
Recent Advances on the Roles of PCSK-9 Inhibitors in the Management of Acute Ischemic Stroke Patients


 ,
,  ,
,
Abstract
:1. Introduction
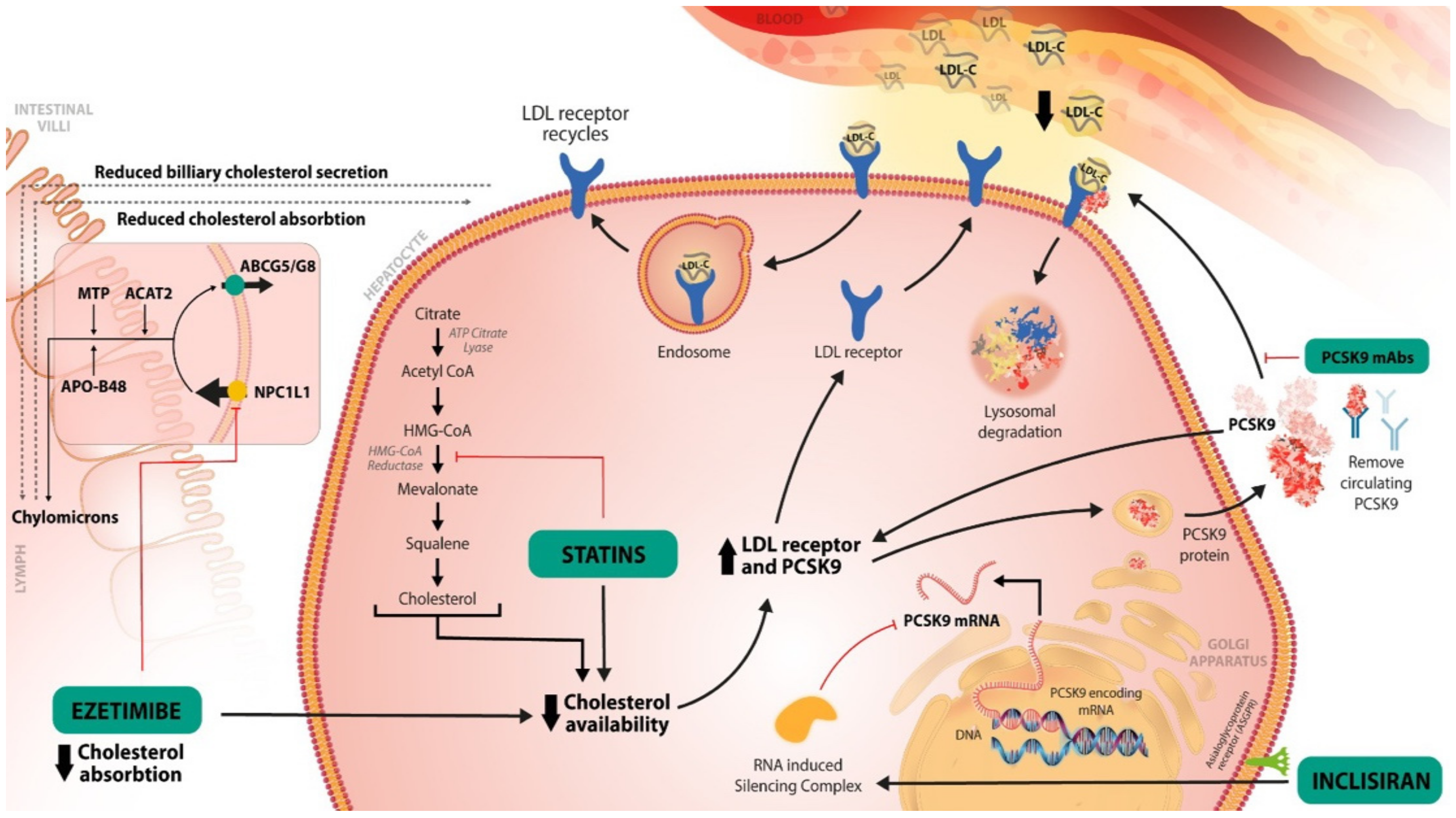
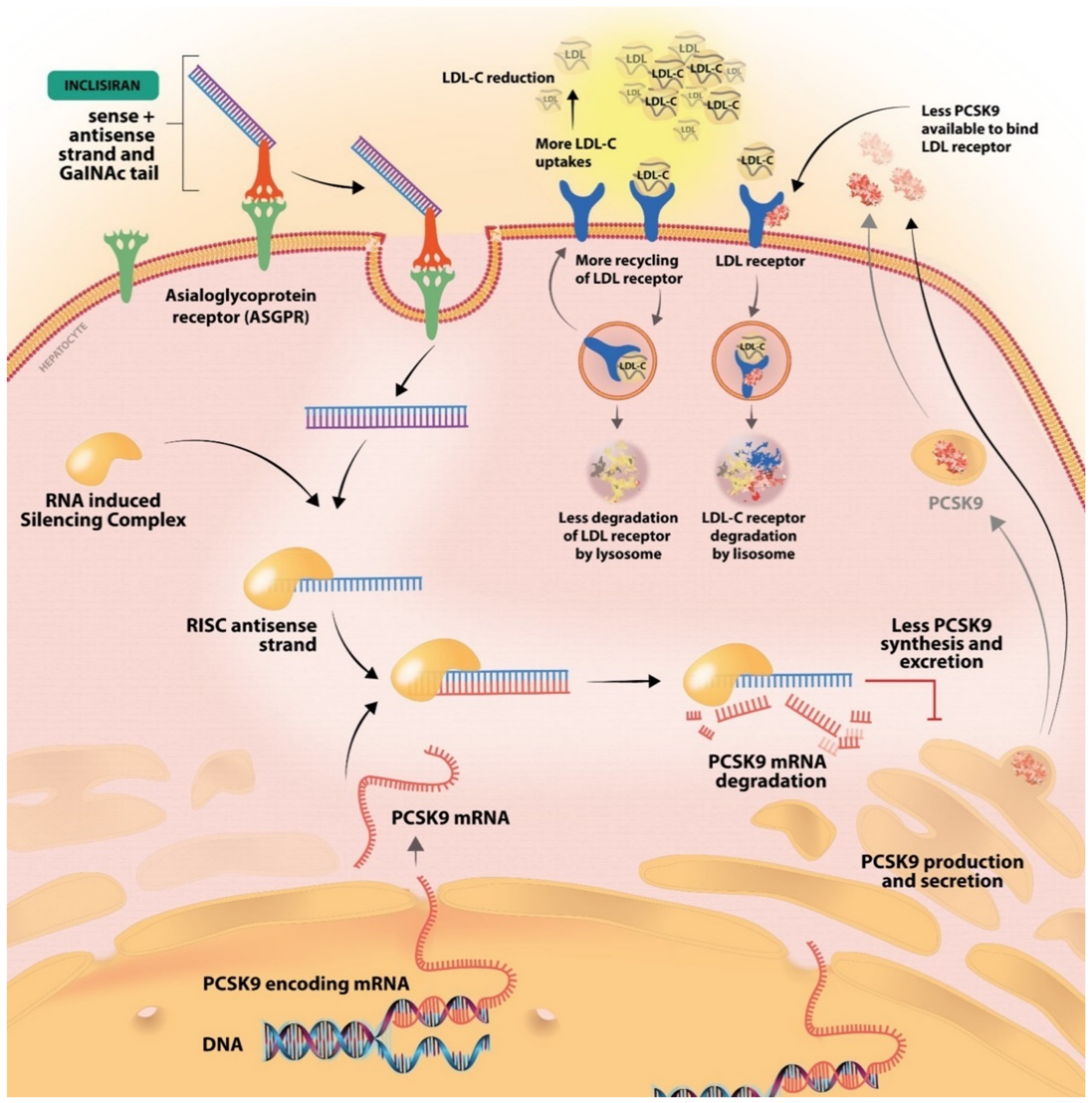
2. Mechanisms of the Hypolipidemic Treatments
3. PCSK-9 Inhibitors in Clinical Practice
4. PCSK-9 Inhibitors in Clinical Trials
5. PCSK-9 Inhibitors and Adverse Reactions
6. Ongoing Clinical Trials Involving PCSK-9 Inhibitors and Future Directions
7. New Approaches for PCSK-9 Inhibition
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart Disease and Stroke Statistics—2022 Update: A Report From the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar] [CrossRef] [PubMed]
- Wafa, H.A.; Wolfe, C.D.; Emmett, E.; Roth, G.A.; Johnson, C.O.; Wang, Y. Burden of Stroke in Europe. Stroke 2020, 51, 2418–2427. [Google Scholar] [CrossRef]
- De Sousa, D.A.; von Martial, R.; Abilleira, S.; Gattringer, T.; Kobayashi, A.; Gallofré, M.; Fazekas, F.; Szikora, I.; Feigin, V.; Caso, V.; et al. Access to and delivery of acute ischaemic stroke treatments: A survey of national scientific societies and stroke experts in 44 European countries. Eur. Stroke J. 2018, 4, 13–28. [Google Scholar] [CrossRef]
- Kleindorfer, D.O.; Towfighi, A.; Chaturvedi, S.; Cockroft, K.M.; Gutierrez, J.; Lombardi-Hill, D.; Kamel, H.; Kernan, W.N.; Kittner, S.J.; Leira, E.C.; et al. 2021 Guideline for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack: A Guideline From the American Heart Association/American Stroke Association. Stroke 2021, 52, e364–e467. [Google Scholar] [CrossRef] [PubMed]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418, Correction in Stroke 2019, 50, e440–e441. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.P., Jr.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E., 3rd. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef]
- Sirimarco, G.; Lavallée, P.C.; Labreuche, J.; Meseguer, E.; Cabrejo, L.; Guidoux, C.; Klein, I.F.; Olivot, J.-M.; Abboud, H.; Adraï, V.; et al. Overlap of Diseases Underlying Ischemic Stroke: The ASCOD Phenotyping. Stroke 2013, 44, 2427–2433. [Google Scholar] [CrossRef]
- Nelson, R.H. Hyperlipidemia as a Risk Factor for Cardiovascular Disease. Prim. Care Clin. Off. Pract. 2012, 40, 195–211. [Google Scholar] [CrossRef]
- Amarenco, P.; Bogousslavsky, J.; Caplan, L.; Donnan, G.; Wolf, M.; Hennerici, M. The ASCOD Phenotyping of Ischemic Stroke (Updated ASCO Phenotyping). Cerebrovasc. Dis. 2013, 36, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Hill, M.F.; Bordoni, B. Hyperlipidemia. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Qin, J.; Liu, L.; Su, X.D.; Wang, B.B.; Fu, B.S.; Cui, J.Z.; Liu, X.Y. The effect of PCSK9 inhibitors on brain stroke prevention: A systematic review and meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 2234–2243. [Google Scholar] [CrossRef]
- Safeer, R.S.; Ugalat, P.S. Cholesterol treatment guidelines update. Am. Fam. Physician 2002, 65, 871–880. [Google Scholar] [PubMed]
- Cleeman, J.I.; Grundy, S.M. National Cholesterol Education Program Recommendations for Cholesterol Testing in Young Adults. Circulation 1997, 95, 1646–1650. [Google Scholar] [CrossRef]
- Grundy, S.M.; Cleeman, J.I.; Bairey Merz, C.N.; Brewer, H.B.; Clark, L.T.; Hunninghake, D.B.; Pasternak, R.C.; Smith, S.C.; Stone, N.J. Implications of Recent Clinical Trials for the National Cholesterol Education Program Adult Treatment Panel III Guidelines. Circulation 2004, 110, 227–239. [Google Scholar] [CrossRef] [PubMed]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur. Heart J. 2019, 41, 111–188. [Google Scholar] [CrossRef]
- Grundy, S.M.; Stone, N.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; De Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 139, e1082–e1143. [Google Scholar] [CrossRef]
- Sizar, O.; Khare, S.; Jamil, R.T.; Talati, R. Statin Medications. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Toth, P.; Phan, B.A.; Dayspring, T. Ezetimibe therapy: Mechanism of action and clinical update. Vasc. Health Risk Manag. 2012, 8, 415–427. [Google Scholar] [CrossRef] [PubMed]
- Dawson, J.; Béjot, Y.; Christensen, L.M.; De Marchis, G.M.; Dichgans, M.; Hagberg, G.; Heldner, M.R.; Milionis, H.; Li, L.; Pezzella, F.R.; et al. European Stroke Organisation (ESO) guideline on pharmacological interventions for long-term secondary prevention after ischaemic stroke or transient ischaemic attack. Eur. Stroke J. 2022, 7, 23969873221100032. [Google Scholar] [CrossRef]
- Seidah, N.G.; Awan, Z.; Chrétien, M.; Mbikay, M. PCSK9: A key modulator of cardiovascular health. Circ. Res. 2014, 114, 1022–1036. [Google Scholar] [CrossRef]
- Handelsman, Y.; Lepor, N.E. PCSK9 Inhibitors in Lipid Management of Patients With Diabetes Mellitus and High Cardiovascular Risk: A Review. J. Am. Heart Assoc. 2018, 7, e008953. [Google Scholar] [CrossRef]
- Sabatine, M.S.; Giugliano, R.P.; Keech, A.C.; Honarpour, N.; Wiviott, S.D.; Murphy, S.A.; Kuder, J.F.; Wang, H.; Liu, T.; Wasserman, S.M.; et al. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N. Engl. J. Med. 2017, 376, 1713–1722. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.G.; Farnier, M.; Krempf, M.; Bergeron, J.; Luc, G.; Averna, M.; Stroes, E.S.; Langslet, G.; Raal, F.J.; El Shahawy, M.; et al. Efficacy and Safety of Alirocumab in Reducing Lipids and Cardiovascular Events. N. Engl. J. Med. 2015, 372, 1489–1499. [Google Scholar] [CrossRef] [PubMed]
- Board, C.; Kelly, M.; Shapiro, M.D.; Dixon, D.L. PCSK9 Inhibitors in Secondary Prevention—An Opportunity for Personalized Therapy. J. Cardiovasc. Pharmacol. 2020, 75, 410–420. [Google Scholar] [CrossRef] [PubMed]
- Dyrbuś, K.; Gąsior, M.; Penson, P.; Ray, K.K.; Banach, M. Inclisiran—New hope in the management of lipid disorders? J. Clin. Lipidol. 2020, 14, 16–27. [Google Scholar] [CrossRef]
- Buhaescu, I.; Izzedine, H. Mevalonate pathway: A review of clinical and therapeutical implications. Clin. Biochem. 2007, 40, 575–584. [Google Scholar] [CrossRef]
- Ward, N.C.; Watts, G.F.; Eckel, R.H. Statin Toxicity. Mechanistic Insights and Clinical Implications. Circ. Res. 2019, 124, 328–350. [Google Scholar] [CrossRef]
- Nutescu, E.A.; Shapiro, N.L. Ezetimibe: A Selective Cholesterol Absorption Inhibitor. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2003, 23, 1463–1474. [Google Scholar] [CrossRef]
- Jia, L.; Betters, J.L.; Yu, L. Niemann-Pick C1-Like 1 (NPC1L1) Protein in Intestinal and Hepatic Cholesterol Transport. Annu. Rev. Physiol. 2011, 73, 239–259. [Google Scholar] [CrossRef]
- Cannon, C.P.; Blazing, M.A.; Giugliano, R.P.; McCagg, A.; White, J.A.; Théroux, P.; Darius, H.; Lewis, B.S.; Ophuis, T.O.; Jukema, J.W.; et al. Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes. N. Engl. J. Med. 2015, 372, 2387–2397. [Google Scholar] [CrossRef]
- Amarenco, P.; Kim, J.S.; Labreuche, J.; Charles, H.; Abtan, J.; Béjot, Y.; Cabrejo, L.; Cha, J.-K.; Ducrocq, G.; Giroud, M.; et al. A Comparison of Two LDL Cholesterol Targets after Ischemic Stroke. N. Engl. J. Med. 2020, 382, 9–19. [Google Scholar] [CrossRef]
- Cariou, B.; Le May, C.; Costet, P. Clinical aspects of PCSK9. Atherosclerosis 2011, 216, 258–265. [Google Scholar] [CrossRef]
- Roth, E.M.; Davidson, M.H. PCSK9 Inhibitors: Mechanism of Action, Efficacy, and Safety. Rev. Cardiovasc. Med. 2018, 19, 31–46. [Google Scholar] [CrossRef]
- Gil-Núñez, A.; Masjuan, J.; Montaner, J.; Castellanos, M.; Segura, T.; Cardona, P.; Tembl, J.; Purroy, F.; Arenillas, J.; Palacio, E. Proprotein convertase subtilisin/kexin type 9 inhibitors in secondary prevention of vascular events in patients with stroke: Consensus document and practice guidance. Neurologia 2021, 37, 136–150. [Google Scholar] [CrossRef]
- Lamb, Y.N. Inclisiran: First Approval. Drugs 2021, 81, 389–395, Erratum in 2021, 81, 1129. [Google Scholar] [CrossRef]
- FDA Update: Inclisiran Approved as Add-On Therapy to Reduce LDL-C in High-Risk Adults. Available online: https://www.acc.org/Latest-in-Cardiology/Articles/2022/01/12/15/21/http%3a%2f%2fwww.acc.org%2fLatest-in-Cardiology%2fArticles%2f2022%2f01%2f12%2f15%2f21%2fFDA-Update-Inclisiran-Approved-as-Add-On-Therapy-to-Reduce-LDL-C-in-High-Risk-Adults (accessed on 5 August 2022).
- Alshaer, W.; Zureigat, H.; Al Karaki, A.; Al-Kadash, A.; Gharaibeh, L.; Hatmal, M.M.; Aljabali, A.A.; Awidi, A. siRNA: Mechanism of action, challenges, and therapeutic approaches. Eur. J. Pharmacol. 2021, 905, 174178. [Google Scholar] [CrossRef]
- German, C.A.; Shapiro, M.D. Small Interfering RNA Therapeutic Inclisiran: A New Approach to Targeting PCSK9. BioDrugs Clin. Immunother. Biopharm. Gene Ther. 2019, 34, 1–9. [Google Scholar] [CrossRef]
- Fitzgerald, K.; White, S.; Borodovsky, A.; Bettencourt, B.R.; Strahs, A.; Clausen, V.; Wijngaard, P.; Horton, J.D.; Taubel, J.; Brooks, A.; et al. A Highly Durable RNAi Therapeutic Inhibitor of PCSK9. N. Engl. J. Med. 2017, 376, 41–51. [Google Scholar] [CrossRef]
- Nair, J.K.; Willoughby, J.L.S.; Chan, A.; Charisse, K.; Alam, R.; Wang, Q.; Hoekstra, M.; Kandasamy, P.; Kel’In, A.V.; Milstein, S.; et al. Multivalent N-Acetylgalactosamine-Conjugated siRNA Localizes in Hepatocytes and Elicits Robust RNAi-Mediated Gene Silencing. J. Am. Chem. Soc. 2014, 136, 16958–16961. [Google Scholar] [CrossRef]
- Susan-Resiga, D.; Girard, E.; Essalmani, R.; Roubtsova, A.; Marcinkiewicz, J.; Derbali, R.M.; Evagelidis, A.; Byun, J.H.; Lebeau, P.F.; Austin, R.C.; et al. Asialoglycoprotein receptor 1 is a novel PCSK9-independent ligand of liver LDLR cleaved by furin. J. Biol. Chem. 2021, 297, 101177. [Google Scholar] [CrossRef]
- Henney, N.C.; Banach, M.; Penson, P.E. RNA Silencing in the Management of Dyslipidemias. Curr. Atheroscler. Rep. 2021, 23, 69. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. FDA Approves Add-On Drug for Ages 10 & Up with Rare Forms of High Cholesterol; FDA: Silver Spring, MD, USA, 2021.
- U.S. Food and Drug Administration. FDA Approves Add-On Therapy for Patients with Genetic Form of Severely High Cholesterol; FDA: Silver Spring, MD, USA, 2021.
- Ferri, N.; Corsini, A.; Sirtori, C.R.; Ruscica, M. Bococizumab for the treatment of hypercholesterolaemia. Expert Opin. Biol. Ther. 2016, 17, 237–243. [Google Scholar] [CrossRef] [Green Version]
- U.S. Food and Drug Administration. FDA Approves Add-On Therapy to Lower Cholesterol among Certain High-Risk Adults; FDA: Silver Spring, MD, USA, 2021.
- EMA Repatha. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/repatha (accessed on 4 August 2022).
- Sabatine, M.S.; Giugliano, R.P.; Wiviott, S.D.; Raal, F.J.; Blom, D.J.; Robinson, J.; Ballantyne, C.M.; Somaratne, R.; Legg, J.; Wasserman, S.M.; et al. Efficacy and Safety of Evolocumab in Reducing Lipids and Cardiovascular Events. N. Engl. J. Med. 2015, 372, 1500–1509. [Google Scholar] [CrossRef] [PubMed]
- EMA Praluent. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/praluent (accessed on 4 August 2022).
- EMA Leqvio. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/leqvio (accessed on 4 August 2022).
- Ray, K.K.; Landmesser, U.; Leiter, L.A.; Kallend, D.; Dufour, R.; Karakas, M.; Hall, T.; Troquay, R.P.; Turner, T.; Visseren, F.L.; et al. Inclisiran in Patients at High Cardiovascular Risk with Elevated LDL Cholesterol. N. Engl. J. Med. 2017, 376, 1430–1440. [Google Scholar] [CrossRef] [PubMed]
- Raedler, L.A. Praluent (Alirocumab): First PCSK9 Inhibitor Approved by the FDA for Hypercholesterolemia. Am. Health Drug Benefits 2016, 9, 123–126. [Google Scholar]
- Jukema, J.W.; Zijlstra, L.E.; Bhatt, D.L.; Bittner, V.A.; Diaz, R.; Drexel, H.; Goodman, S.G.; Kim, Y.-U.; Pordy, R.; Reiner, Ž.; et al. Effect of Alirocumab on Stroke in ODYSSEY OUTCOMES. Circulation 2019, 140, 2054–2062. [Google Scholar] [CrossRef]
- Szarek, M.; White, H.D.; Schwartz, G.G.; Alings, M.; Bhatt, D.L.; Bittner, V.A.; Chiang, C.-E.; Diaz, R.; Edelberg, J.M.; Goodman, S.G.; et al. Alirocumab Reduces Total Nonfatal Cardiovascular and Fatal Events: The ODYSSEY OUTCOMES Trial. J. Am. Coll. Cardiol. 2018, 73, 387–396. [Google Scholar] [CrossRef]
- Giugliano, R.P.; Pedersen, T.R.; Saver, J.L.; Sever, P.S.; Keech, A.C.; Bohula, E.A.; Murphy, S.A.; Wasserman, S.M.; Honarpour, N.; Wang, H.; et al. Stroke Prevention With the PCSK9 (Proprotein Convertase Subtilisin-Kexin Type 9) Inhibitor Evolocumab Added to Statin in High-Risk Patients With Stable Atherosclerosis. Stroke 2020, 51, 1546–1554. [Google Scholar] [CrossRef]
- Oyama, K.; Giugliano, R.P.; Tang, M.; Bonaca, M.P.; Saver, J.L.; Murphy, S.A.; Ruzza, A.; Keech, A.C.; Sever, P.S.; Sabatine, M.S.; et al. Effect of evolocumab on acute arterial events across all vascular territories: Results from the FOURIER trial. Eur. Heart J. 2021, 42, 4821–4829. [Google Scholar] [CrossRef]
- Koba, S.; Inoue, I.; Cyrille, M.; Lu, C.; Inomata, H.; Shimauchi, J.; Kajinami, K. Evolocumab vs. Ezetimibe in Statin-Intolerant Hyperlipidemic Japanese Patients: Phase 3 GAUSS-4 Trial. J. Atheroscler. Thromb. 2020, 27, 471–484. [Google Scholar] [CrossRef]
- Koren, M.J.; Sabatine, M.S.; Giugliano, R.P.; Langslet, G.; Wiviott, S.D.; Ruzza, A.; Ma, Y.; Hamer, A.W.; Wasserman, S.M.; Raal, F.J. Long-Term Efficacy and Safety of Evolocumab in Patients With Hypercholesterolemia. J. Am. Coll. Cardiol. 2019, 74, 2132–2146. [Google Scholar] [CrossRef]
- Nicholls, S.J.; Puri, R.; Anderson, T.; Ballantyne, C.M.; Cho, L.; Kastelein, J.J.; Koenig, W.; Somaratne, R.; Kassahun, H.; Yang, J.; et al. Effect of Evolocumab on Coronary Plaque Composition. J. Am. Coll. Cardiol. 2018, 72, 2012–2021. [Google Scholar] [CrossRef]
- Sever, P.; Gouni-Berthold, I.; Keech, A.; Giugliano, R.; Pedersen, T.R.; Im, K.; Wang, H.; Knusel, B.; Sabatine, M.S.; O’Donoghue, M.L. LDL-cholesterol lowering with evolocumab, and outcomes according to age and sex in patients in the FOURIER Trial. Eur. J. Prev. Cardiol. 2020, 28, 805–812. [Google Scholar] [CrossRef] [PubMed]
- Alhajri, L.; Alhadhrami, A.; Almheiri, S.; Almutawa, Y.; Alhashimi, Z. The efficacy of evolocumab in the management of hyperlipidemia: A systematic review. Ther. Adv. Cardiovasc. Dis. 2017, 11, 155–169. [Google Scholar] [CrossRef] [PubMed]
- Toth, P.P.; Sattar, N.; Blom, D.J.; Martin, S.S.; Jones, S.R.; Monsalvo, M.L.; Elliott, M.; Davis, M.; Somaratne, R.; Preiss, D. Effect of Evolocumab on Lipoprotein Particles. Am. J. Cardiol. 2017, 121, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Toth, P.P.; Worthy, G.; Gandra, S.R.; Sattar, N.; Bray, S.; Cheng, L.; Bridges, I.; Worth, G.M.; Dent, R.; Forbes, C.A.; et al. Systematic Review and Network Meta-Analysis on the Efficacy of Evolocumab and Other Therapies for the Management of Lipid Levels in Hyperlipidemia. J. Am. Heart Assoc. 2017, 6, e005367. [Google Scholar] [CrossRef]
- Daviglus, M.L.; Ferdinand, K.C.; López, J.A.G.; Wu, Y.; Monsalvo, M.L.; Rodriguez, C.J. Effects of Evolocumab on Low-Density Lipoprotein Cholesterol, Non–High Density Lipoprotein Cholesterol, Apolipoprotein B, and Lipoprotein(a) by Race and Ethnicity: A Meta-Analysis of Individual Participant Data From Double-Blind and Open-Label Extension Studies. J. Am. Heart Assoc. 2021, 10, e016839. [Google Scholar] [CrossRef] [PubMed]
- Talasaz, A.H.; Ho, A.C.; Bhatty, F.; Koenig, R.A.; Dixon, D.L.; Baker, W.L.; Van Tassell, B.W. Meta-analysis of clinical outcomes of PCSK9 modulators in patients with established ASCVD. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2021, 41, 1009–1023. [Google Scholar] [CrossRef]
- Ying, H.; Wang, J.; Shen, Z.; Wang, M.; Zhou, B. Impact of Lowering Low-Density Lipoprotein Cholesterol with Contemporary Lipid-Lowering Medicines on Cognitive Function: A Systematic Review and Meta-Analysis. Cardiovasc. Drugs Ther. 2020, 35, 153–166. [Google Scholar] [CrossRef]
- Murphy, S.A.; Pedersen, T.R.; Gaciong, Z.A.; Ceska, R.; Ezhov, M.V.; Connolly, D.L.; Jukema, J.W.; Toth, K.; Tikkanen, M.J.; Im, K.; et al. Effect of the PCSK9 Inhibitor Evolocumab on Total Cardiovascular Events in Patients With Cardiovascular Disease. JAMA Cardiol. 2019, 4, 613–619. [Google Scholar] [CrossRef]
- Schmidt, A.F.; Carter, J.-P.L.; Pearce, L.S.; Wilkins, J.T.; Overington, J.P.; Hingorani, A.D.; Casas, J. PCSK9 monoclonal antibodies for the primary and secondary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2020, 2020, CD011748. [Google Scholar] [CrossRef]
- Sagris, D.; Ntaios, G.; Georgiopoulos, G.; Pateras, K.; Milionis, H. Proprotein Convertase Subtilisin-Kexin Type 9 inhibitors and stroke prevention: A meta-analysis. Eur. J. Intern. Med. 2021, 85, 130–132. [Google Scholar] [CrossRef]
- Bajaj, N.S.; Patel, N.; Kalra, R.; Ahmad, A.; Venkatraman, A.; Arora, G.; Arora, P. Neurological effects of proprotein convertase subtilisin/kexin type 9 inhibitors: Direct comparisons. Eur. Heart J. Qual. Care Clin. Outcomes 2017, 4, 132–141. [Google Scholar] [CrossRef] [PubMed]
- Karatasakis, A.; Danek, B.A.; Karacsonyi, J.; Rangan, B.V.; Roesle, M.K.; Knickelbine, T.; Miedema, M.D.; Khalili, H.; Ahmad, Z.; Abdullah, S.; et al. Effect of PCSK9 Inhibitors on Clinical Outcomes in Patients With Hypercholesterolemia: A Meta-Analysis of 35 Randomized Controlled Trials. J. Am. Heart Assoc. 2017, 6, e006910. [Google Scholar] [CrossRef] [PubMed]
- Guedeney, P.; Giustino, G.; Sorrentino, S.; Claessen, B.E.; Camaj, A.; Kalkman, D.N.; Vogel, B.; Sartori, S.; De Rosa, S.; Baber, U.; et al. Efficacy and safety of alirocumab and evolocumab: A systematic review and meta-analysis of randomized controlled trials. Eur. Heart J. 2019, 43, e17–e25. [Google Scholar] [CrossRef]
- Giugliano, R.P.; Pedersen, T.R.; Park, J.-G.; De Ferrari, G.M.; Gaciong, Z.A.; Ceska, R.; Toth, K.; Gouni-Berthold, I.; Lopez-Miranda, J.; Schiele, F.; et al. Clinical efficacy and safety of achieving very low LDL-cholesterol concentrations with the PCSK9 inhibitor evolocumab: A prespecified secondary analysis of the FOURIER trial. Lancet 2017, 390, 1962–1971. [Google Scholar] [CrossRef]
- Ridker, P.M.; Revkin, J.; Amarenco, P.; Brunell, R.; Curto, M.; Civeira, F.; Flather, M.; Glynn, R.J.; Gregoire, J.; Jukema, J.W.; et al. Cardiovascular Efficacy and Safety of Bococizumab in High-Risk Patients. N. Engl. J. Med. 2017, 376, 1527–1539. [Google Scholar] [CrossRef]
- Ridker, P.M.; Tardif, J.-C.; Amarenco, P.; Duggan, W.; Glynn, R.J.; Jukema, J.W.; Kastelein, J.J.; Kim, A.M.; Koenig, W.; Nissen, S.; et al. Lipid-Reduction Variability and Antidrug-Antibody Formation with Bococizumab. N. Engl. J. Med. 2017, 376, 1517–1526. [Google Scholar] [CrossRef] [PubMed]
- Pfizer Discontinues Global Development of Bococizumab, Its Investigational PCSK9 Inhibitor | Pfizer. Available online: https://www.pfizer.com/news/press-release/press-release-detail/pfizer_discontinues_global_development_of_bococizumab_its_investigational_pcsk9_inhibitor (accessed on 4 August 2022).
- Raal, F.J.; Kallend, D.; Ray, K.K.; Turner, T.; Koenig, W.; Wright, R.S.; Wijngaard, P.L.; Curcio, D.; Jaros, M.J.; Leiter, L.A.; et al. Inclisiran for the Treatment of Heterozygous Familial Hypercholesterolemia. N. Engl. J. Med. 2020, 382, 1520–1530. [Google Scholar] [CrossRef]
- Giugliano, R.P.; Mach, F.; Zavitz, K.; Kurtz, C.; Im, K.; Kanevsky, E.; Schneider, J.; Wang, H.; Keech, A.; Pedersen, T.R.; et al. Cognitive Function in a Randomized Trial of Evolocumab. N. Engl. J. Med. 2017, 377, 633–643. [Google Scholar] [CrossRef]
- Gencer, B.; Mach, F.; Guo, J.; Im, K.; Ruzza, A.; Wang, H.; Kurtz, C.E.; Pedersen, T.R.; Keech, A.C.; Ott, B.R.; et al. Cognition After Lowering LDL-Cholesterol With Evolocumab. J. Am. Coll. Cardiol. 2020, 75, 2283–2293. [Google Scholar] [CrossRef]
- Janik, M.J.; Urbach, D.V.; van Nieuwenhuizen, E.; Zhao, J.; Yellin, O.; Baccara-Dinet, M.T.; Pordy, R.; Manvelian, G. Alirocumab treatment and neurocognitive function according to the CANTAB scale in patients at increased cardiovascular risk: A prospective, randomized, placebo-controlled study. Atherosclerosis 2021, 331, 20–27. [Google Scholar] [CrossRef]
- Kyriakos, G.; Quiles-Sánchez, L.V.; Diamantis, E.; Farmaki, P.; Garmpis, N.; Damaskos, C.; Savvanis, S.; Patsouras, A.; Stelianidi, A.; Voutyritsa, E.; et al. Lipid-lowering Drugs and Neurocognitive Function: A Systematic Review. In Vivo 2020, 34, 3109–3114. [Google Scholar] [CrossRef] [PubMed]
- Harvey, P.D.; Sabbagh, M.N.; Harrison, J.E.; Ginsberg, H.N.; Chapman, M.J.; Manvelian, G.; Moryusef, A.; Mandel, J.; Farnier, M. No evidence of neurocognitive adverse events associated with alirocumab treatment in 3340 patients from 14 randomized Phase 2 and 3 controlled trials: A meta-analysis of individual patient data. Eur. Heart J. 2017, 39, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Raccah, B.H.; Yanovsky, A.; Treves, N.; Rotshild, V.; Renoux, C.; Danenberg, H.; Eliaz, R.; Matok, I. Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) inhibitors and the risk for neurocognitive adverse events: A systematic review, meta-analysis and meta-regression. Int. J. Cardiol. 2021, 335, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Van Bruggen, F.H.; Nijhuis, G.B.J.; Zuidema, S.U.; Luijendijk, H. Serious adverse events and deaths in PCSK9 inhibitor trials reported on ClinicalTrials.gov: A systematic review. Expert Rev. Clin. Pharmacol. 2020, 13, 787–796. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.R.; Bavishi, C.; Riaz, H.; Farid, T.A.; Khan, S.; Atlas, M.; Hirsch, G.; Ikram, S.; Bolli, R. Increased Risk of Adverse Neurocognitive Outcomes With Proprotein Convertase Subtilisin-Kexin Type 9 Inhibitors. Circ. Cardiovasc. Qual. Outcomes 2017, 10, e003153. [Google Scholar] [CrossRef] [PubMed]
- Da Dalt, L.; Ruscica, M.; Bonacina, F.; Balzarotti, G.; Dhyani, A.; Di Cairano, E.; Baragetti, A.; Arnaboldi, L.; De Metrio, S.; Pellegatta, F.; et al. PCSK9 deficiency reduces insulin secretion and promotes glucose intolerance: The role of the low-density lipoprotein receptor. Eur. Heart J. 2019, 40, 357–368. [Google Scholar] [CrossRef]
- Yang, S.-H.; Li, S.; Zhang, Y.; Xu, R.-X.; Guo, Y.-L.; Zhu, C.-G.; Wu, N.-Q.; Cui, C.-J.; Sun, J.; Li, J.-J. Positive correlation of plasma PCSK9 levels with HbA1c in patients with type 2 diabetes. Diabetes/Metab. Res. Rev. 2015, 32, 193–199. [Google Scholar] [CrossRef]
- Nicholls, S.J.; Puri, R.; Anderson, T.; Ballantyne, C.M.; Cho, L.; Kastelein, J.J.P.; Koenig, W.; Somaratne, R.; Kassahun, H.; Yang, J.; et al. Effect of Evolocumab on Progression of Coronary Disease in Statin-Treated Patients: The GLAGOV Randomized Clinical Trial. JAMA 2016, 316, 2373–2384. [Google Scholar] [CrossRef]
- Deedwania, P.; Murphy, S.A.; Scheen, A.; Badariene, J.; Pineda, A.L.; Honarpour, N.; Keech, A.C.; Sever, P.S.; Pedersen, T.R.; Sabatine, M.S.; et al. Efficacy and Safety of PCSK9 Inhibition With Evolocumab in Reducing Cardiovascular Events in Patients With Metabolic Syndrome Receiving Statin Therapy: Secondary Analysis From the FOURIER Randomized Clinical Trial. JAMA Cardiol. 2021, 6, 139–147. [Google Scholar] [CrossRef]
- O’Brien, J.; Hayder, H.; Zayed, Y.; Peng, C. Overview of MicroRNA Biogenesis, Mechanisms of Actions, and Circulation. Front. Endocrinol. 2018, 9, 402. [Google Scholar] [CrossRef]
- Ardekani, A.M.; Naeini, M.M. The Role of MicroRNAs in Human Diseases. Avicenna J. Med. Biotechnol. 2010, 2, 161–179. [Google Scholar] [PubMed]
- Goedeke, L.; Aranda, J.F.; Fernández-Hernando, C. microRNA regulation of lipoprotein metabolism. Curr. Opin. Lipidol. 2014, 25, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Ma, N.; Fan, L.; Dong, Y.; Xu, X.; Yu, C.; Chen, J.; Ren, J. New PCSK9 inhibitor miR-552-3p reduces LDL-C via enhancing LDLR in high fat diet-fed mice. Pharmacol. Res. 2021, 167, 105562. [Google Scholar] [CrossRef]
- Pal, M.; Herold, M.J. CRISPR base editing applications for identifying cancer-driving mutations. Biochem. Soc. Trans. 2021, 49, 269–280. [Google Scholar] [CrossRef]
- Ahamad, S.; Mathew, S.; Khan, W.A.; Mohanan, K. Development of small-molecule PCSK9 inhibitors for the treatment of hypercholesterolemia. Drug Discov. Today 2022, 27, 1332–1349. [Google Scholar] [CrossRef] [PubMed]
- Masuda, Y.; Yamaguchi, S.; Suzuki, C.; Aburatani, T.; Nagano, Y.; Miyauchi, R.; Suzuki, E.; Yamamura, N.; Nagatomo, K.; Ishihara, H.; et al. Generation and Characterization of a Novel Small Biologic Alternative to Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Antibodies, DS-9001a, Albumin Binding Domain–Fused Anticalin Protein. J. Pharmacol. Exp. Ther. 2018, 365, 368–378. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, T.; Chao, G.; Sitkoff, D.; Lo, F.; Monshizadegan, H.; Meyers, D.; Low, S.; Russo, K.; DiBella, R.; Denhez, F.; et al. Pharmacologic Profile of the Adnectin BMS-962476, a Small Protein Biologic Alternative to PCSK9 Antibodies for Low-Density Lipoprotein Lowering. J. Pharmacol. Exp. Ther. 2014, 350, 412–424. [Google Scholar] [CrossRef]
- Abdul-Rahman, T.; Bukhari, S.M.A.; Herrera, E.C.; Awuah, W.A.; Lawrence, J.; de Andrade, H.; Patel, N.; Shah, R.; Shaikh, R.; Capriles, C.A.A.; et al. Lipid Lowering Therapy: An Era Beyond Statins. Curr. Probl. Cardiol. 2022, 101342. [Google Scholar] [CrossRef]
- Blom, D.J.; Hala, T.; Bolognese, M.; Lillestol, M.J.; Toth, P.D.; Burgess, L.; Ceska, R.; Roth, E.; Koren, M.J.; Ballantyne, C.M.; et al. A 52-Week Placebo-Controlled Trial of Evolocumab in Hyperlipidemia. N. Engl. J. Med. 2014, 370, 1809–1819. [Google Scholar] [CrossRef]
- Salvatore, T.; Morganti, R.; Marchioli, R.; De Caterina, R. Cholesterol Lowering and Stroke: No Longer Room for Pleiotropic Effects of Statins—Confirmation from PCSK9 Inhibitor Studies. Am. J. Med. 2019, 133, 95–99.e6. [Google Scholar] [CrossRef]
- Tsankof, A.; Tziomalos, K. The Role of Lipid-Lowering Treatment in the Secondary Prevention of Ischemic Stroke. Diseases 2021, 10, 3. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Name | Indication | Administration | Benefit | Common Adverse Reactions | Ref. |
|---|---|---|---|---|---|
| Evolocumab | Primary and secondary hypercholesterolemia HoFH * Established ASCVD * | 140 mg every 2 weeks subcutaneous or 420 mg once monthly | LDL-C level reduction by 61% Reduced CV events | Local injection site reaction Pruritus Upper respiratory tract symptoms | [47,48] |
| Alirocumab | Primary and secondary hypercholesterolemia Establish ASCVD * | 75 mg every 2 weeks subcutaneous or 300 mg once monthly | LDL-C * level reduction by 62% decreased the rate of MACE * | Local injection site reaction Pruritus Upper respiratory tract symptoms | [23,49] |
| Inclisiran | Primary and secondary hypercholesterolemia | 284 mg single administration subcutaneous, then repeated at 3 months, followed by every 6 months | LDL-C level reduction between 27% and 53%, depending on the number of doses | Local injection site reaction | [50,51] |
| Nr. Crt. | Study Name | Number | Drug | Aim |
|---|---|---|---|---|
| 1 | EVOCAR-1 study | NCT03931161 | Evolocumab | Determine the efficacy of evolocumab on carotid plaque morphology and composition in asymptomatic patients with >50% carotid artery stenosis. |
| 2 | CARUSO study | NCT04730973 | Evolocumab | Determine the efficacy of evolocumab in promoting carotid plaque morphological stabilization and regression compared to traditional lipid-lowering therapy. |
| 3 | TOPICAL-MRI | NCT05001984 | Alirocumab | Determine the efficacy and safety of alirocumab on patients with intracranial atherosclerotic plaque. |
| 4 | INSIST-HRMRI | NCT03753555 | Evolocumab | Determine the effectiveness of intensive hypolipemic drug (statins vs. evolocumab, probucol) on patients with AIS and intracranial atherosclerotic plaque. |
| 5 | Study of Predictive Factors Related to Prognosis of Patients with Ischemic Stroke due to Large-artery Atherosclerosis | NCT04847752 | PCSK-9 inhibitor | Determine the in-hospital factors that could predict the outcome of AIS patients and provide more evidence-based suggestions in the treatment and prognosis of atherosclerotic ischemic cerebrovascular disease. |
| 6 | sICASBLM | NCT05397405 | PCSK-9 Inhibitors | Assess the impact of improving blood lipid management on clinical outcome of moderate to severe symptomatic intracranial atherosclerotic stenosis patients (LDL-C > 1.8 mmol/L) without endovascular therapy. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilut, S.; Pirlog, B.O.; Pirlog, R.; Nutu, A.; Vacaras, V.; Armean, S.M. Recent Advances on the Roles of PCSK-9 Inhibitors in the Management of Acute Ischemic Stroke Patients. Int. J. Mol. Sci. 2022, 23, 10221. https://doi.org/10.3390/ijms231810221
Ilut S, Pirlog BO, Pirlog R, Nutu A, Vacaras V, Armean SM. Recent Advances on the Roles of PCSK-9 Inhibitors in the Management of Acute Ischemic Stroke Patients. International Journal of Molecular Sciences. 2022; 23(18):10221. https://doi.org/10.3390/ijms231810221
Chicago/Turabian StyleIlut, Silvina, Bianca O. Pirlog, Radu Pirlog, Andreea Nutu, Vitalie Vacaras, and Sebastian M. Armean. 2022. "Recent Advances on the Roles of PCSK-9 Inhibitors in the Management of Acute Ischemic Stroke Patients" International Journal of Molecular Sciences 23, no. 18: 10221. https://doi.org/10.3390/ijms231810221
APA StyleIlut, S., Pirlog, B. O., Pirlog, R., Nutu, A., Vacaras, V., & Armean, S. M. (2022). Recent Advances on the Roles of PCSK-9 Inhibitors in the Management of Acute Ischemic Stroke Patients. International Journal of Molecular Sciences, 23(18), 10221. https://doi.org/10.3390/ijms231810221