
Intraperitoneal Glucose Transport to Micrometastasis: A Multimodal In Vivo Imaging Investigation in a Mouse Lymphoma Model

 , , , and
, , , and
Abstract
1. Introduction
2. Results
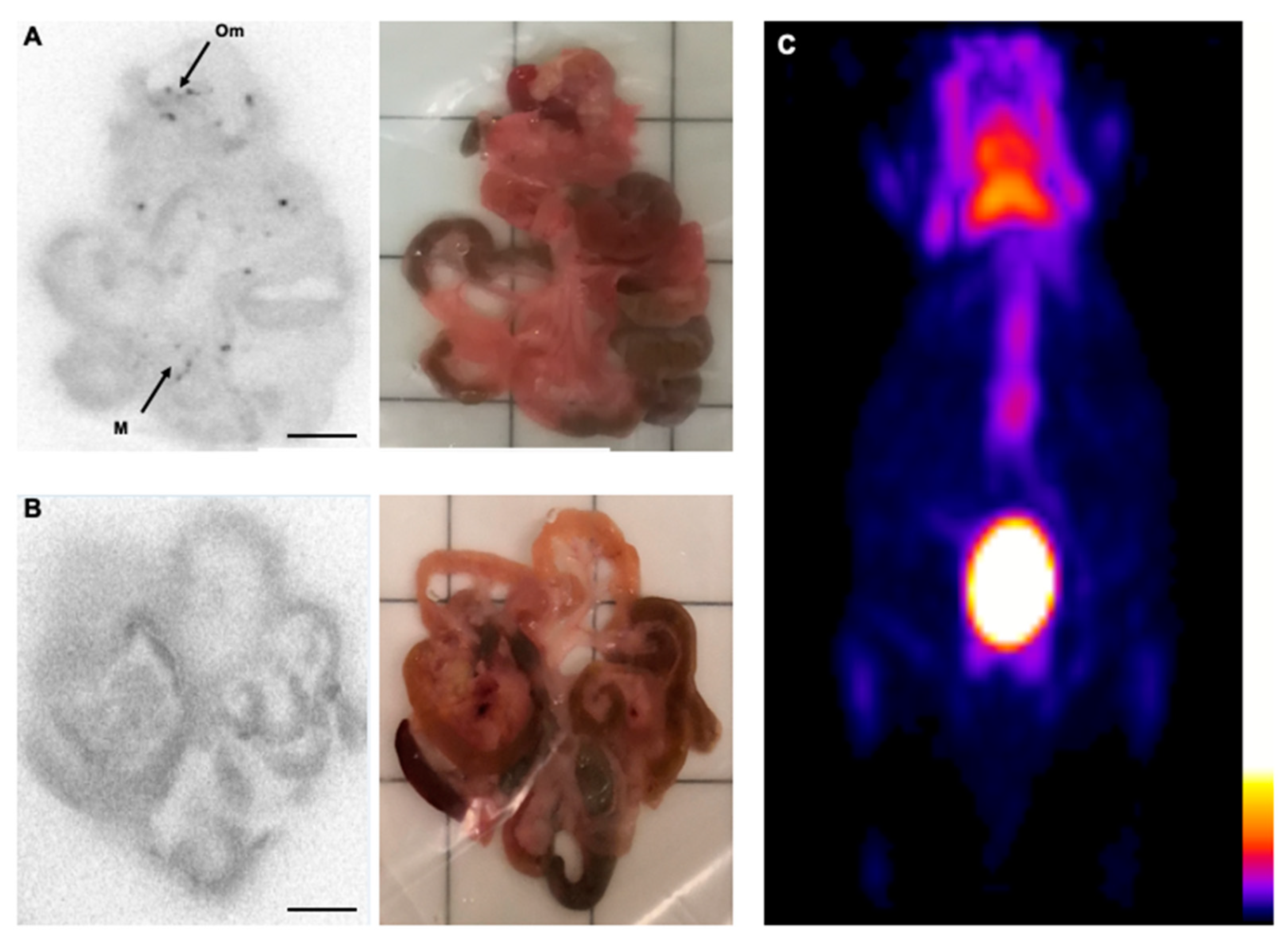
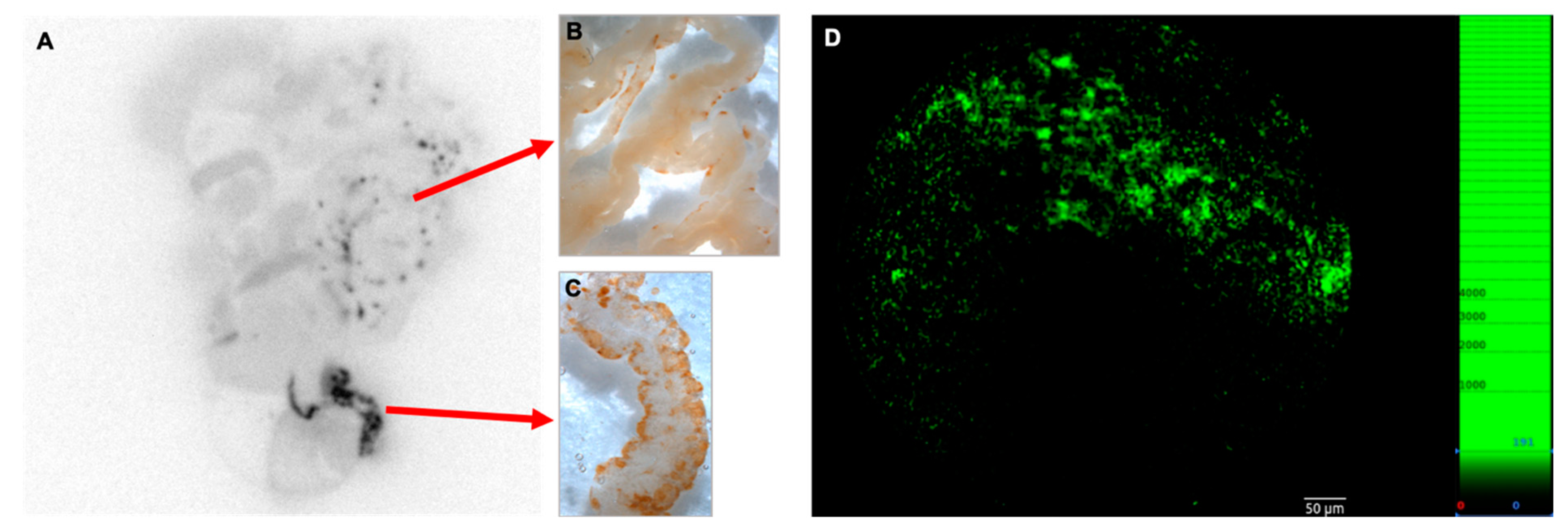
2.1. Monitoring of Early Distribution of Bc.DLFL1 Lymphoma Cells after Intraperitoneal Inoculation Using Systemic and Topical [18F]FDG Administration
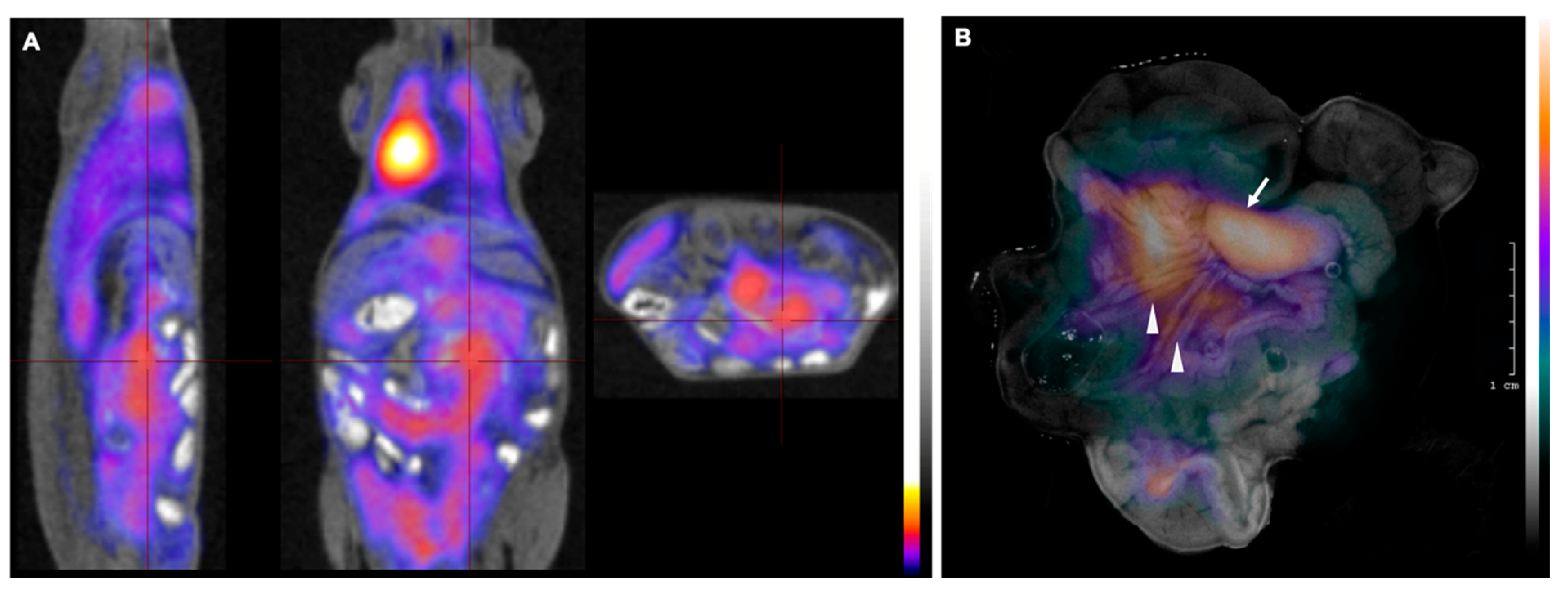
2.2. Successful Monitoring of Lymphoma Expansion in Nodal Metastasis by PET/MR and Subsequent CLI
3. Discussion
4. Methods
4.1. [18F]FDG Uptake Test of Bc.DLFL1 Mouse Lymphoma Cells In Vitro
4.2. Experimental Animals and Bc-DLFL.1 Lymphoma Propagation
4.3. In Vivo Imaging Using [18F]FDG PET
4.4. In Vivo Imaging Using PET/MRI
4.5. Processing of Ex Vivo Tissues for Autoradiography and CLI
4.6. Autoradiography
4.7. Cerenkov Light Imaging Ex Vivo
4.8. Fiber-Optic Confocal Endomicroscopy Imaging of FITC Molecules Ex Vivo
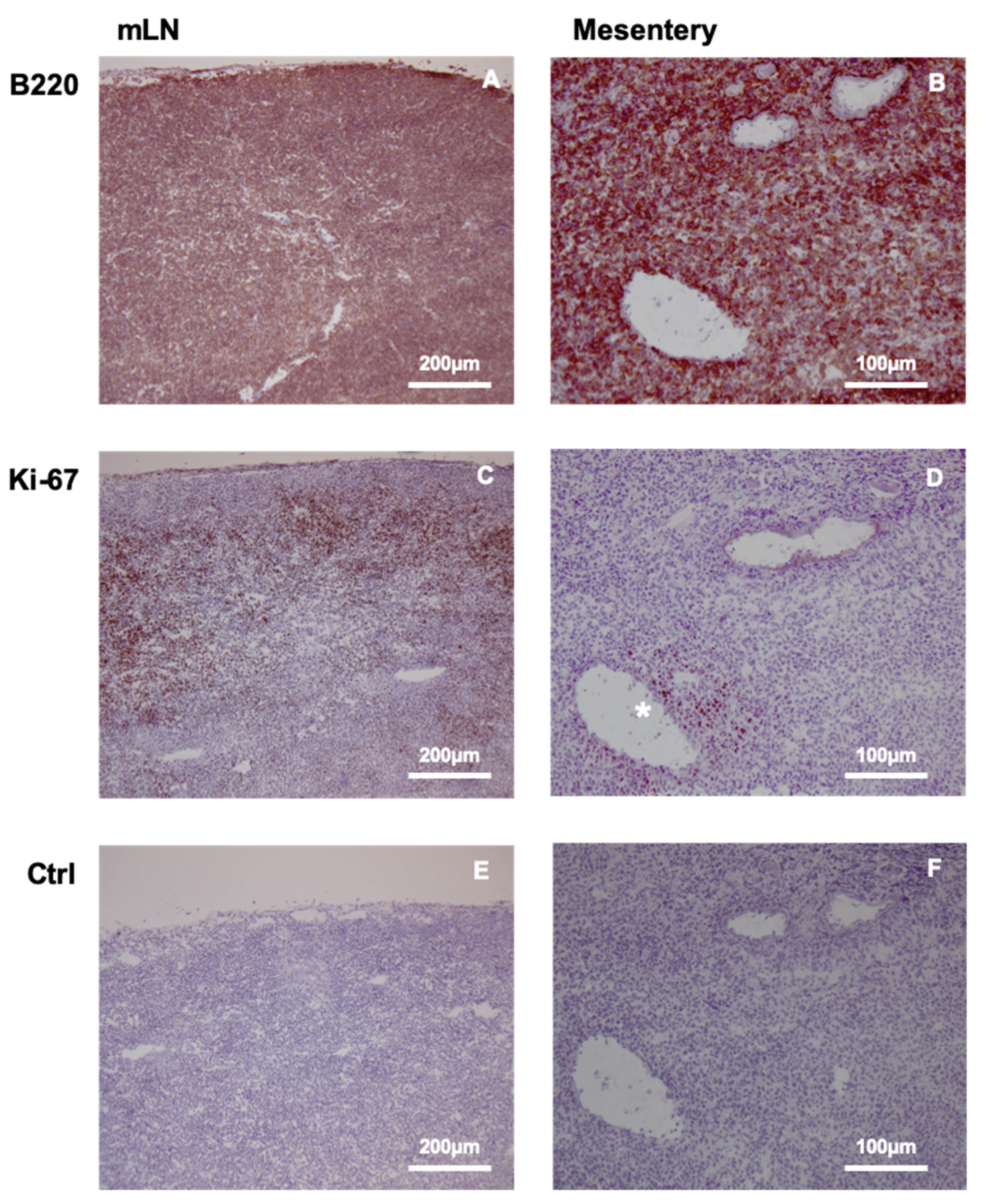
4.9. Immunohistochemistry
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Boellaard, R.; O’Doherty, M.J.; Weber, W.A.; Mottaghy, F.M.; Lonsdale, M.N.; Stroobants, S.G.; Oyen, W.J.; Kotzerke, J.; Hoekstra, O.S.; Pruim, J.; et al. FDG PET and PET/CT: EANM procedure guidelines for tumour PET imaging: Version 1.0. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 181–200. [Google Scholar] [CrossRef] [PubMed]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: The Lugano classification. J. Clin. Oncol. 2014, 32, 3059–3068. [Google Scholar] [CrossRef]
- Cerci, J.J.; Tabacchi, E.; Bogoni, M. Fluorodeoxyglucose-PET/Computed Tomography-Guided Biopsy. PET Clin. 2016, 11, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Manzella, A.; Borba-Filho, P.; D’Ippolito, G.; Farias, M. Abdominal manifestations of lymphoma: Spectrum of imaging features. ISRN Radiol. 2013, 2013, 483069. [Google Scholar] [CrossRef]
- Barrington, S.F.; Mikhaeel, N.G.; Kostakoglu, L.; Meignan, M.; Hutchings, M.; Müeller, S.P.; Schwartz, L.H.; Zucca, E.; Fisher, R.I.; Trotman, J.; et al. Role of imaging in the staging and response assessment of lymphoma: Consensus of the International Conference on Malignant Lymphomas Imaging Working Group. J. Clin. Oncol. 2014, 32, 3048–3058. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D. PET/CT in Lymphoma: Current Overview and Future Directions. Semin. Nucl. Med. 2018, 48, 76–81. [Google Scholar] [CrossRef]
- Kostakoglu, L.; Chauvie, S. Metabolic Tumor Volume Metrics in Lymphoma. Semin. Nucl. Med. 2018, 48, 50–66. [Google Scholar] [CrossRef] [PubMed]
- Kostakoglu, L.; Chauvie, S. PET-Derived Quantitative Metrics for Response and Prognosis in Lymphoma. PET Clin. 2019, 14, 317–329. [Google Scholar] [CrossRef]
- Vercellino, L.; Cottereau, A.S.; Casasnovas, O.; Tilly, H.; Feugier, P.; Chartier, L.; Fruchart, C.; Roulin, L.; Oberic, L.; Pica, G.M.; et al. High total metabolic tumor volume at baseline predicts survival independent of response to therapy. Blood 2020, 135, 1396–1405. [Google Scholar] [CrossRef]
- Vojkovics, D.; Kellermayer, Z.; Heidt, D.; Mihalj, M.; Kajtár, B.; Ernszt, D.; Kovács, T.; Németh, P.; Balogh, P. Isolation and Characterization of a Murine Spontaneous High-Grade Follicular Lymphoma with Restricted In Vivo Spreading--a Model for Lymphatic Metastasis Via the Mesentery. Pathol. Oncol. Res. 2016, 22, 421–430. [Google Scholar] [CrossRef]
- Jia, X.; Gábris, F.; Jacobsen, Ó.; Bedics, G.; Botz, B.; Helyes, Z.; Kellermayer, Z.; Vojkovics, D.; Berta, G.; Nagy, N.; et al. Foliate Lymphoid Aggregates as Novel Forms of Serous Lymphocyte Entry Sites of Peritoneal B Cells and High-Grade B Cell Lymphomas. J. Immunol. 2020, 204, 23–36. [Google Scholar] [CrossRef] [PubMed]
- Gerber, S.A.; Rybalko, V.Y.; Bigelow, C.E.; Lugade, A.A.; Foster, T.H.; Frelinger, J.G.; Lord, E.M. Preferential attachment of peritoneal tumor metastases to omental immune aggregates and possible role of a unique vascular microenvironment in metastatic survival and growth. Am. J. Pathol. 2006, 169, 1739–1752. [Google Scholar] [CrossRef]
- Lee, W.; Ko, S.Y.; Mohamed, M.S.; Kenny, H.A.; Lengyel, E.; Naora, H. Neutrophils facilitate ovarian cancer premetastatic niche formation in the omentum. J. Exp. Med. 2019, 216, 176–194. [Google Scholar] [CrossRef]
- Kitayama, J.; Emoto, S.; Yamaguchi, H.; Ishigami, H.; Watanabe, T. CD90+ mesothelial-like cells in peritoneal fluid promote peritoneal metastasis by forming a tumor permissive microenvironment. PLoS ONE 2014, 9, e86516. [Google Scholar] [CrossRef] [PubMed]
- Levy, A.D.; Shaw, J.C.; Sobin, L.H. Secondary tumors and tumorlike lesions of the peritoneal cavity: Imaging features with pathologic correlation. Radiographics 2009, 29, 347–373. [Google Scholar] [CrossRef]
- Lungoci, C.; Mironiuc, A.I.; Muntean, V.; Oniu, T.; Leebmann, H.; Mayr, M.; Piso, P. Multimodality treatment strategies have changed prognosis of peritoneal metastases. World J. Gastrointest. Oncol. 2016, 8, 67–82. [Google Scholar] [CrossRef] [PubMed]
- Narasimhan, V.; Ooi, G.; Michael, M.; Ramsay, R.; Lynch, C.; Heriot, A. Colorectal peritoneal metastases: Pathogenesis, diagnosis and treatment options—An evidence-based update. ANZ J. Surg. 2020, 90, 1592–1597. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.A. FDG uptake, tumour characteristics and response to therapy: A review. Nucl. Med. Commun. 1998, 19, 97–105. [Google Scholar] [CrossRef]
- Huang, H.; Xiao, F.; Han, X.; Zhong, L.; Zhong, H.; Xu, L.; Zhu, J.; Ni, B.; Liu, J.; Fang, Y.; et al. Correlation of pretreatment 18F-FDG uptake with clinicopathological factors and prognosis in patients with newly diagnosed diffuse large B-cell lymphoma. Nucl. Med. Commun. 2016, 37, 689–698. [Google Scholar] [CrossRef] [PubMed]
- Hirose, Y.; Suefuji, H.; Kaida, H.; Hayakawa, M.; Hattori, S.; Kurata, S.; Watanabe, Y.; Kunou, Y.; Kawahara, A.; Okamura, T.; et al. Relationship between 2-deoxy-2-[(18)F]-fluoro-d-glucose uptake and clinicopathological factors in patients with diffuse large B-cell lymphoma. Leuk. Lymphoma 2014, 55, 520–525. [Google Scholar] [CrossRef] [PubMed]
- Cottone, L.; Valtorta, S.; Capobianco, A.; Belloli, S.; Rovere-Querini, P.; Fazio, F.; Manfredi, A.A.; Moresco, R.M. Evaluation of the role of tumor-associated macrophages in an experimental model of peritoneal carcinomatosis using (18)F-FDG PET. J. Nucl. Med. 2011, 52, 1770–1777. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.C.; Chen, J.H.; Liang, J.A.; Huang, W.S.; Cheng, K.Y.; Kao, C.H. PET or PET/CT for detection of peritoneal carcinomatosis: A meta-analysis. Clin. Nucl. Med. 2013, 38, 623–629. [Google Scholar] [CrossRef]
- Kim, S.J.; Lee, S.W. Diagnostic accuracy of. Br. J. Radiol. 2018, 91, 20170519. [Google Scholar] [CrossRef] [PubMed]
- Cunha, L.; Horvath, I.; Ferreira, S.; Lemos, J.; Costa, P.; Vieira, D.; Veres, D.S.; Szigeti, K.; Summavielle, T.; Máthé, D.; et al. Preclinical imaging: An essential ally in modern biosciences. Mol. Diagn. Ther. 2014, 18, 153–173. [Google Scholar] [CrossRef]
- Wong, K.P.; Sha, W.; Zhang, X.; Huang, S.C. Effects of administration route, dietary condition, and blood glucose level on kinetics and uptake of 18F-FDG in mice. J. Nucl. Med. 2011, 52, 800–807. [Google Scholar] [CrossRef]
- Kim, C.; Kim, I.H.; Kim, S.I.; Kim, Y.S.; Kang, S.H.; Moon, S.H.; Kim, T.S.; Kim, S.K. Comparison of the Intraperitoneal, Retroorbital and per Oral Routes for F-18 FDG Administration as Effective Alternatives to Intravenous Administration in Mouse Tumor Models Using Small Animal PET/CT Studies. Nucl. Med. Mol. Imaging 2011, 45, 169–176. [Google Scholar] [CrossRef][Green Version]
- Schiffer, W.K.; Mirrione, M.M.; Dewey, S.L. Optimizing experimental protocols for quantitative behavioral imaging with 18F-FDG in rodents. J. Nucl. Med. 2007, 48, 277–287. [Google Scholar]
- Aung, W.; Jin, Z.H.; Furukawa, T.; Claron, M.; Boturyn, D.; Sogawa, C.; Tsuji, A.B.; Wakizaka, H.; Fukumura, T.; Fujibayashi, Y.; et al. Micro-positron emission tomography/contrast-enhanced computed tomography imaging of orthotopic pancreatic tumor-bearing mice using the αvβ₃ integrin tracer ⁶⁴Cu-labeled cyclam-RAFT-c(-RGDfK-)₄. Mol. Imaging 2013, 12, 376–387. [Google Scholar] [CrossRef] [PubMed]
- Yoshii, Y.; Matsumoto, H.; Yoshimoto, M.; Oe, Y.; Zhang, M.R.; Nagatsu, K.; Sugyo, A.; Tsuji, A.B.; Higashi, T. Cu-Intraperitoneal Radioimmunotherapy: A Novel Approach for Adjuvant Treatment in a Clinically Relevant Preclinical Model of Pancreatic Cancer. J. Nucl. Med. 2019, 60, 1437–1443. [Google Scholar] [CrossRef]
- Lee, H.J.; Tantawy, M.N.; Nam, K.T.; Choi, I.; Peterson, T.E.; Price, R.R. Evaluation of an intraperitoneal ovarian cancer syngeneic mouse model using 18F-FDG MicroPET imaging. Int. J. Gynecol. Cancer 2011, 21, 22–27. [Google Scholar] [CrossRef] [PubMed]
- DeBerardinis, R.J.; Chandel, N.S. Fundamentals of cancer metabolism. Sci. Adv. 2016, 2, e1600200. [Google Scholar] [CrossRef]
- Schmidt, K.C.; Smith, C.B. Resolution, sensitivity and precision with autoradiography and small animal positron emission tomography: Implications for functional brain imaging in animal research. Nucl. Med. Biol. 2005, 32, 719–725. [Google Scholar] [CrossRef] [PubMed]
- Fanchon, L.M.; Dogan, S.; Moreira, A.L.; Carlin, S.A.; Schmidtlein, C.R.; Yorke, E.; Apte, A.P.; Burger, I.A.; Durack, J.C.; Erinjeri, J.P.; et al. Feasibility of in situ, high-resolution correlation of tracer uptake with histopathology by quantitative autoradiography of biopsy specimens obtained under 18F-FDG PET/CT guidance. J. Nucl. Med. 2015, 56, 538–544. [Google Scholar] [CrossRef]
- Dedrick, R.L.; Myers, C.E.; Bungay, P.M.; DeVita, V.T. Pharmacokinetic rationale for peritoneal drug administration in the treatment of ovarian cancer. Cancer Treat. Rep. 1978, 62, 1–11. [Google Scholar] [PubMed]
- Sugarbaker, P.H. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in the management of gastrointestinal cancers with peritoneal metastases: Progress toward a new standard of care. Cancer Treat. Rev. 2016, 48, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Flood, M.; Narasimhan, V.; Waters, P.; Ramsay, R.; Michael, M.; Warrier, S.; Heriot, A. Survival after cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for colorectal peritoneal metastases: A systematic review and discussion of latest controversies. Surgeon 2020. [Google Scholar] [CrossRef]
- Mitchell, G.S.; Gill, R.K.; Boucher, D.L.; Li, C.; Cherry, S.R. In vivo Cerenkov luminescence imaging: A new tool for molecular imaging. Philos. Trans. A Math Phys. Eng. Sci. 2011, 369, 4605–4619. [Google Scholar] [CrossRef]
- Tamura, R.; Pratt, E.C.; Grimm, J. Innovations in Nuclear Imaging Instrumentation: Cerenkov Imaging. Semin. Nucl. Med. 2018, 48, 359–366. [Google Scholar] [CrossRef]
- Liu, H.; Carpenter, C.M.; Jiang, H.; Pratx, G.; Sun, C.; Buchin, M.P.; Gambhir, S.S.; Xing, L.; Cheng, Z. Intraoperative imaging of tumors using Cerenkov luminescence endoscopy: A feasibility experimental study. J. Nucl. Med. 2012, 53, 1579–1584. [Google Scholar] [CrossRef]
- Lábadi, A.; Balogh, P. Differential preferences in serosal homing and distribution of peritoneal B-cell subsets revealed by in situ CFSE labeling. Int. Immunol. 2009, 21, 1047–1056. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BcDLFL.1 Mouse Lymphoma Cells (n = 6 Measurements) | Healthy Mouse White Blood Cells (n = 6 Measurements) | Mean Lymphoma to Healthy Cell Uptake Proportions | |
|---|---|---|---|
| Mean (SD) Ratio of Counts Per Minute | Mean (SD) Ratio of Counts Per Minute | 14.77 | |
| Cell Pellet to Whole Incubate | 47.56% (3.22%) | 2.77% (2.22%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ritter, Z.; Zámbó, K.; Jia, X.; Szöllősi, D.; Dezső, D.; Alizadeh, H.; Horváth, I.; Hegedűs, N.; Tuch, D.; Vyas, K.; et al. Intraperitoneal Glucose Transport to Micrometastasis: A Multimodal In Vivo Imaging Investigation in a Mouse Lymphoma Model. Int. J. Mol. Sci. 2021, 22, 4431. https://doi.org/10.3390/ijms22094431
Ritter Z, Zámbó K, Jia X, Szöllősi D, Dezső D, Alizadeh H, Horváth I, Hegedűs N, Tuch D, Vyas K, et al. Intraperitoneal Glucose Transport to Micrometastasis: A Multimodal In Vivo Imaging Investigation in a Mouse Lymphoma Model. International Journal of Molecular Sciences. 2021; 22(9):4431. https://doi.org/10.3390/ijms22094431
Chicago/Turabian StyleRitter, Zsombor, Katalin Zámbó, Xinkai Jia, Dávid Szöllősi, Dániel Dezső, Hussain Alizadeh, Ildikó Horváth, Nikolett Hegedűs, David Tuch, Kunal Vyas, and et al. 2021. "Intraperitoneal Glucose Transport to Micrometastasis: A Multimodal In Vivo Imaging Investigation in a Mouse Lymphoma Model" International Journal of Molecular Sciences 22, no. 9: 4431. https://doi.org/10.3390/ijms22094431
APA StyleRitter, Z., Zámbó, K., Jia, X., Szöllősi, D., Dezső, D., Alizadeh, H., Horváth, I., Hegedűs, N., Tuch, D., Vyas, K., Balogh, P., Máthé, D., & Schmidt, E. (2021). Intraperitoneal Glucose Transport to Micrometastasis: A Multimodal In Vivo Imaging Investigation in a Mouse Lymphoma Model. International Journal of Molecular Sciences, 22(9), 4431. https://doi.org/10.3390/ijms22094431