact of these diseases on our functional ability depends not only on the severity of the process but also on the treatment that will be applied. In this way, rehabilitation treatments play a fundamental role in the results that follow any type of orthopedic or sports injury or perhaps a surgical procedure. In these cases, several basic goals must be pursued, such as early mobilization and the establishment of adequate objectives to carry out such mobilization [
1]. Many people with MSK pathologies benefit from the association of rehabilitation along with complementary medical treatments, so symptoms and disability are reduced, improving functional ability [
2].
Prior to the establishment of a treatment, both medical or rehabilitative, a correct diagnosis is essential. The diagnostic task begins with an appropriate medical history, which is, usually, complemented with various imaging tests. These ones include simple X-ray, axial tomography, magnetic resonance or USI (UltraSound Imaging). USI is a non-invasive, safe (there is no radiation), repeatable technique and provides a dynamic study; therefore, it is widely accepted by both patients and medical services. In addition, thanks to technological advances, the resolution of USI equipment has been improved remarkably, hence it provides better quality images.
In the last decade [
3,
4], the use of ultrasound for imaging in the context of MSK evaluation in rehabilitation environments has expanded dramatically because it allows high-resolution images to be available in real time. Pioneering applications of ultrasound at MSK studies date back from 1970, for research on the rotator cuff [
5]. Nowdays, this image technology adds accuracy on diagnosis and certainty to guide the needle insertion in therapeutic interventional procedures [
6] such as drainage, infiltrations, etc. These benefits have led, in advanced countries, to its growing use in MSK clinics and rehabilitation installations, by providing clinical, anatomical, and technical integration in a one-day-evaluation [
6].
Despite its obvious benefits, USI is a strongly operator-dependent technique, both at the image capturing stage and at the following evaluation stage. The sonoanatomy of MSK structures differs from magnetic resonance and radiographic and tomographic images, in such a way that USI images are harder to understand [
6]. Firstly, relating 2D ultrasound imaging to a familiar 3D anatomical model is not a trivial issue. This difficulty can only be overcome by training, hence experience becomes of fundamental relevance [
7]. In fact, USI technique is being incorporated into numerous university education curricula in different medical specialties, as it has proven to be very useful along with physical exploration [
8]. The physician must learn to properly establish the position and orientation of the transducer (probe), and then he has to be able to interpret the obtained images. To do this task, it is necessary to get a correct mental model, that is, the relationship between hand movements and probe orientation with the resulting US image, that will let the learning curve improve [
9]. The cost of equipment is high enough to make it impossible to have a device available for individual practice for medicine students. At present, the best way to acquire a good mental model in USI is a procedure with a simulator, which can transfer the knowledge from an expert [
10]. At this procedure, haptics-based simulators provide a realistic feedback mechanism that allows the trainees to learn from their mistakes and to improve their technique, accelerating their learning process to develop accurate skills, as at our case of study, on MSK diagnosis.
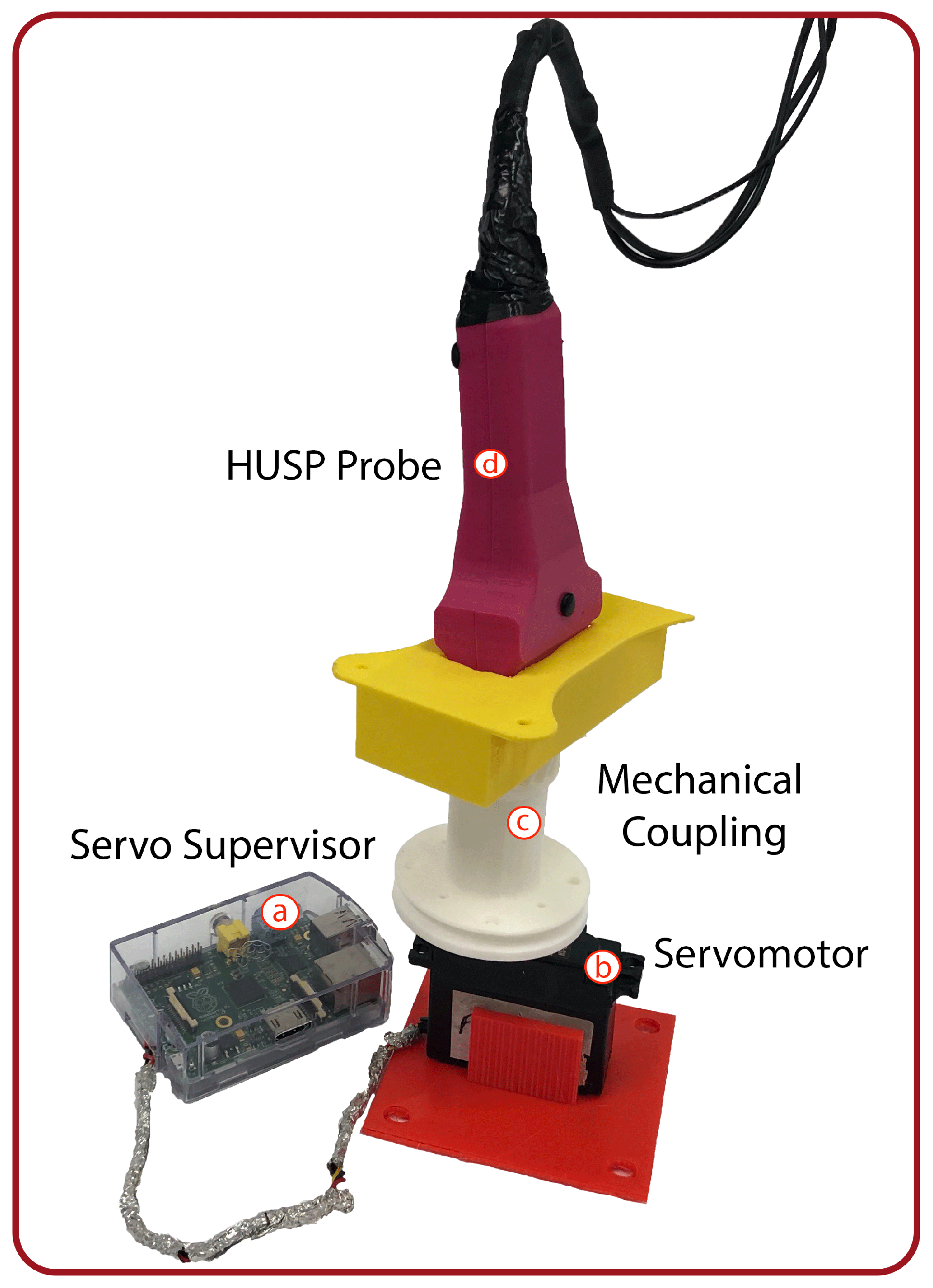
The aim of this paper is to present a tool to train or instruct beginners in the recognition of different MSK tissues through the visualization of a US image. Our solution consists of two components: a probe replica that mimics a real US transducer and a multi-platform desktop application. The probe replica, referred to as HUSP (Haptic US Probe), will be equipped with sensors to capture the movement of a trainee’s hand. The software application reproduces US images, pre-recorded with real equipment, according to the probe movements as it is manipulated by the trainee. The portable nature of the device HUSP facilitates in-home training for the diagnosis of MSK diseases outside clinical and academical institutions. Obviously, the system applicability is not restricted to this medical diagnostic activity area.
Our innovative application needs to estimate the orientation (roll, pitch, yaw) of the HUSP. Inertial sensors can be used to capture data about the orientation of the object that includes the sensor. As a consequence of the huge development in Micro-electromechanical Systems (MEMS) technologies, IMU (Inertial Measurement Unit) sensors become more accurate, lightweight, compact and inexpensive. In [
11], a complete review of the pose estimation methods using MEMS devices can be found.
The measurements of the gyroscope, magnetometer and accelerometer present errors due to bias, noise, magnetic interferences and other external disturbances [
11]. Hence, their accuracy of orientation estimation may be poor if these measurements are considered individually. To improve the orientation estimation accuracy, sensor fusion algorithms (SFAs) are necessary, where accelerometer and magnetometer measurements are used for compensating the drift during gyroscope data integration. In [
12], a comprehensive and systematic review of existing methods to reduce the effect of indoor magnetic disturbances is presented. Following this systematic review, we are going to categorize the SFA proposed in our work to estimate the 3D orientation of the probe.
Among the existing methods to decouple the estimation of the pitch and roll angles from the magnetic disturbance, our method uses the two-step orientation estimation. First, the pitch and roll angles using acceleration and angular velocity are estimated, and then yaw angle with the estimated pitch, roll angles and the magnetometer data are calculated. Ref. [
13] proposed a quaternion-based procedure that, as our proposal, isolates the effect of magnetic disturbances over inclination (pitch and roll) estimations, but it is more sensible to the drift at gyroscope signals. With respect to the methods that address the problem of yaw estimation errors that are related to gyroscope bias, a model-based gyro bias estimation method is used in our solution. In this way, the state vector in the SFA is increased by adding the gyro bias, thus estimating the orientation and the gyro bias simultaneously. Where the SFA selected is concerned, this is a dual-extended Kalman filter with gyro bias estimation, where the orientation is directly represented by the Euler angles. Kalman filters (KFs) and extended Kalman filters (EKFs) are the preferred sensor fusion methods for estimating the attitude (orientation) using IMUs [
14,
15].
The rest of the paper is organized as follows. In
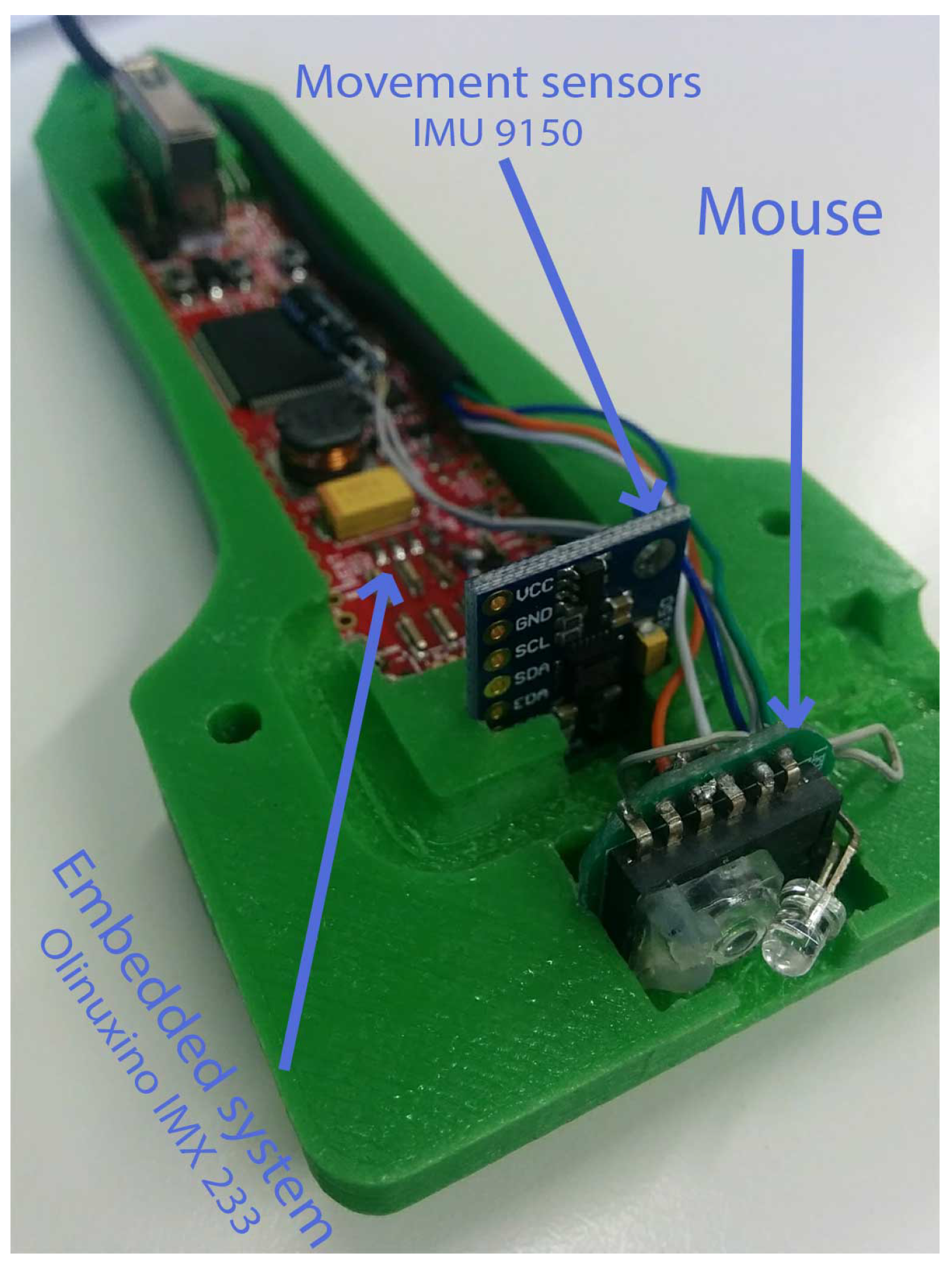
Section 2, the ultrasound probe design will be exposed, and the main components of the hardware design will be described. As a main characteristic, it can be considered as a low cost and powerful embedded system. One key element of this hardware are the sensors, among which the IMU device has a central role. When estimating the orientation of the probe, it will be useful to describe the relationship between the fixed frame and the frame attached to the body (probe). In addition, the algorithm that is needed to estimate the hand orientation in the embedded system will be exposed. In
Section 3, the main results of the computed orientation will be shown. In addition, the global simulating environment will be presented, and a case of study of the use of the probe in a real image based diagnostic task will be exposed. Finally, the discussion and the main conclusions of the work will be presented.
4. Discussion
Diagnosis and treatment of musculoskeletal pathologies, in medical rehabilitation tasks, have benefited from the use of image treatment techniques, where USI stands out for being widely accepted by specialists and patients since it is not a technique based on ionizing radiation. This technology adds the needed accuracy on diagnosis and certainty to guide the professional at therapeutics interventional procedures. However, this technique has a steep learning curve, since the specialists must acquire knowledge that allows them to relate the anatomy of the human body (that is, a three-dimensional space) with the one they will see in the two-dimensional ultrasound images. In order to achieve this mental model, that relates the hand movements and probe orientation with the desired US image, our tool provides an economic learning path with good results.
The learning process can occur at any place with lower hardware requirements than other proposals such as [
19], without loss of precision in the capture of movements. Data on trainee’s hand movements related to 3D orientation (roll, pitch and yaw angles) are captured by means of an inertial sensor based on microelectromechanical systems (MEMS), which meets the cost, payload and space restrictions imposed on HUSP. In [
20], several devices are described in such a way that our base device (MPU-9150) is included. An onboard motion fusion module, named the digital motion processor (DMP), and calibration firmware was integrated into MPU-9150, which enables users to quickly develop motion-based functionality. They show that the performance of the set constituted by this MEMS and its DMP is very poor, but it has interesting advantages such as price, availability or dimensions that we have exploited.
Thus, we have needed to develop our own sensor fusion algorithm which, as shown, has good performance. This is due to the solid work done with our algorithmic proposal: A dual EKF that decouples the estimation of the pitch and roll angles from the magnetic disturbance, using the two-step orientation estimation. In the first step, the EKF estimates pitch and roll using gyro data at the prediction stage and accelerometer data at the correction phase. In the second step, the EKF estimates yaw using, at the prediction stage, the gyro data and the estimated pitch and roll and, at the correction stage, the magnetometer data. The definition of a reduced system state (as in [
16,
17,
18]) at the first EKF achieves: (1) The system model depends only on the pitch and roll angle and it is independent of the yaw angle; (2) the system model is easily linearized; and (3), in the measurement model, the accelerometer output is used directly without further complex transformations. Unlike [
17], at the second EKF, the state of the system includes gyro bias to solve the problem of estimation errors related to gyro bias. Along with the sound formalization of the proposed SFA, an exhaustive calibration of the mathematical models has been carried out.
With all of them, the trainee sensation is completely free of delays as shown in (
http://gro.usal.es/videos/probe.mp4). By considering the complete software interface that has been developed (with an impressive HMI), our proposal system can be used, at any time, by specialists that want to acquire the mental model needed by USI based rehabilitation tasks.

 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}







