
Decreased Platelet Specific Receptor Expression of P-Selectin and GPIIb/IIIa Predict Future Non-Surgical Bleeding in Patients after Left Ventricular Assist Device Implantation
 , ,
, ,
Abstract
1. Introduction
2. Results
2.1. Patient Characteristics
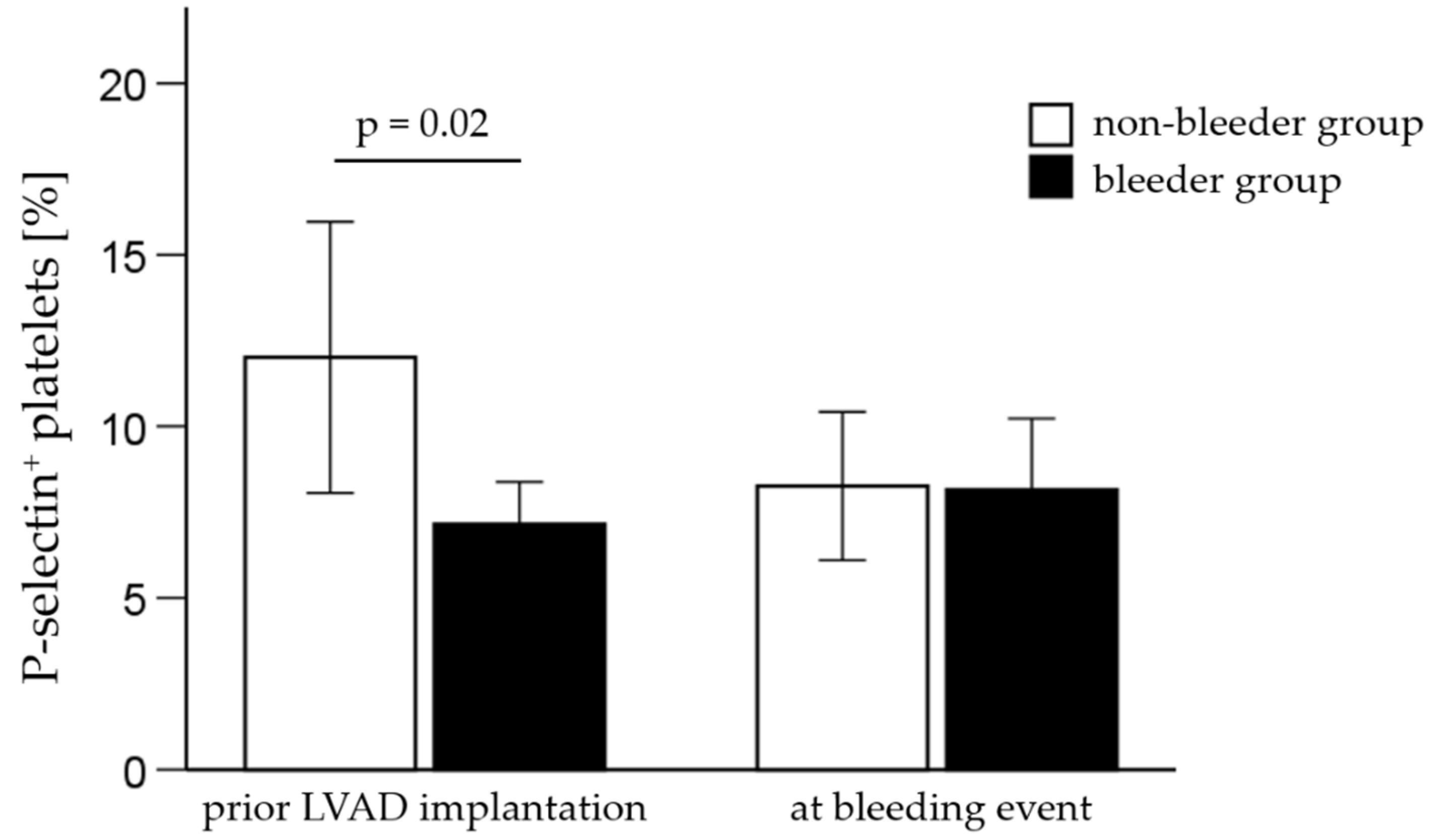
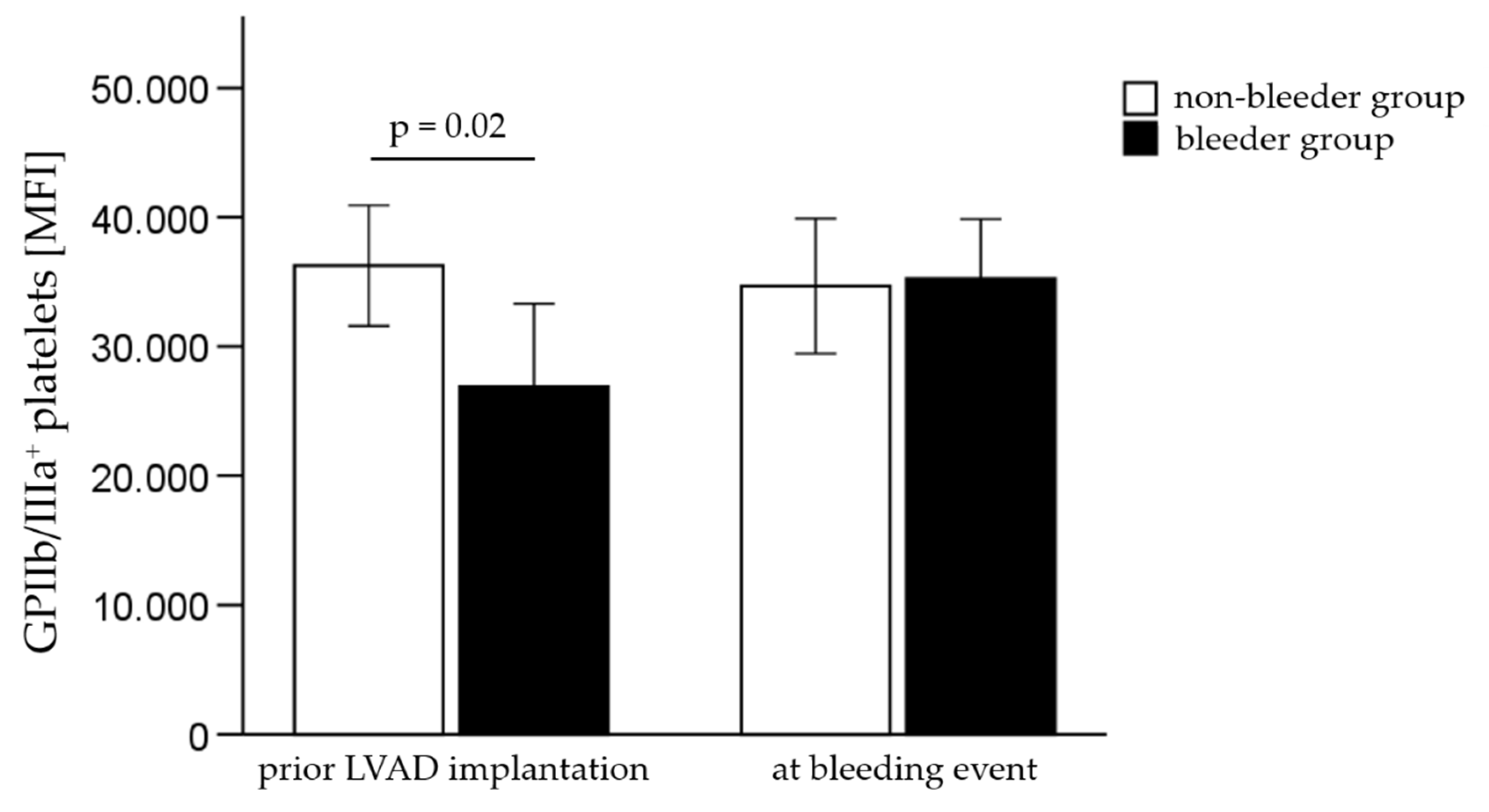
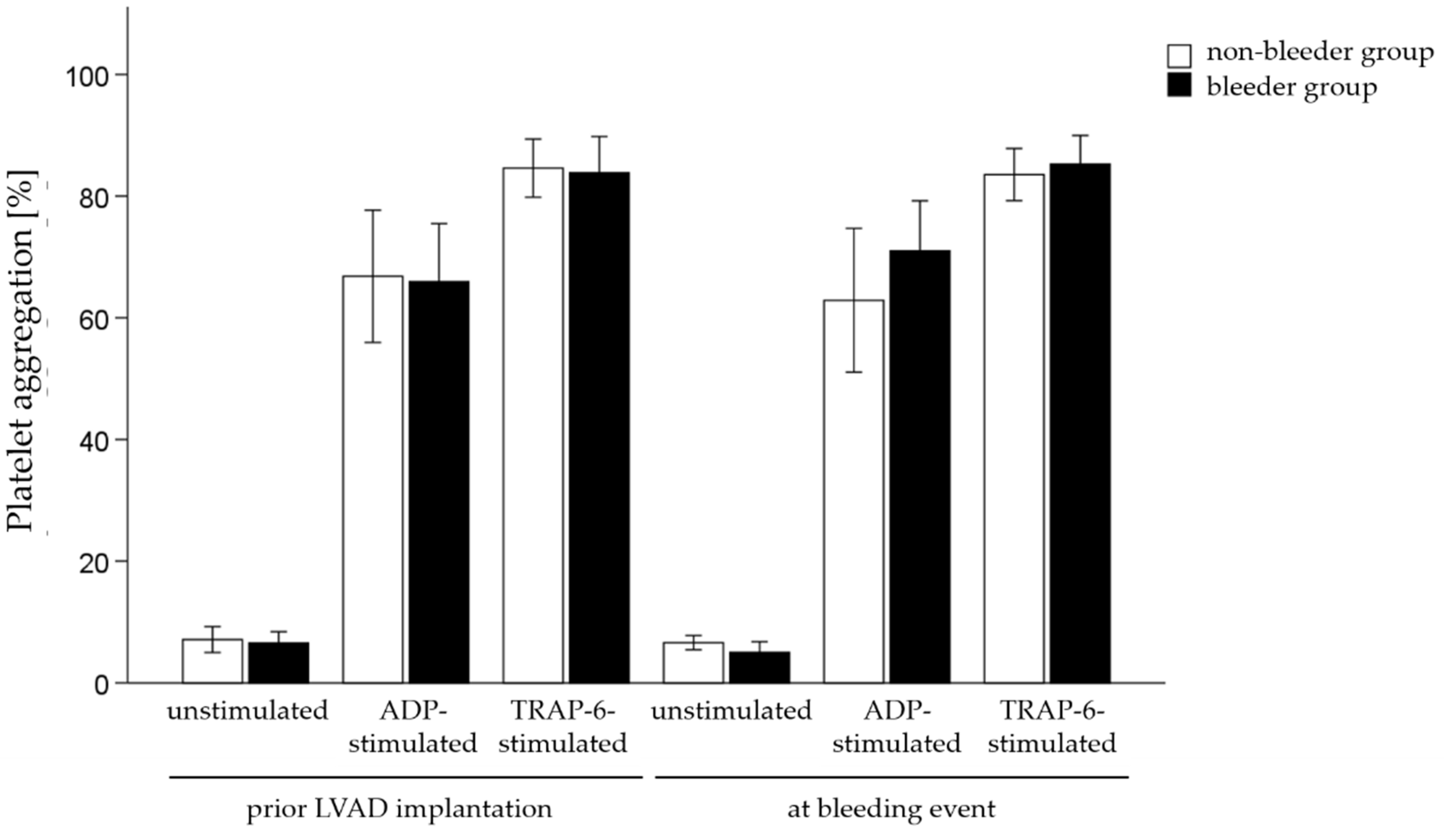
2.2. Analysis of Platelet Receptor Expression and Platelet Aggregation Measurements
2.3. Analysis of Intra-Platelet Oxidative Stress Level
2.4. Serum Analysis of VEGF Expression and Soluble P-Selectin
3. Discussion
4. Materials and Methods
4.1. Study Groups and Clinical Characteristics
4.2. Blood Sampling
4.3. Flow Cytometry
4.4. Platelet Aggregation Measurements
4.5. Elisa
4.6. Statistics
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bhagra, S.K.; Pettit, S.; Parameshwar, J. Implantable left ventricular assist device: Indications, eligibility and current outcomes. Heart 2022, 108, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Pourtau, L.; Beneyto, M.; Porterie, J.; Roncalli, J.; Massot, M.; Biendel, C.; Fournier, P.; Itier, R.; Galinier, M.; Lairez, O.; et al. Prevalence, management, and outcomes of haemorrhagic events in left ventricular assist device recipients. ESC Heart Fail. 2022, 9, 1931–1941. [Google Scholar] [CrossRef] [PubMed]
- Veasey, T.M.; Floroff, C.K.; Strout, S.E.; McElray, K.L.; Brisco-Bacik, M.A.; Cook, J.L.; Toole, J.M.; Craig, M.L.; Van Bakel, A.B.; Meadows, H.B.; et al. Evaluation of anticoagulation and nonsurgical major bleeding in recipients of continuous-flow left ventricular assist devices. Artif. Organs. 2019, 43, 736–744. [Google Scholar] [CrossRef] [PubMed]
- Muthiah, K.; Connor, D.; Ly, K.; Gardiner, E.E.; Andrews, R.K.; Qiao, J.; Rutgers, D.; Robson, D.; Low, J.; Jarvis, S.; et al. Longitudinal changes in hemostatic parameters and reduced pulsatility contribute to non-surgical bleeding in patients with centrifugal continuous-flow left ventricular assist devices. J. Heart Lung Transplant. 2016, 35, 743–751. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.; Bittner, K.; Bartell, N.; Aranez, J.; Alexis, J.D.; Carlson, B.; Chen, L.; McNitt, S.; Kothari, T.; Kaul, V.; et al. Outcomes of gastrointestinal bleeding in patients with left ventricular assist devices: A tertiary care experience. Endosc. Int. Open 2020, 8, E301–E309. [Google Scholar] [CrossRef]
- Arias, K.; Sun, W.; Wang, S.; Sorensen, E.N.; Feller, E.; Kaczorowski, D.; Griffith, B.; Wu, Z.J. Acquired platelet defects are responsible for non-surgical bleeding in left ventricular assist device recipients. Artif. Organs. 2022. [Google Scholar] [CrossRef]
- Hennessy-Strahs, S.; Kang, J.; Krause, E.; Dowling, R.D.; Rame, J.E.; Bartoli, C.R. Patient-specific severity of von Willebrand factor degradation identifies patients with a left ventricular assist device at high risk for bleeding. J. Thorac. Cardiovasc. Surg. 2022. [Google Scholar] [CrossRef]
- Koliopoulou, A.; Selzman, C.H. Stop the LVAD bleeding. J. Thorac. Dis. 2017, 9, E437–E439. [Google Scholar] [CrossRef][Green Version]
- Mondal, N.K.; Chen, Z.; Trivedi, J.R.; Sorensen, E.N.; Pham, S.M.; Slaughter, M.S.; Griffith, B.P.; Wu, Z.J. Association of Oxidative Stress and Platelet Receptor Glycoprotein GPIbα and GPVI Shedding During Nonsurgical Bleeding in Heart Failure Patients with Continuous-Flow Left Ventricular Assist Device Support. ASAIO J. 2018, 64, 462–471. [Google Scholar] [CrossRef]
- Chen, Z.; Mondal, N.K.; Ding, J.; Koenig, S.C.; Slaughter, M.S.; Griffith, B.P.; Wu, Z.J. Activation and shedding of platelet glycoprotein IIb/IIIa under non-physiological shear stress. Mol. Cell Biochem. 2015, 409, 93–101. [Google Scholar] [CrossRef]
- Chen, Z.; Mondal, N.K.; Ding, J.; Koenig, S.C.; Slaughter, M.S.; Wu, Z.J. Paradoxical Effect of Non-Physiological Shear Stress on Platelets and von Willebrand factor. Artif. Organs. 2016, 40, 659–668. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Zhang, J.; Kareem, K.; Tran, D.; Conway, R.G.; Arias, K.; Griffith, B.P.; Wu, Z.J. Device-induced platelet dysfunction in mechanically assisted circulation increases the risks of thrombosis and bleeding. Artif. Organs. 2019, 43, 745–755. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Mondal, N.K.; Sorensen, E.N.; Cai, L.; Fang, H.B.; Griffith, B.P.; Wu, Z.J. Platelet glycoprotein Ibα ectodomain shedding and non-surgical bleeding in heart failure patients supported by continuous-flow left ventricular assist devices. J. Heart Lung Transplant. 2014, 33, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Klaeske, K.; Dieterlen, M.-T.; Eifert, S.; Scholz, U.; Garbade, J.; Jawad, K.; Sieg, F.; Borger, M.A.; Meyer, A.L. Device-induced platelet dysfunction in patients after left ventricular assist device implantation. J. Thromb. Haemost. 2021, 19, 1331–1341. [Google Scholar] [CrossRef]
- Mehra, M.R. The burden of haemocompatibility with left ventricular assist systems: A complex weave. Eur. Heart J. 2019, 40, 673–677. [Google Scholar] [CrossRef]
- Youmans, Q.R.; Zhou, A.; Harap, R.; Eskender, M.H.; Anderson, A.S.; Ezema, A.U.; Ghafourian, K.; Ohiomoba, R.; Pham, D.T.; Rich, J.D.; et al. Association of cigarette smoking and adverse events in left ventricular assist device patients. Int. J. Artif. Organs. 2021, 44, 181–187. [Google Scholar] [CrossRef]
- Shah, P.; Tantry, U.S.; Bliden, K.P.; Gurbel, P.A. Bleeding and thrombosis associated with ventricular assist device therapy. J. Heart Lung Transplant. 2017, 36, 1164–1173. [Google Scholar] [CrossRef]
- Gurvits, G.E.; Fradkov, E. Bleeding with the artificial heart: Gastrointestinal hemorrhage in CF-LVAD patients. World J. Gastroenterol. 2017, 23, 3945–3953. [Google Scholar] [CrossRef]
- Malik, S.; Malik, S.A.; Ulmer, L.L.; Jha, L.K.; Strupp, M.S.; Raichlin, E.; Lyden, E.R.; Hewlett, A.T. Gastrointestinal Bleeding With Left Ventricular Assist Devices (LVAD): Locating the Leak and Identifying Outcomes. J. Clin. Gastroenterol. 2019, 53, e202–e207. [Google Scholar] [CrossRef]
- Kanwar, M.K.; Pagani, F.D.; Mehra, M.R.; Estep, J.D.; Pinney, S.P.; Silvestry, S.C.; Uriel, N.; Goldstein, D.J.; Long, J.; Cleveland, J.C., Jr.; et al. Center Variability in Patient Outcomes Following HeartMate 3 Implantation: An Analysis of the MOMENTUM 3 Trial. J. Card. Fail. 2022, 28, 1158–1168. [Google Scholar] [CrossRef]
- Kapuria, D.; Khumri, T.; Shamim, S.; Surana, P.; Khan, S.; Al-Khalisi, N.; Aggarwal, S.; Koh, C.; Chhabra, R. Characterization and timing of gastrointestinal bleeding in continuous flow left ventricular assist device recipients. Heliyon 2020, 6, e04695. [Google Scholar] [CrossRef] [PubMed]
- Leebeek, F.W.G.; Muslem, R. Bleeding in critical care associated with left ventricular assist devices: Pathophysiology, symptoms, and management. Hematol. Am. Soc. Hematol. Educ. Program. 2019, 2019, 88–96. [Google Scholar] [CrossRef]
- Cochrane, J.; Jackson, C.; Schlepp, G.; Strong, R. Gastrointestinal angiodysplasia is associated with significant gastrointestinal bleeding in patients with continuous left ventricular assist devices. Endosc. Int. Open 2016, 4, E371–E377. [Google Scholar] [CrossRef] [PubMed]
- Meyer, A.L.; Malehsa, D.; Budde, U.; Bara, C.; Haverich, A.; Strueber, M. Acquired von Willebrand syndrome in patients with a centrifugal or axial continuous flow left ventricular assist device. JACC Heart Fail. 2014, 2, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Uriel, N.; Pak, S.W.; Jorde, U.P.; Jude, B.; Susen, S.; Vincentelli, A.; Ennezat, P.V.; Cappleman, S.; Naka, Y.; Mancini, D. Acquired von Willebrand syndrome after continuous-flow mechanical device support contributes to a high prevalence of bleeding during long-term support and at the time of transplantation. J. Am. Coll. Cardiol. 2010, 56, 1207–1213. [Google Scholar] [CrossRef]
- Slaughter, M.S. Hematologic effects of continuous flow left ventricular assist devices. J. Cardiovasc. Transl. Res. 2010, 3, 618–624. [Google Scholar] [CrossRef]
- Crow, S.; Chen, D.; Milano, C.; Thomas, W.; Joyce, L.; Piacentino, V., 3rd; Sharma, R.; Wu, J.; Arepally, G.; Bowles, D.; et al. Acquired von Willebrand syndrome in continuous-flow ventricular assist device recipients. Ann. Thorac. Surg. 2010, 90, 1263–1269. [Google Scholar] [CrossRef]
- Kalbhenn, J.; Schlagenhauf, A.; Rosenfelder, S.; Schmutz, A.; Zieger, B. Acquired von Willebrand syndrome and impaired platelet function during venovenous extracorporeal membrane oxygenation: Rapid onset and fast recovery. J. Heart Lung Transplant. 2018, 37, 985–991. [Google Scholar] [CrossRef]
- Geisen, U.; Brehm, K.; Trummer, G.; Berchtold-Herz, M.; Heilmann, C.; Beyersdorf, F.; Schelling, J.; Schlagenhauf, A.; Zieger, B. Platelet secretion defects and acquired von Willebrand syndrome in patients with ventricular assist devices. J. Am. Heart Assoc. 2018, 7, e006519. [Google Scholar] [CrossRef]
- Portier, I.; Campbell, R.A. Role of platelets in detection and regulation of infection. Arterioscler. Thromb. Vasc. Biol. 2021, 41, 70–78. [Google Scholar] [CrossRef]
- Caruso, R.; Verde, A.; Campolo, J.; Milazzo, F.; Russo, C.; Boroni, C.; Parolini, M.; Trunfio, S.; Paino, R.; Martinelli, L.; et al. Severity of oxidative stress and inflammatory activation in end-stage heart failure patients are unaltered after 1 month of left ventricular mechanical assistance. Cytokine 2012, 59, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Doherty, E.; Perl, A. Measurement of Mitochondrial Mass by Flow Cytometry during Oxidative Stress. React. Oxyg. Species 2017, 4, 275–283. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Bleeders | Non-Bleeders | p-Value |
|---|---|---|---|
| (n = 18) | (n = 18) | ||
| Body mass index (kg/m2) | 28.0 ± 4.7 | 27.0 ± 4.9 | 0.52 |
| Blood type | 0.79 | ||
| A | 8 (44%) | 9 (50%) | |
| B | 1 (6%) | 1 (6%) | |
| AB | 1 (6%) | 0 (0%) | |
| O | 8 (44%) | 8 (44%) | |
| Etiology of heart disease | 0.18 | ||
| NICM | 6 (33%) | 11 (61%) | |
| ICM | 12 (67%) | 7 (39%) | |
| LVEF | |||
| 30–40% | 1 (6%) | 1 (6%) | 1.00 |
| <30% | 17 (94%) | 17 (94%) | 1.00 |
| Comorbidities | |||
| hypertension | 14 (78%) | 18 (100%) | 0.1 |
| diabetes mellitus type 2 | 10 (56%) | 7 (39%) | 0.51 |
| myocardial infraction | 5 (28%) | 2 (11%) | 0.4 |
| chronic kidney disease | 13 (72%) | 9 (50%) | 0.31 |
| hyperproteinemia | 11 (61%) | 6 (33%) | 0.18 |
| Smoking | 0.72 | ||
| current | 3 (17%) | 4 (22%) | |
| former | 10 (56%) | 7 (39%) | |
| never | 2 (11%) | 4 (22%) | |
| unknown | 3 (17%) | 3 (17%) | |
| Alcohol abuse | 0.71 | ||
| current | 1 (6%) | 1 (6%) | |
| former | 3 (17%) | 6 (33%) | |
| never | 10 (56%) | 8 (44%) | |
| unknown | 4 (22%) | 3 (17%) | |
| NYHA classification | 0.18 | ||
| class III | 8 (44%) | 12 (67%) | |
| class IV | 10 (56%) | 5 (28%) | |
| Device strategy | 0.51 | ||
| DT | 10 (55%) | 8 (45%) | |
| BTT | 5 (28%) | 4 (22%) | |
| BTD/BTC | 3 (17%) | 6 (33%) | |
| Implanted LVAD type | 1.00 | ||
| HM 3 | 15 (83%) | 16 (89%) | |
| HVAD | 3 (17%) | 2 (11%) | |
| Pump characteristics | |||
| pump speed )rpm) | 4889 ± 1091 | 4800 ± 855 | 0.79 |
| pump flow (L/min) | 4.1 ± 0.6 | 3.9 ± 0.4 | 0.17 |
| pump power (W) | 3.9 ± 0.6 | 3.6 ± 0.3 | 0.02 |
| Anticoagulation | |||
| phenprocoumon | 18 (100%) | 18 (100%) | 1.00 |
| clopidogrel | 1 (6%) | 2 (11%) | 1.00 |
| acetylsalicylic acid | 15 (83%) | 16 (89%) | 1.00 |
| Hospitalization after LVAD implantation (d) | 56 ± 34 | 48 ± 16 | 0.38 |
| Re-hospitalization | 12 (67%) | 12 (67%) | 1.00 |
| Bleeders | Non-Bleeders | p-Value | |
|---|---|---|---|
| (n = 18) | (n = 18) | ||
| Thromboembolic event prior LVAD implantation | |||
| thrombosis | 8 (44%) | 6 (33%) | 0.73 |
| ischemic stroke | 8 (44%) | 6 (33%) | 0.73 |
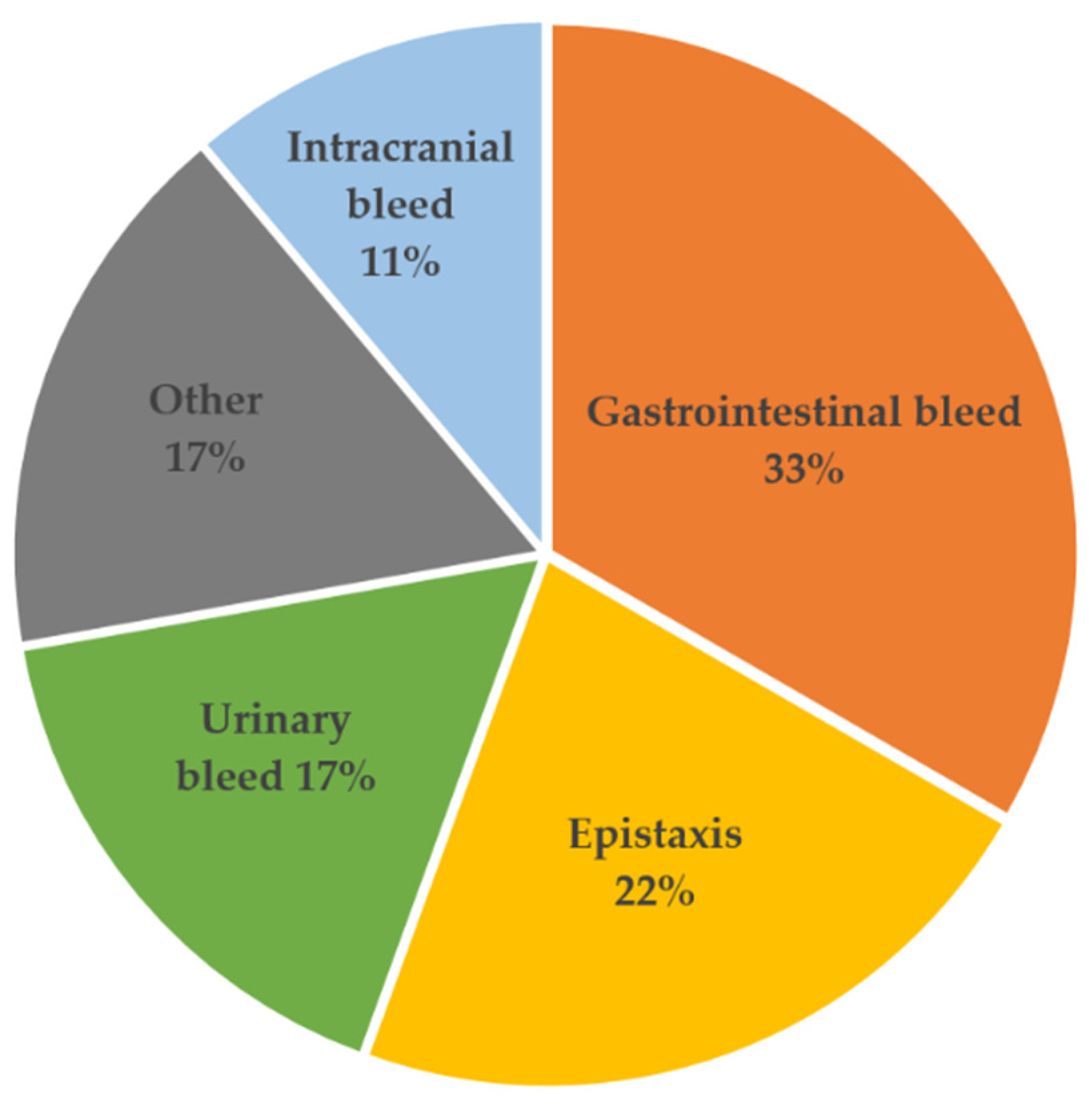
| Hemorrhagic events after LVAD implantation * | - | ||
| Gastrointestinal tract | 6 (33%) | - | |
| Vascular (epistaxis) | 4 (22%) | - | |
| Intracranial | 2 (11%) | - | |
| Urinary tract (hematuria) | 3 (17%) | - | |
| other (hematoma) | 3 (17%) | - | |
| Thromboembolic event after LVAD implantation * | |||
| thrombosis | 3 (17%) | 1 (6%) | 0.6 |
| ischemic stroke | 0 (0%) | 3 (17%) | 0.23 |
| Patient | Bleeding Site | Symptoms | GI Procedure | Minor/Major | Days Post-Implant |
|---|---|---|---|---|---|
| 1 | GI | Rectal hemorrhage, melena | no | major | 93 |
| 2 | other / intramyocardial | hematoma | no | minor | 9 |
| 3 | GI | melena, Forrest 1b | yes | major | 22 |
| 4 | vascular | epistaxis | no | minor | 233 |
| 5 | vascular | epistaxis | no | minor | 55 |
| 6 | GI | melena | no | major | 69 |
| 7 | GI | melena | no | major | 29 |
| 8 | GI | melena, Forrest 1a | yes | major | 128 |
| 9 | vascular | epistaxis | no | minor | 144 |
| 10 | other/abdominal | retroperitoneal hematoma | no | major | 18 |
| 11 | other/skin | hematoma | no | minor | 16 |
| 12 | intracranial | subdural hematoma | no | major | 9 |
| 13 | intracranial | subarachnoid hemorrhage | no | major | 4 |
| 14 | GI | Forrest 1b | yes | major | 26 |
| 15 | Urinary tract | hematuria | yes | major | 112 |
| 16 | vascular | epistaxis | no | minor | 280 |
| 17 | Urinary tract, GI | hematuria, melena | yes | major | 8 |
| 18 | Urinary tract | hematuria | no | minor | 12 |
| Parameter | Bleeders Prior LVAD (n = 18) | Non-Bleeders Prior LVAD (n = 18) | Bleeders at Bleeding Event (n = 18) | p-Value Prior LVAD |
|---|---|---|---|---|
| Erythrocytes (Tpt/L) | 3.6 ± 0.6 | 4.1 ± 0.7 | 3.1 ± 0.8 | 0.02 |
| Hematocrit | 0.31 ± 0.05 | 0.34 ± 0.05 | 0.27 ± 0.07 | 0.13 |
| Hemoglobin (mmol/L) | 6.5 ± 1.0 | 7.3 ± 1.1 | 5.6 ± 1.6 | 0.04 |
| Platelets (Gpt/L) | 225 ± 78 | 253 ± 129 | 282 ± 60 | 0.44 |
| INR | 1.1 ± 0.2 | 1.2 ± 0.4 | 2.1 ± 0.8 | 0.41 |
| Bilirubin (µmol/L) | 15.9 ± 10.8 | 14.6 ± 9.6 | 12.6 ± 9.9 | 0.70 |
| LDH (µmol/(L/s)) | 3.8 ± 1.1 | 5.1 ± 3.7 | 10.9 ± 24.5 | 0.16 |
| aPTT (sec) | 43.3 ± 15.3 | 47.4 ± 13.6 | 60.2 ± 29.1 | 0.41 |
| Parameter. | Bleeders (n = 11) | Non-Bleeders (n = 10) | p-Value |
|---|---|---|---|
| vWF antigen (%) | 186.1 ± 52.0 | 185.7 ± 58.2 | 0.99 |
| vWF activity (%) | 129.1 ± 28.1 | 138.8 ± 37.4 | 0.51 |
| vWF CB activity (%) | 126.4 ± 40.3 | 135.1 ± 44.4 | 0.67 |
| Factor VIII, procoagulant (%) | 195.8 ± 64.0 | 204.2 ± 47.5 | 0.74 |
| Parameter | Bleeders (n = 18) | Non-Bleeders (n = 18) | p-Value |
|---|---|---|---|
| % P-selectin+ platelets | 7.2 ± 2.6 | 12.4 ± 8.1 | 0.02 |
| % GP1bα+ platelets | 88.4 ± 25.5 | 93.4 ± 14.2 | 0.47 |
| % CD63+ platelets | 0.57 ± 0.32 | 3.29 ± 6.14 | 0.08 |
| % GPIIb/IIIa+ platelets | 77.8 ± 42.7 | 94.5 ± 23.6 | 0.16 |
| % DHR123+ platelets | 88.4 ± 9.6 | 84.4 ± 7.7 | 0.17 |
| % MitoTracker Green+ platelets | 30.0 ± 25.2 | 23.5 ± 13.9 | 0.34 |
| MFI P-selectin+ platelets | 1227 ± 354 | 1330 ± 463 | 0.46 |
| MFI GP1bα+ platelets | 930 ± 807 | 674 ± 257 | 0.21 |
| MFI CD63+ platelets | 1544 ± 1169 | 2727 ± 3020 | 0.14 |
| MFI GPIIb/IIIa+ platelets | 26,900 ± 13,608 | 36,259 ± 9913 | 0.02 |
| MFI DHR123+ platelets | 742 ± 435 | 575 ± 285 | 0.18 |
| Parameter | Bleeders (n = 18) | Non-Bleeders (n = 18) | p-Value |
|---|---|---|---|
| % P-selectin+ platelets | 8.15 ± 4.40 | 8.26 ± 4.45 | 0.94 |
| % GP1bα+ platelets | 97.3 ± 1.5 | 97.2 ± 2.2 | 0.95 |
| % CD63+ platelets | 1.37 ± 3.42 | 0.65 ± 0.42 | 0.38 |
| % GPIIb/IIIa+ platelets | 94.5 ± 23.5 | 94.4 ± 23.5 | 1.00 |
| % DHR123+ platelets | 87.1 ± 9.0 | 86.1 ± 11.9 | 0.76 |
| % MitoTracker Green+ platelets | 19.6 ± 17.7 | 17.0 ± 19.8 | 0.68 |
| MFI P-selectin+ platelets | 1342 ± 334 | 1369 ± 334 | 0.81 |
| MFI GP1bα+ platelets | 672 ± 217 | 630 ± 124 | 0.48 |
| MFI CD63+ platelets | 1448 ± 1084 | 1564 ± 914 | 0.73 |
| MFI GPIIb/IIIa+ platelets | 35,240 ± 9806 | 34,676 ± 11,088 | 0.87 |
| MFI DHR123+ platelets | 742 ± 561 | 638 ± 386 | 0.52 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klaeske, K.; Meyer, A.L.; Saeed, D.; Eifert, S.; Jawad, K.; Sieg, F.; Haunschild, J.; Borger, M.A.; Dieterlen, M.-T. Decreased Platelet Specific Receptor Expression of P-Selectin and GPIIb/IIIa Predict Future Non-Surgical Bleeding in Patients after Left Ventricular Assist Device Implantation. Int. J. Mol. Sci. 2022, 23, 10252. https://doi.org/10.3390/ijms231810252
Klaeske K, Meyer AL, Saeed D, Eifert S, Jawad K, Sieg F, Haunschild J, Borger MA, Dieterlen M-T. Decreased Platelet Specific Receptor Expression of P-Selectin and GPIIb/IIIa Predict Future Non-Surgical Bleeding in Patients after Left Ventricular Assist Device Implantation. International Journal of Molecular Sciences. 2022; 23(18):10252. https://doi.org/10.3390/ijms231810252
Chicago/Turabian StyleKlaeske, Kristin, Anna L. Meyer, Diyar Saeed, Sandra Eifert, Khalil Jawad, Franz Sieg, Josephina Haunschild, Michael A. Borger, and Maja-Theresa Dieterlen. 2022. "Decreased Platelet Specific Receptor Expression of P-Selectin and GPIIb/IIIa Predict Future Non-Surgical Bleeding in Patients after Left Ventricular Assist Device Implantation" International Journal of Molecular Sciences 23, no. 18: 10252. https://doi.org/10.3390/ijms231810252
APA StyleKlaeske, K., Meyer, A. L., Saeed, D., Eifert, S., Jawad, K., Sieg, F., Haunschild, J., Borger, M. A., & Dieterlen, M.-T. (2022). Decreased Platelet Specific Receptor Expression of P-Selectin and GPIIb/IIIa Predict Future Non-Surgical Bleeding in Patients after Left Ventricular Assist Device Implantation. International Journal of Molecular Sciences, 23(18), 10252. https://doi.org/10.3390/ijms231810252