
Liquiritin Carbomer Gel Cold Paste Promotes Healing of Solar Dermatitis in Mice

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Results
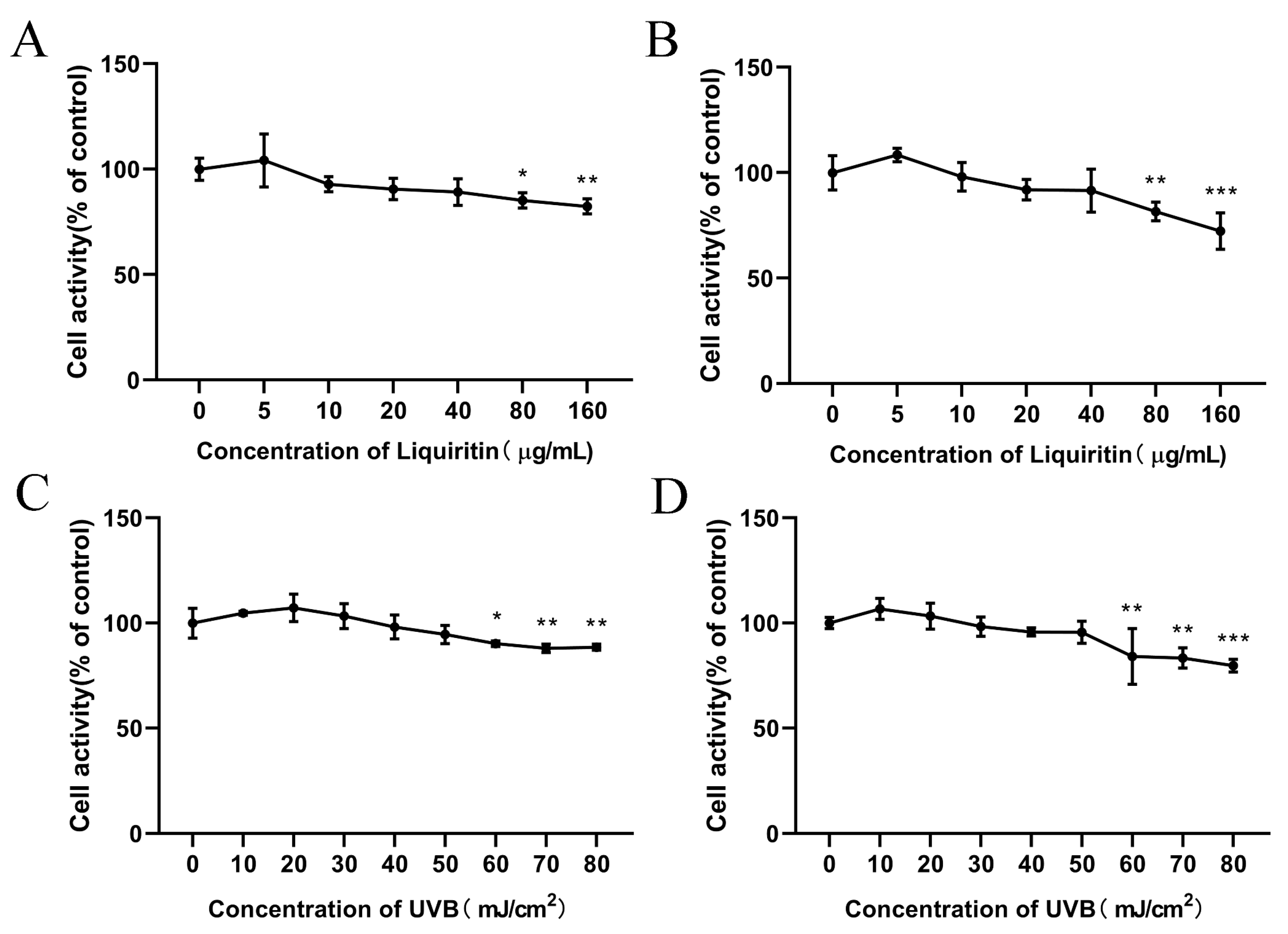
2.1. Effect of LQ and UVB on Cell Proliferation Viability
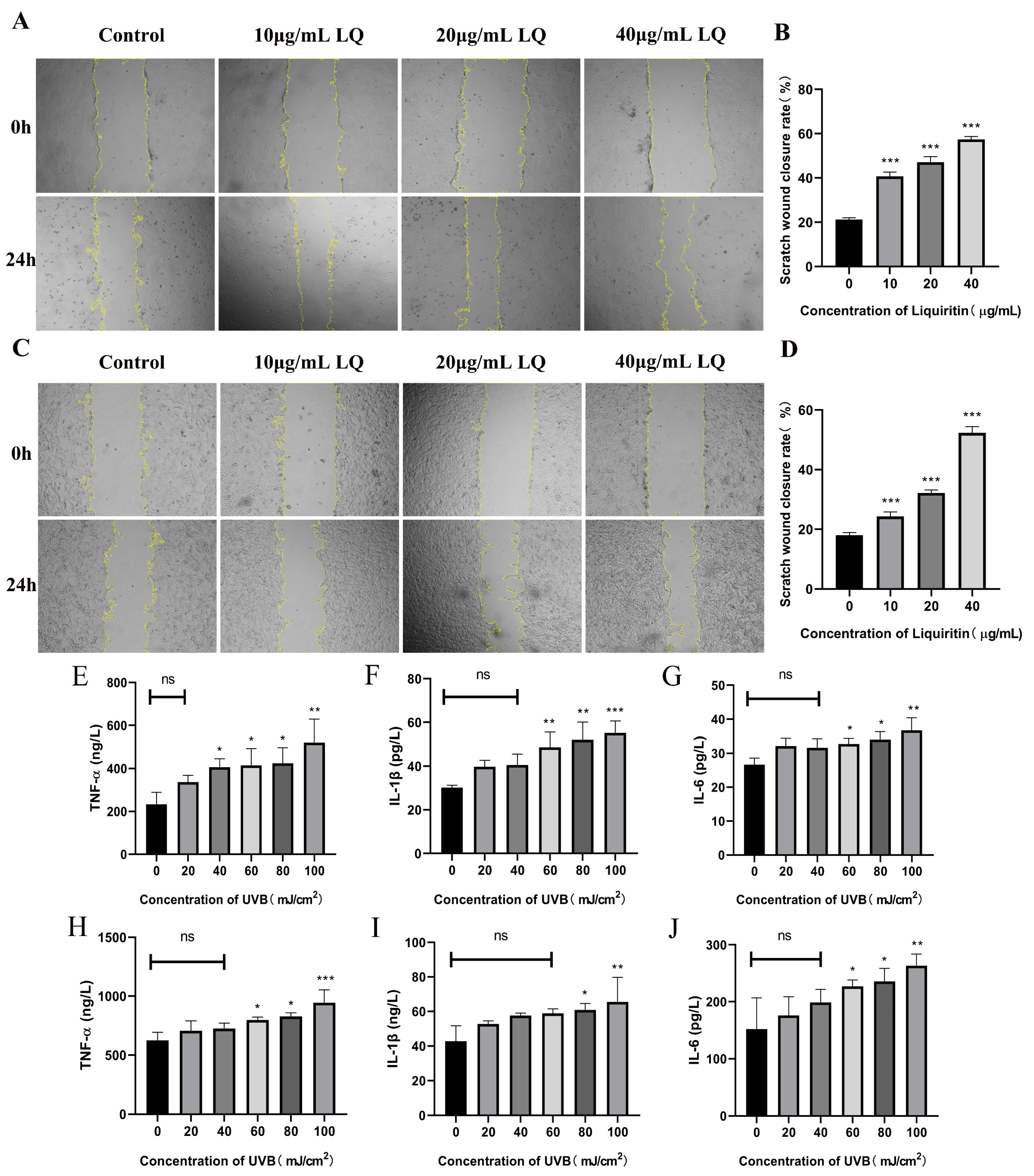
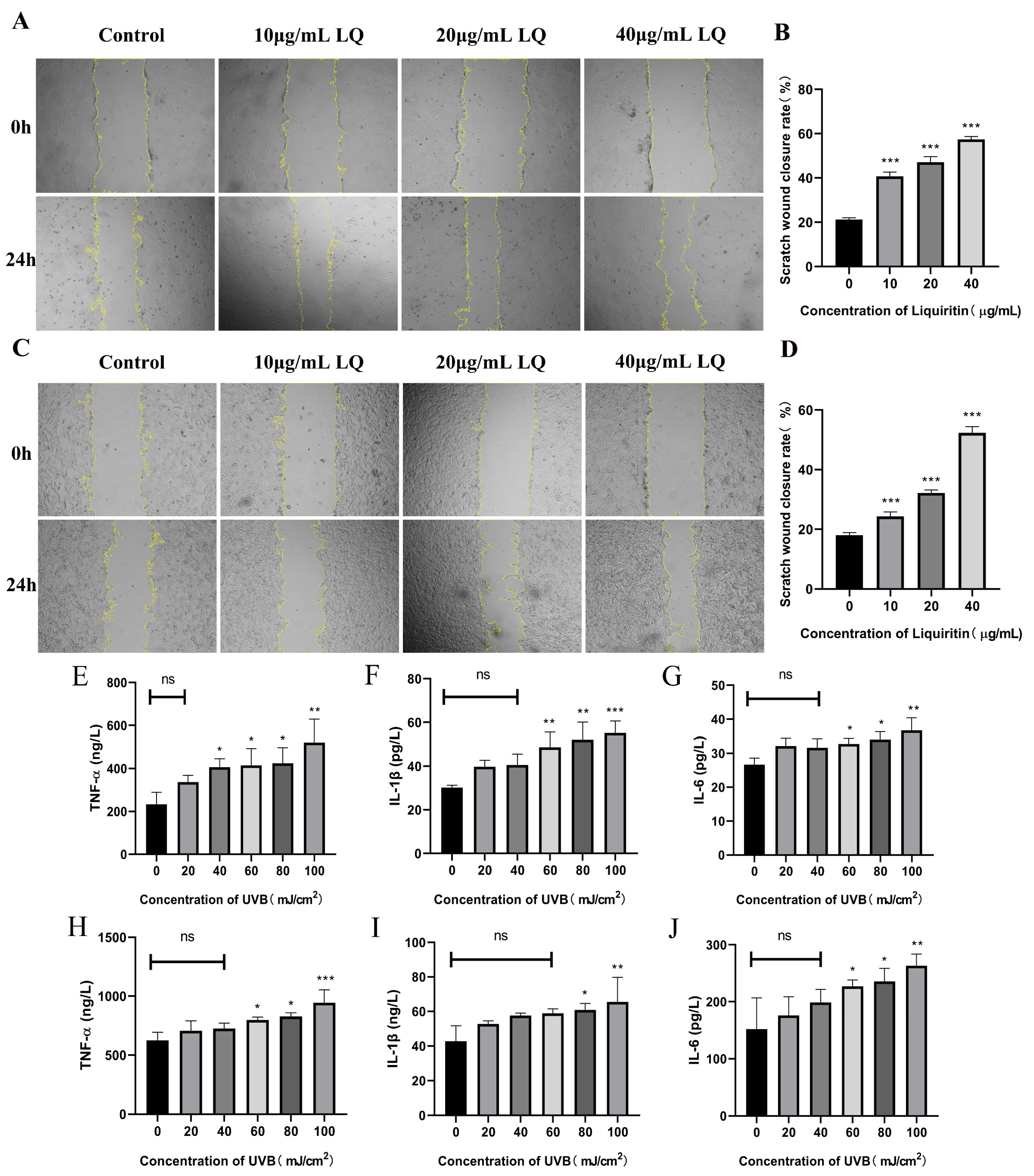
2.2. Effect of LQ on Cell Migration Capacity and UVB on Cell Secretion of Inflammatory Factors
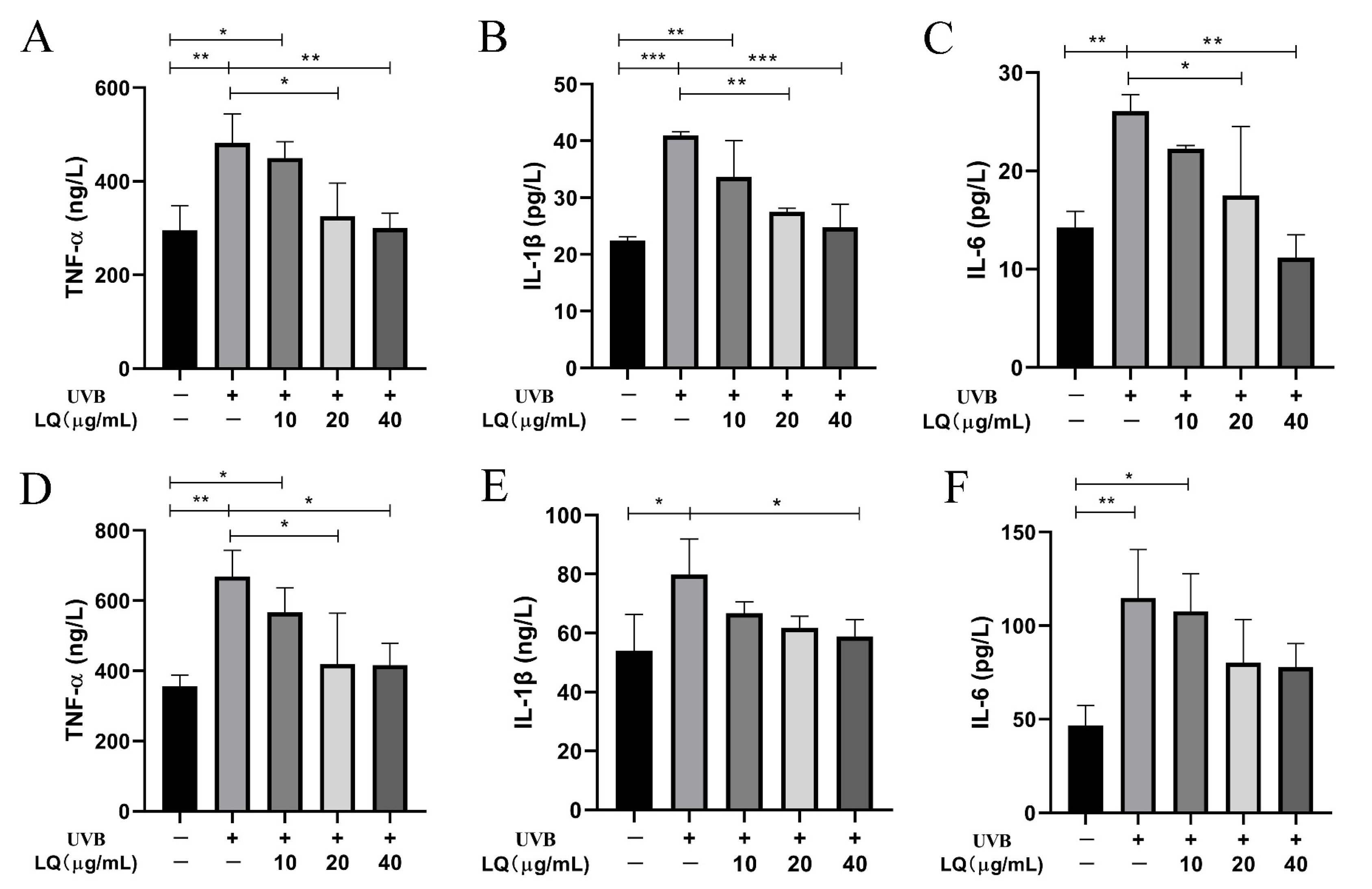
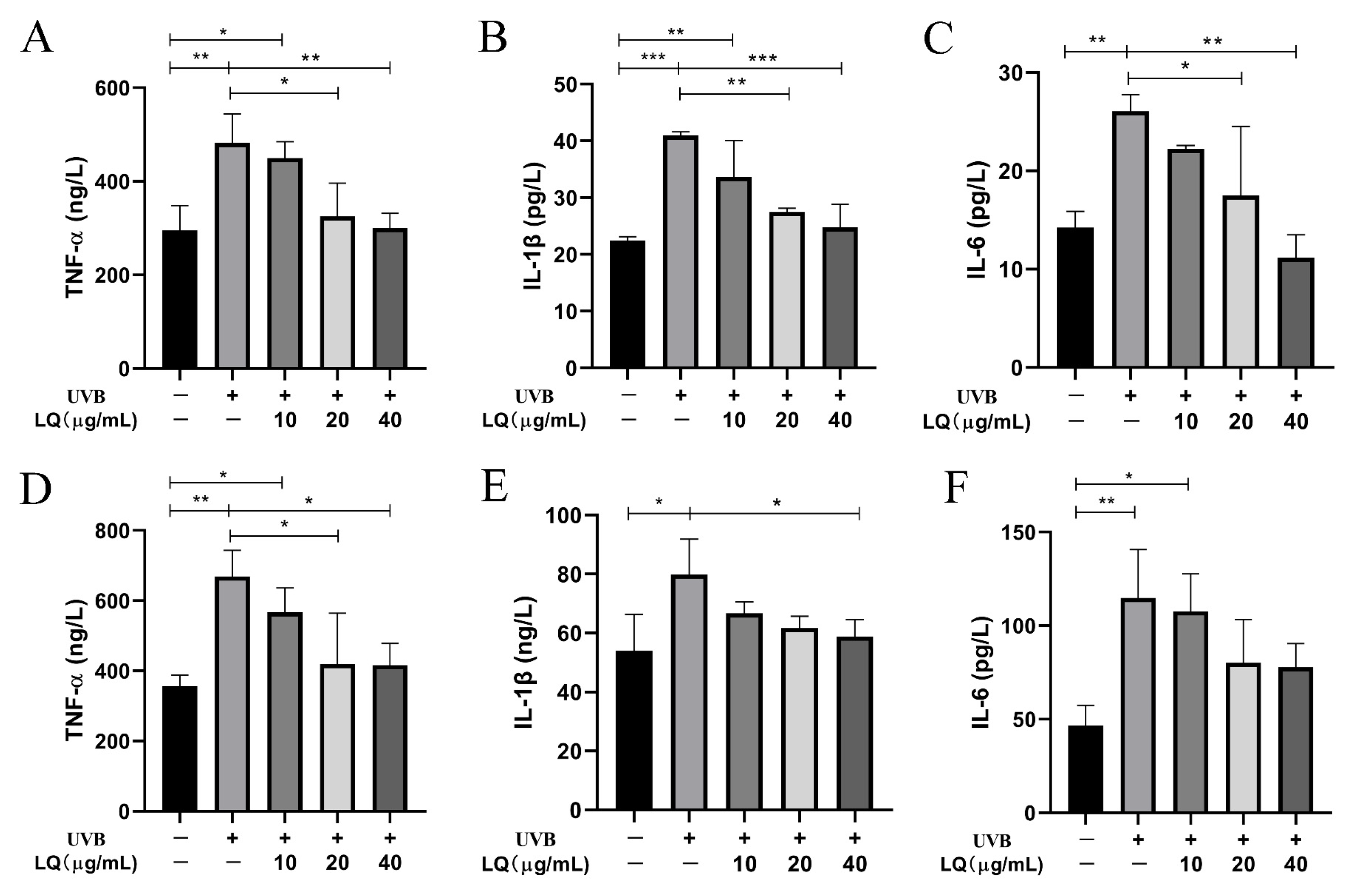
2.3. Effect of LQ on Cell Secretion of Inflammatory Factors after UVB Irradiation
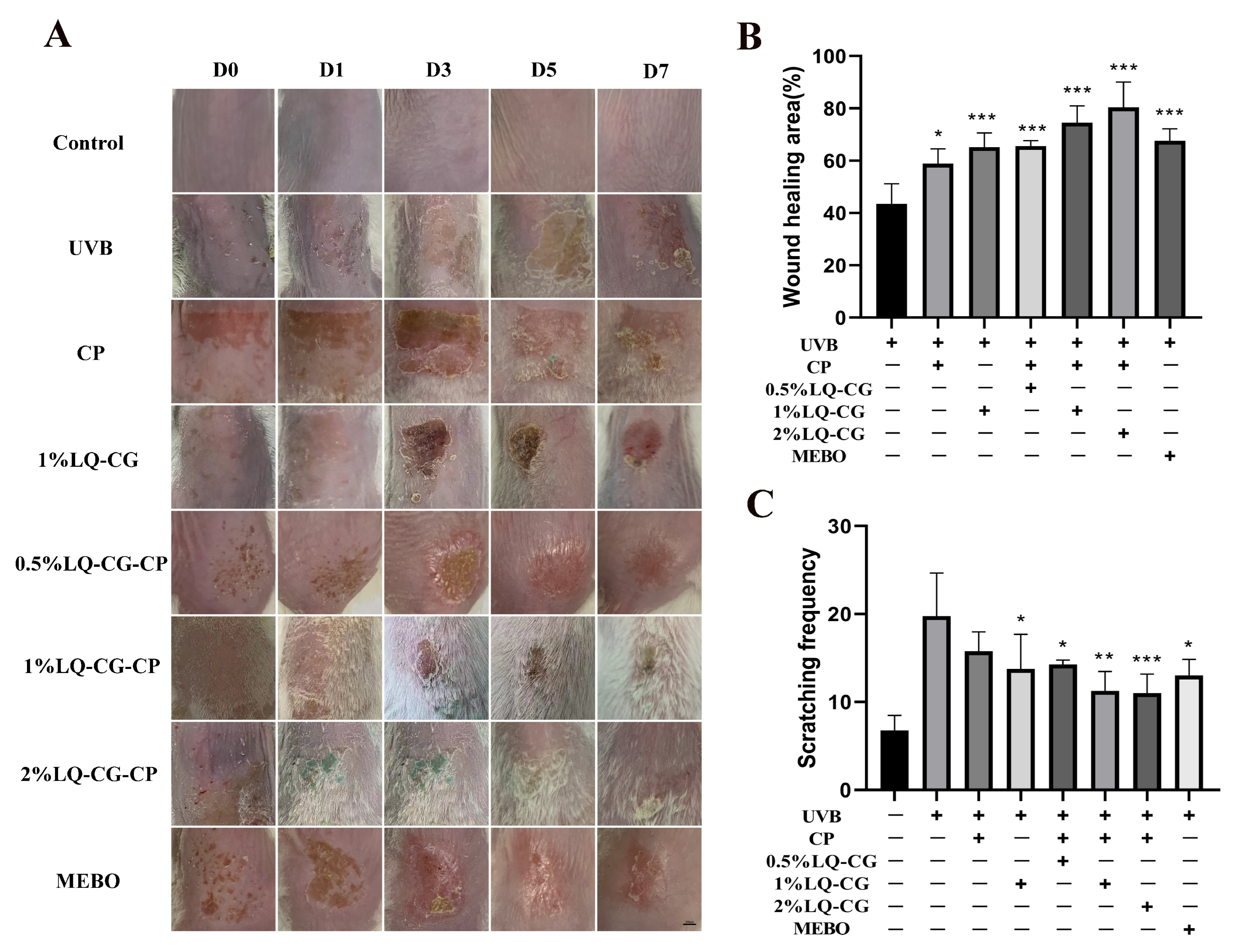
2.4. The Promoting Effect of LQ on Skin Wound Healing and Its Ability to Alleviate Itching Symptoms in Mice
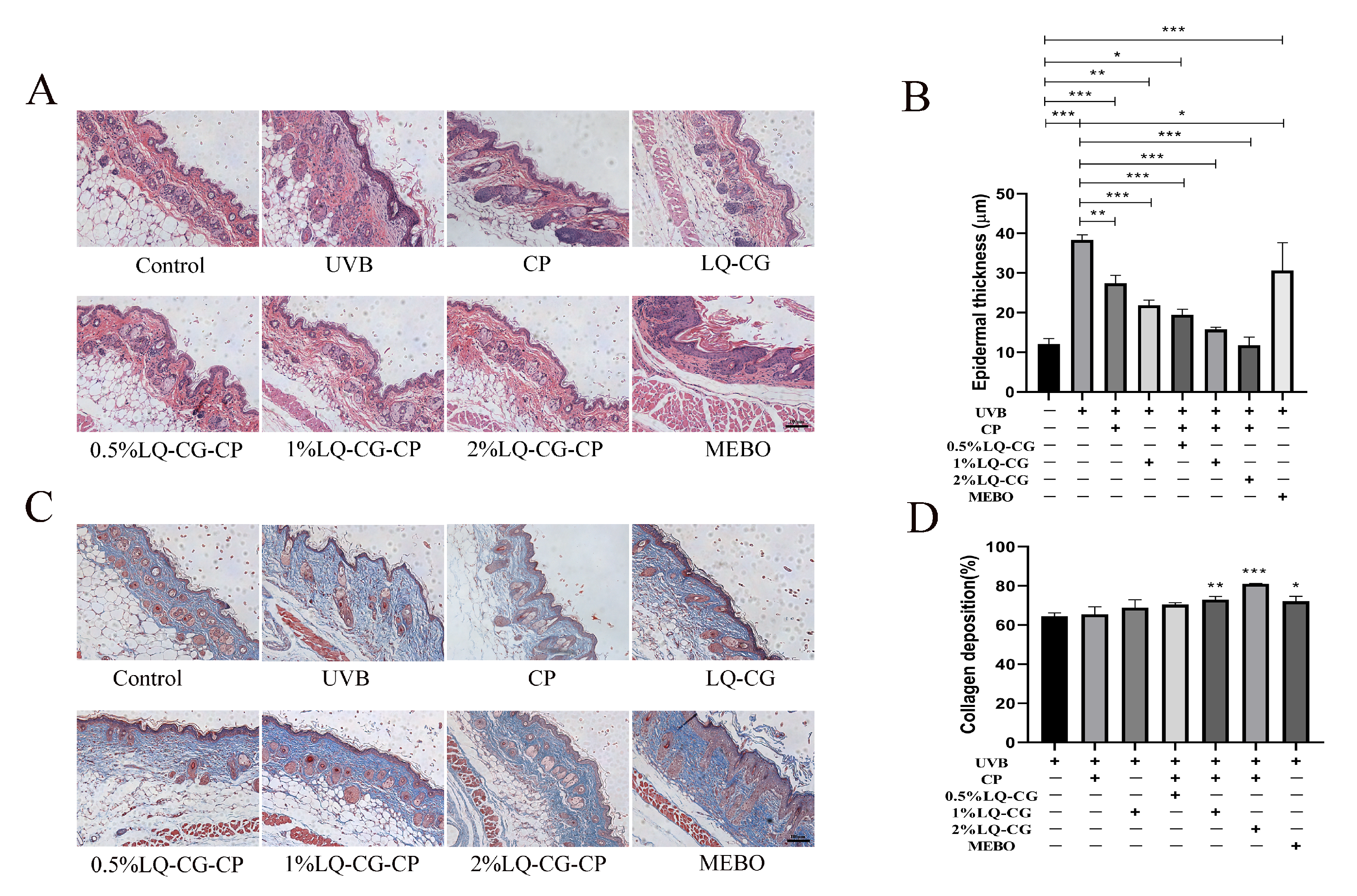
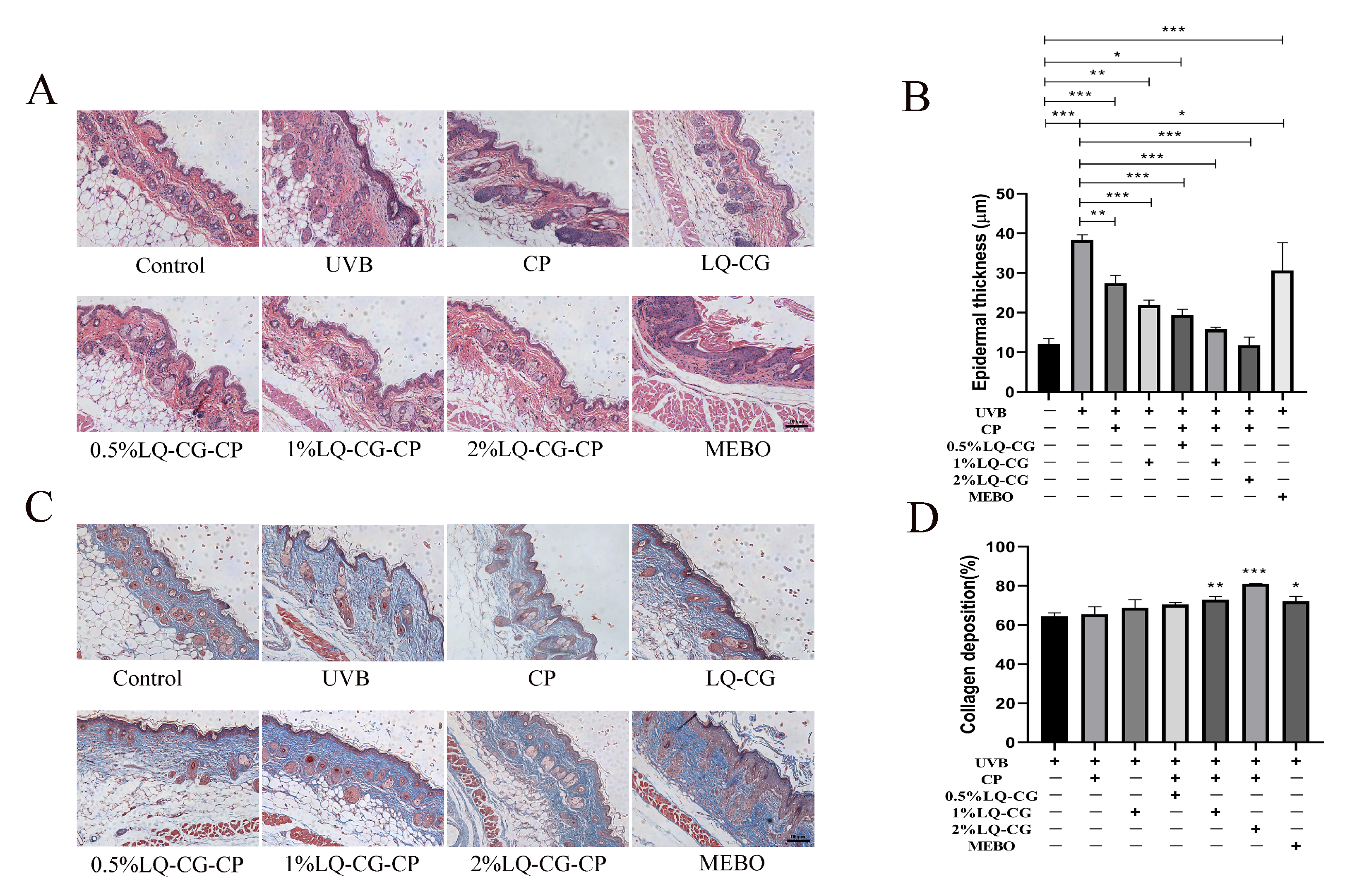
2.5. Staining Results of Wound Skin Tissues
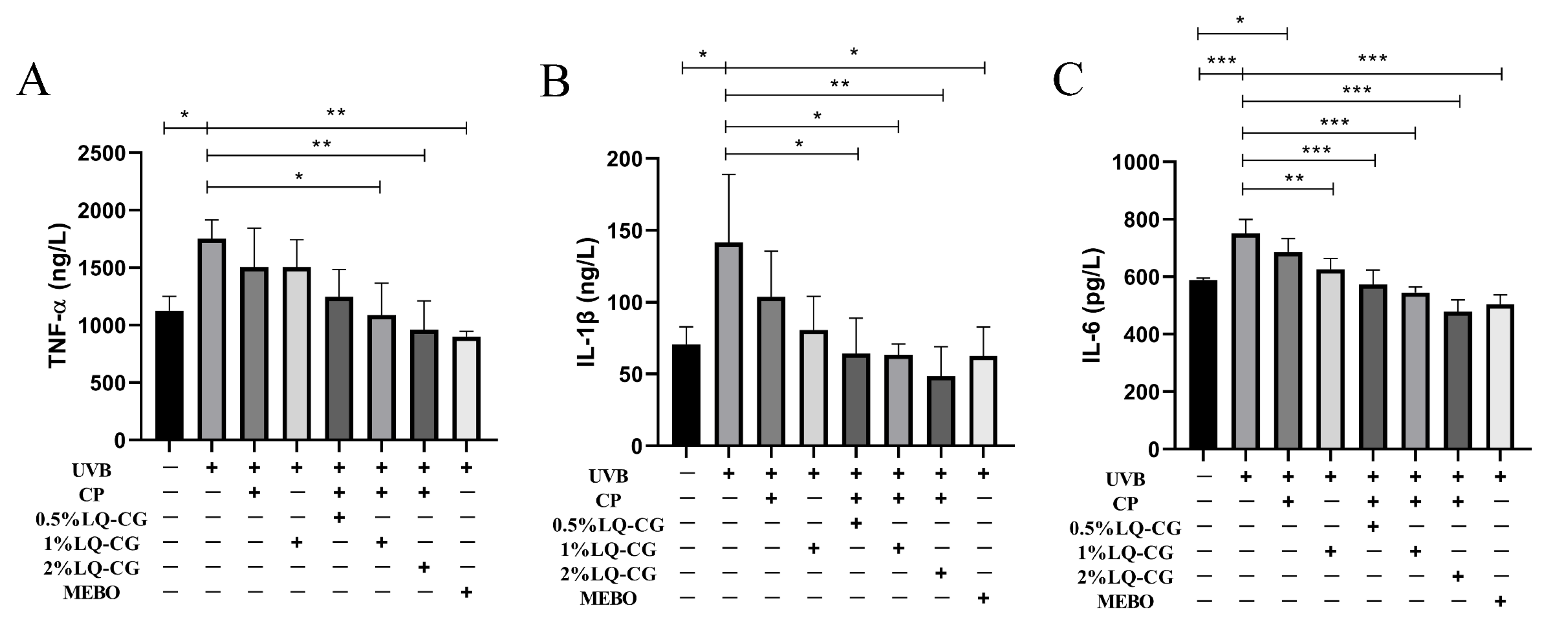
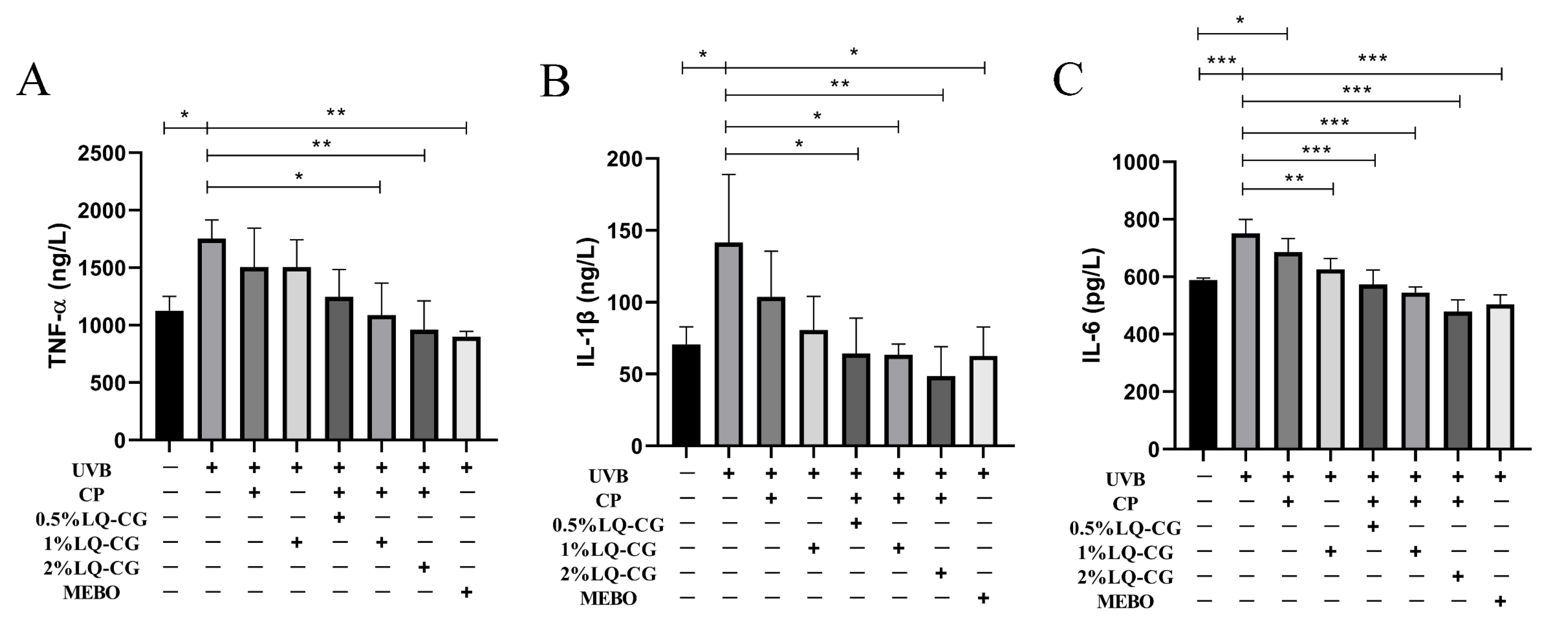
2.6. Effect of LQ-CG-CP on Inflammatory Factors in a Mouse Model of Solar Dermatitis
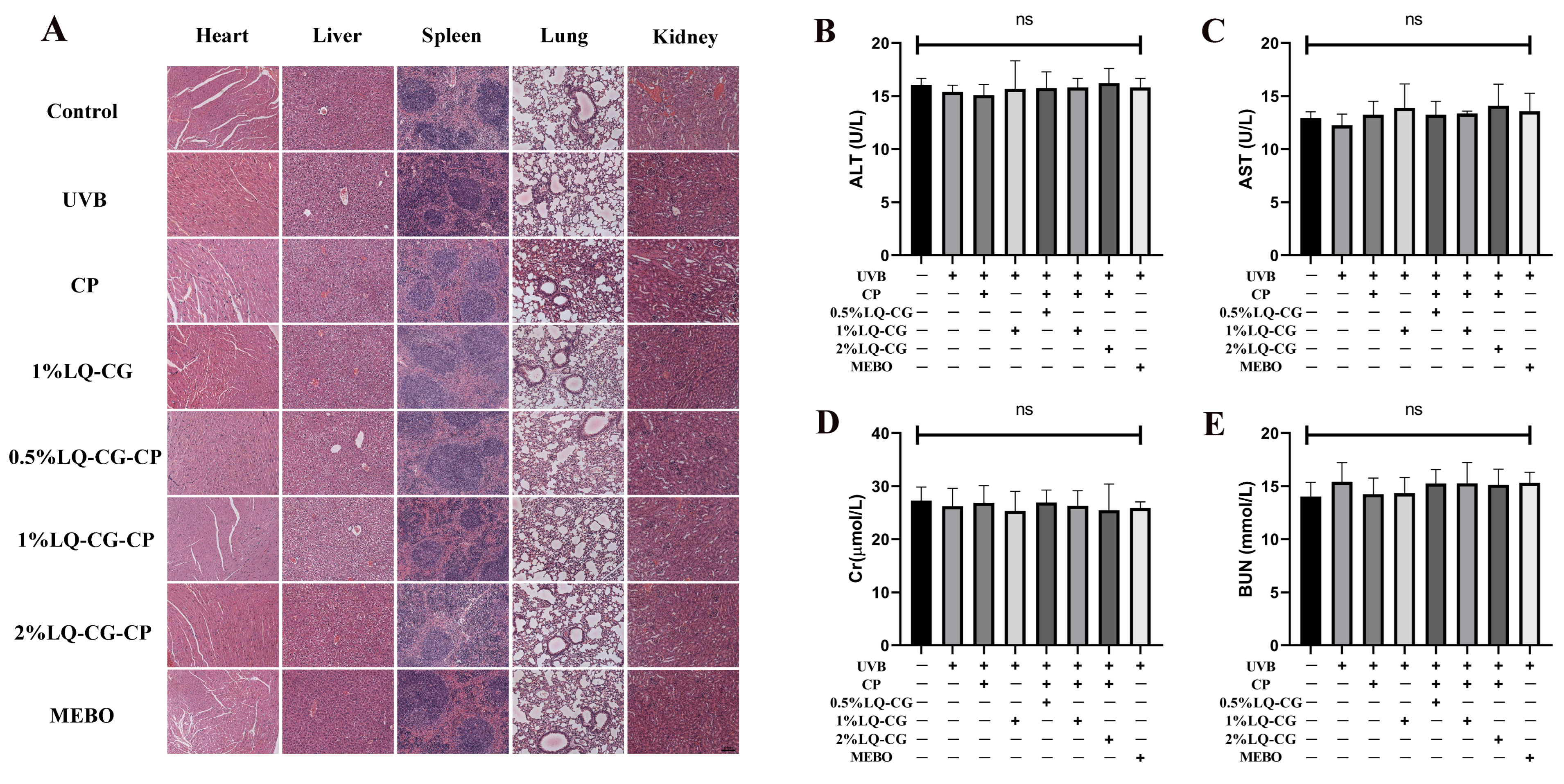
2.7. Biosafety Research
2.7.1. Histopathologic Results of Mouse Viscera
2.7.2. Blood Biochemical Indicators
3. Discussion
4. Materials and Methods
4.1. Cell Culture and Treatment
4.2. Cell Viability Assay
4.3. Cell Migration Assay
4.4. Preparation of LQ-CG-CP
4.5. Establishment and Treatment of Mouse Solar Dermatitis Model
4.6. Enzyme-Linked Immunosorbent Assay (ELISA)
4.7. Histopathological Examination
4.8. Biosafety Validation
4.9. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhou, G.; Peng, L.; Gao, W.; Zou, Y.; Tan, Y.; Ding, Y.; Li, S.; Sun, H.; Chen, R. The acute effects of ultraviolet radiation exposure on solar dermatitis in Shanghai, China. Int. J. Biometeorol. 2020, 64, 585–591. [Google Scholar] [CrossRef]
- Holman, D.M.; Ragan, K.R.; Julian, A.K.; Perna, F.M. The Context of Sunburn Among U.S. Adults: Common Activities and Sun Protection Behaviors. Am. J. Prev. Med. 2021, 60, e213–e220. [Google Scholar] [CrossRef]
- Guy, G.P., Jr.; Berkowitz, Z.; Watson, M. Estimated Cost of Sunburn-Associated Visits to US Hospital Emergency Departments. JAMA Dermatol. 2017, 153, 90–92. [Google Scholar] [CrossRef]
- Gandini, S.; Sera, F.; Cattaruzza, M.S.; Pasquini, P.; Picconi, O.; Boyle, P.; Melchi, C.F. Meta-analysis of risk factors for cutaneous melanoma: II. Sun exposure. Eur. J. Cancer 2005, 41, 45–60. [Google Scholar] [CrossRef]
- Zou, W.; Gonzalez, A.; Jampaiah, D.; Ramanathan, R.; Taha, M.; Walia, S.; Sriram, S.; Bhaskaran, M.; Dominguez-Vera, J.M.; Bansal, V. Skin color-specific and spectrally-selective naked-eye dosimetry of UVA, B and C radiations. Nat. Commun. 2018, 9, 3743. [Google Scholar] [CrossRef]
- Willis, I.; Cylus, L. UVA erythema in skin: Is it a sunburn? J. Investig. Dermatol. 1977, 68, 128–129. [Google Scholar] [CrossRef]
- Adhami, V.M.; Afaq, F.; Ahmad, N. Suppression of ultraviolet B exposure-mediated activation of NF-kappaB in normal human keratinocytes by resveratrol. Neoplasia 2003, 5, 74–82. [Google Scholar] [CrossRef]
- Nicolaou, A.; Pilkington, S.M.; Rhodes, L.E. Ultraviolet-radiation induced skin inflammation: Dissecting the role of bioactive lipids. Chem. Phys. Lipids 2011, 164, 535–543. [Google Scholar] [CrossRef]
- Maverakis, E.; Miyamura, Y.; Bowen, M.P.; Correa, G.; Ono, Y.; Goodarzi, H. Light, including ultraviolet. J. Autoimmun. 2010, 34, J247–J257. [Google Scholar] [CrossRef] [PubMed]
- Martinez, R.M.; Pinho-Ribeiro, F.A.; Steffen, V.S.; Caviglione, C.V.; Vignoli, J.A.; Barbosa, D.S.; Baracat, M.M.; Georgetti, S.R.; Verri, W.A.; Casagrande, R. Naringenin Inhibits UVB Irradiation-Induced Inflammation and Oxidative Stress in the Skin of Hairless Mice. J. Nat. Prod. 2015, 78, 1647–1655. [Google Scholar] [CrossRef] [PubMed]
- Melo, C.P.; Saito, P.; Vale, D.L.; Rodrigues, C.C.; Pinto, I.C.; Martinez, R.M.; Bezerra, J.R.; Baracat, M.M.; Verri, W.A.; Fonseca-Bazzo, Y.M.; et al. Protective effect of oral treatment with Cordia verbenacea extract against UVB irradiation deleterious effects in the skin of hairless mouse. J. Photochem. Photobiol. B: Biol. 2021, 216, 112151. [Google Scholar] [CrossRef] [PubMed]
- Peng, F.; Du, Q.; Peng, C.; Wang, N.; Tang, H.; Xie, X.; Shen, J.; Chen, J. A Review: The Pharmacology of Isoliquiritigenin. Phytother. Res. PTR 2015, 29, 969–977. [Google Scholar] [CrossRef]
- Qin, J.; Chen, J.; Peng, F.; Sun, C.; Lei, Y.; Chen, G.; Li, G.; Yin, Y.; Lin, Z.; Wu, L.; et al. Pharmacological activities and pharmacokinetics of liquiritin: A review. J. Ethnopharmacol. 2022, 293, 115257. [Google Scholar] [CrossRef]
- El-Saber Batiha, G.; Magdy Beshbishy, A.; El-Mleeh, A.; Abdel-Daim, M.M.; Prasad Devkota, H. Traditional Uses, Bioactive Chemical Constituents, and Pharmacological and Toxicological Activities of Glycyrrhiza glabra L. (Fabaceae). Biomolecules 2020, 10, 352. [Google Scholar] [CrossRef] [PubMed]
- Zhai, K.F.; Duan, H.; Cui, C.Y.; Cao, Y.Y.; Si, J.L.; Yang, H.J.; Wang, Y.C.; Cao, W.G.; Gao, G.Z.; Wei, Z.J. Liquiritin from Glycyrrhiza uralensis Attenuating Rheumatoid Arthritis via Reducing Inflammation, Suppressing Angiogenesis, and Inhibiting MAPK Signaling Pathway. J. Agric. Food Chem. 2019, 67, 2856–2864. [Google Scholar] [CrossRef]
- Zhou, H.; Yang, T.; Lu, Z.; He, X.; Quan, J.; Liu, S.; Chen, Y.; Wu, K.; Cao, H.; Liu, J.; et al. Liquiritin exhibits anti-acute lung injury activities through suppressing the JNK/Nur77/c-Jun pathway. Chin. Med. 2023, 18, 35. [Google Scholar] [CrossRef]
- Holman, D.M.; Ding, H.; Berkowitz, Z.; Hartman, A.M.; Perna, F.M. Sunburn prevalence among US adults, National Health Interview Survey 2005, 2010, and 2015. J. Am. Acad. Dermatol. 2019, 80, 817–820. [Google Scholar] [CrossRef] [PubMed]
- Kolto, A.; Rodriguez, L.; McAvoy, H.; Nic Gabhainn, S. Sunburn, Sun Safety and Indoor Tanning Among Schoolchildren in Ireland. Int. J. Public. Health 2021, 66, 1604045. [Google Scholar] [CrossRef]
- Brand, R.M.; Stottlemyer, J.M.; Paglia, M.C.; Carey, C.D.; Falo, L.D., Jr. Ethanol consumption synergistically increases ultraviolet radiation induced skin damage and immune dysfunction. J. Dermatol. Sci. 2021, 101, 40–48. [Google Scholar] [CrossRef]
- Connolly, S.; Bertinetti, M.; Teague, W.J.; Gabbe, B.J.; Tracy, L.M. Sunburn Injuries Admitted to Burn Services in Australia and New Zealand. JAMA Dermatol. 2021, 157, 729–731. [Google Scholar] [CrossRef]
- Gurtner, G.; Werner, S.; Barrandon, Y.; Longaker, T. Wound repair and regeneration. Nature 2008, 453, 314–321. [Google Scholar] [CrossRef]
- Rodrigues, M.; Kosaric, N.; Bonham, C.A.; Gurtner, G.C. Wound Healing: A Cellular Perspective. Physiol. Rev. 2019, 99, 665–706. [Google Scholar] [CrossRef]
- Chang, H.Y.; Chi, J.T.; Dudoit, S.; Bondre, C.; van de Rijn, M.; Botstein, D.; Brown, P.O. Diversity, topographic differentiation, and positional memory in human fibroblasts. Proc. Natl. Acad. Sci. USA 2002, 99, 12877–12882. [Google Scholar] [CrossRef]
- Barrientos, S.; Stojadinovic, O.; Golinko, M.S.; Brem, H.; Tomic-Canic, M. Growth factors and cytokines in wound healing. Wound Repair Regen. Off. Publ. Wound Heal. Soc. Eur. Tissue Repair Soc. 2008, 16, 585–601. [Google Scholar]
- Grada, A.; Otero-Vinas, M.; Prieto-Castrillo, F.; Obagi, Z.; Falanga, V. Research Techniques Made Simple: Anal-ysis of Collective Cell Migration Using the Wound Healing Assay. J. Investig. Dermatol. 2017, 137, e11–e16. [Google Scholar] [CrossRef]
- Masson-Meyers, D.S.; Andrade, T.A.M.; Caetano, G.F.; Guimaraes, F.R.; Leite, M.N.; Leite, S.N.; Frade, M.A.C. Experimental models and methods for cutaneous wound healing assessment. Int. J. Exp. Pathol. 2020, 101, 21–37. [Google Scholar] [CrossRef]
- Goldberg, M.T.; Han, Y.P.; Yan, C.; Shaw, M.C.; Garner, W.L. TNF-alpha suppresses alpha-smooth muscle actin expression in human dermal fibroblasts: An implication for abnormal wound healing. J. Investig. Dermatol. 2007, 127, 2645–2655. [Google Scholar] [CrossRef]
- Sorg, H.; Tilkorn, D.J.; Hager, S.; Hauser, J.; Mirastschijski, U. Skin Wound Healing: An Update on the Current Knowledge and Concepts. Eur. Surg. Res. 2016, 58, 81–94. [Google Scholar] [CrossRef]
- Aumailley, M.; Gayraud, B. Structure and biological activity of the extracellular matrix. J. Mol. Med. 1998, 76, 253–265. [Google Scholar] [CrossRef]
- Huang, J.; Heng, S.; Zhang, W.; Liu, Y.; Xia, T.; Ji, C.; Zhang, L.J. Dermal extracellular matrix molecules in skin development, homeostasis, wound regeneration and diseases. Semin. Cell Dev. Biol. 2022, 128, 137–144. [Google Scholar] [CrossRef]
- Castaño, O.; Pérez-Amodio, S.; Navarro-Requena, C.; Mateos-Timoneda, M.; Engel, E. Instructive microenvironments in skin wound healing: Biomaterials as signal releasing platforms. Adv. Drug Deliv. Rev. 2018, 129, 95–117. [Google Scholar] [CrossRef] [PubMed]
- Salgado, R.M.; Alcántara, L.; Mendoza-Rodríguez, C.A.; Cerbón, M.; Hidalgo-González, C.; Mercadillo, P.; Moreno, L.M.; Alvarez-Jiménez, R.; Krötzsch, E. Post-burn hypertrophic scars are characterized by high levels of IL-1β mRNA and protein and TNF-α type I receptors. Burn. J. Int. Soc. Burn Inj. 2012, 38, 668–676. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.C.; Zhao, W.Y.; Cao, Y.; Liu, Y.Q.; Sun, Q.; Shi, P.; Cai, J.Q.; Shen, X.Z.; Tan, W.Q. The Roles of Inflammation in Keloid and Hypertrophic Scars. Front. Immunol. 2020, 11, 603187. [Google Scholar] [CrossRef] [PubMed]
- Hassanshahi, A.; Moradzad, M.; Ghalamkari, S.; Fadaei, M.; Cowin, A.J.; Hassanshahi, M. Macrophage-Mediated Inflammation in Skin Wound Healing. Cells 2022, 11, 2953. [Google Scholar] [CrossRef] [PubMed]
- Wilder-Smith, A.J. Hell’s itch due to sunburn. J. Travel Med. 2019, 26, tay124. [Google Scholar] [CrossRef] [PubMed]
- Dyhre-Petersen, N.; Gazerani, P. Presence and characteristics of senile pruritus among Danish elderly living in nursing homes. Future Sci. OA 2019, 5, Fso399. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.; Yue, X.; Zhao, Y.; Du, L.; Xie, Z.; Yuan, Y.; Zhang, S.; Li, F.; Feng, J.; Hu, H. Mechanisms of Broad-Band UVB Irradiation—Induced Itch in Mice. J. Investig. Dermatol. 2021, 141, 2499–2508.e3. [Google Scholar] [CrossRef]
- Huang, X.; Yang, J.; Zhang, R.; Ye, L.; Li, M.; Chen, W. Phloroglucinol Derivative Carbomer Hydrogel Accelerates MRSA-Infected Wounds’ Healing. Int. J. Mol. Sci. 2022, 23, 8682. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Y.; Li, S.; Pan, J.; Song, C.; Chen, W.; Zhang, Y. Liquiritin Carbomer Gel Cold Paste Promotes Healing of Solar Dermatitis in Mice. Int. J. Mol. Sci. 2024, 25, 3767. https://doi.org/10.3390/ijms25073767
Huang Y, Li S, Pan J, Song C, Chen W, Zhang Y. Liquiritin Carbomer Gel Cold Paste Promotes Healing of Solar Dermatitis in Mice. International Journal of Molecular Sciences. 2024; 25(7):3767. https://doi.org/10.3390/ijms25073767
Chicago/Turabian StyleHuang, Yanfang, Sijia Li, Jinghua Pan, Congjing Song, Weiqiang Chen, and Yun Zhang. 2024. "Liquiritin Carbomer Gel Cold Paste Promotes Healing of Solar Dermatitis in Mice" International Journal of Molecular Sciences 25, no. 7: 3767. https://doi.org/10.3390/ijms25073767
APA StyleHuang, Y., Li, S., Pan, J., Song, C., Chen, W., & Zhang, Y. (2024). Liquiritin Carbomer Gel Cold Paste Promotes Healing of Solar Dermatitis in Mice. International Journal of Molecular Sciences, 25(7), 3767. https://doi.org/10.3390/ijms25073767