Abstract
This study aimed to evaluate the diagnostic potential of soluble Programmed Death Ligand 1 (sPD-L1) and Programmed Death 1 (sPD-1) molecules in plasma, along with urinary mRNA biomarkers—Prostate-Specific Membrane Antigen (PSMA), Prostate Cancer Antigen 3 (PCA3), and androgen receptor (AR) genes—for identifying clinically significant prostate cancer (PCa), defined as pathological stage 3. In a cohort of 68 PCa patients, sPD-L1 and sPD-1 levels were quantified using ELISA, while mRNA transcripts were measured by RT-qPCR. Results highlight the potential of integrating these liquid-based biomarkers. In particular, the combination of sPD-L1, sPD-1, and AR demonstrated the most significant improvement in diagnostic performance, increasing the area under the curve (AUC) from 0.65 to 0.81 and sensitivity from 60% to 88%, compared to AR alone. PSMA demonstrated an AUC of 0.82 and a specificity of 52.8%, which improved to an AUC of 0.85 and a specificity of 94.4% with the inclusion of sPD-L1 and sPD-1. Similarly, PCA3 achieved an AUC of 0.75 and a specificity of 53.8%, increasing to an AUC of 0.78 and a specificity of 76.9% when combined with these biomarkers. Incorporating sPD-L1 into a three-gene panel further elevated the AUC from 0.74 to 0.94. These findings underscore the value of multimodal liquid-based diagnostic panels in improving the management of clinically significant PCa.
1. Introduction
Prostate cancer (PCa) remains the second most prevalent cancer in men globally [1,2], comprising roughly 15% of all cancer diagnoses worldwide. Forecasts indicate that the annual number of new prostate cancer cases is expected to increase from 1.4 million in 2020 to 2.9 million by 2040, based on analysis of global demographic shifts and the rising rates of life expectancy [3]. Considering that PCa is characterized as a heterogeneous disease [4], a variety of risk factors are involved in prostate cancer progression such as environmental, genetic and molecular factors [5]. Given this complexity, there is an urgent need for innovative, minimally invasive diagnostic strategies that prioritize precision oncology and personalized medicine. Liquid biopsy has recently gained significant attention as a promising tool in prostate cancer stratification, especially in genome sequencing profiling methods [6]. Meanwhile, liquid biopsy techniques that analyze soluble molecules by ELISA methods and urinary mRNA transcripts using RT-qPCR are well-suited for routine diagnostic applications. Compared to genome sequencing profiling, these methods provide enhanced scalability, cost-efficiency and economic feasibility. They also offer reliable predictive value and significantly shorter turnaround times, making them practical for widespread clinical implementation across diverse healthcare settings. Circulating plasma molecules such as soluble PD-L1 and PD-1 (sPD-L1 and sPD-1) have drawn notable focus in recent research due to their potential as prognostic and predictive markers in different cancer types [7,8,9] and demonstrated prognostic significance in our previous research on prostate cancer [10]. Urinary mRNAs, including those of PSMA, PCA3, and AR, play a significant role in prostate cancer development. These biomarkers provide valuable insights into the genetic landscape of tumors and are widely utilized in the diagnosis of prostate cancer [11,12,13,14,15,16,17,18]. The novel approach of combining multiple biomarkers has the potential to improve the accuracy of PCa detection and risk stratification. By integrating data from diverse biomarkers, a comprehensive immune and molecular profile of the patient’s disease can be constructed, providing valuable insights into the prediction of clinically significant prostate cancer. This approach underscores the expanded utility of liquid biopsies in future clinical applications.
2. Results
2.1. Biomarker Association with Prostate Cancer Clinical Features
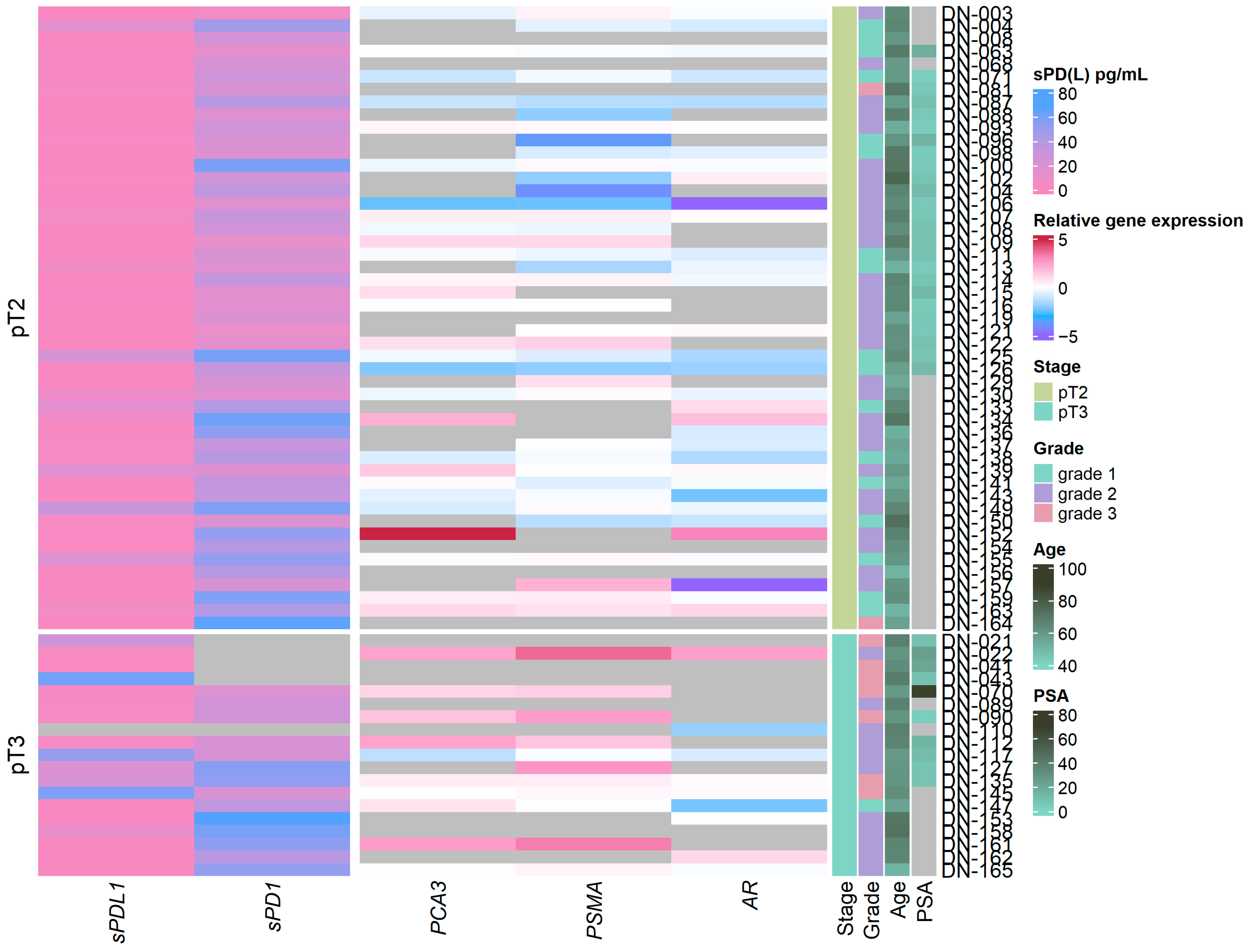
Analysis of relative AR, PCA3, and PSMA mRNA expression in urine discovered a significant increase in PSMA (p ≤ 0.001) and PCA3 (p ≤ 0.05) expression in clinically significant PCa when compared with clinically insignificant PCa cases, if classified as pathological stage pT3 (Figure 1 and Figure S1a), as well as significant associations between PSMA expression and tumor grade (grade 1 vs. grade 3 p = 0.005, grade 1 vs. grade 2 p = 0.011) (Figure S2a).
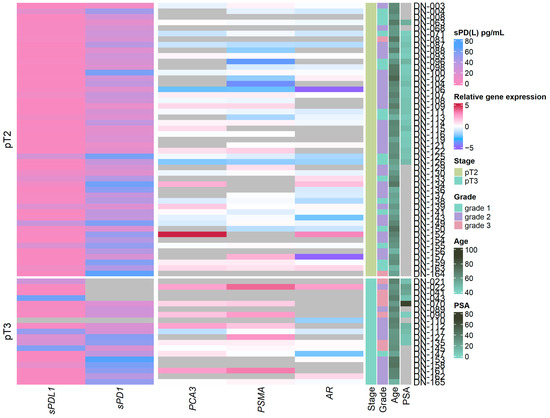
Figure 1.
Heatmap depicting sPD-L1/sPD-1 biomarker concentrations in plasma and gene expression in urine sediment samples from prostate cancer patients together with clinical features. Clinically significant cases: pathological stage pT3. ISUP grade 1, 2 or 3. Grey color depicts no available data.
Soluble PD-1 and PD-L1 revealed sPD-L1 association with clinically significant PCa (sPDL1 p = 0.031) (Figure S1b), and grade 3 PCa (grade 2 vs. grade 3 sPDL1 = 0.026) (Figure S2b), while sPD-1 showed no differences in any of the clinical features examined.
No significant association between relative AR, PCA3, and PSMA mRNA expression and either the plasma biomarkers (sPD-L1 or sPD-1) or other clinical features (age, serum PSA concentration or immune cell count) was discovered.
2.2. Prediction of Clinically Significant PCa Using Liquid Biopsy Biomarkers
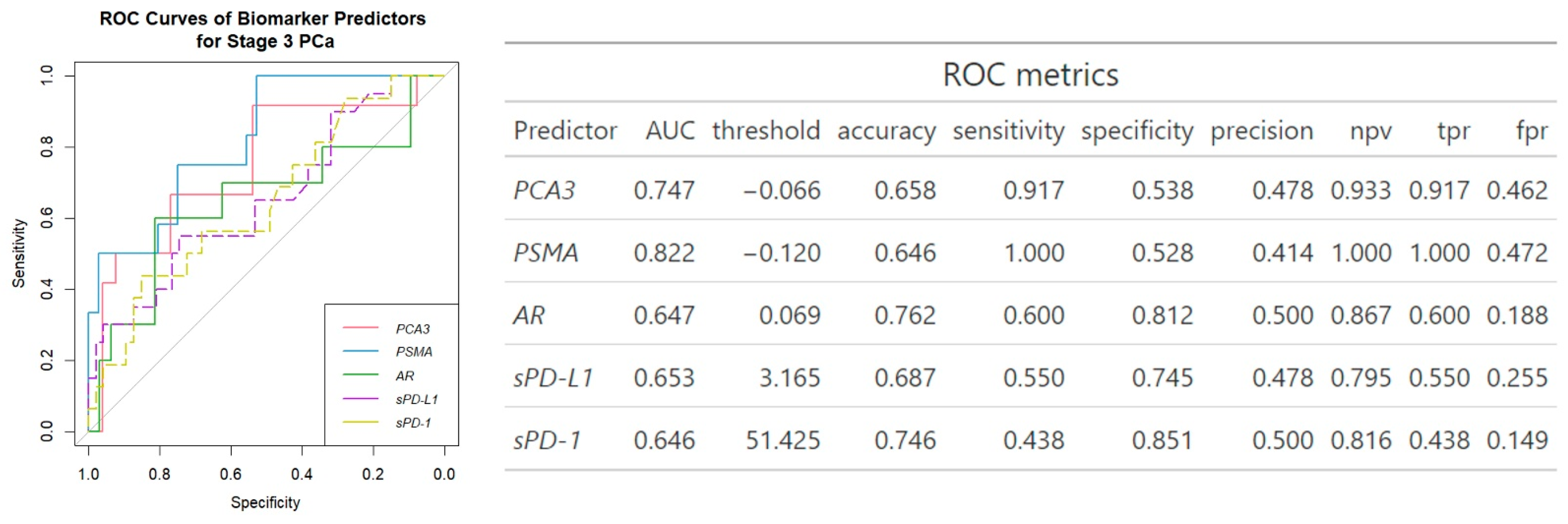
ROC analysis revealed PSMA to be the best single gene expression biomarker predictor of clinically significant PCa (AUC = 0.82) (Figure 2) with the highest sensitivity (1.00). On the other hand, sPD-1 showed the best single biomarker specificity (0.85), but lowest sensitivity (0.44).
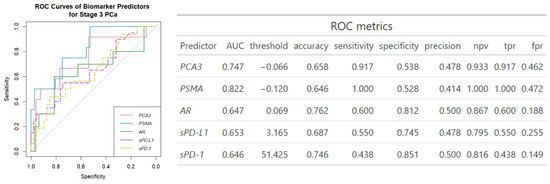
Figure 2.
ROC analysis of biomarker prediction of clinically significant PCa. npv—negative predictive value, tpr—true positive rate, fpr—false positive rate.
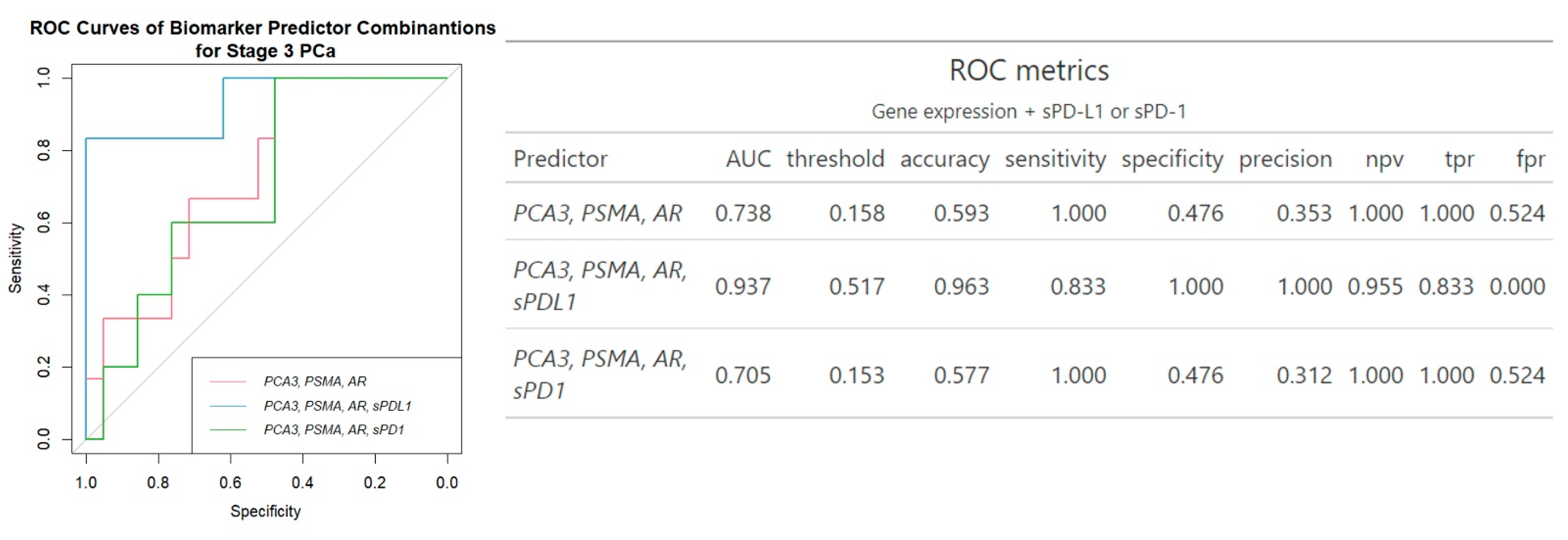
Regarding the combination of urine and plasma biomarkers together, an increase in AUC values was noticed. While combining the three mRNAs’ expression did not increase the prediction of clinically significant PCa (AUC 0.74 vs. AUC 0.82 of PSMA and AUC 0.75 of PCA3 biomarker), the panel comprising three mRNA transcripts along with sPD-L1 demonstrates significant enhancement in diagnostic properties compared to mRNA transcripts without sPD-L1, with an AUC of 0.94, accuracy of 0.96, sensitivity of 0.83 and specificity of 100%. The inclusion of sPD-1 did not enhance the diagnostic performance of the three-gene panel (Figure 3).
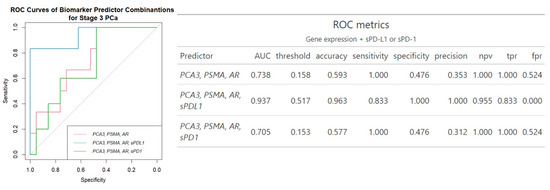
Figure 3.
ROC analysis of biomarker combinations for prediction of clinically significant PCa. Npv—negative predictive value, tpr—true positive rate, fpr—false positive rate.
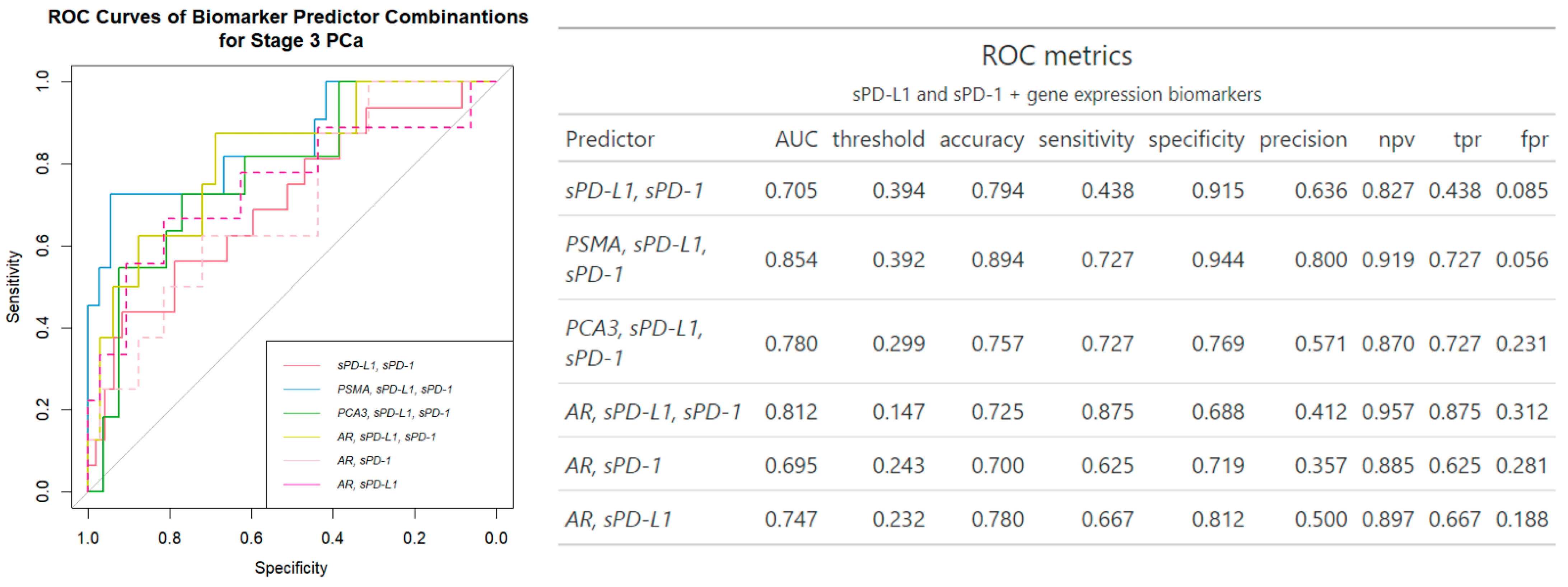
Of note, the addition of plasma sPD-L1 and sPD-1 to PSMA and PCA3 gene expression biomarkers slightly increased AUC by (0.82 to 0.85) and (0.75 to 0.78), respectively, compared to the biomarkers alone. The combination of AR and two plasma biomarkers overall showed the most substantial improvement (AUC 0.65 to 0.81), compared to a single mRNA alone, in separation of clinically significant PCa out of all biomarkers examined.
While PSMA emerged as the most robust standalone biomarker (AUC 0.82), AR demonstrated modest performance (AUC 0.65). However, the combination of AR mRNA from urine with sPD-L1 and sPD-1 significantly improved diagnostic accuracy, increasing AUC from 0.65 to 0.81 and sensitivity from 60% to 88% (Figure 2 and Figure 4). This combination achieved comparable performance to the best PSMA + sPD-L1 + sPD-1 combination (AUC 0.81 vs. 0.85) and outperformed the combination with PCA3 (AUC 0.78) (Figure 4).
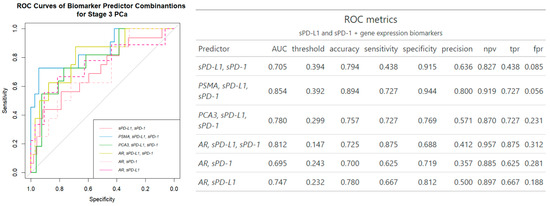
Figure 4.
ROC analysis of single gene expression and serum biomarker combinations for prediction of clinically significant PCa. Npv—negative predictive value, tpr—true positive rate, fpr—false positive rate.
3. Discussion
3.1. Significance of sPD-L1 and sPD-1 Along with mRNA of PSMA, PCA3 and AR Genes in PCa
In the context of intensive investigations on convenient biomarkers, a novel multifactorial approach that combines urine and blood biomarkers encompassing various aspects of the disease not only enhances detection but also offers a comprehensive assessment of prostate cancer. This approach highlights the potential of non-invasive liquid biopsies in improving the diagnosis and management of PCa. Building on our previous research, which identified plasma sPD-L1/sPD-1 as a potential biomarker of PCa [10], we investigated gene expression in the urine samples of the same patients. As shown in Figure 1 and Figures S1b and S2b, sPD-L1 can differentiate between clinically significant and non-significant prostate cancer and is associated with higher tumor stages (p = 0.031) and ISUP grading (p = 0.026) in PCa. Similarly, elevated sPD-L1 levels are consistently linked to larger tumors, advanced stages, and metastasis across different cancers [19,20].
In our study, significant associations were identified between PSMA (p ≤ 0.001) and PCA3 (p ≤ 0.05) expression and clinically significant prostate cancer (Figure 1 and Figure S1a), and among the three genes examined, PSMA emerged as the most reliable single biomarker for predicting clinically significant PCa with an AUC of 0.82 (Figure 2). Similarly, Rigau reported that PSMA (AUC 0.74) outperformed PSGR (AUC 0.66) and PCA3 (AUC 0.61) in predicting PCa within the PSA “gray zone” of 4–10 ng/mL [21]. Furthermore, PSMA was also linked to ISUP grading (Figure 1 and Figure S2a), indicating its potential as a biomarker for disease severity and progression. Despite AR not demonstrating any association with cancer advancement, in single-biomarker assessment, it exhibited higher diagnostic accuracy (0.76 vs. 0.59) and specificity (0.81 vs. 0.48) than all three urine biomarkers combined (Figure 2 and Figure 3). Comparative analysis with other studies also suggests the involvement of PSMA, PCA3, and AR genes in prognosis and prediction of PCa. Blood PSMA-based biomarkers have been linked to malignancy risk [22] and predicted worse survival rates in metastatic PCa [23]. Higher PSMA expression correlated with advanced tumor stages and grades in biopsies and prostatectomy specimens [24]. Urine exosomal PSMA showed high diagnostic accuracy for significant PCa, correlating strongly with Gleason scores [25]. Similarly, PCA3 scores have been associated with tumor aggressiveness [26], higher Gleason scores [15,27] and advanced clinical stages [27]. Moreover, various non-coding RNAs have been shown to influence prostate cancer progression by modulating AR signaling, highlighting their potential as biomarkers and therapeutic targets [28].
Although studies have demonstrated the utility of monitoring RNA transcripts from PSMA, PCA3, and AR genes for prostate cancer diagnosis, relying solely on these biomarkers may be limiting. These biomarkers, while associated with disease progression, may not fully capture the multifaceted nature of prostate cancer, including its clinical heterogeneity. As a result, important aspects of the disease, such as its diverse pathways, could remain undetected.
3.2. Combinations of Plasma sPD-L1/sPD-1 with mRNA of PSMA, PCA3 and AR Genes in PCa
The combination of several different biomarkers has been shown to be a promising approach to improve PCa diagnosis [29,30]. In our study, the combination of all three mRNA expressions did not improve the prediction of clinically significant prostate cancer (AUC 0.74) compared to using PSMA and PCA3 alone (AUC 0.82 and 0.75, respectively) (Figure 2 and Figure 3). However, adding sPD-L1 to the triple gene expression panel significantly enhanced the model’s performance. This resulted in a diagnostic accuracy of 0.96, an AUC of 0.94, and an increase in specificity from 48% to 100%, as shown in Figure 3. The composition of three genes along with sPD-1 did not improve the diagnostic efficacy (Figure 3). Such a multifaceted approach, combining mRNA expression analysis of PCA3, PSMA, and AR genes with sPD-L1 levels, provides a comprehensive understanding of prostate cancer’s characteristics. Together, PSMA, PCA3, and AR, which play pivotal roles in prostate cancer development, represent key aspects of tumor biology, such as cancer progression [12,14] and androgen-dependent growth [16,17]. When integrated with sPD-L1 levels, indicative of immune evasion [9], these biomarkers collectively may offer an in-depth perspective on tumor biology, immune response dynamics, and the heterogeneity of prostate cancer, supporting improved diagnostic and therapeutic strategies. sPD-L1 has emerged as a promising biomarker for various cancers, including gastric [31] and lung cancers [32]. These findings highlight sPD-L1’s broader applicability across cancers, making it valuable for diagnostics and treatment monitoring, due to its direct involvement in immune suppression [33], correlation with tumor burden, aggressiveness [34] and consistent association with clinical outcomes [8,35,36]. In contrast, sPD-1 primarily reflects immune activation; however, high pretherapeutic sPD-1 levels suggest worse prognosis [9,37]. Previous studies have described correlations rather than combinations involving sPD-L1 and sPD-1. sPD-L1 is linked to neutrophil-to-lymphocyte ratio in advanced cancers [36]. Higher levels are linked to low hemoglobin and albumin and elevated C-reactive protein in gastric cancer [38]. In pancreatic cancer, combining sPD-L1/PD-L2/B7-H5/CA19-9 improves diagnostic sensitivity, though sPD-1 did not add significance [39]. sPD-1 and sPD-L1 levels together indicated treatment outcomes in PD-1 blockade therapy as well [40,41].
The combination of three mRNA transcripts along with sPD-L1 demonstrated the strongest distinction of clinically significant PCa cases among all biomarker combinations tested (Figure 3). Furthermore, combination of urinary sediment mRNA and circulating molecules (AR, sPD-L1, sPD-1), showed the most significant improvement over other biomarkers, highlighting its potential; the mRNA of urinary AR provides insights into the androgen receptor pathway, which is implicated in PCa development and progression [42,43]. Meanwhile, plasma sPD-L1 and PD-1 levels potentially reflect the tumor’s immune microenvironment [9,37]. Androgen receptor signaling has been found to affect the expression of PD-L1 in prostate cancer, with AR activation linked to higher PD-L1 levels [44,45]. Additionally, scores for AR activity were significantly positively correlated with PD-1 methylation, resulting in an association with significantly reduced BCR (biochemical recurrence)-free survival after radical prostatectomy [46], suggesting an AR influence on the PD-L1/PD-1 axis. To analyze this promising combination in more detail, the influence of each soluble molecule was examined individually. Notably, while sPD-L1 and sPD-1 together, along with PSMA and PCA3, each showed a 3-unit increase in AUC (Figure 2 and Figure 4), even single sPD-1 combined with AR demonstrated the ability to increase AUC with a 5-unit improvement from 0.65 to 0.70 (Figure 4).
This study serves as an initial exploration of combining sPD-1 with a non-sPD-L1 biomarker across multiple cancers, demonstrating that incorporating sPD-1 has the potential to further enhance the diagnostic capabilities of the AR biomarker. A diagnostic panel combining AR with sPD-L1 and sPD-1 may offer potential economic benefits and practical applicability for implementation. These findings require further investigation in larger cohorts and hold the potential to advance understanding of the mechanistic interplay between AR and sPD-L1/sPD-1 signaling. Integrating blood and urine biomarkers together significantly improves PCa detection and is supported by commercially available tests. SelectMDx Urine Test, including DLX1, HOXC6, KLK3(PSA) and other parameters achieved an AUC of 0.85 with 93% sensitivity and 47% specificity [47], while the Michigan Prostate Score (MiPS), consisting of urine mRNA of T2-ERG and PCA3 with serum PSA also outperformed the regular PSA test [48]. Additionally, scientific studies confirm the effectiveness of combining biomarkers obtained from different body fluids. Urinary exosomal PCA3 and PSMA with serum PSA and PI-RADS achieved higher AUC than PSA alone [49], as well as urinary PCA3 enhanced diagnostic performance of PSA in high-risk populations [50].
4. Materials and Methods
4.1. Characteristics of PCa Population
In a cohort of PCa patients evaluated for soluble PD-L1 and PD-1 levels in our previous research [10], gene expression was additionally examined in 72 cases to further assess their diagnostic value in this study. Four cases were removed due to outlier values in gene expression; thus, the study included 68 PCa patients. The PCa cases were divided into clinically significant and not clinically significant PCa groups where clinical significance was defined as cases with pathological stage pT3, following the high-risk prostate cancer criteria summarized in the review by Wilkins [51]. These patients were deemed to have an unfavorable PCa risk. The clinical characteristics of the PCa group are provided in Table 1.

Table 1.
Clinical characteristics of the PCa group.
The inclusion and exclusion criteria are well described in the paper by Bosas, clearly outlining the participant selection process [52].
4.2. Blood Sampling
The blood sampling of sPD-L1 and sPD-1 is thoroughly detailed in our previous paper [10].
4.3. Urine Sampling
The urine sampling is described in detail in previous research [53].
4.4. Analysis of Soluble PD-L1 and PD-1
Commercially available ELISA kits for PD-L1 and PD-1 were used to measure the soluble forms of both proteins in plasma, following the manufacturer’s instructions (Invitrogen, Thermo Fisher Scientific, Vienna, Austria). sPD-L1 and sPD-1 control samples were included in each kit at known concentrations. The optical density was measured using plate reader BioTek Elx800 TM (BIO-Tek Instruments, Inc., Winooski, VT, USA) at 450 nm. Two duplicates of each sample were measured. Blanks and standards were assayed as directed by manufacturers.
4.5. Analysis of mRNA Expression of PCA3, PSMA and AR Genes
Total RNA from washed urine sediment samples was extracted using the TRIzol Reagent (Invitrogen, Thermo Fisher Scientific (TFS), Carsbad, CA, USA) following the manufacturer’s protocol. The RNA concentration and purity were assessed using a Nanodrop 2000 spectrophotometer (Thermo Scientific, Wilmington, DE, USA). The RNA samples were stored at −80 °C until the copy DNA (cDNA) synthesis step. Two-Step RT-qPCR was used to assay AR, PSMA, and PCA3 mRNA relative quantities in the urine sediment samples. The Maxima First Stand cDNA Synthesis Kit for RT-qPCR with dsDNase (TFS, Vilnius, Lithuania) and the Maxima SYBR Green qPCR Master Mix (2X), with separate ROX vial (TFS, Vilnius, Lithuania), were used for two-step RT-qPCR following the manufacturer’s protocols. The qPCR reactions were performed on QuantStudio 5 Real-Time PCR System (Applied Biosystems, TFS, Singapore). RT-qPCR data pre-processing was performed on QuantStudio Design & Analysis software v1.4.3 (Applied biosystems, TFS, Singapore). The quantification cycle (Ct) values were reported using the automatic threshold baseline. Ct values <35 cycles were removed from subsequent analysis. For each sample, melt–curve analysis was performed to evaluate the amplicon size. The initial Ct values normalized to the HPRT1 gene expression using log22−ΔCt and then divided by the PSA gene expression; these normalized relative expression values were used in further statistical data analysis.
4.6. Statistical Analysis
Statistical analysis and data visualization was performed on Python version 3.11.5 (Python Software Foundation) and R version 4.3.1 [54,55] software. Data normalcy was determined using Shapiro–Wilk W tests. Cases exceeding three interquartile ranges were deemed outliers and removed from all statistical analysis. Associations between two independent samples were tested using Welch’s t test or Mann–Whitney U test as appropriate. Receiver operating characteristic curve (ROC) analysis [56] together with logistic regression was utilized to measure biomarker and feature combination accuracy to predict clinically significant PCa. In each ROC curve, continuous biomarker values were used in the analysis. For each ROC curve, the best threshold value was determined using the Youden method. Results were considered significant when p ≤ 0.05.
5. Conclusions
Our results demonstrate that the combination of multiple biomarkers presents new opportunities for liquid biopsies to identify effective combinations that reflect the multifactorial nature of the disease. The inclusion of plasma sPD-L1 and sPD-1 in a diagnostic panel, together with urinary PSMA, PCA3, and AR mRNA transcripts, has the potential to significantly improve PCa diagnostics. Urine and plasma are easily accessible biofluids, allowing for less invasive and repeatable sampling and longitudinal monitoring and potentially reducing unnecessary biopsies [57]. Future efforts should focus on refining multimodal liquid-based data panels for more precise cancer management, while also emphasizing the adoption of commonly used, cost-effective laboratory methods to improve accessibility.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/ijms26020704/s1.
Limitations of the Study
There were some limitations in the current study. First, this is a single-center study, with a relatively small study cohort that does not include healthy subjects. Second, the cohort does not include cases with high Gleason grades. Third, the small cohort size may influence test metrics such as NPV.
Author Contributions
Conceptualization: M.Ž., I.V., R.S. and V.P.; Methodology: M.Ž., I.V., Ž.S., P.B., N.D. and A.M.; Validation: M.Ž., I.V., R.S. and V.P.; Formal analysis: I.V., Ž.S. and M.Ž.; Investigation: M.Ž., I.V., Ž.S., P.B., N.D. and A.M.; Data curation: M.Ž., I.V., Ž.S., P.B., N.D. and A.M.; Writing—original draft preparation: M.Ž. and I.V.; Writing—review and editing R.S. and V.P.; Visualization M.Ž., I.V., R.S. and V.P.; Supervision: R.S. and V.P.; Project administration: V.P. All authors have read and agreed to the published version of the manuscript.
Funding
The present study was supported by the National Cancer Institute of Lithuania’s scientific fund and supported in part by the Research Council of Lithuania as a grant for MZ PhD studies.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the Regional Review Board (Vilnius, Lithuania, 158200-17-928-442). All research methods were carried out in accordance with the relevant Lithuanian national guidelines and regulations.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to protection of participant’s privacy.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
sPD-L1—programmed death ligand; sPD-1—programmed death; PSMA—prostate-specific membrane antigen; PCA3—prostate cancer antigen 3; AR—androgen receptor; PCa—prostate cancer; AUC—Area Under Curve; PSA—prostate specific antigen; ISUP—International Society of Urological Pathology; ELISA—Enzyme-Linked Immunosorbent Assay; ROC—Receiver Operating Characteristic.
References
- Bergengren, O.; Pekala, K.R.; Matsoukas, K.; Fainberg, J.; Mungovan, S.F.; Bratt, O.; Brawley, O.; Luckenbaugh, A.N.; Mucci, L.; Morgan, M.T.; et al. 2022 Update on Prostate Cancer Epidemiology and Risk Factors—A Systematic Review. Eur. Urol. 2023, 84, 191–206. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Cancer statistics for the year 2020: An overview. Int. J. Cancer 2021, 149, 778–789. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Haffner, M.C.; Zwart, W.; Roudier, M.P.; True, L.D.; Nelson, W.G.; Epstein, J.I.; Epstein, J.I.; De Marzo, A.M.; Nelson, P.S.; Yegnasubramanian, S. Genomic and phenotypic heterogeneity in prostate cancer. Nat. Rev. Urol. 2021, 18, 79–92. [Google Scholar] [CrossRef]
- Sekhoacha, M.; Riet, K.; Motloung, P.; Gumenku, L.; Adegoke, A.; Mashele, S. Prostate Cancer Review: Genetics, Diagnosis, Treatment Options, and Alternative Approaches. Molecules 2022, 27, 5730. [Google Scholar] [CrossRef]
- Hennigan, S.T.; Trostel, S.Y.; Terrigino, N.T.; Voznesensky, O.S.; Schaefer, R.J.; Whitlock, N.C.; Wilkinson, S.; Carrabba, N.V.; Atway, R.; Shema, S.; et al. Low Abundance of Circulating Tumor DNA in Localized Prostate Cancer. JCO Precis. Oncol. 2019, 3, 1–13. [Google Scholar] [CrossRef]
- Bailly, C.; Thuru, X.; Quesnel, B. Soluble Programmed Death Ligand-1 (sPD-L1): A Pool of Circulating Proteins Implicated in Health and Diseases. Cancers 2021, 13, 3034. [Google Scholar] [CrossRef]
- Wei, W.; Xu, B.; Wang, Y.; Wu, C.; Jiang, J.; Wu, C. Prognostic significance of circulating soluble programmed death ligand-1 in patients with solid tumors: A meta-analysis. Medicine 2018, 97, e9617. [Google Scholar] [CrossRef]
- Khan, M.; Zhao, Z.; Arooj, S.; Fu, Y.; Liao, G. Soluble PD-1: Predictive, Prognostic, and Therapeutic Value for Cancer Immunotherapy. Front. Immunol. 2020, 11, 587460. [Google Scholar] [CrossRef] [PubMed]
- Zvirble, M.; Survila, Z.; Bosas, P.; Dobrovolskiene, N.; Mlynska, A.; Zaleskis, G.; Jursenaite, J.; Characiejus, D. Prognostic significance of soluble PD-L1 in prostate cancer. Front. Immunol. 2024, 15, 1401097. [Google Scholar] [CrossRef]
- Han, S.; Woo, S.; Kim, Y.J.; Suh, C.H. Impact of 68 Ga-PSMA PET on the Management of Patients with Prostate Cancer: A Systematic Review and Meta-analysis. Eur. Urol. 2018, 74, 179–190. [Google Scholar] [CrossRef]
- Bravaccini, S.; Puccetti, M.; Bocchini, M.; Ravaioli, S.; Celli, M.; Scarpi, E.; De Giorgi, U.; Tumedi, M.M.; Raulli, G.; Cardinale, L.; et al. PSMA expression: A potential ally for the pathologist in prostate cancer diagnosis. Sci. Rep. 2018, 8, 4254. [Google Scholar] [CrossRef]
- Fujita, K.; Nonomura, N. Urinary biomarkers of prostate cancer. Int. J. Urol. 2018, 25, 770–779. [Google Scholar] [CrossRef]
- Lemos, A.E.G.; Matos, A.d.R.; Ferreira, L.B.; Gimba, E.R.P. The long non-coding RNA PCA3: An update of its functions and clinical applications as a biomarker in prostate cancer. Oncotarget 2019, 10, 6589–6603. [Google Scholar] [CrossRef]
- Chunhua, L.; Zhao, H.; Zhao, H.; Lu, Y.; Wu, J.; Gao, Z.; Li, G.; Zhang, Y.; Wang, K. Clinical Significance of Peripheral Blood PCA3 Gene Expression in Early Diagnosis of Prostate Cancer. Transl. Oncol. 2018, 11, 628–632. [Google Scholar] [CrossRef]
- Fujita, K.; Nonomura, N. Role of Androgen Receptor in Prostate Cancer: A Review. World J. Men’s Health 2019, 37, 288. [Google Scholar] [CrossRef] [PubMed]
- Aurilio, G.; Cimadamore, A.; Mazzucchelli, R.; Lopez-Beltran, A.; Verri, E.; Scarpelli, M.; Massari, F.; Cheng, L.; Santoni, M.; Montironi, R. Androgen Receptor Signaling Pathway in Prostate Cancer: From Genetics to Clinical Applications. Cells 2020, 9, 2653. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.J.; Lee, Y.H.; Koo, K.C. Current Status and Future Perspectives of Androgen Receptor Inhibition Therapy for Prostate Cancer: A Comprehensive Review. Biomolecules 2021, 11, 492. [Google Scholar] [CrossRef] [PubMed]
- Chivu-Economescu, M.; Herlea, V.; Dima, S.; Sorop, A.; Pechianu, C.; Procop, A.; Kitahara, S.; Necula, L.; Matei, L.; Dragu, D.; et al. Soluble PD-L1 as a diagnostic and prognostic biomarker in resectable gastric cancer patients. Gastric Cancer 2023, 26, 934–946. [Google Scholar] [CrossRef]
- Vikerfors, A.; Davidsson, S.; Frey, J.; Jerlström, T.; Carlsson, J. Soluble PD-L1 in Serum and Urine in Urinary Bladder Cancer Patients. Cancers 2021, 13, 5841. [Google Scholar] [CrossRef]
- Rigau, M.; Ortega, I.; Mir, M.C.; Ballesteros, C.; Garcia, M.; Llauradó, M.; Colás, E.; Pedrola, N.; Montes, M.; Sequeiros, T.; et al. A three-gene panel on urine increases PSA specificity in the detection of prostate cancer. Prostate 2011, 71, 1736–1745. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, M.M.; Abdel Hamid, F.F.; Abdelgawad, I.; Ismail, A.; Malash, I.; Ibrahim, D.M. Diagnostic Efficacy of PSMA and PSCA mRNAs Combined to PSA in Prostate Cancer Patients. Asian Pac. J. Cancer Prev. 2023, 2, 223–229. [Google Scholar] [CrossRef]
- Gupta, S.; Halabi, S.; Yang, Q.; Roy, A.; Tubbs, A.; Gore, Y.; George, D.J.; Nanus, D.M.; Antonarakis, E.S.; Danila, D.C.; et al. PSMA-positive Circulating Tumor Cell Detection and Outcomes with Abiraterone or Enzalutamide Treatment in Men with Metastatic Castrate-resistant Prostate Cancer. Clin. Cancer Res. 2023, 29, 1929–1937. [Google Scholar] [CrossRef]
- Hupe, M.C.; Philippi, C.; Roth, D.; Kümpers, C.; Ribbat-Idel, J.; Becker, F.; Joerg, V.; Duensing, S.; Lubczyk, V.H.; Kirfel, J.; et al. Expression of Prostate-Specific Membrane Antigen (PSMA) on Biopsies Is an Independent Risk Stratifier of Prostate Cancer Patients at Time of Initial Diagnosis. Front. Oncol. 2018, 8, 623. [Google Scholar] [CrossRef]
- Wang, C.-B.; Chen, S.-H.; Zhao, L.; Jin, X.; Chen, X.; Ji, J.; Mo, Z.; Wang, F. Urine-derived exosomal PSMA is a promising diagnostic biomarker for the detection of prostate cancer on initial biopsy. Clin. Transl. Oncol. 2023, 25, 758–767. [Google Scholar] [CrossRef] [PubMed]
- Merola, R.; Tomao, L.; Antenucci, A.; Sperduti, I.; Sentinelli, S.; Masi, S.; Mandoj, C.; Orlandi, G.; Papalia, R.; Guaglianone, S.; et al. PCA3 in prostate cancer and tumor aggressiveness detection on 407 high-risk patients: A National Cancer Institute experience. J. Exp. Clin. Cancer Res. 2015, 34, 15. [Google Scholar] [CrossRef]
- Wei, W.; Leng, J.; Shao, H.; Wang, W. High PCA3 scores in urine correlate with poor-prognosis factors in prostate cancer patients. Int. J. Clin. Exp. Med. 2015, 8, 16606–16612. [Google Scholar] [PubMed]
- Yang, Y.; Liu, K.Y.; Liu, Q.; Cao, Q. Androgen Receptor-Related Non-coding RNAs in Prostate Cancer. Front. Cell Dev. Biol. 2021, 9, 660853. [Google Scholar] [CrossRef] [PubMed]
- Neves, A.F.; Araújo, T.G.; Biase, W.K.F.S.; Meola, J.; Alcântara, T.M.; Freitas, D.G.; Goulart, L.R. Combined Analysis of Multiple MRNA Markers by RT-PCR Assay for Prostate Cancer Diagnosis. Clin. Biochem. 2008, 41, 1191–1198. [Google Scholar] [CrossRef]
- Mao, Z.; Ji, A.; Yang, K.; He, W.; Hu, Y.; Zhang, Q.; Zhang, D.; Xie, L. Diagnostic Performance of PCA3 and HK2 in Combination with Serum PSA for Prostate Cancer. Medicine 2018, 97, e12806. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Bu, Z.; Liu, X.; Zhang, L.; Li, Z.; Wu, A.; Wu, X.; Cheng, X.; Xing, X.; Du, H.; et al. Level of circulating PD-L1 expression in patients with advanced gastric cancer and its clinical implications. Chin. J. Cancer Res. 2014, 26, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Wang, C.; Wang, Y.; Dai, L. Soluble PD-L1 as a predictive biomarker in lung cancer: A systematic review and meta-analysis. Future Oncol. 2022, 18, 261–273. [Google Scholar] [CrossRef]
- Hassounah, N.B.; Malladi, V.S.; Huang, Y.; Freeman, S.S.; Beauchamp, E.M.; Koyama, S.; Souders, N.; Martin, S.; Dranoff, G.; Wong, K.; et al. Identification and characterization of an alternative cancer-derived PD-L1 splice variant. Cancer Immunol. Immunother. 2019, 68, 407–420. [Google Scholar] [CrossRef]
- Mahoney, K.M.; Ross-Macdonald, P.; Yuan, L.; Song, L.; Veras, E.; Wind-Rotolo, M.; McDermott, D.F.; Hodi, F.S.; Choueiri, T.K.; Freeman, G.J. Soluble PD-L1 as an early marker of progressive disease on nivolumab. J. Immunother. Cancer 2022, 10, e003527. [Google Scholar] [CrossRef]
- Scirocchi, F.; Strigari, L.; Di Filippo, A.; Napoletano, C.; Pace, A.; Rahimi, H.; Botticelli, A.; Rughetti, A.; Nuti, M.; Zizzari, I.G. Soluble PD-L1 as a Prognostic Factor for Immunotherapy Treatment in Solid Tumors: Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2022, 23, 14496. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.Y.; Kim, S.; Keam, B.; Kim, T.M.; Kim, D.-W. Soluble PD-L1 is a predictive and prognostic biomarker in advanced cancer patients who receive immune checkpoint blockade treatment. Sci. Rep. 2021, 11, 19712. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Lang, J. Soluble PD-1 and PD-L1: Predictive and prognostic significance in cancer. Oncotarget 2017, 8, 97671–97682. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Sasaki, T.; Kano, M.; Shiraishi, T.; Suito, H.; Murakami, K.; Toyozumi, T.; Otsuka, R.; Kinoshita, K.; Iida, S.; et al. Soluble PD-L1 reflects cachexia status in patients with gastric cancer and is an independent prognostic marker for relapse-free survival after radical surgery. Mol. Clin. Oncol. 2023, 18, 39. [Google Scholar] [CrossRef]
- Wu, W.; Xia, X.; Cheng, C.; Niu, L.; Wu, J.; Qian, Y. Serum Soluble PD-L1, PD-L2, and B7-H5 as Potential Diagnostic Biomarkers of Human Pancreatic Cancer. Clin. Lab. 2021, 67, 1512–1519. [Google Scholar] [CrossRef]
- Kurosaki, T.; Chamoto, K.; Suzuki, S.; Kanemura, H.; Mitani, S.; Tanaka, K.; Kawakami, H.; Kishimoto, Y.; Haku, Y.; Ito, K.; et al. The combination of soluble forms of PD-1 and PD-L1 as a predictive marker of PD-1 blockade in patients with advanced cancers: A multicenter retrospective study. Front. Immunol. 2023, 14, 1325462. [Google Scholar] [CrossRef]
- Ugurel, S.; Schadendorf, D.; Horny, K.; Sucker, A.; Schramm, S.; Utikal, J.; Pföhler, C.; Herbst, R.; Schilling, B.; Blank, B.; et al. Elevated baseline serum PD-1 or PD-L1 predicts poor outcome of PD-1 inhibition therapy in metastatic melanoma. Ann. Oncol. 2020, 31, 144–152. [Google Scholar] [CrossRef]
- Messner, E.A.; Steele, T.M.; Tsamouri, M.M.; Hejazi, N.; Gao, A.C.; Mudryj, M.; Ghosh, P.M. The Androgen Receptor in Prostate Cancer: Effect of Structure, Ligands and Spliced Variants on Therapy. Biomedicines 2020, 8, 422. [Google Scholar] [CrossRef] [PubMed]
- Jacob, A.; Raj, R.; Allison, D.B.; Myint, Z.W. Androgen Receptor Signaling in Prostate Cancer and Therapeutic Strategies. Cancers 2021, 13, 5417. [Google Scholar] [CrossRef]
- Gevensleben, H.; Dietrich, D.; Golletz, C.; Steiner, S.; Jung, M.; Thiesler, T.; Majores, M.; Stein, J.; Uhl, B.; Müller, S.; et al. The Immune Checkpoint Regulator PD-L1 Is Highly Expressed in Aggressive Primary Prostate Cancer. Clin. Cancer Res. 2016, 22, 1969–1977. [Google Scholar] [CrossRef]
- Li, Y.; Huang, Q.; Zhou, Y.; He, M.; Chen, J.; Gao, Y.; Wang, X. The Clinicopathologic and Prognostic Significance of Programmed Cell Death Ligand 1 (PD-L1) Expression in Patients with Prostate Cancer: A Systematic Review and Meta-Analysis. Front. Pharmacol. 2019, 9, 1494. [Google Scholar] [CrossRef]
- Goltz, D.; Gevensleben, H.; Dietrich, J.; Ellinger, J.; Landsberg, J.; Kristiansen, G.; Dietrich, D. Promoter methylation of the immune checkpoint receptor PD-1 (PDCD1) is an independent prognostic biomarker for biochemical recurrence-free survival in prostate cancer patients following radical prostatectomy. Oncoimmunology 2016, 5, e1221555. [Google Scholar] [CrossRef] [PubMed]
- Haese, A.; Trooskens, G.; Steyaert, S.; Hessels, D.; Brawer, M.; Vlaeminck-Guillem, V.; Ruffion, A.; Tilki, D.; Shalken, J.; Groskopf, J.; et al. Multicenter Optimization and Validation of a 2-Gene mRNA Urine Test for Detection of Clinically Significant Prostate Cancer before Initial Prostate Biopsy. J Urol. 2019, 202, 256–263. [Google Scholar] [CrossRef]
- Wang, L.; He, W.; Shi, G.; Zhao, G.; Cen, Z.; Xu, F.; Tian, W.; Zhao, X.; Mo, C. Accuracy of novel urinary biomarker tests in the diagnosis of prostate cancer: A systematic review and network meta-analysis. Front. Oncol. 2022, 12, 1048876. [Google Scholar] [CrossRef]
- Gan, J.; Zeng, X.; Wang, X.; Wu, Y.; Lei, P.; Wang, Z.; Yang, C.; Hu, Z. Effective Diagnosis of Prostate Cancer Based on mRNAs from Urinary Exosomes. Front. Med. 2022, 9, 736110. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.; Lee, C.H.; Ning, J.; Handy, B.C.; Wagar, E.A.; Meng, Q.H. Combination of Prostate Cancer Antigen 3 and Prostate-Specific Antigen Improves Diagnostic Accuracy in Men at Risk of Prostate Cancer. Arch. Pathol. Lab. Med. 2018, 142, 1106–1112. [Google Scholar] [CrossRef]
- Wilkins, L.J.; Tosoian, J.J.; Sundi, D.; Ross, A.E.; Grimberg, D.; Klein, E.A.; Chapin, B.F.; Nyame, Y.A. Surgical management of high-risk, localized prostate cancer. Nat. Rev. Urol. 2020, 17, 679–690. [Google Scholar] [CrossRef] [PubMed]
- Bosas, P.; Zaleskis, G.; Dabkevičiene, D.; Dobrovolskiene, N.; Mlynska, A.; Tikuišis, R.; Ulys, A.; Pašukoniene, V.; Jarmalaitė, S.; Jankevičius, F. Immunophenotype Rearrangement in Response to Tumor Excision May Be Related to the Risk of Biochemical Recurrence in Prostate Cancer Patients. J. Clin. Med. 2021, 10, 3709. [Google Scholar] [CrossRef] [PubMed]
- Januskevicius, T.; Sabaliauskaite, R.; Dabkeviciene, D.; Vaicekauskaite, I.; Kulikiene, I.; Sestokaite, A.; Vidrinskaite, A.; Bakavicius, A.; Jankeviscius, F.; Ulys, A.; et al. Urinary DNA as a Tool for Germline and Somatic Mutation Detection in Castration-Resistant Prostate Cancer Patients. Biomedicines 2023, 11, 761. [Google Scholar] [CrossRef] [PubMed]
- Therneau, T.M. A Package for Survival Analysis in R, version, 3.8-3; R Foundation for Statistical Computing: Vienna, Austria, 2024; Available online: https://CRAN.R-project.org/package=survival (accessed on 31 October 2024).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2023; Available online: https://www.R-project.org/ (accessed on 31 October 2024).
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Hirahata, T.; Ul Quraish, R.; Quraish, A.U.; Ul Quraish, S.; Naz, M.; Razzaq, M.A. Liquid Biopsy: A Distinctive Approach to the Diagnosis and Prognosis of Cancer. Cancer Inform. 2021, 21, 11769351221076062. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).