
Protective Effect of Betulin on Streptozotocin–Nicotinamide-Induced Diabetes in Female Rats

 , ,
, ,  ,
, 
Abstract
1. Introduction
2. Results
2.1. Quantification of Betulin Content in the Emulsion during the Stability Test
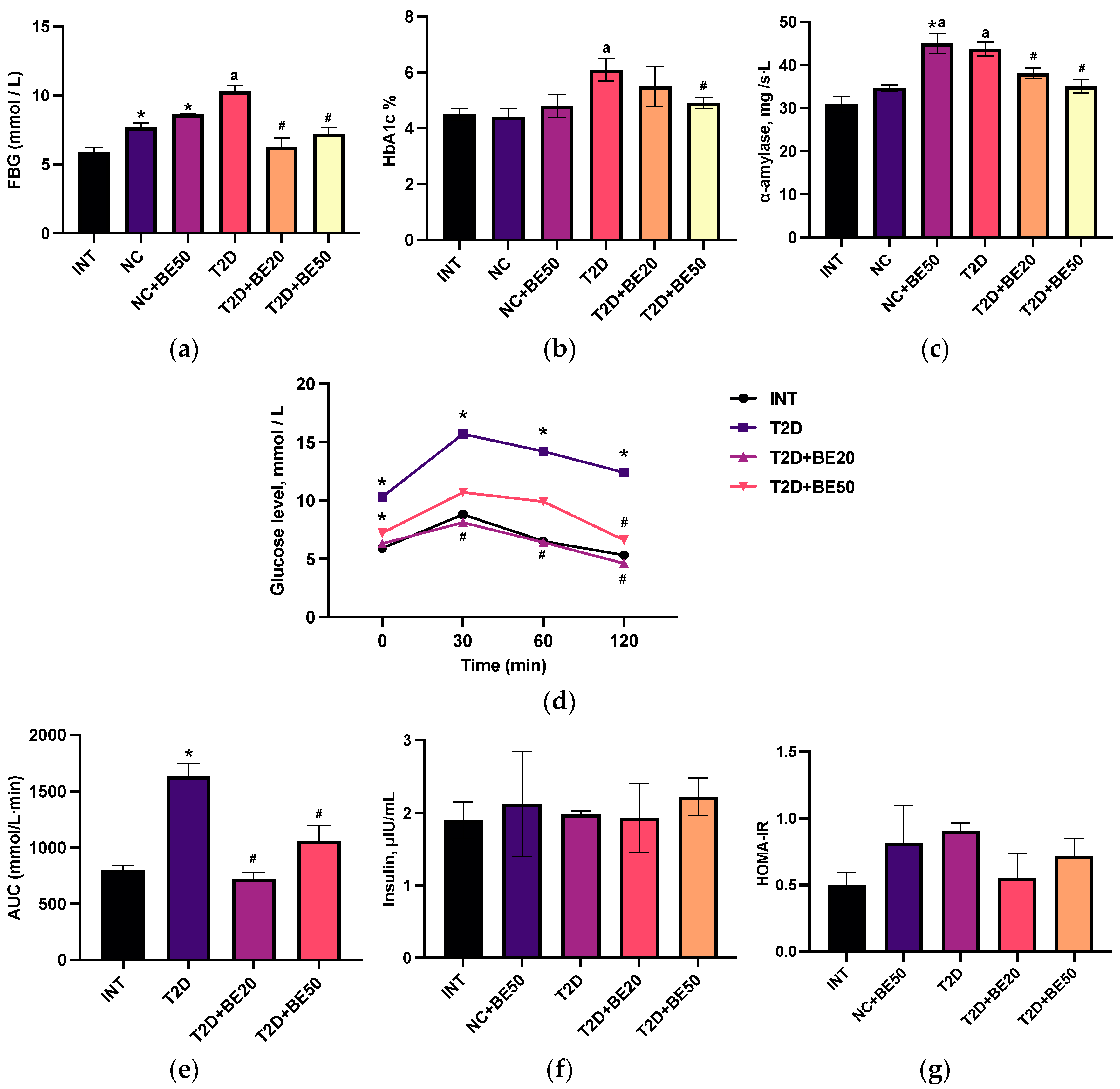
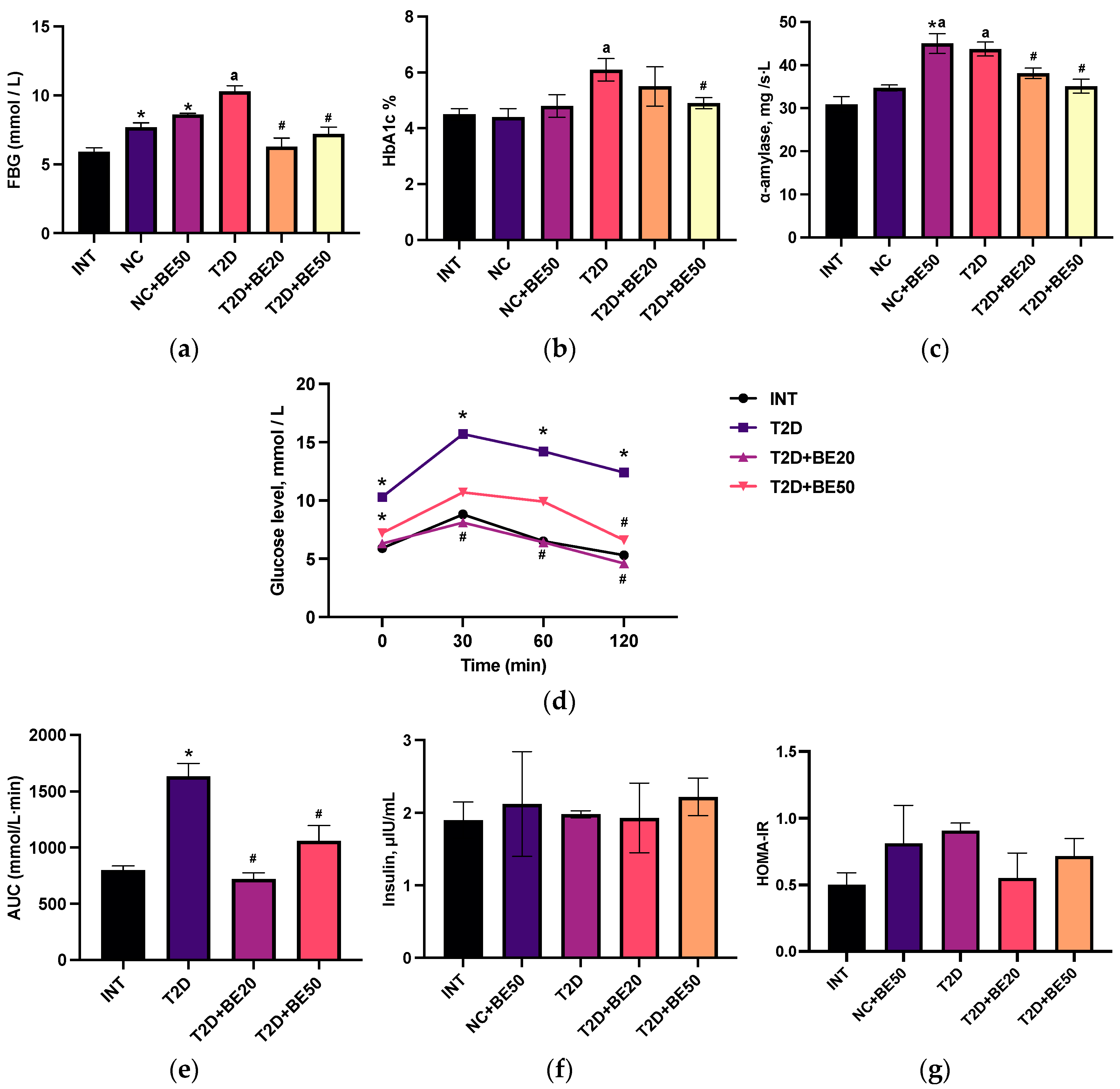
2.2. Effect of Betulin on Blood Glucose, Glycosylated Hemoglobin, α–Amylase, and Glucose Tolerance
2.3. Effect of Betulin on the Serum Insulin Concentration and Homeostatic Model Assessment for Insulin Resistance Score
2.4. Effect of Betulin on Hepatic and Renal Functions in Induced T2D
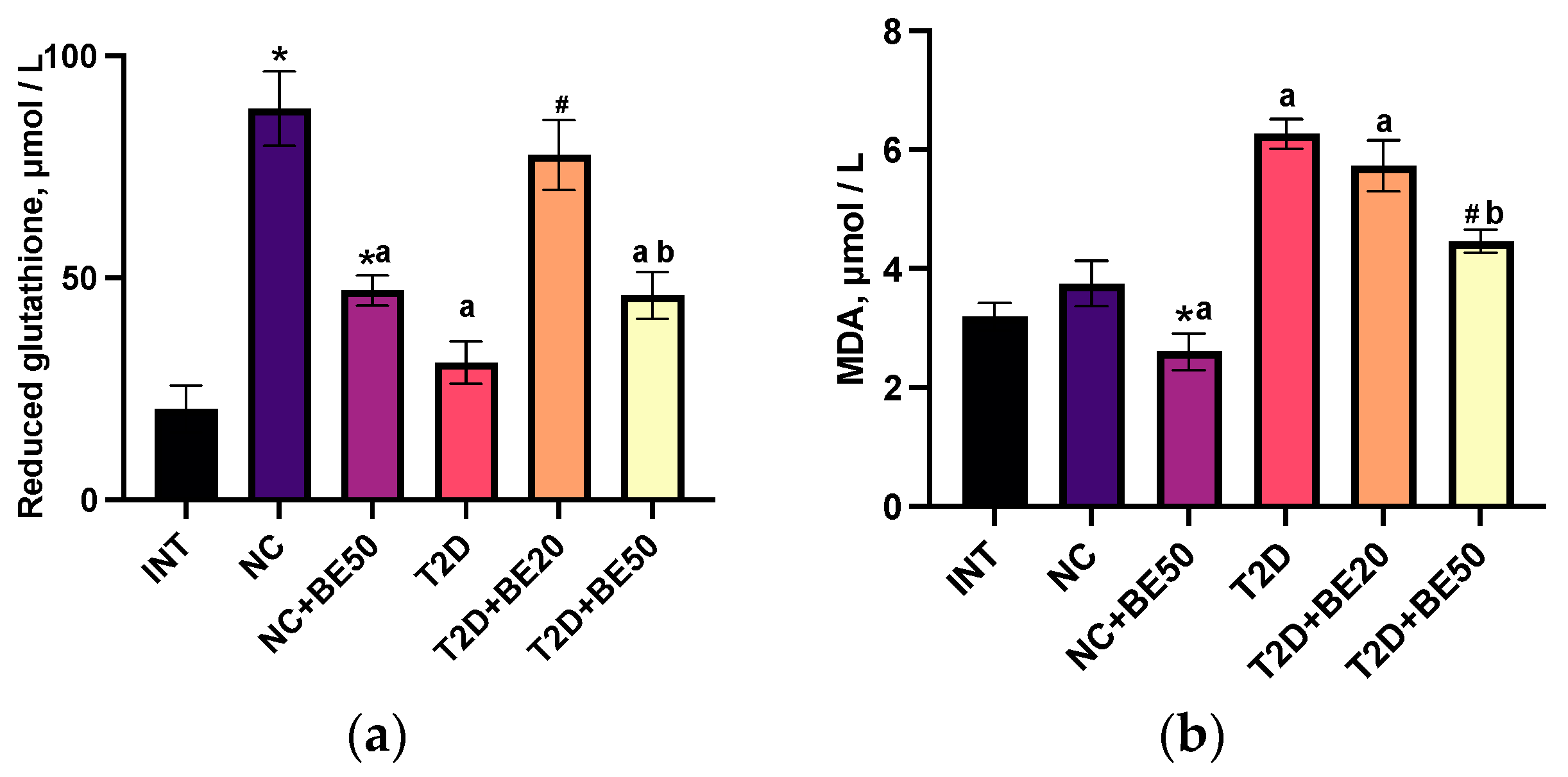
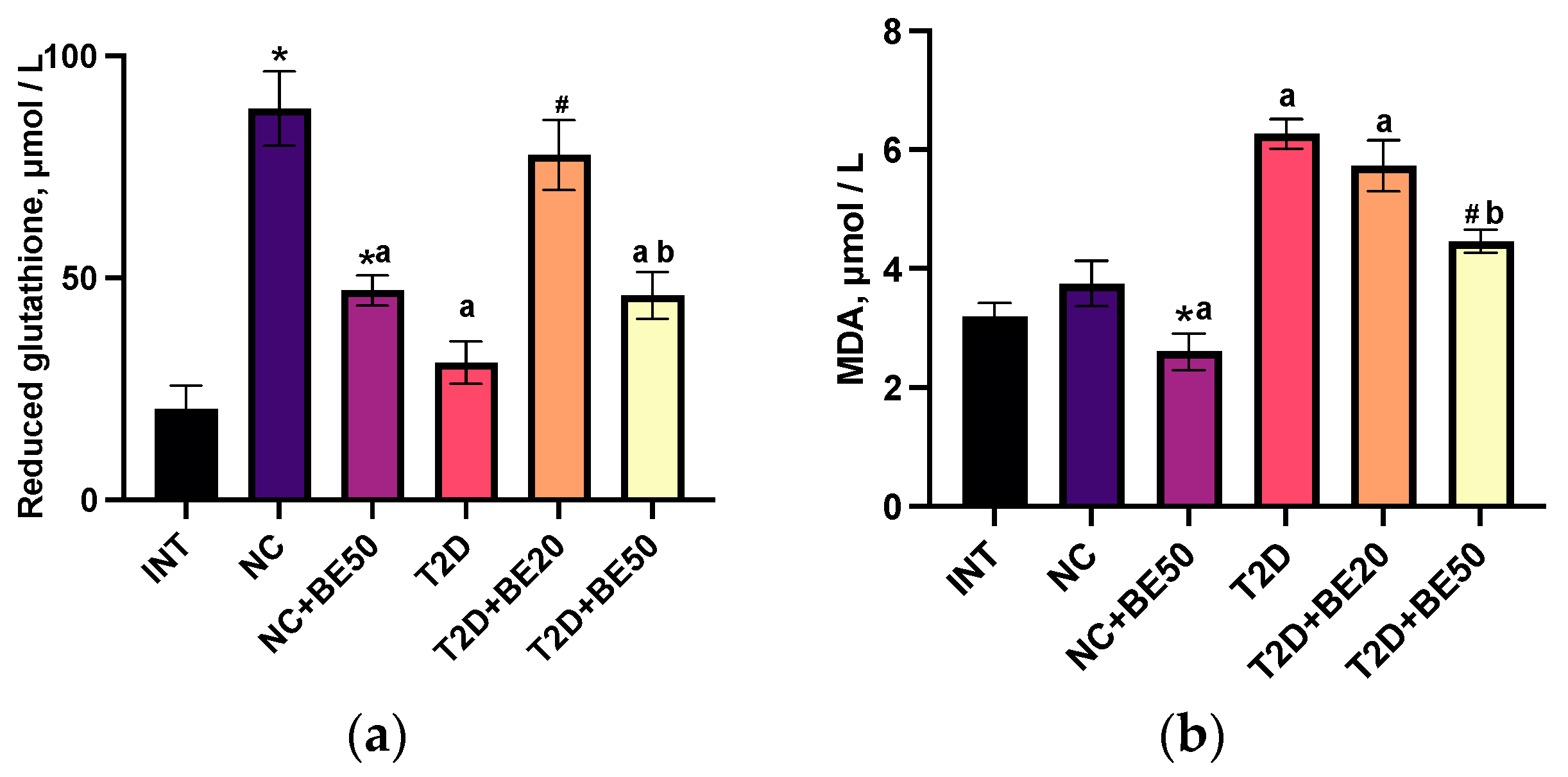
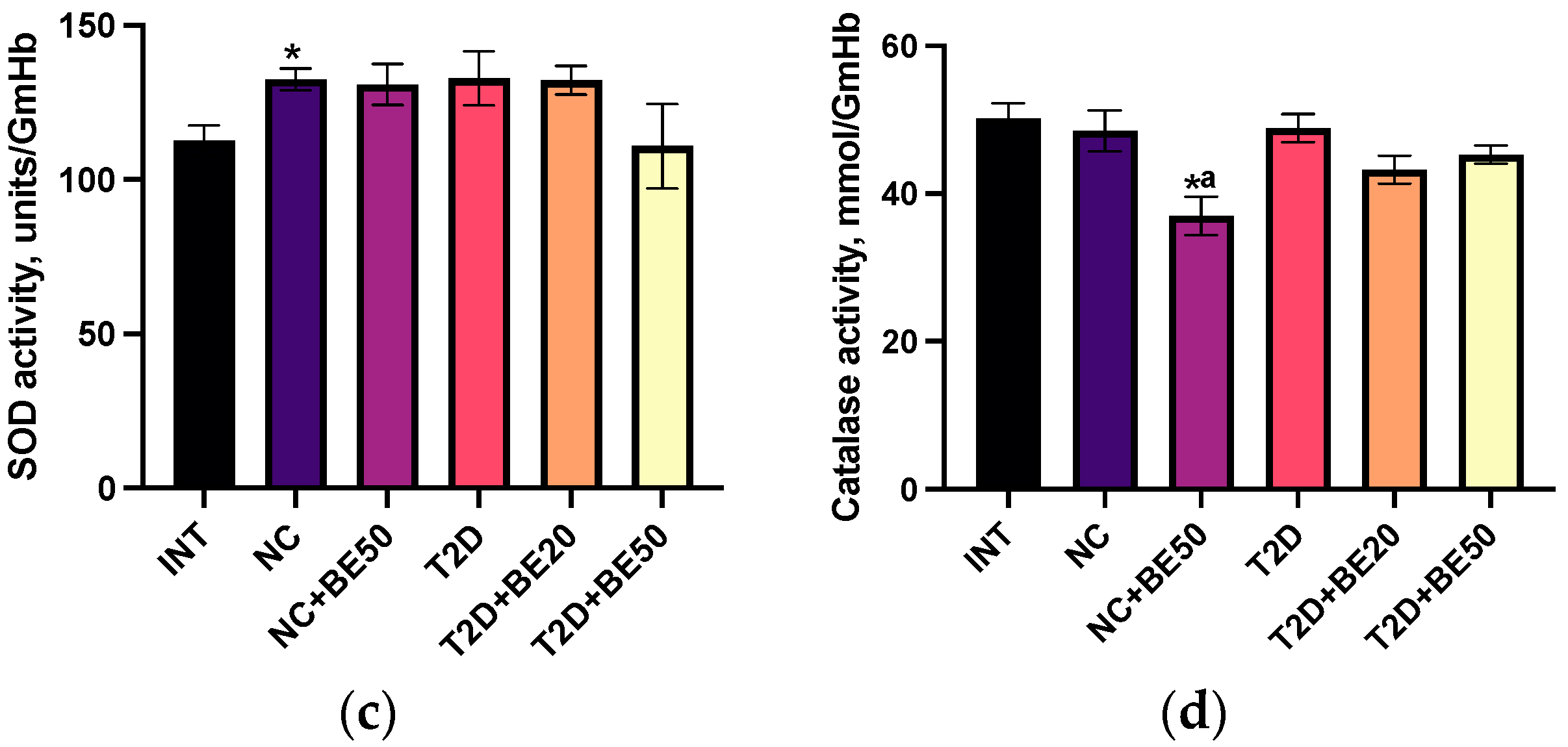
2.5. Effects of Betulin on Oxidative Stress Parameters
2.6. Effects of Betulin on Hematological Parameters
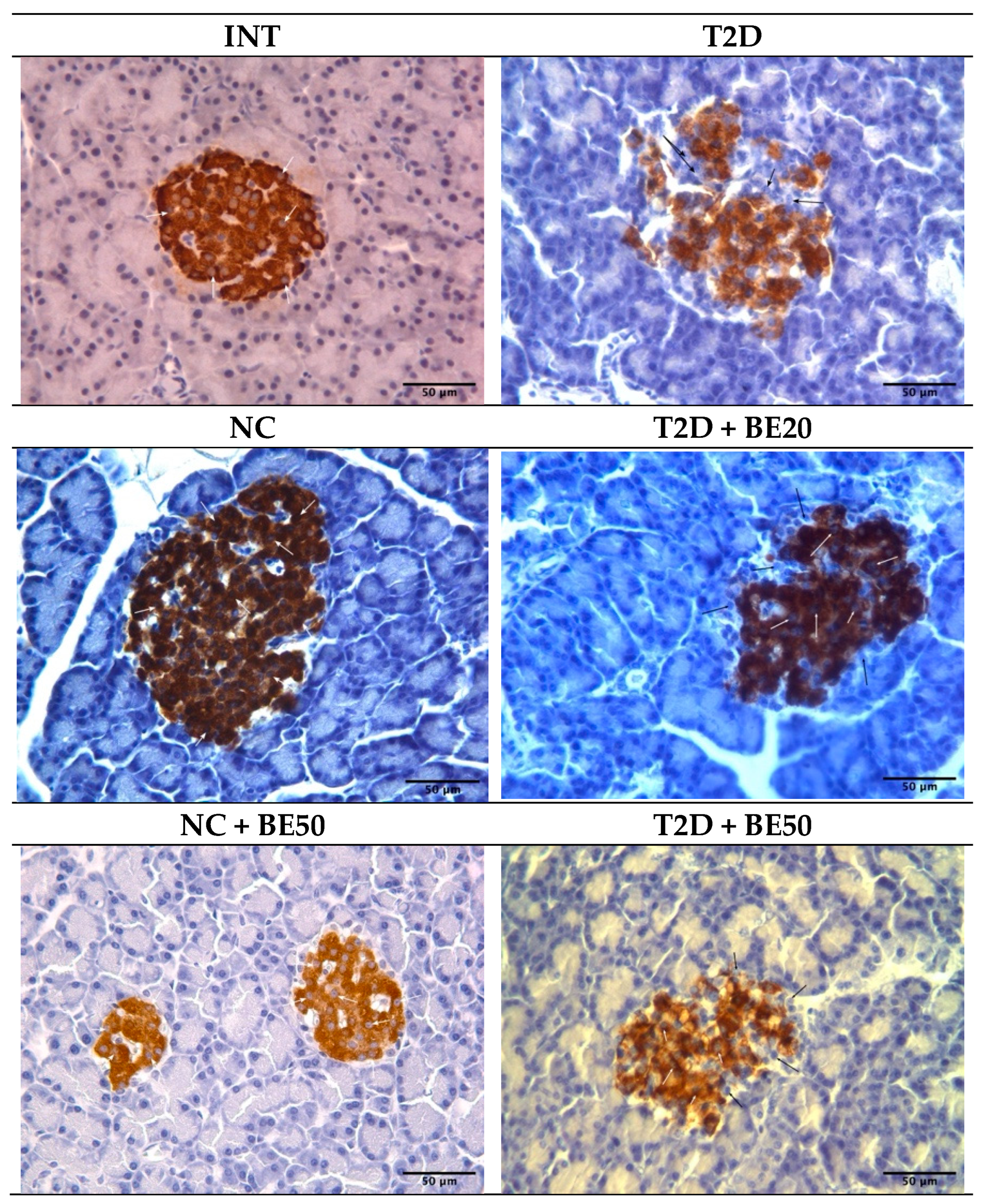
2.7. Effect of Betulin on Pancreatic Islet β–Cells
3. Discussion
4. Materials and Methods
4.1. Preparation of Betulin Emulsion
4.2. HPLC Validation of Betulin in Emulsions
4.3. Animal Model and Betulin Treatment
4.4. Experimental Animals and Design
4.5. Fasting Blood Glucose, Oral Glucose Tolerance Test, and Glycated Hemoglobin
4.6. Insulin Levels and Homeostatic Model Assessment for Insulin Resistance
4.7. Determination of Oxidative Stress Parameters
4.8. Hepatic and Renal Function Parameters
4.9. Hematological Parameter Determination
4.10. Immunohistochemical Evaluation of Pancreatic Tissues
4.11. Morphometric Analysis
4.12. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas 2021; IDF Diabetes Atlas: Brussels, Belgium, 2021. [Google Scholar]
- Szkudelski, T. Streptozotocin-Nicotinamide-Induced Diabetes in the Rat. Characteristics of the Experimental Model. Exp. Biol. Med. 2012, 237, 481–490. [Google Scholar] [CrossRef]
- Birgani, G.A.; Ahangarpour, A.; Khorsandi, L.; Moghaddam, H.F. Anti-Diabetic Effect of Betulinic Acid on Streptozotocin- Nicotinamide Induced Diabetic Male Mouse Model. Braz. J. Pharm. Sci. 2018, 54, 1–7. [Google Scholar] [CrossRef]
- Duru, K.C.; Mukhlynina, E.A.; Moroz, G.A.; Gette, I.F.; Danilova, I.G.; Kovaleva, E.G. Anti-Diabetic Effect of Isoflavone Rich Kudzu Root Extract in Experimentally Induced Diabetic Rats. J. Funct. Foods 2020, 68, 103922. [Google Scholar] [CrossRef]
- Najafian, M. The Effects of Curcumin on Alpha Amylase in Diabetics Rats. Zahedan J. Res. Med. Sci. 2015, in press. [CrossRef]
- Nazaruk, J.; Borzym-Kluczyk, M. The Role of Triterpenes in the Management of Diabetes Mellitus and Its Complications. Phytochem. Rev. 2015, 14, 675–690. [Google Scholar] [CrossRef]
- Tan, M.J.; Ye, J.M.; Turner, N.; Hohnen-Behrens, C.; Ke, C.Q.; Tang, C.P.; Chen, T.; Weiss, H.C.; Gesing, E.R.; Rowland, A.; et al. Antidiabetic Activities of Triterpenoids Isolated from Bitter Melon Associated with Activation of the AMPK Pathway. Chem. Biol. 2008, 15, 263–273. [Google Scholar] [CrossRef]
- Perumal, P.; Dhanasundaram, S.; Aravinth, A.; Kamaraj, C.; Santhanam, P.; Rajaram, R. In Vitro Evaluation of the Anticancer Potential of Betulin, Isolated from the Seaweed Sargassum Ilicifolium, against Hep-2, THP-1 and HeLa Cell Lines. S. Afr. J. Bot. 2023, 163, 443–456. [Google Scholar] [CrossRef]
- Barakat, K.; Saleh, M. Bioactive Betulin Produced by Marine Paecilomyces WE3-F. J. Appl. Pharm. Sci. 2016, 6, 34–40. [Google Scholar] [CrossRef]
- Adepoju, F.O.; Duru, K.C.; Li, E.; Kovaleva, E.G.; Tsurkan, M.V. Pharmacological Potential of Betulin as a Multitarget Compound. Biomolecules 2023, 13, 1105. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.; Cai, X.; Liu, X.; Liu, J.; Zhu, N. Betulin Alleviates Myocardial Ischemia–Reperfusion Injury in Rats via Regulating the Siti1/NLRP3/NF-κB Signaling Pathway. Inflammation 2021, 44, 1096–1107. [Google Scholar] [CrossRef] [PubMed]
- Wen, Y.; Geng, L.; Zhou, L.; Pei, X.; Yang, Z.; Ding, Z. Betulin Alleviates on Myocardial Inflammation in Diabetes Mice via Regulating Siti1/NLRP3/NF-κB Pathway. Int. Immunopharmacol. 2020, 85, 106653. [Google Scholar] [CrossRef] [PubMed]
- Alsaadi, J.H. Hussien. Isolation, Purification and Identification of Active Chemical Compound Lup-20(29)-Ene-3, 28-Diol (Betulin) from Tetradium Daniellii Leaves and Study the Hypoglycemic Effect on Rabbits. Univ. Thi-Qar J. Sci. 2016, 6, 54–61. [Google Scholar] [CrossRef]
- Tang, J.J.; Li, J.G.; Qi, W.; Qiu, W.W.; Li, P.S.; Li, B.L.; Song, B.L. Inhibition of SREBP by a Small Molecule, Betulin, Improves Hyperlipidemia and Insulin Resistance and Reduces Atherosclerotic Plaques. Cell Metab. 2011, 13, 44–56. [Google Scholar] [CrossRef]
- Sakaguchi, K.; Takeda, K.; Maeda, M.; Ogawa, W.; Sato, T.; Okada, S.; Ohnishi, Y.; Nakajima, H.; Kashiwagi, A. Glucose Area under the Curve during Oral Glucose Tolerance Test as an Index of Glucose Intolerance. Diabetol. Int. 2016, 7, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Masiello, P.; Broca, C.; Gross, R.; Roye, M.; Manteghetti, M.; Hillaire-Buys, D.; Novelli, M.; Ribes, G. Experimental NIDDM: Development of a New Model in Adult Rats Administered Streptozotocin and Nicotinamide. Diabetes 1998, 47, 224–229. [Google Scholar] [CrossRef]
- Wu, J.T. Review of Diabetes: Identification of Markers for Early Detection, Glycemic Control, and Monitoring Clinical Complications. J. Clin. Lab. Anal. 1993, 7, 293–300. [Google Scholar] [CrossRef]
- Poovitha, S.; Parani, M. In Vitro and in Vivo α-Amylase and α-Glucosidase Inhibiting Activities of the Protein Extracts from Two Varieties of Bitter Gourd (Momordica charantia L.). BMC Complement. Altern. Med. 2016, 16, 185. [Google Scholar] [CrossRef]
- Ko, B.S.; Kang, S.; Moon, B.R.; Ryuk, J.A.; Park, S. A 70% Ethanol Extract of Mistletoe Rich in Betulin, Betulinic Acid, and Oleanolic Acid Potentiated β-Cell Function and Mass and Enhanced Hepatic Insulin Sensitivity. Evid.-Based Complement. Altern. Med. 2016, 2016, 7836823. [Google Scholar] [CrossRef]
- Zhao, X.; Wang, W.; Zu, Y.; Zhang, Y.; Li, Y.; Sun, W.; Shan, C.; Ge, Y. Preparation and Characterization of Betulin Nanoparticles for Oral Hypoglycemic Drug by Antisolvent Precipitation. Drug Deliv. 2014, 21, 467–479. [Google Scholar] [CrossRef]
- Ma, C.; Long, H. Protective Effect of Betulin on Cognitive Decline in Streptozotocin (STZ)-Induced Diabetic Rats. Neurotoxicology 2016, 57, 104–111. [Google Scholar] [CrossRef]
- Ratna Wulan, D.; Priyo Utomo, E.; Mahdi, C. Antidiabetic Activity of Ruellia tuberosa L., Role of α-Amylase Inhibitor: In Silico, In Vitro, and In Vivo Approaches. Biochem. Res. Int. 2015, 2015, 349261. [Google Scholar] [CrossRef] [PubMed]
- Harris, E.H. Elevated Liver Function Tests in Type 2 Diabetes. Clin. Diabetes 2005, 23, 115–119. [Google Scholar] [CrossRef]
- Mandal, A.; Bhattarai, B.; Kafle, P.; Khalid, M.; Jonnadula, S.K.; Lamicchane, J.; Kanth, R.; Gayam, V. Elevated Liver Enzymes in Patients with Type 2 Diabetes Mellitus and Non-Alcoholic Fatty Liver Disease. Cureus 2018, 10, e3626. [Google Scholar] [CrossRef] [PubMed]
- Ahangarpour, A.; Shabani, R.; Farbood, Y. The Effect of Betulinic Acid on Leptin, Adiponectin, Hepatic Enzyme Levels and Lipid Profiles in Streptozotocin-Nicotinamide-Induced Diabetic Mice. Res. Pharm. Sci. 2018, 13, 142. [Google Scholar] [CrossRef] [PubMed]
- Besseling, P.J.; Pieters, T.T.; Nguyen, I.T.N.; de Bree, P.M.; Willekes, N.; Dijk, A.H.; Bovee, D.M.; Hoorn, E.J.; Rookmaaker, M.B.; Gerritsen, K.G.; et al. A Plasma Creatinine- And Urea-Based Equation to Estimate Glomerular Filtration Rate in Rats. Am. J. Physiol. Renal. Physiol. 2021, 320, F518–F524. [Google Scholar] [CrossRef] [PubMed]
- Hernández, F. Glycolysis and Gluconeogenesis: A Teaching View. J. Biol. Chem. 2021, 296, 100016. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Song, G.C.; Weng, F.Y.; Zou, B.; Jin, J.Y.; Yan, D.M.; Tan, B.; Zhao, J.; Li, Y.; Qiu, F.R. Hepatoprotective Effects of Glycyrrhetinic Acid on Lithocholic Acid-Induced Cholestatic Liver Injury Through Choleretic and Anti-Inflammatory Mechanisms. Front. Pharmacol. 2022, 13, 881231. [Google Scholar] [CrossRef] [PubMed]
- Nowotny, K.; Jung, T.; Höhn, A.; Weber, D.; Grune, T. Advanced Glycation End Products and Oxidative Stress in Type 2 Diabetes Mellitus. Biomolecules 2015, 5, 194–222. [Google Scholar] [CrossRef]
- Yin, W.; Luo, S.; Xiao, Z.; Zhang, Z.; Liu, B.; Zhou, Z. Latent Autoimmune Diabetes in Adults: A Focus on β-Cell Protection and Therapy. Front. Endocrinol. 2022, 13, 959011. [Google Scholar] [CrossRef]
- Ikegami, H.; Babaya, N.; Noso, S. β-Cell Failure in Diabetes: Common Susceptibility and Mechanisms Shared between Type 1 and Type 2 Diabetes. J. Diabetes Investig. 2021, 12, 1526–1539. [Google Scholar] [CrossRef]
- Klöppel, G.; Löhr, M.; Habich, K.; Oberholzer, M.; Heitz, P.U. Islet Pathology and the Pathogenesis of Type 1 and Type 2 Diabetes Mellitus Revisited. Surv. Synth. Pathol. Res. 1985, 4, 110–125. [Google Scholar] [CrossRef]
- Khataylou, Y.J.; Afshar, S.A.; Mirzakhani, N. Betulinic Acid Reduces the Complications of Autoimmune Diabetes on the Body and Kidney through Effecting on Inflammatory Cytokines in C57BL/6 Mice. Vet. Res. Forum 2021, 12, 203. [Google Scholar] [CrossRef]
- Zhao, H.; Zheng, Q.; Hu, X.; Shen, H.; Li, F. Betulin Attenuates Kidney Injury in Septic Rats through Inhibiting TLR4/NF-κB Signaling Pathway. Life Sci. 2016, 144, 185–193. [Google Scholar] [CrossRef]
- Hu, H.C.; Lei, Y.H.; Zhang, W.H.; Luo, X.Q. Antioxidant and Anti-Inflammatory Properties of Resveratrol in Diabetic Nephropathy: A Systematic Review and Meta-Analysis of Animal Studies. Front. Pharmacol. 2022, 13, 841818. [Google Scholar] [CrossRef]
- Zheng, Z.; Yin, Y.; Lu, R.; Jiang, Z. Lycopene Ameliorated Oxidative Stress and Inflammation in Type 2 Diabetic Rats. J. Food Sci. 2019, 84, 1194–1200. [Google Scholar] [CrossRef]
- Buko, V.; Kuzmitskaya, I.; Kirko, S.; Belonovskaya, E.; Naruta, E.; Lukivskaya, O.; Shlyahtun, A.; Ilyich, T.; Zakreska, A.; Zavodnik, I. Betulin Attenuated Liver Damage by Prevention of Hepatic Mitochondrial Dysfunction in Rats with Alcoholic Steatohepatitis. Physiol. Int. 2019, 106, 323–334. [Google Scholar] [CrossRef]
- Kamaraj, Y.; Dhayalan, S.; Chinnaiyan, U.; Kumaresan, V.; Subramaniyan, S.; Kumar, D.; Muniyandi, K.; Punamalai, G. Triterpenoid Compound Betulin Attenuates Allergic Airway Inflammation by Modulating Antioxidants, Inflammatory Cytokines and Tissue Transglutaminase in Ovalbumin-Induced Asthma Mice Model. J. Pharm. Pharmacol. 2021, 73, 968–978. [Google Scholar] [CrossRef] [PubMed]
- Kruszniewska-Rajs, C.; Strzałka-Mrozik, B.; Kimsa-Dudek, M.; Synowiec-Wojtarowicz, A.; Chrobak, E.; Bębenek, E.; Boryczka, S.; Głuszek, S.; Gola, J.M. The Influence of Betulin and Its Derivatives EB5 and ECH147 on the Antioxidant Status of Human Renal Proximal Tubule Epithelial Cells. Int. J. Mol. Sci. 2022, 23, 2524. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Jiang, H.; Yang, J.; Jin, M.; Du, Y.; Sun, Q.; Cao, L.; Xu, H. Safety Assessment and Antioxidant Evaluation of Betulin by LC-MS Combined with Free Radical Assays. Anal. Biochem. 2019, 587, 113460. [Google Scholar] [CrossRef] [PubMed]
- Arkew, M.; Yemane, T.; Mengistu, Y.; Gemechu, K.; Tesfaye, G. Hematological Parameters of Type 2 Diabetic Adult Patients at Debre Berhan Referral Hospital, Northeast Ethiopia: A Comparative Cross-Sectional Study. PLoS ONE 2021, 16, 0253286. [Google Scholar] [CrossRef] [PubMed]
- Mahdiani, A.; Kheirandish, M.; Bonakdaran, S. Correlation Between White Blood Cell Count and Insulin Resistance in Type 2 Diabetes. Curr. Diabetes Rev. 2018, 15, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Shin, A.; Connolly, S.; Kabytaev, K. Protein Glycation in Diabetes Mellitus. In Advances in Clinical Chemistry; Elsevier: Amsterdam, The Netherlands, 2023; Volume 113. [Google Scholar]
- Twig, G.; Afek, A.; Shamiss, A.; Derazne, E.; Tzur, D.; Gordon, B.; Tirosh, A. White Blood Cells Count and Incidence of Type 2 Diabetes in Young Men. Diabetes Care 2013, 36, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Abreu, J.S.; Takahashi, L.S.; Hoshiba, M.A.; Urbinati, E.C. Biological Indicators of Stress in Pacu (Piaractus mesopotamicus) after Capture. Braz. J. Biol. 2009, 69, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Maes, M.; Van Der Planken, M.; Van Gastel, A.; Bruyland, K.; Van Hunsel, F.; Neels, H.; Hendriks, D.; Wauters, A.; Demedts, P.; Janca, A.; et al. Influence of Academic Examination Stress on Hematological Measurements in Subjectively Healthy Volunteers. Psychiatry Res. 1998, 80, 201–212. [Google Scholar] [CrossRef] [PubMed]
- Günther, A.; Makuch, E.; Nowak, A.; Duchnik, W.; Kucharski, Ł.; Pełech, R.; Klimowicz, A. Enhancement of the Antioxidant and Skin Permeation Properties of Betulin and Its Derivatives. Molecules 2021, 26, 3435. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.W.; Xing, Y.; Wen, C.; Yu, X.X.; Sun, W.L.; Xiu, Z.L.; Dong, Y. sheng Pentacyclic Triterpenes as α-Glucosidase and α-Amylase Inhibitors: Structure-Activity Relationships and the Synergism with Acarbose. Bioorg. Med. Chem. Lett. 2017, 27, 5065–5070. [Google Scholar] [CrossRef] [PubMed]
- Amiri, S.; Dastghaib, S.; Ahmadi, M.; Mehrbod, P.; Khadem, F.; Behrouj, H.; Aghanoori, M.R.; Machaj, F.; Ghamsari, M.; Rosik, J.; et al. Betulin and Its Derivatives as Novel Compounds with Different Pharmacological Effects. Biotechnol. Adv. 2020, 38, 107409. [Google Scholar] [CrossRef]
- Zavorokhina, N.V.; Pankratieva, N.A.; Goncharova, N.A. Betulin Nanosuspension as a Promising Raw Material for the Production of Long-Term Storage Bread. IOP Conf. Ser. Earth Environ. Sci. 2020, 548, 082017. [Google Scholar] [CrossRef]
- EUR-Lex-32010L006-EN -EUR-Lex. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=celex%3A32010L0063 (accessed on 9 December 2023).
- Zakrzeska, A.; Kitlas, P.; Shlyahtun, A.; Krasińska, N.; Jabłoński, R.; Tomulewicz, M. Hypoglycemic Effect of Betulin in Rats with Experimental Diabetes. Acta Pol. Pharm. 2023, 80, 795. [Google Scholar] [CrossRef]
- Danilova, I.G.; Bulavintceva, T.S.; Gette, I.F.; Yu, S.; Emelyanov, V.V.; Abidov, M.T. Partial Recovery from Alloxan-Induced Diabetes by Sodium Phthalhydrazide in Rats. Biomed. Pharmacother. 2017, 95, 103–110. [Google Scholar] [CrossRef]
- Feizi, A.; Meamar, R.; Eslamian, M.; Amini, M.; Nasri, M.; Iraj, B. Area under the Curve during OGTT in First-Degree Relatives of Diabetic Patients as an Efficient Indicator of Future Risk of Type 2 Diabetes and Prediabetes. Clin. Endocrinol. 2017, 87, 696–705. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis Model Assessment: Insulin Resistance and β-Cell Function from Fasting Plasma Glucose and Insulin Concentrations in Man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Rukmini, M.S.; D’Souza, B.; D’Souza, V. Superoxide Dismutase and Catalase Activities and Their Correlation with Malondialdehyde in Schizophrenic Patients. Indian J. Clin. Biochem. 2004, 19, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Beauchamp, C.; Fridovich, I. Superoxide Dismutase: Improved Assays and an Assay Applicable to Acrylamide Gels. Anal. Biochem. 1971, 44, 276–287. [Google Scholar] [CrossRef] [PubMed]
- Verevkina, I.V.; Tochilkin, A.I.; Popova, N.A. Colorimetric Method for Determining SH Groups and SS Bonds in Proteins Using 5, 5-Dithiobis (2-Nitrobenzoic) Acid. Mod. Methods Biochem.–M. Med. 1977, 1, 223–231. [Google Scholar]
- Ohkawa, H.; Ohishi, N.; Yagi, K. Assay for Lipid Peroxides in Animal Tissues by Thiobarbituric Acid Reaction. Anal. Biochem. 1979, 95, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Kaur, N.; Kumar, V.; Nayak, S.K.; Wadhwa, P.; Kaur, P.; Sahu, S.K. Alpha-Amylase as Molecular Target for Treatment of Diabetes Mellitus: A Comprehensive Review. Chem. Biol. Drug Des. 2021, 98, 539–560. [Google Scholar] [CrossRef] [PubMed]
- Antony Samy, J.V.R.; Kumar, N.; Singaravel, S.; Krishnamoorthy, R.; Alshuniaber, M.A.; Gatasheh, M.K.; Venkatesan, A.; Natesan, V.; Kim, S.J. Effect of Prunetin on Streptozotocin-Induced Diabetic Nephropathy in Rats—A Biochemical and Molecular Approach. Biomol. Ther. 2023, 31, 619. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Aspartate Aminotransferase µmol/min∙L | Alanine Aminotransferase µmol/min∙L | Alkaline Phosphatase µmol/min∙L | Total Protein g/L | Urea mmol/L | Creatinine µmol/L | |
|---|---|---|---|---|---|---|
| INT | 16.1 ± 0.6 | 12.6 ± 0.6 | 51.5 ± 3.3 | 70.5 ± 1.3 | 5.2 ± 0.2 | 62.3 ± 1.5 |
| NC | 18.5 ± 0.8 | 12.8 ± 0.7 | 48.5 ± 4.3 | 67.3 ± 2.2 | 5.9 ± 0.3 | 60.2 ± 1.7 |
| NC + BE50 | 17.4 ± 1.7 | 13.1 ± 0.8 | 32.0 ± 2.4 *,a | 67.6 ± 1.3 | 5.2 ± 0.4 | 64.3 ± 1.6 |
| T2D | 24.7 ± 1.7 a | 18.6 ± 1.2 a | 40.8 ± 4.0 | 64.3 ± 2.1 | 7.9 ± 0.4 a | 67.7 ± 0.7 a |
| T2D + BE20 | 21.7 ± 1.4 | 13.6 ± 0.8 # | 30.4 ± 1.4 a,# | 62.1 ± 1.6 | 7.0 ± 0.3 a | 68.0 ± 3.3 a |
| T2D + BE50 | 20.2 ± 2.6 | 11.3 ± 1.4 # | 27.6 ± 1.7 a,# | 68.0 ± 1.5 b | 5.8 ± 0.1 #,b | 64.3 ± 1.9 |
| Parameter | INT | NC | NC + BE50 | T2D | T2D + BE20 | T2D + BE50 |
|---|---|---|---|---|---|---|
| Leukocytes (×103/µL) | 7.73 ± 0.41 | 7.71 ± 0.43 | 6.18 ± 0.57 | 7.61 ± 0.56 | 7.98 ± 0.83 | 6.74 ± 0.58 |
| Lymphocytes (×103/µL) | 5.10 ± 0.40 | 5.14 ± 0.48 | 4.18 ± 0.46 | 5.65 ± 0.48 | 6.16 ± 0.44 | 4.98 ± 0.52 |
| Mid-range cells (×103/µL) | 0.72 ± 0.18 | 0.74 ± 0.10 | 0.45 ± 0.09 | 0.95 ± 0.16 | 0.84 ± 0.13 # | 1.04 ± 0.10 # |
| Granulocytes (×103/µL) | 1.92 ± 0.42 | 1.53 ± 0.32 | 1.62 ± 0.24 | 1.63 ± 0.39 | 0.98 ± 0.38 | 0.72 ± 0.14 |
| Erythrocytes (×106/µL) | 8.01 ± 0.28 | 9.14 ± 0.22 * | 9.06 ± 0.20 * | 8.88 ± 0.32 | 8.54 ± 0.44 | 9.16 ± 0.27 |
| Hemoglobin (g/L) | 13.7 ± 0.4 | 16.2 ± 0.8 * | 15.1 ± 0.2 * | 16.2 ± 0.3 | 16.1 ± 0.7 | 17.2 ± 0.5 |
| Hematocrit (%) | 41.2 ± 1.2 | 43.4 ± 0.3 | 42.9 ± 0.7 | 43.8 ± 0.7 | 47.4 ± 2.7 | 45.7 ± 1.6 |
| MCH (pg) | 17.1 ± 0.3 | 17.5 ± 0.4 | 16.7 ± 0.4 | 18.7 ± 0.2 # | 18.9 ± 0.2 a | 18.7 ± 0.1 a |
| MCHC (g/dL) | 33.2 ± 0.5 | 35.8 ± 0.8 * | 35.3 ± 0.3 * | 36.6 ± 0.6 | 34.4 ± 0.7 | 37.6 ± 0.3 b |
| PLT (×103/µL) | 602.0 ± 26.7 | 487.7 ± 59.8 | 578.8 ± 57.8 | 565.8 ± 20.1 | 432.4 ± 65.7 | 529.0 ± 14.7 |
| Parameter | INT | NC | NC + BE50 | T2D | T2D + BE20 | T2D + BE50 |
|---|---|---|---|---|---|---|
| % of pancreatic islets with positive insulin staining | 100.00 ± 0.00 | 99.55 ± 0.45 | 100.00 ± 0.00 | 98.10 ± 1.31 | 93.53 ± 5.49 | 100.00 ± 0.00 |
| Number of pancreatic islets, N/mm2 | 4.19 ± 0.56 | 3.18 ± 0.24 | 2.38± 0.12 #,a | 1.53 ± 0.12 *,a | 2.45 ± 0.41 * | 3.34 ± 0.47 # |
| Area of pancreatic islet, mkm2 | 7426 ± 1331 | 9995 ± 726 | 7333.51 ± 1922 | 9083 ± 919 | 6699 ± 1153 | 6990.55 ± 1231 |
| % of IPC in the pancreatic islet | 79.71 ± 1.37 a | 85.63 ± 1.90 # | 93.77 ± 1.23 *,b,# | 57.22 ± 7.97 *,a | 65.83 ± 11.35 | 78.80 ± 2.11 # |
| Optical intensity of cytoplasm in IPC | 0.41 ± 0.03 | 0.63 ± 0.04 | 0.51 ± 0.07 | 0.47 ± 0.06 | 0.61 ± 0.03 | 0.54 ± 0.07 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adepoju, F.O.; Sokolova, K.V.; Gette, I.F.; Danilova, I.G.; Tsurkan, M.V.; Mondragon, A.C.; Kovaleva, E.G.; Miranda, J.M. Protective Effect of Betulin on Streptozotocin–Nicotinamide-Induced Diabetes in Female Rats. Int. J. Mol. Sci. 2024, 25, 2166. https://doi.org/10.3390/ijms25042166
Adepoju FO, Sokolova KV, Gette IF, Danilova IG, Tsurkan MV, Mondragon AC, Kovaleva EG, Miranda JM. Protective Effect of Betulin on Streptozotocin–Nicotinamide-Induced Diabetes in Female Rats. International Journal of Molecular Sciences. 2024; 25(4):2166. https://doi.org/10.3390/ijms25042166
Chicago/Turabian StyleAdepoju, Feyisayo O., Ksenia V. Sokolova, Irina F. Gette, Irina G. Danilova, Mikhail V. Tsurkan, Alicia C. Mondragon, Elena G. Kovaleva, and Jose Manuel Miranda. 2024. "Protective Effect of Betulin on Streptozotocin–Nicotinamide-Induced Diabetes in Female Rats" International Journal of Molecular Sciences 25, no. 4: 2166. https://doi.org/10.3390/ijms25042166
APA StyleAdepoju, F. O., Sokolova, K. V., Gette, I. F., Danilova, I. G., Tsurkan, M. V., Mondragon, A. C., Kovaleva, E. G., & Miranda, J. M. (2024). Protective Effect of Betulin on Streptozotocin–Nicotinamide-Induced Diabetes in Female Rats. International Journal of Molecular Sciences, 25(4), 2166. https://doi.org/10.3390/ijms25042166