
Protein-Based Predictive Biomarkers to Personalize Neoadjuvant Therapy for Bladder Cancer—A Systematic Review of the Current Status

 , ,
, ,
Abstract
1. Introduction
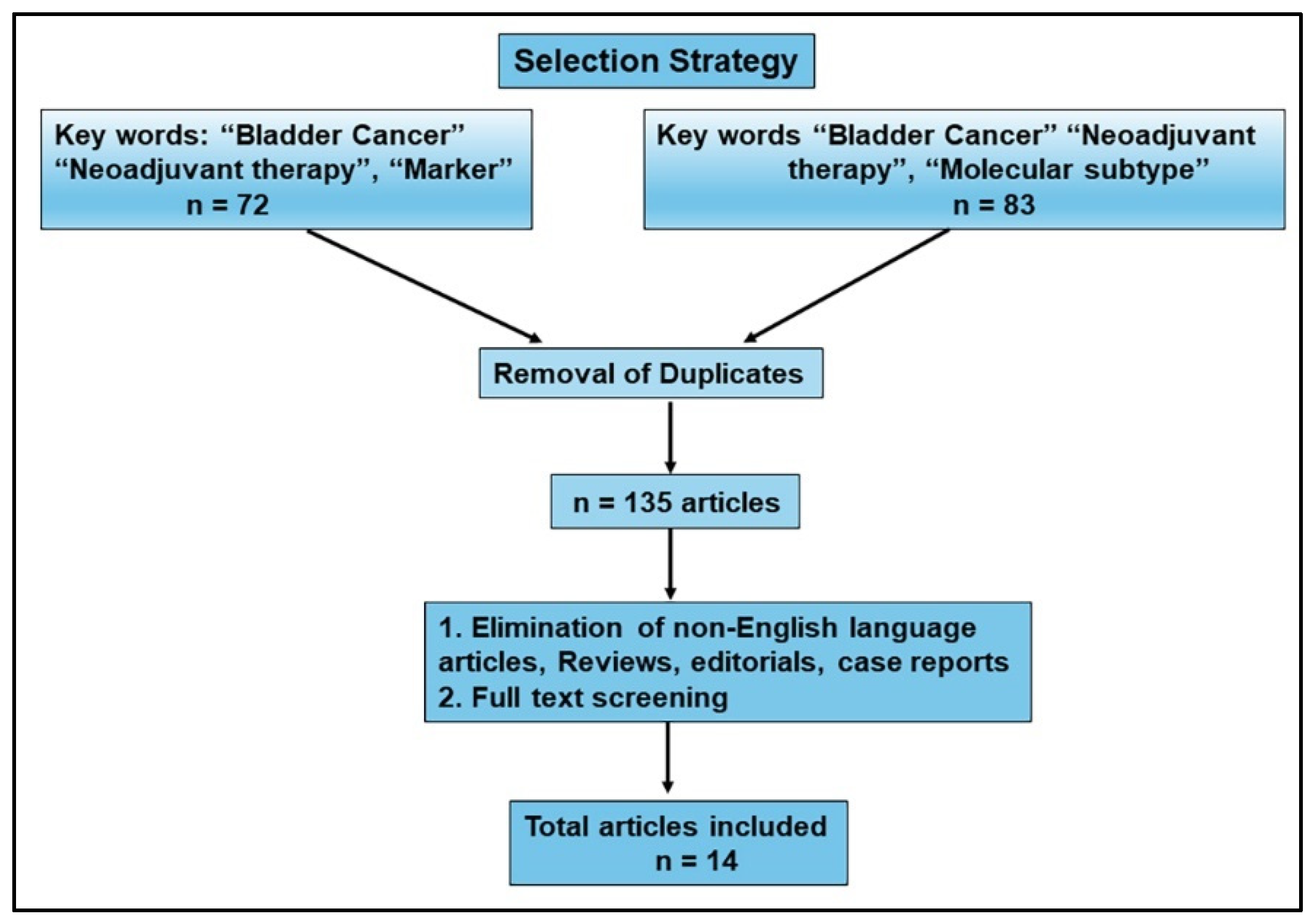
2. Methods
Search Strategy
3. Results
3.1. Literature Review
3.2. Predicting Neoadjuvant Chemotherapy Response
3.3. Using IHC to Characterize Subtypes and Their Response to NAC
3.4. Cancer Stem Cell Markers as Predictors of NAC Response
3.5. Epithelial–Mesenchymal Transition (EMT) Markers as Predictors of NAC Response
3.6. Apoptosis-Related Markers and Response to NAC
3.7. Actin/Cytoskeleton Organization and Its Potential to Predict Response to NAC
3.8. Tumor-Infiltrating Immune Cells for Predicting Response to NAC
4. Discussion and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Contieri, R.; Martini, A.; Mertens, L.S.; Giannatempo, P.; Hurle, R.; Witjes, J.A.; Ribal, M.J.; van Rhijn, B.W.; Malavaud, B. The Financial Burden of Guideline-recommended Cancer Medications for Metastatic Urothelial Carcinoma. Eur. Urol. Focus. 2024, in press. [Google Scholar] [CrossRef] [PubMed]
- Soares, A.; Bourlon, M.T.; Wong, A.; Joshi, A.; Jardim, D.; Korbenfeld, E.; Karak, F.E.; Orlandi, F.; Sze, H.; Ansari, J.; et al. Management of Metastatic Urothelial Carcinoma in Emerging Markets (EM): An Expert Opinion. Clin. Genitourin. Cancer 2024, 22, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.B.; Hudgins, H.K.; Ray-Zack, M.D.; Chamie, K.; Smaldone, M.C.; Boorjian, S.A.; Daneshmand, S.; Black, P.C.; Kamat, A.M.; Goebell, P.J.; et al. Systematic Review of Factors Associated with the Utilization of Radical Cystectomy for Bladder Cancer. Eur. Urol. Oncol. 2019, 2, 119–125. [Google Scholar] [CrossRef]
- Lokeshwar, S.D.; Lopez, M.; Sarcan, S.; Aguilar, K.; Morera, D.S.; Shaheen, D.M.; Lokeshwar, B.L.; Lokeshwar, V.B. Molecular Oncology of Bladder Cancer from Inception to Modern Perspective. Cancers 2022, 14, 2578. [Google Scholar] [CrossRef]
- Kawada, T.; Yanagisawa, T.; Bekku, K.; Laukhtina, E.; von Deimling, M.; Chlosta, M.; Pradere, B.; Teoh, J.Y.; Babjuk, M.; Araki, M.; et al. The efficacy and safety outcomes of lower dose BCG compared to intravesical chemotherapy in non-muscle-invasive bladder cancer: A network meta-analysis. Urol. Oncol. 2023, 41, 261–273. [Google Scholar] [CrossRef]
- Yanagisawa, T.; Quhal, F.; Kawada, T.; Mostafaei, H.; Motlagh, R.S.; Laukhtina, E.; Rajwa, P.; Deimling, M.V.; Bianchi, A.; Pallauf, M.; et al. A Systematic Review and Meta-analysis of Chemoablation for Non-muscle-invasive Bladder Cancer. Eur. Urol. Focus. 2023, 9, 463–479. [Google Scholar] [CrossRef]
- Alfred Witjes, J.; Max Bruins, H.; Carrion, A.; Cathomas, R.; Comperat, E.; Efstathiou, J.A.; Fietkau, R.; Gakis, G.; Lorch, A.; Martini, A.; et al. European Association of Urology Guidelines on Muscle-invasive and Metastatic Bladder Cancer: Summary of the 2023 Guidelines. Eur. Urol. 2024, 85, 17–31. [Google Scholar] [CrossRef]
- Hamid, A.; Ridwan, F.R.; Parikesit, D.; Widia, F.; Mochtar, C.A.; Umbas, R. Meta-analysis of neoadjuvant chemotherapy compared to radical cystectomy alone in improving overall survival of muscle-invasive bladder cancer patients. BMC Urol. 2020, 20, 158. [Google Scholar] [CrossRef]
- Mellema, J.J.; van Rhijn, B.W.G.; van der Heijden, M.S. Recent developments in perioperative combination therapy in muscle-invasive bladder cancer. Curr. Opin. Urol. 2023, 33, 404–411. [Google Scholar] [CrossRef]
- Lopez-Beltran, A.; Cookson, M.S.; Guercio, B.J.; Cheng, L. Advances in diagnosis and treatment of bladder cancer. BMJ 2024, 384, e076743. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Yao, Y.; Guan, F.; Sun, L.; Zhang, G. Neoadjuvant Chemotherapy for Different Stages of Muscle-Invasive Bladder Cancer: A Systematic Review and Meta-analysis. Dis. Markers 2022, 2022, 8493519. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.H.; Cho, K.S.; Moon, Y.J.; Chung, D.Y.; Jung, H.D.; Lee, J.Y. Effect of neoadjuvant chemotherapy on overall survival of patients with T2-4aN0M0 bladder cancer: A systematic review and meta-analysis according to EAU COVID-19 recommendation. PLoS ONE 2022, 17, e0267410. [Google Scholar] [CrossRef] [PubMed]
- Ruiz de Porras, V.; Pardo, J.C.; Etxaniz, O.; Font, A. Neoadjuvant therapy for muscle-invasive bladder cancer: Current clinical scenario, future perspectives, and unsolved questions. Crit. Rev. Oncol. Hematol. 2022, 178, 103795. [Google Scholar] [CrossRef]
- Rani, B.; Ignatz-Hoover, J.J.; Rana, P.S.; Driscoll, J.J. Current and Emerging Strategies to Treat Urothelial Carcinoma. Cancers 2023, 15, 4886. [Google Scholar] [CrossRef]
- Boydell, E.; Sandoval, J.L.; Michielin, O.; Obeid, M.; Addeo, A.; Friedlaender, A. Neoadjuvant Immunotherapy: A Promising New Standard of Care. Int. J. Mol. Sci. 2023, 24, 11849. [Google Scholar] [CrossRef]
- Bedke, J.; Black, P.C.; Szabados, B.; Guerrero-Ramos, F.; Shariat, S.F.; Xylinas, E.; Brinkmann, J.; Blake-Haskins, J.A.; Cesari, R.; Redorta, J.P. Optimizing outcomes for high-risk, non-muscle-invasive bladder cancer: The evolving role of PD-(L)1 inhibition. Urol. Oncol. 2023, 41, 461–475. [Google Scholar] [CrossRef]
- Cathomas, R.; Lorch, A.; Bruins, H.M.; Comperat, E.M.; Cowan, N.C.; Efstathiou, J.A.; Fietkau, R.; Gakis, G.; Hernández, V.; Espinós, E.L.; et al. The 2021 Updated European Association of Urology Guidelines on Metastatic Urothelial Carcinoma. Eur. Urol. 2022, 81, 95–103. [Google Scholar] [CrossRef]
- Ogbuji, V.; Paster, I.C.; Recio-Boiles, A.; Carew, J.S.; Nawrocki, S.T.; Chipollini, J. Current Landscape of Immune Checkpoint Inhibitors for Metastatic Urothelial Carcinoma: Is There a Role for Additional T-Cell Blockade? Cancers 2023, 16, 131. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.C.; Lee, S.; Lee, J.G.; Chen, H.; Zaleski, M.; Choi, W.; McConkey, D.J.; Wei, P.; Czerniak, B. Molecular profile of bladder cancer progression to clinically aggressive subtypes. Nat. Rev. Urol. 2024, 21, 391–405. [Google Scholar] [CrossRef]
- Warrick, J. Molecular Subtypes of Bladder Cancer: Component Signatures and Potential Value in Clinical Decision-making. Adv. Anat. Pathol. 2024, 31, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Morera, D.S.; Hasanali, S.L.; Belew, D.; Ghosh, S.; Klaassen, Z.; Jordan, A.R.; Wang, J.; Terris, M.K.; Bollag, R.J.; Merseburger, A.S.; et al. Clinical parameters outperform molecular subtypes for predicting outcome in bladder cancer: Results from multiple cohorts, including TCGA. J. Urol. 2020, 203, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Galsky, M.D.; Arija, J.A.A.; Bamias, A.; Davis, I.D.; De Santis, M.; Kikuchi, E.; Garcia-Del-Muro, X.; De Giorgi, U.; Mencinger, M.; Izumi, K.; et al. Atezolizumab with or without chemotherapy in metastatic urothelial cancer (IMvigor130): A multicentre, randomised, placebo-controlled phase 3 trial. Lancet 2020, 395, 1547–1557. [Google Scholar] [CrossRef]
- Bahlinger, V.; Hartmann, A.; Eckstein, M. Immunotherapy in Genitourinary Cancers: Role of Surgical Pathologist for Detection of Immunooncologic Predictive Factors. Adv. Anat. Pathol. 2023, 30, 203–210. [Google Scholar] [CrossRef]
- Necchi, A.; Raggi, D.; Gallina, A.; Madison, R.; Colecchia, M.; Luciano, R.; Montironi, R.; Giannatempo, P.; Farè, E.; Pederzoli, F.; et al. Updated Results of PURE-01 with Preliminary Activity of Neoadjuvant Pembrolizumab in Patients with Muscle-invasive Bladder Carcinoma with Variant Histologies. Eur. Urol. 2020, 77, 439–446. [Google Scholar] [CrossRef]
- Necchi, A.; Anichini, A.; Raggi, D.; Briganti, A.; Massa, S.; Luciano, R.; Colecchia, M.; Giannatempo, P.; Mortarini, R.; Bianchi, M.; et al. Pembrolizumab as Neoadjuvant Therapy Before Radical Cystectomy in Patients with Muscle-Invasive Urothelial Bladder Carcinoma (PURE-01): An Open-Label, Single-Arm, Phase II Study. J. Clin. Oncol. 2018, 36, 3353–3360. [Google Scholar] [CrossRef] [PubMed]
- Basile, G.; Bandini, M.; Gibb, E.A.; Ross, J.S.; Raggi, D.; Marandino, L.; Costa de Padua, T.; Crupi, E.; Colombo, R.; Colecchia, M.; et al. Neoadjuvant Pembrolizumab and Radical Cystectomy in Patients with Muscle-Invasive Urothelial Bladder Cancer: 3-Year Median Follow-Up Update of PURE-01 Trial. Clin. Cancer Res. 2022, 28, 5107–5114. [Google Scholar] [CrossRef]
- Powles, T.; Csoszi, T.; Ozguroglu, M.; Matsubara, N.; Geczi, L.; Cheng, S.Y.; Fradet, Y.; Oudard, S.; Vulsteke, C.; Morales Barrera, R.; et al. Pembrolizumab alone or combined with chemotherapy versus chemotherapy as first-line therapy for advanced urothelial carcinoma (KEYNOTE-361): A randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 931–945. [Google Scholar] [CrossRef]
- Garcia-Perdomo, H.A.; Davila-Raigoza, A.M.; Korkes, F. Metabolomics for the diagnosis of bladder cancer: A systematic review. Asian J. Urol. 2024, 11, 221–241. [Google Scholar] [CrossRef]
- Pereira, F.; Domingues, M.R.; Vitorino, R.; Guerra, I.M.S.; Santos, L.L.; Ferreira, J.A.; Ferreira, R. Unmasking the Metabolite Signature of Bladder Cancer: A Systematic Review. Int. J. Mol. Sci. 2024, 25, 3347. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Uman, L.S. Systematic reviews and meta-analyses. J. Can. Acad. Child. Adolesc. Psychiatry 2011, 20, 57–59. [Google Scholar] [PubMed]
- Helal, D.S.; Darwish, S.A.; Awad, R.A.; Ali, D.A.; El-Guindy, D.M. Immunohistochemical based molecular subtypes of muscle-invasive bladder cancer: Association with HER2 and EGFR alterations, neoadjuvant chemotherapy response and survival. Diagn. Pathol. 2023, 18, 11. [Google Scholar] [CrossRef] [PubMed]
- Morselli, S.; Campi, R.; Gacci, M.; Sebastianelli, A.; Fattorini, C.; Villari, D.; Carini, M.; Minervini, A.; Serni, S.; Raspollini, M.R. Potential utility of a 4-marker immunohistochemistry panel to predict response to cisplatin-based neoadjuvant chemotherapy in patients with muscle-invasive bladder cancer: A single-center preliminary experience. Minerva Urol. Nephrol. 2021, 73, 424–427. [Google Scholar] [CrossRef]
- Pryma, C.; Villamil, C.; Gibb, E.A.; Oo, H.Z.; Seiler, R.; Contreras-Sanz, A.; Douglas, J.; Black, P.C.; Wang, G. Uroplakin II as a single marker for luminal versus basal molecular subtypes in muscle invasive urothelial carcinoma. Virchows Arch. 2022, 481, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Razzaghdoust, A.; Ghajari, M.; Basiri, A.; Torbati, P.M.; Jafari, A.; Fattahi, M.R.; Salahi, M.; Mofid, B. Association of immunohistochemical markers of tumor subtype with response to neoadjuvant chemotherapy and survival in patients with muscle-invasive bladder cancer. Investig. Clin. Urol. 2021, 62, 274–281. [Google Scholar] [CrossRef]
- Sjödahl, G.; Abrahamsson, J.; Holmsten, K.; Bernardo, C.; Chebil, G.; Eriksson, P.; Johansson, I.; Kollberg, P.; Lindh, C.; Lövgren, K.; et al. Different Responses to Neoadjuvant Chemotherapy in Urothelial Carcinoma Molecular Subtypes. Eur. Urol. 2022, 81, 523–532. [Google Scholar] [CrossRef]
- Schallenberg, S.; Dragomir, M.P.; Anders, P.; Ebner, B.; Volz, Y.; Eismann, L.; Rodler, S.; Casuscelli, J.; Buchner, A.; Klauschen, F.; et al. Intratumoral Heterogeneity of Molecular Subtypes in Muscle-invasive Bladder Cancer-An Extensive Multiregional Immunohistochemical Analysis. Eur. Urol. Focus. 2023, 9, 788–798. [Google Scholar] [CrossRef]
- Blomqvist, M.; Koskinen, I.; Löyttyniemi, E.; Mirtti, T.; Boström, P.J.; Taimen, P. Prognostic and predictive value of ALDH1, SOX2 and SSEA-4 in bladder cancer. Sci. Rep. 2021, 11, 13684. [Google Scholar] [CrossRef]
- Hensley, P.J.; Kyprianou, N.; Purdom, M.S.; He, D.; DiCarlo, V.; Wang, C.; James, A.C. Predictive Value of Phenotypic Signatures of Bladder Cancer Response to Cisplatin-Based Neoadjuvant Chemotherapy; Elsevier: Amsterdam, The Netherlands, 2019; pp. 572.e1–572.e11. [Google Scholar]
- Turker, P.; Segersten, U.; Malmström, P.-U.; Hemdan, T. Is Bcl-2 a predictive marker of neoadjuvant chemotherapy response in patients with urothelial bladder cancer undergoing radical cystectomy? Scand. J. Urol. 2019, 53, 45–50. [Google Scholar] [CrossRef]
- Türker, P.; Wernroth, M.-L.; Malmström, P.-U.; Segersten, U.; Hemdan, T. Combination of biomarkers for neoadjuvant systemic chemotherapy before cystectomy in patients with urinary bladder cancer. Transl. Res. 2021, 235, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Taniyama, D.; Sakamoto, N.; Takashima, T.; Takeda, M.; Pham, Q.T.; Ukai, S.; Maruyama, R.; Harada, K.; Babasaki, T.; Sekino, Y.; et al. Prognostic impact of Schlafen 11 in bladder cancer patients treated with platinum-based chemotherapy. Cancer Sci. 2022, 113, 784–795. [Google Scholar] [CrossRef] [PubMed]
- Wahlin, S.; Nodin, B.; Leandersson, K.; Boman, K.; Jirström, K. Clinical impact of T cells, B cells and the PD-1/PD-L1 pathway in muscle invasive bladder cancer: A comparative study of transurethral resection and cystectomy specimens. Oncoimmunology 2019, 8, e1644108. [Google Scholar] [CrossRef] [PubMed]
- Beckabir, W.; Wobker, S.E.; Damrauer, J.S.; Midkiff, B.; De la Cruz, G.; Makarov, V.; Flick, L.; Woodcock, M.G.; Grivas, P.; Bjurlin, M.A.; et al. Spatial Relationships in the Tumor Microenvironment Demonstrate Association with Pathologic Response to Neoadjuvant Chemoimmunotherapy in Muscle-invasive Bladder Cancer. Eur. Urol. 2024, 85, 242–253. [Google Scholar] [CrossRef]
- Myint, Z.W.; Chahine, Z.; Jayswal, R.; Bachert, E.; McDonald, R.J.; Strup, S.E.; James, A.C.; Hensley, P.J.; Allison, D.B. Association of CD47 Expression with Clinicopathologic Characteristics and Survival Outcomes in Muscle Invasive Bladder Cancer. J. Pers. Med. 2023, 13, 885. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.; Czerniak, B.; Ochoa, A.; Su, X.; Siefker-Radtke, A.; Dinney, C.; McConkey, D.J. Intrinsic basal and luminal subtypes of muscle-invasive bladder cancer. Nat. Rev. Urol. 2014, 11, 400–410. [Google Scholar] [CrossRef]
- Kamoun, A.; de Reyniès, A.; Allory, Y.; Sjödahl, G.; Robertson, A.G.; Seiler, R.; Hoadley, K.A.; Groeneveld, C.S.; Al-Ahmadie, H.; Choi, W.; et al. A Consensus Molecular Classification of Muscle-invasive Bladder Cancer. Eur. Urol. 2020, 77, 420–433. [Google Scholar] [CrossRef]
- Seiler, R.; Ashab, H.A.D.; Erho, N.; van Rhijn, B.W.G.; Winters, B.; Douglas, J.; Van Kessel, K.E.; Fransen van de Putte, E.E.; Sommerlad, M.; Wang, N.Q.; et al. Impact of Molecular Subtypes in Muscle-invasive Bladder Cancer on Predicting Response and Survival after Neoadjuvant Chemotherapy. Eur. Urol. 2017, 72, 544–554. [Google Scholar] [CrossRef]
- Choi, W.; Porten, S.; Kim, S.; Willis, D.; Plimack, E.R.; Hoffman-Censits, J.; Roth, B.; Cheng, T.; Tran, M.; Lee, I.L.; et al. Identification of distinct basal and luminal subtypes of muscle-invasive bladder cancer with different sensitivities to frontline chemotherapy. Cancer Cell 2014, 25, 152–165. [Google Scholar] [CrossRef] [PubMed]
- Yorozu, T.; Sato, S.; Kimura, T.; Iwatani, K.; Onuma, H.; Yanagisawa, T.; Miki, J.; Egawa, S.; Ikegami, M.; Takahashi, H. HER2 Status in Molecular Subtypes of Urothelial Carcinoma of the Renal Pelvis and Ureter. Clin. Genitourin. Cancer 2020, 18, e443–e449. [Google Scholar] [CrossRef]
- Pagni, F.; Zannella, S.; Ronchi, S.; Garanzini, C.; Leone, B.E. HER2 status of gastric carcinoma and corresponding lymph node metastasis. Pathol. Oncol. Res. 2013, 19, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Sigismund, S.; Avanzato, D.; Lanzetti, L. Emerging functions of the EGFR in cancer. Mol. Oncol. 2018, 12, 3–20. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, P.; Sjödahl, G.; Chebil, G.; Liedberg, F.; Höglund, M. HER2 and EGFR amplification and expression in urothelial carcinoma occurs in distinct biological and molecular contexts. Oncotarget 2017, 8, 48905–48914. [Google Scholar] [CrossRef] [PubMed]
- Höglund, M.; Bernardo, C.; Sjödahl, G.; Eriksson, P.; Axelson, H.; Liedberg, F. The Lund taxonomy for bladder cancer classification—From gene expression clustering to cancer cell molecular phenotypes, and back again. J. Pathol. 2023, 259, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Tian, W.; Guner, G.; Miyamoto, H.; Cimino-Mathews, A.; Gonzalez-Roibon, N.; Argani, P.; Li, X.; Sharma, R.; Subhawong, A.P.; Rezaei, K.; et al. Utility of uroplakin II expression as a marker of urothelial carcinoma. Hum. Pathol. 2015, 46, 58–64. [Google Scholar] [CrossRef]
- Cyll, K.; Ersvær, E.; Vlatkovic, L.; Pradhan, M.; Kildal, W.; Avranden Kjær, M.; Kleppe, A.; Hveem, T.S.; Carlsen, B.; Gill, S.; et al. Tumour heterogeneity poses a significant challenge to cancer biomarker research. Br. J. Cancer 2017, 117, 367–375. [Google Scholar] [CrossRef]
- Zhou, H.; Hu, Y.; Luo, R.; Zhao, Y.; Pan, H.; Ji, L.; Zhou, T.; Zhang, L.; Long, H.; Fu, J.; et al. Multi-region exome sequencing reveals the intratumoral heterogeneity of surgically resected small cell lung cancer. Nat. Commun. 2021, 12, 5431. [Google Scholar] [CrossRef] [PubMed]
- Sjödahl, G.; Eriksson, P.; Lövgren, K.; Bernardo, C.; Nordentoft, I.; Dyrskjøt, L.; Liedberg, F.; Höglund, M. Discordant molecular subtype classification in the basal-squamous subtype of bladder tumors and matched lymph-node metastases. Mod. Pathol. 2018, 31, 1869–1881. [Google Scholar] [CrossRef]
- Sirab, N.; Drubay, D.; Maillé, P.; Popova, T.; Ngo, C.; Gentien, D.; Moktefi, A.; Soyeux-Porte, P.; Pelletier, R.; Reyes, C.; et al. Multilayer spectrum of intratumoral heterogeneity in basal bladder cancer. J. Pathol. 2022, 256, 108–118. [Google Scholar] [CrossRef]
- Jakobsson, L.; Chebil, G.; Marzouka, N.-A.-D.; Liedberg, F.; Sjödahl, G. Low frequency of intratumor heterogeneity in bladder cancer tissue microarrays. Bladder Cancer 2018, 4, 327–337. [Google Scholar] [CrossRef]
- Beck, B.; Blanpain, C. Unravelling cancer stem cell potential. Nat. Rev. Cancer 2013, 13, 727–738. [Google Scholar] [CrossRef] [PubMed]
- Allegra, A.; Alonci, A.; Penna, G.; Innao, V.; Gerace, D.; Rotondo, F.; Musolino, C. The cancer stem cell hypothesis: A guide to potential molecular targets. Cancer Investig. 2014, 32, 470–495. [Google Scholar] [CrossRef]
- Haselbeck, R.J.; Hoffmann, I.; Duester, G. Distinct functions for Aldh1 and Raldh2 in the control of ligand production for embryonic retinoid signaling pathways. Dev. Genet. 1999, 25, 353–364. [Google Scholar] [CrossRef]
- Huang, E.H.; Hynes, M.J.; Zhang, T.; Ginestier, C.; Dontu, G.; Appelman, H.; Fields, J.Z.; Wicha, M.S.; Boman, B.M. Aldehyde dehydrogenase 1 is a marker for normal and malignant human colonic stem cells (SC) and tracks SC overpopulation during colon tumorigenesis. Cancer Res. 2009, 69, 3382–3389. [Google Scholar] [CrossRef] [PubMed]
- Keymoosi, H.; Gheytanchi, E.; Asgari, M.; Shariftabrizi, A.; Madjd, Z. ALDH1 in combination with CD44 as putative cancer stem cell markers are correlated with poor prognosis in urothelial carcinoma of the urinary bladder. Asian Pac. J. Cancer Prev. 2014, 15, 2013–2020. [Google Scholar] [CrossRef]
- Su, Y.; Qiu, Q.; Zhang, X.; Jiang, Z.; Leng, Q.; Liu, Z.; Stass, S.A.; Jiang, F. Aldehyde dehydrogenase 1 A1-positive cell population is enriched in tumor-initiating cells and associated with progression of bladder cancer. Cancer Epidemiol. Biomark. Prev. 2010, 19, 327–337. [Google Scholar] [CrossRef]
- Senol, S.; Yildırım, A.; Akalin, I.; Uruç, F.; Çobanoğlu, B.; Yilmaz, S.; Ceyran, B.; Kösemetin, D.; Ece, D.; Aydın, A. Relation of stem cell markers ALDH1 and CD44 with clinicopathological factors in urothelial carcinomas of urinary bladder. Int. J. Clin. Exp. Med. 2015, 8, 4195–4203. [Google Scholar]
- Sarkar, A.; Hochedlinger, K. The sox family of transcription factors: Versatile regulators of stem and progenitor cell fate. Cell Stem Cell 2013, 12, 15–30. [Google Scholar] [CrossRef]
- Takahashi, K.; Yamanaka, S. Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell 2006, 126, 663–676. [Google Scholar] [CrossRef]
- Arnold, K.; Sarkar, A.; Yram, M.A.; Polo, J.M.; Bronson, R.; Sengupta, S.; Seandel, M.; Geijsen, N.; Hochedlinger, K. Sox2(+) adult stem and progenitor cells are important for tissue regeneration and survival of mice. Cell Stem Cell 2011, 9, 317–329. [Google Scholar] [CrossRef]
- Lundberg, I.V.; Löfgren Burström, A.; Edin, S.; Eklöf, V.; Öberg, Å.; Stenling, R.; Palmqvist, R.; Wikberg, M.L. SOX2 expression is regulated by BRAF and contributes to poor patient prognosis in colorectal cancer. PLoS ONE 2014, 9, e101957. [Google Scholar] [CrossRef] [PubMed]
- Sholl, L.M.; Barletta, J.A.; Yeap, B.Y.; Chirieac, L.R.; Hornick, J.L. Sox2 protein expression is an independent poor prognostic indicator in stage I lung adenocarcinoma. Am. J. Surg. Pathol. 2010, 34, 1193–1198. [Google Scholar] [CrossRef]
- Russo, M.V.; Esposito, S.; Tupone, M.G.; Manzoli, L.; Airoldi, I.; Pompa, P.; Cindolo, L.; Schips, L.; Sorrentino, C.; Di Carlo, E. SOX2 boosts major tumor progression genes in prostate cancer and is a functional biomarker of lymph node metastasis. Oncotarget 2016, 7, 12372–12385. [Google Scholar] [CrossRef]
- Ruan, J.; Wei, B.; Xu, Z.; Yang, S.; Zhou, Y.; Yu, M.; Liang, J.; Jin, K.; Huang, X.; Lu, P.; et al. Predictive value of Sox2 expression in transurethral resection specimens in patients with T1 bladder cancer. Med. Oncol. 2013, 30, 445. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Miyata, Y.; Matsuo, T.; Shida, Y.; Hakariya, T.; Ohba, K.; Taima, T.; Ito, A.; Suda, T.; Hakomori, S.I.; et al. Stage-specific embryonic antigen-4 is a histological marker reflecting the malignant behavior of prostate cancer. Glycoconj. J. 2019, 36, 409–418. [Google Scholar] [CrossRef]
- Gheldof, A.; Berx, G. Cadherins and epithelial-to-mesenchymal transition. Prog. Mol. Biol. Transl. Sci. 2013, 116, 317–336. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.H.; Cooper, L.M.; Anastasiadis, P.Z. Cadherins and catenins in cancer: Connecting cancer pathways and tumor microenvironment. Front. Cell Dev. Biol. 2023, 11, 1137013. [Google Scholar] [CrossRef]
- Dev, A., Jr.; Vachher, M.; Prasad, C.P. beta-catenin inhibitors in cancer therapeutics: Intricacies and way forward. Bioengineered 2023, 14, 2251696. [Google Scholar] [CrossRef]
- Martin, B.; Paesmans, M.; Berghmans, T.; Branle, F.; Ghisdal, L.; Mascaux, C.; Meert, A.P.; Steels, E.; Vallot, F.; Verdebout, J.M.; et al. Role of Bcl-2 as a prognostic factor for survival in lung cancer: A systematic review of the literature with meta-analysis. Br. J. Cancer 2003, 89, 55–64. [Google Scholar] [CrossRef]
- Seong, M.-K.; Lee, J.-Y.; Byeon, J.; Sohn, Y.-J.; Seol, H.; Lee, J.-K.; Kim, E.K.; Kim, H.A.; Noh, W.C. Bcl-2 is a highly significant prognostic marker of hormone-receptor-positive, human epidermal growth factor receptor-2-negative breast cancer. Breast Cancer Res. Treat. 2015, 150, 141–148. [Google Scholar] [CrossRef]
- Yoshino, T.; Shiina, H.; Urakami, S.; Kikuno, N.; Yoneda, T.; Shigeno, K.; Igawa, M. Bcl-2 expression as a predictive marker of hormone-refractory prostate cancer treated with taxane-based chemotherapy. Clin. Cancer Res. 2006, 12, 6116–6124. [Google Scholar] [CrossRef] [PubMed]
- Cooke, P.; James, N.; Ganesan, R.; Burton, A.; Young, L.; Wallace, D. Bcl-2 expression identifies patients with advanced bladder cancer treated by radiotherapy who benefit from neoadjuvant chemotherapy. BJU Int. 2000, 85, 829–835. [Google Scholar] [CrossRef] [PubMed]
- Kiss, B.; Skuginna, V.; Fleischmann, A.; Bell, R.H.; Collins, C.; Thalmann, G.N.; Seiler, R. Bcl-2 Predicts Response to Neoadjuvant Chemotherapy and Is Overexpressed in Lymph Node Metastases of Urothelial Cancer of the Bladder; Elsevier: Amsterdam, The Netherlands, 2015; pp. 166.e1–166.e8. [Google Scholar]
- Guo, H.; Li, R.; Zucker, S.; Toole, B.P. EMMPRIN (CD147), an inducer of matrix metalloproteinase synthesis, also binds interstitial collagenase to the tumor cell surface. Cancer Res. 2000, 60, 888–891. [Google Scholar] [PubMed]
- Wheatley, S.P.; Altieri, D.C. Survivin at a glance. J. Cell Sci. 2019, 132, jcs223826. [Google Scholar] [CrossRef]
- Als, A.B.; Dyrskjøt, L.; von der Maase, H.; Koed, K.; Mansilla, F.; Toldbod, H.E.; Jensen, J.L.; Ulhøi, B.P.; Sengeløv, L.; Jensen, K.M.; et al. Emmprin and survivin predict response and survival following cisplatin-containing chemotherapy in patients with advanced bladder cancer. Clin. Cancer Res. 2007, 13, 4407–4414. [Google Scholar] [CrossRef]
- Vaezi, A.E.; Bepler, G.; Bhagwat, N.R.; Malysa, A.; Rubatt, J.M.; Chen, W.; Hood, B.L.; Conrads, T.P.; Wang, L.; Kemp, C.E.; et al. Choline phosphate cytidylyltransferase-α is a novel antigen detected by the anti-ERCC1 antibody 8F1 with biomarker value in patients with lung and head and neck squamous cell carcinomas. Cancer 2014, 120, 1898–1907. [Google Scholar] [CrossRef]
- Hemdan, T.; Turker, P.; Malmström, P.-U.; Segersten, U. Choline-phosphate cytidylyltransferase-α as a possible predictor of survival and response to cisplatin neoadjuvant chemotherapy in urothelial cancer of the bladder. Scand. J. Urol. 2018, 52, 200–205. [Google Scholar] [CrossRef]
- Collazo, J.; Zhu, B.; Larkin, S.; Martin, S.K.; Pu, H.; Horbinski, C.; Koochekpour, S.; Kyprianou, N. Cofilin drives cell-invasive and metastatic responses to TGF-β in prostate cancer. Cancer Res. 2014, 74, 2362–2373. [Google Scholar] [CrossRef]
- Lv, S.; Chen, Z.; Mi, H.; Yu, X. Cofilin Acts as a Booster for Progression of Malignant Tumors Represented by Glioma. Cancer Manag. Res. 2022, 14, 3245–3269. [Google Scholar] [CrossRef]
- Hensley, P.J.; Zetter, D.; Horbinski, C.M.; Strup, S.E.; Kyprianou, N. Association of epithelial-mesenchymal transition and nuclear cofilin with advanced urothelial cancer. Hum. Pathol. 2016, 57, 68–77. [Google Scholar] [CrossRef]
- Schreiber, R.D.; Old, L.J.; Smyth, M.J. Cancer immunoediting: Integrating immunity’s roles in cancer suppression and promotion. Science 2011, 331, 1565–1570. [Google Scholar] [CrossRef] [PubMed]
- Yu, A.; Mansure, J.J.; Solanki, S.; Siemens, D.R.; Koti, M.; Dias, A.B.; Burnier, M.M.; Brimo, F.; Kassouf, W. Presence of lymphocytic infiltrate cytotoxic T lymphocyte CD3+, CD8+, and immunoscore as prognostic marker in patients after radical cystectomy. PLoS ONE 2018, 13, e0205746. [Google Scholar] [CrossRef] [PubMed]
- Winerdal, M.E.; Krantz, D.; Hartana, C.A.; Zirakzadeh, A.A.; Linton, L.; Bergman, E.A.; Rosenblatt, R.; Vasko, J.; Alamdari, F.; Hansson, J. Urinary bladder cancer tregs suppress MMP2 and potentially regulate invasiveness. Cancer Immunol. Res. 2018, 6, 528–538. [Google Scholar] [CrossRef]
- Laumont, C.M.; Nelson, B.H. B cells in the tumor microenvironment: Multi-faceted organizers, regulators, and effectors of anti-tumor immunity. Cancer Cell 2023, 41, 466–489. [Google Scholar] [CrossRef] [PubMed]
- Bardhan, K.; Anagnostou, T.; Boussiotis, V.A. The PD1: PD-L1/2 pathway from discovery to clinical implementation. Front. Immunol. 2016, 7, 550. [Google Scholar] [CrossRef]
- Rose, T.L.; Harrison, M.R.; Deal, A.M.; Ramalingam, S.; Whang, Y.E.; Brower, B.; Dunn, M.; Osterman, C.K.; Heiling, H.M.; Bjurlin, M.A.; et al. Phase II Study of Gemcitabine and Split-Dose Cisplatin Plus Pembrolizumab as Neoadjuvant Therapy Before Radical Cystectomy in Patients with Muscle-Invasive Bladder Cancer. J. Clin. Oncol. 2021, 39, 3140–3148. [Google Scholar] [CrossRef]
- Olcucuoglu, E.; Sirin, M.E.; Aydog, G.; Gazel, E.; Tastemur, S.; Odabas, O. Relationship between immunohistochemical staining extent of CD47 and histopathologic features of bladder tumor. Cent. Eur. J. Urol. 2017, 70, 349. [Google Scholar]
- Xu, N.; Shao, M.-M.; Zhang, H.-T.; Jin, M.-S.; Dong, Y.; Ou, R.-J.; Wang, H.M.; Shi, A.P. Aldehyde dehydrogenase 1 (ALDH1) expression is associated with a poor prognosis of bladder cancer. Cancer Epidemiol. 2015, 39, 375–381. [Google Scholar] [CrossRef]
- Hu, R.; Tao, T.; Yu, L.; Ding, Q.; Zhu, G.; Peng, G.; Zheng, S.; Yang, L.; Wu, S. Multi-Omics Characterization of Tumor Microenvironment Heterogeneity and Immunotherapy Resistance Through Cell States–Based Subtyping in Bladder Cancer. Front. Cell Dev. Biol. 2022, 9, 809588. [Google Scholar] [CrossRef]
- Lerner, S.P.; McConkey, D.J.; Tangen, C.M.; Meeks, J.J.; Flaig, T.W.; Hua, X.; Daneshmand, S.; Alva, A.S.; Lucia, M.S.; Theodorescu, D.; et al. Association of Molecular Subtypes with Pathologic Response, PFS, and OS in a Phase II Study of COXEN with Neoadjuvant Chemotherapy for Muscle-invasive Bladder Cancer. Clin. Cancer Res. 2024, 30, 444–449. [Google Scholar] [CrossRef]

{kind=link}
| PMID & Reference | a Markers | Sample Size | d Study Type | Tumor Grade | T-Stage | NAC Regimen | i Clinical Outcome | j Statistical Methods | Predictive Biomarkers (p-Values) |
|---|---|---|---|---|---|---|---|---|---|
| 36737799 [33] | KRT5, KRT6, GATA3, p53, HER2, EGFR | 60 | Single | HG | T2–T4 | f Gem+Cis; Cis ineligible Gem+Carbo | CR; OS; DFS | KM; Cox | NAC response correlates with KRT5/6 (+) (basal subtype (p = 0.045) |
| 34494414 [34] | KRT5, KRT6, KRT20, CD44, GATA3 | 16 | Single | Not provided | Ta–T4a | Gem + Cis | CR; PR | Descriptive | KRT20 (p = 0.013) small study |
| 35612672 [35] | UPII | 80 | Multi | e Not provided | T2–T4 | Not provided | OS; CSS | KM | Not significant Prediction of luminal subtype–cut-off 50% -> 90% accuracy |
| 33943049 [36] | KRT5, KRT6, KRT20 | 63 | Multi | LG (2); HG (61) | LG: Ta; HG tumors: T2–T4 | Gem+Cis; cis ineligible—Gem+Carbo | CR; OS | LR; KM; Cox | KRT5/6 (+)/KRT20 (−) combined marker (p = 0.037) |
| 34782206 [37] | 13-Marker LundTax Panel | 148 | Multi | Gx, G2, G3 | T2–T4 | Cis-based | CR; PR; NR | KM; Cox | Basal/squamous subtype: Poor response; osteopontin–subtype dependent response prediction |
| 37076398 [38] | c 12 markers | 208 | Single | Not provided | T2–T4 | Not provided | DFS | KM; LR; Chi-sq; FE | None significant |
| 34211078 [39] | ALDH1, SOX2, SSEA-4 | 269 | Multi | LG (1); HG (68); Unknown (5) | Ta, Tis, T1 = 22 T2–T4 | Gem+Cis (90% pts); Gem+Carbo (10% pts) | CR; PR | KM; Chi-sq | None significant |
| 31326313 [40] | E-cadherin, N-cadherin, vimentin, zeb-1, β-catenin, cofilin, phospho cofilin α-tubulin | 90 | Multi | Not provided | T2 | MVAC or Gem+Cis | OC vs. EV; CR | LR; KM; WSR; HM | NAC response prediction: N-cadherin (p = 0.027); α-tubulin (p = 0.037) |
| 30806186 [41] | Bcl-2 | 247 | Multi | Not provided | T2–T4 | MVAC | OS | LR; KM; Cox | Not significant |
| 33766713 [42] | Emmprin, Survivin, Bcl-2, CCTα | 639 | Multi | Not provided | T2–T4 | MVAC | OS | KM; Cox | CCTα (p = 0.009); CCTα (-)/Emmprin (-) better survival |
| 34808009 [43] | SLFN11 | 120 | Multi | LG (6); HG (44) | T2–T4 | Carbo or Cis based | OS | KM; Cox | SLFN11 (p = 0.018) |
| 31646091 [44] | CD8, FoxP3, CD20, PD-1, PD-L1 | 135 | Single | HG | T2–T4 | g MVAC; plus adjuvant chemotherapy | CR; PR | KM; Cox | None significant |
| 38092611 [45] | b proteomic digital spatial profiling–52 markers | 36 | Multi | Not provided | T2–T4 | h Gem+Cis + Immunotherapy | OS; CR; PR | KM, FE, WSR, DL | Intratumoral heterogeneity of DSP markers; certain DSP-based markers (Ki67; HER2) in a spatial context potentially predict response |
| 37373873 [46] | CD47 | 87 | Single | HG | T2–T4 | Cis-based | CR; PR | KM; Cox | Not significant |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bedore, S.; van der Eerden, J.; Boghani, F.; Patel, S.J.; Yassin, S.; Aguilar, K.; Lokeshwar, V.B. Protein-Based Predictive Biomarkers to Personalize Neoadjuvant Therapy for Bladder Cancer—A Systematic Review of the Current Status. Int. J. Mol. Sci. 2024, 25, 9899. https://doi.org/10.3390/ijms25189899
Bedore S, van der Eerden J, Boghani F, Patel SJ, Yassin S, Aguilar K, Lokeshwar VB. Protein-Based Predictive Biomarkers to Personalize Neoadjuvant Therapy for Bladder Cancer—A Systematic Review of the Current Status. International Journal of Molecular Sciences. 2024; 25(18):9899. https://doi.org/10.3390/ijms25189899
Chicago/Turabian StyleBedore, Stacy, Joshua van der Eerden, Faizan Boghani, Saloni J. Patel, Samer Yassin, Karina Aguilar, and Vinata B. Lokeshwar. 2024. "Protein-Based Predictive Biomarkers to Personalize Neoadjuvant Therapy for Bladder Cancer—A Systematic Review of the Current Status" International Journal of Molecular Sciences 25, no. 18: 9899. https://doi.org/10.3390/ijms25189899
APA StyleBedore, S., van der Eerden, J., Boghani, F., Patel, S. J., Yassin, S., Aguilar, K., & Lokeshwar, V. B. (2024). Protein-Based Predictive Biomarkers to Personalize Neoadjuvant Therapy for Bladder Cancer—A Systematic Review of the Current Status. International Journal of Molecular Sciences, 25(18), 9899. https://doi.org/10.3390/ijms25189899