Abstract
The five-year survival rate of lung cancer patients is very low, mainly because most newly diagnosed patients present with locally advanced or metastatic disease. Therefore, early diagnosis is key to the successful treatment and management of lung cancer. Unfortunately, early detection methods of lung cancer are not ideal. In this brief review, we described early detection methods such as chest X-rays followed by bronchoscopy, sputum analysis followed by cytological analysis, and low-dose computed tomography (LDCT). In addition, we discussed the potential of metabolomic fingerprinting, compared to that of other biomarkers, including molecular targets, as a low-cost, high-throughput blood-based test that is both feasible and affordable for early-stage lung cancer screening of at-risk populations. Accordingly, we proposed a paradigm shift to metabolomics as an alternative to molecular and proteomic-based markers in lung cancer screening, which will enable blood-based routine testing and be accessible to those patients at the highest risk for lung cancer.
1. Introduction
Cancer is a leading cause of death worldwide, accounting for nearly 10 million deaths in 2020 [1]. Among the most common global cancer-related death in 2020, lung cancer accounted for 1.8 million deaths. In addition, there were 2.21 million new cases of lung cancer around the world [1]. According to the World Cancer Research Fund, lung cancer is the most common cancer in men and the third most common cancer in women [2]. Although the American Cancer Society recommends that those over 40 years undergo yearly cancer check-ups, this recommendation is usually not followed. Consequently, survival tends to be poorer, when patients show cancer symptoms at a later stage of development [3].
The early diagnosis of lung cancer is key to a successful treatment regimen and improved prognosis; however, current early detection methods for lung cancer are not adequate. Furthermore, some of these technologies used in those methods are invasive, cause discomfort and pain to the patients and may present a greater risk of complications. Personalized disease risk based on genomic information has assisted therapeutic decisions. However, genomics remains relatively limited in predicting disease onset, mainly because genomic information does not account for the dynamic environmental influences (phenotype). Thus, to better understand lung cancer, the examination of downstream changes occurring at the level of the protein and metabolites might provide helpful information about the disease. Although there are a number of recent reviews on the topic of metabolomics in human health and disease [4,5,6,7,8,9,10,11,12,13], there is a paucity of information regarding the utility of metabolomics as a robust cancer diagnostic platform. Accordingly, the purpose of this brief review was to chart a general cancer diagnostic landscape and various approaches in the diagnosis of lung cancer, but with a major focus on the use of liquid biopsy. We also highlighted the role of metabolomics and how it has been underutilized as a tool in cancer diagnostics, particularly for the detection of early-stage lung cancer. We, therefore, searched PubMed for primary research articles regarding the potential of clinical applications of metabolomics. Specifically, the search strategy used the following search terms for relevant articles over the last 10 years: biomarkers, metabolomics, lung cancer, early-stage lung cancer, and liquid Biopsy.
2. Challenges and Importance of Better Screening Approaches for Early-Stage Lung Cancer
The two main types of lung cancer are small-cell lung carcinoma (SCLC) and non-small-cell lung carcinoma (NSCLC), with NSCLC accounting for 85–90% of observed cancers [14,15]. The vast majority (85–90%) of lung cancer cases are due to long-term tobacco use, while 10–15% of cases occur in people who have never smoked [16]. Non-smokers typically develop lung cancer through exposure to radon gas, asbestos, second-hand smoke, air pollution, toxic metals, soot, sawdust, and/or coal dust [17,18,19,20]. The typical age at diagnosis is 70, with slightly more men diagnosed than women [21]. The five-year survival rate of lung cancer patients is approximately 21%, mainly because most newly diagnosed patients present with advanced or metastatic disease.
Lung cancer is histologically categorized into adenocarcinoma, large-cell carcinoma, and squamous cell carcinoma. The stages of lung cancer are based on the staging system established by the American Joint Committee of Cancer (AJCC). The staging system is acronymized as TNM, where T stands for the size of the primary tumor, N stands for the spread of the tumor to lymph nodes, and M stands for metastasis. Despite decades of research and the introduction of many advanced therapeutics, survival rates for lung cancer have remained essentially unchanged [22]. However, when lung cancer is detected at stage I (T < 5 cm, no spread to lymph nodes, no metastasis), the 10-year survival rate increases to 88%, and if the tumor is resected within one month of detection, the survival rate is 92% [23]. The five-year survival rates for NSCLC have been reported to range from 14% to 49% for stage I to stage IIIa lung cancer and <5% for stages IIIb/IV (Table 1), but with the advancement of treatment regimens, some improvements have been observed [24].

Table 1.
TNM of malignant tumor classification.
Although advances in multimodality therapeutics for lung cancer have been made, the overall five-year survival rate among newly diagnosed lung cancer patients at a late stage remains in the range of 15–17% [26,27]. Although surgical resection is the treatment of choice for early-stage NSCLC, if lung cancer is detected at an early stage, the 5-year survival is reported to range from 36% to 70% [28,29,30]. On the other hand, multimodality treatment with adjuvant chemotherapy has improved survival rates by only 5% [28,30]. It should be noted that until the last decade, the five-year overall survival rate for patients with metastatic NSCLC was <5%; however, with an improved understanding of the pathophysiology of lung cancer, the overall survival rate has improved to 25% to 40% [31]. Since 90% of lung cancer cases are detected among smokers and former smokers, this high-risk population group would benefit from a screening test with the goal of detecting lung cancer while it is in stage I [32] or earlier.
These data strongly support the contention that early diagnosis is fundamental to the successful treatment of lung cancer. Unfortunately, current early detection methods of lung cancer are not ideal. These methods include chest X-rays, bronchoscopy, sputum analysis followed by cytological analysis, and low-dose computed tomography (LDCT). Although radiation exposure during chest X-rays may be problematic, a major reason for not using X-rays may be attributed to the poor performance of the test concerning sensitivity and specificity. Accordingly, as of 2016, the Canadian Task Force on Preventative Health Care (CTFPHC) has recommended against using chest X-rays for lung cancer screening [33]. Some of the issues with bronchoscopies are that they are invasive, not readily available and associated with potential complications. In addition, false-negative bronchoscopic results are commonly experienced, and the diagnostic accuracy of this technique is sub-optimal, with sensitivities ranging between 34% and 88%, particularly for the diagnosis of peripheral malignant lesions [34]. Indeed, these sensitivities depend on the size and the localization of the primary tumor and the number of parallel tests performed per bronchoscopy [35,36,37].
The diagnosis of lung cancer using standard cytological sputum analysis can be tedious, prone to unsatisfactory sample collection and often exhibits poor sensitivity [38]. To achieve a diagnosis, indeterminate sputum results may necessitate repeated sputum collection or escalation to more costly and invasive testing methods. LDCT, while more sensitive than chest X-rays, is expensive, exposes patients to a higher radiation dose than chest X-rays, is not routinely accessible to many patients and has a 96% rate of false positives (with a 4 mm non-calcified nodule size cut-off) [39]. In an assessment conducted by the National Lung Screening Trial in the USA, the over-diagnosis rate of lung cancer by LDCT was estimated to be 18.5% [40]. LDCT screening can thus lead to invasive interventions (needle biopsy and/or surgery) [41] for many patients with benign lesions, leading to patient morbidity and high health care costs. Additionally, cumulative radiation exposure from repeated scans may increase the risk of developing cancers [42]. Indeed, a widespread issue with LDCT lung cancer screening is the potential harm attributed to exposure to ionizing radiation as well as in cases during the work-up of suspicious lesions discovered at LDCT [43]. However, in the Continuous Observation of Smoking Subject (COSMOS) lung cancer study, it was found that one radiation-induced major cancer would be expected for every 108 (259/2.4) lung cancers detected through screening. It was concluded that radiation exposure and cancer risk associated with lung cancer LDCT screening are not insignificant but acceptable due to a highly significant reduction in mortality achieved with screening [44]. Nevertheless, a 20% reduction in lung cancer mortality has been reported using intensive LDCT screening of heavy smokers [45].
It should be mentioned that the Nederland’s Leuvens Longkanker Screenings Onderzoek (NELSON) trial was conducted based on a volumetry-based screening strategy [46]. Of the lung cancers diagnosed, around 71% were diagnosed at stage I and approximately 8% at stages IIIb–IV, and 51.2% were adenocarcinomas, thus demonstrating that, unlike other comparable trials, the NELSON trial screen-detected lung cancers are more often diagnosed at stage I and less frequently at stages IIIb–IV. However, it was suggested that the screening strategy of the NELSON trial results in a favorable diagnosis [46] with a reduction in mortality from lung cancer [47]. Still, the complete consensus for a systematic lung cancer screening is yet to be attained [47].
3. Molecular Approaches and Directions in Lung Cancer Detection
Given the limitations detailed above, it is clear that better, less expensive, less invasive, and broader screening approaches to early lung cancer detection are urgently needed. To address this need, many researchers have looked to the development of non-invasive or mildly invasive molecular tests using breath [48], urine [49], sputum [50], breath condensate [51], or blood-based assays [52]. The molecular markers being used include proteins [53,54], tumor-associated autoantibodies [55], circulating DNA [56], circulating tumor cells [57], microRNA [58], methylated DNA [59], and metabolites [60]. Many of these reports tend to focus on diagnosing late-stage lung cancer as opposed to early-stage lung cancer. Among those focused on early-stage lung cancer, some of the better molecular tests reported the area under the receiver operating characteristic (AUROCs) curves of 0.84 [61,62] to 0.90 [63]. To date, very few molecular tests have been validated on larger populations. Only one molecular blood test for early-stage lung cancer has reached the market; unfortunately, this test only shows a 37% sensitivity and a 90% specificity [64,65]. However, it should be noted that a randomized ongoing clinical trial led by Oncimmune and Lung Cancer Scotland (ECLS) was designed to confirm these findings [66]. Dama et al. [67] have recently reviewed some of the current technologies used in the early detection of lung cancer. Overall, liquid biopsy has shown some clinical applicability as a tool for the early detection of lung cancer, and its use as a screening/diagnostic/prognostic test for cancer detection remains to be fully validated for implementation in clinical practice [68].
4. The Interrelationship between Genes, Proteins, and Metabolites
There are a number of factors that can influence the metabolome of an individual, including age, sex, diet, geographical location, environment, ethnicity, time of day, and even the individual’s endogenous genetic make-up [69,70]. Metabolites and genes are intimately connected [71]. In this regard, it has been suggested that a single DNA base change in a given gene can lead to 10,000-fold endogenous metabolite shift levels [72]. This substantial increase in metabolite concentration is attributed to the fact that metabolites are the downstream products and interactions of multiple intracellular elements, including genes, transcriptional activators, RNA transcripts, protein transporters, and enzymes [73].
This amplification of the metabolomic signal, depicted in Figure 1 (adapted from [72]), involves the transmission of the message from DNA to proteins to metabolites. In other words, it can also be described in terms of the number of genes (20,000) versus the number of (expected) metabolites (~1 million) and the diversity of chemicals used to assemble genes (4 nucleotides) or proteins (20 amino acids) versus the variety of chemicals seen in the metabolome (3000 chemical classes) [72]. The organs of the body produce or utilize specific metabolites that can serve as metabolomic fingerprints in health and different pathophysiological conditions [72]. Thus, metabolomic fingerprinting provides a unique opportunity for the use of metabolites as a panel of biomarkers of different diseases, including cancer, which can exhibit highly specific metabolic signatures that have both diagnostic and prognostic value.
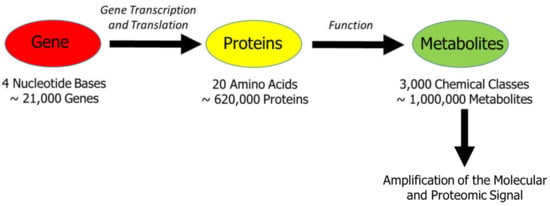
Figure 1.
The interrelationship between genes, proteins, and metabolites. This scheme illustrates the amplification of the metabolomic signal, which involves the initial message transfer from DNA to functional proteins and then organ-specific metabolites. Adapted from Wishart, DS [72].
5. Metabolic Fingerprints
It has been known for a long time that cancer can be regarded as a metabolic disease [74]. Since metabolism reflects the biochemical state of a healthy or unhealthy cell, then the unique metabolic characteristics (fingerprints) may assist in the determination of the stage and location of a carcinoma in a non-invasive manner and allow for the distinction between metabolic processes in healthy cells as well as cancer cells [74]. Such metabolic disorder helps to support high proliferative rates despite poor vascularization that limits oxygen and nutrient supply [75,76]. Accordingly, the field of cancer metabolomics is primarily based on the fact that metabolic activities are altered in cancer cells relative to normal cells that represent a characteristic metabolic profile that sustains malignancy and is thus considered a hallmark of cancer [77,78]. In cancer cells, biochemical pathways are disturbed due to the disruption of gene regulation and genetic polymorphisms, unusual chromosome repetitions, and mutations [78,79]. These disruptions may occur within the pathway itself or from downstream effects caused by dysfunctional proteins in adjacent pathways. Dysfunctional proteins in pathways are often related to cancers and can cause an imbalance in metabolite concentrations that are different from healthy cells [72,74]. It is thus conceivable that each other type of cancer may be caused by different mutations (differing dysfunctional proteins) with unique metabolomic profiles. However, the exact nature and mechanisms responsible for metabolic reprogramming in cancer cells remain to be fully explored [79].
From the aforementioned, lung cancer diagnosis generally occurs at the late stages of the disease, when curative treatments are not efficacious or possible anymore. Thus, new methodologies were explored to identify early signs of the disease. One of them, the presence of specific metabolites in different body fluids, might offer an answer for an early diagnosis. Metabolomics has been used to detect and quantify metabolites related to cancer. Fluids such as serum, plasma, urine, and sputum have been evaluated as potential sources of specific metabolites. A summary of the studies that evaluated the metabolomics of lung cancer versus healthy controls using body fluids is described in Table 2. In these studies, metabolites with sufficient power to discriminate the lung cancer groups from the healthy controls were indicated after statistical analyses. Although this finding constitutes a significant advance in discovering universal biomarkers, no matching was observed when comparing the metabolites between the studies.
Table 2.
Dysregulated metabolites among various types of lung cancer.
Furthermore, although changes in similar biochemical pathways were observed, no specific metabolite(s) have been found, as represented in all of the studies. It should be mentioned that while the use of various fluids such as serum, plasma, urine, and sputum for metabolic studies has been described, another important fluid proposed more recently for lung cancer studies is bronchoalveolar lavage fluid (BALF), due to its vicinity to cancerous tissue. In this regard, technological advances in separating and detecting exfoliated tumor cells from BALF for lung cancer diagnosis have recently been reported [97]. In addition, cell-free DNA (cfDNA) from BALF has also been used to identify lung cancer. Indeed, cfDNA profiling can distinguish small malignant tumors (≤2cm in diameter) from benign pulmonary nodules with a reported 83% sensitivity and an 87.5% specificity, thus potentially being of diagnostic value [98]. In addition, exhaled breath condensate (EBC) and breath biomarkers for lung cancer have also been proposed as a testing sample for lung cancer diagnosis [99]. However, the cost and reproducibility are concerning. Furthermore, interference effects and staging of patients for early detection still need to be explored to establish the clinical applicability of metabolomics of EBC and breath biomarkers in lung cancer diagnostics.
It should be noted that the data presented in Table 2 reflect the dysregulated metabolites in different biofluids, even though the metabolomics of lung cancer tissue were also reported in some of these studies. It is the intent of this review to focus on biofluids only as the trend is now on liquid biopsy as a valuable diagnostic tool. However, finding universal biomarkers for disease diagnosis is difficult because of the complexity of the analyzed fluids, especially serum and plasma. In addition, the lack of a standardization protocol generates variations between the studies. Some of the concerns in the performance of the studies are as follows.
5.1. Variations of Metabolites
Metabolite variation in individuals has been analyzed, and the need for thousands of patients has been suggested to obtain robust epidemiological studies [100]. Metabolite levels could fluctuate daily during the year and significantly if diets are changed. Generally, studies do not assess the effect of ethnic groups of the cohort, and the variability in the studies can be caused by different nutrients. In addition, biochemical pathways may undergo changes based on ethnicity [101,102].
5.2. Collection, Storage, and Processing
The stability of metabolites during collection until the analysis is critical to obtain consistent results. For example, plasma was shown to be more stable than serum, and other factors should be considered, such as clotting time, ambient temperature, and freezing-thawing cycles [103]. Moreover, studies have shown that glycolysis intermediates, amino acids (e.g., histidine), acetate, and diacylglycerol levels might be compromised by this processing [104]. In the case of urine samples, different profiles were observed, when the same sample was stored at 4 °C and −20 °C. The results showed a significant reduction in 14 metabolites (e.g., N-acetyl glycine, adenosine, creatine, pyridoxal, and succinic acid) in samples stored at 4 °C compared to a more stable level at −20 °C [105].
5.3. Variations of Manufacturing Kits
The comparison of the results obtained by the platforms Biocrates and Metabolon showed some discrepancies that should be considered a metabolite variation. For example, the metabolite lysoPC a C20:4 showed a low correlation with the same cohort results [106]. This variation probably originated from the way both platforms analyzed this specific metabolite. For example, Metabolon quantified lysoPC 20:4 fatty acid chain at position sn1, whereas Biocrates did not discriminate between positions sn1 and sn2 and it quantified only the total levels of both fatty acids.
5.4. Instrumentation and Data Processing
Two types of mass spectrometry (MS) instruments are used in metabolomics. They include gas- and liquid-chromatography (GC and LC, respectively). Upon measuring the masses of the metabolites, a library is necessary to determine the identity of each one. This analysis represents a potential impact on data analysis and processing, as different libraries are available. Each one has different algorithms that might bring slight differences in a study. For example, the libraries accurately identify known metabolites but may be less efficient for unknown molecules.
Other factors in the performance of the instruments are related to the analysis of hundreds of samples that might bring differences based on the instrument performance. For example, analytical changes result from column degradation, GC/LC conditions, mass spectrometer contamination, or metabolite degradation/decay due to the waiting time [107,108].
5.5. Effect of Underlying Diseases or Non-Related Metabolites
It is important to determine the impact of medications on underlying diseases/conditions when analyzing metabolomics results. For example, therapies related to underlying diseases in lung cancer comorbidities are metabolized mainly in the liver. This metabolism could generate novel metabolites by introducing errors in the metabolomic analysis. In addition, the microbiome might also metabolize drugs that can be reabsorbed in the bloodstream [109], introducing confounding factors. Other examples include the presence of paracetamol as a metabolite with high significance, which is probably the residual of a drug consumed by the patients [87].
Moreover, the presence of bisphenol A in the list of metabolites is problematic as this is a synthetic molecule, and its presence can be related either to an error in the identification of the molecule or, less probably, to high-consumption bottle beverages as bisphenol A is used in the manufacturing of polycarbonate bottles. In addition, as bisphenol A is poorly soluble in water, the presence in blood can result from high levels in drinking water [92]. Finally, it should be pointed out that a number of different factors need to be considered when undertaking metabolomic studies, including diet [110] and comorbidities [111,112,113,114,115,116,117,118,119]. In this regard, obesity [111,112], chronic obstructive pulmonary disease [113,114,115], kidney disease [116], diabetes [117,118], and cardiovascular disease [94] have all been reported to have a major impact on the metabolome that can confound metabolomic studies in cancer, and thus, their influence cannot be underestimated.
Although the application of metabolomics is growing for cancer diagnosis, more studies are necessary to be implemented for a final use for biomarker measurement. As mentioned above, there is an inconsistency in the chosen metabolites that discriminate lung cancer from healthy individuals. In addition, the heterogeneity of samples related to the types of lung cancer, together with the different stages in the patients, is adding more variability. Overall, the validation of new biomarkers in lung cancer diagnosis needs studies that include thousands of patients stratified according to their cancer types and stages of the disease and effects of other clinical parameters, including comorbidities and drug interactions.
We have focused on the polyamine pathway due to its connection to many types of cancer. Multiple proteins constitute this pathway, and when one of them does not function properly, the levels of metabolite at the point of dysfunction will be altered until they reach a new equilibrium that allows cancer to grow. Using this concept, we have defined and validated the preliminary fingerprint for lung cancer and are in the process of determining the fingerprint for breast cancer. Using quantitative metabolite tests instead of genetic tests, protein tests, or X-ray imaging allows such a test to be quickly and inexpensively integrated into the existing clinical testing infrastructure. It also makes the test far more reproducible and much more accurate [96]. As of yet, no other high-performing chemical/metabolite test for lung cancer screening has been developed anywhere in the world.
6. Potential Impact on Patients
The Canadian Task Force on Preventative Health Care recommends screening by LDCT for adults aged 55–74 years old who smoke or used to smoke in the last 15 years and smoked 30 pack years. However, there are significant challenges with implementing and adopting such a program, including radiation exposure, poor patient uptake due to lengthy follow-up processes, and resources required to implement and successfully execute a provincial LDCT screening program. Furthermore, LDCT has a very high false-positive rate contributing to further health care resource depletion through unnecessary follow-up procedures and biopsies, increased health care costs, increased patient risk, and patient anxiety. A more straightforward, inexpensive, more accurate early-detection lung cancer test would benefit cancer patients as follows: (1) Earlier, more accurate diagnosis will lead to better patient health for high-risk individuals. Smokers would immediately benefit from low-cost population-based screening for lung cancer. (2) Early detection will save lives and reduce costs related to treatment at advanced stages, targeting the detection of stage I lung cancer (over 53% of patients are asymptomatic), would significantly improve the cure rates as compared to detection at late-stage disease. (3) The dynamics of patient triage and quality of care will change. A metabolomics blood-based test will enable physicians to make evidence-based prevention and treatment decisions. A blood-based test makes sample collection very simple, and it is more likely to encourage patient participation in screening programs. (4) Patient anxiety will be reduced. Obtaining the result of a lung cancer test within hours will decrease the anxiety associated with waiting. If the test is positive, patients will be placed in a correct health care stream for immediate treatment. This test would be expected to fit into the physician’s workflow and current programs quickly.
There are bottlenecks associated with the identification and application of metabolomics. Outstanding concerns preventing the widespread clinical use of metabolomics as a diagnostic/predictive tool are the scalability of data interpretation, the standardization of sample handling practice, and e-infrastructure [120]. However, as these issues become resolved, it is conceivable that the routine utilization of metabolomics at the patient and population levels will constitute an integral part of future healthcare provision [120] and the improved management of patients with cancer [121].
7. Conclusions
Cancer is a metabolic disease caused by mutations in key metabolic pathways and key metabolic regulators. Metabolomics has led to identifying several oncometabolites and many high-performing cancer metabolite biomarkers. Thus, the use of metabolomic assays and multi-metabolite markers allows for the rapid, accurate diagnosis and monitoring of not only lung cancer but has the potential applicability in multiple types of cancer. The utility of metabolomics as a fast, accurate, cheap liquid biopsy technique in cancer is under-exploited and thus represents an enormous opportunity in cancer diagnostics and prognostics. We hope the nature of this review contributes to existing knowledge in the field of metabolomics in cancer and how it can be utilized as a robust diagnostic tool for the early detection of lung cancer. Therefore, developing a low-cost, high-throughput metabolomic test will make early-stage lung cancer screening feasible and affordable globally, where survival rates are low, particularly for at-risk populations. In addition, such a paradigm shift in lung cancer screening will make blood-based testing routines accessible to those patients at the highest risk for lung cancer and serve as a viable alternative to molecular and proteomic-based markers for the early detection of lung cancer.
Author Contributions
Conceptualization, R.A.B., J.-F.H., P.S.T.; writing-original draft preparation, J.-F.H., P.S.T. and R.A.B., responsibility for the final draft and the scientific background of the manuscript, R.A.B., H.B., P.S.T., P.J. and B.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Note applicable.
Data Availability Statement
Not appliable.
Acknowledgments
Infrastructural support was provided by the Albrechtsen Research Centre, St. Boniface Hospital.
Conflicts of Interest
R.A.B. is the President and Chief Executive Officer of BioMark Diagnostics Inc. and J.-F. H. is Chief Scientific Officer and General Manager of BioMark Diagnostics Inc. P.S.T. is a mi-nor shareholder of BioMark Diagnostics Inc. The authors have no other relevant affilia-tions or financial involvement with any organization or entity with a financial interest or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
References
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today. Lyon: International Agency for Research on Cancer; 2020. Available online: https://gco.iarc.fr/today (accessed on 16 November 2021).
- World Cancer Research Fund. Available online: https://www.wcrf.org/dietandcancer/lung-cancer-statistics/ (accessed on 16 November 2021).
- Chadder, J.; Dewar, R.; Shack, L.; Nishri, D.; Niu, J.; Lockwood, G. A first look at relative survival by stage for colorectal and lung cancers in Canada. Curr. Oncol. 2016, 23, 119–124. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Jin, Q.; Ma, R.C.W. Metabolomics in diabetes and diabetic complications: Insights from epidemiological studies. Cells 2021, 10, 2832. [Google Scholar] [CrossRef]
- Brennan, L.; Hu, F.B.; Sun, Q. Metabolomics meets nutritional epidemiology: Harnessing the potential in metabolomics data. Metabolites 2021, 11, 709. [Google Scholar] [CrossRef] [PubMed]
- Onuh, J.O.; Qiu, H. Metabolic profiling and metabolites fingerprints in human hypertension: Discovery and potential. Metabolites 2021, 11, 687. [Google Scholar] [CrossRef]
- McGranaghan, P.; Kirwan, J.A.; Garcia-Rivera, M.A.; Pieske, B.; Edelmann, F.; Blaschke, F.; Appunni, S.; Saxena, A.; Rubens, M.; Veledar, E.; et al. Lipid metabolite biomarkers in cardiovascular disease: Discovery and biomechanism translation from human studies. Metabolites 2021, 11, 621. [Google Scholar] [CrossRef] [PubMed]
- LeVatte, M.; Keshteli, A.H.; Zarei, P.; Wishart, D.S. Applications of metabolomics to precision nutrition. Lifestyle Genom. 2021, 8, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Schultheiss, U.T.; Kosch, R.; Kotsis, F.; Altenbuchinger, M.; Zacharias, H.U. Chronic kidney disease cohort studies: A guide to metabolome analyses. Metabolites 2021, 11, 460. [Google Scholar] [CrossRef]
- Walker, A.; Schmitt-Kopplin, P. The role of fecal sulfur metabolome in inflammatory bowel diseases. Int. J. Med. Microbiol. 2021, 311, 151513. [Google Scholar] [CrossRef]
- Liang, L.; Sun, F.; Wang, H.; Hu, Z. Metabolomics, metabolic flux analysis and cancer pharmacology. Pharmacol. Ther. 2021, 224, 107827. [Google Scholar] [CrossRef]
- Alldritt, I.; Greenhaff, P.L.; Wilkinson, D.J. Metabolomics as an important tool for determining the mechanisms of human skeletal muscle deconditioning. Int. J. Mol. Sci. 2021, 22, 13575. [Google Scholar] [CrossRef] [PubMed]
- Daisley, B.A.; Koenig, D.; Engelbrecht, K.; Doney, L.; Hards, K.; Al, K.F.; Reid, G.; Burton, J.P. Emerging connections between gut microbiome bioenergetics and chronic metabolic diseases. Cell Rep. 2021, 37, 110087. [Google Scholar] [CrossRef]
- Zhou, J.; Huang, Z.A.; Kumar, U.; Chen, D.D.Y. Review of recent developments in determining volatile organic compounds in exhaled breath as biomarkers for lung cancer diagnosis. Anal. Chim. Acta. 2017, 996, 1–9. [Google Scholar] [CrossRef]
- Sher, T.; Dy, G.K.; Adjei, A.A. Small cell lung cancer. Mayo. Clin. Proc. 2008, 83, 355–367. [Google Scholar] [CrossRef] [PubMed]
- Samet, J.M.; Avila-Tang, E.; Boffetta, P.; Hannan, L.M.; Olivo-Marston, S.; Thun, M.J.; Rudin, C.M. Lung cancer in never smokers: Clinical epidemiology and environmental risk factors. Clin. Cancer Res. 2009, 15, 5626–5645. [Google Scholar] [CrossRef]
- Hubaux, R.; Becker-Santos, D.D.; Enfield, K.S.; Lam, S.; Lam, W.L.; Martinez, V.D. Arsenic, asbestos and radon: Emerging players in lung tumorigenesis. Environ. Health 2012, 11, 89. [Google Scholar] [CrossRef] [PubMed]
- Vineis, P.; Forastiere, F.; Hoek, G.; Lipsett, M. Outdoor air pollution and lung cancer: Recent epidemiologic evidence. Int. J. Cancer. 2004, 111, 647–652. [Google Scholar] [CrossRef] [PubMed]
- Vallières, E.; Pintos, J.; Parent, M.E.; Siemiatycki, J. Occupational exposure to wood dust and risk of lung cancer in two population-based case-control studies in Montreal, Canada. Environ. Health 2015, 14, 1. [Google Scholar] [CrossRef] [PubMed]
- Öberg, M.; Jaakkola, M.S.; Woodward, A.; Peruga, A.; Prüss-Ustün, A. Worldwide burden of disease from exposure to second-hand smoke: A retrospective analysis of data from 192 countries. Lancet 2011, 377, 139–146. [Google Scholar] [CrossRef]
- Sagerup, C.M.; Småstuen, M.; Johannesen, T.B.; Helland, Å.; Brustugun, O.T. Sex-specific trends in lung cancer incidence and survival: A population study of 40,118 cases. Thorax 2011, 66, 301–307. [Google Scholar] [CrossRef] [PubMed]
- CancerControl AB, Surveillance & Reporting: 2012 Report on Cancer Statistics in Alberta. 2015. Available online: https://www.albertahealthservices.ca/cancer/Page2407.aspx (accessed on 16 November 2021).
- International Early Lung Cancer Action Program Investigators; Henschke, C.I.; Yankelevitz, D.F.; Libby, D.M.; Pasmantier, M.W.; Smith, J.P.; Miettinen, O.S. Survival of patients with stage I lung cancer detected on CT screening. N. Engl. J. Med. 2006, 355, 1763–1771. [Google Scholar]
- Ko, E.C.; Raben, D.; Formenti, S.C. The integration of radiotherapy with immunotherapy for the treatment of non-small cell lung cancer. Clin. Cancer Res. 2018, 24, 5792–5806. [Google Scholar] [CrossRef]
- Nooreldeen, R.; Bach, H. Current and future development in lung cancer diagnosis. Int. J. Mol. Sci. 2021, 22, 8661. [Google Scholar] [CrossRef]
- Wald, O. CXCR4 Based therapeutics for non-small cell lung cancer (NSCLC). J. Clin. Med. 2018, 7, 303. [Google Scholar] [CrossRef]
- Tang, Y.; Qiao, G.; Xu, E.; Xuan, Y.; Liao, M.; Yin, G. Biomarkers for early diagnosis, prognosis, prediction, and recurrence monitoring of non-small cell lung cancer. Onco. Targets Ther. 2017, 10, 4527–4534. [Google Scholar] [CrossRef]
- Gatteschi, L.; Iannopollo, M.; Gonfiotti, A. Neoadjuvant immunotherapy in resectable non-small cell lung cancer. A narrative review. Life 2021, 11, 1036. [Google Scholar] [CrossRef] [PubMed]
- Knight, S.B.; Crosbie, P.A.; Balata, H.; Chudziak, J.; Hussell, T.; Dive, C. Progress and prospects of early detection in lung cancer. Open Biol. 2017, 7, 170070. [Google Scholar] [CrossRef] [PubMed]
- Gobbini, E.; Levra, M.G. Is there a room for immune checkpoint inhibitors in early stage non-small cell lung cancer? J. Thorac. Dis. 2018, 10, S1427–S1437. [Google Scholar] [CrossRef]
- Arbour, K.C.; Riely, G.J. Systemic therapy for locally advanced and metastatic non-small cell lung cancer: A review. JAMA. 2019, 322, 764–774. [Google Scholar] [CrossRef]
- Dominioni, L.; Strauss, G.M.; Imperatori, A.; Rovera, F.; Dionigi, G. Screening for lung cancer. Chest Surg Clin. N. Am. 2000, 10, 729–736. [Google Scholar] [PubMed]
- Canadian-Task-Force-on-Preventive-Health-Care. Recommendations on screening for lung cancer. CMAJ 2016, 188, 425–432. [Google Scholar] [CrossRef]
- Labbé, C.; Beaudoin, S.; Martel, S.; Delage, A.; Joubert, P.; Drapeau, C.; Provencher, S. Diagnostic yield of non-guided flexible bronchoscopy for peripheral pulmonary neoplasia. Thorac. Cancer 2015, 6, 517–523. [Google Scholar] [CrossRef]
- Rivera, M.P.; Mehta, A.C.; Wahidi, M.M. Establishing the diagnosis of lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013, 143, e142S–e165S. [Google Scholar] [CrossRef] [PubMed]
- Shirakawa, T.; Imamura, F.; Hamamoto, J.; Honda, I.; Fukushima, K.; Sugimoto, M.; Shirkakusa, T. Usefulness of endobronchial ultrasonography for transbronchial lung biopsies of peripheral lung lesions. Respiration 2004, 71, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, G.; McCrory, D.C. Performance characteristics of different modalities for diagnosis of suspected lung cancer: Summary of published evidence. Chest 2003, 123, 115s–128s. [Google Scholar] [CrossRef] [PubMed]
- Rivera, M.P.; Detterbeck, F.; Mehta, A.C. Diagnosis of lung cancer: The guidelines. Chest 2003, 123, 129s–136s. [Google Scholar] [CrossRef]
- Aberle, D.R.; Abtin, F.; Brown, K. Computed tomography screening for lung cancer: Has it finally arrived? Implications of the national lung screening trial. J. Clin. Oncol. 2013, 31, 1002–1008. [Google Scholar] [CrossRef]
- Patz, E.F., Jr.; Pinsky, P.; Gatsonis, C.; Sicks, J.D.; Kramer, B.S.; Tammemägi, M.C.; Chiles, C.; Black, W.C.; Aberle, D.R.; NLST Overdiagnosis Manuscript Writing Team. Overdiagnosis in low-dose computed tomography screening for lung cancer. JAMA Intern. Med. 2014, 174, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Sharma, D.; Newman, T.G.; Aronow, W.S. Lung cancer screening: History, current perspectives, and future directions. Arch. Med. Sci. 2015, 11, 1033–1043. [Google Scholar] [PubMed]
- Griffey, R.T.; Sodickson, A. Cumulative radiation exposure and cancer risk estimates in emergency department patients undergoing repeat or multiple CT. AJR Am. J. Roentgenol. 2009, 192, 887–892. [Google Scholar] [CrossRef] [PubMed]
- Mascalchi, M.; Sali, L. Lung cancer screening with low dose CT and radiation harm-from prediction models to cancer incidence data. Ann. Transl. Med. 2017, 5, 360. [Google Scholar] [CrossRef]
- Rampinelli, C.; De Marco, P.; Origgi, D.; Maisonneuve, P.; Casiraghi, M.; Veronesi, G.; Spaggiari, L.; Bellomi, M. Exposure to low dose computed tomography for lung cancer screening and risk of cancer: Secondary analysis of trial data and risk-benefit analysis. BMJ 2017, 356, j347. [Google Scholar] [CrossRef]
- Berg, C.D. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011, 365, 395–409. [Google Scholar]
- Horeweg, N.; van der Aalst, C.M.; Thunnissen, E.; Nackaerts, K.; Weenink, C.; Groen, H.J.; Lammers, J.W.; Aerts, J.G.; Scholten, E.T.; van Rosmalen, J.; et al. Characteristics of lung cancers detected by computer tomography screening in the randomized NELSON trial. Am. J. Respir. Crit. Care Med. 2013, 187, 848–854. [Google Scholar] [CrossRef]
- Duquenne, J.B.; Paulus, A.; Sibille, A.; Corhay, J.L.; Louis, R.; Duysinx, B. Pre-cancerous lung lesions and lung cancer screening. Rev. Med. Liege. 2021, 76, 440–445. [Google Scholar]
- Nardi-Agmon, I.; Peled, N. Exhaled breath analysis for the early detection of lung cancer: Recent developments and future prospects. Lung Cancer 2017, 8, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Leng, W.; Sun, C.; Lu, T.; Chen, Z.; Men, X.; Wang, Y.; Wang, G.; Zhen, B.; Qin, J. Urine Proteome profiling predicts lung cancer from control cases and other tumors. EBioMedicine 2018, 30, 120–128. [Google Scholar] [CrossRef]
- Hubers, A.J.; Prinsen, C.F.; Sozzi, G.; Witte, B.I.; Thunnissen, E. Molecular sputum analysis for the diagnosis of lung cancer. Br. J. Cancer 2013, 109, 530–537. [Google Scholar] [CrossRef]
- Mehta, A.; Cordero, J.; Dobersch, S.; Romero-Olmedo, A.J.; Savai, R.; Bodner, J.; Chao, C.M.; Fink, L.; Guzmán-Díaz, E.; Singh, I.; et al. Non-invasive lung cancer diagnosis by detection of GATA6 and NKX2-1 isoforms in exhaled breath condensate. EMBO Mol. Med. 2016, 8, 1380–1389. [Google Scholar] [CrossRef]
- Mamdani, H.; Ahmed, S.; Armstrong, S.; Mok, T.; Jalal, S.I. Blood-based tumor biomarkers in lung cancer for detection and treatment. Transl. Lung Cancer Res. 2017, 6, 648–660. [Google Scholar] [CrossRef] [PubMed]
- Paci, M.; Rapicetta, C.; Maramotti, S. New biomarkers for lung cancer. Expert Opin Med. Diagn. 2010, 4, 201–224. [Google Scholar] [CrossRef] [PubMed]
- Zamay, T.N.; Zamay, G.S.; Kolovskaya, O.S.; Zukov, R.A.; Petrova, M.M.; Gargaun, A.; Berezovski, M.V.; Kichkailo, A.S. Current and prospective protein biomarkers of lung cancer. Cancers 2017, 9, 155. [Google Scholar] [CrossRef]
- Zhong, L.; Coe, S.P.; Stromberg, A.J.; Khattar, N.H.; Jett, J.R.; Hirschowitz, E.A. Profiling tumor-associated antibodies for early detection of non-small cell lung cancer. J. Thorac. Oncol. 2006, 1, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Heitzer, E.; Ulz, P.; Geigl, J.B. Circulating tumor DNA as a liquid biopsy for cancer. Clin. Chem. 2015, 61, 112–123. [Google Scholar] [CrossRef] [PubMed]
- Hussain, S.H.; Huertas, C.S.; Mitchell, A.; Deman, A.L.; Laurenceau, E. Biosensors for circulating tumor cells (CTCs)-biomarker detection in lung and prostate cancer: Trends and prospects. Biosens. Bioelectron. 2021, 197, 113770. [Google Scholar] [CrossRef]
- Rabinowits, G.; Gerçel-Taylor, C.; Day, J.M.; Taylor, D.D.; Kloecker, G.H. Exosomal microRNA: A diagnostic marker for lung cancer. Clin. Lung Cancer 2009, 10, 42–46. [Google Scholar] [CrossRef]
- Ostrow, K.L.; Hoque, M.O.; Loyo, M.; Brait, M.; Greenberg, A.; Siegfried, J.M.; Grandis, J.R.; Davis, A.G.; Bigbee, W.L.; Rom, W.; et al. Molecular analysis of plasma DNA for the early detection of lung cancer by quantitative methylation-specific PCR. Clin. Cancer Res. 2010, 16, 3463–3472. [Google Scholar] [CrossRef] [PubMed]
- Duarte, I.F.; Rocha, C.M.; Gil, A.M. Metabolic profiling of biofluids: Potential in lung cancer screening and diagnosis. Expert Rev. Mol. Diagn. 2013, 13, 737–748. [Google Scholar] [CrossRef]
- Blanco-Prieto, S.; De Chiara, L.; Rodríguez-Girondo, M.; Vázquez-Iglesias, L.; Rodríguez-Berrocal, F.J.; Fernández-Villar, A.; Botana-Rial, M.I.; de la Cadena, M.P. Highly sensitive marker panel for guidance in lung cancer rapid diagnostic units. Sci. Rep. 2017, 7, 41151. [Google Scholar] [CrossRef] [PubMed]
- Boeri, M.; Verri, C.; Conte, D.; Roz, L.; Modena, P.; Facchinetti, F.; Calabrò, E.; Croce, C.M.; Pastorino, U.; Sozzi, G. MicroRNA signatures in tissues and plasma predict development and prognosis of computed tomography detected lung cancer. Proc. Natl. Acad. Sci. USA 2011, 108, 3713–3718. [Google Scholar] [CrossRef]
- Ostroff, R.M.; Bigbee, W.L.; Franklin, W.; Gold, L.; Mehan, M.; Miller, Y.E.; Pass, H.I.; Rom, W.N.; Siegfried, J.M.; Stewart, A.; et al. Unlocking biomarker discovery: Large scale application of aptamer proteomic technology for early detection of lung cancer. PLoS ONE 2010, 5, e15003. [Google Scholar] [CrossRef] [PubMed]
- Boyle, P.; Chapman, C.J.; Holdenrieder, S.; Murray, A.; Robertson, C.; Wood, W.C.; Maddison, P.; Healey, G.; Fairley, G.H.; Barnes, A.C.; et al. Clinical validation of an autoantibody test for lung cancer. Ann. Oncol. 2011, 22, 383–389. [Google Scholar] [CrossRef]
- Jett, J.R.; Peek, L.J.; Fredericks, L.; Jewell, W.; Pingleton, W.W.; Robertson, J.F. Audit of the autoantibody test, EarlyCDT(R)-lung, in 1600 patients: An evaluation of its performance in routine clinical practice. Lung Cancer 2014, 83, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics: A 2020 Special Report on Lung Cancer; Canadian Cancer Society: Toronto, ON, Canada, 2020. [Google Scholar]
- Dama, E.; Colangelo, T.; Fina, E.; Cremonesi, M.; Kallikourdis, M.; Veronesi, G.; Bianchi, F. Biomarkers and lung cancer early detection: State of the art. Cancers 2021, 13, 3919. [Google Scholar] [CrossRef] [PubMed]
- Freitas, C.; Sousa, C.; Machado, F.; Serino, M.; Santos, V.; Cruz-Martins, N.; Teixeira, A.; Cunha, A.; Pereira, T.; Oliveira, H.P.; et al. The role of liquid biopsy in early diagnosis of lung cancer. Front. Oncol. 2021, 11, 634316. [Google Scholar] [CrossRef]
- Kim, K.; Mall, C.; Taylor, S.L.; Hitchcock, S.; Zhang, C.; Wettersten, H.I.; Jones, A.D.; Chapman, A.; Weiss, R.H. Mealtime, temporal, and daily variability of the human urinary and plasma metabolomes in a tightly controlled environment. PLoS ONE 2014, 9, e86223. [Google Scholar] [CrossRef]
- Suhre, K.; Raffler, J.; Kastenmüller, G. Biochemical insights from population studies with genetics and metabolomics. Arch. Biochem. Biophys. 2016, 589, 168–176. [Google Scholar] [CrossRef]
- Wishart, D.S. Systems biology resources arising from the human metabolome project. In Genetics Meets Metabolomics: From Experiment to Systems Biology; Suhre, K., Ed.; Springer: New York, NY, USA, 2012; pp. 157–175. [Google Scholar]
- Wishart, D.S. Metabolomics for investigating physiological and pathophysiological processes. Physiol. Rev. 2019, 99, 1819–1875. [Google Scholar] [CrossRef]
- Fiehn, O. Metabolomics–the link between genotypes and phenotypes. Plant. Mol. Biol. 2002, 48, 155–171. [Google Scholar] [CrossRef]
- Wishart, D.S.; Mandal, R.; Stanislaus, A.; Ramirez-Gaona, M. Cancer metabolomics and the human metabolome database. Metabolites 2016, 6, 10. [Google Scholar] [CrossRef]
- Vanhove, K.; Graulus, G.J.; Mesotten, L.; Thomeer, M.; Derveaux, E.; Noben, J.P.; Guedens, W.; Adriaensens, P. The metabolic landscape of lung cancer: New insights in a disturbed glucose metabolism. Front. Oncol. 2019, 9, 1215. [Google Scholar] [CrossRef] [PubMed]
- Anastasiou, D. Tumour microenvironment factors shaping the cancer metabolism landscape. Br. J. Cancer 2017, 116, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef]
- Pavlova, N.N.; Thompson, C.B. The emerging hallmarks of cancer metabolism. Cell Metab. 2016, 23, 27–47. [Google Scholar] [CrossRef] [PubMed]
- DeBerardinis, R.J.; Chandel, N.S. Fundamentals of cancer metabolism. Sci. Adv. 2016, 2, e1600200. [Google Scholar] [CrossRef]
- Kowalczyk, T.; Kisluk, J.; Pietrowska, K.; Godzien, J.; Kozlowski, M.; Reszeć, J.; Sierko, E.; Naumnik, W.; Mróz, R.; Moniuszko, M.; et al. The Ability of metabolomics to discriminate non-small-cell lung cancer subtypes depends on the stage of the disease and the type of material studied. Cancers 2021, 13, 3314. [Google Scholar] [CrossRef] [PubMed]
- Singhal, S.; Rolfo, C.; Maksymiuk, A.W.; Tappia, P.S.; Sitar, D.S.; Russo, A.; Akhtar, P.S.; Khatun, N.; Rahnuma, P.; Rashiduzzaman, A.; et al. Liquid biopsy in lung cancer screening: The contribution of metabolomics. Results of a pilot study. Cancers 2019, 11, 1069. [Google Scholar] [CrossRef] [PubMed]
- Wen, T.; Gao, L.; Wen, Z.; Wu, C.; Tan, C.S.; Toh, W.Z.; Ong, C.N. Exploratory investigation of plasma metabolomics in human lung adenocarcinoma. Mol. Biosyst. 2013, 9, 2370–2378. [Google Scholar] [CrossRef]
- Zhang, X.; Zhu, X.; Wang, C.; Zhang, H.; Cai, Z. Non-targeted and targeted metabolomics approaches to diagnosing lung cancer and predicting patient prognosis. Oncotarget 2016, 7, 63437–63448. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Zheng, J.; Ahmed, R.; Huang, G.; Reid, J.; Mandal, R.; Maksymiuk, A.; Sitar, D.S.; Tappia, P.S.; Ramjiawan, B.; et al. A high-performing plasma metabolite panel for early-stage lung cancer detection. Cancers 2020, 12, 622. [Google Scholar] [CrossRef]
- Callejón-Leblic, B.; García-Barrera, T.; Pereira-Vega, A.; Gómez-Ariza, J.L. Metabolomic study of serum, urine and bronchoalveolar lavage fluid based on gas chromatography mass spectrometry to delve into the pathology of lung cancer. J. Pharm. Biomed. Anal. 2019, 163, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Ma, Z.; Li, A.; Li, H.; Wang, B.; Zhong, J.; Min, L.; Dai, L. Metabolomic profiling of human serum in lung cancer patients using liquid chromatography/hybrid quadrupole time-of-flight mass spectrometry and gas chromatography/mass spectrometry. J. Cancer Res. Clin. Oncol. 2015, 141, 705–718. [Google Scholar] [CrossRef] [PubMed]
- Fahrmann, J.F.; Kim, K.; DeFelice, B.C.; Taylor, S.L.; Gandara, D.R.; Yoneda, K.Y.; Cooke, D.T.; Fiehn, O.; Kelly, K.; Miyamoto, S. Investigation of metabolomic blood biomarkers for detection of adenocarcinoma lung cancer. Cancer Epidemiol. Biomark. Prev. 2015, 24, 1716–1723. [Google Scholar] [CrossRef] [PubMed]
- Mu, Y.; Zhou, Y.; Wang, Y.; Li, W.; Zhou, L.; Lu, X.; Gao, P.; Gao, M.; Zhao, Y.; Wang, Q.; et al. Serum metabolomics study of non smoking female patients with non-small cell lung cancer using gas chromatography-mass spectrometry. J. Proteome Res. 2019, 18, 2175–2184. [Google Scholar] [CrossRef] [PubMed]
- Ni, J.; Xu, L.; Li, W.; Zheng, C.; Wu, L. Targeted metabolomics for serum amino acids and acylcarnitines in patients with lung cancer. Exp. Ther. Med. 2019, 18, 188–198. [Google Scholar] [CrossRef]
- Pamungkas, A.D.; Park, C.; Lee, S.; Jee, S.H.; Park, Y.H. High resolution metabolomics to discriminate compounds in serum of male lung cancer patients in South Korea. Respir. Res. 2016, 17, 100. [Google Scholar] [CrossRef] [PubMed]
- Ruiying, C.; Zeyun, L.; Yongliang, Y.; Zijia, Z.; Ji, Z.; Xin, T.; Xiaojian, Z. A comprehensive analysis of metabolomics and transcriptomics in non-small cell lung cancer. PLoS ONE 2020, 15, e0232272. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Zhao, W.; Wang, L.; Guo, F.; Song, D.; Zhang, Q.; Zhang, D.; Fan, Y.; Wang, J. Integration of metabolomic and transcriptomic profiles to identify biomarkers in serum of lung cancer. J. Cell. Biochem. 2019. Epub Ahead of Print. [Google Scholar] [CrossRef]
- Zheng, Y.; He, Z.; Kong, Y.; Huang, X.; Zhu, W.; Liu, Z.; Gong, L. Combined metabolomics with transcriptomics reveals important serum biomarkers correlated with lung cancer proliferation through a calcium signaling pathway. J. Proteome Res. 2021, 20, 3444–3454. [Google Scholar] [CrossRef] [PubMed]
- Cameron, S.J.; Lewis, K.E.; Beckmann, M.; Allison, G.G.; Ghosal, R.; Lewis, P.D.; Mur, L.A. The metabolomic detection of lung cancer biomarkers in sputum. Lung Cancer 2016, 94, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Mathé, E.A.; Patterson, A.D.; Haznadar, M.; Manna, S.K.; Krausz, K.W.; Bowman, E.D.; Shields, P.G.; Idle, J.R.; Smith, P.B.; Anami, K.; et al. Noninvasive urinary metabolomic profiling identifies diagnostic and prognostic markers in lung cancer. Cancer Res. 2014, 74, 3259–3270. [Google Scholar] [CrossRef]
- Zhao, C.; Kong, X.; Han, S.; Li, X.; Wu, T.; Zhou, J.; Guo, Y.; Bu, Z.; Liu, C.; Zhang, C.; et al. Analysis of differential metabolites in lung cancer patients based on metabolomics and bioinformatics. Future Oncol. 2020, 16, 1269–1287. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Liu, Y.; Zhang, W.; Lin, L.; Zhang, J.; Xiong, Y.; Nie, L.; Liu, X.; Li, H.; Wang, W. A rapid liquid biopsy of lung cancer by separation and detection of exfoliated tumor cells from bronchoalveolar lavage fluid with a dual-layer “PERFECT” filter system. Theranostics 2020, 10, 6517–6529. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Mu, C.; Zhao, J.; Zeng, D.; Wang, C.; Ye, J.; Xu, J.; Su, J.; Han-Zhang, H.; Li, B.; et al. Cell-free DNA from bronchoalveolar lavage fluid (BALF) for the identification of lung cancer: A new medium of liquid biopsy. Cancer Res. 2020, 80, 2311. [Google Scholar]
- Pérez-Sánchez, C.; Barbarroja, N.; Pantaleão, L.C.; López-Sánchez, L.M.; Ozanne, S.E.; Jurado-Gámez, B.; Aranda, E.; Lopez-Pedrera, C.; Rodríguez-Ariza, A. Clinical Utility of microRNAs in Exhaled Breath Condensate as Biomarkers for Lung Cancer. J. Pers. Med. 2021, 11, 111. [Google Scholar] [CrossRef]
- Sampson, J.N.; Boca, S.M.; Shu, X.O.; Stolzenberg-Solomon, R.Z.; Matthews, C.E.; Hsing, A.W.; Tan, Y.T.; Ji, B.T.; Chow, W.H.; Cai, Q.; et al. Metabolomics in epidemiology: Sources of variability in metabolite measurements and implications. Cancer Epidemiol. Biomark. Prev. 2013, 22, 631–640. [Google Scholar] [CrossRef]
- Sanchez, O.A.; Duprez, D.A.; Bahrami, H.; Daniels, L.B.; Folsom, A.R.; Lima, J.A.; Maisel, A.; Peralta, C.A.; Jacobs, D.R., Jr. The associations between metabolic variables and NT-proBNP are blunted at pathological ranges: The Multi-Ethnic Study of Atherosclerosis. Metabolism 2014, 63, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Sato, S.; Parr, E.B.; Devlin, B.L.; Hawley, J.A.; Sassone-Corsi, P. Human metabolomics reveal daily variations under nutritional challenges specific to serum and skeletal muscle. Mol. Metab. 2018, 16, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Hirayama, A.; Sugimoto, M.; Suzuki, A.; Hatakeyama, Y.; Enomoto, A.; Harada, S.; Soga, T.; Tomita, M.; Takebayashi, T. Effects of processing and storage conditions on charged metabolomic profiles in blood. Electrophoresis 2015, 36, 2148–2155. [Google Scholar] [CrossRef]
- Ferreira, D.L.S.; Maple, H.J.; Goodwin, M.; Brand, J.S.; Yip, V.; Min, J.L.; Groom, A.; Lawlor, D.A.; Ring, S. The effect of pre-analytical conditions on blood metabolomics in epidemiological studies. Metabolites 2019, 9, 64. [Google Scholar] [CrossRef]
- Laparre, J.; Kaabia, Z.; Mooney, M.; Buckley, T.; Sherry, M.; Le Bizec, B.; Dervilly-Pinel, G. Impact of storage conditions on the urinary metabolomics fingerprint. Anal. Chim. Acta 2017, 951, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Yet, I.; Menni, C.; Shin, S.Y.; Mangino, M.; Soranzo, N.; Adamski, J.; Suhre, K.; Spector, T.D.; Kastenmüller, G.; Bell, J.T. Genetic influences on metabolite levels: A comparison across metabolomic platforms. PLoS ONE 2016, 11, e0153672. [Google Scholar] [CrossRef]
- Zelena, E.; Dunn, W.B.; Broadhurst, D.; Francis-McIntyre, S.; Carroll, K.M.; Begley, P.; O’Hagan, S.; Knowles, J.D.; Halsall, A.; Wilson, I.D.; et al. Development of a robust and repeatable UPLC-MS method for the long-term metabolomic study of human serum. Anal. Chem. 2009, 81, 1357–1364. [Google Scholar] [CrossRef]
- Gika, H.G.; Macpherson, E.; Theodoridis, G.A.; Wilson, I.D. Evaluation of the repeatability of ultra-performance liquid chromatography-TOF-MS for global metabolic profiling of human urine samples. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2008, 871, 299–305. [Google Scholar] [CrossRef]
- Noh, K.; Kang, Y.R.; Nepal, M.R.; Shakya, R.; Kang, M.J.; Kang, W.; Lee, S.; Jeong, H.G.; Jeong, T.C. Impact of gut microbiota on drug metabolism: An update for safe and effective use of drugs. Arch. Pharm. Res. 2017, 40, 1345–1355. [Google Scholar] [CrossRef]
- Emwas, A.M.; Al-Rifai, N.; Szczepski, K.; Alsuhaymi, S.; Rayyan, S.; Almahasheer, H.; Jaremko, M.; Brennan, L.; Lachowicz, J.I. You are what you eat: Application of metabolomics approaches to advance nutrition research. Foods 2021, 10, 1249. [Google Scholar] [CrossRef] [PubMed]
- Cheng, D.; Zhao, X.; Yang, S.; Cui, H.; Wang, G. Metabolomic signature between metabolically healthy overweight/obese and metabolically unhealthy overweight/obese: A systematic review. Diabetes Metab. Syndr. Obes. 2021, 14, 991–1010. [Google Scholar] [CrossRef] [PubMed]
- Handakas, E.; Lau, C.H.; Alfano, R.; Chatzi, V.L.; Plusquin, M.; Vineis, P.; Robinson, O. A systematic review of metabolomic studies of childhood obesity: State of the evidence for metabolic determinants and consequences. Obes. Rev. 2021, e13384. [Google Scholar] [CrossRef] [PubMed]
- Fuschillo, S.; Paris, D.; Tramice, A.; Ambrosino, P.; Palomba, L.; Maniscalco, M.; Motta, A. Metabolomic profiling of exhaled breath condensate and plasma/serum in chronic obstructive pulmonary disease. Curr. Med. Chem. 2021. Epub Ahead of Print. [Google Scholar] [CrossRef]
- Esther, C.R., Jr.; O’Neal, W.K.; Anderson, W.H.; Kesimer, M.; Ceppe, A.; Doerschuk, C.M.; Alexis, N.E.; Hastie, A.T.; Barr, R.G.; Bowler, R.P.; et al. SPIROMICS. Identification of sputum biomarkers predictive of pulmonary exacerbations in chronic obstructive pulmonary disease. Chest 2021, in press. [Google Scholar]
- Choudhury, P.; Bhattacharya, A.; Dasgupta, S.; Ghosh, N.; Senpupta, S.; Joshi, M.; Bhattacharyya, P.; Chaudhury, K. Identification of novel metabolic signatures potentially involved in the pathogenesis of COPD associated pulmonary hypertension. Metabolomics 2021, 17, 94. [Google Scholar] [CrossRef]
- Lin, B.M.; Zhang, Y.; Yu, B.; Boerwinkle, E.; Thygarajan, B.; Yunes, M.; Daviglus, M.L.; Qi, Q.; Kaplan, R.; Lash, J.; et al. Metabolome-wide association study of estimated glomerular filtration rates in Hispanics. Kidney Int. 2021, 101, 144–151. [Google Scholar] [CrossRef]
- Hameed, A.; Mojsak, P.; Buczynska, A.; Suleria, H.A.R.; Kretowski, A.; Ciborowski, M. Altered metabolome of lipids and amino acids species: A source of early signature biomarkers of T2DM. J. Clin. Med. 2020, 9, 2257. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.Z.; Gerszten, R.E. Metabolomics and proteomics in type 2 diabetes. Circ. Res. 2020, 126, 1613–1627. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.; Shah, S.H.; Corwin, E.J.; Fiehn, O.; Fitzgerald, R.L.; Gerszten, R.E.; Illig, T.; Rhee, E.P.; Srinivas, P.R.; Wang, T.J.; et al. Potential impact and study considerations of metabolomics in cardiovascular health and disease: A scientific statement from the American Heart Association. Circ. Cardiovasc. Genet. 2017, 10, e000032. [Google Scholar] [CrossRef] [PubMed]
- Ashrafian, H.; Sounderajah, V.; Glen, R.; Ebbels, T.; Blaise, B.J.; Kalra, D.; Kultima, K.; Spjuth, O.; Tenori, L.; Salek, R.M.; et al. Metabolomics: The Stethoscope for the Twenty-First Century. Med Princ. Pract. 2021, 30, 301–310. [Google Scholar] [CrossRef]
- Schmidt, D.R.; Patel, R.; Kirsch, D.G.; Lewis, C.A.; Heiden, M.G.V.; Locasale, J.W. Metabolomics in cancer research and emerging applications in clinical oncology. CA Cancer J. Clin. 2021, 71, 333–358. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).