
Thrombelastography and Conventional Coagulation Markers in Chronic Obstructive Pulmonary Disease: A Prospective Paired-Measurements Study Comparing Exacerbation and Stable Phases
 , ,
, ,  ,
,  , , , and
, , , and 
Abstract
1. Introduction
2. Results
2.1. Main Analysis
2.2. Sensitivity Analyses
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Sample Size
4.3. Study Participants
4.4. Study Material
4.5. Statistical Analysis
4.5.1. Main Analysis
4.5.2. Sensitivity Analysis
4.5.3. Data Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferrera, M.C.; Labaki, W.W.; Han, M.K. Advances in Chronic Obstructive Pulmonary Disease. Annu. Rev. Med. 2021, 72, 119–134. [Google Scholar] [CrossRef]
- Soler-Cataluna, J.J.; Martinez-Garcia, M.A.; Roman Sanchez, P.; Salcedo, E.; Navarro, M.; Ochando, R. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax 2005, 60, 925–931. [Google Scholar] [CrossRef]
- Anecchino, C.; Rossi, E.; Fanizza, C.; De Rosa, M.; Tognoni, G.; Romero, M.; Working Group ARNO Project. Prevalence of chronic obstructive pulmonary disease and pattern of comorbidities in a general population. Int. J. Chron. Obs. Pulmon. Dis. 2007, 2, 567–574. [Google Scholar]
- (GOLD) GIfCOLD. Global Initiative for Chronic Obstructive Lung Disease (GOLD). 2023. Available online: https://goldcopd.org/ (accessed on 23 November 2023).
- (WHO) WHO. Chronic Obstructive Pulmonary Disease (COPD). 2023. Available online: https://www.nhs.uk/conditions/chronic-obstructive-pulmonary-disease-copd/ (accessed on 23 November 2023).
- Labaki, W.W.; Rosenberg, S.R. Chronic Obstructive Pulmonary Disease. Ann. Intern. Med. 2020, 173, ITC17–ITC32. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, A.I.; Wedzicha, J.A. Definition, Causes, Pathogenesis, and Consequences of Chronic Obstructive Pulmonary Disease Exacerbations. Clin. Chest Med. 2020, 41, 421–438. [Google Scholar] [CrossRef]
- Flattet, Y.; Garin, N.; Serratrice, J.; Perrier, A.; Stirnemann, J.; Carballo, S. Determining prognosis in acute exacerbation of COPD. Int. J. Chron. Obs. Pulmon. Dis. 2017, 12, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Maritano Furcada, J.; Castro, H.M.; De Vito, E.L.; Grande Ratti, M.F.; Posadas-Martinez, M.L.; Giunta, D.H.; Vazquez, F.J.; Ferreyro, B.L. Diagnosis of pulmonary embolism in patients with acute exacerbations of chronic obstructive pulmonary disease: A cross-sectional study. Clin. Respir. J. 2020, 14, 1176–1181. [Google Scholar] [CrossRef]
- MacLeod, M.; Papi, A.; Contoli, M.; Beghe, B.; Celli, B.R.; Wedzicha, J.A.; Fabbri, L.M. Chronic obstructive pulmonary disease exacerbation fundamentals: Diagnosis, treatment, prevention and disease impact. Respirology 2021, 26, 532–551. [Google Scholar] [CrossRef]
- Groenewegen, K.H.; Schols, A.M.; Wouters, E.F. Mortality and mortality-related factors after hospitalization for acute exacerbation of COPD. Chest 2003, 124, 459–467. [Google Scholar] [CrossRef]
- Rizkallah, J.; Man, S.F.P.; Sin, D.D. Prevalence of pulmonary embolism in acute exacerbations of COPD: A systematic review and metaanalysis. Chest 2009, 135, 786–793. [Google Scholar] [CrossRef]
- Gunen, H.; Gulbas, G.; In, E.; Yetkin, O.; Hacievliyagil, S.S. Venous thromboemboli and exacerbations of COPD. Eur. Respir. J. 2010, 35, 1243–1248. [Google Scholar] [CrossRef]
- Aleva, F.E.; Voets, L.; Simons, S.O.; de Mast, Q.; van der Ven, A.; Heijdra, Y.F. Prevalence and Localization of Pulmonary Embolism in Unexplained Acute Exacerbations of COPD: A Systematic Review and Meta-analysis. Chest 2017, 151, 544–554. [Google Scholar] [CrossRef]
- Dentali, F.; Pomero, F.; Micco, P.D.; La Regina, M.; Landini, F.; Mumoli, N.; Pieralli, F.; Giorgi-Pierfranceschi, M.; Re, R.; Vitale, J.; et al. Prevalence and risk factors for pulmonary embolism in patients with suspected acute exacerbation of COPD: A multi-center study. Eur. J. Intern. Med. 2020, 80, 54–59. [Google Scholar] [CrossRef]
- Couturaud, F.; Sanchez, O.; Bertoletti, L. Pulmonary Embolism Prevalence Among Hospitalized Patients with COPD-Reply. JAMA 2021, 325, 1903. [Google Scholar] [CrossRef] [PubMed]
- Meitei, S.P.; Tale, S.; Negi, A.K.; Dua, R.; Walia, R.; Saxena, S. Prevalence and characteristics of venous thromboembolism in severe exacerbation of chronic obstructive pulmonary disease in a tertiary care hospital in India. Monaldi Arch. Chest Dis. 2021, 91, 1742. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Jiao, X.; Gong, X.; Nie, Q.; Li, Y.; Zhen, G.; Cheng, M.; He, J.; Yuan, Y.; Yang, Y. Prevalence, Risk Factor and Clinical Characteristics of Venous Thrombus Embolism in Patients with Acute Exacerbation of COPD: A Prospective Multicenter Study. Int. J. Chron. Obs. Pulmon. Dis. 2023, 18, 907–917. [Google Scholar] [CrossRef] [PubMed]
- Burton, A.G.; Jandrey, K.E. Use of Thromboelastography in Clinical Practice. Vet Clin. N. Am. Small Anim. Pract. 2020, 50, 1397–1409. [Google Scholar] [CrossRef] [PubMed]
- Shaydakov, M.E.; Sigmon, D.F.; Blebea, J. Thromboelastography; StatPearls: Treasure Island, FL, USA, 2023. [Google Scholar]
- Zhou, Y.; Yu, J.; Zhou, H. Changes in Thrombelastography in Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease and the Relationship with Lung Function. Emerg. Med. Int. 2022, 2022, 4313394. [Google Scholar] [CrossRef]
- Chen, L.; Xu, W.; Chen, J.; Zhang, H.; Huang, X.; Ma, L.; Yu, G.; Zhou, Y.; Ma, B.; Chen, C.; et al. Evaluating the clinical role of fibrinogen, D-dimer, mean platelet volume in patients with acute exacerbation of COPD. Heart Lung 2023, 57, 54–58. [Google Scholar] [CrossRef]
- Ashitani, J.; Mukae, H.; Arimura, Y.; Matsukura, S. Elevated plasma procoagulant and fibrinolytic markers in patients with chronic obstructive pulmonary disease. Intern. Med. 2002, 41, 181–185. [Google Scholar] [CrossRef]
- Lankeit, M.; Held, M. Incidence of venous thromboembolism in COPD: Linking inflammation and thrombosis? Eur. Respir. J. 2016, 47, 369–373. [Google Scholar] [CrossRef]
- Sundhedsfaglige Portal, Lægehåndbogen. 2023. Available online: https://www.sundhed.dk/sundhedsfaglig/laegehaandbogen/undersoegelser-og-proever/klinisk-biokemi/blodproever/fibrin-d-dimer/ (accessed on 10 December 2023).
- Husebo, G.R.; Gabazza, E.C.; D’Alessandro Gabazza, C.; Yasuma, T.; Toda, M.; Aanerud, M.; Nielsen, R.; Bakke, P.S.; Eagan, T.M.L. Coagulation markers as predictors for clinical events in COPD. Respirology 2021, 26, 342–351. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Hu, R.; Jiang, X.; Mei, X. Coagulation dysfunction in patients with AECOPD and its relation to infection and hypercapnia. J. Clin. Lab. Anal. 2021, 35, e23733. [Google Scholar] [CrossRef] [PubMed]
- Kamstrup, P.; Rastoder, E.; Hellmann, P.H.; Sivapalan, P.; Larsen, E.L.; Vestbo, J.; Ulrik, C.S.; Goetze, J.P.; Knop, F.K.; Jensen, J.U.S. Effect of 10-Day Treatment with 50 mg Prednisolone Once-Daily on Haemostasis in Healthy Men-A Randomised Placebo-Controlled Trial. Biomedicines 2023, 11, 2052. [Google Scholar] [CrossRef] [PubMed]
- Wageck, B.; Cox, N.S.; Holland, A.E. Recovery Following Acute Exacerbations of Chronic Obstructive Pulmonary Disease—A Review. COPD 2019, 16, 93–103. [Google Scholar] [CrossRef]
- COPTRIN. The CODEX-P Trial (COPD Exacerbation and Pulmonary Hypertension Trial. 2022. Available online: http://coptrin.dk/wp-content/uploads/2022/10/aim3.pdf (accessed on 23 November 2023).
- Mads Andersen, M.K.E.a.M.K.P. Dansk Cardiologisk Selskab—Pulmonal Hypertension. 2023. Available online: https://nbv.cardio.dk/pah#133-diagnostik-og-undersgelser (accessed on 23 November 2023).
- Woodhams, B.; Girardot, O.; Blanco, M.J.; Colesse, G.; Gourmelin, Y. Stability of coagulation proteins in frozen plasma. Blood Coagul. Fibrinolysis 2001, 12, 229–236. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Number of Participants n = 100 | |
|---|---|
| Sex, n (%) | |
| Female | 66 (66) |
| Age, median (range) | 78.5 (70–82) |
| ≤62, n (%) | 11 (11) |
| 63–70, n (%) | 18 (18) |
| 71–77, n (%) | 24 (24) |
| ≥78, n (%) | 47 (47) |
| BMI, median (range) | 23.7 (20.8–29) |
| ≤18.4 kg/m2, n (%) | 18 (18) |
| 18.5–24.9 kg/m2, n (%) | 45 (45) |
| 25–30 kg/m2, n (%) | 16 (16) |
| >30 kg/m2, n (%) | 20 (20) |
| Missing value, n (%) | 1 (1) |
| Smoking status, n (%) | |
| Former smoker/non-smokers | 61 (61) |
| Current smokers | 38 (38) |
| Missing value | 1 (1) |
| GOLD stage, n (%) | |
| GOLD 1 | 3 (3) |
| GOLD 2 | 26 (26) |
| GOLD 3 | 47 (47) |
| GOLD 4 | 17 (17) |
| Missing value | 7 (7) |
| Comorbidities, n (%) | |
| Diabetes mellitus | 13 (13) |
| Asthma | 17 (17) |
| Atrial fibrillation | 18 (18) |
| Previous VTE | 7 (7) |
| Essential hypertension | 45 (45) |
| Previous cancer | 8 (8) |
| Medication, n (%) | |
| Antithrombotic treatment | 34 (34) |
| Anticoagulant therapy | 22 (22) |
| Antiplatelet therapy | 12 (12) |
| Anticoagulant therapy after enrolment * | 4 (4) |
| Number of Participants with Antithrombotic Treatment | |
|---|---|
| n = 34 | |
| Sex, n (%) | |
| Female | 22 (64.7) |
| Age, median (range) | 79.5 (72–82) |
| BMI, median (range) | 23.4 (21–29) |
| Smoking status, n (%) | |
| Former smoker/non-smoker | 21 (61.8) |
| Current smoker | 12 (35.3) |
| Missing value | 1 (2.9) |
| GOLD stage, n (%) | |
| GOLD 1 | 2 (5.9) |
| GOLD 2 | 11 (32.4) |
| GOLD 3 | 16 (47.1) |
| GOLD 4 | 2 (5.9) |
| Missing value | 3 (8.8) |
| Comorbidities, n (%) | |
| Diabetes mellitus | 5 (14.7) |
| Asthma | 7 (20.6) |
| Atrial fibrillation | 18 (52.9) |
| Previous VTE | 7 (20.6) |
| Essential hypertension | 21 (61.8) |
| Previous cancer | 3 (8.8) |
| Medication, n (%) | |
| Anticoagulant therapy | 22 (64.7) |
| Antiplatelet therapy | 12 (35.3) |
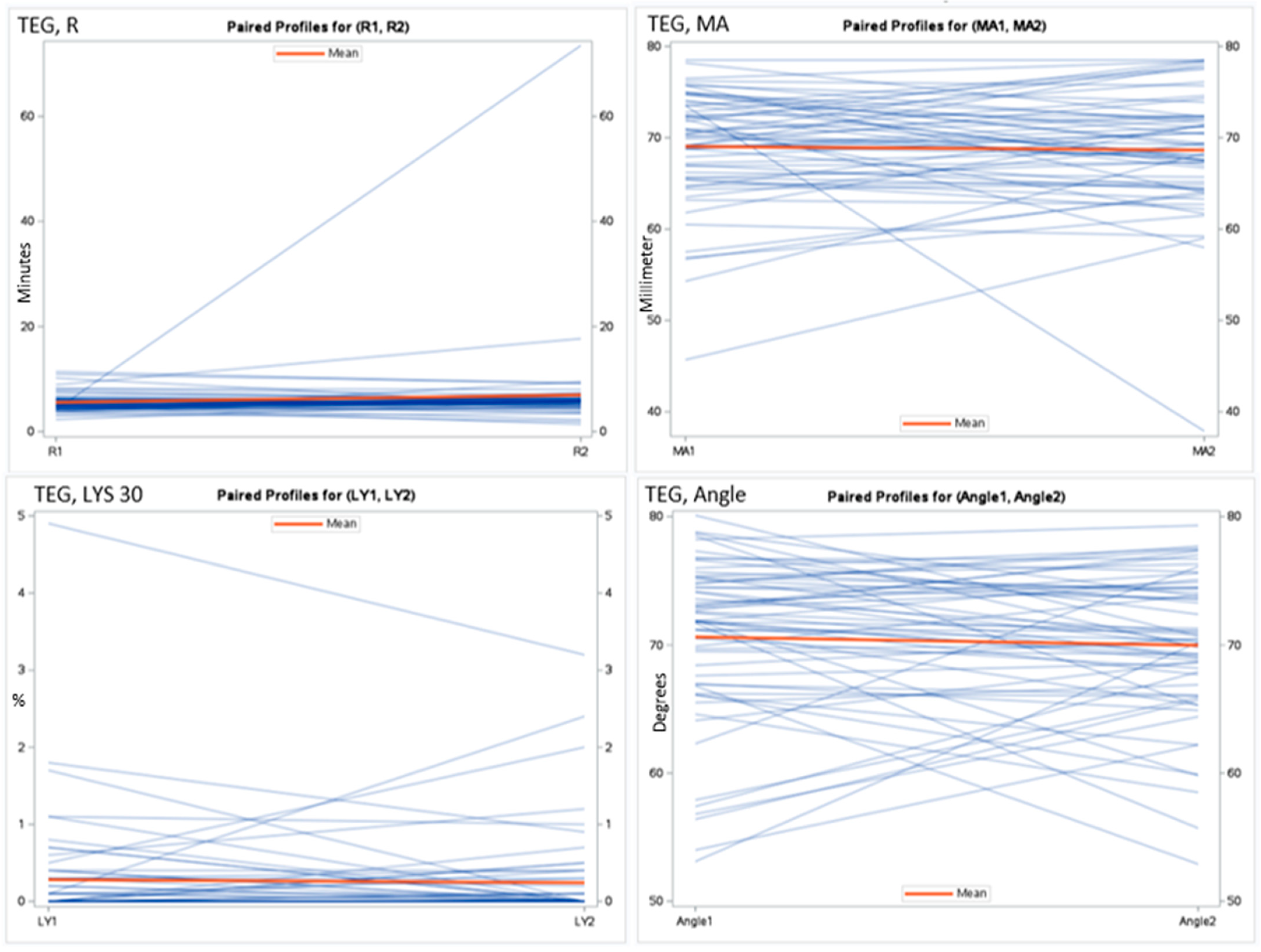
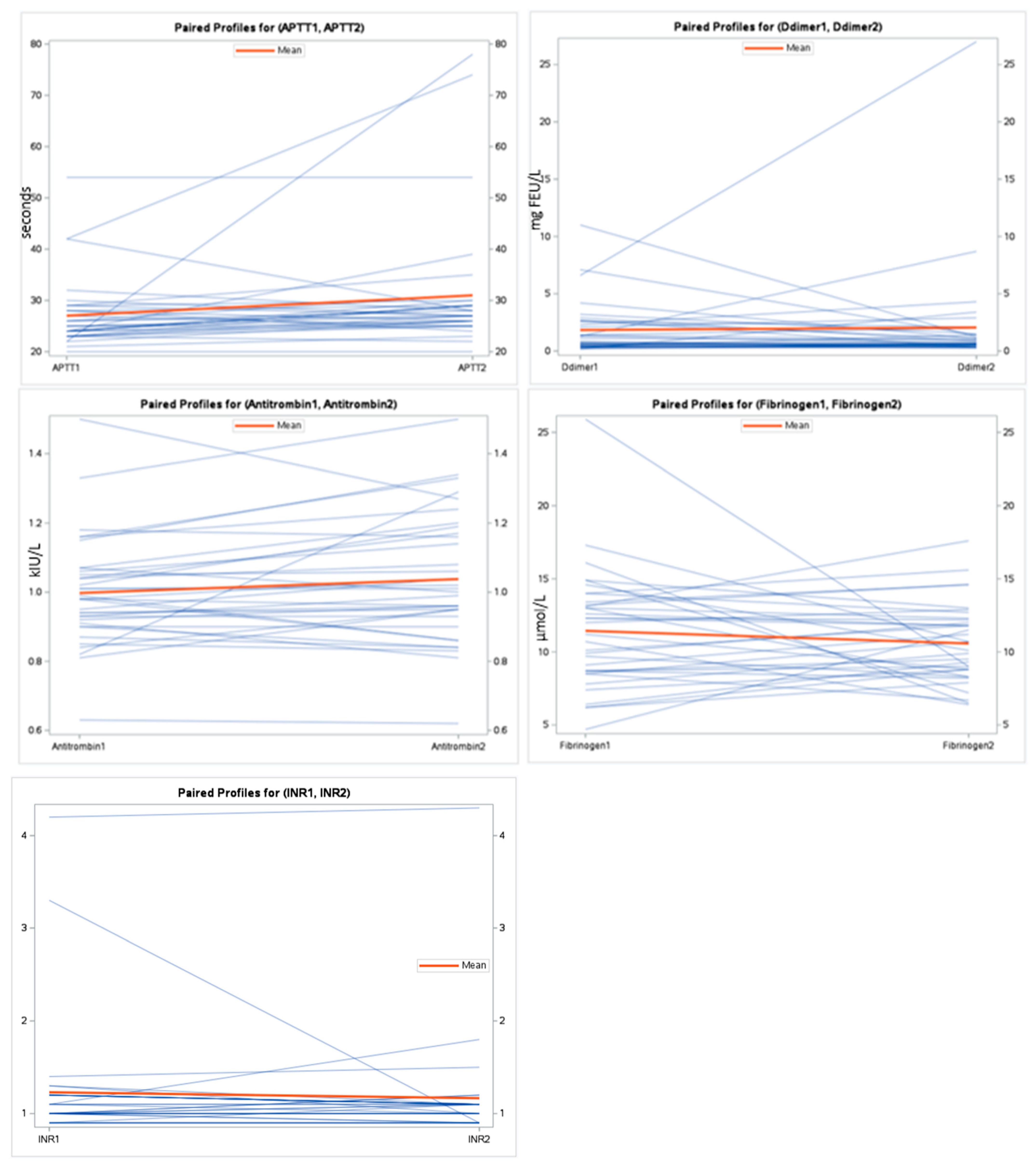
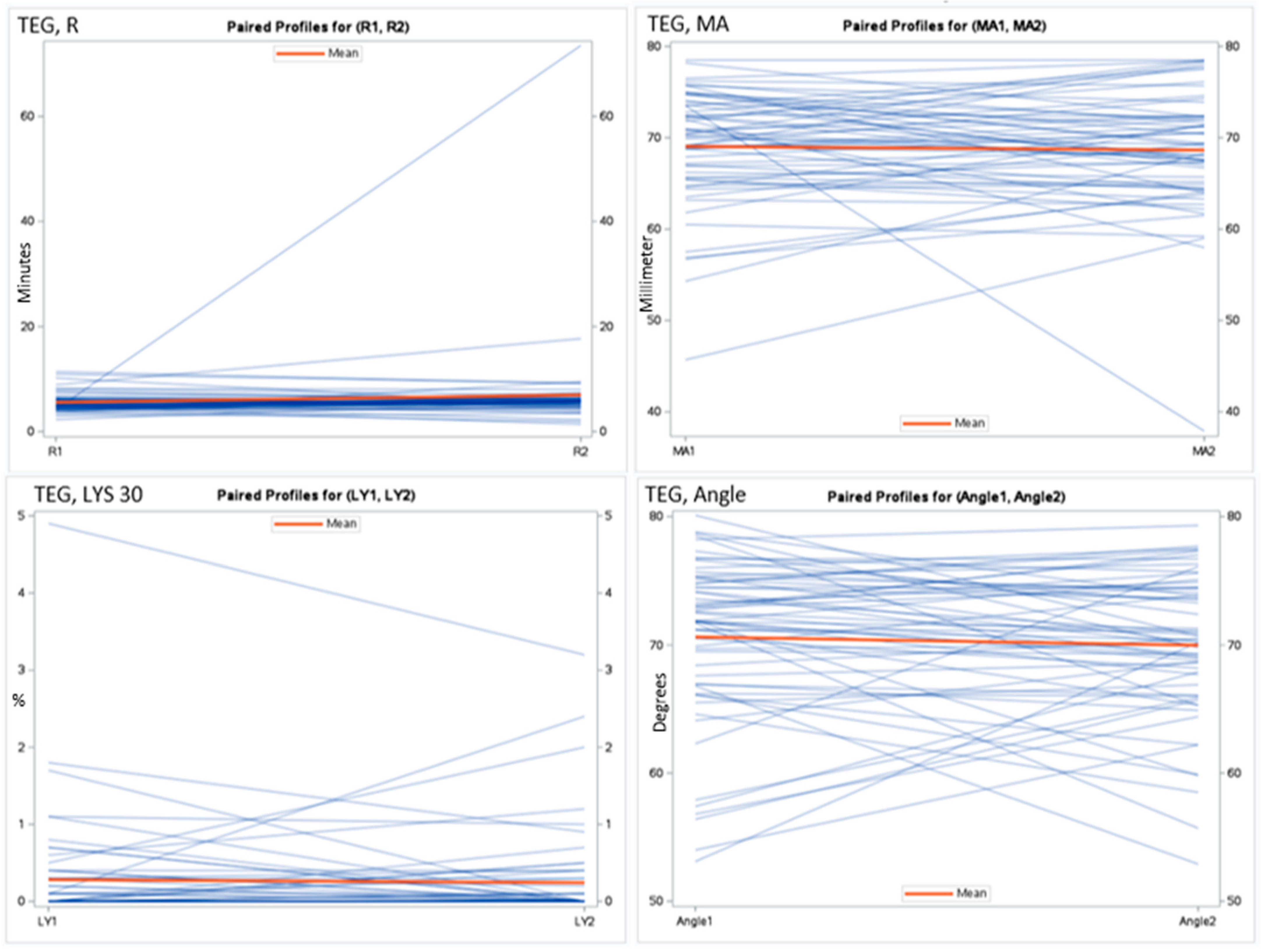
| Marker | Exacerbation, Mean ± SD | Follow-Up, Mean ± SD | Mean Difference (95% CI) | p-Value |
|---|---|---|---|---|
| MA (mm) | 69.06 ± 6.2 | 68.64 ± 6.6 | 0.41 (−1.42–+2.25) | 0.65 |
| R (min) | 5.56 ± 1.7 | 6.98 ± 8.8 | −1.42 (−3.70–+0.86) | 0.22 |
| Angle (degrees) | 70.63 ± 6.3 | 69.98 ± 5.6 | 0.64 (−0.92–+2.21) | 0.41 |
| Lys 30 (%) | 0.28 ± 0.7 | 0.24 ± 0.6 | 0.04 (−0.11–0.18) | 0.59 |
| Fibrinogen (µmol/L) | 11.23 ± 4.2 | 10.19 ± 2.6 | 1.05 (−0.76–+2.86) | 0.25 |
| Antithrombin (kIU/L) | 1.00 ± 0.2 | 1.02 ± 0.2 | −0.02 (−0.07–+0.02) | 0.31 |
| D-dimer (mg FEU/L) | 2.04 ± 2.5 | 2.40 ± 5.1 | −0.37 (−2.24–+1.51) | 0.69 |
| INR | 1.16 ± 0.4 | 1.08 ± 0.2 | 0.08 (−0.12–+0.27) | 0.42 |
| APTT (seconds) | 26.68 ± 5.2 | 30.96 ± 13.2 | −4.29 (−9.19–+0.62) | 0.08 |
| Paired t-Test | Wilcoxon Two-Sample Test | |
|---|---|---|
| Marker | p-Value | p-Value |
| MA (mm) | 0.65 | 0.67 |
| R (min) | 0.22 | 0.11 |
| Lys 30 (%) | 0.59 | 0.08 |
| Angle (degrees) | 0.41 | 0.54 |
| D-dimer (mg FEU/L) | 0.69 | 0.97 |
| Antithrombin (kIU/L) | 0.31 | 0.38 |
| Fibrinogen (µmol/L) | 0.25 | 0.23 |
| APTT (seconds) | 0.08 | 0.12 |
| INR | 0.42 | 0.38 |
| p-Value | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Marker | Age | Sex | BMI | Smoking Status | Atrial Fibrillation | Diabetes Mellitus | Antithrombotic Treatment | Essential Hypertension | Previous VTE |
| MA (mm) | 0.00 | 0.58 | 0.46 | 0.49 | 0.94 | 0.60 | 1.00 | 0.44 | 0.22 |
| R (min) | 0.64 | 0.49 | 0.97 | 0.92 | 0.41 | 0.34 | 0.21 | 0.30 | 0.50 |
| Lys 30 (%) | 0.03 | 0.29 | 0.18 | 0.44 | 0.03 | 0.11 | 0.59 | 0.03 | 0.54 |
| Angle (degrees) | 0.01 | 0.98 | 0.95 | 0.49 | 0.87 | 0.28 | 0.66 | 0.48 | 0.23 |
| D-dimer (mg FEU/L) | 0.17 | 0.29 | 0.56 | 0.00 | 0.35 | 0.14 | 0.16 | 0.86 | 0.60 |
| Antithrombin (kIU/L) | 0.33 | 0.57 | 0.47 | 0.62 | 0.74 | 0.56 | 0.43 | 0.77 | 0.11 |
| Fibrinogen (µmol/L) | 0.11 | 0.22 | 0.38 | 0.57 | 0.18 | 0.82 | 0.93 | 0.41 | 0.82 |
| APTT (seconds) | 0.32 | 0.41 | 0.01 | 0.63 | 0.89 | 0.01 | 0.10 | 0.37 | 0.32 |
| INR | 0.63 | 0.86 | 0.27 | 0.85 | 0.47 | 0.26 | 0.14 | 0.13 | 0.80 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rastoder, E.; Kamstrup, P.; Hedsund, C.; Jordan, A.; Sivapalan, P.; Rømer, V.; Falkvist, F.; Hamidi, S.; Bendstrup, E.; Sperling, S.; et al. Thrombelastography and Conventional Coagulation Markers in Chronic Obstructive Pulmonary Disease: A Prospective Paired-Measurements Study Comparing Exacerbation and Stable Phases. Int. J. Mol. Sci. 2024, 25, 2051. https://doi.org/10.3390/ijms25042051
Rastoder E, Kamstrup P, Hedsund C, Jordan A, Sivapalan P, Rømer V, Falkvist F, Hamidi S, Bendstrup E, Sperling S, et al. Thrombelastography and Conventional Coagulation Markers in Chronic Obstructive Pulmonary Disease: A Prospective Paired-Measurements Study Comparing Exacerbation and Stable Phases. International Journal of Molecular Sciences. 2024; 25(4):2051. https://doi.org/10.3390/ijms25042051
Chicago/Turabian StyleRastoder, Ema, Peter Kamstrup, Caroline Hedsund, Alexander Jordan, Pradeesh Sivapalan, Valdemar Rømer, Frederikke Falkvist, Sadaf Hamidi, Elisabeth Bendstrup, Søren Sperling, and et al. 2024. "Thrombelastography and Conventional Coagulation Markers in Chronic Obstructive Pulmonary Disease: A Prospective Paired-Measurements Study Comparing Exacerbation and Stable Phases" International Journal of Molecular Sciences 25, no. 4: 2051. https://doi.org/10.3390/ijms25042051
APA StyleRastoder, E., Kamstrup, P., Hedsund, C., Jordan, A., Sivapalan, P., Rømer, V., Falkvist, F., Hamidi, S., Bendstrup, E., Sperling, S., Dons, M., Biering-Sørensen, T., Falster, C., Laursen, C. B., Carlsen, J., & Jensen, J.-U. S. (2024). Thrombelastography and Conventional Coagulation Markers in Chronic Obstructive Pulmonary Disease: A Prospective Paired-Measurements Study Comparing Exacerbation and Stable Phases. International Journal of Molecular Sciences, 25(4), 2051. https://doi.org/10.3390/ijms25042051