
Evolution in Bone Tissue Regeneration: From Grafts to Innovative Biomaterials

 and
and 
Abstract
1. Introduction
2. Literature Review
Leading Causes of Bone Injuries: Trauma and Congenital Diseases
3. Innovations and Applications of Biomaterials in Bone Repair and Regeneration
3.1. Nanostructured Materials: Manufacturing Methods and Clinical Applications in Bone Regeneration
3.2. Conventional Techniques in Bone Regeneration and Orthopedic Implants: Bioinert, Bioactive, and Biodegradable
3.3. Bone Grafts
3.3.1. Autologous Bone
3.3.2. Allogenic Bone
3.3.3. Xenogeneic Bone
3.3.4. Organic Synthetic Grafts
3.3.5. Inorganic Synthetic Grafts
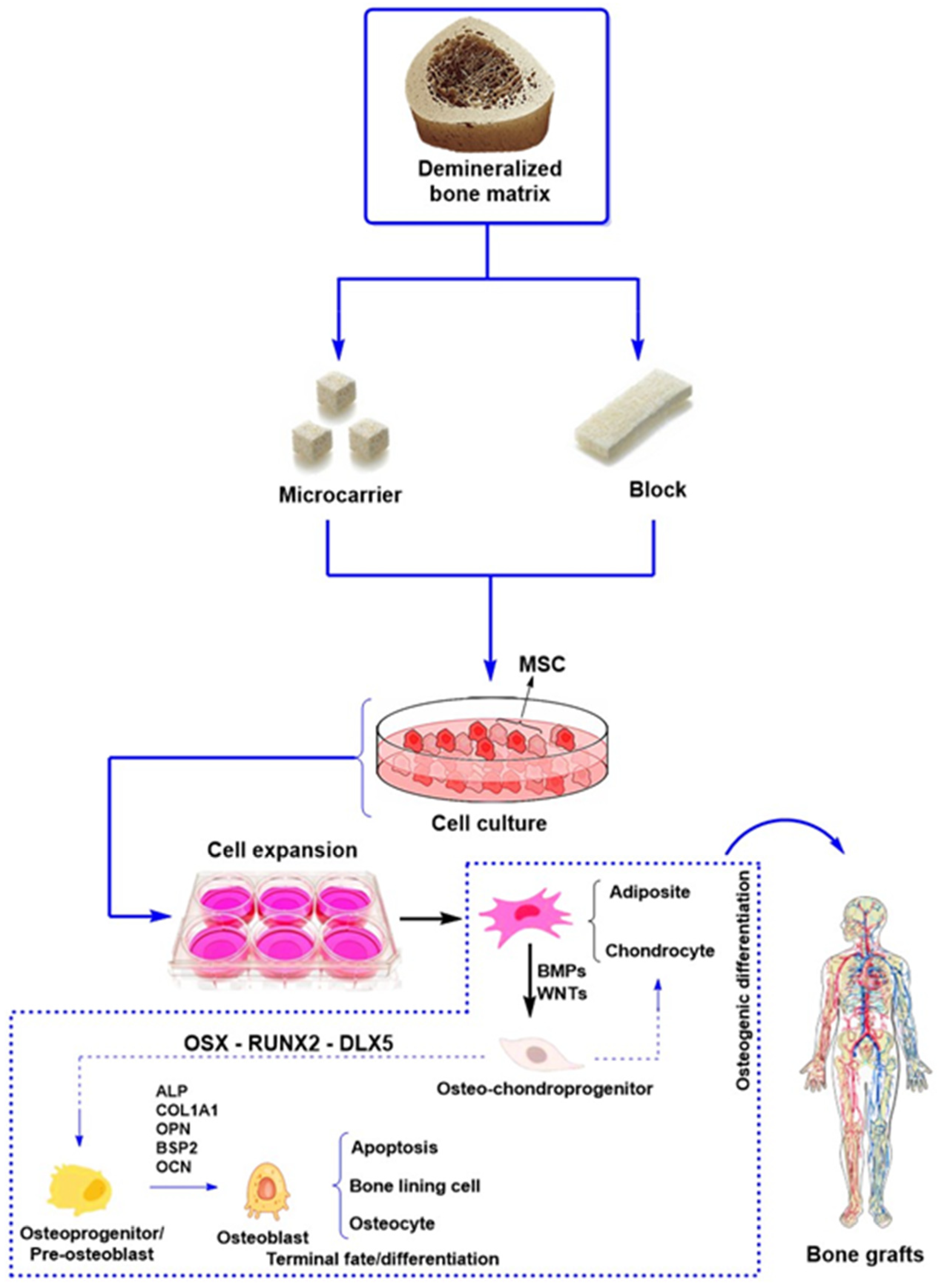
3.4. Demineralized Bone Matrix
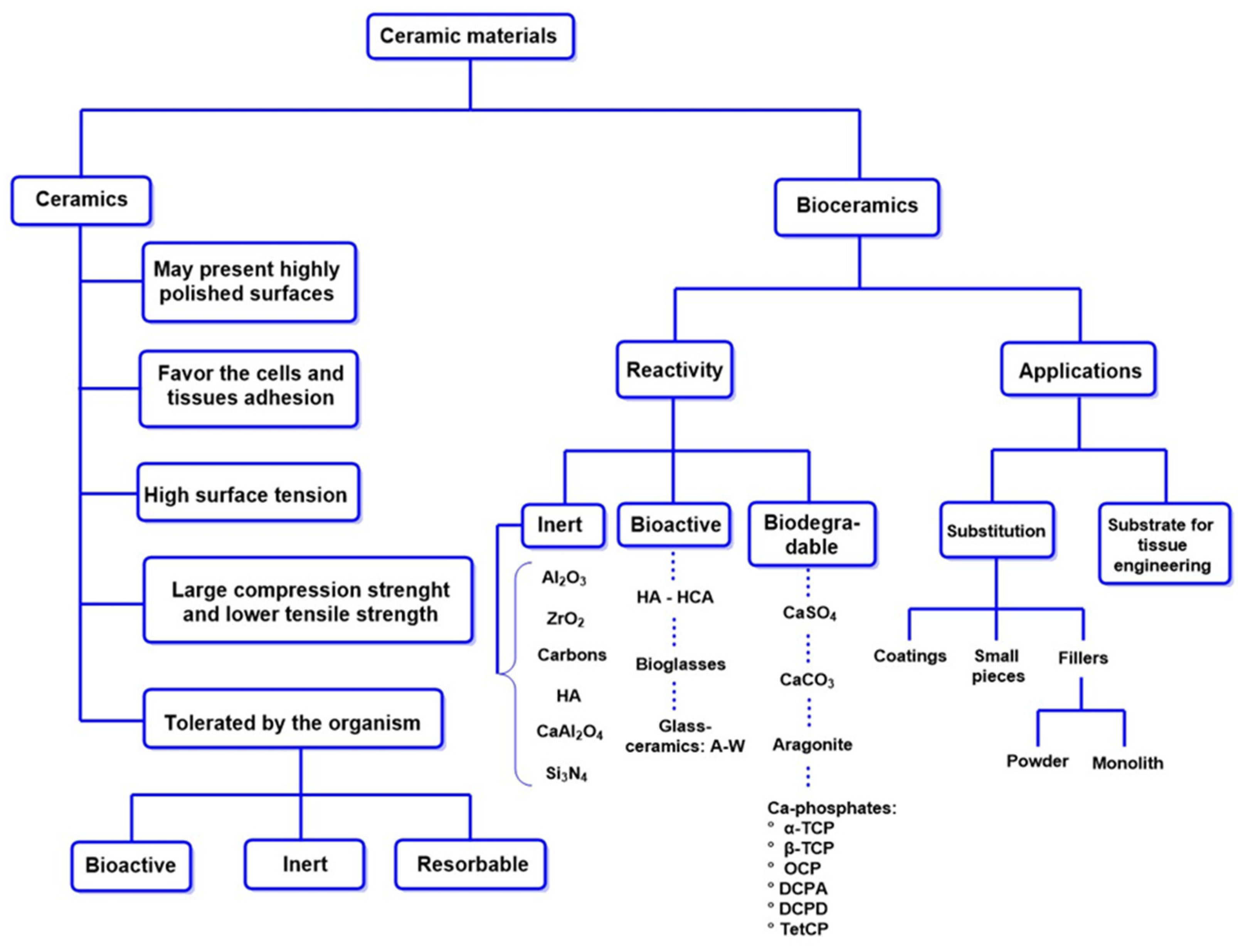
3.5. Ceramic Materials for Bone Scaffolds: Properties and Applications in Bone Regeneration
3.5.1. Ceramics
- Bioinert ceramics (Al2O3, ZrO2): These ceramics do not interact with bone tissue and belong to the first generation.
- Bioactive ceramics (calcium phosphates, bioactive glasses): Facilitate bone integration and possess osteoconductive properties, classified as second-generation materials.
- Third-generation ceramics: Combine features of both previous categories, offering improved mechanical and biological properties.
- Biodegradable ceramics: Incorporate biodegradable polymers to enhance performance in bone regeneration.
Inert Al2O3 and ZrO2 Ceramics in Bone Repair
Calcium Phosphates in Bone Repair: Bioactivity and Tissue Formation
3.5.2. Bioceramics
3.6. Bioglasses: Properties, Synthesis, and Applications in Bone Regeneration
Nanobioglasses: Properties and Applications in Regenerative Medicine
3.7. Synthetic and Natural Polymers Used in Bone Tissue Regeneration
3.7.1. Synthetic and Natural Polymers as a Basis for Nanobiocomposites in Bone Regeneration: Functionality and Advanced Applications
3.7.2. Advances in Potential Nanobiocomposites for Regenerative Medicine
Controlled-Release Systems of Bioactive Molecules for Bone Regeneration
Injectable Cell Therapy for Bone Fractures
4. Smart Stimulus-Responsive Biomaterials for Bone Regeneration
- BT enhances the osteogenic differentiation of MSCs, promoting cell adhesion, proliferation, and migration.
- BN, in nanotube form, exhibits a high protein adsorption capacity, facilitating the osteogenic differentiation of MSCs.
- ZnO increases the bioactivity and mechanical strength of biomaterials, improving their integration with bone tissue.
- Iron oxide nanoparticles have been shown to enhance osteoinduction in vitro, even without external magnetic stimulation;
- When incorporated into bioceramic or polymeric scaffolds, MNPs can further enhance bone regeneration through interactions with the physiological environment.
4.1. Thermosensitive Materials in Promoting Bone Growth and Regeneration
4.2. Piezoelectric Materials
4.3. Photosensitive Hydrogels in Bone Regeneration: Photoinitiators and Modification of Bioactive Properties
- Type I generates free radicals via intramolecular bond cleavage under ultraviolet (UV) light. Representative examples include 2,2-dimethoxy-2-phenylacetophenone (DMPA) and lithium acylphosphinate (LAP).
- Uncontrolled phosphate release, which may affect its osteogenic efficacy;
- Potential long-term cytotoxicity due to phosphorus accumulation in the cellular microenvironment.
4.4. Magnetically Responsive Hydrogels in Bone Regeneration: Nanoparticles, Stimulation, and Controlled Drug Release
- Iron oxides, such as magnetite (Fe3O4) and maghemite (γ-Fe2O3), are widely used due to their biocompatibility and magnetic properties;
- Metallic nanoparticles, composed of cobalt, iron, and nickel, which exhibit higher magnetization but also pose increased cytotoxicity risks.
- High-intensity ultrasound, which facilitates the rapid and uniform formation of nanoparticles;
- Thermal decomposition, a technique used to produce MNPs with controlled size and morphology;
- Co-precipitation, a widely adopted method due to its simplicity and high efficiency in generating superparamagnetic nanoparticles [315].
5. The Future: Advances in Gene Therapies Targeting Tissue Engineering to Promote Bone Formation
6. Conclusions and Future Perspectives
- Design and synthesize hybrid materials that integrate and enhance osteoinductive, osteoconductive, and antimicrobial properties.
- Optimize the thermal stability and biocompatibility of everyday materials used in orthopedic procedures to synchronize the biodegradation time with the healing of the bone defect.
- Explore innovative, low-cost functionalization strategies using nanoparticles that reduce their cytotoxic potential and enhance their integration into common biomaterials in orthopedic procedures.
- It is necessary to strengthen the scalability of these materials to ensure the effective transition and widespread use of these materials in clinical procedures.
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Florencio-Silva, R.; Sasso, G.R.D.S.; Sasso-Cerri, E.; Simões, M.J.; Cerri, P.S. Biology of Bone Tissue: Structure, Function, and Factors That Influence Bone Cells. Biomed Res. Int. 2015, 2015, 421746. [Google Scholar] [CrossRef] [PubMed]
- Manzini, B.M.; Machado, L.M.R.; Noritomi, P.Y.; da Silva, J.V.L. Advances in Bone Tissue Engineering: A Fundamental Review. J. Biosci. 2021, 46, 17. [Google Scholar] [CrossRef]
- Doblaré, M.; García, J.M.; Gómez, M.J. Modelling Bone Tissue Fracture and Healing: A Review. Eng. Fract. Mech. 2004, 71, 1809–1840. [Google Scholar] [CrossRef]
- Collins, M.N.; Ren, G.; Young, K.; Pina, S.; Reis, R.L.; Oliveira, J.M. Scaffold Fabrication Technologies and Structure/Function Properties in Bone Tissue Engineering. Adv. Funct. Mater. 2021, 31, 2010609. [Google Scholar] [CrossRef]
- Vidal, L.; Kampleitner, C.; Brennan, M.; Hoornaert, A.; Layrolle, P. Reconstruction of Large Skeletal Defects: Current Clinical Therapeutic Strategies and Future Directions Using 3D Printing. Front. Bioeng. Biotechnol. 2020, 8, 61. [Google Scholar] [CrossRef] [PubMed]
- Singha, K.; Kumar, V.; Maity, S.; Pandit, P. Development and Processing of Bioinert Polymers and Composites. In Woodhead Publishing in Materials; Ahmed, S.B.T.-A.G.M., Ed.; Woodhead Publishing: Cambridge, UK, 2021; pp. 411–421. ISBN 978-0-12-819988-6. [Google Scholar]
- Ferraz, M.P. Bone Grafts in Dental Medicine: An Overview of Autografts, Allografts and Synthetic Materials. Materials 2023, 16, 4117. [Google Scholar] [CrossRef]
- Kneser, U.; Schaefer, D.J.; Munder, B.; Klemt, C.; Andree, C.; Stark, G.B. Tissue Engineering of Bone. Minim. Invasive Ther. Allied Technol. 2002, 11, 107–116. [Google Scholar] [CrossRef]
- Pape, H.C.; Evans, A.; Kobbe, P. Autologous Bone Graft: Properties and Techniques. J. Orthop. Trauma 2010, 24, 36–40. [Google Scholar] [CrossRef]
- Migliorini, F.; Cuozzo, F.; Torsiello, E.; Spiezia, F.; Oliva, F.; Maffulli, N. Autologous Bone Grafting in Trauma and Orthopaedic Surgery: An Evidence-Based Narrative Review. J. Clin. Med. 2021, 10, 4347. [Google Scholar] [CrossRef]
- Oehme, S.; Burger, J.A.; Krafzick, S.; Bartek, B.; Winkler, T.; Jung, T. Autologous Bone Grafting in Combination with Autologous Chondrocyte Implantation Yields Favourable Outcomes in the Treatment of Osteochondral Defects of the Knee: A Systematic Literature Review. Knee Surg. Sport. Traumatol. Arthrosc. 2024, 32, 2999–3014. [Google Scholar] [CrossRef]
- Diomede, F.; Marconi, G.D.; Fonticoli, L.; Pizzicanella, J.; Merciaro, I.; Bramanti, P.; Mazzon, E.; Trubiani, O. Functional Relationship between Osteogenesis and Angiogenesis in Tissue Regeneration. Int. J. Mol. Sci. 2020, 21, 3242. [Google Scholar] [CrossRef] [PubMed]
- Rather, H.A.; Jhala, D.; Vasita, R. Dual Functional Approaches for Osteogenesis Coupled Angiogenesis in Bone Tissue Engineering. Mater. Sci. Eng. C 2019, 103, 109761. [Google Scholar] [CrossRef] [PubMed]
- Kashte, S.; Jaiswal, A.K.; Kadam, S. Artificial Bone via Bone Tissue Engineering: Current Scenario and Challenges. Tissue Eng. Regen. Med. 2017, 14, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Lima, J.L.D.O.; Sendyk, D.I.; Sendyk, W.R.; Polo, C.I.; Correa, L.; Deboni, M.C.Z. Growth Dynamic of Allogeneic and Autogenous Bone Grafts in a Vertical Model. Braz. Dent. J. 2018, 29, 325–334. [Google Scholar] [CrossRef]
- Zhang, J.; Feng, Y.; Zhou, X.; Shi, Y.; Wang, L. Research Status of Artificial Bone Materials. Int. J. Polym. Mater. Polym. Biomater. 2021, 70, 37–53. [Google Scholar] [CrossRef]
- Feng, P.; Zhao, R.; Tang, W.; Yang, F.; Tian, H.; Peng, S.; Pan, H.; Shuai, C. Structural and Functional Adaptive Artificial Bone: Materials, Fabrications, and Properties. Adv. Funct. Mater. 2023, 33, 2214726. [Google Scholar] [CrossRef]
- Stupp, S.I.; Ciegler, G.W. Organoapatites: Materials for Artificial Bone. I. Synthesis and Microstructure. J. Biomed. Mater. Res. 1992, 26, 169–183. [Google Scholar] [CrossRef] [PubMed]
- Sopyan, I.; Mel, M.; Ramesh, S.; Khalid, K.A. Porous Hydroxyapatite for Artificial Bone Applications. Sci. Technol. Adv. Mater. 2007, 8, 116–123. [Google Scholar] [CrossRef]
- Xu, N.; Ye, X.; Wei, D.; Zhong, J.; Chen, Y.; Xu, G.; He, D. 3D Artificial Bones for Bone Repair Prepared by Computed Tomography-Guided Fused Deposition Modeling for Bone Repair. ACS Appl. Mater. Interfaces 2014, 6, 14952–14963. [Google Scholar] [CrossRef]
- Eivazzadeh-Keihan, R.; Bahojb Noruzi, E.; Khanmohammadi Chenab, K.; Jafari, A.; Radinekiyan, F.; Hashemi, S.M.; Ahmadpour, F.; Behboudi, A.; Mosafer, J.; Mokhtarzadeh, A.; et al. Metal-Based Nanoparticles for Bone Tissue Engineering. J. Tissue Eng. Regen. Med. 2020, 14, 1687–1714. [Google Scholar] [CrossRef]
- Salinas, A.J.; Esbrit, P.; Vallet-Regí, M. A Tissue Engineering Approach Based on the Use of Bioceramics for Bone Repair. Biomater. Sci. 2013, 1, 40–51. [Google Scholar] [CrossRef] [PubMed]
- Biswal, T. Biopolymers for Tissue Engineering Applications: A Review. Mater. Today Proc. 2021, 41, 397–402. [Google Scholar] [CrossRef]
- Bauso, L.V.; La Fauci, V.; Longo, C.; Calabrese, G. Bone Tissue Engineering and Nanotechnology: A Promising Combination for Bone Regeneration. Biology 2024, 13, 237. [Google Scholar] [CrossRef]
- Babuska, V.; Kasi, P.B.; Chocholata, P.; Wiesnerova, L.; Dvorakova, J.; Vrzakova, R.; Nekleionova, A.; Landsmann, L.; Kulda, V. Nanomaterials in Bone Regeneration. Appl. Sci. 2022, 12, 6793. [Google Scholar] [CrossRef]
- Kumar, V.; Tripathi, B.; Srivastava, A.; Saxena, P.S. Nanocomposites as Bone Implant Material BT. In Springer Handbook of Nanomaterials; Vajtai, R., Ed.; Springer: Berlin/Heidelberg, Germany, 2013; pp. 941–976. ISBN 978-3-642-20595-8. [Google Scholar]
- Liu, W.; Zhang, K.; Nan, J.; Lei, P.; Sun, Y.; Hu, Y. Nano Artificial Periosteum PCL/Ta/ZnO Accelerates Repair of Periosteum via Antibacterial, Promoting Vascularization and Osteogenesis. Biomater. Adv. 2023, 154, 213624. [Google Scholar] [CrossRef] [PubMed]
- Ansari, A.I.; Sheikh, N.A. A Review of Bone Regeneration Mechanisms and Bone Scaffold Fabrication Techniques (Conventional and Non-Conventional). J. Inst. Eng. Ser. C 2022, 103, 1485–1513. [Google Scholar] [CrossRef]
- Rahmati, M.; Mills, D.K.; Urbanska, A.M.; Saeb, M.R.; Venugopal, J.R.; Ramakrishna, S.; Mozafari, M. Electrospinning for Tissue Engineering Applications. Prog. Mater. Sci. 2021, 117, 100721. [Google Scholar] [CrossRef]
- Hollinger, J.O.; Einhorn, T.A.; Doll, B.A.; Sfeir, C. Bone Tissue Engineering; CRC Press: Boca Raton, FL, USA, 2004; pp. 1–337. [Google Scholar] [CrossRef]
- Janicki, P.; Schmidmaier, G. What Should Be the Characteristics of the Ideal Bone Graft Substitute? Combining Scaffolds with Growth Factors and/or Stem Cells. Injury 2011, 42, S77–S81. [Google Scholar] [CrossRef]
- Giannoudis, P.V.; Dinopoulos, H.T. Autologous Bone Graft: When Shall We Add Growth Factors? Foot Ankle Clin. 2010, 15, 597–609. [Google Scholar] [CrossRef]
- Gillman, C.E.; Jayasuriya, A.C. FDA-Approved Bone Grafts and Bone Graft Substitute Devices in Bone Regeneration. Mater. Sci. Eng. C 2021, 130, 112466. [Google Scholar] [CrossRef]
- Tollemar, V.; Collier, Z.J.; Mohammed, M.K.; Lee, M.J.; Ameer, G.A.; Reid, R.R. Stem Cells, Growth Factors and Scaffolds in Craniofacial Regenerative Medicine. Genes Dis. 2016, 3, 56–71. [Google Scholar] [CrossRef]
- Swanson, W.B.; Omi, M.; Zhang, Z.; Nam, H.K.; Jung, Y.; Wang, G.; Ma, P.X.; Hatch, N.E.; Mishina, Y. Macropore Design of Tissue Engineering Scaffolds Regulates Mesenchymal Stem Cell Differentiation Fate. Biomaterials 2021, 272, 120769. [Google Scholar] [CrossRef]
- Chen, R.; Hao, Z.; Wang, Y.; Zhu, H.; Hu, Y.; Chen, T.; Zhang, P.; Li, J. Mesenchymal Stem Cell-Immune Cell Interaction and Related Modulations for Bone Tissue Engineering. Stem Cells Int. 2022, 2022, 3584. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Mikos, A.G. Emerging Strategies in Reprogramming and Enhancing the Fate of Mesenchymal Stem Cells for Bone and Cartilage Tissue Engineering. J. Control. Release 2021, 330, 565–574. [Google Scholar] [CrossRef]
- Maraghelli, D.; Giusti, F.; Marini, F.; Brandi, M.L. Bone Tissue and Mineral Metabolism in Hereditary Endocrine Tumors: Clinical Manifestations and Genetic Bases. Orphanet J. Rare Dis. 2020, 15, 102. [Google Scholar] [CrossRef] [PubMed]
- Wade, E.; Messner, S.; Richer, E. Fractures BT. In Handbook of Interpersonal Violence and Abuse Across the Lifespan: A Project of the National Partnership to End Interpersonal Violence Across the Lifespan (NPEIV); Geffner, R., White, J.W., Hamberger, L.K., Rosenbaum, A., Vaughan-Eden, V., Vieth, V.I., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 449–508. ISBN 978-3-319-89999-2. [Google Scholar]
- Forriol, F.; Mazzola, A. Bone Fractures: Generalities BT. In Textbook of Musculoskeletal Disorders; Longo, U.G., Denaro, V., Eds.; Springer International Publishing: Cham, Switzerland, 2023; pp. 241–249. ISBN 978-3-031-20987-1. [Google Scholar]
- Whang, P.G.; Vaccaro, A.R.; Poelstra, K.A.; Patel, A.A.; Anderson, D.G.; Albert, T.J.; Hilibrand, A.S.; Harrop, J.S.; Sharan, A.D.; Ratliff, J.K.; et al. The Influence of Fracture Mechanism and Morphology on the Reliability and Validity of Two Novel Thoracolumbar Injury Classification Systems. Spine 2007, 32, 791–795. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.W.; Herbert, B.; Hao, J.; Min, W.; Ziran, B.H.; Mauffrey, C. Acetabular Fractures in Elderly Patients: A Comparative Study of Low-Energy versus High-Energy Injuries. Int. Orthop. 2015, 39, 1175–1179. [Google Scholar] [CrossRef]
- Li, S.R.; Man, Q.W.; Gao, X.; Lin, H.; Wang, J.; Su, F.C.; Wang, H.Q.; Bu, L.L.; Liu, B.; Chen, G. Tissue-Derived Extracellular Vesicles in Cancers and Non-Cancer Diseases: Present and Future. J. Extracell. Vesicles 2021, 10, e12175. [Google Scholar] [CrossRef]
- Larizza, L.; Roversi, G.; Volpi, L. Rothmund-Thomson Syndrome. Orphanet J. Rare Dis. 2010, 5, 2. [Google Scholar] [CrossRef]
- Lauper, J.M.; Krause, A.; Vaughan, T.L.; Monnat, R.J. Spectrum and Risk of Neoplasia in Werner Syndrome: A Systematic Review. PLoS ONE 2013, 8, e59709. [Google Scholar] [CrossRef]
- Muthusamy, S.; Conway, S.A.; Temple, H.T. Five Polyostotic Conditions That General Orthopedic Surgeons Should Recognize (or Should Not Miss). Orthop. Clin. 2014, 45, 417–429. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.; Zhang, C.; Li, B.; Zhan, S.; Wang, S.; Song, C. Global Burden of Hip Fracture: The Global Burden of Disease Study. Osteoporos. Int. 2024, 35, 41–52. [Google Scholar] [CrossRef]
- Gnoli, M.; Ponti, F.; Sangiorgi, L. Tumor Syndromes That Include Bone Tumors: An Update. Surg. Pathol. Clin. 2017, 10, 749–764. [Google Scholar] [CrossRef]
- Franchi, A. Epidemiology and Classification of Bone Tumors. Clin. Cases Miner. Bone Metab. 2012, 9, 92–95. [Google Scholar]
- Marini, F.; Giusti, F.; Iantomasi, T.; Brandi, M.L. Genetic Determinants of Inherited Endocrine Tumors: Do They Have a Direct Role in Bone Metabolism Regulation and Osteoporosis? Genes 2021, 12, 1286. [Google Scholar] [CrossRef]
- Gerstenfeld, L.C.; Cullinane, D.M.; Barnes, G.L.; Graves, D.T.; Einhorn, T.A. Fracture Healing as a Post-Natal Developmental Process: Molecular, Spatial, and Temporal Aspects of Its Regulation. J. Cell. Biochem. 2003, 88, 873–884. [Google Scholar] [CrossRef] [PubMed]
- Muire, P.J.; Mangum, L.H.; Wenke, J.C. Time Course of Immune Response and Immunomodulation During Normal and Delayed Healing of Musculoskeletal Wounds. Front. Immunol. 2020, 11, 1056. [Google Scholar] [CrossRef] [PubMed]
- Schmidt-Bleek, K.; Schell, H.; Kolar, P.; Pfaff, M.; Perka, C.; Buttgereit, F.; Duda, G.; Lienau, J. Composition of the Initial Fracture Hematoma Compared to a Muscle Hematoma: A Study in Sheep. J. Orthop. Res. 2009, 27, 1147. [Google Scholar] [CrossRef]
- Einhorn, T.A.; Gerstenfeld, L.C. Fracture Healing: Mechanisms and Interventions. Nat. Rev. Rheumatol. 2015, 11, 45–54. [Google Scholar] [CrossRef]
- Łuczak, J.W.; Palusińska, M.; Matak, D.; Pietrzak, D.; Nakielski, P.; Lewicki, S.; Grodzik, M.; Szymański, Ł. The Future of Bone Repair: Emerging Technologies and Biomaterials in Bone Regeneration. Int. J. Mol. Sci. 2024, 25, 12766. [Google Scholar] [CrossRef]
- Jeffery, E.C.; Mann, T.L.A.; Pool, J.A.; Zhao, Z.; Morrison, S.J. Bone Marrow and Periosteal Skeletal Stem/Progenitor Cells Make Distinct Contributions to Bone Maintenance and Repair. Cell Stem Cell 2022, 29, 1547.e6–1561.e6. [Google Scholar] [CrossRef] [PubMed]
- Sharifi, M.; Kheradmandi, R.; Salehi, M.; Alizadeh, M.; ten Hagen, T.L.M.; Falahati, M. Criteria, Challenges, and Opportunities for Acellularized Allogeneic/Xenogeneic Bone Grafts in Bone Repairing. ACS Biomater. Sci. Eng. 2022, 8, 3199–3219. [Google Scholar] [CrossRef] [PubMed]
- Henning, C.; Poglia, G.; Leie, M.A.; Galia, C.R. Comparative Study of Subtalar Arthrodesis after Calcaneal Frature Malunion with Autologous Bone Graft or Freeze-Dried Xenograft. J. Exp. Orthop. 2015, 2, 10. [Google Scholar] [CrossRef] [PubMed]
- Kubosch, E.J.; Bernstein, A.; Wolf, L.; Fretwurst, T.; Nelson, K.; Schmal, H. Clinical Trial and In-Vitro Study Comparing the Efficacy of Treating Bony Lesions with Allografts versus Synthetic or Highly-Processed Xenogeneic Bone Grafts. BMC Musculoskelet. Disord. 2016, 17, 77. [Google Scholar] [CrossRef]
- Malkova, T.A.; Borzunov, D.Y. International Recognition of the Ilizarov Bone Reconstruction Techniques: Current Practice and Research (Dedicated to 100th Birthday of G. A. Ilizarov). World J. Orthop. 2021, 12, 515–533. [Google Scholar] [CrossRef]
- Papakostidis, C.; Giannoudis, P.V. Reconstruction of Infected Long Bone Defects: Issues and Challenges. Injury 2023, 54, 807–810. [Google Scholar] [CrossRef]
- Sun, H.; Zhang, C.; Zhang, B.; Song, P.; Xu, X.; Gui, X.; Chen, X.; Lu, G.; Li, X.; Liang, J.; et al. 3D Printed Calcium Phosphate Scaffolds with Controlled Release of Osteogenic Drugs for Bone Regeneration. Chem. Eng. J. 2022, 427, 130961. [Google Scholar] [CrossRef]
- Van der Heide, D.; Cidonio, G.; Stoddart, M.J.; D’Este, M. 3D Printing of Inorganic-Biopolymer Composites for Bone Regeneration. Biofabrication 2022, 14, 042003. [Google Scholar] [CrossRef]
- Frączek, W.; Kotela, A.; Kotela, I.; Grodzik, M. Nanostructures in Orthopedics: Advancing Diagnostics, Targeted Therapies, and Tissue Regeneration. Materials 2024, 17, 6162. [Google Scholar] [CrossRef]
- Shrivats, A.R.; Alvarez, P.; Schutte, L.; Hollinger, J.O. Bone Regeneration. In Principles of Tissue Engineering, 4th ed.; Elsevier: Amsterdam, The Netherlands, 2013; pp. 1201–1221. [Google Scholar] [CrossRef]
- Matić, A.; Sher, E.K.; Farhat, E.K.; Sher, F. Nanostructured Materials for Drug Delivery and Tissue Engineering Applications. In Molecular Biotechnology; Springer: Berlin/Heidelberg, Germany, 2023. [Google Scholar] [CrossRef]
- Cui, Y.; Li, H.; Li, Y.; Mao, L. Novel Insights into Nanomaterials for Immunomodulatory Bone Regeneration. Nanoscale Adv. 2022, 4, 334–352. [Google Scholar] [CrossRef]
- De Armentia, S.L.; Del Real, J.C.; Paz, E.; Dunne, N. Advances in Biodegradable 3D Printed Scaffolds with Carbon-Based Nanomaterials for Bone Regeneration. Materials 2020, 13, 5083. [Google Scholar] [CrossRef]
- La, W.G.; Jang, J.; Kim, B.S.; Lee, M.S.; Cho, D.W.; Yang, H.S. Systemically Replicated Organic and Inorganic Bony Microenvironment for New Bone Formation Generated by a 3D Printing Technology. RSC Adv. 2016, 6, 11546–11553. [Google Scholar] [CrossRef]
- Saijo, H.; Igawa, K.; Kanno, Y.; Mori, Y.; Kondo, K.; Shimizu, K.; Suzuki, S.; Chikazu, D.; Iino, M.; Anzai, M.; et al. Maxillofacial Reconstruction Using Custom-Made Artificial Bones Fabricated by Inkjet Printing Technology. J. Artif. Organs 2009, 12, 200–205. [Google Scholar] [CrossRef]
- Haberstroh, K.; Ritter, K.; Kuschnierz, J.; Bormann, K.; Kaps, C.; Carvalho, C.; Mülhaupt, R.; Sittinger, M.; Gellrich, N. Bone Repair by Cell-seeded 3D-bioplotted Composite Scaffolds Made of Collagen Treated Tricalciumphosphate or Tricalciumphosphate-chitosan-collagen Hydrogel or PLGA in Ovine Critical-sized Calvarial Defects. J. Biomed. Mater. Res. Part B Appl. Biomater. 2010, 93, 520–530. [Google Scholar] [CrossRef]
- Lopez, C.D.; Diaz-Siso, J.R.; Witek, L.; Bekisz, J.M.; Cronstein, B.N.; Torroni, A.; Flores, R.L.; Rodriguez, E.D.; Coelho, P.G. Three Dimensionally Printed Bioactive Ceramic Scaffold Osseoconduction across Critical-Sized Mandibular Defects. J. Surg. Res. 2018, 223, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Xia, L.; Zhai, D.; Shi, M.; Luo, Y.; Feng, C.; Fang, B.; Yin, J.; Chang, J.; Wu, C. Mesoporous Bioactive Glass Nanolayer-Functionalized 3D-Printed Scaffolds for Accelerating Osteogenesis and Angiogenesis. Nanoscale 2015, 7, 19207–19221. [Google Scholar] [CrossRef]
- Habibovic, P.; Gbureck, U.; Doillon, C.J.; Bassett, D.C.; van Blitterswijk, C.A.; Barralet, J.E. Osteoconduction and Osteoinduction of Low-Temperature 3D Printed Bioceramic Implants. Biomaterials 2008, 29, 944–953. [Google Scholar] [CrossRef]
- Abarrategi, A.; Moreno-Vicente, C.; Martínez-Vázquez, F.J.; Civantos, A.; Ramos, V.; Sanz-Casado, J.V.; Martínez-Corriá, R.; Perera, F.H.; Mulero, F.; Miranda, P.; et al. Biological Properties of Solid Free Form Designed Ceramic Scaffolds with Bmp-2: In Vitro and In Vivo Evaluation. PLoS ONE 2012, 7, e34117. [Google Scholar] [CrossRef]
- Shim, J.-H.; Moon, T.-S.; Yun, M.-J.; Jeon, Y.-C.; Jeong, C.-M.; Cho, D.-W.; Huh, J.-B. Stimulation of Healing within a Rabbit Calvarial Defect by a PCL/PLGA Scaffold Blended with TCP Using Solid Freeform Fabrication Technology. J. Mater. Sci. Mater. Med. 2012, 23, 2993–3002. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.-H.; Kim, S.E.; Park, J.Y.; Kundu, J.; Kim, S.W.; Kang, S.S.; Cho, D.-W. Three-Dimensional Printing of RhBMP-2-Loaded Scaffolds with Long-Term Delivery for Enhanced Bone Regeneration in a Rabbit Diaphyseal Defect. Tissue Eng. Part A 2014, 20, 1980–1992. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.-H.; Yoon, M.-C.; Jeong, C.-M.; Jang, J.; Jeong, S.-I.; Cho, D.-W.; Huh, J.-B. Efficacy of RhBMP-2 Loaded PCL/PLGA/β-TCP Guided Bone Regeneration Membrane Fabricated by 3D Printing Technology for Reconstruction of Calvaria Defects in Rabbit. Biomed. Mater. 2014, 9, 65006. [Google Scholar] [CrossRef]
- Kim, J.; McBride, S.; Tellis, B.; Alvarez-Urena, P.; Song, Y.-H.; Dean, D.D.; Sylvia, V.L.; Elgendy, H.; Ong, J.; Hollinger, J.O. Rapid-Prototyped PLGA/β-TCP/Hydroxyapatite Nanocomposite Scaffolds in a Rabbit Femoral Defect Model. Biofabrication 2012, 4, 25003. [Google Scholar] [CrossRef] [PubMed]
- Xia, Y.; Zhou, P.; Cheng, X.; Xie, Y.; Liang, C.; Li, C.; Xu, S. Selective Laser Sintering Fabrication of Nano-Hydroxyapatite/Poly-ε-Caprolactone Scaffolds for Bone Tissue Engineering Applications. Int. J. Nanomed. 2013, 8, 4197–4213. [Google Scholar]
- Chen, X.; Gao, C.; Jiang, J.; Wu, Y.; Zhu, P.; Chen, G. 3D Printed Porous PLA/NHA Composite Scaffolds with Enhanced Osteogenesis and Osteoconductivity in Vivo for Bone Regeneration. Biomed. Mater. 2019, 14, 65003. [Google Scholar] [CrossRef]
- Rasperini, G.; Pilipchuk, S.P.; Flanagan, C.L.; Park, C.H.; Pagni, G.; Hollister, S.J.; Giannobile, W.V. 3D-Printed Bioresorbable Scaffold for Periodontal Repair. J. Dent. Res. 2015, 94, 153S–157S. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.; Gao, J.; Xu, W.; Wang, X.; Shen, Y.; Tang, J.; Cui, S.; Yang, X.; Liu, Q.; Yu, L. Structural Mechanics of 3D-Printed Poly (Lactic Acid) Scaffolds with Tetragonal, Hexagonal and Wheel-like Designs. Biofabrication 2019, 11, 35009. [Google Scholar] [CrossRef]
- Ge, Z.; Tian, X.; Heng, B.C.; Fan, V.; Yeo, J.F.; Cao, T. Histological Evaluation of Osteogenesis of 3D-Printed Poly-Lactic-Co-Glycolic Acid (PLGA) Scaffolds in a Rabbit Model. Biomed. Mater. 2009, 4, 21001. [Google Scholar] [CrossRef] [PubMed]
- Adamzyk, C.; Kachel, P.; Hoss, M.; Gremse, F.; Modabber, A.; Hölzle, F.; Tolba, R.; Neuss, S.; Lethaus, B. Bone Tissue Engineering Using Polyetherketoneketone Scaffolds Combined with Autologous Mesenchymal Stem Cells in a Sheep Calvarial Defect Model. J. Cranio-Maxillofac. Surg. 2016, 44, 985–994. [Google Scholar] [CrossRef]
- Kang, J.; Wang, L.; Yang, C.; Wang, L.; Yi, C.; He, J.; Li, D. Custom Design and Biomechanical Analysis of 3D-Printed PEEK Rib Prostheses. Biomech. Model. Mechanobiol. 2018, 17, 1083–1092. [Google Scholar] [CrossRef]
- Sheikh, Z.; Najeeb, S.; Khurshid, Z.; Verma, V.; Rashid, H.; Glogauer, M. Biodegradable Materials for Bone Repair and Tissue Engineering Applications. Materials 2015, 8, 5744–5794. [Google Scholar] [CrossRef]
- Jasmine, S.; Krishnamoorthy, R. Biodegradable Materials for Bone Defect Repair. Biodegrad. Mater. Their Appl. 2022, 7, 457–470. [Google Scholar] [CrossRef]
- Bandyopadhyay, A.; Mitra, I.; Goodman, S.B.; Kumar, M.; Bose, S. Improving Biocompatibility for next Generation of Metallic Implants. Prog. Mater. Sci. 2023, 133, 101053. [Google Scholar] [CrossRef] [PubMed]
- Kamboj, N.; Piili, H.; Ganvir, A.; Gopaluni, A.; Nayak, C.; Moritz, N.; Salminen, A. Bioinert Ceramics Scaffolds for Bone Tissue Engineering by Laser-Based Powder Bed Fusion: A Preliminary Review. IOP Conf. Ser. Mater. Sci. Eng. 2023, 1296, 012022. [Google Scholar] [CrossRef]
- Nasiri-Tabrizi, B.; Basirun, W.J.; Yeong, C.H.; Thein, W.M. Development of the Third Generation of Bioceramics: Doping Hydroxyapatite with s-, p-, d-, and f-Blocks Cations and Their Potential Applications in Bone Regeneration and Void Filling. Ceram. Int. 2023, 49, 7142–7179. [Google Scholar] [CrossRef]
- De Wildt, B.W.M.; Ansari, S.; Sommerdijk, N.A.J.M.; Ito, K.; Akiva, A.; Hofmann, S. From Bone Regeneration to Three-Dimensional in Vitro Models: Tissue Engineering of Organized Bone Extracellular Matrix. Curr. Opin. Biomed. Eng. 2019, 10, 107–115. [Google Scholar] [CrossRef]
- Wang, S.; Wang, X.; Draenert, F.G.; Albert, O.; Schröder, H.C.; Mailänder, V.; Mitov, G.; Müller, W.E.G. Bioactive and Biodegradable Silica Biomaterial for Bone Regeneration. Bone 2014, 67, 292–304. [Google Scholar] [CrossRef]
- Dimitriou, R.; Jones, E.; McGonagle, D.; Giannoudis, P.V. Bone Regeneration: Current Concepts and Future Directions. BMC Med. 2011, 9, 66. [Google Scholar] [CrossRef] [PubMed]
- Drăgan, E.; Nemţoi, A. Review of the Long-Term Outcomes of Guided Bone Regeneration and Autologous Bone Block Augmentation for Vertical Dental Restoration of Dental Implants. Med. Sci. Monit. 2022, 28, e937433-1. [Google Scholar] [CrossRef]
- Zwingenberger, S.; Nich, C.; Valladares, R.D.; Yao, Z.; Stiehler, M.; Goodman, S.B. Recommendations and Considerations for the Use of Biologics in Orthopedic Surgery. BioDrugs 2012, 26, 245–256. [Google Scholar] [CrossRef]
- Marino, J.T.; Ziran, B.H. Use of Solid and Cancellous Autologous Bone Graft for Fractures and Nonunions. Orthop. Clin. 2010, 41, 15–26. [Google Scholar] [CrossRef]
- Kungvarnchaikul, I.; Subbalekha, K.; Sindhavajiva, P.R.; Suwanwela, J. Deproteinized Bovine Bone and Freeze-Dried Bone Allograft in Sinus Floor Augmentation: A Randomized Controlled Trial. Clin. Implant Dent. Relat. Res. 2023, 25, 343–351. [Google Scholar] [CrossRef]
- Clark, D.; Rajendran, Y.; Paydar, S.; Ho, S.; Cox, D.; Ryder, M.; Dollard, J.; Kao, R.T. Advanced Platelet-Rich Fibrin and Freeze-Dried Bone Allograft for Ridge Preservation: A Randomized Controlled Clinical Trial. J. Periodontol. 2018, 89, 379–387. [Google Scholar] [CrossRef]
- Wei, L.; Miron, R.J.; Shi, B.; Zhang, Y. Osteoinductive and Osteopromotive Variability among Different Demineralized Bone Allografts. Clin. Implant Dent. Relat. Res. 2015, 17, 533–542. [Google Scholar] [CrossRef]
- Rosen, P.S.; Reynolds, M.A. A Retrospective Case Series Comparing the Use of Demineralized Freeze-Dried Bone Allograft and Freeze-Dried Bone Allograft Combined with Enamel Matrix Derivative for the Treatment of Advanced Osseous Lesions. J. Periodontol. 2002, 73, 942–949. [Google Scholar] [CrossRef]
- Miron, R.J. Optimized Bone Grafting. Periodontology 2000 2024, 94, 143–160. [Google Scholar] [CrossRef]
- Donos, N.; Dereka, X.; Calciolari, E. The Use of Bioactive Factors to Enhance Bone Regeneration: A Narrative Review. J. Clin. Periodontol. 2019, 46, 124–161. [Google Scholar] [CrossRef]
- Amid, R.; Kheiri, A.; Kheiri, L.; Kadkhodazadeh, M.; Ekhlasmandkermani, M. Structural and Chemical Features of Xenograft Bone Substitutes: A Systematic Review of In Vitro Studies. Biotechnol. Appl. Biochem. 2021, 68, 1432–1452. [Google Scholar] [CrossRef]
- Long, B.; Dan, L.; Jian, L.; Yunyu, H.; Shu, H.; Zhi, Y. Evaluation of a Novel Reconstituted Bone Xenograft Using Processed Bovine Cancellous Bone in Combination with Purified Bovine Bone Morphogenetic Protein. Xenotransplantation 2012, 19, 122–132. [Google Scholar] [CrossRef]
- Bracey, D.N.; Seyler, T.M.; Jinnah, A.H.; Lively, M.O.; Willey, J.S.; Smith, T.L.; Van Dyke, M.E.; Whitlock, P.W. A Decellularized Porcine Xenograft-Derived Bone Scaffold for Clinical Use as a Bone Graft Substitute: A Critical Evaluation of Processing and Structure. J. Funct. Biomater. 2018, 9, 45. [Google Scholar] [CrossRef]
- Bakhtiar, H.; Mazidi, A.; Mohammadi-Asl, S.; Hasannia, S.; Ellini, M.R.; Pezeshki-Modaress, M.; Ostad, S.N.; Galler, K.; Azarpazhooh, A.; Kishen, A. Potential of Treated Dentin Matrix Xenograft for Dentin-Pulp Tissue Engineering. J. Endod. 2020, 46, 57.e1–64.e1. [Google Scholar] [CrossRef]
- Glowacki, J. Demineralized Bone and BMPs: Basic Science and Clinical Utility. J. Oral Maxillofac. Surg. 2015, 73, S126–S131. [Google Scholar] [CrossRef] [PubMed]
- Badylak, S.F. Xenogeneic Extracellular Matrix as a Scaffold for Tissue Reconstruction. Transpl. Immunol. 2004, 12, 367–377. [Google Scholar] [CrossRef]
- Castillo-Dalí, G.; Velázquez-Cayón, R.; Angeles Serrera-Figallo, M.; Rodríguez-González-Elipe, A.; Gutierrez-Pérez, J.L.; Torres-Lagares, D. Importance of Poly(Lactic-Co-Glycolic Acid) in Scaffolds for Guided Bone Regeneration: A Focused Review. J. Oral Implantol. 2015, 41, e152–e157. [Google Scholar] [CrossRef] [PubMed]
- Benatti, A.C.B.; Pattaro, A.F.; Rodrigues, A.A.; Xavier, M.V.; Kaasi, A.; Barbosa, M.I.R.; Jardini, A.L.; Filho, R.M.; Kharmandayan, P. Chapter 4—Bioreabsorbable Polymers for Tissue Engineering: PLA, PGA, and Their Copolymers. In Materials for Biomedical Engineering; Holban, A.-M., Grumezescu, A.M., Eds.; Elsevier: Amsterdam, The Netherlands, 2019; pp. 83–116. ISBN 978-0-12-816901-8. [Google Scholar]
- Lewandrowski, K.-U.; Hile, D.D.; Thompson, B.M.J.; Wise, D.L.; Tomford, W.W.; Trantolo, D.J. Quantitative Measures of Osteoinductivity of a Porous Poly(Propylene Fumarate) Bone Graft Extender. Tissue Eng. 2003, 9, 85–93. [Google Scholar] [CrossRef]
- Tahriri, M.; Bader, R.; Yao, W.; Dehghani, S.; Khoshroo, K.; Rasoulianboroujeni, M.; Tayebi, L. Bioactive Glasses and Calcium Phosphates. In Biomaterials for Oral and Dental Tissue Engineering; Tayebi, L., Moharamzadeh, K.B.T., Eds.; Woodhead Publishing: Cambridge, UK, 2017; pp. 7–24. ISBN 978-0-08-100961-1. [Google Scholar]
- Shearer, A.; Montazerian, M.; Sly, J.J.; Hill, R.G.; Mauro, J.C. Trends and Perspectives on the Commercialization of Bioactive Glasses. Acta Biomater. 2023, 160, 14–31. [Google Scholar] [CrossRef]
- Zhou, W.; Shi, P.; Dong, J.; Li, S.; Lv, P.; Liu, C. Scaffolds of Bioactive Glass (Bioglass®) Combined with Recombinant Human Bone Morphogenetic Protein-9 (RhBMP-9) for Tooth Extraction Site Preservation. Heliyon 2022, 8, e08796. [Google Scholar] [CrossRef]
- Yan, A.; Mei, H.B.; Liu, K.; Wu, J.Y.; Tang, J.; Zhu, G.H.; Ye, W.H. Wrapping Grafting for Congenital Pseudarthrosis of the Tibia. Medicine 2017, 96, e8835. [Google Scholar] [CrossRef] [PubMed]
- Pastl, K.; Schimetta, W. The Application of an Allogeneic Bone Screw for Osteosynthesis in Hand and Foot Surgery: A Case Series. Arch. Orthop. Trauma Surg. 2022, 142, 2567–2575. [Google Scholar] [CrossRef]
- Ding, Y.; Wang, L.; Su, K.; Gao, J.; Li, X.; Cheng, G. Horizontal Bone Augmentation and Simultaneous Implant Placement Using Xenogeneic Bone Rings Technique: A Retrospective Clinical Study. Sci. Rep. 2021, 11, 4947. [Google Scholar] [CrossRef]
- Gruskin, E.; Doll, B.A.; Futrell, F.W.; Schmitz, J.P.; Hollinger, J.O. Demineralized Bone Matrix in Bone Repair: History and Use. Adv. Drug Deliv. Rev. 2012, 64, 1063–1077. [Google Scholar] [CrossRef]
- Ku, J.-K.; Jeong, Y.K.; Um, I.-W. Review of Allogeneic Dentin Graft for Maxillofacial Bone Defects. Tissue Eng. Part C Methods 2021, 27, 472–480. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Yang, L.; Li, J.; Zhang, Y.; Xu, W.; Ren, Y.; Liu, B.; Yang, B.; Li, B. GS/DBM/PLA Porous Composite Biomaterial for the Treatment of Infective Femoral Condyle Defect in Rats. Exp. Ther. Med. 2016, 11, 2107–2116. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wang, J.; Wang, J.; Niu, X.; Liu, J.; Gao, L.; Zhai, X.; Chu, K. Preparation of Porous PLA/DBM Composite Biomaterials and Experimental Research of Repair Rabbit Radius Segmental Bone Defect. Cell Tissue Bank. 2015, 16, 615–622. [Google Scholar] [CrossRef]
- Li, Q.; Zhang, W.; Zhou, G.; Cao, Y.; Liu, W.; Zhang, Z.Y. Demineralized Bone Matrix-Based Microcarrier Scaffold Favors Vascularized Large Bone Regeneration in Vivo in a Rat Model. J. Biomater. Appl. 2018, 33, 182–195. [Google Scholar] [CrossRef]
- Ponzetti, M.; Rucci, N. Osteoblast Differentiation and Signaling: Established Concepts and Emerging Topics. Int. J. Mol. Sci. 2021, 22, 6651. [Google Scholar] [CrossRef]
- Ravindran, S.; Huang, C.C.; Gajendrareddy, P.; Narayanan, R. Biomimetically Enhanced Demineralized Bone Matrix for Bone Regenerative Applications. Front. Physiol. 2015, 6, 292. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J.; Kim, J.H.; Shim, J.H.; Hwang, N.S.; Heo, C.Y. Bioactive Calcium Phosphate Materials and Applications in Bone Regeneration. Biomater. Res. 2025, 23, 4. [Google Scholar] [CrossRef] [PubMed]
- Dorozhkin, S.V. Biphasic, Triphasic and Multiphasic Calcium Orthophosphates. Acta Biomater. 2012, 8, 963–977. [Google Scholar] [CrossRef]
- Zhu, Q.; Ablikim, Z.; Chen, T.; Cai, Q.; Xia, J.; Jiang, D.; Wang, S. The Preparation and Characterization of HA/β-TCP Biphasic Ceramics from Fish Bones. Ceram. Int. 2017, 43, 12213–12220. [Google Scholar] [CrossRef]
- Arcos, D. Calcium Phosphate Bioceramics. In Bio-Ceramics with Clinical Applications; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2014; pp. 23–71. ISBN 9781118406748. [Google Scholar]
- Dorozhkin, S.V. Calcium Orthophosphate-Based Bioceramics. Materials 2013, 6, 3840–3942. [Google Scholar] [CrossRef]
- Sheikh, Z.; Abdallah, M.N.; Hanafi, A.A.; Misbahuddin, S.; Rashid, H.; Glogauer, M. Mechanisms of in Vivo Degradation and Resorption of Calcium Phosphate Based Biomaterials. Materials 2015, 8, 7913–7925. [Google Scholar] [CrossRef] [PubMed]
- Shavandi, A.; Bekhit, A.E.D.A.; Ali, M.A.; Sun, Z.; Gould, M. Development and Characterization of Hydroxyapatite/β-TCP/Chitosan Composites for Tissue Engineering Applications. Mater. Sci. Eng. C 2015, 56, 481–493. [Google Scholar] [CrossRef]
- Helaehil, J.V.; Lourenço, C.B.; Huang, B.; Helaehil, L.V.; de Camargo, I.X.; Chiarotto, G.B.; Santamaria, M., Jr.; Bártolo, P.; Caetano, G.F. In Vivo Investigation of Polymer-Ceramic Pcl/Ha and Pcl/β-Tcp 3d Composite Scaffolds and Electrical Stimulation for Bone Regeneration. Polymers 2022, 14, 65. [Google Scholar] [CrossRef] [PubMed]
- Ventura, R.D.; Padalhin, A.R.; Kim, B.; Park, M.K.; Lee, B.T. Evaluation of Bone Regeneration Potential of Injectable Extracellular Matrix (ECM) from Porcine Dermis Loaded with Biphasic Calcium Phosphate (BCP) Powder. Mater. Sci. Eng. C 2020, 110, 110663. [Google Scholar] [CrossRef]
- Bendtsen, S.T.; Wei, M. Synthesis and Characterization of a Novel Injectable Alginate–Collagen–Hydroxyapatite Hydrogel for Bone Tissue Regeneration. J. Mater. Chem. B 2015, 3, 3081–3090. [Google Scholar] [CrossRef]
- Moeinzadeh, S.; Park, Y.; Lin, S.; Yang, Y.P. In-Situ Stable Injectable Collagen-Based Hydrogels for Cell and Growth Factor Delivery. Materialia 2021, 15, 100954. [Google Scholar] [CrossRef] [PubMed]
- Vallet-Regí, M.; Salinas, A.J. Ceramics as Bone Repair Materials, 2nd ed.; Elsevier: Amsterdam, The Netherlands, 2018; ISBN 9780081024515. [Google Scholar]
- Sun, J.; Ye, D.; Zou, J.; Chen, X.; Wang, Y.; Yuan, J.; Liang, H.; Qu, H.; Binner, J.; Bai, J. A Review on Additive Manufacturing of Ceramic Matrix Composites. J. Mater. Sci. Technol. 2023, 138, 1–16. [Google Scholar] [CrossRef]
- Ikumapayi, O.M.; Ogedengbe, T.S.; Ogundipe, A.T.; Nnochiri, E.S.; Obende, B.A.; Afolalu, S.A. Ceramics Matrix Composites for Biomedical Applications—A Review. Mater. Today Proc. 2023. [Google Scholar] [CrossRef]
- Bangash, M.K.; Collins, M.N. Ceramic Materials BT—Engineering Materials: Fundamentals, Processing and Properties; Shaker, K., Nawab, Y., Eds.; Springer Nature: Cham, Switzerland, 2025; pp. 79–106. ISBN 978-3-031-72263-9. [Google Scholar]
- Bose, S.; Sarkar, N.; Vahabzadeh, S.; Ke, D.; Bandyopadhyay, A. Additive Manufacturing of Ceramics. In Additive Manufacturing, 2nd ed.; CRC Press: Boca Raton, FL, USA, 2019; pp. 183–231. [Google Scholar]
- Han, J.; Göksel, B.; Mohajernia, S.; Killian, M.S.; Vleugels, J.; Braem, A.; Castagne, S. Ultrashort Pulsed Laser Ablation of Zirconia Toughened Alumina: Material Removal Mechanism and Surface Characteristics. Appl. Surf. Sci. 2023, 615, 156407. [Google Scholar] [CrossRef]
- Whenish, R.; Velu, R.; Anand Kumar, S.; Ramprasath, L.S. Additive Manufacturing Technologies for Biomedical Implants Using Functional Biocomposites. In High-Performance Composite Structures: Additive Manufacturing and Processing; Springer: Berlin/Heidelberg, Germany, 2021; pp. 25–44. [Google Scholar]
- Malinverni, C.; Salvo, M.; De Zanet, A.; D’Isanto, F.; Smeacetto, F.; Bertrand, P.; Puchas, G.; Schafföner, S.; Casalegno, V. Glass-Ceramics for Joining Oxide-Based Ceramic Matrix Composites (Al2O3f/Al2O3-ZrO2) Operating under Direct Flame Exposure. J. Eur. Ceram. Soc. 2023, 43, 3621–3629. [Google Scholar] [CrossRef]
- Rout, S.; Panigrahi, D.; Patel, S.K. Effect of Machining Environments on the Crack Behavior of ZrO2-Al2O3 Composite during Short-Pulsed Laser Processing. Compos. Commun. 2024, 52, 102119. [Google Scholar] [CrossRef]
- Chai, Y.C.; Carlier, A.; Bolander, J.; Roberts, S.J.; Geris, L.; Schrooten, J.; Van Oosterwyck, H.; Luyten, F.P. Current Views on Calcium Phosphate Osteogenicity and the Translation into Effective Bone Regeneration Strategies. Acta Biomater. 2012, 8, 3876–3887. [Google Scholar] [CrossRef] [PubMed]
- Safari, B.; Davaran, S.; Aghanejad, A. Osteogenic Potential of the Growth Factors and Bioactive Molecules in Bone Regeneration. Int. J. Biol. Macromol. 2021, 175, 544–557. [Google Scholar] [CrossRef] [PubMed]
- Shen, H.; Zhuang, Y.; Zhang, C.; Zhang, C.; Yuan, Y.; Yu, H.; Si, J.; Shen, G. Osteoclast-Driven Osteogenesis, Bone Remodeling and Biomaterial Resorption: A New Profile of BMP2-CPC-Induced Alveolar Bone Regeneration. Int. J. Mol. Sci. 2022, 23, 12204. [Google Scholar] [CrossRef]
- Borkowski, L.; Jojczuk, M.; Belcarz, A.; Pawlowska-Olszewska, M.; Kruk-Bachonko, J.; Radzki, R.; Bienko, M.; Slowik, T.; Lübek, T.; Nogalski, A.; et al. Comparing the Healing Abilities of Fluorapatite and Hydroxyapatite Ceramics in Regenerating Bone Tissue: An In Vivo Study. Materials 2023, 16, 5992. [Google Scholar] [CrossRef] [PubMed]
- Mondal, S.; Pal, U.; Dey, A. Natural Origin Hydroxyapatite Scaffold as Potential Bone Tissue Engineering Substitute. Ceram. Int. 2016, 42, 18338–18346. [Google Scholar] [CrossRef]
- Lu, J.; Descamps, M.; Dejou, J.; Koubi, G.; Hardouin, P.; Lemaitre, J.; Proust, J.-P. The Biodegradation Mechanism of Calcium Phosphate Biomaterials in Bone. J. Biomed. Mater. Res. 2002, 63, 408–412. [Google Scholar] [CrossRef]
- Ballouze, R.; Marahat, M.H.; Mohamad, S.; Saidin, N.A.; Kasim, S.R.; Ooi, J.P. Biocompatible Magnesium-Doped Biphasic Calcium Phosphate for Bone Regeneration. J. Biomed. Mater. Res. Part B Appl. Biomater. 2021, 109, 1426–1435. [Google Scholar] [CrossRef]
- Kolmas, J.; Romaniuk, P.; Predoi, D.; Drobniewska, A.; Burdan, K.; Kołodziejska, B. Magnesium Ion Substitution in Various Calcium Phosphates: A Way towards Bone Regeneration. Ceram. Int. 2025, 51, 1153–1160. [Google Scholar] [CrossRef]
- Putri, T.S.; Hayashi, K.; Ishikawa, K. Bone Regeneration Using β-Tricalcium Phosphate (β-TCP) Block with Interconnected Pores Made by Setting Reaction of β-TCP Granules. J. Biomed. Mater. Res. Part A 2020, 108, 625–632. [Google Scholar] [CrossRef]
- Wiltfang, J.; Merten, H.A.; Schlegel, K.A.; Schultze-Mosgau, S.; Kloss, F.R.; Rupprecht, S.; Kessler, P. Degradation Characteristics of α and β Tri-Calcium-Phosphate (TCP) in Minipigs. J. Biomed. Mater. Res. 2002, 63, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Bohner, M.; Santoni, B.L.G.; Döbelin, N. β-Tricalcium Phosphate for Bone Substitution: Synthesis and Properties. Acta Biomater. 2020, 113, 23–41. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Zhou, Y.; Lei, Q.; Lin, D.; Chen, J.; Wu, C. Effect of Inorganic Phosphate on Migration and Osteogenic Differentiation of Bone Marrow Mesenchymal Stem Cells. BMC Dev. Biol. 2021, 21, 1. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.K.; Lu, Q.Z.; Pei, R.; Ji, H.J.; Zhou, G.S.; Zhao, X.L.; Tang, R.K.; Zhang, M. The Effect of Extracellular Calcium and Inorganic Phosphate on the Growth and Osteogenic Differentiation of Mesenchymal Stem Cells in Vitro: Implication for Bone Tissue Engineering. Biomed. Mater. 2009, 4, 25004. [Google Scholar] [CrossRef]
- Shih, Y.R.V.; Hwang, Y.; Phadke, A.; Kang, H.; Hwang, N.S.; Caro, E.J.; Nguyen, S.; Siu, M.; Theodorakis, E.A.; Gianneschi, N.C.; et al. Calcium Phosphate-Bearing Matrices Induce Osteogenic Differentiation of Stem Cells through Adenosine Signaling. Proc. Natl. Acad. Sci. USA 2014, 111, 990–995. [Google Scholar] [CrossRef]
- Tanvir, M.A.H.; Khaleque, M.A.; Kim, G.H.; Yoo, W.Y.; Kim, Y.Y. The Role of Bioceramics for Bone Regeneration: History, Mechanisms, and Future Perspectives. Biomimetics 2024, 9, 230. [Google Scholar] [CrossRef]
- Vallet-Regí, M.; Victoria Ragel, C.; Salinas, A.J. Glasses with Medical Applications. Eur. J. Inorg. Chem. 2003, 2003, 1029–1042. [Google Scholar] [CrossRef]
- Hench, L.L.; Polak, J.M. Third-Generation Biomedical Materials. Science 2002, 295, 1014–1017. [Google Scholar] [CrossRef]
- Vallet-Regí, M.; Ruiz-Hernández, E. Bioceramics: From Bone Regeneration to Cancer Nanomedicine. Adv. Mater. 2011, 23, 5177–5218. [Google Scholar] [CrossRef]
- Dziadek, M.; Stodolak-Zych, E.; Cholewa-Kowalska, K. Biodegradable Ceramic-Polymer Composites for Biomedical Applications: A Review. Mater. Sci. Eng. C 2017, 71, 1175–1191. [Google Scholar] [CrossRef]
- Šupová, M. Substituted Hydroxyapatites for Biomedical Applications: A Review. Ceram. Int. 2015, 41, 9203–9231. [Google Scholar] [CrossRef]
- Kalita, S.J.; Bhatt, H.A. Nanocrystalline Hydroxyapatite Doped with Magnesium and Zinc: Synthesis and Characterization. Mater. Sci. Eng. C 2007, 27, 837–848. [Google Scholar] [CrossRef]
- Heness, G.; Ben-Nissan, B. Innovative Bioceramics. Mater. Forum 2007, 27, 104–114. [Google Scholar]
- Heimann, R.B. Structure, Properties, and Biomedical Performance of Osteoconductive Bioceramic Coatings. Surf. Coat. Technol. 2013, 233, 27–38. [Google Scholar] [CrossRef]
- Olofsson, J.; Pettersson, M.; Teuscher, N.; Heilmann, A.; Larsson, K.; Grandfield, K.; Persson, C.; Jacobson, S.; Engqvist, H. Fabrication and Evaluation of SixNy Coatings for Total Joint Replacements. J. Mater. Sci. Mater. Med. 2012, 23, 1879–1889. [Google Scholar] [CrossRef]
- Cao, W.; Hench, L.L. Bioactive Materials. Ceram. Int. 1996, 22, 493–507. [Google Scholar] [CrossRef]
- Hench, L.L. Bioceramics: From Concept to Clinic. J. Am. Ceram. Soc. 1991, 74, 1487–1510. [Google Scholar] [CrossRef]
- Hutmacher, D.W.; Schantz, J.T.; Lam, C.X.F.; Tan, K.C.; Lim, T.C. State of the Art and Future Directions of Scaffold-Based Bone Engineering from a Biomaterials Perspective. J. Tissue Eng. Regen. Med. 2007, 1, 245–260. [Google Scholar] [CrossRef]
- LeGeros, R.Z. Calcium Phosphate-Based Osteoinductive Materials. Chem. Rev. 2008, 108, 4742–4753. [Google Scholar] [CrossRef]
- Surmenev, R.A.; Surmeneva, M.A.; Ivanova, A.A. Significance of Calcium Phosphate Coatings for the Enhancement of New Bone Osteogenesis—A Review. Acta Biomater. 2014, 10, 557–579. [Google Scholar]
- Ortega, B.; Gardner, C.; Roberts, S.; Chung, A.; Wang, J.C.; Buser, Z. Ceramic Biologics for Bony Fusion—A Journey from First to Third Generations. Curr. Rev. Musculoskelet. Med. 2020, 13, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Kargozar, S.; Milan, P.B.; Amoupour, M.; Kermani, F.; Gorgani, S.; Nazarnezhad, S.; Hooshmand, S.; Baino, F. Osteogenic Potential of Magnesium (Mg)—Doped Multicomponent Bioactive Glass: In Vitro and In Vivo Animal Studies. Materials 2022, 15, 318. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.; Wu, X.; Dong, Y.; Shao, R.; Chen, X.; Zhou, P.; Xu, F. In Vivo Behavior of Bioactive Glass-Based Composites in Animal Models for Bone Regeneration. Biomater. Sci. 2021, 9, 1924–1944. [Google Scholar] [CrossRef]
- Li, F.; Chen, X.; Liu, P. A Review on Three-Dimensional Printed Silicate-Based Bioactive Glass/Biodegradable Medical Synthetic Polymer Composite Scaffolds. Tissue Eng. Part B Rev. 2023, 29, 244–259. [Google Scholar] [CrossRef]
- Aldhaher, A.; Shahabipour, F.; Shaito, A.; Al-Assaf, S.; Elnour, A.A.M.; Sallam, E.B.; Teimourtash, S.; Elfadil, A.A. 3D Hydrogel/Bioactive Glass Scaffolds in Bone Tissue Engineering: Status and Future Opportunities. Heliyon 2023, 9, e17050. [Google Scholar] [CrossRef]
- Giannotti, L.; Di Chiara Stanca, B.; Nitti, P.; Spedicato, F.; Damiano, F.; Demitri, C.; Calabriso, N.; Carluccio, M.A.; Palermo, A.; Ferrante, F.; et al. Hydroxyapatite–Silicon Scaffold Promotes Osteogenic Differentiation of CGF Primary Cells. Biology 2023, 12, 528. [Google Scholar] [CrossRef]
- Du, M.; Chen, J.; Liu, K.; Xing, H.; Song, C. Recent Advances in Biomedical Engineering of Nano-Hydroxyapatite Including Dentistry, Cancer Treatment and Bone Repair. Compos. Part B Eng. 2021, 215, 108790. [Google Scholar] [CrossRef]
- Al-Harbi, N.; Mohammed, H.; Al-Hadeethi, Y.; Bakry, A.S.; Umar, A.; Hussein, M.A.; Abbassy, M.A.; Vaidya, K.G.; Al Berakdar, G.; Mkawi, E.M.; et al. Silica-Based Bioactive Glasses and Their Applications in Hard Tissue Regeneration: A Review. Pharmaceuticals 2021, 14, 75. [Google Scholar] [CrossRef]
- Tulyaganov, D.U.; Fiume, E.; Akbarov, A.; Ziyadullaeva, N.; Murtazaev, S.; Rahdar, A.; Massera, J.; Verné, E.; Baino, F. In Vivo Evaluation of 3D-Printed Silica-Based Bioactive Glass Scaffolds for Bone Regeneration. J. Funct. Biomater. 2022, 13, 74. [Google Scholar] [CrossRef]
- Krishnan, L.; Chakrabarty, P.; Govarthanan, K.; Rao, S.; Santra, T.S. Bioglass and Nano Bioglass: A next-Generation Biomaterial for Therapeutic and Regenerative Medicine Applications. Int. J. Biol. Macromol. 2024, 277, 133073. [Google Scholar] [CrossRef]
- Zhao, F.; Yang, Z.; Liu, L.; Chen, D.; Shao, L.; Chen, X. Design and Evaluation of a Novel Sub-Scaffold Dental Implant System Based on the Osteoinduction of Micro-Nano Bioactive Glass. Biomater. Transl. 2020, 1, 82–88. [Google Scholar] [CrossRef] [PubMed]
- El-Fiqi, A. Nano-Bioactive Glass: Advances and Applications. In Bioactive Glasses and Glass-Ceramics; Wiley Online Library: Hoboken, NJ, USA, 2022; pp. 173–201. ISBN 9781119724193. [Google Scholar]
- Ramírez Rodríguez, G.B.; Patrício, T.M.F.; Delgado López, J.M. Natural Polymers for Bone Repair. In Woodhead Publishing Series in Biomaterials, 2nd ed.; Pawelec, K.M., Planell, J.A.B.T., Eds.; Woodhead Publishing: Cambridge, UK, 2019; pp. 199–232. ISBN 978-0-08-102451-5. [Google Scholar]
- Kudiyarasu, S.; Karuppan Perumal, M.K.; Rajan Renuka, R.; Manickam Natrajan, P. Chitosan Composite with Mesenchymal Stem Cells: Properties, Mechanism, and Its Application in Bone Regeneration. Int. J. Biol. Macromol. 2024, 275, 133502. [Google Scholar] [CrossRef] [PubMed]
- Duminis, T. Natural Polymers with Bioactive Glass Additives for Bone Regeneration: Chemistry and Trends. Nat. Prod. J. 2024, 14, 51–67. [Google Scholar] [CrossRef]
- Sreena, R.; Raman, G.; Manivasagam, G.; Nathanael, A.J. Bioactive Glass–Polymer Nanocomposites: A Comprehensive Review on Unveiling Their Biomedical Applications. J. Mater. Chem. B 2024, 12, 11278–11301. [Google Scholar] [CrossRef]
- Venkatesan, J.; Nithya, R.; Sudha, P.N.; Kim, S.-K. Chapter Four—Role of Alginate in Bone Tissue Engineering. In Marine Carbohydrates: Fundamentals and Applications, Part B; Kim, S., Ed.; Academic Press: Cambridge, MA, USA, 2014; Volume 73, pp. 45–57. ISBN 1043-4526. [Google Scholar]
- Shanmugavadivu, A.; Lavanya, K.; Selvamurugan, N. Chapter 13—Nanomaterials in Bone Tissue Engineering. In Micro and Nano Technologies; Malik, M.I., Hussain, D., Shah, M.R., Guo, D., Eds.; Elsevier: Amsterdam, The Netherlands, 2024; pp. 321–357. ISBN 978-0-323-95513-3. [Google Scholar]
- Wu, C.; Zhu, Y.; Chang, J.; Zhang, Y.; Xiao, Y. Bioactive Inorganic-Materials/Alginate Composite Microspheres with Controllable Drug-Delivery Ability. J. Biomed. Mater. Res. Part B Appl. Biomater. 2010, 94B, 32–43. [Google Scholar] [CrossRef]
- Wu, J.; Xue, K.; Li, H.; Sun, J.; Liu, K. Improvement of PHBV Scaffolds with Bioglass for Cartilage Tissue Engineering. PLoS ONE 2013, 8, e71563. [Google Scholar] [CrossRef]
- Li, X.; Shi, J.; Dong, X.; Zhang, L.; Zeng, H. A Mesoporous Bioactive Glass/Polycaprolactone Composite Scaffold and Its Bioactivity Behavior. J. Biomed. Mater. Res. Part A 2008, 84A, 84–91. [Google Scholar] [CrossRef]
- Niu, Y.; Guo, L.; Liu, J.; Shen, H.; Su, J.; An, X.; Yu, B.; Wei, J.; Shin, J.-W.; Guo, H.; et al. Bioactive and Degradable Scaffolds of the Mesoporous Bioglass and Poly(l-Lactide) Composite for Bone Tissue Regeneration. J. Mater. Chem. B 2015, 3, 2962–2970. [Google Scholar] [CrossRef]
- Keshaw, H.; Georgiou, G.; Blaker, J.J.; Forbes, A.; Knowles, J.C.; Day, R.M. Assessment of Polymer/Bioactive Glass-Composite Microporous Spheres for Tissue Regeneration Applications. Tissue Eng. Part A 2008, 15, 1451–1461. [Google Scholar] [CrossRef]
- Girón, J.; Kerstner, E.; Medeiros, T.; Oliveira, L.; Machado, G.M.; Malfatti, C.F.; Pranke, P. Biomaterials for Bone Regeneration: An Orthopedic and Dentistry Overview. Braz. J. Med. Biol. Res. 2021, 54, e11055. [Google Scholar] [CrossRef]
- Khodaverdi, K.; Naghib, S.M.; Mozafari, M.R. Chitosan/Bioglass Nanocomposites for Bone Tissue Engineering and Regenerative Medicine: An Overview of Promising Biomaterials. Curr. Org. Chem. 2024, 28, 1437–1451. [Google Scholar] [CrossRef]
- Roppolo, I.; Chiappone, A.; Chiadò, A.; Palmara, G.; Frascella, F. Biomedical Applications. In High Resolution Manufacturing from 2D to 3D/4D Printing: Applications in Engineering and Medicine; Springer: Berlin/Heidelberg, Germany, 2022; pp. 155–189. [Google Scholar] [CrossRef]
- Kumari, S.; Singh, D.; Srivastava, P.; Singh, B.N.; Mishra, A. Generation of Graphene Oxide and Nano-Bioglass Based Scaffold for Bone Tissue Regeneration. Biomed. Mater. 2022, 17, 65012. [Google Scholar] [CrossRef] [PubMed]
- Szymański, T.; Semba, J.A.; Mieloch, A.A.; Cywoniuk, P.; Kempa, M.; Rybka, J.D. Hyaluronic Acid and Multiwalled Carbon Nanotubes as Bioink Additives for Cartilage Tissue Engineering. Sci. Rep. 2023, 13, 646. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Muduli, C.; Senanayak, S.P.; Goswami, L. Graphite Nanopowder Incorporated Xanthan Gum Scaffold for Effective Bone Tissue Regeneration Purposes with Improved Biomineralization. Int. J. Biol. Macromol. 2023, 234, 123724. [Google Scholar] [CrossRef]
- Silva-Barroso, A.S.; Cabral, C.S.D.; Ferreira, P.; Moreira, A.F.; Correia, I.J. Lignin-Enriched Tricalcium Phosphate/Sodium Alginate 3D Scaffolds for Application in Bone Tissue Regeneration. Int. J. Biol. Macromol. 2023, 239, 124258. [Google Scholar] [CrossRef]
- Seyyed Nasrollah, S.A.; Karimi-Soflou, R.; Karkhaneh, A. Photo-Click Crosslinked Hydrogel Containing MgO2-Loaded PLGA Microsphere with Concurrent Magnesium and Oxygen Release for Bone Tissue Engineering. Mater. Today Chem. 2023, 28, 101389. [Google Scholar] [CrossRef]
- Yu, H.-S.; Jang, J.-H.; Kim, T.-I.; Lee, H.-H.; Kim, H.-W. Apatite-Mineralized Polycaprolactone Nanofibrous Web as a Bone Tissue Regeneration Substrate. J. Biomed. Mater. Res. Part A 2009, 88A, 747–754. [Google Scholar] [CrossRef]
- Ni, P.; Ding, Q.; Fan, M.; Liao, J.; Qian, Z.; Luo, J.; Li, X.; Luo, F.; Yang, Z.; Wei, Y. Injectable Thermosensitive PEG–PCL–PEG Hydrogel/Acellular Bone Matrix Composite for Bone Regeneration in Cranial Defects. Biomaterials 2014, 35, 236–248. [Google Scholar] [CrossRef]
- Chandra, S. Natural and Synthetic Polymers. In Polymers in Concrete; CRC Press: Boca Raton, FL, USA, 2020; pp. 5–25. [Google Scholar] [CrossRef]
- Alonso-Fernández, I.; Haugen, H.J.; López-Peña, M.; González-Cantalapiedra, A.; Muñoz, F. Use of 3D-Printed Polylactic Acid/Bioceramic Composite Scaffolds for Bone Tissue Engineering in Preclinical in Vivo Studies: A Systematic Review. Acta Biomater. 2023, 168, 1–21. [Google Scholar] [CrossRef]
- Rao, S.H.; Harini, B.; Shadamarshan, R.P.K.; Balagangadharan, K.; Selvamurugan, N. Natural and Synthetic Polymers/Bioceramics/Bioactive Compounds-Mediated Cell Signalling in Bone Tissue Engineering. Int. J. Biol. Macromol. 2018, 110, 88–96. [Google Scholar] [CrossRef]
- Fraile-Martínez, O.; García-Montero, C.; Coca, A.; Álvarez-Mon, M.A.; Monserrat, J.; Gómez-Lahoz, A.M.; Coca, S.; Álvarez-Mon, M.; Acero, J.; Bujan, J.; et al. Applications of Polymeric Composites in Bone Tissue Engineering and Jawbone Regeneration. Polymers 2021, 13, 3429. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Han, D.; Dong, J.-S.; Shen, G.-X.; Chai, G.; Yu, Z.-Y.; Lang, W.-J.; Ai, S.-T. Rapid Prototyped PGA/PLA Scaffolds in the Reconstruction of Mandibular Condyle Bone Defects. Int. J. Med. Robot. Comput. Assist. Surg. 2010, 6, 66–72. [Google Scholar] [CrossRef]
- Ma, C.; Ma, Z.; Yang, F.; Wang, J.; Liu, C. Poly (Propylene Fumarate)/β-Calcium Phosphate Composites for Enhanced Bone Repair. Biomed. Mater. 2019, 14, 045002. [Google Scholar] [CrossRef] [PubMed]
- Hasirci, V.; Litman, A.E.; Trantolo, D.J.; Gresser, J.D.; Wise, D.L.; Margolis, H.C. PLGA Bone Plates Reinforced with Crosslinked PPF. J. Mater. Sci. Mater. Med. 2002, 13, 159–167. [Google Scholar] [CrossRef]
- Xu, H.; Liao, H.; Liu, X.; Miller, A.L.; Elder, B.D.; Lu, L. Spinal Fusion of Biodegradable Poly(Propylene Fumarate) and Poly(Propylene Fumarate-Co-Caprolactone) Copolymers in Rabbits. J. Orthop. 2024, 48, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Wagner, E.R.; Parry, J.; Dadsetan, M.; Bravo, D.; Riester, S.M.; Van Wijnen, A.J.; Yaszemski, M.J.; Kakar, S. VEGF-Mediated Angiogenesis and Vascularization of a Fumarate-Crosslinked Polycaprolactone (PCLF) Scaffold. Connect. Tissue Res. 2018, 59, 542–549. [Google Scholar] [CrossRef]
- Filippi, M.; Born, G.; Chaaban, M.; Scherberich, A. Natural Polymeric Scaffolds in Bone Regeneration. Front. Bioeng. Biotechnol. 2020, 8, 474. [Google Scholar] [CrossRef]
- Aoki, K.; Saito, N. Biodegradable Polymers as Drug Delivery Systems for Bone Regeneration. Pharmaceutics 2020, 12, 95. [Google Scholar] [CrossRef]
- Hasnain, M.S.; Ahmad, S.A.; Chaudhary, N.; Hoda, M.N.; Nayak, A.K. Biodegradable Polymer Matrix Nanocomposites for Bone Tissue Engineering; Elsevier Inc.: Amsterdam, The Netherlands, 2018; ISBN 9780128137574. [Google Scholar]
- Idumah, C.I. Progress in Polymer Nanocomposites for Bone Regeneration and Engineering. Polym. Polym. Compos. 2021, 29, 509–527. [Google Scholar] [CrossRef]
- Bharadwaz, A.; Jayasuriya, A.C. Recent Trends in the Application of Widely Used Natural and Synthetic Polymer Nanocomposites in Bone Tissue Regeneration. Mater. Sci. Eng. C 2020, 110, 110698. [Google Scholar] [CrossRef]
- Vahidi, M.; Rizkalla, A.S.; Mequanint, K. Extracellular Matrix-Surrogate Advanced Functional Composite Biomaterials for Tissue Repair and Regeneration. Adv. Healthc. Mater. 2024, 13, 2401218. [Google Scholar] [CrossRef] [PubMed]
- Fattahi, R.; Mohebichamkhorami, F.; Taghipour, N.; Keshel, S.H. The Effect of Extracellular Matrix Remodeling on Material-Based Strategies for Bone Regeneration: Review Article. Tissue Cell 2022, 76, 101748. [Google Scholar] [CrossRef]
- Abbas, M.; Alqahtani, M.S.; Alhifzi, R. Recent Developments in Polymer Nanocomposites for Bone Regeneration. Int. J. Mol. Sci. 2023, 24, 3312. [Google Scholar] [CrossRef]
- Xiao, D.; Zhang, J.; Zhang, C.; Barbieri, D.; Yuan, H.; Moroni, L.; Feng, G. The Role of Calcium Phosphate Surface Structure in Osteogenesis and the Mechanisms Involved. Acta Biomater. 2020, 106, 22–33. [Google Scholar] [CrossRef] [PubMed]
- Sagadevan, S.; Schirhagl, R.; Rahman, M.Z.; Bin Ismail, M.F.; Lett, J.A.; Fatimah, I.; Mohd Kaus, N.H.; Oh, W.-C. Recent Advancements in Polymer Matrix Nanocomposites for Bone Tissue Engineering Applications. J. Drug Deliv. Sci. Technol. 2023, 82, 104313. [Google Scholar] [CrossRef]
- Rogel, M.R.; Qiu, H.; Ameer, G.A. The Role of Nanocomposites in Bone Regeneration. J. Mater. Chem. 2008, 18, 4233–4241. [Google Scholar] [CrossRef]
- Sahoo, N.G.; Pan, Y.Z.; Li, L.; He, C. Bin Nanocomposites for Bone Tissue Regeneration. Nanomedicine 2013, 8, 639–653. [Google Scholar] [CrossRef] [PubMed]
- Sadeghzadeh, H.; Dianat-Moghadam, H.; Del Bakhshayesh, A.R.; Mohammadnejad, D.; Mehdipour, A. A Review on the Effect of Nanocomposite Scaffolds Reinforced with Magnetic Nanoparticles in Osteogenesis and Healing of Bone Injuries. Stem Cell Res. Ther. 2023, 14, 194. [Google Scholar] [CrossRef]
- Madhav, H.; Singh, N.; Jaiswar, G. Chapter 4—Thermoset, Bioactive, Metal–Polymer Composites for Medical Applications; Grumezescu, V., Grumezescu, A.M.B.T., Eds.; Elsevier: Amsterdam, The Netherlands, 2019; pp. 105–143. ISBN 978-0-12-816874-5. [Google Scholar]
- Abdulmajeed, A.A.; Walboomers, X.F.; Massera, J.; Kokkari, A.K.; Vallittu, P.K.; Närhi, T.O. Blood and Fibroblast Responses to Thermoset BisGMA–TEGDMA/Glass Fiber-Reinforced Composite Implants In Vitro. Clin. Oral Implant. Res. 2014, 25, 843–851. [Google Scholar] [CrossRef]
- Petersen, R. Titanium Implant Osseointegration Problems with Alternate Solutions Using Epoxy/Carbon-Fiber-Reinforced Composite. Metals 2014, 4, 549–569. [Google Scholar] [CrossRef]
- Baican, M.; Stoleru, E.; Vasile, C. Chapter 13—Cellular Response to Synthetic Polymers. In Woodhead Publishing Series in Biomaterials; Mozafari, M.B.T., Ed.; Woodhead Publishing: Cambridge, UK, 2020; pp. 269–319. ISBN 978-0-08-102967-1. [Google Scholar]
- Rohani Shirvan, A.; Nouri, A.; Wen, C. Structural Polymer Biomaterials. In Woodhead Publishing Series in Biomaterials; Wen, C.B.T., Ed.; Woodhead Publishing: Cambridge, UK, 2021; pp. 395–439. ISBN 978-0-12-818831-6. [Google Scholar]
- Ghosh, S.; Mostafavi, E. Functionalized Carbon Nanotubes for Artificial Bone Tissue Engineering. In Functionalized Carbon Nanotubes for Biomedical Applications; Wiley: Hoboken, NJ, USA, 2023; pp. 225–256. ISBN 9781119905080. [Google Scholar]
- Bozorgi, A.; Khazaei, M.; Soleimani, M.; Jamalpoor, Z. Application of Nanoparticles in Bone Tissue Engineering; a Review on the Molecular Mechanisms Driving Osteogenesis. Biomater. Sci. 2021, 9, 4541–4567. [Google Scholar] [CrossRef] [PubMed]
- Tariq, A.; Bhawani, S.A.; Alotaibi, K.M. Xanthan Gum-Based Nanocomposites for Tissue Engineering. In Woodhead Publishing Series in Biomaterials; Bhawani, S.A., Karim, Z., Jawaid, M.B.T., Eds.; Woodhead Publishing: Cambridge, UK, 2021; pp. 191–206. ISBN 978-0-12-821230-1. [Google Scholar]
- Mohammadinejad, R.; Kumar, A.; Ranjbar-Mohammadi, M.; Ashrafizadeh, M.; Han, S.S.; Khang, G.; Roveimiab, Z. Recent Advances in Natural Gum-Based Biomaterials for Tissue Engineering and Regenerative Medicine: A Review. Polymers 2020, 12, 176. [Google Scholar] [CrossRef] [PubMed]
- Su, C.; Chen, Y.; Tian, S.; Lu, C.; Lv, Q. Research Progress on Emerging Polysaccharide Materials Applied in Tissue Engineering. Polymers 2022, 14, 3268. [Google Scholar] [CrossRef] [PubMed]
- Jose, M.V.; Thomas, V.; Johnson, K.T.; Dean, D.R.; Nyairo, E. Aligned PLGA/HA Nanofibrous Nanocomposite Scaffolds for Bone Tissue Engineering. Acta Biomater. 2009, 5, 305–315. [Google Scholar] [CrossRef]
- Zhao, X.; Han, Y.; Li, J.; Cai, B.; Gao, H.; Feng, W.; Li, S.; Liu, J.; Li, D. BMP-2 Immobilized PLGA/Hydroxyapatite Fibrous Scaffold via Polydopamine Stimulates Osteoblast Growth. Mater. Sci. Eng. C 2017, 78, 658–666. [Google Scholar] [CrossRef]
- Ma, D.; An, G.; Liang, M.; Liu, Y.; Zhang, B.; Wang, Y. A Composited PEG-Silk Hydrogel Combining with Polymeric Particles Delivering RhBMP-2 for Bone Regeneration. Mater. Sci. Eng. C 2016, 65, 221–231. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, R.; Wu, W.; Qing, Y.; Tang, X.; Ye, W.; Zhang, Z.; Qin, Y. Adhesion and Proliferation of Osteoblast-Like Cells on Porous Polyetherimide Scaffolds. Biomed Res. Int. 2018, 2018, 1491028. [Google Scholar] [CrossRef]
- Xu, X.; Wang, H.; Zhang, S.; Mei, X.; Ying, B.; Li, R.; Qin, Y. ECM-Inspired 3D Printed Polyetherimide Scaffold with Arg-Gly-Asp Peptides for the Improvement of Bioactivity and Osteogenic Differentiation of Osteoblasts. Mater. Today Commun. 2022, 30, 103166. [Google Scholar] [CrossRef]
- Ramesh, N.; Moratti, S.C.; Dias, G.J. Hydroxyapatite–Polymer Biocomposites for Bone Regeneration: A Review of Current Trends. J. Biomed. Mater. Res. Part B Appl. Biomater. 2018, 106, 2046–2057. [Google Scholar] [CrossRef]
- Mulchandani, N.; Prasad, A.; Katiyar, V. Chapter 4—Resorbable Polymers in Bone Repair and Regeneration; Grumezescu, V., Grumezescu, A.M.B.T., Eds.; Elsevier: Amsterdam, The Netherlands, 2019; pp. 87–125. ISBN 978-0-12-818415-8. [Google Scholar]
- Davison, N.L.; Barrère-de Groot, F.; Grijpma, D.W. Degradation of Biomaterials, 2nd ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2014; ISBN 9780124201453. [Google Scholar]
- Wu, C.; Chang, J. Multifunctional Mesoporous Bioactive Glasses for Effective Delivery of Therapeutic Ions and Drug/Growth Factors. J. Control. Release 2014, 193, 282–295. [Google Scholar] [CrossRef]
- Cacciotti, I. Bivalent Cationic Ions Doped Bioactive Glasses: The Influence of Magnesium, Zinc, Strontium and Copper on the Physical and Biological Properties. J. Mater. Sci. 2017, 52, 8812–8831. [Google Scholar] [CrossRef]
- Taye, M.B. Biomedical Applications of Ion-Doped Bioactive Glass: A Review. Appl. Nanosci. 2022, 12, 3797–3812. [Google Scholar] [CrossRef]
- Bettany, J.T.; Peet, N.M.; Wolowacz, R.G.; Skerry, T.M.; Grabowski, P.S. Tetracyclines Induce Apoptosis in Osteoclasts. Bone 2000, 27, 75–80. [Google Scholar] [CrossRef]
- Gomes, K.D.N.; Alves, A.P.N.N.; Dutra, P.G.P.; Viana, G.S.D.B. Doxycycline Induces Bone Repair and Changes in Wnt Signalling. Int. J. Oral Sci. 2017, 9, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Miron, R.; Sculean, A.; Kaskel, S.; Doert, T.; Schulze, R.; Zhang, Y. Proliferation, Differentiation and Gene Expression of Osteoblasts in Boron-Containing Associated with Dexamethasone Deliver from Mesoporous Bioactive Glass Scaffolds. Biomaterials 2011, 32, 7068–7078. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Tan, H.; Xu, W.; Wang, Z.; Zhang, J.; Li, S.; Zhou, T.; Li, J.; Niu, X. A Self-Healing, Magnetic and Injectable Biopolymer Hydrogel Generated by Dual Cross-Linking for Drug Delivery and Bone Repair. Acta Biomater. 2022, 153, 159–177. [Google Scholar] [CrossRef]
- Jahan, K.; Tabrizian, M. Composite Biopolymers for Bone Regeneration Enhancement in Bony Defects. Biomater. Sci. 2016, 4, 25–39. [Google Scholar] [CrossRef]
- Lucateli, R.L.; Marciano, M.A.; Ferreira, S.; Garcia Júnior, I.R.; Camilleri, J.; Mariano, R.C. Doxycycline and Autogenous Bone in Repair of Critical-Size Defects. Implant Dent. 2018, 27, 461–466. [Google Scholar] [CrossRef]
- Mardegan Issa, J.P.; Lucia, C.I.D.; Santos Kotake, B.G.D.; Gonzaga, M.G.; Tocchini de Figueiredo, F.A.; Iyomasa, D.M.; Macedo, A.P.; Ervolino, E. The Effect of Simvastatin Treatment on Bone Repair of Femoral Fracture in Animal Model. Growth Factors 2015, 33, 139–148. [Google Scholar] [CrossRef]
- Hoshi, S.; Akizuki, T.; Matsuura, T.; Ikawa, T.; Kinoshita, A.; Oda, S.; Tabata, Y.; Matsui, M.; Izumi, Y. Ridge Augmentation Using Recombinant Human Fibroblast Growth Factor-2 with Biodegradable Gelatin Sponges Incorporating β-Tricalcium Phosphate: A Preclinical Study in Dogs. J. Periodontal Res. 2016, 51, 77–85. [Google Scholar] [CrossRef]
- Ruskin, J.D.; Hardwick, R.; Buser, D.; Dahlin, C.; Schenk, R.K. Alveolar Ridge Repair in a Canine Model Using RhTGF-Β1 with Barrier Membranes. Clin. Oral Implant. Res. 2000, 11, 107–115. [Google Scholar] [CrossRef]
- Sun, R.; Liang, C.; Sun, Y.; Xu, Y.; Geng, W.; Li, J. Effects of Metformin on the Osteogenesis of Alveolar BMSCs from Diabetic Patients and Implant Osseointegration in Rats. Oral Dis. 2022, 28, 1170–1180. [Google Scholar] [CrossRef] [PubMed]
- Sun, T.; Huang, J.; Zhang, W.; Zheng, X.; Wang, H.; Liu, J.; Leng, H.; Yuan, W.; Song, C. Simvastatin-Hydroxyapatite Coatings Prevent Biofilm Formation and Improve Bone Formation in Implant-Associated Infections. Bioact. Mater. 2023, 21, 44–56. [Google Scholar] [CrossRef] [PubMed]
- Horwitz, E.M.; Prockop, D.J.; Gordon, P.L.; Koo, W.W.K.; Fitzpatrick, L.A.; Neel, M.D.; McCarville, M.E.; Orchard, P.J.; Pyeritz, R.E.; Brenner, M.K. Clinical Responses to Bone Marrow Transplantation in Children with Severe Osteogenesis Imperfecta. Blood 2001, 97, 1227–1231. [Google Scholar] [CrossRef] [PubMed]
- Hernigou, P.; Poignard, A.; Beaujean, F.; Rouard, H. Percutaneous Autologous Bone-Marrow Grafting for Nonunions: Influence of the Number and Concentration of Progenitor Cells. JBJS 2005, 87, 1430–1437. [Google Scholar] [CrossRef]
- Xu, C.; Su, P.; Chen, X.; Meng, Y.; Yu, W.; Xiang, A.P.; Wang, Y. Biocompatibility and Osteogenesis of Biomimetic Bioglass-Collagen-Phosphatidylserine Composite Scaffolds for Bone Tissue Engineering. Biomaterials 2011, 32, 1051–1058. [Google Scholar] [CrossRef]
- Marelli, B.; Ghezzi, C.E.; Mohn, D.; Stark, W.J.; Barralet, J.E.; Boccaccini, A.R.; Nazhat, S.N. Accelerated Mineralization of Dense Collagen-Nano Bioactive Glass Hybrid Gels Increases Scaffold Stiffness and Regulates Osteoblastic Function. Biomaterials 2011, 32, 8915–8926. [Google Scholar] [CrossRef]
- Williams, D.F. On the Nature of Biomaterials. Biomaterials 2009, 30, 5897–5909. [Google Scholar] [CrossRef]
- Ott, H.C.; Matthiesen, T.S.; Goh, S.-K.; Black, L.D.; Kren, S.M.; Netoff, T.I.; Taylor, D.A. Perfusion-Decellularized Matrix: Using Nature’s Platform to Engineer a Bioartificial Heart. Nat. Med. 2008, 14, 213–221. [Google Scholar] [CrossRef]
- Spalazzi, J.P.; Doty, S.B.; Moffat, K.L.; Levine, W.N.; Lu, H.H. Development of Controlled Matrix Heterogeneity on a Triphasic Scaffold for Orthopedic Interface Tissue Engineering. Tissue Eng. 2006, 12, 3497–3508. [Google Scholar] [CrossRef]
- Downing, T.L.; Soto, J.; Morez, C.; Houssin, T.; Fritz, A.; Yuan, F.; Chu, J.; Patel, S.; Schaffer, D.V.; Li, S. Biophysical Regulation of Epigenetic State and Cell Reprogramming. Nat. Mater. 2013, 12, 1154–1162. [Google Scholar] [CrossRef] [PubMed]
- Razavi, M.; Thakor, A.S. An Oxygen Plasma Treated Poly(Dimethylsiloxane) Bioscaffold Coated with Polydopamine for Stem Cell Therapy. J. Mater. Sci. Mater. Med. 2018, 29, 54. [Google Scholar] [CrossRef]
- Kargozar, S.; Singh, R.K.; Kim, H.-W.; Baino, F. “Hard” Ceramics for “Soft” Tissue Engineering: Paradox or Opportunity? Acta Biomater. 2020, 115, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Pittenger, M.F.; Mackay, A.M.; Beck, S.C.; Jaiswal, R.K.; Douglas, R.; Mosca, J.D.; Moorman, M.A.; Simonetti, D.W.; Craig, S.; Marshak, D.R. Multilineage Potential of Adult Human Mesenchymal Stem Cells. Science 1999, 284, 143–147. [Google Scholar] [CrossRef]
- Kitoh, H.; Kawasumi, M.; Kaneko, H.; Ishiguro, N. Differential Effects of Culture-Expanded Bone Marrow Cells on the Regeneration of Bone Between the Femoral and the Tibial Lengthenings. J. Pediatr. Orthop. 2009, 29, 643–649. [Google Scholar] [CrossRef] [PubMed]
- Morishita, T.; Honoki, K.; Ohgushi, H.; Kotobuki, N.; Matsushima, A.; Takakura, Y. Tissue Engineering Approach to the Treatment of Bone Tumors: Three Cases of Cultured Bone Grafts Derived From Patients’ Mesenchymal Stem Cells. Artif. Organs 2006, 30, 115–118. [Google Scholar] [CrossRef]
- Hernigou, P.; Poignard, A.; Zilber, S.; Rouard, H. Cell Therapy of Hip Osteonecrosis with Autologous Bone Marrow Grafting. Indian J. Orthop. 2009, 43, 40–45. [Google Scholar] [CrossRef]
- Gangji, V.; Hauzeur, J.-P.; Matos, C.; De Maertelaer, V.; Toungouz, M.; Lambermont, M. Treatment of Osteonecrosis of the Femoral Head with Implantation of Autologous Bone-Marrow Cells: A Pilot Study. JBJS 2004, 86, 1153–1160. [Google Scholar] [CrossRef]
- El-Husseiny, H.M.; Mady, E.A.; El-Dakroury, W.A.; Zewail, M.B.; Noshy, M.; Abdelfatah, A.M.; Doghish, A.S. Smart/Stimuli-Responsive Hydrogels: State-of-the-Art Platforms for Bone Tissue Engineering. Appl. Mater. Today 2022, 29, 101560. [Google Scholar] [CrossRef]
- Bai, X.; Gao, M.; Syed, S.; Zhuang, J.; Xu, X.; Zhang, X.-Q. Bioactive Hydrogels for Bone Regeneration. Bioact. Mater. 2018, 3, 401–417. [Google Scholar] [CrossRef]
- Short, A.R.; Koralla, D.; Deshmukh, A.; Wissel, B.; Stocker, B.; Calhoun, M.; Dean, D.; Winter, J.O. Hydrogels That Allow and Facilitate Bone Repair, Remodeling, and Regeneration. J. Mater. Chem. B 2015, 3, 7818–7830. [Google Scholar] [CrossRef] [PubMed]
- Rajabi, A.H.; Jaffe, M.; Arinzeh, T.L. Piezoelectric Materials for Tissue Regeneration: A Review. Acta Biomater. 2015, 24, 12–23. [Google Scholar] [CrossRef] [PubMed]
- Tandon, B.; Blaker, J.J.; Cartmell, S.H. Piezoelectric Materials as Stimulatory Biomedical Materials and Scaffolds for Bone Repair. Acta Biomater. 2018, 73, 1–20. [Google Scholar] [CrossRef]
- Ji, J.; Yang, C.; Shan, Y.; Sun, M.; Cui, X.; Xu, L.; Liang, S.; Li, T.; Fan, Y.; Luo, D.; et al. Research Trends of Piezoelectric Nanomaterials in Biomedical Engineering. Adv. NanoBiomed Res. 2023, 3, 2200088. [Google Scholar] [CrossRef]
- Lyons, J.G.; Plantz, M.A.; Hsu, W.K.; Hsu, E.L.; Minardi, S. Nanostructured Biomaterials for Bone Regeneration. Front. Bioeng. Biotechnol. 2020, 8, 922. [Google Scholar] [CrossRef]
- Dasari, A.; Xue, J.; Deb, S. Magnetic Nanoparticles in Bone Tissue Engineering. Nanomaterials 2022, 12, 757. [Google Scholar] [CrossRef]
- Lu, D.; Wu, X.; Wang, W.; Ma, C.; Pei, B.; Wu, S. Synthesis and Application of Iron Oxide Nanoparticles in Bone Tissue Repair. J. Nanomater. 2021, 2021, 3762490. [Google Scholar] [CrossRef]
- Pan, C.; Hao, X.; Deng, X.; Lu, F.; Liu, J.; Hou, W.; Xu, T. The Roles of Hippo/YAP Signaling Pathway in Physical Therapy. Cell Death Discov. 2024, 10, 197. [Google Scholar] [CrossRef] [PubMed]
- Brandaõ, A.S.; Bensimon-Brito, A.; Lourenço, R.; Borbinha, J.; Soares, A.R.; Mateus, R.; Jacinto, A. Yap Induces Osteoblast Differentiation by Modulating Bmp Signalling during Zebrafish Caudal Fin Regeneration. J. Cell Sci. 2019, 132. [Google Scholar] [CrossRef]
- Zhang, X.; Cheng, G.; Xing, X.; Liu, J.; Cheng, Y.; Ye, T.; Wang, Q.; Xiao, X.; Li, Z.; Deng, H. Near-Infrared Light-Triggered Porous AuPd Alloy Nanoparticles To Produce Mild Localized Heat To Accelerate Bone Regeneration. J. Phys. Chem. Lett. 2019, 10, 4185–4191. [Google Scholar] [CrossRef]
- Shi, W.; Wang, Z.; Bian, L.; Wu, Y.; Huiya, M.; Zhou, Y.; Zhang, Z.; Wang, Q.; Zhao, P.; Lu, X. Periodic Heat Stress Licenses EMSC Differentiation into Osteoblasts via YAP Signaling Pathway Activation. Stem Cells Int. 2022, 2022, 3715471. [Google Scholar] [CrossRef]
- Ding, F.; Zhang, L.; Chen, X.; Yin, W.; Ni, L.; Wang, M. Photothermal Nanohybrid Hydrogels for Biomedical Applications. Front. Bioeng. Biotechnol. 2022, 10, 1066617. [Google Scholar] [CrossRef]
- Tan, L.; Hu, Y.; Li, M.; Zhang, Y.; Xue, C.; Chen, M.; Luo, Z.; Cai, K. Remotely-Activatable Extracellular Matrix-Mimetic Hydrogel Promotes Physiological Bone Mineralization for Enhanced Cranial Defect Healing. Chem. Eng. J. 2022, 431, 133382. [Google Scholar] [CrossRef]
- Ma, H.; Jiang, C.; Zhai, D.; Luo, Y.; Chen, Y.; Lv, F.; Yi, Z.; Deng, Y.; Wang, J.; Chang, J.; et al. A Bifunctional Biomaterial with Photothermal Effect for Tumor Therapy and Bone Regeneration. Adv. Funct. Mater. 2016, 26, 1197–1208. [Google Scholar] [CrossRef]
- Khare, D.; Basu, B.; Dubey, A.K. Electrically Stimulated Piezoelectric Biomaterials as next Generation Implants for Orthopedic Applications. Biomaterials 2020, 258, 10-2139. [Google Scholar] [CrossRef]
- Khare, D.; Basu, B.; Dubey, A.K. Electrical Stimulation and Piezoelectric Biomaterials for Bone Tissue Engineering Applications. Biomaterials 2020, 258, 120280. [Google Scholar] [CrossRef]
- Damaraju, S.M.; Shen, Y.; Elele, E.; Khusid, B.; Eshghinejad, A.; Li, J.; Jaffe, M.; Arinzeh, T.L. Three-Dimensional Piezoelectric Fibrous Scaffolds Selectively Promote Mesenchymal Stem Cell Differentiation. Biomaterials 2017, 149, 51–62. [Google Scholar] [CrossRef]
- Opoku, C.; Dahiya, A.S.; Oshman, C.; Cayrel, F.; Poulin-Vittrant, G.; Alquier, D.; Camara, N. Fabrication of ZnO Nanowire Based Piezoelectric Generators and Related Structures. Phys. Procedia 2015, 70, 858–862. [Google Scholar] [CrossRef]
- Jacob, J.; More, N.; Kalia, K.; Kapusetti, G. Piezoelectric Smart Biomaterials for Bone and Cartilage Tissue Engineering. Inflamm. Regen. 2018, 38, 2. [Google Scholar] [CrossRef]
- Ehterami, A.; Kazemi, M.; Nazari, B.; Saraeian, P.; Azami, M. Fabrication and Characterization of Highly Porous Barium Titanate Based Scaffold Coated by Gel/HA Nanocomposite with High Piezoelectric Coefficient for Bone Tissue Engineering Applications. J. Mech. Behav. Biomed. Mater. 2018, 79, 195–202. [Google Scholar] [CrossRef]
- Martins, P.; Lopes, A.C.; Lanceros-Mendez, S. Electroactive Phases of Poly(Vinylidene Fluoride): Determination, Processing and Applications. Prog. Polym. Sci. 2014, 39, 683–706. [Google Scholar] [CrossRef]
- Samadi, A.; Ahmadi, R.; Hosseini, S.M. Influence of TiO2-Fe3O4-MWCNT Hybrid Nanotubes on Piezoelectric and Electromagnetic Wave Absorption Properties of Electrospun PVDF Nanocomposites. Org. Electron. 2019, 75, 105405. [Google Scholar] [CrossRef]
- Gimenes, R.; Zaghete, M.A.; Bertolini, M.; Varela, J.A.; Coelho, L.O.; Silva, N.F., Jr. Composites PVDF-TrFE/BT Used as Bioactive Membranes for Enhancing Bone Regeneration. In Proceedings of the SPIE, San Diego, CA, USA, 27 July 2004; Volume 5385, pp. 539–547. [Google Scholar]
- Saburi, E.; Islami, M.; Hosseinzadeh, S.; Moghadam, A.S.; Mansour, R.N.; Azadian, E.; Joneidi, Z.; Nikpoor, A.R.; Ghadiani, M.H.; Khodaii, Z.; et al. In Vitro Osteogenic Differentiation Potential of the Human Induced Pluripotent Stem Cells Augments When Grown on Graphene Oxide-Modified Nanofibers. Gene 2019, 696, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Yang, J.; Zhang, W.; Khoie, R.; Li, Y.M.; Zhu, J.G.; Chen, Z.Q. Manufacture and Cytotoxicity of a Lead-Free Piezoelectric Ceramic as a Bone Substitute-Consolidation of Porous Lithium Sodium Potassium Niobate by Cold Isostatic Pressing. Int. J. Oral Sci. 2009, 1, 99–104. [Google Scholar] [CrossRef]
- Chen, C.; Zhu, Y.; Ji, J.; Cai, F.; Zhang, Y.; Zhang, N.; Wang, A. Fabrication and Performance of Porous Lithium Sodium Potassium Niobate Ceramic. Mater. Res. Express 2018, 5, 25404. [Google Scholar] [CrossRef]
- Yao, T.; Chen, J.; Wang, Z.; Zhai, J.; Li, Y.; Xing, J.; Hu, S.; Tan, G.; Qi, S.; Chang, Y.; et al. The Antibacterial Effect of Potassium-Sodium Niobate Ceramics Based on Controlling Piezoelectric Properties. Colloids Surf. B Biointerfaces 2019, 175, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Verma, A.S.; Sharma, A.; Kumar, A.; Mukhopadhyay, A.; Kumar, D.; Dubey, A.K. Multifunctional Response of Piezoelectric Sodium Potassium Niobate (NKN)-Toughened Hydroxyapatite-Based Biocomposites. ACS Appl. Bio Mater. 2020, 3, 5287–5299. [Google Scholar] [CrossRef]
- Tariverdian, T.; Behnamghader, A.; Brouki Milan, P.; Barzegar-Bafrooei, H.; Mozafari, M. 3D-Printed Barium Strontium Titanate-Based Piezoelectric Scaffolds for Bone Tissue Engineering. Ceram. Int. 2019, 45, 14029–14038. [Google Scholar] [CrossRef]
- Chernozem, R.V.; Guselnikova, O.; Surmeneva, M.A.; Postnikov, P.S.; Abalymov, A.A.; Parakhonskiy, B.V.; De Roo, N.; Depla, D.; Skirtach, A.G.; Surmenev, R.A. Diazonium Chemistry Surface Treatment of Piezoelectric Polyhydroxybutyrate Scaffolds for Enhanced Osteoblastic Cell Growth. Appl. Mater. Today 2020, 20, 100758. [Google Scholar] [CrossRef]
- Chernozem, R.V.; Surmeneva, M.A.; Shkarina, S.N.; Loza, K.; Epple, M.; Ulbricht, M.; Cecilia, A.; Krause, B.; Baumbach, T.; Abalymov, A.A.; et al. Piezoelectric 3-D Fibrous Poly(3-Hydroxybutyrate)-Based Scaffolds Ultrasound-Mineralized with Calcium Carbonate for Bone Tissue Engineering: Inorganic Phase Formation, Osteoblast Cell Adhesion, and Proliferation. ACS Appl. Mater. Interfaces 2019, 11, 19522–19533. [Google Scholar] [CrossRef]
- Zhu, H.; Yang, H.; Ma, Y.; Lu, T.J.; Xu, F.; Genin, G.M.; Lin, M. Spatiotemporally Controlled Photoresponsive Hydrogels: Design and Predictive Modeling from Processing through Application. Adv. Funct. Mater. 2020, 30, 2000639. [Google Scholar] [CrossRef] [PubMed]
- Piluso, S.; Flores Gomez, D.; Dokter, I.; Moreira Texeira, L.; Li, Y.; Leijten, J.; Van Weeren, R.; Vermonden, T.; Karperien, M.; Malda, J. Rapid and Cytocompatible Cell-Laden Silk Hydrogel Formation: Via Riboflavin-Mediated Crosslinking. J. Mater. Chem. B 2020, 8, 9566–9575. [Google Scholar] [CrossRef] [PubMed]
- Xue, X.; Hu, Y.; Wang, S.; Chen, X.; Jiang, Y.; Su, J. Fabrication of Physical and Chemical Crosslinked Hydrogels for Bone Tissue Engineering. Bioact. Mater. 2022, 12, 327–339. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.; Wu, J.; Gu, Z. Black Phosphorus Hydrogel Scaffolds Enhance Bone Regeneration via a Sustained Supply of Calcium-Free Phosphorus. ACS Appl. Mater. Interfaces 2019, 11, 2908–2916. [Google Scholar] [CrossRef]
- Municoy, S.; Álvarez Echazú, M.I.; Antezana, P.E.; Galdopórpora, J.M.; Olivetti, C.; Mebert, A.M.; Foglia, M.L.; Tuttolomondo, M.V.; Alvarez, G.S.; Hardy, J.G.; et al. Stimuli-Responsive Materials for Tissue Engineering and Drug Delivery. Int. J. Mol. Sci. 2020, 21, 4724. [Google Scholar] [CrossRef]
- Fan, D.; Wang, Q.; Zhu, T.; Wang, H.; Liu, B.; Wang, Y.; Liu, Z.; Liu, X.; Fan, D.; Wang, X. Recent Advances of Magnetic Nanomaterials in Bone Tissue Repair. Front. Chem. 2020, 8, 745. [Google Scholar] [CrossRef]
- Montoya, C.; Du, Y.; Gianforcaro, A.L.; Orrego, S.; Yang, M.; Lelkes, P.I. On the Road to Smart Biomaterials for Bone Research: Definitions, Concepts, Advances, and Outlook. Bone Res. 2021, 9, 12. [Google Scholar] [CrossRef]
- De la Vega, R.E.; Atasoy-Zeybek, A.; Panos, J.A.; Van Griensven, M.; Evans, C.H.; Balmayor, E.R. Gene Therapy for Bone Healing: Lessons Learned and New Approaches. Transl. Res. 2021, 236, 1–16. [Google Scholar] [CrossRef]
- Chu, X.; Xiong, Y.; Lu, L.; Wang, Y.; Wang, J.; Zeng, R.; Hu, L.; Yan, C.; Zhao, Z.; Lin, S.; et al. Research Progress of Gene Therapy Combined with Tissue Engineering to Promote Bone Regeneration. APL Bioeng. 2024, 8, 551. [Google Scholar] [CrossRef]
- Watanabe, M.; Nishikawaji, Y.; Kawakami, H.; Kosai, K.I. Adenovirus Biology, Recombinant Adenovirus, and Adenovirus Usage in Gene Therapy. Viruses 2021, 13, 2502. [Google Scholar] [CrossRef]
- Sharma, S.; Sapkota, D.; Xue, Y.; Rajthala, S.; Yassin, M.A.; Finne-Wistrand, A.; Mustafa, K. Delivery of VEGFA in Bone Marrow Stromal Cells Seeded in Copolymer Scaffold Enhances Angiogenesis, but Is Inadequate for Osteogenesis as Compared with the Dual Delivery of VEGFA and BMP2 in a Subcutaneous Mouse Model. Stem Cell Res. Ther. 2018, 9, 23. [Google Scholar] [CrossRef] [PubMed]
- Oh, W.-T.; Yang, Y.-S.; Xie, J.; Ma, H.; Kim, J.-M.; Park, K.-H.; Oh, D.S.; Park-Min, K.-H.; Greenblatt, M.B.; Gao, G.; et al. WNT-Modulating Gene Silencers as a Gene Therapy for Osteoporosis, Bone Fracture, and Critical-Sized Bone Defects. Mol. Ther. 2023, 31, 435–453. [Google Scholar] [CrossRef]
- Vhora, I.; Lalani, R.; Bhatt, P.; Patil, S.; Misra, A. Lipid-Nucleic Acid Nanoparticles of Novel Ionizable Lipids for Systemic BMP-9 Gene Delivery to Bone-Marrow Mesenchymal Stem Cells for Osteoinduction. Int. J. Pharm. 2019, 563, 324–336. [Google Scholar] [CrossRef]
- Xiang, Y.; Oo, N.N.L.; Lee, J.P.; Li, Z.; Loh, X.J. Recent Development of Synthetic Nonviral Systems for Sustained Gene Delivery. Drug Discov. Today 2017, 22, 1318–1335. [Google Scholar] [CrossRef]
- Su, N.; Villicana, C.; Yang, F. Immunomodulatory Strategies for Bone Regeneration: A Review from the Perspective of Disease Types. Biomaterials 2022, 286, 121604. [Google Scholar] [CrossRef]
- Khan, A.R.; Grewal, N.S.; Jun, Z.; Tawfiq, F.M.O.; Tchier, F.; Muhammad Zulqarnain, R.; Zhang, H.-J. Raising the Bar: Progress in 3D-Printed Hybrid Bone Scaffolds for Clinical Applications: A Review. Cell Transplant. 2024, 33, 09636897241273562. [Google Scholar] [CrossRef] [PubMed]
- Bariwal, J.; Ma, H.; Altenberg, G.A.; Liang, H. Nanodiscs: A Versatile Nanocarrier Platform for Cancer Diagnosis and Treatment. Chem. Soc. Rev. 2022, 51, 1702–1728. [Google Scholar] [CrossRef]
- Xing, H.; Wang, X.; Xiao, G.; Zhao, Z.; Zou, S.; Li, M.; Richardson, J.J.; Tardy, B.L.; Xie, L.; Komasa, S.; et al. Hierarchical Assembly of Nanostructured Coating for SiRNA-Based Dual Therapy of Bone Regeneration and Revascularization. Biomaterials 2020, 235, 119784. [Google Scholar] [CrossRef] [PubMed]
- Simunovic, F.; Finkenzeller, G. Vascularization Strategies in Bone Tissue Engineering. Cells 2021, 10, 1749. [Google Scholar] [CrossRef]
- Pal, S. Design of Artificial Human Joints & Organs. Des. Artif. Hum. Jt. Organs 2014, 1, 9781461462. [Google Scholar] [CrossRef]
- Black, N.R.; Winslade, W.J.; Lindsey, R.W.; Gugala, Z. The Legal, Ethical, and Scientific Considerations for Returning Explanted Orthopaedic Hardware to the Patient. JBJS 2022, 104, e37. [Google Scholar] [CrossRef] [PubMed]
- Willemsen, K.; Nizak, R.; Noordmans, H.J.; Castelein, R.M.; Weinans, H.; Kruyt, M.C. Challenges in the Design and Regulatory Approval of 3D-Printed Surgical Implants: A Two-Case Series. Lancet Digit. Health 2019, 1, e163–e171. [Google Scholar] [CrossRef] [PubMed]

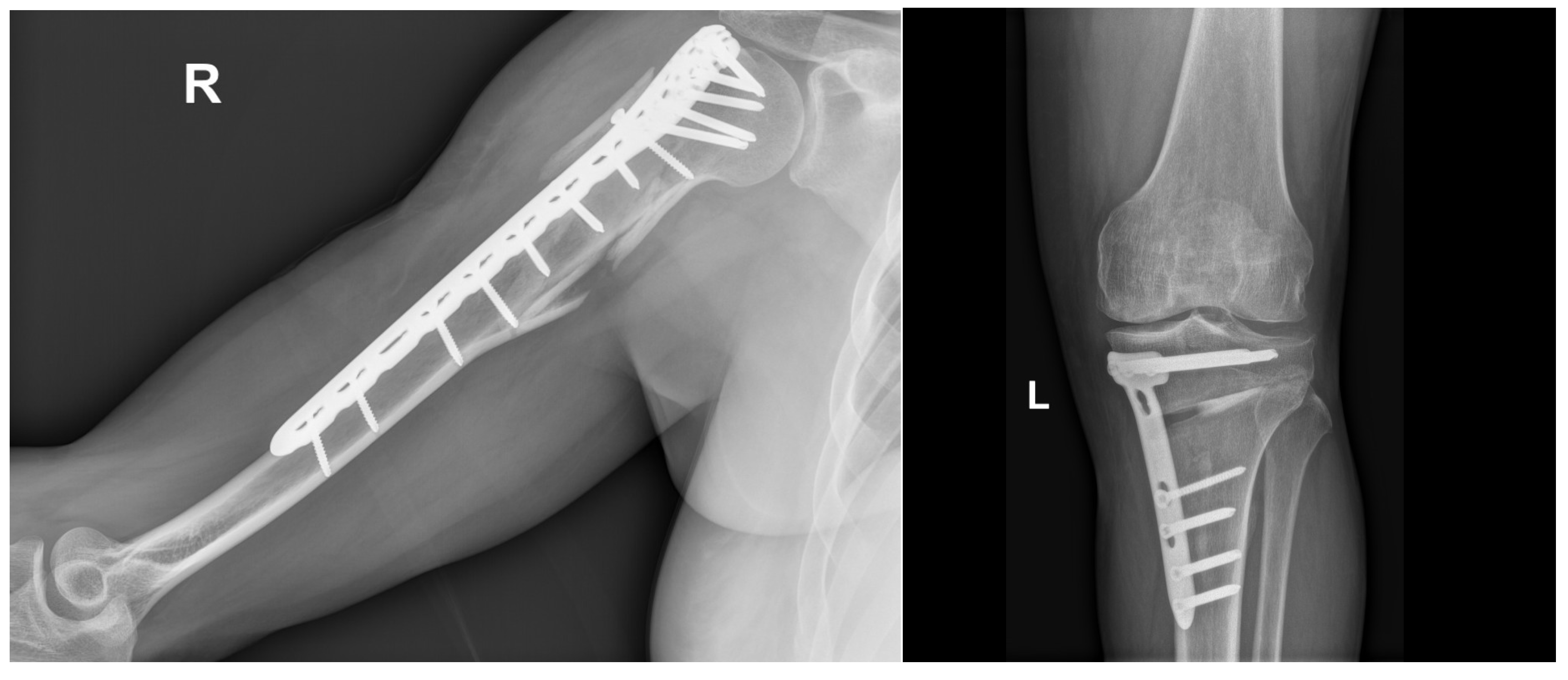
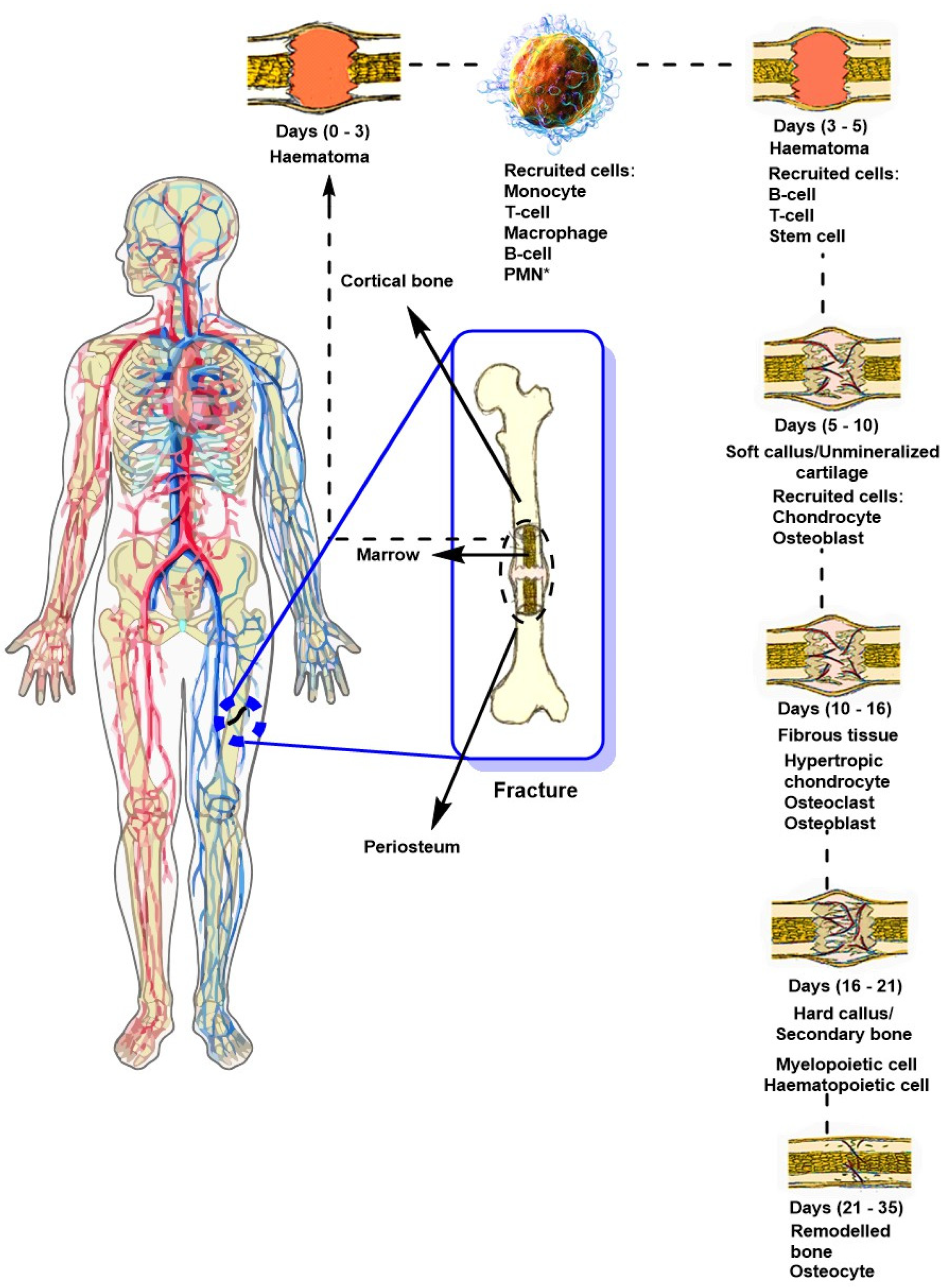
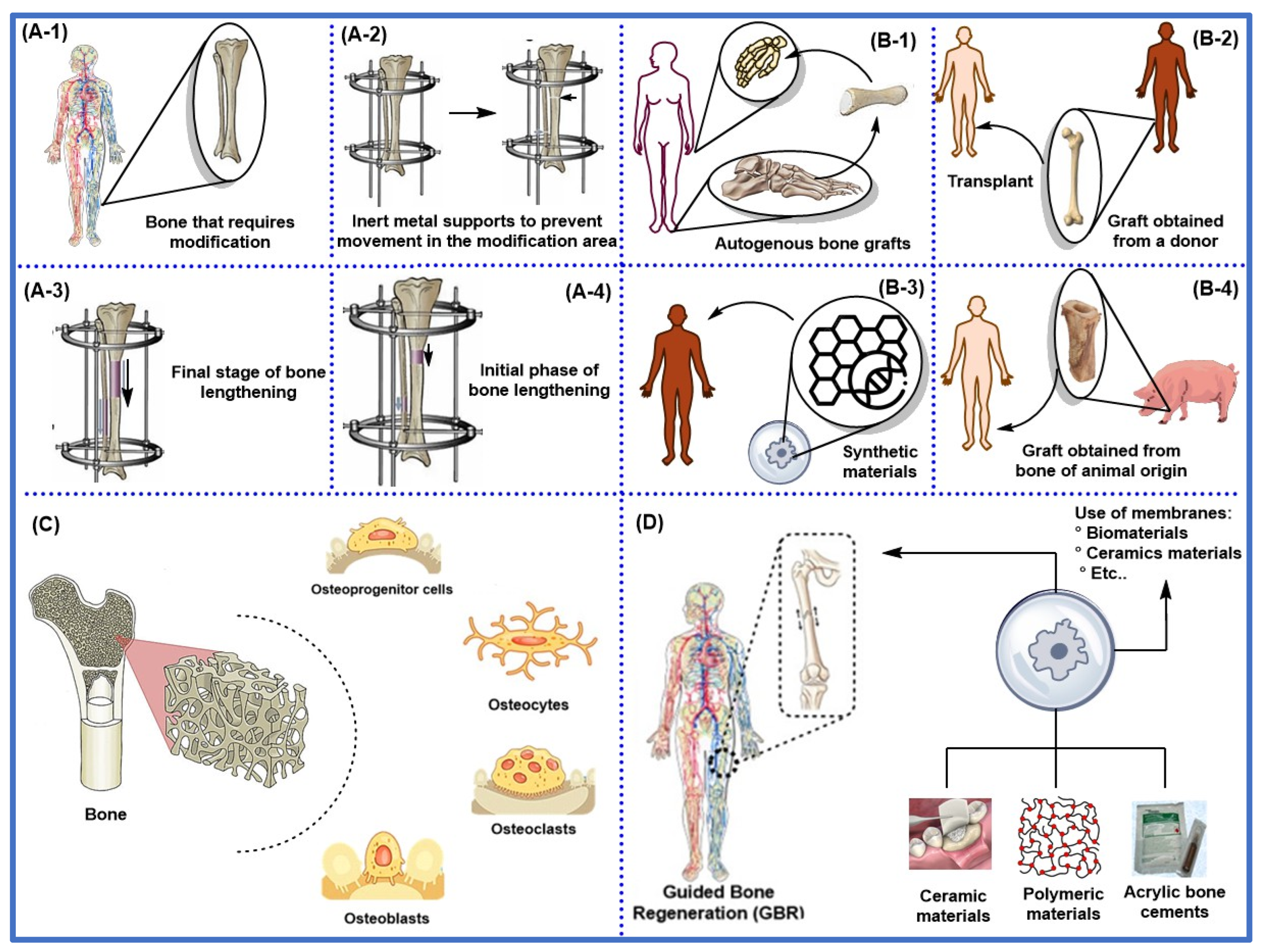
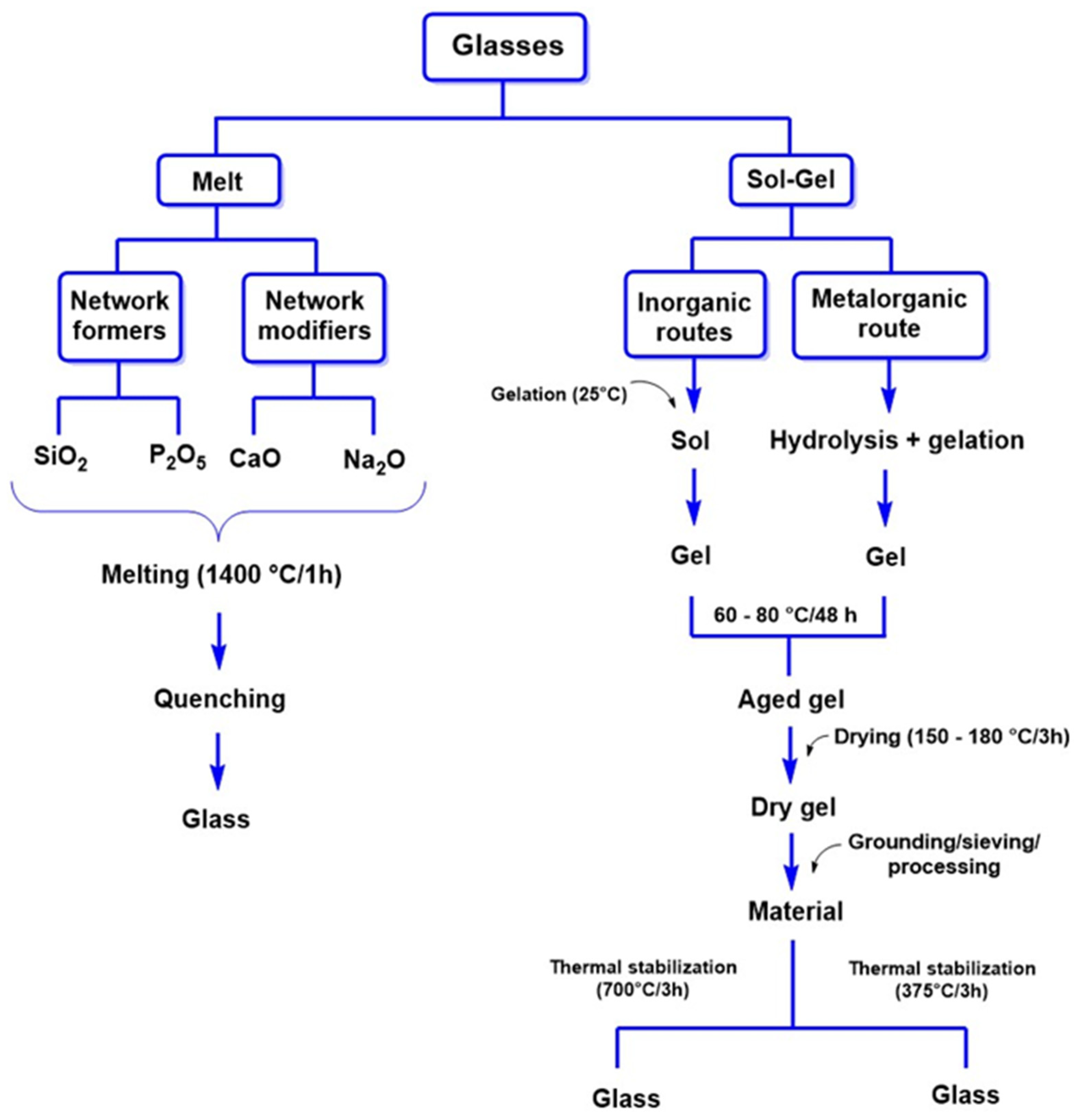
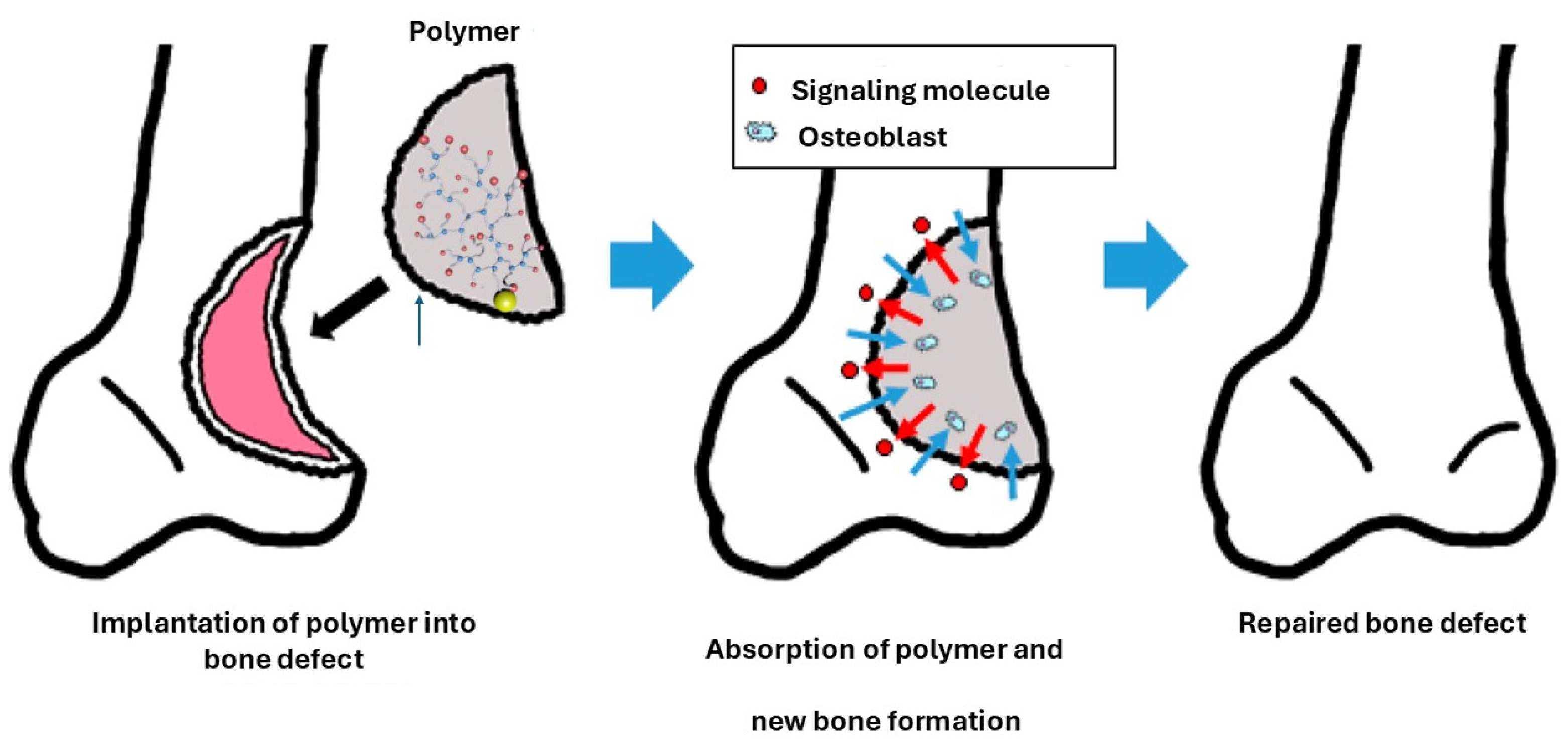

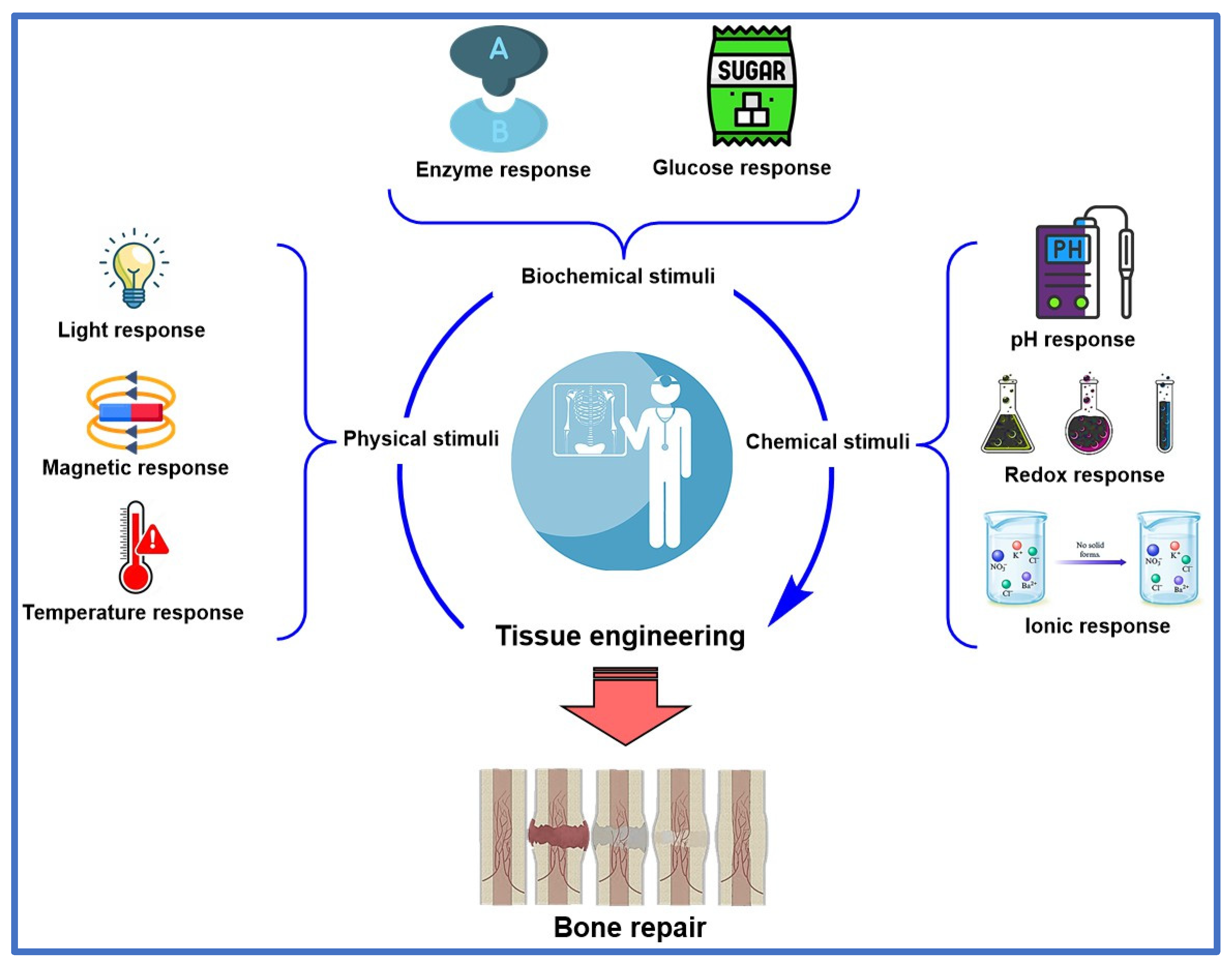

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Classification | Type of Fracture | Description | Graft or Biomaterial Requirements | Ref. |
|---|---|---|---|---|
| According to the type of fracture | Cross | Line that forms a right angle with the longitudinal axis of the bone. | - | [39] |
| Oblique | The line is presented at an angle about the longitudinal axis of the bone. | - | ||
| Spiral | A helix-shaped line that surrounds the contour of the bone. | - | ||
| Linear | Line that extends parallel to the longitudinal axis of the bone without displacement. | - | ||
| Green stem | A partial fracture is common in childhood, where the bone is deformed by bending without breaking completely. | Hydroxyapatite to mimic the chemical composition of bone and promote cell migration and/or communication at both ends of the fracture. | ||
| According to the type of damage | Complete | The bone fractures into two or more segments. | Phosphate-based nanobiocomposites to promote bone regeneration in complicated fractures. | [40] |
| Incomplete | Cracks or incomplete fractures in the bone. | - | ||
| Comminuted | The bone breaks into several fragments. | Grafts extracted from the same patient (autologous grafts) or a donor (allogeneic grafts). | ||
| Composed | The fracture pierces the skin, exposing the bone to the outside environment. | Synthetic biomaterials such as hydroxyapatite and/or calcium phosphates are required as fillers in bone defects. | ||
| Closed | There is no connection between the fracture and the external environment. | Nanobiocomposites, hydroxyapatites, and 3D scaffolds with stem cells to promote osteogenesis. | ||
| According to the mechanism of injury | Flexion | It occurs as a result of forces that induce the bone to bend. | - | [41] |
| Torsion | It arises from forces that cause a twisting movement. | - | ||
| Compression | It occurs due to forces that exert pressure on the bone, causing it to collapse. | - | ||
| Sharing | It occurs when two forces exert pressure on the same bone in opposite directions. | - | ||
| Pathological | They occur due to medical conditions compromising bone strength, such as osteoporosis or tumors. | Osteoinductive materials that stimulate bone formation. | ||
| Fatigue or stress | Minor fractures caused by repeated stress are common among athletes. | Nanostructured grafts to improve the stability and mechanical resistance of the affected area. | ||
| According to the energy of trauma | High energy | Caused by severe trauma, such as in accidents, these fractures often show considerable fragmentation and affect the surrounding tissues. | - | [42] |
| Low energy | They occur due to falls or inappropriate movements, especially in older people with fragile bones. | Hydroxyapatites, calcium phosphates, 3D scaffolds with stem cells and growth factors to promote osteogenesis and to treat compromised bone mass. |
| Type of Material | Material | Manufacturing Technique | Modifications | Type of Sterilization | In Vivo Applications | Implantation Site | Ref. |
|---|---|---|---|---|---|---|---|
| Ceramics | α-TCP 1 | Inkjet printing. | - | Autoclave | Human | Maxillofacial | [70] |
| TCP 2 | Dispensing by tracing. | Impregnation with osteoblasts and coating with collagen. | Plasma | Sheep | Calvary | [71] | |
| β-TCP 3 | Robocasting. | Coating with mesoporous bioglasses. | - | Rabbit | Mandible, skull | [72,73] | |
| Dicalcium phosphate | Dispensing by tracing. | - | γ-irradiation | Goat | Lumbar area | [74] | |
| Biphasic calcium phosphates | Robocasting. | Impregnation with bone morphogenetic proteins. | Heating | Pig and rabbit | Mandible, tibia | [75] | |
| Composites | PCL 4/PLGA 5 | Additive manufacturing. | Collagen enriched with rhBMP-2. | Ultraviolet | Rabbit | Calvaria and radio | [76,77] |
| PCL/PLGA/β-TCP | Additive manufacturing. | Collagen enriched with rhBMP-2. | - | Rabbit | Calvaria | [76,78] | |
| PLGA/β-TCP | Fused deposition modeling. | HA coating. | Ethylene oxide | Rabbit | Femur | [79] | |
| PCL/HA 6 | Selective laser sintering. | - | - | Rabbit | Femur | [80] | |
| PLA/nHA 7 | Fused deposition modeling. | - | Impregnation with ethanol | Rabbit | Femur | [81] | |
| TCP/CS 8/ Collagen hydrogel | Dispensing by tracing. | Impregnation with osteoblasts. | Plasma | Sheep | Calvaria | [71] | |
| Synthetic biodegradable polymers | PCL | Selective laser sintering. | Impregnation with recombinant human platelet-derived growth factors. | Ethylene oxide | Human | Periodontal | [82] |
| PLA 9 | Fused deposition modeling. | - | Impregnation with ethanol | Rats | Femur | [83] | |
| PLGA | Dispensing by tracing. | - | Rabbit | Iliac bone | [84] | ||
| Non-degradable synthetic polymers | PEKK 10 | Selective laser sintering. | Autologous bone. | Autoclave | Sheep | Calvaria | [85] |
| Fused deposition modeling. | - | - | Human | Rib | [86] |
| Type of Bone Graft | Origin | Advantages | Disadvantages | Reported Cases | Ref. |
|---|---|---|---|---|---|
| Autologous bone | It is extracted from the same patient. | It presents functional osteoblasts, excellent osteoconductivity, biocompatibility, and bone induction properties. | It requires additional surgical procedures, which may compromise nerves, tissues, and arteries and increase morbidity. | Autologous iliac bone graft for the treatment of tibial nonunion. This graft has demonstrated osteoblast activity and BMP- and glycoprotein-induced osteogenesis in 51 patients. | [116] |
| Allogenic bone | The graft comes from a donor. It may be genetically different from the donor, but from the same species as the recipient. | It presents functional growth factors, various types of functional tissue cells, extracellular matrix, and other relevant factors. | It presents a high antigenic risk, the spread of diseases, and the risk of rejection. | Allogeneic bone screw implantation in hands and feet in 32 patients. The implant demonstrated rapid immune acceptance by the patient and a swift recovery with minimal pain. | [117] |
| Xenogeneic bone | The graft originates from a species different from the patient’s (usually bovine or porcine), thus having a distinct genetic origin. | They have a large volume and are abundantly available. Additionally, some species exhibit good osteoconductivity. | It is highly antigenic, has a high propensity for disease, and presents risks of rejection by the patient. | In 11 patients, a xenogeneic bone ring graft was used to treat horizontal alveolar bone defects. All patients achieved 100% implant survival and acceptance rates. | [118] |
| Generation of the Material | Material Name | Biological Behavior | Clinical Application | Example | Ref. |
|---|---|---|---|---|---|
| First generation | Aluminas, Zirconia | Bioinert | Coatings for tissue growth. Orthopedic, dental, and maxillofacial applications. | ZrO2, composed of PE-HA y Al2O3 | [167] |
| Titanium Nitride, Zirconium Nitride | Bioinert | Knee prosthesis, anti-wear coating on bone joints. | TiN, ZrN | [168] | |
| Silicon Nitride | Bioinert | Anti-wear coating on joints. | Si3N4 | [169] | |
| Second generation | HA | Bioactive | Bone cavity filling, cartilage implants, vertebral replacement, hip implants, bone and orthopedic scaffolding. | Carbon fiber composites-PLA, HA, bioactive glass, and glass ceramics | [170] |
| Bioglass | Bioactive | Bone replacement. | Bioactive glass and glass-ceramics | [171] | |
| β-TCP | Bioactive O/Biodegradable | Bone replacement. | Ca3(PO4)2 | [172] | |
| HA/PCL | Biodegradable | Scaffolds in tissue engineering. | - | ||
| DCPD | Biodegradable | Bone regeneration, osteoconductivity. | - | [173] | |
| Calcium Phosphate | Promotes tissue growth and vascularization. | Ca3(PO4)2 | [174] | ||
| Third generation | Biodegradable ceramics | Bioactive/Biodegradable | These materials are based on scaffolds that support cell attachment and growth, actively participating in the healing process by releasing growth factors or other bioactive substances. | - | [175] |
| Biopolymers | Nanobioglass | Resulting Compound | Applications | Ref. |
|---|---|---|---|---|
| Alginate | Mesoporous with 10% by weight. | Microspheres | Increases drug loading and release capacity due to its surface area. | [193] |
| PHBV | 45S5 10% by weight. | Scaffolding | Cartilage transplants and repair. | [194] |
| PCL | Mesoporous 5% by weight. | Scaffolding | Bone regeneration. | [195] |
| PLLA | Mesoporous 15% by weight. | Scaffolding bases | Bone regeneration. | [196] |
| PLGA | 45S5 | Microspheres | Endothelial activity | [197] |
| Collagen | Mesoporous 10% by weight. | - | Cartilage regeneration and transplantation. | [198] |
| Chitosan | - | Nanofibers | It improves biomineralization and stimulates the formation of bone extracellular matrix by osteoblasts. | [199] |
| PLA | Mesoporous 10% by weight. | Nanocomposite | Repairs bone tissue and prevents microbial contamination. | [200] |
| CS-G-NBG-GO | - | Scaffold | It has excellent cytocompatibility with MG-63 cell lines. | [201] |
| Material | Cells | Method | Advantages | Disadvantages | Ref. |
|---|---|---|---|---|---|
| LNKN | Osteoblasts | CIP 1 | It promotes extracellular matrix-like topography, improves biological performance, and enhances piezoelectricity through CIP using sodium, lithium, and potassium niobate samples. It also exhibits positive in vitro effects on osteoblast adhesion and proliferation. | It is limited in permissible doses, has a long synthesis time, and is expensive, which restricts its applicability in regenerative medicine. Furthermore, these improved properties only occur through unconventional methods such as CIP. | [303] |
| LNKN | - | Foam formation | It exhibits relative dielectric and piezoelectric constants of 67.29 and 48 pC/N, respectively. The piezoelectric properties are optimized by 65% by weight of solids and 30% by weight of foaming agent, which improves its ability to stimulate osteoblast production and facilitates its application and production. | Increasing the amount of foaming agents increases the material’s porosity, resulting in a more uniform pore structure. However, this decreases the density and dielectric constant. | [304] |
| KNN 2 | BMSC 3 | Mechanosynthesis | Improved cell adhesion and colony reduction in Staphylococcus aureus bacteria, which is attractive for preventing infections, and BMSC cell proliferation induced by piezoceramics. | Low efficiency and high costs. | [305] |
| KNN/HA | MG-63 | Mechanosynthesis | The mechanical properties of the HA composite containing 30% by weight of KNN are as follows: a hardness of 93%, a fracture toughness of 209%, a flexural strength of 88%, and a compressive strength of 112%. This is attractive for applications in problematic bone defects. | A significant reduction in bacterial viability (E. coli and S. aureus) was observed in samples of HA-KNN composites subjected to in vitro polarization, which is concerning for applications in regenerative medicine, particularly bone regeneration and limb preservation. | [306] |
| Barium strontium titanate (BST)/β-TCP | BMSC | 3D printing | Samples containing 40% β-TCP and 60% BST exhibit high compressive strength, flexural strength, elasticity, and a high Young’s modulus. Furthermore, these samples exhibit significant bone apatite formation after 28 days in SBF. | It involves temperatures of up to 770 °C, where significant weight loss is recorded due to solvent evaporation during drying. This situation limits its performance and increases costs. | [307] |
| PHB 4/PCL | Osteoblasts | Electrospinning | Improved wettability and cell dispersion in PHB (piezoelectric) and PCL (non-piezoelectric) scaffolds. This combination improves mechanical strength and biocompatibility. | Reduction in the piezoelectric coefficient d33 (from 2.5 ± 0.3 to 2.1 ± 0.4 pC/N) and in the surface electric potential (from 510 ± 56 to 458 ± 25 mV) by surface treatment with diazonium. | [308] |
| PHB/CaCO3 PHBV/CaCO3 | Osteoblasts | Ultrasound | The piezoelectric coefficient of PHB is higher (d33 = 3.0 ± 0.5 pC/N) than PHBV scaffolds (d33 = 0.7 ± 0.5 pC/N). Furthermore, PHB exhibits higher porosity (approximately 15%) than PHBV scaffolds due to the homogeneous growth of CaCO3 on the 3D fibrous structures. | Low efficiency. | [309] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carrascal-Hernández, D.C.; Martínez-Cano, J.P.; Rodríguez Macías, J.D.; Grande-Tovar, C.D. Evolution in Bone Tissue Regeneration: From Grafts to Innovative Biomaterials. Int. J. Mol. Sci. 2025, 26, 4242. https://doi.org/10.3390/ijms26094242
Carrascal-Hernández DC, Martínez-Cano JP, Rodríguez Macías JD, Grande-Tovar CD. Evolution in Bone Tissue Regeneration: From Grafts to Innovative Biomaterials. International Journal of Molecular Sciences. 2025; 26(9):4242. https://doi.org/10.3390/ijms26094242
Chicago/Turabian StyleCarrascal-Hernández, Domingo Cesar, Juan Pablo Martínez-Cano, Juan David Rodríguez Macías, and Carlos David Grande-Tovar. 2025. "Evolution in Bone Tissue Regeneration: From Grafts to Innovative Biomaterials" International Journal of Molecular Sciences 26, no. 9: 4242. https://doi.org/10.3390/ijms26094242
APA StyleCarrascal-Hernández, D. C., Martínez-Cano, J. P., Rodríguez Macías, J. D., & Grande-Tovar, C. D. (2025). Evolution in Bone Tissue Regeneration: From Grafts to Innovative Biomaterials. International Journal of Molecular Sciences, 26(9), 4242. https://doi.org/10.3390/ijms26094242