
SOAT1: A Suitable Target for Therapy in High-Grade Astrocytic Glioma?

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Tissue Samples
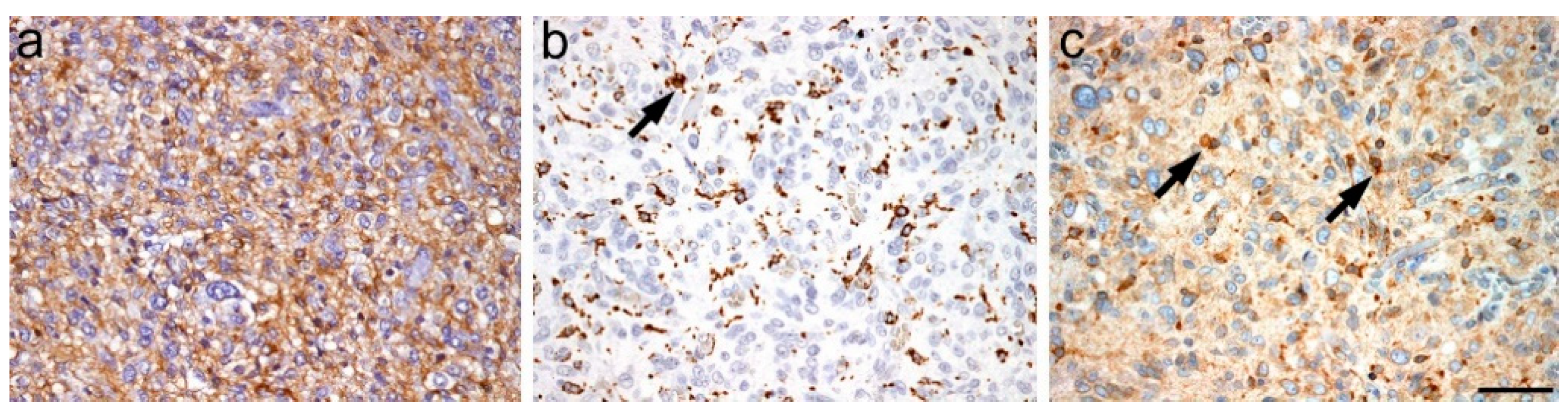
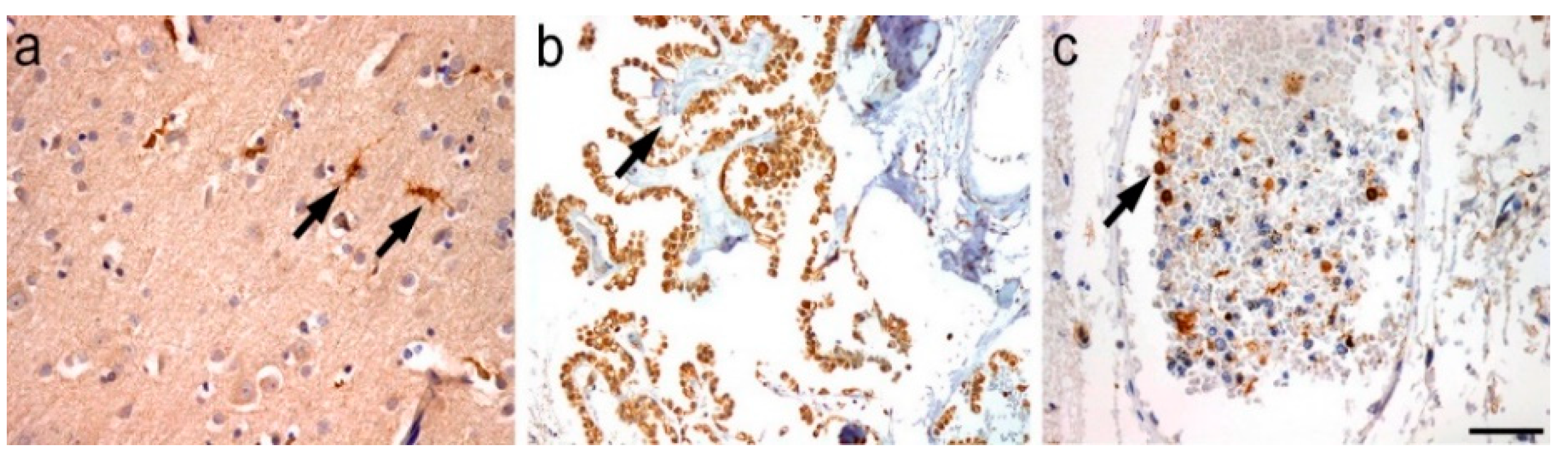
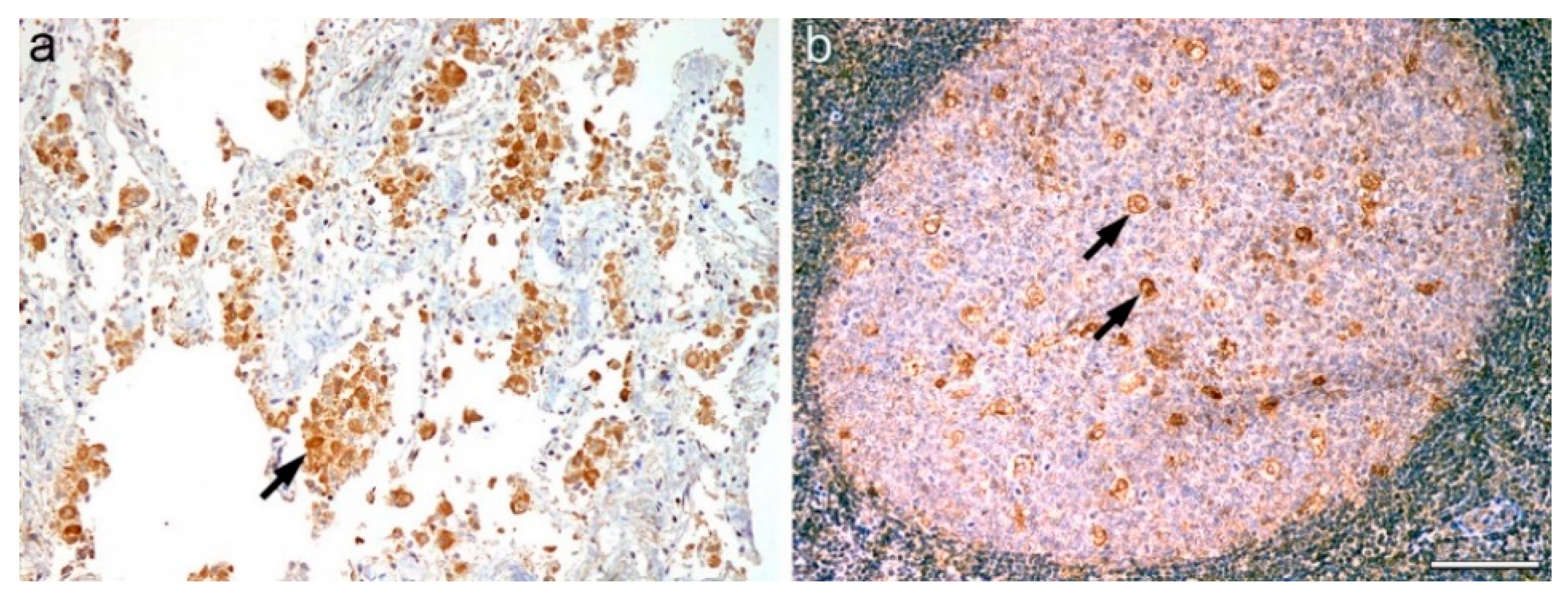
2.2. Single Staining
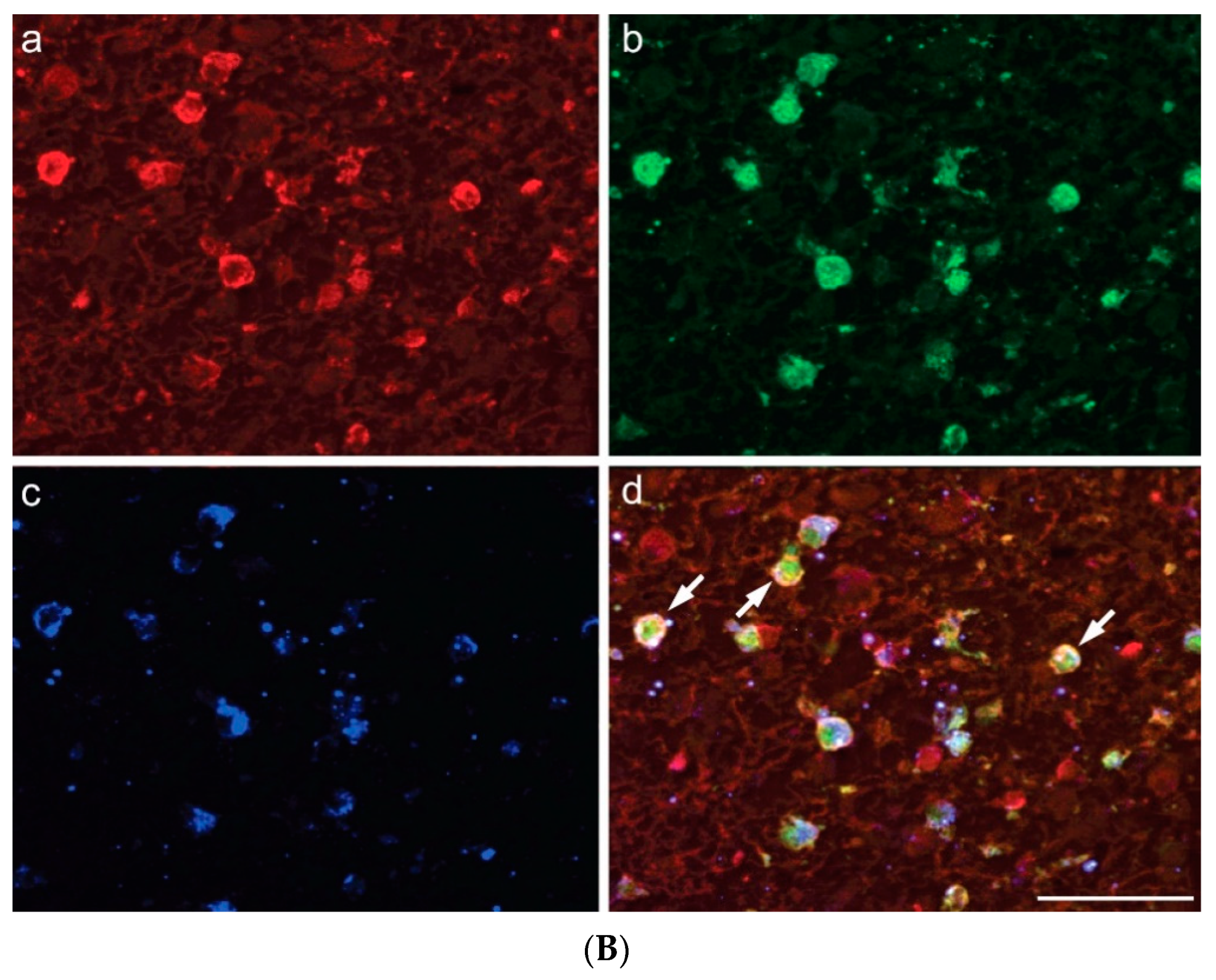
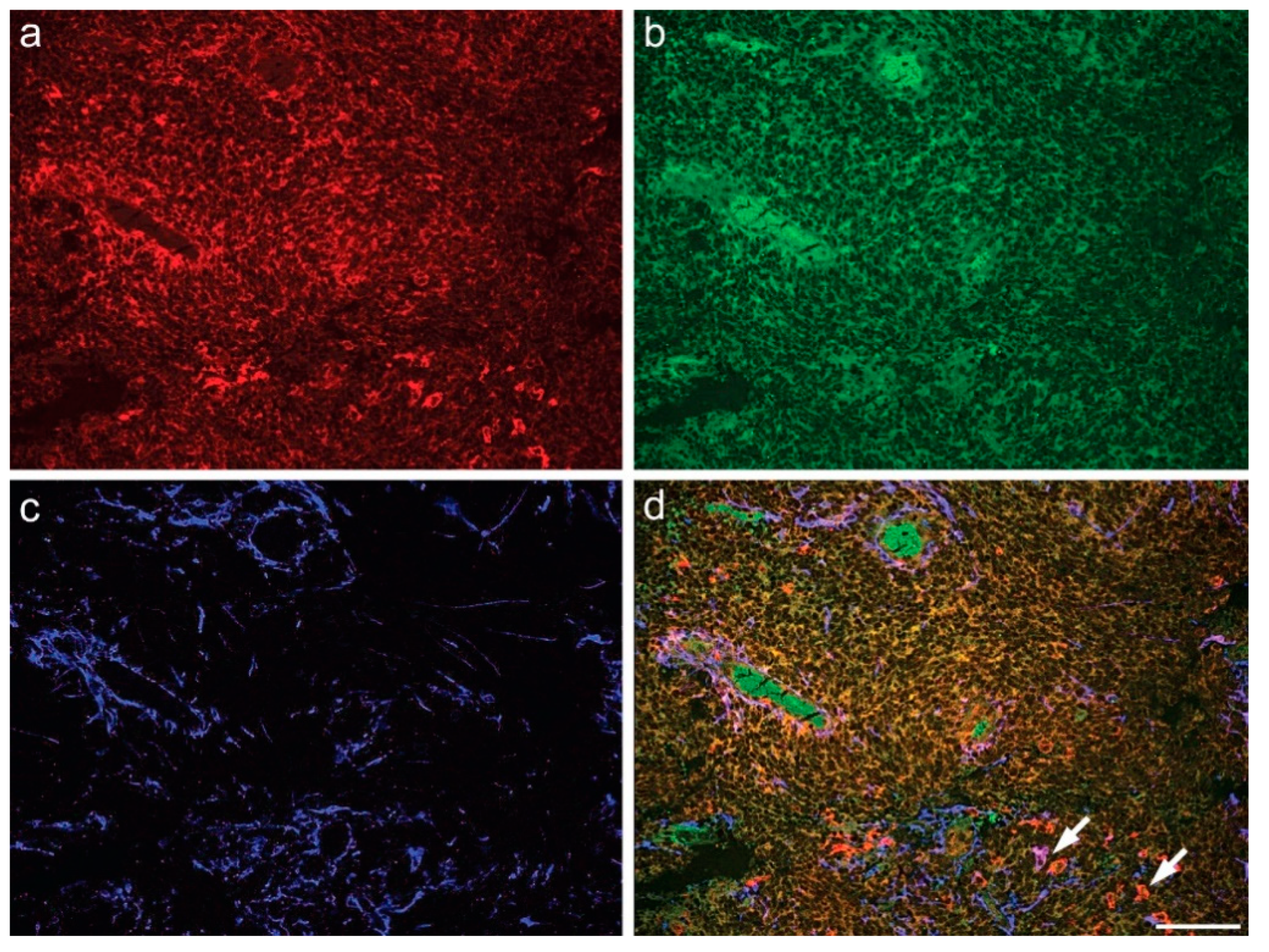
2.3. Multiple Fluorescence Labeling
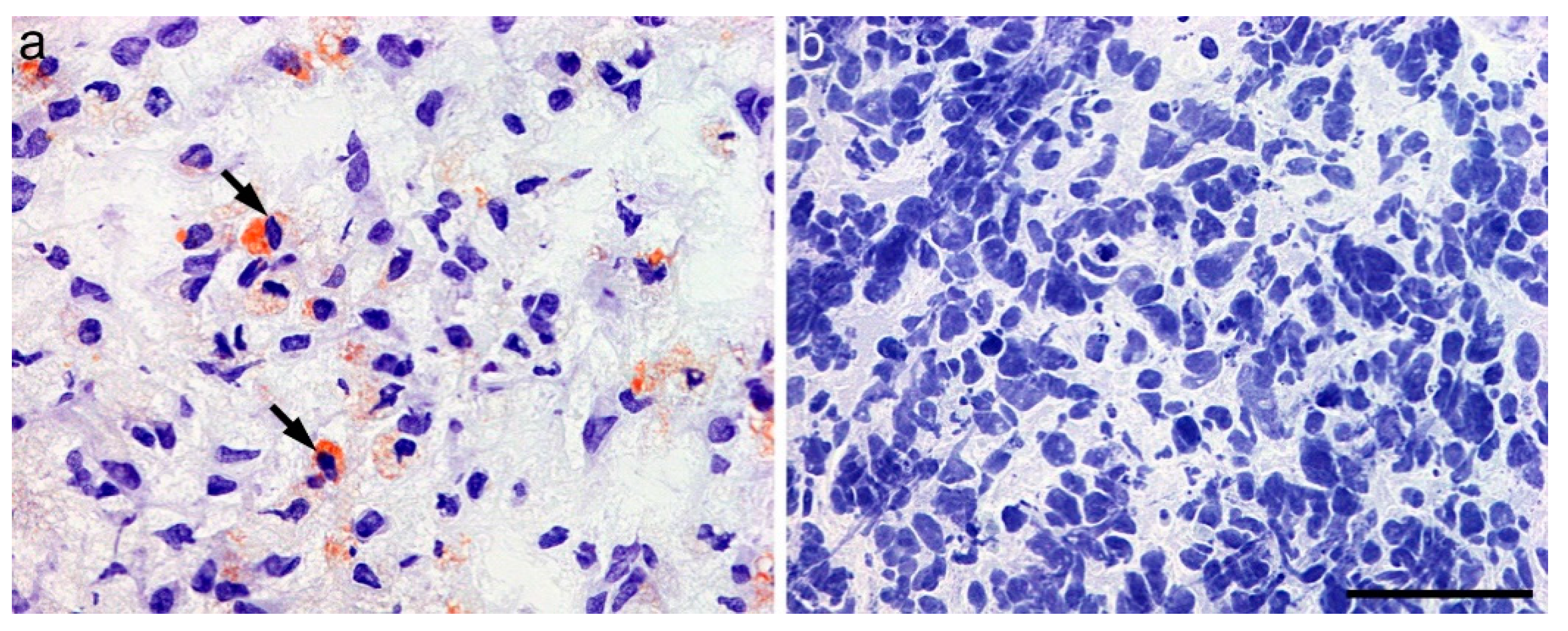
2.4. Oil Red O Staining
3. Discussion
4. Materials and Methods
4.1. Single Immunohistoperoxidase Staining
4.2. Oil Red O Staining
4.3. Immunofluorescence Labeling
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Snaebjornsson, M.T.; Janaki-Raman, S.; Schulze, A. Greasing the Wheels of the Cancer Machine: The Role of Lipid Metabolism in Cancer. Cell Metab. 2020, 31, 62–76. [Google Scholar] [CrossRef]
- Broadfield, L.A.; Pane, A.A.; Talebi, A.; Swinnen, J.V.; Fendt, S.M. Lipid metabolism in cancer: New perspectives and emerging mechanisms. Dev. Cell 2021, 56, 1363–1393. [Google Scholar] [CrossRef] [PubMed]
- Eckhardt, C.; Sbiera, I.; Krebs, M.; Sbiera, S.; Spahn, M.; Kneitz, B.; Joniau, S.; Fassnacht, M.; Kübler, H.; Weigand, I.; et al. High expression of Sterol-O-Acyl transferase 1 (SOAT1), an enzyme involved in cholesterol metabolism, is associated with earlier biochemical recurrence in high risk prostate cancer. Prostate Cancer Prostatic Dis. 2021, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Tardif, J.C.; Gregoire, J.; L’Allier, P.L.; Anderson, T.J.; Bertrand, O.; Reeves, F.; Title, L.M.; Alfonso, F.; Schampaert, E.; Hassan, A.; et al. Effects of the acyl coenzyme A:cholesterol acyltransferase inhibitor avasimibe on human atherosclerotic lesions. Circulation 2004, 110, 3372–3377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.J.; Oh, J.E.; Lee, S.H. Arctigenin shows preferential cytotoxicity to acidity-tolerant prostate carcinoma PC-3cells through ROS-mediated mitochondrial damage and the inhibition of PI3K/Akt/mTOR pathway. Biochem. Biophys. Res. Commun. 2018, 505, 1244–1250. [Google Scholar] [CrossRef] [PubMed]
- Geng, F.; Cheng, X.; Wu, X.; Yoo, J.Y.; Cheng, C.; Guo, J.Y.; Mo, X.; Ru, P.; Hurwitz, B.; Kim, S.-H.; et al. Inhibition of SOAT1 Suppresses Glioblastoma Growth via Blocking SREBP-1-Mediated Lipogenesis. Clin. Cancer Res. 2016, 22, 5337–5348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geng, F.; Guo, D. Lipid droplets, potential biomarker and metabolic target in glioblastoma. Intern. Med. Rev. 2017, 3. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.-Y.; Fu, W.-Q.; Zheng, X.-J.; Li, W.; Ren, L.-W.; Wang, J.-H.; Yang, C.; Du, G.-H. Avasimibe exerts anticancer effects on human glioblastoma cells via inducing cell apoptosis and cell cycle arrest. Acta Pharmacol. Sin. 2020, 42, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Bemlih, S.; Poirier, M.-D.; El Andaloussi, A. Acyl-coenzyme A: Cholesterol acyltransferase inhibitor Avasimibe affect survival and proliferation of glioma tumor cell lines. Cancer Biol. Ther. 2010, 9, 1025–1032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sbiera, S.; Leich, E.; Liebisch, G.; Sbiera, I.; Schirbel, A.; Wiemer, L. Mitotane Inhibits Sterol-O- Acyl Transferase 1 Triggering Lipid-Mediated Endoplasmic Reticulum Stress and Apoptosis in Adrenocortical Carcinoma Cells. Endocrinology 2015, 156, 3895–3908. [Google Scholar] [CrossRef] [Green Version]
- Maiter, D.; Bex, M.; Vroonen, L.; T’Sjoen, G.; Gil, T.; Banh, C.; Chadarevian, R. Efficacy and safety of mitotane in the treatment of adrenocortical carcinoma: A retrospective study in 34 Belgian patients. Ann. Endocrinol. 2016, 77, 578–585. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro-Oncology 2021, 23, 1231–1251. [Google Scholar] [CrossRef] [PubMed]
- Ohgaki, H.; Kleihues, P. Population-based studies on incidence, survival rates, and genetic alterations in astrocytic and oligodendroglial gliomas. J. Neuropathol. Exp. Neurol. 2005, 64, 479–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohgaki, H.; Kleihues, P. Epidemiology and etiology of gliomas. Acta Neuropathol. 2005, 109, 93–108. [Google Scholar] [CrossRef] [PubMed]
- Roggendorf, W.; Strupp, S.; Paulus, W. Distribution and characterization of microglia/macrophages in human brain tumors. Acta Neuropathol. 1996, 92, 288–293. [Google Scholar] [CrossRef]
- Johnson, B.E.; Mazor, T.; Hong, C.; Barnes, M.; Aihara, K.; McLean, C.Y. Mutational analysis reveals the origin and therapy-driven evolution of recurrent glioma. Science 2014, 343, 189–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, J.J.; Shih, H.A.; Andronesi, O.C.; Cahill, D.P. Isocitrate dehydrogenase-mutant glioma: Evolving clinical and therapeutic implications. Cancer 2017, 123, 4535–4546. [Google Scholar] [CrossRef] [PubMed]
- Maus, A.; Peters, G.J. Glutamate and alpha-ketoglutarate: Key players in glioma metabolism. Amino Acids 2017, 49, 21–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fack, F.; Tardito, S.; Hochart, G.; Oudin, A.; Zheng, L.; Fritah, S.; Golebiewska, A.; Nazarov, P.V.; Bernard, A.; Hau, A.-C.; et al. Altered metabolic landscape in IDH- mutant gliomas affects phospholipid, energy, and oxidative stress pathways. EMBO Mol. Med. 2017, 9, 1681–1695. [Google Scholar] [CrossRef]
- Pape, E.; Feliu, C.; Yéléhé-Okouma, M.; Colling, N.; Djerada, Z.; Gambier, N.; Weryha, G.; Scala-Bertola, J. High-Dose Mitotane-Induced Encephalopathy in the Treatment of Adrenocortical Carcinoma. Oncologist 2018, 23, 389–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reidy-Lagunes, D.L.; Lung, B.; Untch, B.R.; Raj, N.; Hrabovsky, A.; Kelly, C.; Gerst, S.; Katz, S.; Kampel, L.; Chou, J.; et al. Complete Responses to Mitotane in Metastatic Adrenocortical Carcinoma—A New Look at an Old Drug. Oncologist 2017, 22, 1102–1106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daffara, F.; De Francia, S.; Reimondo, G.; Zaggia, B.; Aroasio, E.; Porpiglia, F.; Volante, M.; Termine, A.; Di Carlo, F.; Dogliotti, L.; et al. Prospective evaluation of mitotane toxicity in adrenocortical cancer patients treated adjuvantly. Endocr.-Relat. Cancer 2008, 15, 1043–1053. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Age at Surgery | Gender | Diagnosis | WHO | MGMT-Status | IDH-Status |
|---|---|---|---|---|---|---|
| 1 | 79 | M | GBM | 4 | methylated | wt |
| 2 | 63 | M | GBM | 4 | unmethylated | wt |
| 3 | 72 | F | GBM | 4 | methylated | wt |
| 4 | 80 | M | GBM | 4 | unmethylated | wt |
| 5 | 67 | F | GBM | 4 | methylated | wt |
| 6 | 74 | F | GBM | 4 | methylated | wt |
| 7 | 68 | M | GBM | 4 | unmethylated | wt |
| 8 | 58 | M | GBM | 4 | methylated | wt |
| 9 | 77 | M | GBM | 4 | methylated | wt |
| 10 | 65 | F | GBM | 4 | methylated | wt |
| 11 | 71 | M | GBM | 4 | methylated | wt |
| 12 | 66 | F | GBM | 4 | unmethylated | wt |
| 13 | 78 | M | GBM | 4 | methylated | wt |
| 14 | 63 | M | GBM | 4 | methylated | wt |
| 15 | 57 | F | GBM | 4 | methylated | wt |
| 16 | 61 | F | GBM | 4 | methylated | wt |
| 17 | 69 | M | GBM | 4 | unmethylated | wt |
| 18 | 73 | M | GBM | 4 | methylated | wt |
| 19 | 56 | F | GBM | 4 | unmethylated | wt |
| 20 | 62 | F | GBM | 4 | methylated | wt |
| 21 | 54 | M | GBM | 4 | methylated | wt |
| 22 | 56 | M | GBM | 4 | unmethylated | wt |
| 23 | 81 | F | GBM | 4 | methylated | wt |
| 24 | 83 | F | GBM | 4 | unmethylated | wt |
| 25 | 72 | M | GBM | 4 | methylated | wt |
| 26 | 71 | M | GBM | 4 | methylated | wt |
| 27 | 59 | M | GBM | 4 | methylated | wt |
| 28 | 41 | F | HGA | 4 | methylated | mutant |
| 29 | 39 | M | HGA | 4 | methylated | mutant |
| 30 | 47 | M | HGA | 4 | methylated | mutant |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Löhr, M.; Härtig, W.; Schulze, A.; Kroiß, M.; Sbiera, S.; Lapa, C.; Mages, B.; Strobel, S.; Hundt, J.E.; Bohnert, S.; et al. SOAT1: A Suitable Target for Therapy in High-Grade Astrocytic Glioma? Int. J. Mol. Sci. 2022, 23, 3726. https://doi.org/10.3390/ijms23073726
Löhr M, Härtig W, Schulze A, Kroiß M, Sbiera S, Lapa C, Mages B, Strobel S, Hundt JE, Bohnert S, et al. SOAT1: A Suitable Target for Therapy in High-Grade Astrocytic Glioma? International Journal of Molecular Sciences. 2022; 23(7):3726. https://doi.org/10.3390/ijms23073726
Chicago/Turabian StyleLöhr, Mario, Wolfgang Härtig, Almut Schulze, Matthias Kroiß, Silviu Sbiera, Constantin Lapa, Bianca Mages, Sabrina Strobel, Jennifer Elisabeth Hundt, Simone Bohnert, and et al. 2022. "SOAT1: A Suitable Target for Therapy in High-Grade Astrocytic Glioma?" International Journal of Molecular Sciences 23, no. 7: 3726. https://doi.org/10.3390/ijms23073726
APA StyleLöhr, M., Härtig, W., Schulze, A., Kroiß, M., Sbiera, S., Lapa, C., Mages, B., Strobel, S., Hundt, J. E., Bohnert, S., Kircher, S., Janaki-Raman, S., & Monoranu, C.-M. (2022). SOAT1: A Suitable Target for Therapy in High-Grade Astrocytic Glioma? International Journal of Molecular Sciences, 23(7), 3726. https://doi.org/10.3390/ijms23073726