
Evaluation of Three-Dimensional Bioprinted Human Cartilage Powder Combined with Micronized Subcutaneous Adipose Tissues for the Repair of Osteochondral Defects in Beagle Dogs


 , ,
, ,
Abstract
:1. Introduction
2. Results
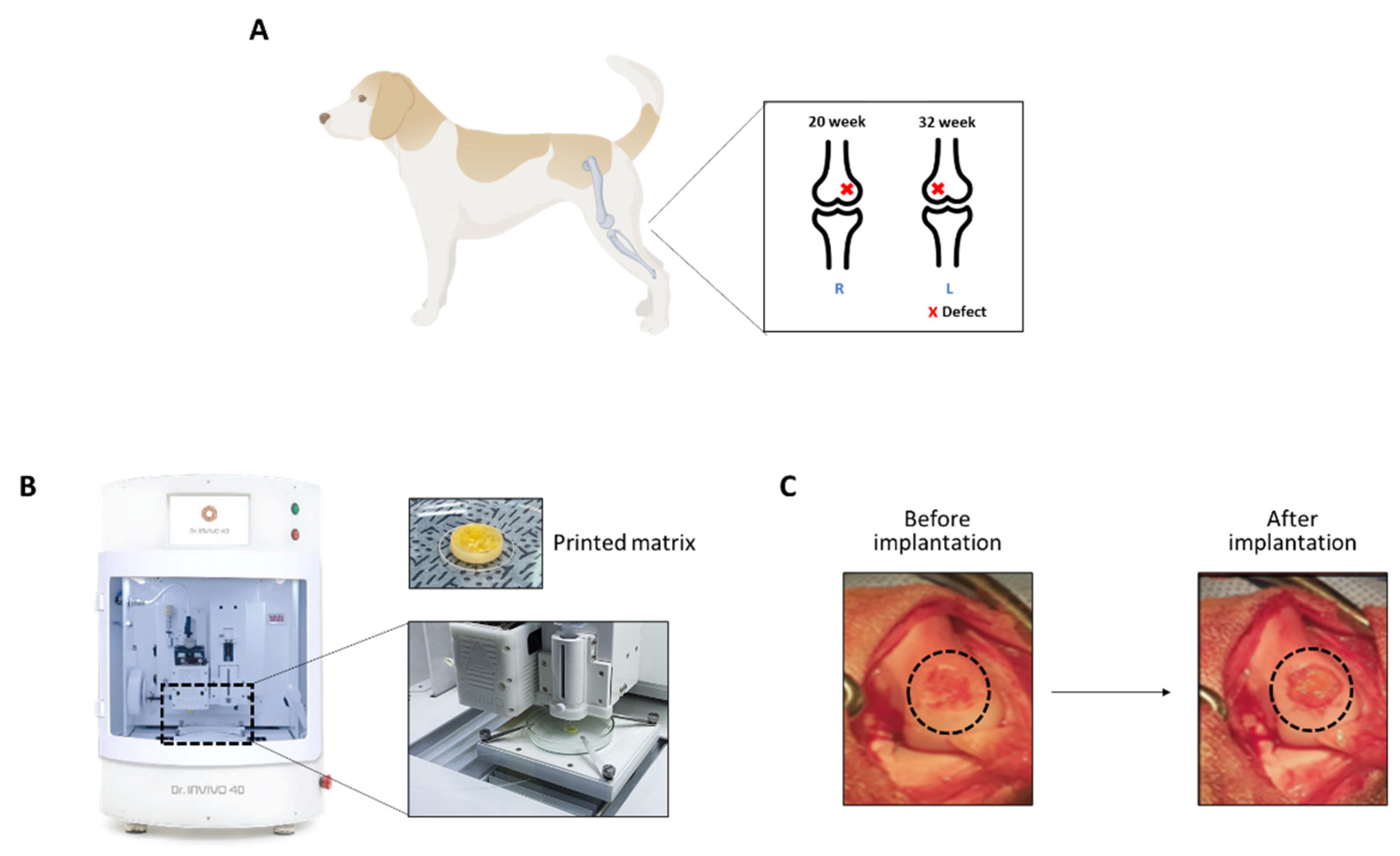
2.1. Generation of Osteochondral Defects and Matrix Implantation
- A defect control without any treatment,
- 2.
- LCCM (lyophilized costal-derived cartilage)
- 3.
- MA-ECM (Minimally manipulated Adipose tissue-Extracellular Matrix (MA-ECM)
- 4.
- LCCM/MA-ECM.
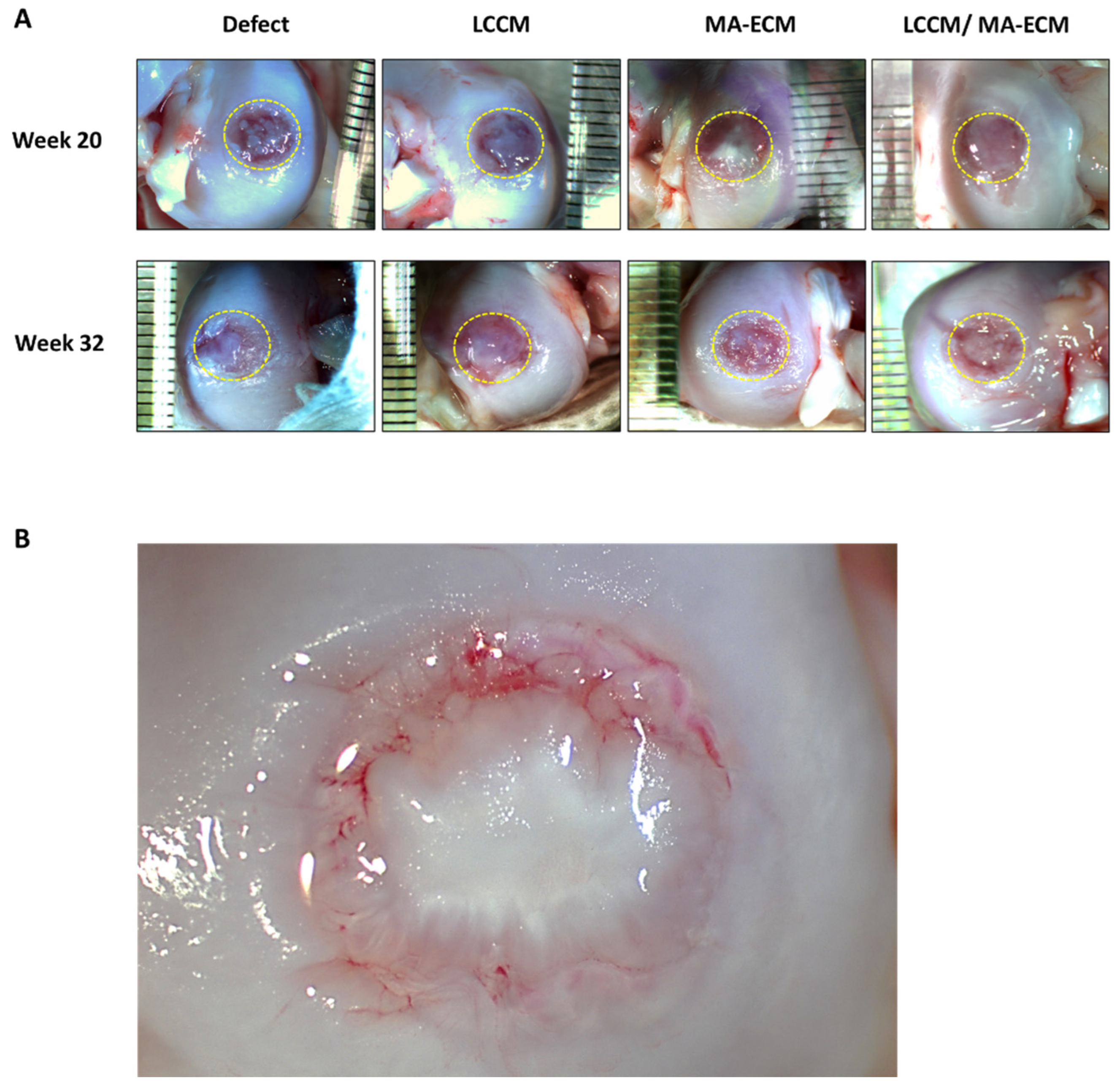
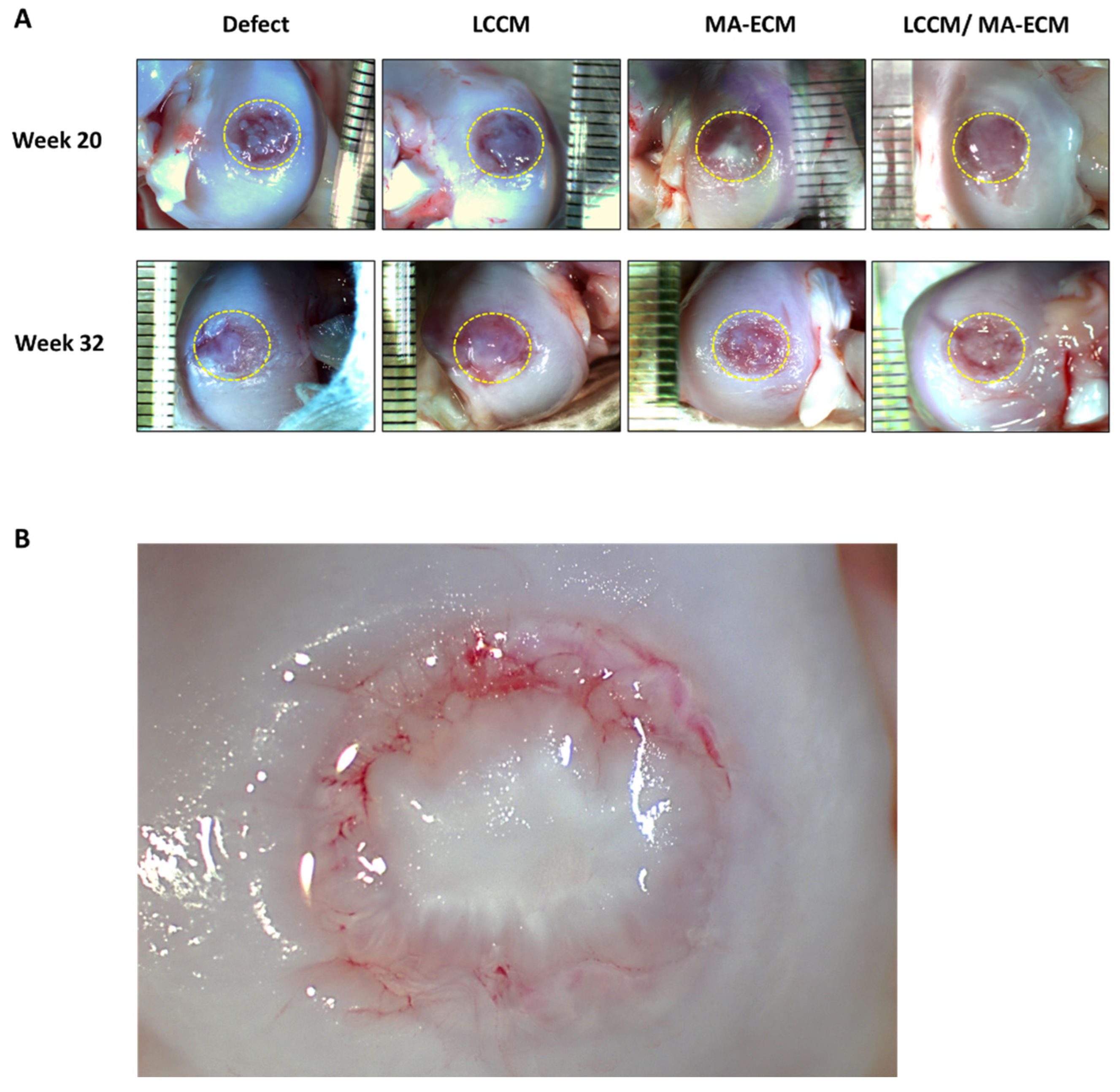
2.2. Gross Appearance of Chondral Defect Area in Each Group
2.3. Serum Level of Matrix Metalloproteinase-3 and -9 (MMP-3 and -9)
2.4. Mechanical Testing
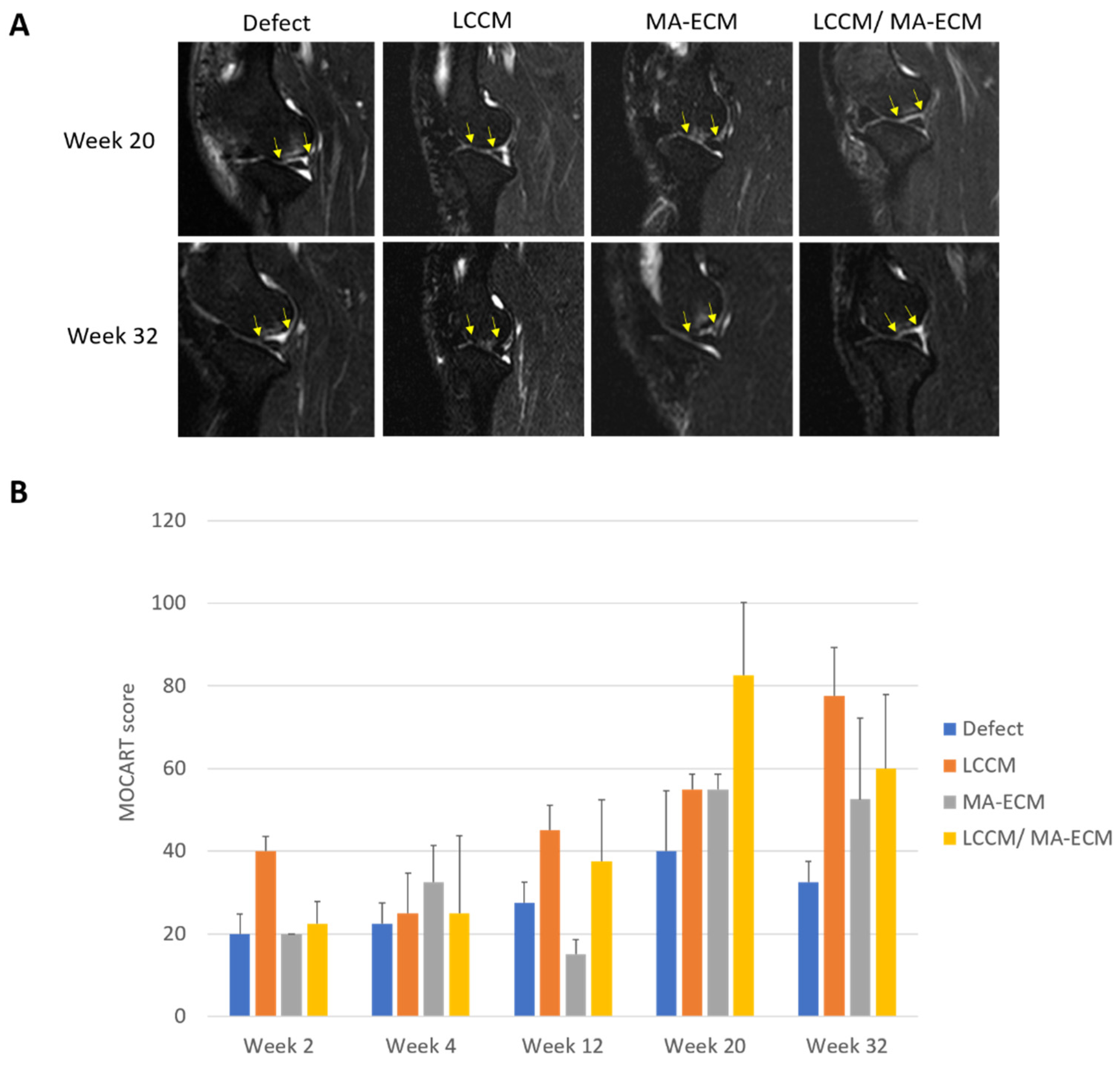
2.5. Magnetic Resonance Imaging (MRI) Analysis
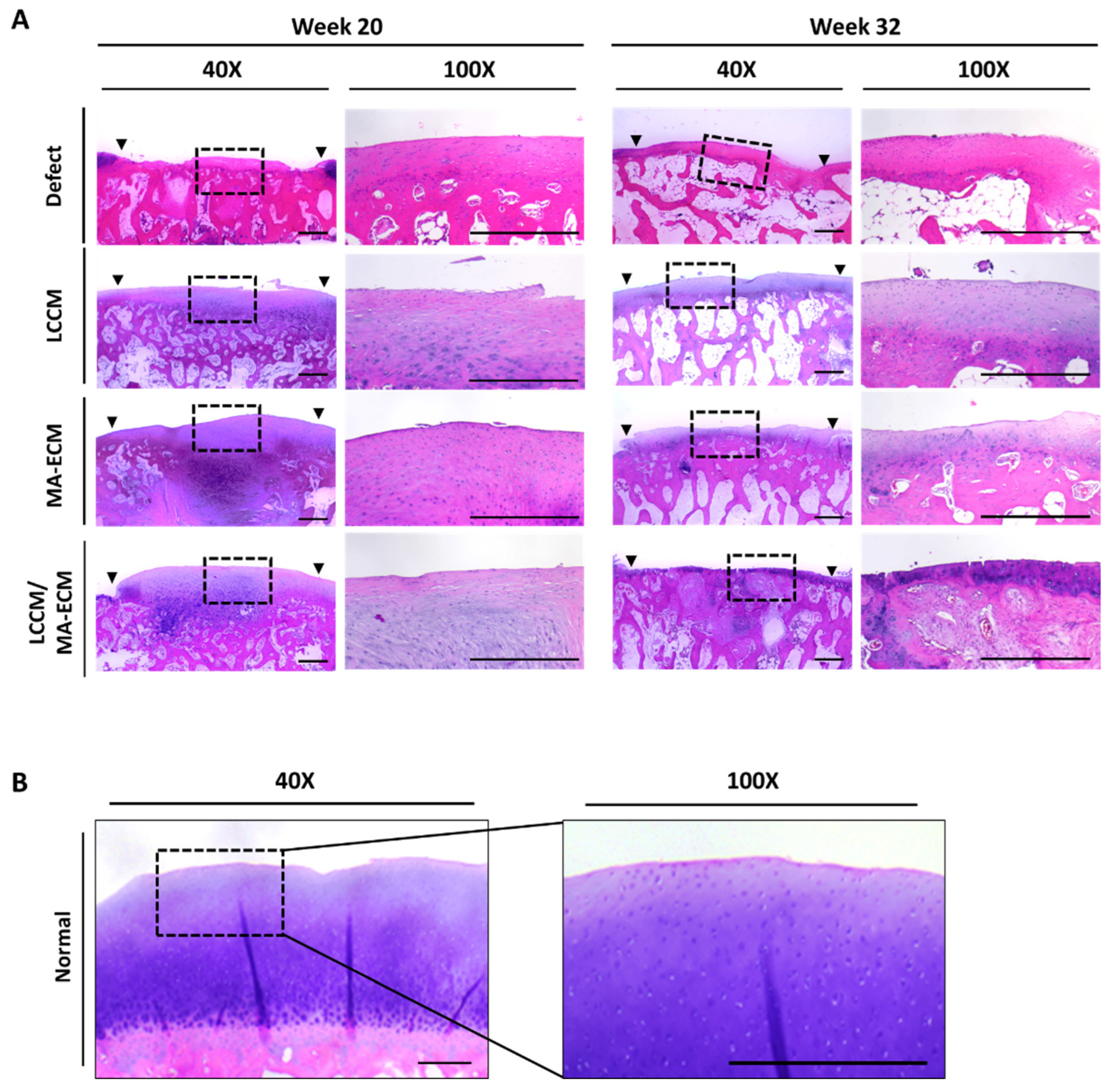
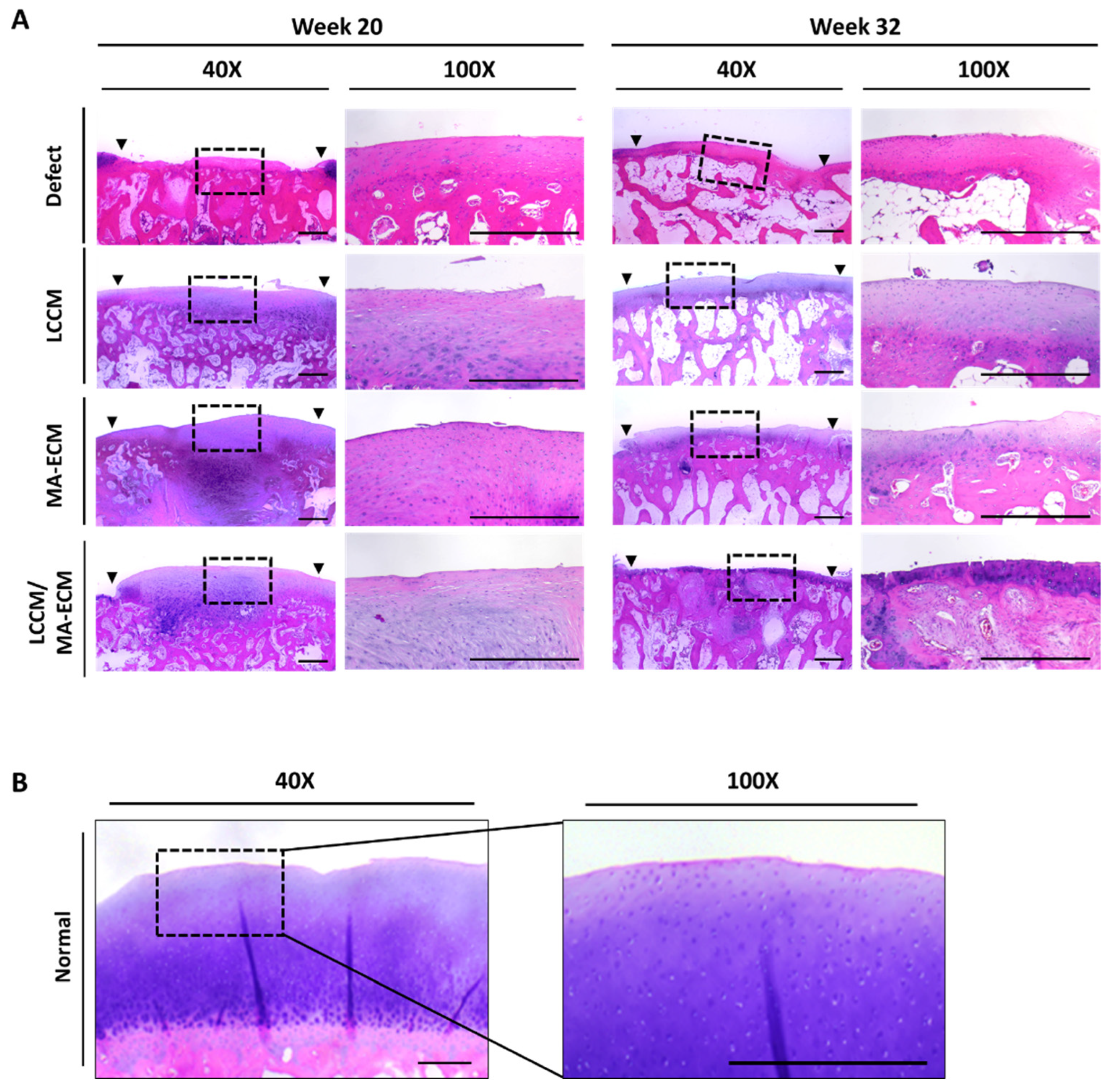
2.6. Microscopic Findings
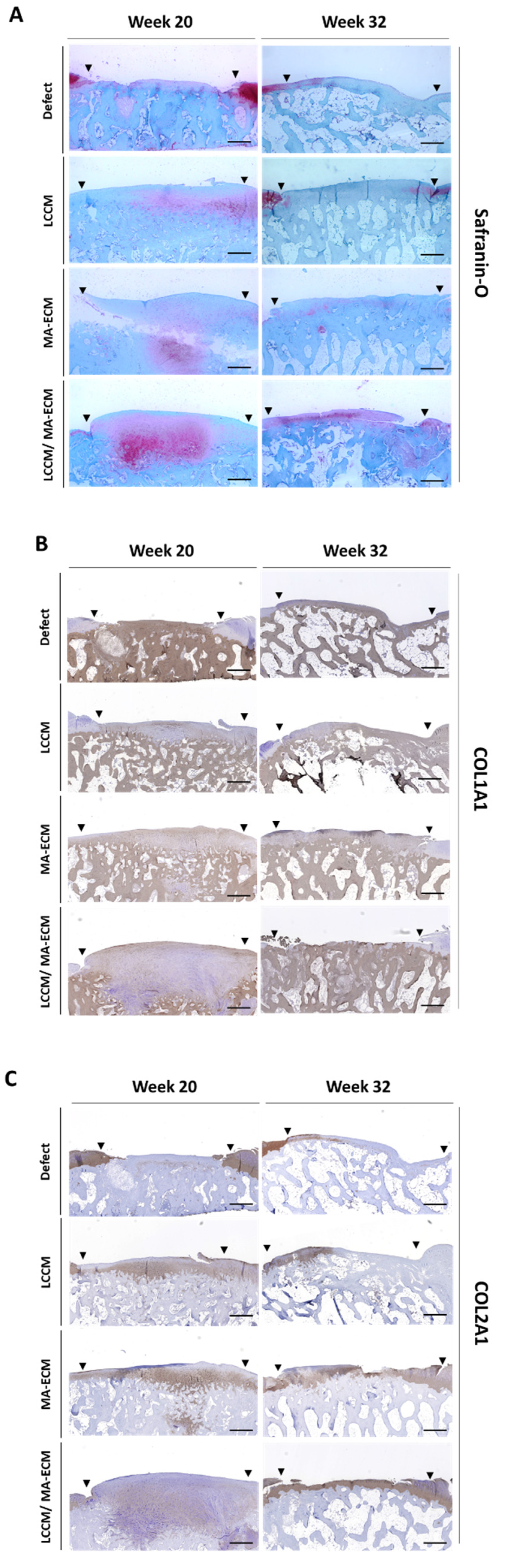
2.7. Safranin-O Staining and Immunohistochemistry (IHC)
3. Discussion
4. Materials and Methods
4.1. Animals and Study Design
4.2. Preparation of Experimental Surgery
4.3. Surgery Procedure
4.4. Preparation of Biomaterial Ink
4.4.1. MA-ECM (Minimally Manipulated Adipose Tissue-Extracellular Matrix)
4.4.2. Mixture of LCCM (Lyophilized Costal Cartilage Matrix) and MA-ECM
4.5. Three-Dimensional Printing Procedure
4.5.1. Fabrication of PCL Supports
4.5.2. Biomatrix Printing
4.6. Magnetic Resonance Imaging (MRI) Examination and MOCART Analysis
- Volume fill of cartilage defect
- Integration into adjacent cartilage
- Surface of the repair tissue
- Structure of repair tissue
- Signal intensity of the repair tissue
- Bony defect or bony overgrowth
4.7. Measurement of Compressive Strength
4.8. Histology and Immunohistochemistry (IHC) Analysis
- I.
- Surface. A smooth, continuous surface is an essential feature of the normal joint.
- II.
- Matrix. The unique combination of collagen and proteoglycans in hyaline cartilage provides the correct viscoelastic properties for the articular surface.
- III.
- Cell distribution. A columnar distribution of cells in the middle and lower zone of the cartilage layer indicates normal maturation, whereas disruption of this alignment indicates abnormal maturation.
- IV.
- Cell population viability. A viable cell population is essential for matrix turnover.
- V.
- Subchondral bone. The subchondral bone determines the geometry of the joint and therefore the pattern of its loading.
- VI.
- Mineralization. Mineralization within the cartilage layer is a pathological phenomenon and is indicative of functional impairment.
4.9. Enzyme-Linked Immunosorbent Assay (ELISA) Analysis of Metalloproteinase-3 and -9
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barbour, K.E.; Helmick, C.G.; Boring, M.; Brady, T.J. Prevalence of doctor-diagnosed arthritis and arthritis-attibutable activity limitation-United States, 2013–2015. MMWR Morb Mortal Wkly Rep. 2017, 66, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Hootman, J.M.; Helmick, C.G.; Barbour, K.E.; Theis, K.A.; Boring, M.A. Updated Projected Prevalence of Self-Reported Doctor-Diagnosed Arthritis and Arthritis-Attributable Activity Limitation Among US Adults, 2015–2040. Arthritis Rheumatol. 2016, 68, 1582–1587. [Google Scholar] [CrossRef]
- Bitton, R. The economic burden of osteoarthritis. Am. J. Manag. Care. 2009, 15, S230–S235. [Google Scholar]
- Murphy, L.B.; Cisternas, M.G.; Pasta, D.J.; Helmick, C.G.; Yelin, E.H. Medical Expenditures and Earnings Losses Among US Adults With Arthritis in 2013. Arthritis Care Res. 2018, 70, 869–876. [Google Scholar] [CrossRef] [PubMed]
- Boeuf, S.; Richter, W. Chondrogenesis of mesenchymal stem cells: Role of tissue source and inducing factors. Stem Cell Res. Ther. 2010, 1, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Setayeshmehr, M.; Esfandiari, E.; Hashemibeni, B.; Tavakoli, A.H.; Rafienia, M.; Samadikuchaksaraei, A.; Moroni, L.; Joghataei, M.T. Chondrogenesis of human adipose-derived mesenchymal stromal cells on the [devitalized costal cartilage matrix/poly(vinyl alcohol)/fibrin] hybrid scaffolds. Eur Polym, J. 2019, 118, 528–541. [Google Scholar] [CrossRef]
- Hosseinkhani, M.; Mehrabani, D.; Karimfar, M.H.; Bakhtiyari, S.; Manafi, A.; Shirazi, R. Tissue Engineered Scaffolds in Regenerative Medicine. World J. Plast Surg. 2014, 3, 3–7. [Google Scholar]
- Cui, H.; Nowicki, M.; Fisher, J.P.; Zhang, L.G. 3D Bioprinting for Organ Regeneration. Adv. Healthc. Mater. 2017, 6, 1601118. [Google Scholar] [CrossRef] [Green Version]
- Nicolas, J.; Magli, S.; Rabbachin, L.; Sampaolesi, S.; Nicotra, F.; Russo, L. 3D extracellular matrix mimics: Fundamental concepts and role of materials chemistry to influence stem cell fate. Biomacromolecules 2020, 21, 1968–1994. [Google Scholar] [CrossRef]
- Ma, S.K.Y.; Chan, A.S.F.; Rubab, A.; Chan, W.C.W.; Chan, D. Extracellular matrix and cellular plasticity in musculoskeletal development. Front. Cell Dev. Biol. 2020, 8, 781. [Google Scholar] [CrossRef]
- Park, S.-Y.; An, J.-H.; Kwon, H.; Choi, S.-Y.; Lim, K.-Y.; Kwak, H.-H.; Hussein, K.H.; Woo, H.-M.; Park, K.-M. Custom-made artificial eyes using 3D printing for dogs: A preliminary study. PLoS ONE 2020, 15, e0242274. [Google Scholar] [CrossRef] [PubMed]
- Schöneberg, J.; De Lorenzi, F.; Theek, B.; Blaeser, A.; Rommel, D.; Kuehne, A.J.C.; Kießling, F.; Fischer, H. Engineering biofunctional in vitro vessel models using a multilayer bioprinting technique. Sci. Rep. 2018, 8, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pati, F.; Ha, D.-H.; Jang, J.; Han, H.H.; Rhie, J.-W.; Cho, D.-W. Biomimetic 3D tissue printing for soft tissue regeneration. Biomaterials 2015, 62, 164–175. [Google Scholar] [CrossRef]
- Zeng, G.; Chen, A.; Li, W.; Song, J.; Gao, C. High MMP-1, MMP-2, and MMP-9 protein levels in osteoarthritis. Genet. Mol. Res. 2015, 14, 14811–14822. [Google Scholar] [CrossRef]
- Pengas, I.; Eldridge, S.; Assiotis, A.; McNicholas, M.; Espregueira-Mendes, J.; Laver, L. MMP-3 in the peripheral serum as a biomarker of knee osteoarthritis, 40 years after open total knee meniscectomy. J. Exp. Orthop. 2018, 5, 21. [Google Scholar] [CrossRef] [PubMed]
- Leong, D.J.; Gu, X.I.; Li, Y.; Lee, J.Y.; Laudier, D.M.; Majeska, R.J.; Schaffler, M.B.; Cardoso, L.; Sun, H.B. Matrix metalloproteinase-3 in articular cartilage is upregulated by joint immobilization and suppressed by passive joint motion. Matrix Biol. 2010, 29, 420–426. [Google Scholar] [CrossRef] [Green Version]
- Jungmann, P.M.; Welsch, G.; Brittberg, M.; Trattnig, S.; Braun, S.; Imhoff, A.B.; Salzmann, G.M. Magnetic Resonance Imaging Score and Classification System (AMADEUS) for Assessment of Preoperative Cartilage Defect Severity. Cartilage. 2016, 8, 272–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schreiner, M.M.; Raudner, M.; Marlovits, S.; Bohndorf, K.; Weber, M.; Zalaudek, M.; Röhrich, S.; Szomolanyi, P.; Filardo, G.; Windhager, R.; et al. The MOCART (Magnetic Resonance Observation of Cartilage Re-pair Tissue) 2.0 Knee Score and Atlas. Cartilage 2021, 13, 571S–587S. [Google Scholar] [CrossRef] [Green Version]
- Brittberg, M.; Peterson, L. Introduction of an articular cartilage classification. ICRS Newsletter. 1998, 1, 5–8. [Google Scholar]
- Hoemann, C.D.; Kandel, R.; Roberts, S.; Saris, D.B.; Creemers, L.; Mainil-Varlet, P.; Méthot, S.; Hollander, A.P.; Buschmann, M. International Cartilage Repair Society (ICRS) Recommended Guidelines for Histological Endpoints for Cartilage Repair Studies in Animal Models and Clinical Trials. Cartilage. 2011, 2, 153–172. [Google Scholar] [CrossRef] [Green Version]
- Beketov, E.E.; Isaeva, E.V.; Yakovleva, N.D.; Demyashkin, G.A.; Arguchinskaya, N.V.; Kisel, A.A.; Lagoda, T.S.; Malakhov, E.P.; Kharlov, V.I.; Osidak, E.O.; et al. Bioprinting of Cartilage with Bioink Based on High-Concentration Collagen and Chondrocytes. Int. J. Mol. Sci. 2021, 22, 11351. [Google Scholar] [CrossRef] [PubMed]
- Mancini, I.A.D.; Schmidt, S.; Brommer, H.; Pouran, B.; Schäfer, S.; Tessmar, J.; Mensinga, A.; van Rijen, M.H.P.; Groll, J.; Blunk, T.; et al. A composite hydrogel-3D printed thermoplast osteochondral anchor as example for a zonal approach to cartilage repair: In vivo performance in a long-term equine model. Biofabrication. 2020, 12, 03502. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, D.; Hägg, D.A.; Forsman, A.; Ekholm, J.; Nimkingratana, P.; Brantsing, C.; Kalogeropoulos, T.; Zaunz, S.; Concaro, S.; Brittberg, M.; et al. Cartilage Tissue Engineering by the 3D Bioprinting of iPS Cells in a Nanocellulose/Alginate Bioink. Sci. Rep. 2017, 7, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kerin, A.J.; Wisnom, M.R.; Adams, M. The compressive strength of articular cartilage. Proc. Inst. Mech. Eng. Part. H J. Eng. Med. 1998, 212, 273–280. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Feature(s) | Defect | LCCM | MA-ECM | LCCM/MA-ECM |
|---|---|---|---|---|---|
| Week 20 | Surface (0–3) | 0 | 3 | 3 | 3 |
| Matrix (0–3) | 2 | 2 | 1 | 1 | |
| Cell distribution (0–3) | 1 | 1 | 2 | 2 | |
| Cell viability (0–3) | 3 | 1 | 3 | 3 | |
| Subchondral bone (0–3) | 2 | 2 | 2 | 2 | |
| Cartilage mineralization (0–3) | 3 | 3 | 3 | 3 | |
| Total score(s) | 11 | 12 | 14 | 14 | |
| Week 32 | Surface (0–3) | 0 | 3 | 3 | 3 |
| Matrix (0–3) | 2 | 2 | 2 | 3 | |
| Cell distribution (0–3) | 0 | 2 | 2 | 2 | |
| Cell viability (0–3) | 3 | 3 | 3 | 3 | |
| Subchondral bone (0–3) | 2 | 2 | 2 | 2 | |
| Cartilage mineralization (0–3) | 3 | 3 | 3 | 3 | |
| Total score(s) | 10 | 15 | 15 | 16 |
| Group(s) | LCCM | MA-ECM | Study Duration | Number of Animals | |
|---|---|---|---|---|---|
| Control | − | − | (Right knee) FU week 20 | (Left knee) FU week 32 | 3 |
| Exp 1. | + | − | 3 | ||
| Exp 2. | − | + | 3 | ||
| Exp 3. | + | + | 3 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ryu, J.; Brittberg, M.; Nam, B.; Chae, J.; Kim, M.; Colon Iban, Y.; Magneli, M.; Takahashi, E.; Khurana, B.; Bragdon, C.R. Evaluation of Three-Dimensional Bioprinted Human Cartilage Powder Combined with Micronized Subcutaneous Adipose Tissues for the Repair of Osteochondral Defects in Beagle Dogs. Int. J. Mol. Sci. 2022, 23, 2743. https://doi.org/10.3390/ijms23052743
Ryu J, Brittberg M, Nam B, Chae J, Kim M, Colon Iban Y, Magneli M, Takahashi E, Khurana B, Bragdon CR. Evaluation of Three-Dimensional Bioprinted Human Cartilage Powder Combined with Micronized Subcutaneous Adipose Tissues for the Repair of Osteochondral Defects in Beagle Dogs. International Journal of Molecular Sciences. 2022; 23(5):2743. https://doi.org/10.3390/ijms23052743
Chicago/Turabian StyleRyu, Jina, Mats Brittberg, Bomi Nam, Jinyeong Chae, Minju Kim, Yhan Colon Iban, Martin Magneli, Eiji Takahashi, Bharti Khurana, and Charles R. Bragdon. 2022. "Evaluation of Three-Dimensional Bioprinted Human Cartilage Powder Combined with Micronized Subcutaneous Adipose Tissues for the Repair of Osteochondral Defects in Beagle Dogs" International Journal of Molecular Sciences 23, no. 5: 2743. https://doi.org/10.3390/ijms23052743
APA StyleRyu, J., Brittberg, M., Nam, B., Chae, J., Kim, M., Colon Iban, Y., Magneli, M., Takahashi, E., Khurana, B., & Bragdon, C. R. (2022). Evaluation of Three-Dimensional Bioprinted Human Cartilage Powder Combined with Micronized Subcutaneous Adipose Tissues for the Repair of Osteochondral Defects in Beagle Dogs. International Journal of Molecular Sciences, 23(5), 2743. https://doi.org/10.3390/ijms23052743