

Development and Validation of an HPLC-UV Method for the Quantification of Acyclovir and Ganciclovir in the Plasma of Pediatric Immunocompromised Patients

Abstract
1. Introduction
2. Results
2.1. Method Development
2.2. Method Validation
2.2.1. Linearity
2.2.2. Sensitivity
2.2.3. Accuracy and Precision
2.2.4. Matrix Effect and Recovery
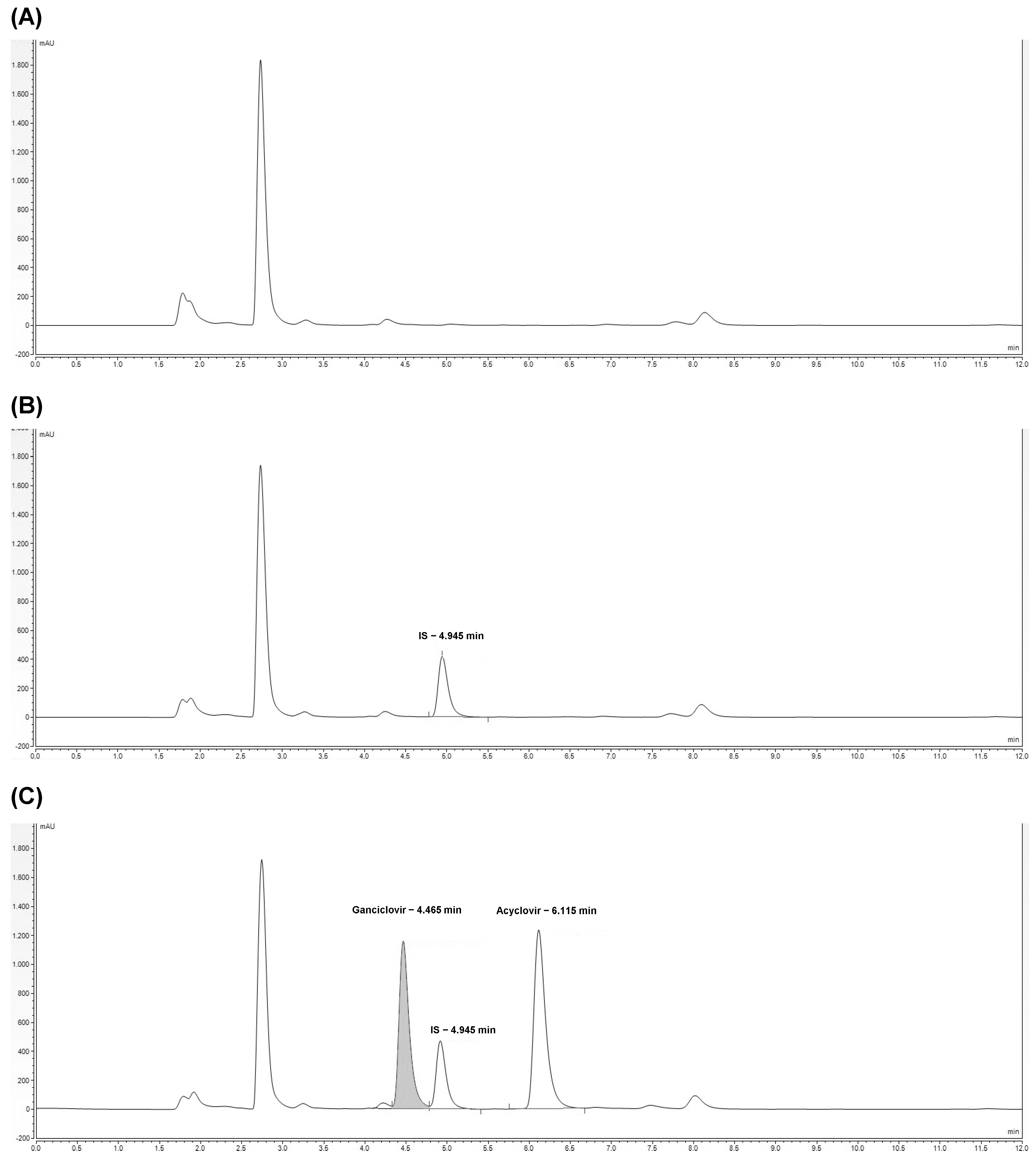
2.2.5. Specificity
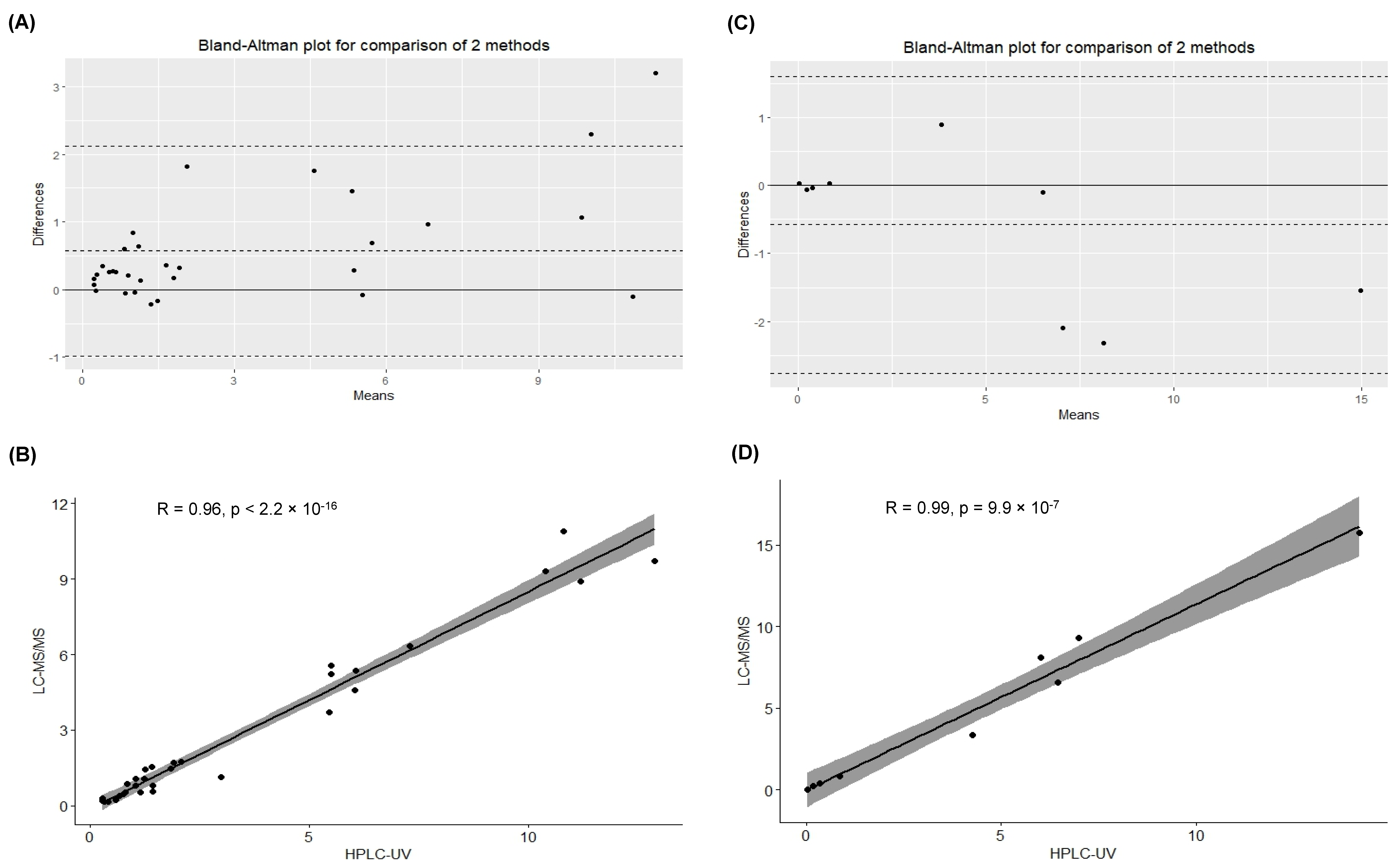
2.3. Method Applicability
3. Discussion
4. Materials and Methods
4.1. Chemicals and Reagents
4.2. Biological Samples
4.3. Stocking and Working Solutions
4.4. HPLC-UV Analysis
4.5. LC-MS/MS Analyses
4.6. Analytical Validation
4.7. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Beyar-Katz, O.; Bitterman, R.; Zuckerman, T.; Ofran, Y.; Yahav, D.; Paul, M. Anti-herpesvirus prophylaxis, pre-emptive treatment or no treatment in adults undergoing allogeneic transplant for haematological disease: Systematic review and meta-analysis. Clin. Microbiol. Infect. 2020, 26, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Kotton, C.N. CMV: Prevention, Diagnosis and Therapy. Am. J. Transplant. 2013, 13 (Suppl. S3), 24–40, quiz 40. [Google Scholar] [CrossRef] [PubMed]
- Huntjens, D.W.; Dijkstra, J.A.; Verwiel, L.N.; Slijkhuis, M.; Elbers, P.; Welkers, M.R.A.; Veldkamp, A.I.; Kuijvenhoven, M.A.; de Leeuw, D.C.; Abdullah-Koolmees, H.; et al. Optimizing Antiviral Dosing for HSV and CMV Treatment in Immunocompromised Patients. Pharmaceutics 2023, 15, 163. [Google Scholar] [CrossRef] [PubMed]
- Maximova, N.; Nisticò, D.; Luci, G.; Simeone, R.; Piscianz, E.; Segat, L.; Barbi, E.; Di Paolo, A. Population Pharmacokinetics of Intravenous Acyclovir in Oncologic Pediatric Patients. Front. Pharmacol. 2022, 13, 865871. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, B.M.; Barreto, J.N.; Barreto, E.F.; Crow, S.A.; Dierkhising, R.A.; Jannetto, P.J.; Tosh, P.K.; Razonable, R.R. Relationship of Ganciclovir Therapeutic Drug Monitoring with Clinical Efficacy and Patient Safety. Antimicrob. Agents Chemother. 2019, 63, 10–1128. [Google Scholar] [CrossRef]
- Stockmann, C.; Roberts, J.K.; Knackstedt, E.D.; Spigarelli, M.G.; Sherwin, C.M. Clinical pharmacokinetics and pharmacodynamics of ganciclovir and valganciclovir in children with cytomegalovirus infection. Expert Opin. Drug Metab. Toxicol. 2015, 11, 205–219. [Google Scholar] [CrossRef] [PubMed]
- Pazhayattil, G.S.; Shirali, A.C. Drug-induced impairment of renal function. Int. J. Nephrol. Renov. Dis. 2014, 7, 457–468. [Google Scholar]
- Nishii, R.; Mizuno, T.; Rehling, D.; Smith, C.; Clark, B.L.; Zhao, X.; Brown, S.A.; Smart, B.; Moriyama, T.; Yamada, Y.; et al. NUDT15 polymorphism influences the metabolism and therapeutic effects of acyclovir and ganciclovir. Nat. Commun. 2021, 12, 4181. [Google Scholar] [CrossRef]
- Kacirova, I.; Urinovska, R.; Sagan, J. Therapeutic monitoring of serum concentrations of acyclovir and its metabolite 9-(carboxymethoxymethyl) guanine in routine clinical practice. Biomed. Pharmacother. 2022, 156, 113852. [Google Scholar] [CrossRef]
- Märtson, A.G.; Edwina, A.E.; Kim, H.Y.; Knoester, M.; Touw, D.J.; Sturkenboom, M.G.G.; Alffenaar, J.C. Therapeutic Drug Monitoring of Ganciclovir: Where Are We? Ther. Drug Monit. 2022, 44, 138–147. [Google Scholar] [CrossRef]
- Zendelovska, D.; Simeska, S.; Atanasovska, E.; Georgievska, K.; Kikerkov, I.; Labachevski, N.; Jakovski, K.; Balkanov, T. Determination of Acyclovir in Human Plasma Samples by HPLC Method with UV Detection: Application to Single-Dose Pharmacokinetic Study. Open Access Maced. J. Med. Sci. 2015, 3, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Grebe, S.K.; Singh, R.J. LC-MS/MS in the Clinical Laboratory—Where to From Here? Clin. Biochem. Rev. 2011, 32, 5–31. [Google Scholar] [PubMed]
- ICH Q2(R2) Guideline on Validation of Analytical Procedures. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/ich-q2r2-guideline-validation-analytical-procedures-step-5-revision-1_en.pdf (accessed on 1 January 2023).
- Pitt, J.J. Principles and applications of liquid chromatography-mass spectrometry in clinical biochemistry. Clin. Biochem. Rev. 2009, 30, 19–34. [Google Scholar] [PubMed]
- Pigliasco, F.; Cafaro, A.; Simeoli, R.; Barco, S.; Magnasco, A.; Faraci, M.; Tripodi, G.; Goffredo, B.M.; Cangemi, G. A UHPLC-MS/MS Method for Therapeutic Drug Monitoring of Aciclovir and Ganciclovir in Plasma and Dried Plasma Spots. Biomedicines 2021, 9, 1379. [Google Scholar] [CrossRef] [PubMed]
- Dao, Y.J.; Jiao, Z.; Zhong, M.K. Simultaneous determination of aciclovir, ganciclovir, and penciclovir in human plasma by high-performance liquid chromatography with fluorescence detection. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2008, 867, 270–276. [Google Scholar] [CrossRef]
- Alffenaar, J.; van Hateren, K.; Martson, A.; van den Bosch, G.; van der Werf, T.; Touw, D.; Alffenaar, J. Determination of ganciclovir and acyclovir in human serum using liquid chromatography-tandem mass spectrometry. J. Appl. Bioanal. 2018, 4, 175–186. [Google Scholar] [CrossRef]
- Ärlemalm, A.; Helldén, A.; Karlsson, L.; Carlsson, B.J.B.C. Rapid determination of acyclovir, its main metabolite 9-carboxymethoxymethylguanine, ganciclovir, and penciclovir in human serum using LC–MS/MS. Biomed. Chromatogr. 2022, 36, e5315. [Google Scholar] [CrossRef]
- Weller, D.R.; Balfour, H.H., Jr.; Vezina, H.E. Simultaneous determination of acyclovir, ganciclovir, and (R)-9-[4-hydroxy-2-(hydroxymethyl)butyl]guanine in human plasma using high-performance liquid chromatography. Biomed. Chromatogr. 2009, 23, 822–827. [Google Scholar] [CrossRef] [PubMed]
- Teshima, D.; Otsubo, K.; Yoshida, T.; Itoh, Y.; Oishi, R. A simple and simultaneous determination of acyclovir and ganciclovir in human plasma by high-performance liquid chromatography. Biomed. Chromatogr. 2003, 17, 500–503. [Google Scholar] [CrossRef]
- Shibata, N.; Kitamura, A.; Yoshikawa, Y.; Inoue, T.; Bamba, T.; Takada, K.J.P.; Communications, P. Simultaneous determination of aciclovir and ganciclovir in plasma by HPLC and pharmacokinetic interactions. Pharm. Pharmacol. Commun. 2000, 6, 501–506. [Google Scholar] [CrossRef]
- Matuszewski, B.K.; Constanzer, M.L.; Chavez-Eng, C.M. Strategies for the assessment of matrix effect in quantitative bioanalytical methods based on HPLC-MS/MS. Anal. Chem. 2003, 75, 3019–3030. [Google Scholar] [CrossRef] [PubMed]
- ICH Guideline M10 on Bioanalytical Method Validation and Study Sample Analysis. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/ich-guideline-m10-bioanalytical-method-validation-step-5_en.pdf (accessed on 1 January 2023).
- Pablo, A.H.; Breaud, A.R.; Clarke, W. Analysis of Immunosuppressant Drugs in Whole Blood by Liquid Chromatography-Tandem Mass Spectrometry (LC-MS/MS). Curr. Protoc. Toxicol. 2020, 84, e92. [Google Scholar] [CrossRef] [PubMed]
- Bunch, D.R.; Wang, S. Measurement of mycophenolic acid in plasma or serum by a commercial enzyme inhibition technique in comparison with a high performance liquid chromatography method. Clin. Chem. Lab. Med. 2008, 46, 1281–1284. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Features | LC-MS/MS Methods (Already in Use) | HPLC-UV Method (Developed) |
|---|---|---|
| Reagents and instrumentation costs | High | Low |
| Availability of instrumentation used | Less frequently available | More frequently available |
| Volume of plasma sample | 150 µL | 100 µL |
| Internal standard used | Acyclovir for ganciclovir quantification; ganciclovir for acyclovir quantification | Bromouracil |
| Time for sample preparation | 15 min | 20 min |
| Injected volume | 5 µL | 20 µL |
| Time for sample analysis | 4 min | 12 min |
| Type of elution of mobile phases | Gradient | Isocratic |
| Acyclovir | |||||||||
| Standard | Nominal Concentration (µg/mL) | 1 | 2 | 3 | Between-Run Accuracy (%) | Between-Run Means (µg/mL) (RSD%) | |||
| Calculated Concentration (µg/mL) | Within-Run Accuracy (%) | Calculated Concentration (µg/mL) | Within-Run Accuracy (%) | Calculated Concentration (µg/mL) | Within-Run Accuracy (%) | ||||
| CAL1 | 0.5 | 0.503 | 99.40 | 0.496 | 100.80 | 0.499 | 100.20 | 100.13 | 0.499 (0.70%) |
| CAL2 | 1 | 0.990 | 101.00 | 1.010 | 99.00 | 1.010 | 99.00 | 99.67 | 1.003 (1.15%) |
| CAL3 | 5 | 4.843 | 103.14 | 5.161 | 96.78 | 5.132 | 97.36 | 99.09 | 5.045 (3.48%) |
| CAL4 | 10 | 10.793 | 92.07 | 9.841 | 101.59 | 9.781 | 102.19 | 98.62 | 10.138 (5.60%) |
| CAL5 | 25 | 24.844 | 100.62 | 25.082 | 99.67 | 24.919 | 100.32 | 100.21 | 24.948 (0.49%) |
| CAL6 | 40 | 39.083 | 102.29 | 39.273 | 101.82 | 39.014 | 102.47 | 102.19 | 39.123 (0.34%) |
| Ganciclovir | |||||||||
| Standard | Nominal Concentration (µg/mL) | 1 | 2 | 3 | Between-Run Accuracy (%) | Between-Run Means (µg/mL) (RSD%) | |||
| Calculated Concentration (µg/mL) | Within-Run Accuracy (%) | Calculated Concentration (µg/mL) | Within-Run Accuracy (%) | Calculated Concentration (µg/mL) | Within-Run Accuracy (%) | ||||
| CAL1 | 0.5 | 0.494 | 101.20 | 0.501 | 99.80 | 0.466 | 106.80 | 102.60 | 0.487 (3.80%) |
| CAL2 | 1 | 1.014 | 98.60 | 0.990 | 101.00 | 0.943 | 105.70 | 101.77 | 0.982 (3.68%) |
| CAL3 | 5 | 4.974 | 100.52 | 5.171 | 96.58 | 5.03 | 99.40 | 98.83 | 5.058 (2.00%) |
| CAL4 | 10 | 10.757 | 92.43 | 9.942 | 100.58 | 9.693 | 103.07 | 98.69 | 10.131 (5.49%) |
| CAL5 | 25 | 24.491 | 102.04 | 25.109 | 99.56 | 24.517 | 101.93 | 101.18 | 24.706 (1.41%) |
| CAL6 | 40 | 38.502 | 103.75 | 39.136 | 102.16 | 38.227 | 104.43 | 103.45 | 38.622 (1.21%) |
| Acyclovir | |||||||||||||
| Standard | Nominal Concentration (µg/mL) | 1 | 2 | 3 | Between-Run Accuracy (%) | Between Run Precision (CV%) | Between-Run Means (µg/mL) (SD) | ||||||
| Within-Run Accuracy (%) | Within-Run Precision (CV%) | Within-Run Means (µg/mL) (SD) | Within-Run Accuracy (%) | Within-Run Precision (CV%) | Within-Run Means (µg/mL) (SD) | Within-Run Accuracy (%) | Within-Run Precision (CV%) | Within-Run Means (µg/mL) (SD) | |||||
| QCI | 2.5 | 100.75 | 5.79 | 2.55 (0.15) | 99.20 | 5.84 | 2.63 (0.15) | 99.42 | 5.81 | 2.62 (0.15) | 99.79 | 5.81 | 2.60 (0.04) |
| QCII | 12.5 | 96.38 | 2.34 | 13.20 (0.31) | 96.04 | 0.02 | 13.49 (0.01) | 94.67 | 2.34 | 13.64 (0.32) | 95.70 | 1.57 | 13.44 (0.22) |
| QCIII | 20 | 99.86 | 0.37 | 20.11 (0.07) | 97.84 | 0.37 | 20.92 (0.08) | 98.17 | 0.37 | 20.78 (0.08) | 98.62 | 0.37 | 20.60 (0.43) |
| Ganciclovir | |||||||||||||
| Standard | Nominal Concentration (µg/mL) | 1 | 2 | 3 | Between-Run Accuracy (%) | Between-Run Precision (CV%) | Between-Run Means (µg/mL) (SD) | ||||||
| Within-Run Accuracy (%) | Within-Run Precision (CV%) | Within-Run Means (µg/mL) (SD) | Within-Run Accuracy (%) | Within-Run Precision (CV%) | Within-Run Means (µg/mL) (SD) | Within-Run Accuracy (%) | Within-Run Precision (CV%) | Within-Run Means (µg/mL) (SD) | |||||
| QCI | 2.5 | 105.66 | 5.68 | 2.32 (0.13) | 99.45 | 5.36 | 2.61 (0.14) | 101.20 | 5.40 | 2.53 (0.14) | 102.10 | 5.48 | 2.48 (0.15) |
| QCII | 12.5 | 98.41 | 2.11 | 12.71 (0.27) | 94.81 | 2.09 | 13.63 (0.28) | 96.12 | 2.09 | 13.29 (0.28) | 96.44 | 2.10 | 13.21 (0.46) |
| QCIII | 20 | 101.65 | 0.48 | 19.41 (0.09) | 98.34 | 0.48 | 20.73 (0.10) | 99.58 | 0.48 | 20.24 (0.10) | 99.86 | 0.48 | 20.12 (0.67) |
| Standard | Acyclovir | Ganciclovir | ||||
|---|---|---|---|---|---|---|
| ME (%) | RE (%) | PE (%) | ME (%) | RE (%) | PE (%) | |
| QCI | 95.69 | 94.89 | 90.80 | 99.53 | 91.53 | 91.10 |
| QCII | 101.57 | 95.99 | 97.49 | 101.64 | 94.55 | 96.10 |
| QCIII | 93.36 | 98.73 | 92.17 | 91.90 | 97.28 | 89.40 |
| ID | Q1 Mass (Da) | Q3 Mass (Da) | DP (V) | EP (V) | CE (V) | CXP (V) |
|---|---|---|---|---|---|---|
| Acyclovir_1 | 226.100 | 152.100 | 60 | 10 | 20 | 5 |
| Acyclovir_2 | 226.100 | 135.100 | 60 | 10 | 35 | 5 |
| Acyclovir_3 | 226.100 | 110.100 | 60 | 10 | 35 | 5 |
| Ganciclovir_1 | 256.100 | 152.100 | 60 | 10 | 20 | 5 |
| Ganciclovir_2 | 256.100 | 135.100 | 60 | 10 | 35 | 5 |
| Ganciclovir_3 | 256.100 | 110.100 | 60 | 10 | 35 | 5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franzin, M.; Ruoso, R.; Del Savio, R.; Addobbati, R. Development and Validation of an HPLC-UV Method for the Quantification of Acyclovir and Ganciclovir in the Plasma of Pediatric Immunocompromised Patients. Int. J. Mol. Sci. 2024, 25, 2685. https://doi.org/10.3390/ijms25052685
Franzin M, Ruoso R, Del Savio R, Addobbati R. Development and Validation of an HPLC-UV Method for the Quantification of Acyclovir and Ganciclovir in the Plasma of Pediatric Immunocompromised Patients. International Journal of Molecular Sciences. 2024; 25(5):2685. https://doi.org/10.3390/ijms25052685
Chicago/Turabian StyleFranzin, Martina, Rachele Ruoso, Rossella Del Savio, and Riccardo Addobbati. 2024. "Development and Validation of an HPLC-UV Method for the Quantification of Acyclovir and Ganciclovir in the Plasma of Pediatric Immunocompromised Patients" International Journal of Molecular Sciences 25, no. 5: 2685. https://doi.org/10.3390/ijms25052685
APA StyleFranzin, M., Ruoso, R., Del Savio, R., & Addobbati, R. (2024). Development and Validation of an HPLC-UV Method for the Quantification of Acyclovir and Ganciclovir in the Plasma of Pediatric Immunocompromised Patients. International Journal of Molecular Sciences, 25(5), 2685. https://doi.org/10.3390/ijms25052685