
Translational Study of Copy Number Variations in Schizophrenia

 ,
, 
 ,
, 
Abstract
:1. Introduction
2. Results
2.1. Development and Optimization of RT-qPCR Test
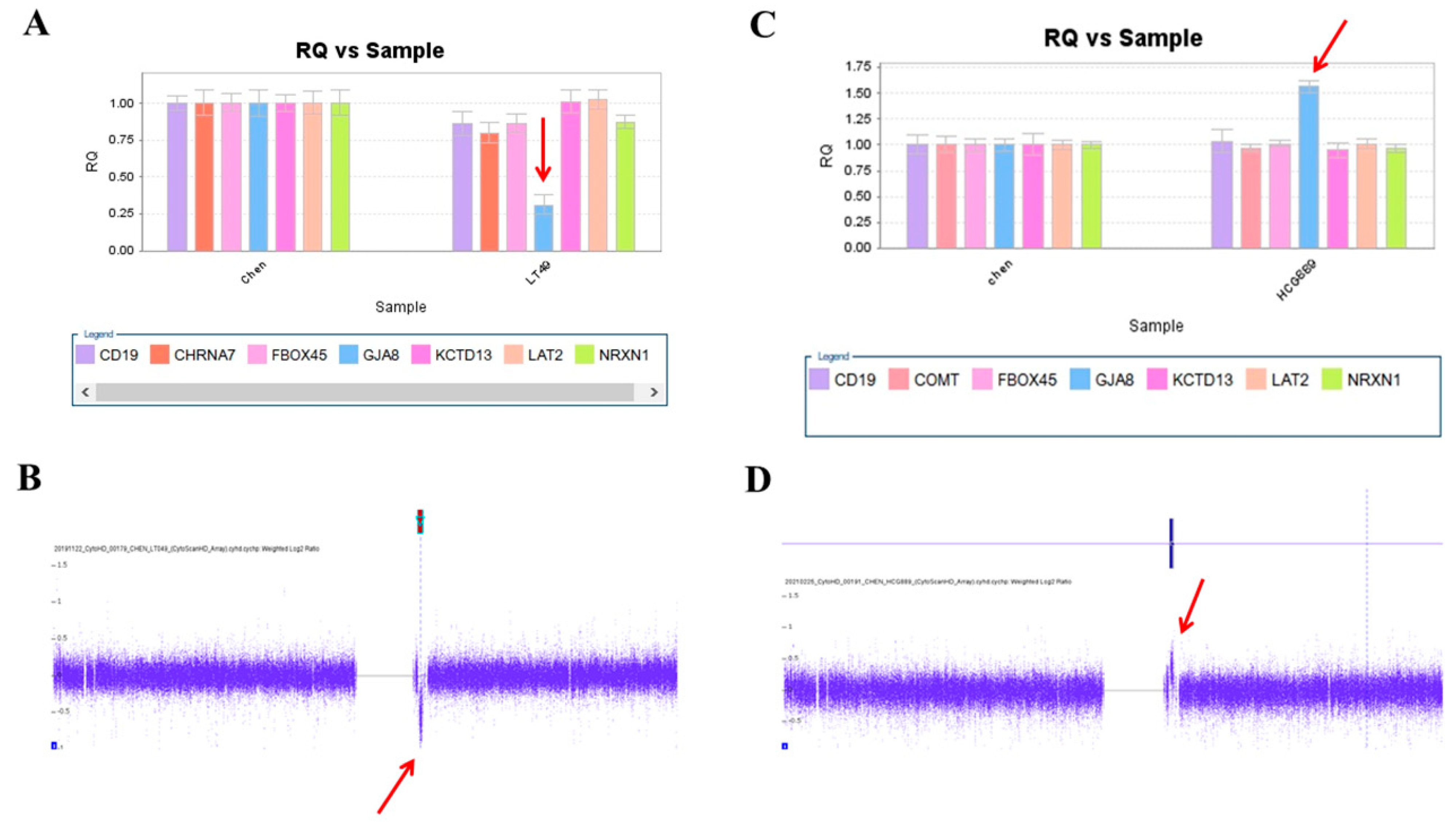
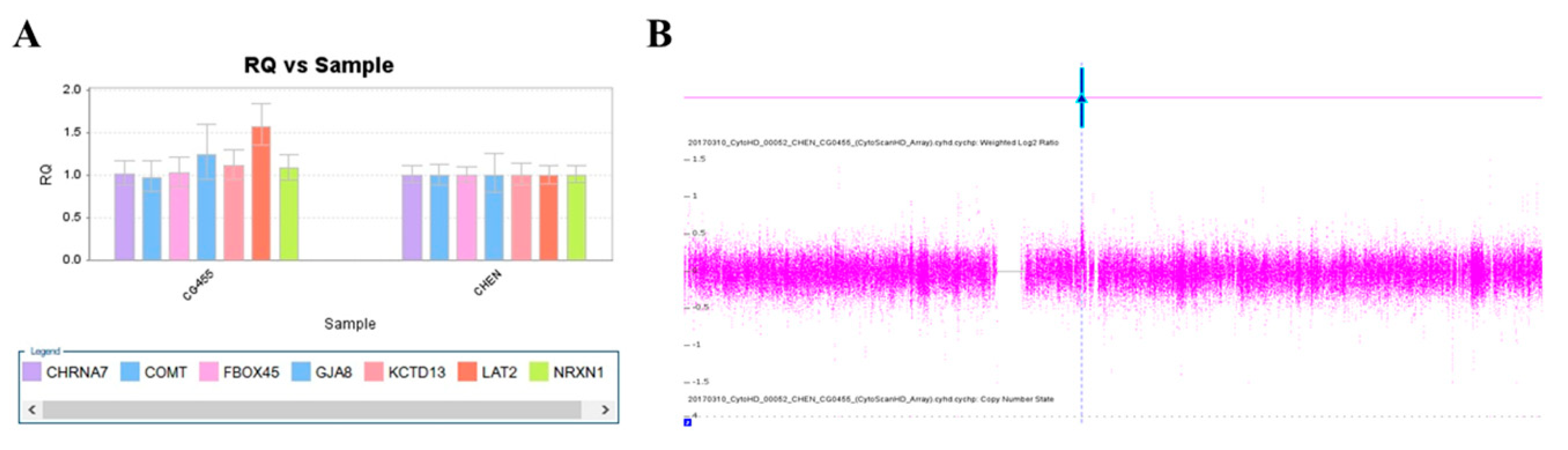
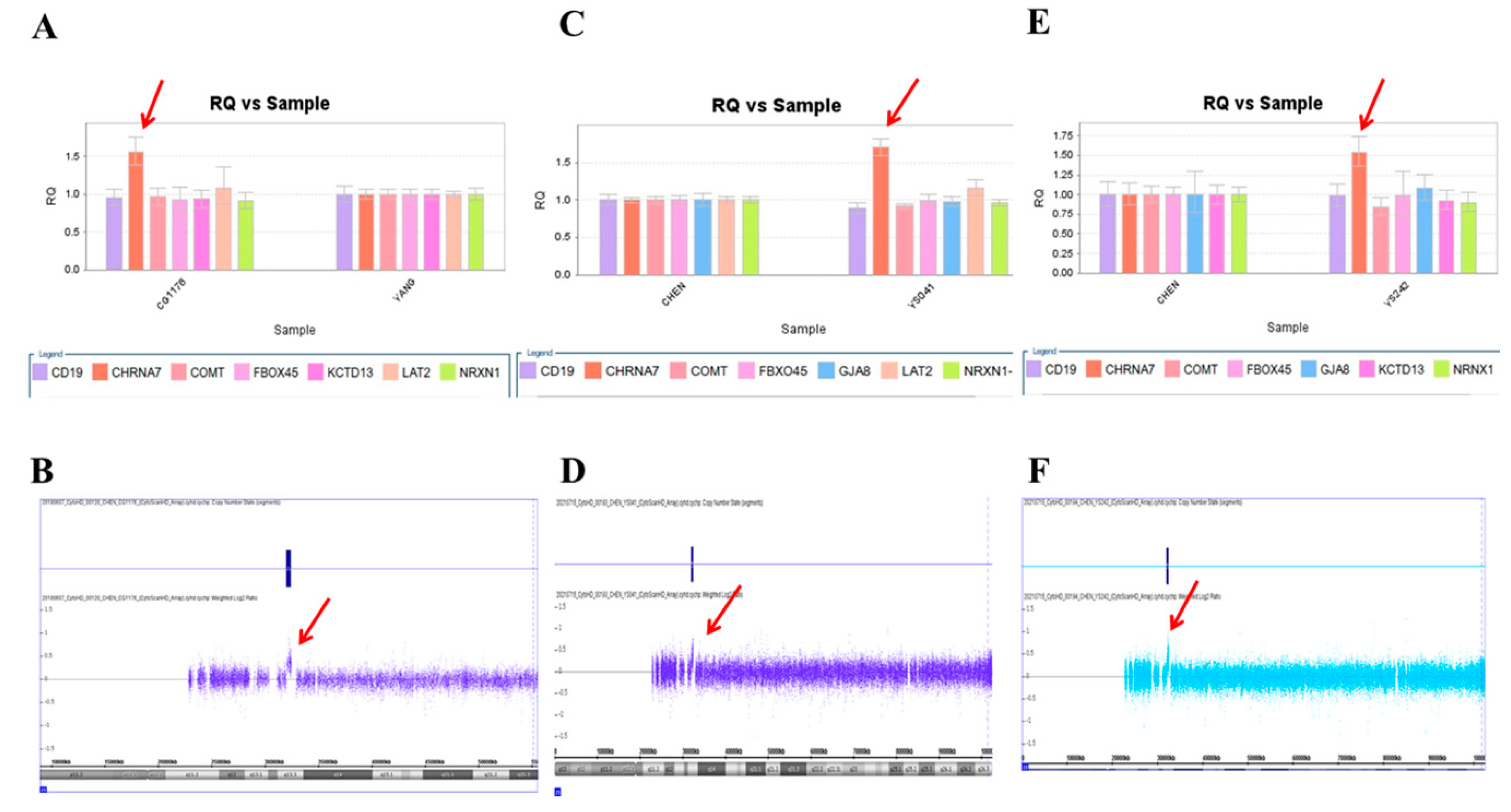
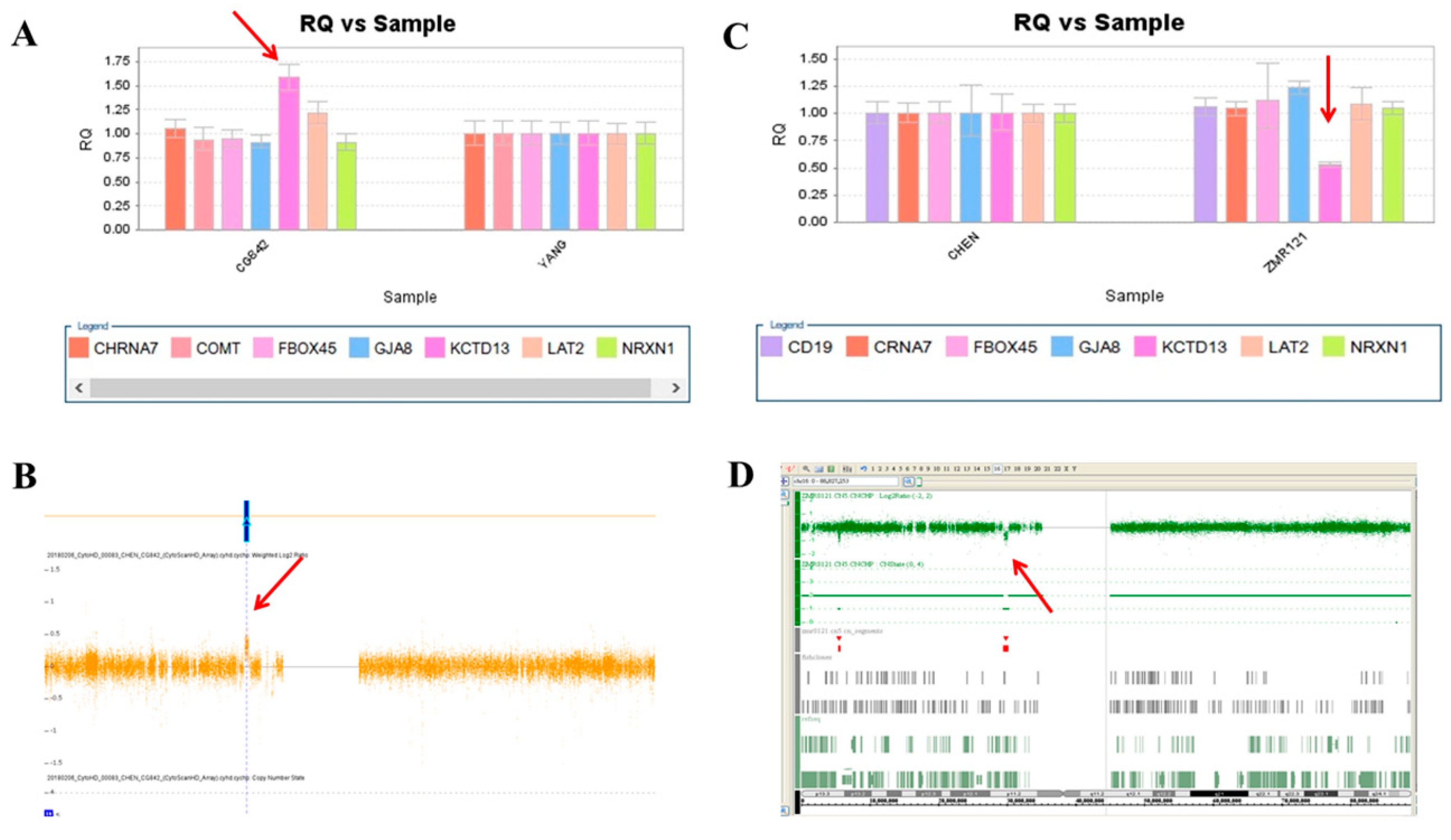
2.2. Screening of Patients with Schizophrenia
2.3. Confirmation by Chromosomal Microarray Analysis (CMA)
3. Discussion
4. Materials and Methods
4.1. Subjects
4.2. Real-Time Quantitative PCR (RT-qPCR) Test of Target Loci
4.3. Chromosomal Microarray Analysis (CMA)
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Trifu, S.C.; Kohn, B.; Vlasie, A.; Patrichi, B.E. Genetics of schizophrenia (Review). Exp. Ther. Med. 2020, 20, 3462–3468. [Google Scholar] [CrossRef]
- Khavari, B.; Cairns, M.J. Epigenomic Dysregulation in Schizophrenia: In Search of Disease Etiology and Biomarkers. Cells 2020, 9, 1837. [Google Scholar] [CrossRef]
- Rees, E.; Kirov, G. Copy number variation and neuropsychiatric illness. Curr. Opin. Genet. Dev. 2021, 68, 57–63. [Google Scholar] [CrossRef]
- Lew, A.R.; Kellermayer, T.R.; Sule, B.P.; Szigeti, K. Copy Number Variations in Adult-onset Neuropsychiatric Diseases. Curr. Genom. 2018, 19, 420–430. [Google Scholar] [CrossRef]
- Insel, T.; Cuthbert, B.; Garvey, M.; Heinssen, R.; Pine, D.S.; Quinn, K.; Sanislow, C.; Wang, P. Research domain criteria (RDoC): Toward a new classification framework for research on mental disorders. Am. J. Psychiatry 2010, 167, 748–751. [Google Scholar] [CrossRef] [Green Version]
- Barlati, S.; Minelli, A.; Ceraso, A.; Nibbio, G.; Carvalho Silva, R.; Deste, G.; Turrina, C.; Vita, A. Social Cognition in a Research Domain Criteria Perspective: A Bridge Between Schizophrenia and Autism Spectra Disorders. Front. Psychiatry 2020, 11, 806. [Google Scholar] [CrossRef]
- Sonderby, I.E.; Ching, C.R.K.; Thomopoulos, S.I.; van der Meer, D.; Sun, D.; Villalon-Reina, J.E.; Agartz, I.; Amunts, K.; Arango, C.; Armstrong, N.J.; et al. Effects of copy number variations on brain structure and risk for psychiatric illness: Large-scale studies from the ENIGMA working groups on CNVs. Hum. Brain Mapp. 2022, 43, 300–328. [Google Scholar] [CrossRef]
- Sonderby, I.E.; Gustafsson, O.; Doan, N.T.; Hibar, D.P.; Martin-Brevet, S.; Abdellaoui, A.; Ames, D.; Amunts, K.; Andersson, M.; Armstrong, N.J.; et al. Dose response of the 16p11.2 distal copy number variant on intracranial volume and basal ganglia. Mol. Psychiatry 2020, 25, 584–602. [Google Scholar] [CrossRef]
- Van der Meer, D.; Sonderby, I.E.; Kaufmann, T.; Walters, G.B.; Abdellaoui, A.; Ames, D.; Amunts, K.; Andersson, M.; Armstrong, N.J.; Bernard, M.; et al. Association of Copy Number Variation of the 15q11.2 BP1-BP2 Region With Cortical and Subcortical Morphology and Cognition. JAMA Psychiatry 2020, 77, 420–430. [Google Scholar] [CrossRef] [Green Version]
- Sonderby, I.E.; van der Meer, D.; Moreau, C.; Kaufmann, T.; Walters, G.B.; Ellegaard, M.; Abdellaoui, A.; Ames, D.; Amunts, K.; Andersson, M.; et al. 1q21.1 distal copy number variants are associated with cerebral and cognitive alterations in humans. Transl. Psychiatry 2021, 11, 182. [Google Scholar] [CrossRef]
- Marshall, C.R.; Howrigan, D.P.; Merico, D.; Thiruvahindrapuram, B.; Wu, W.; Greer, D.S.; Antaki, D.; Shetty, A.; Holmans, P.A.; Pinto, D.; et al. Contribution of copy number variants to schizophrenia from a genome-wide study of 41,321 subjects. Nat. Genet. 2017, 49, 27–35. [Google Scholar] [CrossRef] [Green Version]
- Scionti, F.; Di Martino, M.T.; Pensabene, L.; Bruni, V.; Concolino, D. The Cytoscan HD Array in the Diagnosis of Neurodevelopmental Disorders. High Throughput 2018, 7, 28. [Google Scholar] [CrossRef] [Green Version]
- Manning, M.; Hudgins, L.; Professional, P.; Guidelines, C. Array-based technology and recommendations for utilization in medical genetics practice for detection of chromosomal abnormalities. Genet. Med. 2010, 12, 742–745. [Google Scholar] [CrossRef] [Green Version]
- Miller, D.T.; Adam, M.P.; Aradhya, S.; Biesecker, L.G.; Brothman, A.R.; Carter, N.P.; Church, D.M.; Crolla, J.A.; Eichler, E.E.; Epstein, C.J.; et al. Consensus statement: Chromosomal microarray is a first-tier clinical diagnostic test for individuals with developmental disabilities or congenital anomalies. Am. J. Hum. Genet. 2010, 86, 749–764. [Google Scholar] [CrossRef]
- Michelson, D.J.; Shevell, M.I.; Sherr, E.H.; Moeschler, J.B.; Gropman, A.L.; Ashwal, S. Evidence report: Genetic and metabolic testing on children with global developmental delay: Report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology 2011, 77, 1629–1635. [Google Scholar] [CrossRef] [Green Version]
- Costain, G.; Lionel, A.C.; Merico, D.; Forsythe, P.; Russell, K.; Lowther, C.; Yuen, T.; Husted, J.; Stavropoulos, D.J.; Speevak, M.; et al. Pathogenic rare copy number variants in community-based schizophrenia suggest a potential role for clinical microarrays. Hum. Mol. Genet. 2013, 22, 4485–4501. [Google Scholar] [CrossRef] [Green Version]
- Lowther, C.; Merico, D.; Costain, G.; Waserman, J.; Boyd, K.; Noor, A.; Speevak, M.; Stavropoulos, D.J.; Wei, J.; Lionel, A.C.; et al. Impact of I.Q. on the diagnostic yield of chromosomal microarray in a community sample of adults with schizophrenia. Genome Med. 2017, 9, 105. [Google Scholar] [CrossRef] [Green Version]
- Baker, K.; Costain, G.; Fung, W.L.; Bassett, A.S. Chromosomal microarray analysis-a routine clinical genetic test for patients with schizophrenia. Lancet Psychiatry 2014, 1, 329–331. [Google Scholar] [CrossRef]
- Chen, C.H.; Cheng, M.C.; Hu, T.M.; Ping, L.Y. Chromosomal Microarray Analysis as First-Tier Genetic Test for Schizophrenia. Front. Genet. 2021, 12, 620496. [Google Scholar] [CrossRef]
- Ceulemans, S.; van der Ven, K.; Del-Favero, J. Targeted screening and validation of copy number variations. Methods Mol. Biol. 2012, 838, 311–328. [Google Scholar] [CrossRef]
- Weksberg, R.; Hughes, S.; Moldovan, L.; Bassett, A.S.; Chow, E.W.; Squire, J.A. A method for accurate detection of genomic microdeletions using real-time quantitative PCR. BMC Genom. 2005, 6, 180. [Google Scholar] [CrossRef] [Green Version]
- Chien, W.H.; Gau, S.S.; Wu, Y.Y.; Huang, Y.S.; Fang, J.S.; Chen, Y.J.; Soong, W.T.; Chiu, Y.N.; Chen, C.H. Identification and molecular characterization of two novel chromosomal deletions associated with autism. Clin. Genet. 2010, 78, 449–456. [Google Scholar] [CrossRef]
- Liao, H.M.; Chao, Y.L.; Huang, A.L.; Cheng, M.C.; Chen, Y.J.; Lee, K.F.; Fang, J.S.; Hsu, C.H.; Chen, C.H. Identification and characterization of three inherited genomic copy number variations associated with familial schizophrenia. Schizophr. Res. 2012, 139, 229–236. [Google Scholar] [CrossRef]
- Morris-Rosendahl, D.J.; Crocq, M.A. Neurodevelopmental disorders-the history and future of a diagnostic concept. Dialogues Clin. Neurosci. 2020, 22, 65–72. [Google Scholar] [CrossRef]
- Lowther, C.; Costain, G.; Baribeau, D.A.; Bassett, A.S. Genomic Disorders in Psychiatry-What Does the Clinician Need to Know? Curr. Psychiatry Rep. 2017, 19, 82. [Google Scholar] [CrossRef]
- Nakatochi, M.; Kushima, I.; Ozaki, N. Implications of germline copy-number variations in psychiatric disorders: Review of large-scale genetic studies. J. Hum. Genet. 2021, 66, 25–37. [Google Scholar] [CrossRef]
- Cubells, J.F.; Deoreo, E.H.; Harvey, P.D.; Garlow, S.J.; Garber, K.; Adam, M.P.; Martin, C.L. Pharmaco-genetically guided treatment of recurrent rage outbursts in an adult male with 15q13.3 deletion syndrome. Am. J. Med. Genet. A 2011, 155A, 805–810. [Google Scholar] [CrossRef]
- Casas-Alba, D.; Nolasco, G.A.; Diez-Juan, M.; Mezzatesta, M.; Balana, G.; Fons, C. Targeted therapy with galantamine in a pediatric patient with 15q13.3 deletion syndrome. Am. J. Med. Genet. A 2021, 185, 3897–3899. [Google Scholar] [CrossRef]
- Bodkin, J.A.; Coleman, M.J.; Godfrey, L.J.; Carvalho, C.M.B.; Morgan, C.J.; Suckow, R.F.; Anderson, T.; Ongur, D.; Kaufman, M.J.; Lewandowski, K.E.; et al. Targeted Treatment of Individuals With Psychosis Carrying a Copy Number Variant Containing a Genomic Triplication of the Glycine Decarboxylase Gene. Biol. Psychiatry 2019, 86, 523–535. [Google Scholar] [CrossRef]
- Bassett, A.S.; McDonald-McGinn, D.M.; Devriendt, K.; Digilio, M.C.; Goldenberg, P.; Habel, A.; Marino, B.; Oskarsdottir, S.; Philip, N.; Sullivan, K.; et al. Practical guidelines for managing patients with 22q11.2 deletion syndrome. J. Pediatr. 2011, 159, 332–339. [Google Scholar] [CrossRef]
- Yuan, H.; Shangguan, S.; Li, Z.; Luo, J.; Su, J.; Yao, R.; Zhang, S.; Liang, C.; Chen, Q.; Gao, Z.; et al. CNV profiles of Chinese pediatric patients with developmental disorders. Genet. Med. 2021, 23, 669–678. [Google Scholar] [CrossRef]
- Smajlagic, D.; Lavrichenko, K.; Berland, S.; Helgeland, O.; Knudsen, G.P.; Vaudel, M.; Haavik, J.; Knappskog, P.M.; Njolstad, P.R.; Houge, G.; et al. Population prevalence and inheritance pattern of recurrent CNVs associated with neurodevelopmental disorders in 12,252 newborns and their parents. Eur. J. Hum. Genet. 2021, 29, 205–215. [Google Scholar] [CrossRef]
- Martin, C.L.; Wain, K.E.; Oetjens, M.T.; Tolwinski, K.; Palen, E.; Hare-Harris, A.; Habegger, L.; Maxwell, E.K.; Reid, J.G.; Walsh, L.K.; et al. Identification of Neuropsychiatric Copy Number Variants in a Health Care System Population. JAMA Psychiatry 2020, 77, 1276–1285. [Google Scholar] [CrossRef]
- Kendall, K.M.; Rees, E.; Bracher-Smith, M.; Legge, S.; Riglin, L.; Zammit, S.; O’Donovan, M.C.; Owen, M.J.; Jones, I.; Kirov, G.; et al. Association of Rare Copy Number Variants With Risk of Depression. JAMA Psychiatry 2019, 76, 818–825. [Google Scholar] [CrossRef] [Green Version]
- Chawner, S.; Owen, M.J.; Holmans, P.; Raymond, F.L.; Skuse, D.; Hall, J.; van den Bree, M.B.M. Genotype-phenotype associations in children with copy number variants associated with high neuropsychiatric risk in the U.K. (IMAGINE-ID): A case-control cohort study. Lancet Psychiatry 2019, 6, 493–505. [Google Scholar] [CrossRef]
- Gudmundsson, O.O.; Walters, G.B.; Ingason, A.; Johansson, S.; Zayats, T.; Athanasiu, L.; Sonderby, I.E.; Gustafsson, O.; Nawaz, M.S.; Jonsson, G.F.; et al. Attention-deficit hyperactivity disorder shares copy number variant risk with schizophrenia and autism spectrum disorder. Transl. Psychiatry 2019, 9, 258. [Google Scholar] [CrossRef] [Green Version]
- Lowther, C.; Speevak, M.; Armour, C.M.; Goh, E.S.; Graham, G.E.; Li, C.; Zeesman, S.; Nowaczyk, M.J.; Schultz, L.A.; Morra, A.; et al. Molecular characterization of NRXN1 deletions from 19,263 clinical microarray cases identifies exons important for neurodevelopmental disease expression. Genet. Med. 2017, 19, 53–61. [Google Scholar] [CrossRef] [Green Version]
- Curran, S.; Ahn, J.W.; Grayton, H.; Collier, D.A.; Ogilvie, C.M. NRXN1 deletions identified by array comparative genome hybridisation in a clinical case series-further understanding of the relevance of NRXN1 to neurodevelopmental disorders. J. Mol. Psychiatry 2013, 1, 4. [Google Scholar] [CrossRef] [Green Version]
- Murphy, M.M.; Lindsey Burrell, T.; Cubells, J.F.; Espana, R.A.; Gambello, M.J.; Goines, K.C.B.; Klaiman, C.; Li, L.; Novacek, D.M.; Papetti, A.; et al. Study protocol for The Emory 3q29 Project: Evaluation of neurodevelopmental, psychiatric, and medical symptoms in 3q29 deletion syndrome. BMC Psychiatry 2018, 18, 183. [Google Scholar] [CrossRef] [Green Version]
- Mulle, J.G.; Pulver, A.E.; McGrath, J.A.; Wolyniec, P.S.; Dodd, A.F.; Cutler, D.J.; Sebat, J.; Malhotra, D.; Nestadt, G.; Conrad, D.F.; et al. Reciprocal duplication of the Williams-Beuren syndrome deletion on chromosome 7q11.23 is associated with schizophrenia. Biol. Psychiatry 2014, 75, 371–377. [Google Scholar] [CrossRef] [Green Version]
- Osborne, L.R.; Mervis, C.B. 7q11.23 deletion and duplication. Curr. Opin. Genet. Dev. 2021, 68, 41–48. [Google Scholar] [CrossRef]
- Sanders, S.J.; Ercan-Sencicek, A.G.; Hus, V.; Luo, R.; Murtha, M.T.; Moreno-De-Luca, D.; Chu, S.H.; Moreau, M.P.; Gupta, A.R.; Thomson, S.A.; et al. Multiple recurrent de novo CNVs, including duplications of the 7q11.23 Williams syndrome region, are strongly associated with autism. Neuron 2011, 70, 863–885. [Google Scholar] [CrossRef] [Green Version]
- Klein-Tasman, B.P.; Mervis, C.B. Autism Spectrum Symptomatology Among Children with Duplication 7q11.23 Syndrome. J. Autism Dev. Disord. 2018, 48, 1982–1994. [Google Scholar] [CrossRef]
- Klein-Tasman, B.P.; van der Fluit, F.; Mervis, C.B. Autism Spectrum Symptomatology in Children with Williams Syndrome Who Have Phrase Speech or Fluent Language. J. Autism Dev. Disord. 2018, 48, 3037–3050. [Google Scholar] [CrossRef]
- Hassfurther, A.; Komini, E.; Fischer, J.; Leipoldt, M. Clinical and Genetic Heterogeneity of the 15q13.3 Microdeletion Syndrome. Mol. Syndromol. 2016, 6, 222–228. [Google Scholar] [CrossRef] [Green Version]
- Zhou, D.; Gochman, P.; Broadnax, D.D.; Rapoport, J.L.; Ahn, K. 15q13.3 duplication in two patients with childhood-onset schizophrenia. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2016, 171, 777–783. [Google Scholar] [CrossRef] [Green Version]
- Chung, W.K.; Roberts, T.P.; Sherr, E.H.; Snyder, L.G.; Spiro, J.E. 16p11.2 deletion syndrome. Curr. Opin. Genet. Dev. 2021, 68, 49–56. [Google Scholar] [CrossRef]
- Chawner, S.; Doherty, J.L.; Anney, R.J.L.; Antshel, K.M.; Bearden, C.E.; Bernier, R.; Chung, W.K.; Clements, C.C.; Curran, S.R.; Cuturilo, G.; et al. A Genetics-First Approach to Dissecting the Heterogeneity of Autism: Phenotypic Comparison of Autism Risk Copy Number Variants. Am. J. Psychiatry 2021, 178, 77–86. [Google Scholar] [CrossRef]
- Jutla, A.; Turner, J.B.; Green Snyder, L.; Chung, W.K.; Veenstra-VanderWeele, J. Psychotic symptoms in 16p11.2 copy-number variant carriers. Autism Res. 2020, 13, 187–198. [Google Scholar] [CrossRef]
- Redaelli, S.; Maitz, S.; Crosti, F.; Sala, E.; Villa, N.; Spaccini, L.; Selicorni, A.; Rigoldi, M.; Conconi, D.; Dalpra, L.; et al. Refining the Phenotype of Recurrent Rearrangements of Chromosome 16. Int. J. Mol. Sci. 2019, 20, 1095. [Google Scholar] [CrossRef] [Green Version]
- Niarchou, M.; Chawner, S.; Doherty, J.L.; Maillard, A.M.; Jacquemont, S.; Chung, W.K.; Green-Snyder, L.; Bernier, R.A.; Goin-Kochel, R.P.; Hanson, E.; et al. Psychiatric disorders in children with 16p11.2 deletion and duplication. Transl. Psychiatry 2019, 9, 8. [Google Scholar] [CrossRef] [Green Version]
- Dowden, L.; Tucker, D.; Morgan, S.; Uzun, O.; Syed, Y.A. Contribution of Congenital Heart Disorders Associated With Copy Number Variants in Mediating Risk for Brain Developmental Disorders: Evidence From 20-Year Retrospective Cohort Study. Front. Cardiovasc. Med. 2021, 8, 655463. [Google Scholar] [CrossRef]
- Modenato, C.; Kumar, K.; Moreau, C.; Martin-Brevet, S.; Huguet, G.; Schramm, C.; Jean-Louis, M.; Martin, C.O.; Younis, N.; Tamer, P.; et al. Effects of eight neuropsychiatric copy number variants on human brain structure. Transl. Psychiatry 2021, 11, 399. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No | Locus | Target Gene | Sequences | Size (bp) | Slope | R2 |
|---|---|---|---|---|---|---|
| 1 | 1q21.1 | GJA8 | GJA8-F 5′-TTCAGGTGGGTGAGAAATGGGCG-3′ GJA8-R 5′-CAGAGGCGAATGTGGGAGATGGG-3′ | 249 | −2.98 | 0.993 |
| 2 | 2p16.3 | NRXN1 | NRXN1-Exon 1-F 5′-CTGGCTCGAGCTGAGGGGAATAAC-3′ NRXN1-Exon 1-R 5′-CCACCACCCATCTTTCCCTGTGTA-3′ | 154 | −3.03 | 0.999 |
| 3 | 3q29 | FBXO45 | FBXO45-F 5′-AGATTGGTTTCAGTGAGGGCCGC-3′ FBXO45-R 5′-ATTGTCCACCAGATTCCAGCCCC-3′ | 170 | −2.547 | 0.991 |
| 4 | 7q11.23 | LAT2 | LAT2-F 5′-TCTTGGCCAGAGACCCCATTGC-3′ LAT2-R 5′-CTTCCTCCACCTCCGGCTTTGTC-3′ | 100 | −3.12 | 0.997 |
| 5 | 15q13.3 | CHRNA7 | CHRNA7-F 5′-TCTCTCCTTAAGTGTCCCTGCAA-3′ CHRNA7-R 5′-CACCACGTCCATGATCTGCAGGA-3′ | 151 | −3.124 | 0.999 |
| 6 | distal 16p11.2 | CD19 | CD19-F 5′-GACTGGTGGCTGGAAGGTCTCAG-3′ CD19-R 5′-GATGGTTGTCAGACTGGCCAGAG-3′ | 173 | −3.056 | 0.998 |
| 7 | proximal 16p11.2 | KCTD13 | KCTD13-S 5′-CCCACTAGGTTGGGTGCTGATTGA-3′ KCTD13-AS 5′-AATCAGGCCCTGCACCAGGTAGTA-3‘ | 154 | −3.452 | 0.998 |
| 8 | 22q11.2 | COMT | COMT-S 5′-ATCCTGCAGCCCATCCACAACCTG-3′ COMT-AS 5′-ACGTTCATGGCCCACTCCTTCTGC-3′ | 289 | −3.129 | 0.997 |
| No | Locus | Case | CNV Type | Start | End | Size (kb) |
|---|---|---|---|---|---|---|
| 1 | 1q21.1–1q21.2 | LT49 | Deletion | 146,043,713 | 147,830,830 | 1787 |
| 2 | 1q21.1 | HCG889 | Duplication | 146,498,298 | 147,399,659 | 901 |
| 3 | 7q11.23 | CG455 | Duplication | 73,585,140 | 74,031,427 | 446 |
| 4 | 15q13.3 | CG1176 | Duplication | 32,003,537 | 32,446,830 | 443 |
| 5 | 15q13.3 | YS041 | Duplication | 32,024,190 | 32,444,196 | 420 |
| 6 | 15q13.3 | YS242 | Duplication | 32,011,476 | 32,446,830 | 435 |
| 7 | proximal 16p11.2 | CG842 | Duplication | 29,591,078 | 30,177,224 | 586 |
| 8 | proximal 16p11.2 | ZMR121 | Deletion | 29,425,200 | 30,214,457 | 789 |
| 9 | 22q11.2 | YS0088 | Deletion | 18,876,416 | 20,330,744 | 1454 |
| 10 | 22q11.2 | YS0281 | Deletion | 18,876,416 | 21,572,202 | 2696 |
| 11 | 22q11.2 | YS0358 | Deletion | 18,890,623 | 21,572,202 | 2682 |
| 12 | 22q11.2 | YS0403 | Deletion | 18,876,416 | 21,034,809 | 2185 |
| 13 | 22q11.2 | YS0146 | Deletion | 18,876,416 | 21,465,050 | 2589 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, M.-C.; Chien, W.-H.; Huang, Y.-S.; Fang, T.-H.; Chen, C.-H. Translational Study of Copy Number Variations in Schizophrenia. Int. J. Mol. Sci. 2022, 23, 457. https://doi.org/10.3390/ijms23010457
Cheng M-C, Chien W-H, Huang Y-S, Fang T-H, Chen C-H. Translational Study of Copy Number Variations in Schizophrenia. International Journal of Molecular Sciences. 2022; 23(1):457. https://doi.org/10.3390/ijms23010457
Chicago/Turabian StyleCheng, Min-Chih, Wei-Hsien Chien, Yu-Shu Huang, Ting-Hsuan Fang, and Chia-Hsiang Chen. 2022. "Translational Study of Copy Number Variations in Schizophrenia" International Journal of Molecular Sciences 23, no. 1: 457. https://doi.org/10.3390/ijms23010457
APA StyleCheng, M.-C., Chien, W.-H., Huang, Y.-S., Fang, T.-H., & Chen, C.-H. (2022). Translational Study of Copy Number Variations in Schizophrenia. International Journal of Molecular Sciences, 23(1), 457. https://doi.org/10.3390/ijms23010457