
The Impact of Cesarean Section Delivery on Intestinal Microbiota: Mechanisms, Consequences, and Perspectives—A Systematic Review

 ,
,  ,
,  , ,
, ,  , ,
, ,  and
and 
Abstract
1. Introduction
1.1. Context and Significance
1.2. Mechanisms Involved
1.3. Long-Term Health Implications
1.4. Study Objectives
2. Methods
2.1. Protocol and Registration
2.2. Search Processing
2.3. Inclusion Criteria
- Participants: infant patients, both male and female;
- Interventions: applications of C- section delivery;
- Comparisons: infant administration of vaginal microbiota;
- Outcomes: infant’s GM during the first 1000 days of life is critical for preventing various health issues in later life;
- Study: randomized clinical trials, retrospective and observational studies.
2.4. Exclusion Criteria
2.5. Data Processing
2.6. Quality Assessment
3. Results and Discussion
3.1. Study Selection and Characteristics
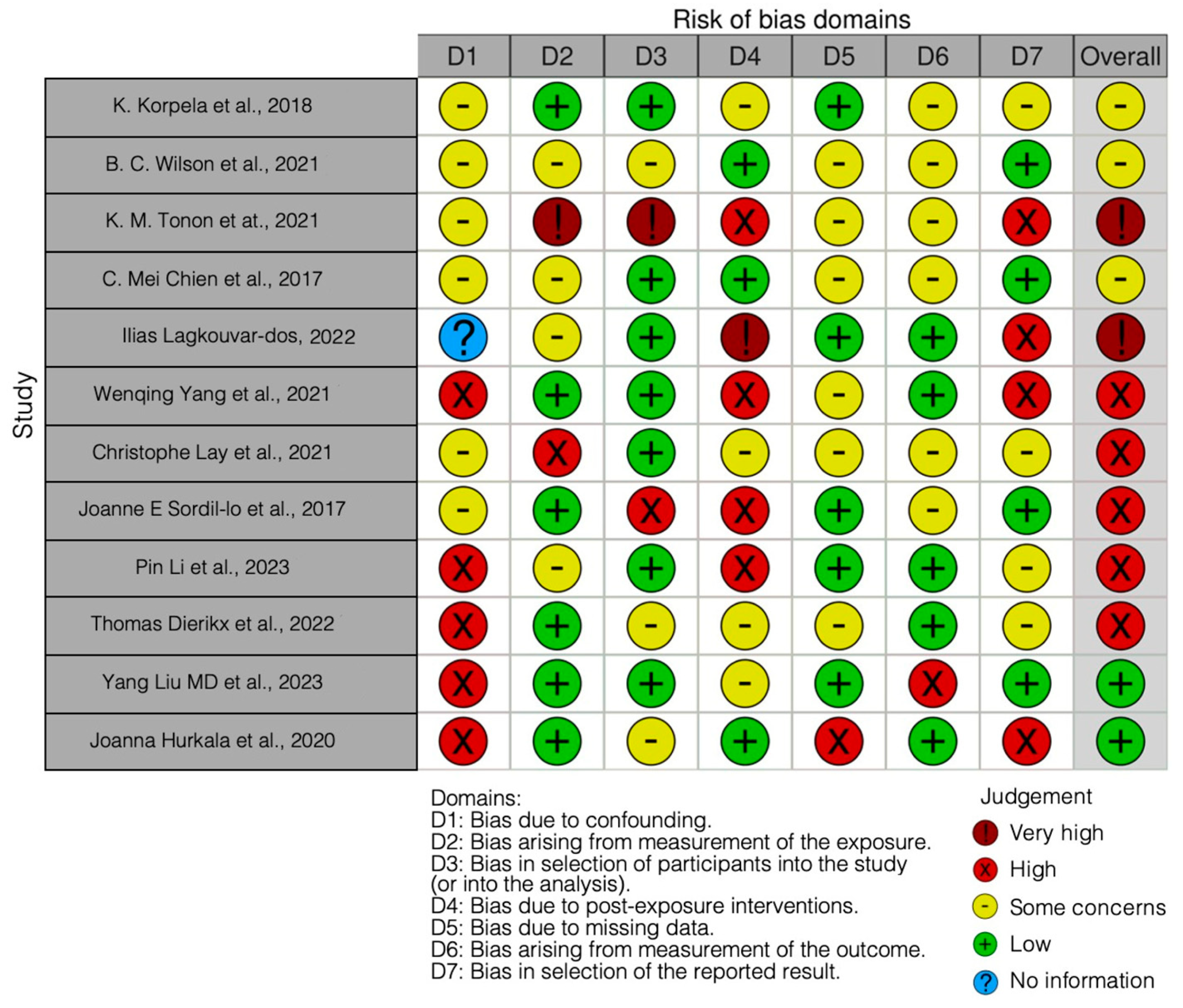
3.2. Quality Assessment and Risk of Bias
4. Conclusions
- CS vs. vaginal birth: Infants born through CS tend to exhibit significant differences in their GM compared with those born naturally. There is a consistent reduction in beneficial bacteria, including Bifidobacterium and Bacteroides, in CS-born infants.
- Probiotic and synbiotic interventions: Some studies suggest that probiotic and synbiotic supplements can help mitigate the negative effects of CS deliveries on an infant’s GM. These interventions promote the colonization of beneficial bacteria and a more balanced microbiome that is crucial for the infant’s long-term health.
- Vaginal seeding: The efficacy of vaginal seeding remains a topic of debate. While some studies did not find significant microbiota changes in CS-born infants after vaginal seeding, concerns about infection risks have been raised. Alternative strategies, like probiotics and delayed antibiotic administration, may offer safer options.
- Breastfeeding: The composition of human milk, particularly the presence of human milk oligosaccharides (HMOs), can influence the GM in infants. It is essential for the growth of beneficial bifidobacteria.
- Prenatal and early life factors: Various factors, including delivery mode, feeding patterns, and antibiotic usage, influence the colonization of an infant’s GM. Identifying these factors helps us to understand how they impact the infant’s long-term health.
- Race and ethnicity: Some studies have shown racial and ethnic disparities in infants’ GMs, which can have implications for variations in disease incidence.
- Maternal antibiotic use: Maternal antibiotic use during CS delivery does not appear to exacerbate colonization disturbances in infants, indicating that antenatal antibiotic exposure may not result in a secondary hit on the infant’s already compromised microbiome.
- Long-term health implications: Early-life microbiome modulation and interventions, especially in CS-born infants, may have far-reaching implications for long-term health outcomes, including reducing the risk of diseases like asthma, allergies, obesity, and diabetes.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CS | Caesarean section |
| CD | Cesarean-born neonates |
| CDL | Cesarean-born neonates supplemented with a probiotic at a lower dosage |
| CDH | Cesarean-born neonates supplemented with a probiotic at a higher dosage |
| COG | Clusters of orthologous groups of proteins |
| FMT | Fecal microbiota transplantation |
| GM | Gut microbiota |
| GOS | Galacto-oligosaccharides |
| sIgA | Fecal secreted immunoglobulin A |
| HMOs | Human milk oligosaccharides |
| IF | Intervention formula |
| Lp N1115 | Lactobacillus paracasei N1115 |
| MS | Mass spectrometry |
| scGOS/lcFOS | Short-chain galactooligosaccharides and long-chain fructooligosaccharides |
| PCR | Polymerase chain reaction |
| RCT | Randomized clinical trial |
| VD | Natural delivery neonates |
| VDAART | Vitamin D antenatal asthma reduction trial |
References
- Zhou, P.; Zhou, Y.; Liu, B.; Jin, Z.; Zhuang, X.; Dai, W.; Yang, Z.; Feng, X.; Zhou, Q.; Liu, Y.; et al. Perinatal Antibiotic Exposure Affects the Transmission between Maternal and Neonatal Microbiota and Is Associated with Early-Onset Sepsis. mSphere 2020, 5, e00984-19. [Google Scholar] [CrossRef] [PubMed]
- Samarra, A.; Esteban-Torres, M.; Cabrera-Rubio, R.; Bernabeu, M.; Arboleya, S.; Gueimonde, M.; Collado, M.C. Maternal-Infant Antibiotic Resistance Genes Transference: What Do We Know? Gut Microbes 2023, 15, 2194797. [Google Scholar] [CrossRef] [PubMed]
- Ballini, A.; Santacroce, L.; Cantore, S.; Bottalico, L.; Dipalma, G.; Topi, S.; Saini, R.; De Vito, D.; Inchingolo, F. Probiotics Efficacy on Oxidative Stress Values in Inflammatory Bowel Disease: A Randomized Double-Blinded Placebo-Controlled Pilot Study. Endocr. Metab. Immune Disord.-Drug Targets 2019, 19, 373–381. [Google Scholar] [CrossRef]
- Zhou, L.; Qiu, W.; Wang, J.; Zhao, A.; Zhou, C.; Sun, T.; Xiong, Z.; Cao, P.; Shen, W.; Chen, J.; et al. Effects of Vaginal Microbiota Transfer on the Neurodevelopment and Microbiome of Cesarean-Born Infants: A Blinded Randomized Controlled Trial. Cell Host Microbe 2023, 31, 1232–1247.e5. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.-W.; Adams, J.B.; Gregory, A.C.; Borody, T.; Chittick, L.; Fasano, A.; Khoruts, A.; Geis, E.; Maldonado, J.; McDonough-Means, S.; et al. Microbiota Transfer Therapy Alters Gut Ecosystem and Improves Gastrointestinal and Autism Symptoms: An Open-Label Study. Microbiome 2017, 5, 10. [Google Scholar] [CrossRef]
- Kang, D.-W.; Adams, J.B.; Coleman, D.M.; Pollard, E.L.; Maldonado, J.; McDonough-Means, S.; Caporaso, J.G.; Krajmalnik-Brown, R. Long-Term Benefit of Microbiota Transfer Therapy on Autism Symptoms and Gut Microbiota. Sci. Rep. 2019, 9, 5821. [Google Scholar] [CrossRef]
- Aagaard, K.; Ma, J.; Antony, K.M.; Ganu, R.; Petrosino, J.; Versalovic, J. The Placenta Harbors a Unique Microbiome. Sci. Transl. Med. 2014, 6, 237ra65. [Google Scholar] [CrossRef]
- Arrieta, M.-C.; Stiemsma, L.T.; Dimitriu, P.A.; Thorson, L.; Russell, S.; Yurist-Doutsch, S.; Kuzeljevic, B.; Gold, M.J.; Britton, H.M.; Lefebvre, D.L.; et al. Early Infancy Microbial and Metabolic Alterations Affect Risk of Childhood Asthma. Sci. Transl. Med. 2015, 7, 307ra152. [Google Scholar] [CrossRef]
- Santacroce, L.; Charitos, I.A.; Ballini, A.; Inchingolo, F.; Luperto, P.; De Nitto, E.; Topi, S. The Human Respiratory System and Its Microbiome at a Glimpse. Biology 2020, 9, 318. [Google Scholar] [CrossRef]
- Liu, Y.; Li, H.-T.; Zhou, S.-J.; Zhou, H.-H.; Xiong, Y.; Yang, J.; Zhou, Y.-B.; Chen, D.-J.; Liu, J.-M. Effects of Vaginal Seeding on Gut Microbiota, Body Mass Index, and Allergy Risks in Infants Born through Cesarean Delivery: A Randomized Clinical Trial. Am. J. Obstet. Gynecol. MFM 2023, 5, 100793. [Google Scholar] [CrossRef]
- Tun, H.M.; Bridgman, S.L.; Chari, R.; Field, C.J.; Guttman, D.S.; Becker, A.B.; Mandhane, P.J.; Turvey, S.E.; Subbarao, P.; Sears, M.R.; et al. Roles of Birth Mode and Infant Gut Microbiota in Intergenerational Transmission of Overweight and Obesity From Mother to Offspring. JAMA Pediatr. 2018, 172, 368–377. [Google Scholar] [CrossRef] [PubMed]
- Estorninos, E.; Lawenko, R.B.; Palestroque, E.; Sprenger, N.; Benyacoub, J.; Kortman, G.A.M.; Boekhorst, J.; Bettler, J.; Cercamondi, C.I.; Berger, B. Term Infant Formula Supplemented with Milk-Derived Oligosaccharides Shifts the Gut Microbiota Closer to That of Human Milk-Fed Infants and Improves Intestinal Immune Defense: A Randomized Controlled Trial. Am. J. Clin. Nutr. 2022, 115, 142–153. [Google Scholar] [CrossRef] [PubMed]
- Alliet, P.; Vandenplas, Y.; Roggero, P.; Jespers, S.N.J.; Peeters, S.; Stalens, J.-P.; Kortman, G.A.M.; Amico, M.; Berger, B.; Sprenger, N.; et al. Safety and Efficacy of a Probiotic-Containing Infant Formula Supplemented with 2′-Fucosyllactose: A Double-Blind Randomized Controlled Trial. Nutr. J. 2022, 21, 11. [Google Scholar] [CrossRef]
- Berger, B.; Porta, N.; Foata, F.; Grathwohl, D.; Delley, M.; Moine, D.; Charpagne, A.; Siegwald, L.; Descombes, P.; Alliet, P.; et al. Linking Human Milk Oligosaccharides, Infant Fecal Community Types, and Later Risk To Require Antibiotics. mBio 2020, 11, e03196-19. [Google Scholar] [CrossRef] [PubMed]
- Vandenplas, Y.; Zakharova, I.; Dmitrieva, Y. Oligosaccharides in Infant Formula: More Evidence to Validate the Role of Prebiotics. Br. J. Nutr. 2015, 113, 1339–1344. [Google Scholar] [CrossRef] [PubMed]
- Wampach, L.; Heintz-Buschart, A.; Hogan, A.; Muller, E.E.L.; Narayanasamy, S.; Laczny, C.C.; Hugerth, L.W.; Bindl, L.; Bottu, J.; Andersson, A.F.; et al. Colonization and Succession within the Human Gut Microbiome by Archaea, Bacteria, and Microeukaryotes during the First Year of Life. Front. Microbiol. 2017, 8, 738. [Google Scholar] [CrossRef]
- Azad, M.B.; Konya, T.; Maughan, H.; Guttman, D.S.; Field, C.J.; Chari, R.S.; Sears, M.R.; Becker, A.B.; Scott, J.A.; Kozyrskyj, A.L. Gut Microbiota of Healthy Canadian Infants: Profiles by Mode of Delivery and Infant Diet at 4 Months. CMAJ 2013, 185, 385–394. [Google Scholar] [CrossRef]
- Azad, M.B.; Konya, T.; Persaud, R.R.; Guttman, D.S.; Chari, R.S.; Field, C.J.; Sears, M.R.; Mandhane, P.J.; Turvey, S.E.; Subbarao, P.; et al. Impact of Maternal Intrapartum Antibiotics, Method of Birth and Breastfeeding on Gut Microbiota during the First Year of Life: A Prospective Cohort Study. BJOG 2016, 123, 983–993. [Google Scholar] [CrossRef]
- Bäckhed, F.; Roswall, J.; Peng, Y.; Feng, Q.; Jia, H.; Kovatcheva-Datchary, P.; Li, Y.; Xia, Y.; Xie, H.; Zhong, H.; et al. Dynamics and Stabilization of the Human Gut Microbiome during the First Year of Life. Cell Host Microbe 2015, 17, 690–703. [Google Scholar] [CrossRef]
- Isacco, C.G.; Ballini, A.; De Vito, D.; Nguyen, K.C.D.; Cantore, S.; Bottalico, L.; Quagliuolo, L.; Boccellino, M.; Di Domenico, M.; Santacroce, L.; et al. Rebalancing the Oral Microbiota as an Efficient Tool in Endocrine, Metabolic and Immune Disorders. Endocr. Metab. Immune Disord.-Drug Targets 2021, 21, 777–784. [Google Scholar] [CrossRef]
- Contaldo, M.; Fusco, A.; Stiuso, P.; Lama, S.; Gravina, A.G.; Itro, A.; Federico, A.; Itro, A.; Dipalma, G.; Inchingolo, F.; et al. Oral Microbiota and Salivary Levels of Oral Pathogens in Gastro-Intestinal Diseases: Current Knowledge and Exploratory Study. Microorganisms 2021, 9, 1064. [Google Scholar] [CrossRef] [PubMed]
- Paolella, G.; Vajro, P. Maternal Microbiota, Prepregnancy Weight, and Mode of Delivery: Intergenerational Transmission of Risk for Childhood Overweight and Obesity. JAMA Pediatr. 2018, 172, 320–322. [Google Scholar] [CrossRef]
- Blaser, M.J.; Dominguez-Bello, M.G. The Human Microbiome before Birth. Cell Host Microbe 2016, 20, 558–560. [Google Scholar] [CrossRef]
- Blustein, J.; Attina, T.; Liu, M.; Ryan, A.M.; Cox, L.M.; Blaser, M.J.; Trasande, L. Association of Caesarean Delivery with Child Adiposity from Age 6 Weeks to 15 Years. Int. J. Obes. 2013, 37, 900–906. [Google Scholar] [CrossRef]
- Ballini, A.; Dipalma, G.; Isacco, C.G.; Boccellino, M.; Di Domenico, M.; Santacroce, L.; Nguyễn, K.C.D.; Scacco, S.; Calvani, M.; Boddi, A.; et al. Oral Microbiota and Immune System Crosstalk: A Translational Research. Biology 2020, 9, 131. [Google Scholar] [CrossRef]
- Signorini, L.; Ballini, A.; Arrigoni, R.; De Leonardis, F.; Saini, R.; Cantore, S.; De Vito, D.; Coscia, M.F.; Dipalma, G.; Santacroce, L.; et al. Evaluation of a Nutraceutical Product with Probiotics, Vitamin D, Plus Banaba Leaf Extracts (Lagerstroemia Speciosa) in Glycemic Control. Endocr. Metab. Immune Disord.-Drug Targets 2021, 21, 1356–1365. [Google Scholar] [CrossRef]
- Koleva, P.T.; Bridgman, S.L.; Kozyrskyj, A.L. The Infant Gut Microbiome: Evidence for Obesity Risk and Dietary Intervention. Nutrients 2015, 7, 2237–2260. [Google Scholar] [CrossRef] [PubMed]
- Butler, É.M.; Chiavaroli, V.; Derraik, J.G.B.; Grigg, C.P.; Wilson, B.C.; Walker, N.; O’Sullivan, J.M.; Cutfield, W.S. Maternal Bacteria to Correct Abnormal Gut Microbiota in Babies Born by C-Section. Medicine 2020, 99, e21315. [Google Scholar] [CrossRef]
- Xie, J.; Tang, C.; Hong, S.; Xin, Y.; Zhang, J.; Lin, Y.; Mao, L.; Xiao, Y.; Wu, Q.; Zhang, X.; et al. Maternal Vaginal Fluids Play a Major Role in the Colonization of the Neonatal Intestinal Microbiota. Front. Cell Infect. Microbiol. 2023, 13, 1065884. [Google Scholar] [CrossRef]
- Song, S.J.; Wang, J.; Martino, C.; Jiang, L.; Thompson, W.K.; Shenhav, L.; McDonald, D.; Marotz, C.; Harris, P.R.; Hernandez, C.D.; et al. Naturalization of the Microbiota Developmental Trajectory of Cesarean-Born Neonates after Vaginal Seeding. Med 2021, 2, 951–964.e5. [Google Scholar] [CrossRef]
- Adina, S. Orthopedic Joint Stability Influences Growth and Maxillary Development: Clinical Aspects. J. Biol. Regul. Homeost. Agents 2020, 34, 747–756. [Google Scholar] [CrossRef]
- Akagawa, S.; Tsuji, S.; Onuma, C.; Akagawa, Y.; Yamaguchi, T.; Yamagishi, M.; Yamanouchi, S.; Kimata, T.; Sekiya, S.-I.; Ohashi, A.; et al. Effect of Delivery Mode and Nutrition on Gut Microbiota in Neonates. Ann. Nutr. Metab. 2019, 74, 132–139. [Google Scholar] [CrossRef]
- Arboleya, S.; Suárez, M.; Fernández, N.; Mantecón, L.; Solís, G.; Gueimonde, M.; de Los Reyes-Gavilán, C.G. C-Section and the Neonatal Gut Microbiome Acquisition: Consequences for Future Health. Ann. Nutr. Metab. 2018, 73 (Suppl. S3), 17–23. [Google Scholar] [CrossRef]
- Isacco, C.G.; Ballini, A.; Vito, D.D.; Inchingolo, A.M.; Cantore, S.; Paduanelli, G.; Nguyen, K.C.D.; Inchingolo, A.D.; Dipalma, G.; Inchingolo, F.; et al. Probiotics in Health and Immunity: A First Step toward Understanding the Importance of Microbiota System in Translational Medicine; IntechOpen: London, UK, 2019; ISBN 978-1-78985-922-5. [Google Scholar]
- Campanella, V.; Syed, J.; Santacroce, L.; Saini, R.; Ballini, A.; Inchingolo, F. Oral Probiotics Influence Oral and Respiratory Tract Infections in Pediatric Population: A Randomized Double-Blinded Placebo-Controlled Pilot Study. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 8034–8041. [Google Scholar] [CrossRef]
- Casu, C.; Mosaico, G.; Natoli, V.; Scarano, A.; Lorusso, F.; Inchingolo, F. Microbiota of the Tongue and Systemic Connections: The Examination of the Tongue as an Integrated Approach in Oral Medicine. Hygiene 2021, 1, 56–68. [Google Scholar] [CrossRef]
- Mueller, N.T.; Mao, G.; Bennet, W.L.; Hourigan, S.K.; Dominguez-Bello, M.G.; Appel, L.J.; Wang, X. Does Vaginal Delivery Mitigate or Strengthen the Intergenerational Association of Overweight and Obesity? Findings from the Boston Birth Cohort. Int. J. Obes. 2017, 41, 497–501. [Google Scholar] [CrossRef]
- Cho, C.E.; Norman, M. Cesarean Section and Development of the Immune System in the Offspring. Am. J. Obstet. Gynecol. 2013, 208, 249–254. [Google Scholar] [CrossRef]
- Cuppari, C.; Manti, S.; Salpietro, A.; Alterio, T.; Arrigo, T.; Leonardi, S.; Salpietro, C. Mode of Delivery and Risk for Development of Atopic Diseases in Children. Allergy Asthma Proc 2015, 36, 344–351. [Google Scholar] [CrossRef]
- Pacifici, L.; Santacroce, L.; Dipalma, G. Gender Medicine: The Impact of Probiotics on Male Patients. La Clin. Ter. 2021, 172, 8–15. [Google Scholar] [CrossRef]
- Ballini, A.; Gnoni, A.; De Vito, D.; Dipalma, G.; Cantore, S.; Gargiulo Isacco, C.; Saini, R.; Santacroce, L.; Topi, S.; Scarano, A.; et al. Effect of Probiotics on the Occurrence of Nutrition Absorption Capacities in Healthy Children: A Randomized Double-Blinded Placebo-Controlled Pilot Study. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 8645–8657. [Google Scholar] [CrossRef]
- Li, H.; Ye, R.; Pei, L.; Ren, A.; Zheng, X.; Liu, J. Caesarean Delivery, Caesarean Delivery on Maternal Request and Childhood Overweight: A Chinese Birth Cohort Study of 181 380 Children. Pediatr. Obes. 2014, 9, 10–16. [Google Scholar] [CrossRef]
- Nagpal, R.; Yamashiro, Y. Gut Microbiota Composition in Healthy Japanese Infants and Young Adults Born by C-Section. Ann. Nutr. Metab. 2018, 73 (Suppl. S3), 4–11. [Google Scholar] [CrossRef] [PubMed]
- Neu, J. Dysbiosis in the Neonatal Period: Role of Cesarean Section. Nestle Nutr. Inst. Workshop Ser. 2017, 88, 57–66. [Google Scholar] [CrossRef]
- Azevedo, M.J.; Garcia, A.; Costa, C.F.F.A.; Ferreira, A.F.; Falcão-Pires, I.; Brandt, B.W.; Ramalho, C.; Zaura, E.; Sampaio-Maia, B. The Contribution of Maternal Factors to the Oral Microbiota of the Child: Influence from Early Life and Clinical Relevance. Jpn. Dent. Sci. Rev. 2023, 59, 191–202. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.D. The Integumentary System and Its Microbiota between Health and Disease. J. Biol. Regul. Homeost. Agents 2021, 35, 8. [Google Scholar] [CrossRef]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Ronsivalle, V.; Shapira, I.; Cicciù, M. Prevalence of Temporomandibular Disorders in Subjects Affected by Parkinson Disease: A Systematic Review and Metanalysis. J. Oral. Rehabil. 2023, 50, 877–885. [Google Scholar] [CrossRef]
- Reddy, L.K.V.; Madithati, P.; Narapureddy, B.R.; Ravula, S.R.; Vaddamanu, S.K.; Alhamoudi, F.H.; Minervini, G.; Chaturvedi, S. Perception about Health Applications (Apps) in Smartphones towards Telemedicine during COVID-19: A Cross-Sectional Study. J. Pers. Med. 2022, 12, 1920. [Google Scholar] [CrossRef] [PubMed]
- Rathi, S.; Chaturvedi, S.; Abdullah, S.; Rajput, G.; Alqahtani, N.M.; Chaturvedi, M.; Gurumurthy, V.; Saini, R.; Bavabeedu, S.S.; Minervini, G. Clinical Trial to Assess Physiology and Activity of Masticatory Muscles of Complete Denture Wearer Following Vitamin D Intervention. Medicina 2023, 59, 410. [Google Scholar] [CrossRef]
- Minervini, G.; Lucchese, A.; Perillo, L.; Serpico, R.; Minervini, G. Unilateral Superior Condylar Neck Fracture with Dislocation in a Child Treated with an Acrylic Splint in the Upper Arch for Functional Repositioning of the Mandible. CRANIO® 2017, 35, 337–341. [Google Scholar] [CrossRef]
- Minervini, G.; D’Amico, C.; Cicciù, M.; Fiorillo, L. Temporomandibular Joint Disk Displacement: Etiology, Diagnosis, Imaging, and Therapeutic Approaches. J. Craniofacial Surg. 2023, 34, 1115–1121. [Google Scholar] [CrossRef]
- Santacroce, L. The Pivotal Role of Oral Microbiota in Health and Disease. J. Biol. Regul. Homeost. Agents 2020, 34, 733–737. [Google Scholar] [CrossRef] [PubMed]
- Cantore, S.; Ballini, A.; De Vito, D.; Abbinante, A.; Altini, V.; Dipalma, G.; Inchingolo, F.; Saini, R. Clinical Results of Improvement in Periodontal Condition by Administration of Oral Probiotics. J. Biol. Regul. Homeost. Agents 2018, 32, 1329–1334. [Google Scholar]
- Hoang, D.M.; Levy, E.I.; Vandenplas, Y. The Impact of Caesarean Section on the Infant Gut Microbiome. Acta Paediatr. 2021, 110, 60–67. [Google Scholar] [CrossRef]
- Marrs, T.; Jo, J.-H.; Perkin, M.R.; Rivett, D.W.; Witney, A.A.; Bruce, K.D.; Logan, K.; Craven, J.; Radulovic, S.; Versteeg, S.A.; et al. Gut Microbiota Development during Infancy: Impact of Introducing Allergenic Foods. J. Allergy Clin. Immunol. 2021, 147, 613–621.e9. [Google Scholar] [CrossRef] [PubMed]
- Carpay, N.C.; Kamphorst, K.; de Meij, T.G.J.; Daams, J.G.; Vlieger, A.M.; van Elburg, R.M. Microbial Effects of Prebiotics, Probiotics and Synbiotics after Caesarean Section or Exposure to Antibiotics in the First Week of Life: A Systematic Review. PLoS ONE 2022, 17, e0277405. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, F.; Dipalma, G.; Cirulli, N.; Cantore, S.; Saini, R.S.; Altini, V.; Santacroce, L.; Ballini, A.; Saini, R. Microbiological Results of Improvement in Periodontal Condition by Administration of Oral Probiotics. J. Biol. Regul. Homeost. Agents 2018, 32, 1323–1328. [Google Scholar] [PubMed]
- Salas Garcia, M.C.; Yee, A.L.; Gilbert, J.A.; Dsouza, M. Dysbiosis in Children Born by Caesarean Section. Ann. Nutr. Metab. 2018, 73 (Suppl. S3), 24–32. [Google Scholar] [CrossRef]
- Chen, X.; Shi, Y. Determinants of Microbial Colonization in the Premature Gut. Mol. Med. 2023, 29, 90. [Google Scholar] [CrossRef] [PubMed]
- Phillips-Farfán, B.; Gómez-Chávez, F.; Medina-Torres, E.A.; Vargas-Villavicencio, J.A.; Carvajal-Aguilera, K.; Camacho, L. Microbiota Signals during the Neonatal Period Forge Life-Long Immune Responses. Int. J. Mol. Sci. 2021, 22, 8162. [Google Scholar] [CrossRef]
- Francavilla, R.; Cristofori, F.; Tripaldi, M.E.; Indrio, F. Intervention for Dysbiosis in Children Born by C-Section. Ann. Nutr. Metab. 2018, 73 (Suppl. S3), 33–39. [Google Scholar] [CrossRef]
- Butler, É.M.; Reynolds, A.J.; Derraik, J.G.B.; Wilson, B.C.; Cutfield, W.S.; Grigg, C.P. The Views of Pregnant Women in New Zealand on Vaginal Seeding: A Mixed-Methods Study. BMC Pregnancy Childbirth 2021, 21, 49. [Google Scholar] [CrossRef] [PubMed]
- Galazzo, G.; van Best, N.; Bervoets, L.; Dapaah, I.O.; Savelkoul, P.H.; Hornef, M.W.; GI-MDH consortium; Lau, S.; Hamelmann, E.; Penders, J. Development of the Microbiota and Associations With Birth Mode, Diet, and Atopic Disorders in a Longitudinal Analysis of Stool Samples, Collected From Infancy Through Early Childhood. Gastroenterology 2020, 158, 1584–1596. [Google Scholar] [CrossRef]
- Samara, J.; Moossavi, S.; Alshaikh, B.; Ortega, V.A.; Pettersen, V.K.; Ferdous, T.; Hoops, S.L.; Soraisham, A.; Vayalumkal, J.; Dersch-Mills, D.; et al. Supplementation with a Probiotic Mixture Accelerates Gut Microbiome Maturation and Reduces Intestinal Inflammation in Extremely Preterm Infants. Cell Host Microbe 2022, 30, 696–711. [Google Scholar] [CrossRef]
- Sassin, A.M.; Johnson, G.J.; Goulding, A.N.; Aagaard, K.M. Crucial Nuances in Understanding (Mis)Associations between the Neonatal Microbiome and Cesarean Delivery. Trends Mol. Med. 2022, 28, 806–822. [Google Scholar] [CrossRef]
- Ballini, A.; Signorini, L.; Inchingolo, A.M.; Saini, R.; Gnoni, A.; Scacco, S.; Cantore, S.; Dipalma, G.; Inchingolo, F.; Santacroce, L. Probiotics May Improve Serum Folate Availability in Pregnant Women: A Pilot Study. Open Access Maced. J. Med. Sci. 2020, 8, 1124–1130. [Google Scholar] [CrossRef]
- Butel, M.-J.; Waligora-Dupriet, A.-J.; Wydau-Dematteis, S. The Developing Gut Microbiota and Its Consequences for Health. J. Dev. Orig. Health Dis. 2018, 9, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Signorini, L. Probiotics May Modulate the Impact of Aging on Adults. J. Biol. Regul. Homeost. Agents 2020, 34, 1601–1606. [Google Scholar] [CrossRef] [PubMed]
- Sordillo, J.E.; Zhou, Y.; McGeachie, M.J.; Ziniti, J.; Lange, N.; Laranjo, N.; Savage, J.R.; Carey, V.; O’Connor, G.; Sandel, M.; et al. Factors Influencing the Infant Gut Microbiome at Age 3–6 Months: Findings from the Ethnically Diverse Vitamin D Antenatal Asthma Reduction Trial (VDAART). J. Allergy Clin. Immunol. 2017, 139, 482–491.e14. [Google Scholar] [CrossRef]
- Sordillo, J.E.; Korrick, S.; Laranjo, N.; Carey, V.; Weinstock, G.M.; Gold, D.R.; O’Connor, G.; Sandel, M.; Bacharier, L.B.; Beigelman, A.; et al. Association of the Infant Gut Microbiome With Early Childhood Neurodevelopmental Outcomes: An Ancillary Study to the VDAART Randomized Clinical Trial. JAMA Netw. Open 2019, 2, e190905. [Google Scholar] [CrossRef]
- Kapourchali, F.R.; Cresci, G.A.M. Early-Life Gut Microbiome-The Importance of Maternal and Infant Factors in Its Establishment. Nutr. Clin. Pract. 2020, 35, 386–405. [Google Scholar] [CrossRef]
- Hurkala, J.; Lauterbach, R.; Radziszewska, R.; Strus, M.; Heczko, P. Effect of a Short-Time Probiotic Supplementation on the Abundance of the Main Constituents of the Gut Microbiota of Term Newborns Delivered by Cesarean Section-A Randomized, Prospective, Controlled Clinical Trial. Nutrients 2020, 12, 3128. [Google Scholar] [CrossRef]
- Van Best, N.; Dominguez-Bello, M.G.; Hornef, M.W.; Jašarević, E.; Korpela, K.; Lawley, T.D. Should We Modulate the Neonatal Microbiome and What Should Be the Goal? Microbiome 2022, 10, 74. [Google Scholar] [CrossRef]
- Mancini, V.O.; Brook, J.; Hernandez, C.; Strickland, D.; Christophersen, C.T.; D’Vaz, N.; Silva, D.; Prescott, S.; Callaghan, B.; Downs, J.; et al. Associations between the Human Immune System and Gut Microbiome with Neurodevelopment in the First 5 Years of Life: A Systematic Scoping Review. Dev. Psychobiol. 2023, 65, e22360. [Google Scholar] [CrossRef]
- Socha-Banasiak, A.; Pawłowska, M.; Czkwianianc, E.; Pierzynowska, K. From Intrauterine to Extrauterine Life-The Role of Endogenous and Exogenous Factors in the Regulation of the Intestinal Microbiota Community and Gut Maturation in Early Life. Front. Nutr. 2021, 8, 696966. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, S.; Mummolo, S.; Tecco, S.; Continenza, M.A.; Marzo, G. Histological Characterization of Sacco’s Concentrated Growth Factors Membrane. Int. J. Morphol. 2017, 35, 114–119. [Google Scholar] [CrossRef]
- Quinzi, V.; Saccomanno, S.; Manenti, R.J.; Giancaspro, S.; Coceani Paskay, L.; Marzo, G. Efficacy of Rapid Maxillary Expansion with or without Previous Adenotonsillectomy for Pediatric Obstructive Sleep Apnea Syndrome Based on Polysomnographic Data: A Systematic Review and Meta-Analysis. Appl. Sci. 2020, 10, 6485. [Google Scholar] [CrossRef]
- Tecco, S.; Mummolo, S.; Marchetti, E.; Tetè, S.; Campanella, V.; Gatto, R.; Gallusi, G.; Tagliabue, A.; Marzo, G. sEMG Activity of Masticatory, Neck, and Trunk Muscles during the Treatment of Scoliosis with Functional Braces. A Longitudinal Controlled Study. J. Electromyogr. Kinesiol. 2011, 21, 885–892. [Google Scholar] [CrossRef] [PubMed]
- Gschwind, R.; Fournier, T.; Butel, M.-J.; Wydau-Dematteis, S. Microbiota establishment: An in utero colonization decisive for future health? Med. Sci. 2018, 34, 331–337. [Google Scholar] [CrossRef]
- Keck-Kester, T.; Hicks, S.D. Infant Saliva Microbiome Activity Modulates Nutritional Impacts on Neurodevelopment. Microorganisms 2023, 11, 2111. [Google Scholar] [CrossRef]
- Plummer, E.L.; Bulach, D.M.; Murray, G.L.; Jacobs, S.E.; Tabrizi, S.N.; Garland, S.M. ProPrems Study Group Gut Microbiota of Preterm Infants Supplemented with Probiotics: Sub-Study of the ProPrems Trial. BMC Microbiol. 2018, 18, 184. [Google Scholar] [CrossRef]
- Beghetti, I.; Barone, M.; Brigidi, P.; Sansavini, A.; Corvaglia, L.; Aceti, A.; Turroni, S. Early-Life Gut Microbiota and Neurodevelopment in Preterm Infants: A Narrative Review. Front. Nutr. 2023, 10, 1241303. [Google Scholar] [CrossRef]
- Korpela, K.; Salonen, A.; Vepsäläinen, O.; Suomalainen, M.; Kolmeder, C.; Varjosalo, M.; Miettinen, S.; Kukkonen, K.; Savilahti, E.; Kuitunen, M.; et al. Probiotic Supplementation Restores Normal Microbiota Composition and Function in Antibiotic-Treated and in Caesarean-Born Infants. Microbiome 2018, 6, 182. [Google Scholar] [CrossRef] [PubMed]
- Wilson, B.C.; Butler, É.M.; Grigg, C.P.; Derraik, J.G.B.; Chiavaroli, V.; Walker, N.; Thampi, S.; Creagh, C.; Reynolds, A.J.; Vatanen, T.; et al. Oral Administration of Maternal Vaginal Microbes at Birth to Restore Gut Microbiome Development in Infants Born by Caesarean Section: A Pilot Randomised Placebo-Controlled Trial. eBioMedicine 2021, 69, 103443. [Google Scholar] [CrossRef]
- Tonon, K.M.; Morais, T.B.; Taddei, C.R.; Araújo-Filho, H.B.; Abrão, A.C.F.V.; Miranda, A.; De Morais, M.B. Gut Microbiota Comparison of Vaginally and Cesarean Born Infants Exclusively Breastfed by Mothers Secreting A1–2 Fucosylated Oligosaccharides in Breast Milk. PLoS ONE 2021, 16, e0246839. [Google Scholar] [CrossRef] [PubMed]
- Chua, M.C.; Ben-Amor, K.; Lay, C.; Goh, A.E.N.; Chiang, W.C.; Rao, R.; Chew, C.; Chaithongwongwatthana, S.; Khemapech, N.; Knol, J.; et al. Effect of Synbiotic on the Gut Microbiota of Cesarean Delivered Infants: A Randomized, Double-Blind, Multicenter Study. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 102–106. [Google Scholar] [CrossRef]
- Lagkouvardos, I.; Intze, E.; Schaubeck, M.; Rooney, J.P.; Hecht, C.; Piloquet, H.; Clavel, T. Early Life Gut Microbiota Profiles Linked to Synbiotic Formula Effects: A Randomized Clinical Trial in European Infants. Am. J. Clin. Nutr. 2023, 117, 326–339. [Google Scholar] [CrossRef]
- Yang, W.; Tian, L.; Luo, J.; Yu, J. Ongoing Supplementation of Probiotics to Cesarean-Born Neonates during the First Month of Life May Impact the Gut Microbial. Am. J. Perinatol. 2021, 38, 1181–1191. [Google Scholar] [CrossRef] [PubMed]
- Lay, C.; Chu, C.W.; Purbojati, R.W.; Acerbi, E.; Drautz-Moses, D.I.; De Sessions, P.F.; Jie, S.; Ho, E.; Kok, Y.J.; Bi, X.; et al. A Synbiotic Intervention Modulates Meta-Omics Signatures of Gut Redox Potential and Acidity in Elective Caesarean Born Infants. BMC Microbiol. 2021, 21, 191. [Google Scholar] [CrossRef]
- Li, P.; Ren, Z.; Zhou, J.; Zhao, A.; Wang, S.; Xun, Y.; Jiang, H.; Wang, P.; Yuan, Q.; Zhang, Y. Effect of Lacticaseibacillus Paracasei N1115 on Immunomodulatory and Gut Microbial Composition in Young Children: A Randomized, Placebo-Controlled Study. Nutrients 2023, 15, 1970. [Google Scholar] [CrossRef]
- Dierikx, T.; Berkhout, D.; Eck, A.; Tims, S.; Van Limbergen, J.; Visser, D.; De Boer, M.; De Boer, N.; Touw, D.; Benninga, M.; et al. Influence of Timing of Maternal Antibiotic Administration during Caesarean Section on Infant Microbial Colonisation: A Randomised Controlled Trial. Gut 2022, 71, 1803–1811. [Google Scholar] [CrossRef]
- Sánchez, C.; Fente, C.; Regal, P.; Lamas, A.; Lorenzo, M.P. Human Milk Oligosaccharides (HMOs) and Infant Microbiota: A Scoping Review. Foods 2021, 10, 1429. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Tapia, E.; Sebastiani, G.; Sailer, S.; Almeida Toledano, L.; Serra-Delgado, M.; García-Algar, Ó.; Andreu-Fernández, V. Probiotic Supplementation during the Perinatal and Infant Period: Effects on Gut Dysbiosis and Disease. Nutrients 2020, 12, 2243. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Wang, N.; Tan, H.-Y.; Li, S.; Zhang, C.; Feng, Y. Function of Akkermansia Muciniphila in Obesity: Interactions With Lipid Metabolism, Immune Response and Gut Systems. Front. Microbiol. 2020, 11, 219. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M.; Han, R.; Yuan, Y.; Xing, Y.; Zhang, W.; Sun, Z.; Liu, Y.; Li, J.; Mao, T. The Role of Akkermansia Muciniphila in Inflammatory Bowel Disease: Current Knowledge and Perspectives. Front. Immunol. 2023, 13, 1089600. [Google Scholar] [CrossRef]
- Abbasi, A.; Bazzaz, S.; Da Cruz, A.G.; Khorshidian, N.; Saadat, Y.R.; Sabahi, S.; Ozma, M.A.; Lahouty, M.; Aslani, R.; Mortazavian, A.M. A Critical Review on Akkermansia Muciniphila: Functional Mechanisms, Technological Challenges, and Safety Issues. Probiotics Antimicr. Prot. 2023, in press. [Google Scholar] [CrossRef] [PubMed]
- Bull, M.J.; Plummer, N.T. Part 1: The Human Gut Microbiome in Health and Disease. Integr. Med. 2014, 13, 17–22. [Google Scholar]
- Vallianou, N.; Dalamaga, M.; Stratigou, T.; Karampela, I.; Tsigalou, C. Do Antibiotics Cause Obesity Through Long-Term Alterations in the Gut Microbiome? A Review of Current Evidence. Curr. Obes. Rep. 2021, 10, 244–262. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Articles screening strategy | KEYWORDS: A: cesarean delivery; B: infant gut microbiota; C: infant oral microbiota. |
| Boolean Indicators: A AND (B OR C) | |
| Timespan: 2013–2023 | |
| Electronic databases: Pubmed; Scopus; WOS |
| Authors (Year) | Study Design | Number of Patients | Materials and Methods | Outcomes |
|---|---|---|---|---|
| K. Korpela et al., 2018 [83] | Randomized clinical trial | 428 infants | The study conducted an analysis of the GM composition in 428 infants at 3 months of age using fecal samples and 16S rRNA gene amplicon sequencing. Mothers were randomized into control and treatment groups during pregnancy, with the treatment group receiving a mixture of specific bacterial strains. Infants continued to receive these capsules after birth, and fecal samples were collected for analysis. Information on birth mode, breastfeeding, formula feeding, and antibiotic use was obtained through questionnaires. | Newborns’ microbiota composition was significantly influenced by probiotic supplementation; breastfed newborns had higher levels of bifidobacteria and lower levels of proteobacteria and clostridia. Probiotics reversed or lessened the effects of antibiotic usage and birth mode, which were linked to altered microbiota in the placebo group. |
| B. C. Wilson et al., 2021 [84] | Randomized clinical trial | 47 babies | Healthy babies born through cesarean delivery were randomly assigned to receive either sterile water (CS-placebo, n = 13) or a 3 mL solution of maternal vaginal microorganisms (CSseeded, n = 12). Neonatal infants born vaginally (VB, n = 22) served as the reference control. Clinical evaluations were performed within the first two hours after birth as well as at one and three months of age. Shotgun metagenomic sequencing was performed on maternal vaginal extracts and infant stool samples from CS women. The composition of the GM at one month of age was the main result. The functional potential of the gut microbiome, maternal strain engraftment, anthropometry, body composition, and adverse events were all secondary outcomes. | The results showed that vaginal seeding had no discernible effect on the microbiome development of CS-born infants, particularly with regard to Bacteroide colonization, regardless of the dosing technique. Therefore, for infants born through CS, maternal fecal microbiota transplantation (FMT) might be a more successful strategy. Additionally, it was discovered that intrapartum antibiotic prophylaxis (IAP), which is frequently used during CS, decreased the exposure of newborns to maternal microbes and might have a deleterious impact on the survivability of transplanted microbes. In summary, this pilot study suggests that the oral administration of maternal vaginal microbiota did not significantly affect the early gut microbiome of CS-born infants, questioning the utility of this procedure in reducing disease risk. |
| K. M. Tonon et al., 2021 [85] | Cross-sectional study | 48 infants | This study involved a subset of mother–infant pairs participating in a cross-sectional observational study aimed at identifying factors associated with human milk oligosaccharide (HMO) concentrations. The participants included healthy full-term singleton infants who were exclusively breastfed and had not received antibiotics, probiotics, water, or any other food besides human milk. Human milk and infant fecal samples were collected at one month postpartum and processed for analysis. Human milk samples were stored at −20 °C for HMOs analysis. Infant feces were collected from disposable diapers, preserved in an ASL buffer, and stored at −20 °C for DNA extraction. The study involved analyzing the fecal microbiota composition through 16S rRNA gene sequencing, and the main bacterial genera and species were quantified using a qPCR with specific primers. Standard curves for quantification were created using reference gene fragments, and results were expressed as bacterial units per gram of feces (U/g of feces). The detection limit for all organisms was 1 cell/g. | The researchers found that infants born through cesarean had lower levels of Bacteroides, less B. longum, and higher levels of Akkermansia as well as Kluyvera in their GM. Despite these differences, the overall composition of the microbiota did not differ significantly between infants born through cesarean and those born vaginally, provided they were breastfed by secretory mothers. In addition, the study noted an increased presence of Verrucomicrobia and Akkermansia, mainly in CSe+ infants. Akkermansia is a bacterium involved in immune regulation and promotion of the intestinal barrier function, which also is associated with lower risks of obesity and allergies in infants. Another distinctive observation was the higher prevalence of proteobacteria, particularly Serratia and Kluyvera, in this group. This differed from previous studies, probably because of socioeconomic differences between the populations. |
| C. Mei Chien et al., 2017 [86] | Randomized Clinical Trial | 152 babies | Infants were given either a non-hydrolyzed cow’s milk-based formula (control formula), a prebiotic formula supplemented with 0.8 g/100 mL of scGOS/lCFOS, or a synbiotic formula supplemented with B. breve M-16V (Morinaga Milk Industry Co. Ltd.) at a dose of 7.5 108 cfu/100 mL. As a reference group, vaginally delivered infants were included. From birth (1–3 days at the latest) until 16 weeks of age (the intervention phase), and study formulae were given. At day 3, day day 5, week 2, week 4, week 8, week 12, and week 22, stool samples were taken. | This study showed that supplementation with scGOS/lcFOS and B. breve M-16V contributes to the early colonization of bifidobacteria in infants born through CS, reproducing the physiological conditions of the intestinal microbiota observed in vaginally born infants. Positive effects have also been observed in terms of the reduction in adverse events such as skin disorders, particularly eczema/atopic dermatitis. |
| Ilias Lagkouvardos, 2022 [87] | Randomized Clinical Trial | 540 infants |
|
|
| Wenqing Yang et al., 2021 [88] | Observational Cohort Study | 26 neonates |
|
|
| Christophe Lay et al., 2021 [89] | Double-blind randomized controlled study | 153 infants | Newborns’ microbiota compositions were significantly influenced by probiotic supplementation; breastfed newborns had higher levels of bifidobacteria and lower levels of proteobacteria and clostridia. Probiotics reversed or lessened the effects of antibiotic usage and birth mode, which were linked to altered microbiota in the placebo group. | Babies delivered vaginally had an environment in their guts that was hypoxic and acidic, with a higher concentration of stringent anaerobes (Bifidobacteriaceae). Enterobacteriaceae enrichment is a sign of a damaged microbiome in infants born after cesarean delivery. |
| Joanne E Sordillo et al., 2017 [69] | Clinical trial | 333 infants | Microbial diversity was calculated using the Shannon index, and 16S rRNA gene sequencing was employed for infants’ stool samples. | White race/ethnicity was associated with lower diversity but higher Bacteroidetes coabundance scores. CS birth was associated with higher diversity but decreased Bacteroidetes coabundance scores. Infants born through CS had higher firmicutes scores. Infants that were breastfed showed reduced levels of Clostridiales. Vitamin D in cord blood is associated with a rise in Lactococcus but a decrease in lactobacteria. |
| Pin Li et al., 2023 [90] | Randomized, placebo-controlled trial | 109 infants | Saliva and stool samples collected at weeks 0, 4, 8, and 12 from infants aged 6–24 months born through CS. |
|
| Thomas Dierikx et al., 2022 [91] | Randomized controlled trial | CS group (n = 40); vaginal group (n = 23) | Microbiota analyzed through 16S rRNA gene sequencing and whole-metagenome shotgun sequencing. Data collected at 1, 7, and 28 days after birth and at 3 years. |
|
| Yang Liu MD et al., 2023 [10] | Randomized clinical trial | A total of 120 pregnant women were divided into two groups as follows: a “vaginal seeding” group (n = 60) and a control group (n = 60). | This randomized controlled trial was conducted at the Liuyang Maternal and Child Health Care Hospital in China to investigate differences in GM between infants born through cesarean delivery and those born through natural childbirth. In the “vaginal seeding” group, sterile gauze soaked in sterile saline solution was inserted into the maternal vagina one hour before delivery and then used to gently swab the infant’s body after birth. In contrast, the control group received standard care. | The results of the study revealed that there were no significant differences in the GM between the two groups of infants. The analyses found that changes in gut bacterial composition were similar in both the “vaginal seeding” group and the control group. In addition, no significant differences in BMI (body mass index) or allergy risks were found between the two groups during the infants’ first 2 years of life. |
| Joanna Hurkala et al., 2020 [72] | Randomized clinical trial | The recruited infants (148) were divided into two groups as follows: the intervention group (71) and the control group (77). | Newborns were divided into two groups as follows: one group received a probiotic product with specific strains of Bifidobacterium and Lactobacillus shortly after birth, while the other group served as the control. The study aimed to investigate the impact of probiotic supplementation on the early GM of newborns born through CS. Stool samples were collected on days 5 or 6 after birth and again after one month. These samples were analyzed to assess the presence and quantity of bacterial genera and species, including beneficial ones like Lactobacillus and Bifidobacterium as well as potentially harmful bacteria. | The intervention group showed a significant increase in Lactobacillus and bifidobacteria levels in their fecal samples compared with the control group. Lactobacillus levels were high, while bifidobacteria levels were higher, indicating the effectiveness of probiotic supplementation in infants. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inchingolo, F.; Inchingolo, A.D.; Palumbo, I.; Trilli, I.; Guglielmo, M.; Mancini, A.; Palermo, A.; Inchingolo, A.M.; Dipalma, G. The Impact of Cesarean Section Delivery on Intestinal Microbiota: Mechanisms, Consequences, and Perspectives—A Systematic Review. Int. J. Mol. Sci. 2024, 25, 1055. https://doi.org/10.3390/ijms25021055
Inchingolo F, Inchingolo AD, Palumbo I, Trilli I, Guglielmo M, Mancini A, Palermo A, Inchingolo AM, Dipalma G. The Impact of Cesarean Section Delivery on Intestinal Microbiota: Mechanisms, Consequences, and Perspectives—A Systematic Review. International Journal of Molecular Sciences. 2024; 25(2):1055. https://doi.org/10.3390/ijms25021055
Chicago/Turabian StyleInchingolo, Francesco, Alessio Danilo Inchingolo, Irene Palumbo, Irma Trilli, Mariafrancesca Guglielmo, Antonio Mancini, Andrea Palermo, Angelo Michele Inchingolo, and Gianna Dipalma. 2024. "The Impact of Cesarean Section Delivery on Intestinal Microbiota: Mechanisms, Consequences, and Perspectives—A Systematic Review" International Journal of Molecular Sciences 25, no. 2: 1055. https://doi.org/10.3390/ijms25021055
APA StyleInchingolo, F., Inchingolo, A. D., Palumbo, I., Trilli, I., Guglielmo, M., Mancini, A., Palermo, A., Inchingolo, A. M., & Dipalma, G. (2024). The Impact of Cesarean Section Delivery on Intestinal Microbiota: Mechanisms, Consequences, and Perspectives—A Systematic Review. International Journal of Molecular Sciences, 25(2), 1055. https://doi.org/10.3390/ijms25021055