
Ex Vivo Optimization of Donor Lungs with Inhaled Sevoflurane during Normothermic Ex Vivo Lung Perfusion (VITALISE): A Pilot and Feasibility Study in Sheep

 , ,
, ,  , ,
, , 
Abstract
1. Introduction
2. Results
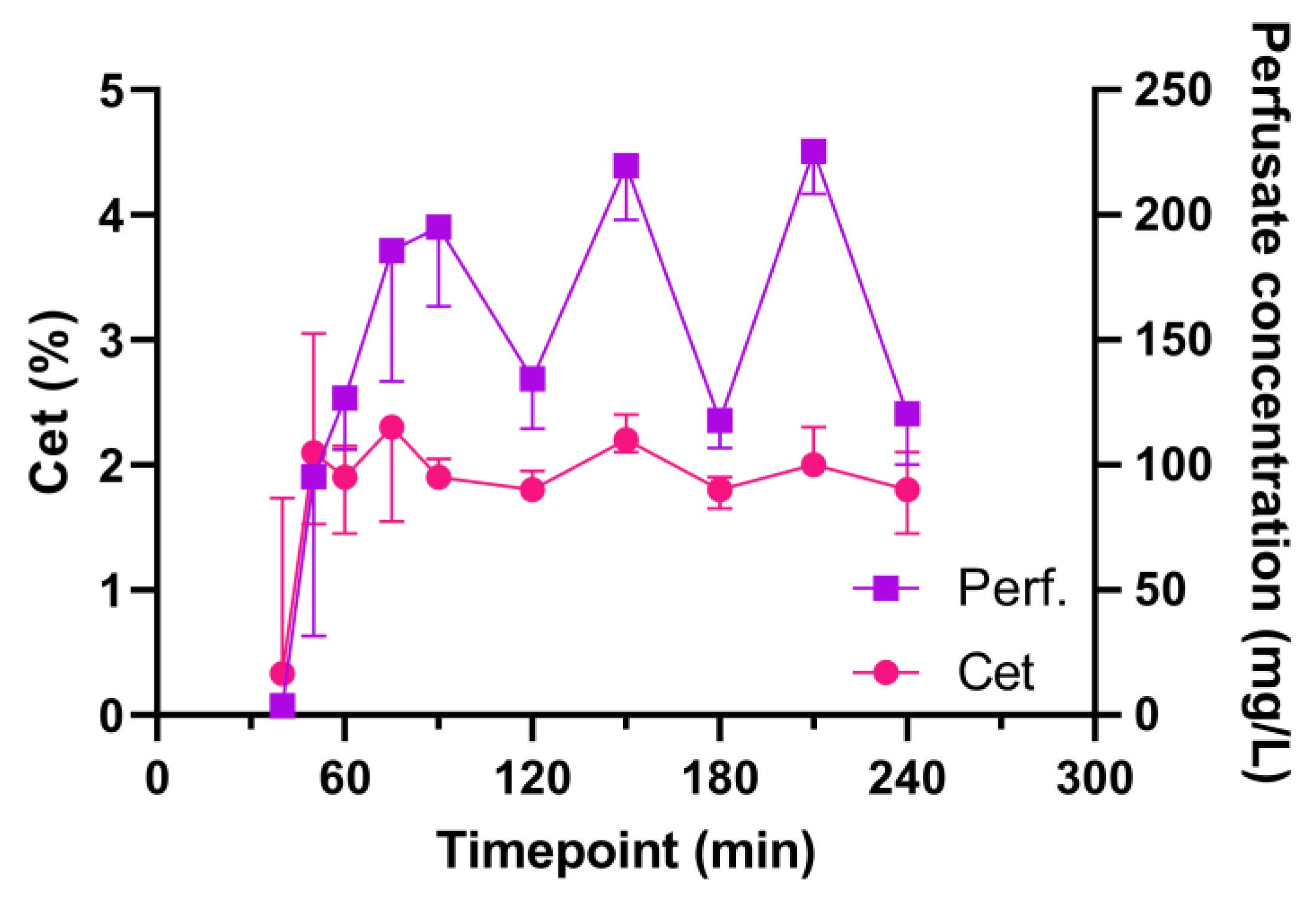
2.1. Sevoflurane Measurements
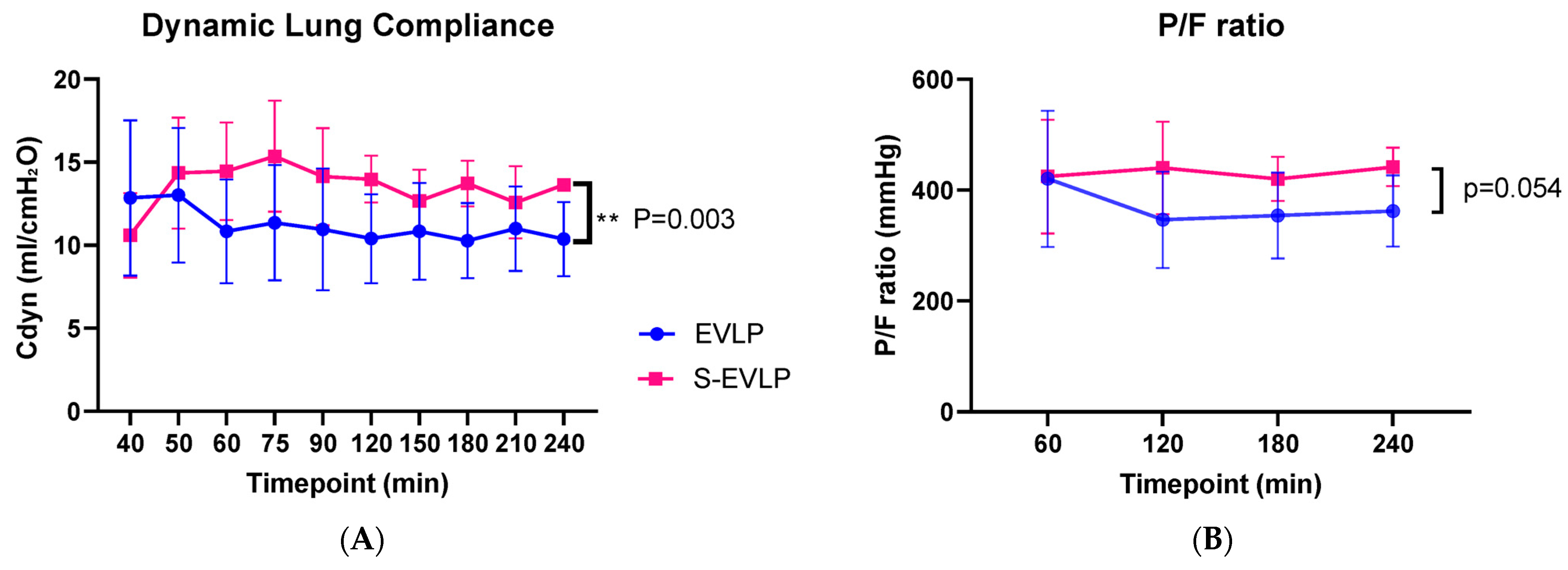
2.2. Functional Lung Evaluation
2.3. Histology
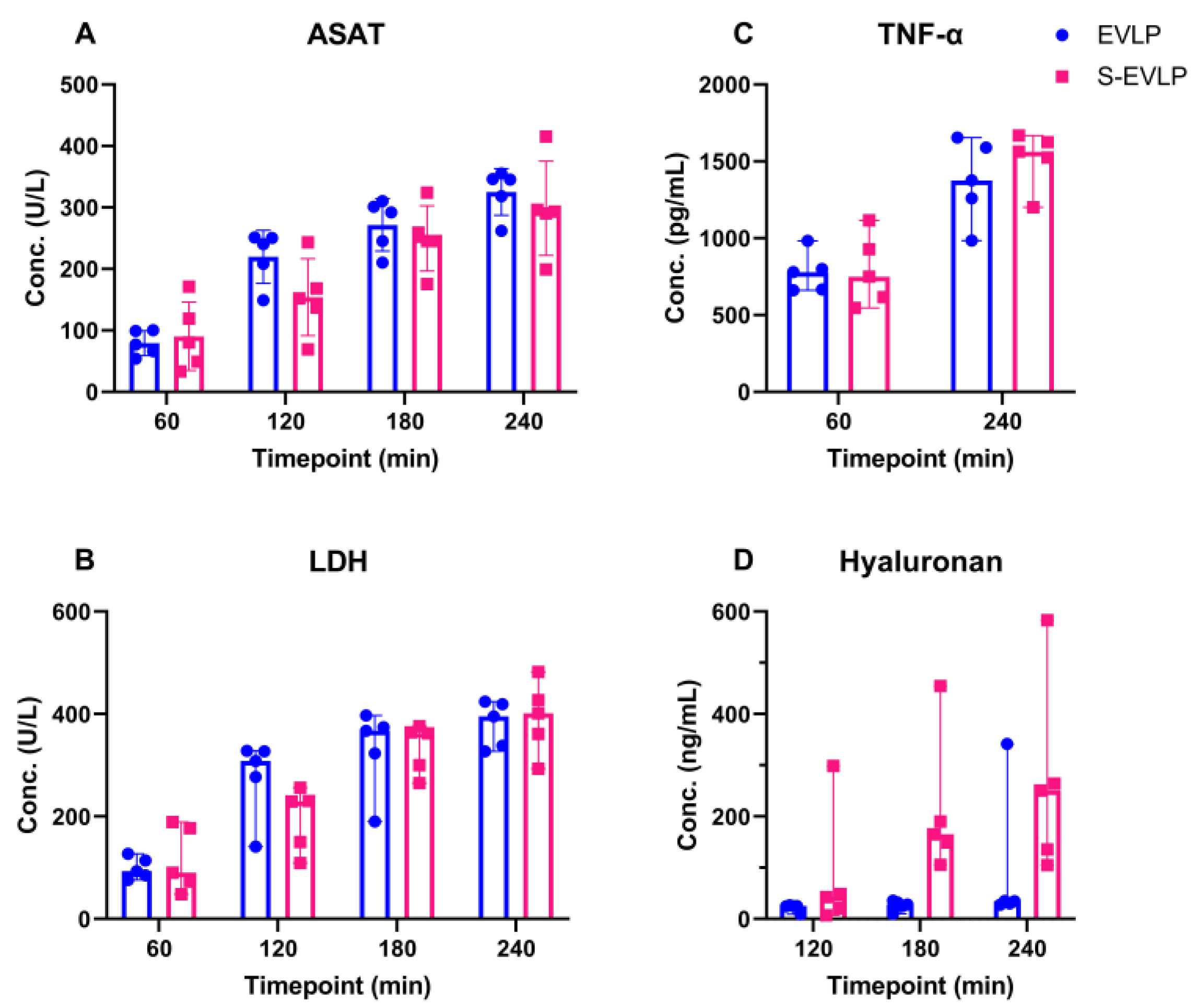
2.4. Perfusate Analysis
2.5. Gene Expression of Cytokines in Tissue Samples
3. Discussion
4. Materials and Methods
4.1. Animal Model and Treatment Groups
4.2. Inclusion/Exclusion Criteria
4.3. Samples
4.4. Data and Sample Measurements
4.4.1. Sevoflurane Measurements
4.4.2. Functional Lung Evaluation and Lung Edema Measurement
4.4.3. Biochemical Analyses
4.4.4. RNA Isolation and Gene Expression Analysis
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Raemdonck, D.; Neyrinck, A.; Cypel, M.; Keshavjee, S. Ex-vivo lung perfusion. Transpl. Int. 2014, 28, 643–656. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Cypel, M. Ex-vivo lung perfusion and ventilation: Where to from here? Curr. Opin. Organ Transplant. 2019, 24, 297–304. [Google Scholar] [CrossRef]
- Cypel, M.; Yeung, J.C.; Liu, M.; Anraku, M.; Chen, F.; Karolak, W.; Sato, M.; Laratta, J.; Azad, S.; Madonik, M.; et al. Normothermic Ex Vivo Lung Perfusion in Clinical Lung Transplantation. N. Engl. J. Med. 2011, 364, 1431–1440. [Google Scholar] [CrossRef]
- Yeung, J.C.; Krueger, T.; Yasufuku, K.; de Perrot, M.; Pierre, A.F.; Waddell, T.K.; Singer, L.G.; Keshavjee, S.; Cypel, M. Outcomes after transplantation of lungs preserved for more than 12 h: A retrospective study. Lancet Respir. Med. 2017, 5, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Aigner, C.; Slama, A.; Hötzenecker, K.; Scheed, A.; Urbanek, B.; Schmid, W.; Nierscher, F.J.; Lang, G.; Klepetko, W. Clinical Ex Vivo Lung Perfusion—Pushing the Limits. Am. J. Transplant. 2012, 12, 1839–1847. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, R.S.; Andrade, C.F. Oxidative Stress and Lung Ischemia-Reperfusion Injury. Oxidative Med. Cell. Longev. 2015, 2015, 590987. [Google Scholar] [CrossRef]
- Laubach, V.E.; Sharma, A.K. Mechanisms of lung ischemia-reperfusion injury. Curr. Opin. Organ Transplant. 2016, 21, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.K.; LaPar, D.J.; Zhao, Y.; Li, L.; Lau, C.L.; Kron, I.L.; Iwakura, Y.; Okusa, M.D.; Laubach, V.E. Natural Killer T Cell–derived IL-17 Mediates Lung Ischemia–Reperfusion Injury. Am. J. Respir. Crit. Care Med. 2011, 183, 1539–1549. [Google Scholar] [CrossRef]
- Fiser, S.M.; Tribble, C.G.; Long, S.M.; Kaza, A.K.; Cope, J.T.; Laubach, V.E.; Kern, J.A.; Kron, I.L. Lung transplant reperfusion injury involves pulmonary macrophages and circulating leukocytes in a biphasic response. J. Thorac. Cardiovasc. Surg. 2001, 121, 1069–1075. [Google Scholar] [CrossRef]
- Welbourn, C.R.B.; Goldman, G.; Paterson, I.S.; Valeri, C.R.; Shepro, D.; Hechtman, H.B. Pathophysiology of ischaemia reperfusion injury: Central role of the neutrophil. Br. J. Surg. 1991, 78, 651–655. [Google Scholar] [CrossRef]
- Chatterjee, S.; Nieman, G.F.; Christie, J.D.; Fisher, A.B. Shear stress-related mechanosignaling with lung ischemia: Lessons from basic research can inform lung transplantation. Am. J. Physiol. Lung Cell. Mol. Physiol. 2014, 307, L668–L680. [Google Scholar] [CrossRef]
- Bonanni, A.; Signori, A.; Alicino, C.; Mannucci, I.; Grasso, M.A.; Martinelli, L.; Deferrari, G. Volatile Anesthetics versus Propofol for Cardiac Surgery with Cardiopulmonary Bypass: Meta-analysis of Randomized Trials. Anesthesiology 2020, 132, 1429–1446. [Google Scholar] [CrossRef] [PubMed]
- Figueira, E.R.R.; Rocha-Filho, J.A.; Lanchotte, C.; Coelho, A.M.M.; Nakatani, M.; Tatebe, E.R.; Lima, J.A.V.; Mendes, C.O.; de Araujo, B.C.R.P.; Abdo, E.E.; et al. Sevoflurane Preconditioning plus Postconditioning Decreases Inflammatory Response with Hemodynamic Recovery in Experimental Liver Ischemia Reperfusion. Gastroenterol. Res. Pract. 2019, 2019, 5758984. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.T.; Chen, S.W.C.; Doetschman, T.C.; Deng, C.; D’Agati, V.D.; Kim, M. Sevoflurane protects against renal ischemia and reperfusion injury in mice via the transforming growth factor-β1 pathway. Am. J. Physiol. Ren. Physiol. 2008, 295, F128–F136. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zhu, Y.-M.; Gao, X.; Ni, Y.; Li, W.; Kent, T.A.; Qiao, S.-G.; Wang, C.; Xu, X.-X.; Zhang, H.-L. Sevoflurane postconditioning attenuates reactive astrogliosis and glial scar formation after ischemia–reperfusion brain injury. Neuroscience 2017, 356, 125–141. [Google Scholar] [CrossRef] [PubMed]
- Wen, X.-R.; Fu, Y.-Y.; Liu, H.-Z.; Wu, J.; Shao, X.-P.; Zhang, X.-B.; Tang, M.; Shi, Y.; Ma, K.; Zhang, F.; et al. Neuroprotection of Sevoflurane Against Ischemia/Reperfusion-Induced Brain Injury Through Inhibiting JNK3/Caspase-3 by Enhancing Akt Signaling Pathway. Mol. Neurobiol. 2016, 53, 1661–1671. [Google Scholar] [CrossRef] [PubMed]
- Ohsumi, A.; Marseu, K.; Slinger, P.; McRae, K.; Kim, H.; Guan, Z.; Hwang, D.M.; Liu, M.; Keshavjee, S.; Cypel, M. Sevoflurane Attenuates Ischemia-Reperfusion Injury in a Rat Lung Transplantation Model. Ann. Thorac. Surg. 2017, 103, 1578–1586. [Google Scholar] [CrossRef] [PubMed]
- Casanova, J.; Simon, C.; Vara, E.; Sanchez, G.; Rancan, L.; Abubakra, S.; Calvo, A.; Gonzalez, F.J.; Garutti, I. Sevoflurane anesthetic preconditioning protects the lung endothelial glycocalyx from ischemia reperfusion injury in an experimental lung autotransplant model. J. Anesth. 2016, 30, 755–762. [Google Scholar] [CrossRef] [PubMed]
- Casanova, J.; Garutti, I.; Simon, C.; Giraldez, A.; Martin, B.; Gonzalez, G.; Azcarate, L.; Garcia, C.; Vara, E. The Effects of Anesthetic Preconditioning with Sevoflurane in an Experimental Lung Autotransplant Model in Pigs. Anesth. Analg. 2011, 113, 742–748. [Google Scholar] [CrossRef]
- Yamada, Y.; Laube, I.; Jang, J.H.; Bonvini, J.M.; Inci, I.; Weder, W.; Beck Schimmer, B.; Jungraithmayr, W. Sevoflurane pre-conditioning protects from posttransplant injury in mouse lung transplantation. J. Surg. Res. 2017, 214, 270–277. [Google Scholar] [CrossRef]
- Wang, X.; Parapanov, R.; Francioli, C.; Perentes, J.Y.; Letovanec, I.; Gonzalez, M.; Kern, C.; Ris, H.-B.; Piquilloud, L.; Marcucci, C.; et al. Experimental ex vivo lung perfusion with sevoflurane: Effects on damaged donor lung grafts. Interact. Cardiovasc. Thorac. Surg. 2018, 26, 977–984. [Google Scholar] [CrossRef] [PubMed]
- Andrews, D.T.; Royse, C.F.; Royse, A.G. The Mitochondrial Permeability Transition Pore and its Role in Anaesthesia-Triggered Cellular Protection during Ischaemia-Reperfusion Injury. Anaesth. Intensive Care 2012, 40, 46–70. [Google Scholar] [CrossRef] [PubMed]
- Argaud, L.; Gateau-Roesch, O.; Raisky, O.; Loufouat, J.; Robert, D.; Ovize, M. Postconditioning Inhibits Mitochondrial Permeability Transition. Circulation 2005, 111, 194–197. [Google Scholar] [CrossRef] [PubMed]
- Annecke, T.; Chappell, D.; Chen, C.; Jacob, M.; Welsch, U.; Sommerhoff, C.; Rehm, M.; Conzen, P.; Becker, B. Sevoflurane preserves the endothelial glycocalyx against ischaemia–reperfusion injury. Br. J. Anaesth. 2010, 104, 414–421. [Google Scholar] [CrossRef]
- Chappell, D.; Heindl, B.; Jacob, M.; Annecke, T.; Chen, C.; Rehm, M.; Conzen, P.; Becker, B.F. Sevoflurane Reduces Leukocyte and Platelet Adhesion after Ischemia-Reperfusion by Protecting the Endothelial Glycocalyx. Anesthesiology 2011, 115, 483–491. [Google Scholar] [CrossRef]
- Chen, C.; Chappell, D.; Annecke, T.; Conzen, P.; Jacob, M.; Welsch, U.; Zwissler, B.; Becker, B.F. Sevoflurane mitigates shedding of hyaluronan from the coronary endothelium, also during ischemia/reperfusion: An ex vivo animal study. Hypoxia 2016, 4, 81–90. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Yang, L.; Xie, P.; Wu, J.; Yu, J.; Yu, T.; Wang, H.; Wang, J.; Xia, Z.; Zheng, H. Sevoflurane postconditioning improves myocardial mitochondrial respiratory function and reduces myocardial ischemia-reperfusion injury by up-regulating HIF-1. Am. J. Transl. Res. 2016, 8, 4415–4424. [Google Scholar]
- Yuki, K.; Eckenhoff, R.G. Mechanisms of the Immunological Effects of Volatile Anesthetics: A Review. Anesth. Analg. 2016, 123, 326–335. [Google Scholar] [CrossRef]
- Oshima, Y.; Otsuki, A.; Endo, R.; Nakasone, M.; Harada, T.; Takahashi, S.; Inagaki, Y. The Effects of Volatile Anesthetics on Lung Ischemia-Reperfusion Injury: Basic to Clinical Studies. J. Surg. Res. 2021, 260, 325–344. [Google Scholar] [CrossRef]
- De la Torre, M.; Gonzalez-Rivas, D.; Fernández-Prado, R.; Delgado, M.; Fieira, E.M.; Centeno, A. Uniportal video-assisted thoracoscopic lobectomy in the animal model. J. Thorac. Dis. 2014, 6, 656. [Google Scholar] [CrossRef]
- Korman, B.; Dash, R.K.; Peyton, P.J. Elucidating the roles of solubility and ventilation-perfusion mismatch in the second gas effect using a two-step model of gas exchange. J. Appl. Physiol. 2020, 128, 1587–1593. [Google Scholar] [CrossRef]
- Di Nardo, M.; Del Sorbo, L.; Sage, A.; Ma, J.; Liu, M.; Yeung, J.C.; Valero, J.; Ghany, R.; Cypel, M.; Keshavjee, S. Predicting donor lung acceptance for transplant during ex vivo lung perfusion: The EX vivo lung PerfusIon pREdiction (EXPIRE). Am. J. Transplant. 2021, 21, 3704–3713. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Cypel, M.; Keshavjee, S. Ex vivo lung perfusion. J. Thorac. Dis. 2021, 13, 6602–6617. [Google Scholar] [CrossRef]
- Tobias, J.D. Therapeutic applications and uses of inhalational anesthesia in the pediatric intensive care unit. Pediatr. Crit. Care Med. 2008, 9, 169–179. [Google Scholar] [CrossRef]
- Nieuwenhuijs-Moeke, G.J.; Bosch, D.J.; Leuvenink, H.G. Molecular Aspects of Volatile Anesthetic-Induced Organ Protection and Its Potential in Kidney Transplantation. Int. J. Mol. Sci. 2021, 22, 2727. [Google Scholar] [CrossRef]
- Lonati, C.; Bassani, G.A.; Brambilla, D.; Leonardi, P.; Carlin, A.; Faversani, A.; Gatti, S.; Valenza, F. Influence of ex vivo perfusion on the biomolecular profile of rat lungs. FASEB J. 2018, 32, 5532–5549. [Google Scholar] [CrossRef]
- Lonati, C.; Bassani, G.A.; Brambilla, D.; Leonardi, P.; Carlin, A.; Maggioni, M.; Zanella, A.; Dondossola, D.; Fonsato, V.; Grange, C.; et al. Mesenchymal stem cell–derived extracellular vesicles improve the molecular phenotype of isolated rat lungs during ischemia/reperfusion injury. J. Heart Lung Transplant. 2019, 38, 1306–1316. [Google Scholar] [CrossRef]
- Sladden, T.M.; Yerkovich, S.; Wall, D.; Tan, M.; Hunt, W.; Hill, J.; Smith, I.; Hopkins, P.; Chambers, D.C. Endothelial Glycocalyx Shedding Occurs during Ex Vivo Lung Perfusion: A Pilot Study. J. Transplant. 2019, 2019, 6748242. [Google Scholar] [CrossRef] [PubMed]
- Syrjälä, S.O.; Nykänen, A.I.; Tuuminen, R.; Raissadati, A.; Keränen, M.A.I.; Arnaudova, R.; Krebs, R.; Koh, G.Y.; Alitalo, K.; Lemström, K.B. Donor Heart Treatment With COMP-Ang1 Limits Ischemia-Reperfusion Injury and Rejection of Cardiac Allografts. Am. J. Transplant. 2015, 15, 2075–2084. [Google Scholar] [CrossRef]
- Syrjälä, S.O.; Tuuminen, R.; Nykänen, A.I.; Raissadati, A.; Dashkevich, A.; Keränen, M.A.I.; Arnaudova, R.; Krebs, R.; Leow, C.C.; Saharinen, P.; et al. Angiopoietin-2 Inhibition Prevents Transplant Ischemia-Reperfusion Injury and Chronic Rejection in Rat Cardiac Allografts. Am. J. Transplant. 2014, 14, 1096–1108. [Google Scholar] [CrossRef]
- Medeiros, I.L.; Pêgo-Fernandes, P.M.; Mariani, A.W.; Fernandes, F.G.; Unterpertinger, F.D.V.; Canzian, M.; Jatene, F.B. Histologic and functional evaluation of lungs reconditioned by ex vivo lung perfusion. J. Heart Lung Transplant. 2012, 31, 305–309. [Google Scholar] [CrossRef]
- Molin, S.Z.D.; Kruel, C.R.; de Fraga, R.S.; Alboim, C.; de Oliveira, J.R.; Alvares-Da-Silva, M.R. Differential protective effects of anaesthesia with sevoflurane or isoflurane: An animal experimental model simulating liver transplantation. Eur. J. Anaesthesiol. 2014, 31, 695–700. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.T.; Ota-Setlik, A.; Fu, Y.; Nasr, S.H.; Emala, C.W. Differential Protective Effects of Volatile Anesthetics against Renal Ischemia–Reperfusion Injury In Vivo. Anesthesiology 2004, 101, 1313–1324. [Google Scholar] [CrossRef] [PubMed]
- Muheet; Malik, H.U.; Parray, O.R.; Bhat, R.A.; Yatoo, M.I. Seasonal and periodic rhythmicity of respiratory infections in small ruminants. Biol. Rhythm. Res. 2020, 51, 1066–1074. [Google Scholar] [CrossRef]
- Zhang, Z.L.; Moeslund, N.; Hu, M.A.; Hoffmann, R.; Venema, L.H.; Van De Wauwer, C.; Timens, W.; Okamoto, T.; Verschuuren, E.A.M.; Leuvenink, H.G.D.; et al. Establishing an economical and widely accessible donation after circulatory death animal abattoir model for lung research using ex vivo lung perfusion. Artif. Organs 2022, 46, 2179–2190. [Google Scholar] [CrossRef]
- Bourdeaux, D.; Sautou-Miranda, V.; Montagner, A.; Perbet, S.; Constantin, J.M.; Bazin, J.-E.; Chopineau, J. Simple assay of plasma sevoflurane and its metabolite hexafluoroisopropanol by headspace GC–MS. J. Chromatogr. B 2010, 878, 45–50. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Sheep Weight (kg) | WIT (min) | SCS (min) | EVLP Duration (min) | Achieved % of Max Flow |
|---|---|---|---|---|---|
| EVLP | 41.6 (41.6/46.0) | 20 (18/26) | 180 | 240 (240/250) | 92.4 (81.1/96.5) |
| S-EVLP | 46.0 (38.4/51.2) | 22 (21/26) | 180 (180/190) | 245 (240/250) | 92.9 (47.7/110.8) |
| p value | 0.421 | 0.690 | 0.310 | 0.548 | >0.99 |
| Variables | S-EVLP | EVLP | p Value |
|---|---|---|---|
| ∆pO2 (kPa) | 3.8 (−4.9/11.1) | −11.7 (−12.0/−3.2) | 0.151 |
| P/F ratio after 4 h EVLP (mmHg) | 437 (420/452) | 347 (341/415) | 0.056 |
| Lung weight gain (%) | 1.39 (−5.12/1.99) | 6.67 (−0.22/8.78) | >0.900 |
| ∆ fluid content (%) | −6.29 (−6.35/−5.18) | 1.24 (−3.31/2.43) | 0.548 |
| ΔPost–Pre EVLP | ΔPost–Pre S-EVLP | p-Value | |
|---|---|---|---|
| E-selectin | 0.019 (0.007, 0.067) | 0.016 (0.003, 0.074) | 0.691 |
| VCAM | 69.56 (29.66, 113.6) | 21.33 (15.99, 199.1) | 0.222 |
| ICAM-1 | 0.002 (−0.094, 0.048) | −0.005 (−1.020, 0.136) | 0.841 |
| PECAM-1 | 6.946 ± 26.79 | −9.957 ± 36.52 | 0.428 |
| VE cadherin | 9.354 ± 61.96 | −60.92 ± 104.5 | 0.232 |
| Ang1 | 0.254 ± 0.545 | −0.931 ± 0.991 | 0.047 |
| Ang2 | 0.531 ± 0.277 | −0.251 ± 0.839 | 0.083 |
| Tie2/TEK | 1.404 ± 8.391 | −6.371 ± 9.551 | 0.209 |
| IL-6 | 3.385 (0.449, 6.103) | 0.708 (0.394, 5.751) | 0.691 |
| TNF-α | 7.71 ± 5.462 | 2.299 ± 2.073 | 0.072 |
| MPO | 0.0004 (−0.0443, 0.0479) | −0.0198 (−0.3413, −0.0028) | 0.222 |
| HIF1a | 2.626 ± 3.406 | −1.202 ± 9.439 | 0.419 |
| VEGF-a | 1.441 ± 1.469 | 0.983 ± 3.035 | 0.769 |
| E-selectin | 0.019 (0.007, 0.067) | 0.016 (0.003, 0.074) | 0.691 |
| VCAM | 69.56 (29.66, 113.6) | 21.33 (15.99, 199.1) | 0.222 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steinkühler, T.; Yang, S.; Hu, M.A.; Jainandunsing, J.S.; Jager, N.M.; Erasmus, M.E.; Struys, M.M.R.F.; Bosch, D.J.; van Meurs, M.; Jabaudon, M.; et al. Ex Vivo Optimization of Donor Lungs with Inhaled Sevoflurane during Normothermic Ex Vivo Lung Perfusion (VITALISE): A Pilot and Feasibility Study in Sheep. Int. J. Mol. Sci. 2024, 25, 2413. https://doi.org/10.3390/ijms25042413
Steinkühler T, Yang S, Hu MA, Jainandunsing JS, Jager NM, Erasmus ME, Struys MMRF, Bosch DJ, van Meurs M, Jabaudon M, et al. Ex Vivo Optimization of Donor Lungs with Inhaled Sevoflurane during Normothermic Ex Vivo Lung Perfusion (VITALISE): A Pilot and Feasibility Study in Sheep. International Journal of Molecular Sciences. 2024; 25(4):2413. https://doi.org/10.3390/ijms25042413
Chicago/Turabian StyleSteinkühler, Timo, Shuqi Yang, Michiel A. Hu, Jayant S. Jainandunsing, Neeltina M. Jager, Michiel E. Erasmus, Michel M. R. F. Struys, Dirk J. Bosch, Matijs van Meurs, Matthieu Jabaudon, and et al. 2024. "Ex Vivo Optimization of Donor Lungs with Inhaled Sevoflurane during Normothermic Ex Vivo Lung Perfusion (VITALISE): A Pilot and Feasibility Study in Sheep" International Journal of Molecular Sciences 25, no. 4: 2413. https://doi.org/10.3390/ijms25042413
APA StyleSteinkühler, T., Yang, S., Hu, M. A., Jainandunsing, J. S., Jager, N. M., Erasmus, M. E., Struys, M. M. R. F., Bosch, D. J., van Meurs, M., Jabaudon, M., Richard, D., Timens, W., Leuvenink, H. G. D., & Nieuwenhuijs-Moeke, G. J. (2024). Ex Vivo Optimization of Donor Lungs with Inhaled Sevoflurane during Normothermic Ex Vivo Lung Perfusion (VITALISE): A Pilot and Feasibility Study in Sheep. International Journal of Molecular Sciences, 25(4), 2413. https://doi.org/10.3390/ijms25042413