
Nourin-Associated miRNAs: Novel Inflammatory Monitoring Markers for Cyclocreatine Phosphate Therapy in Heart Failure



 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Results
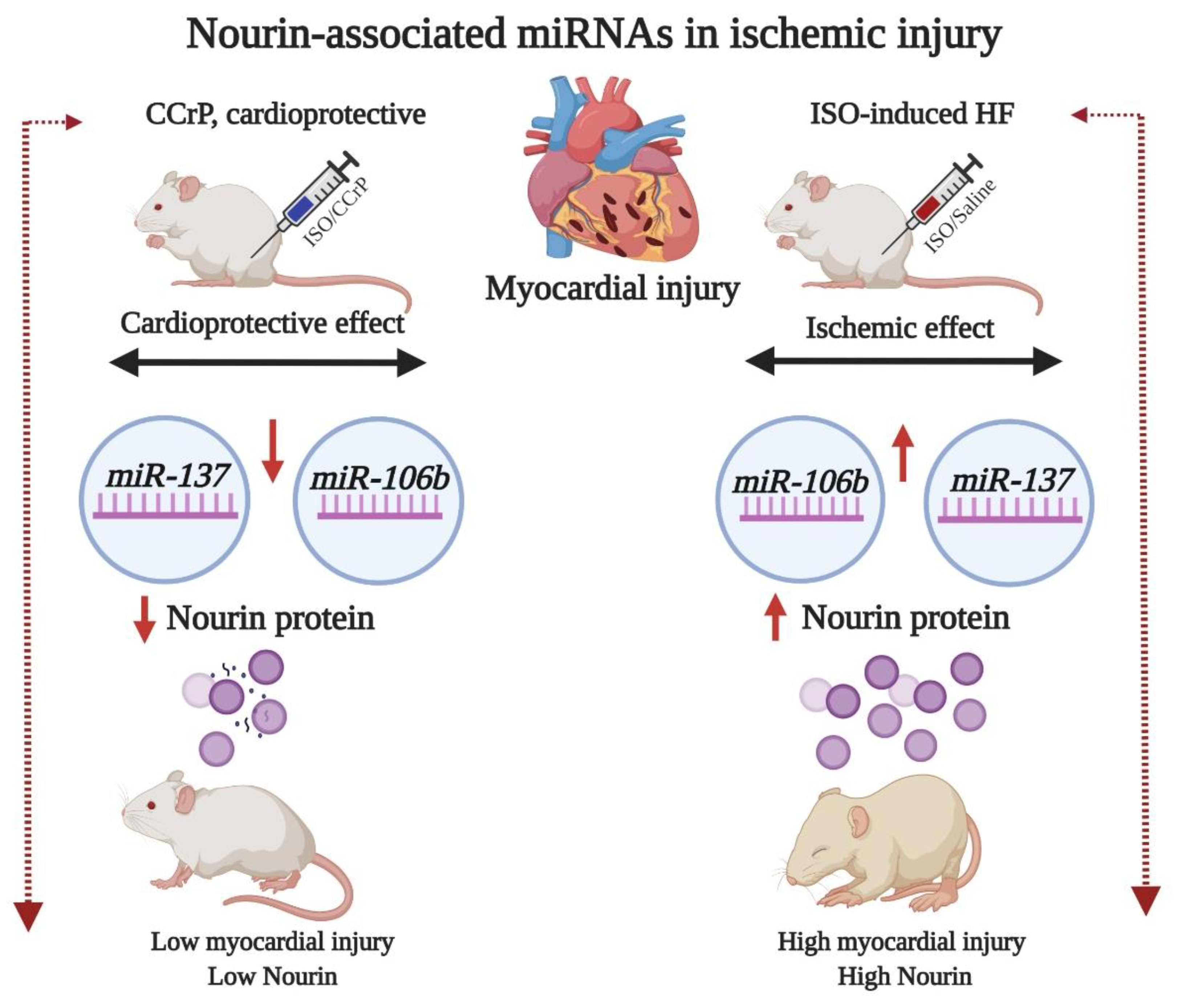
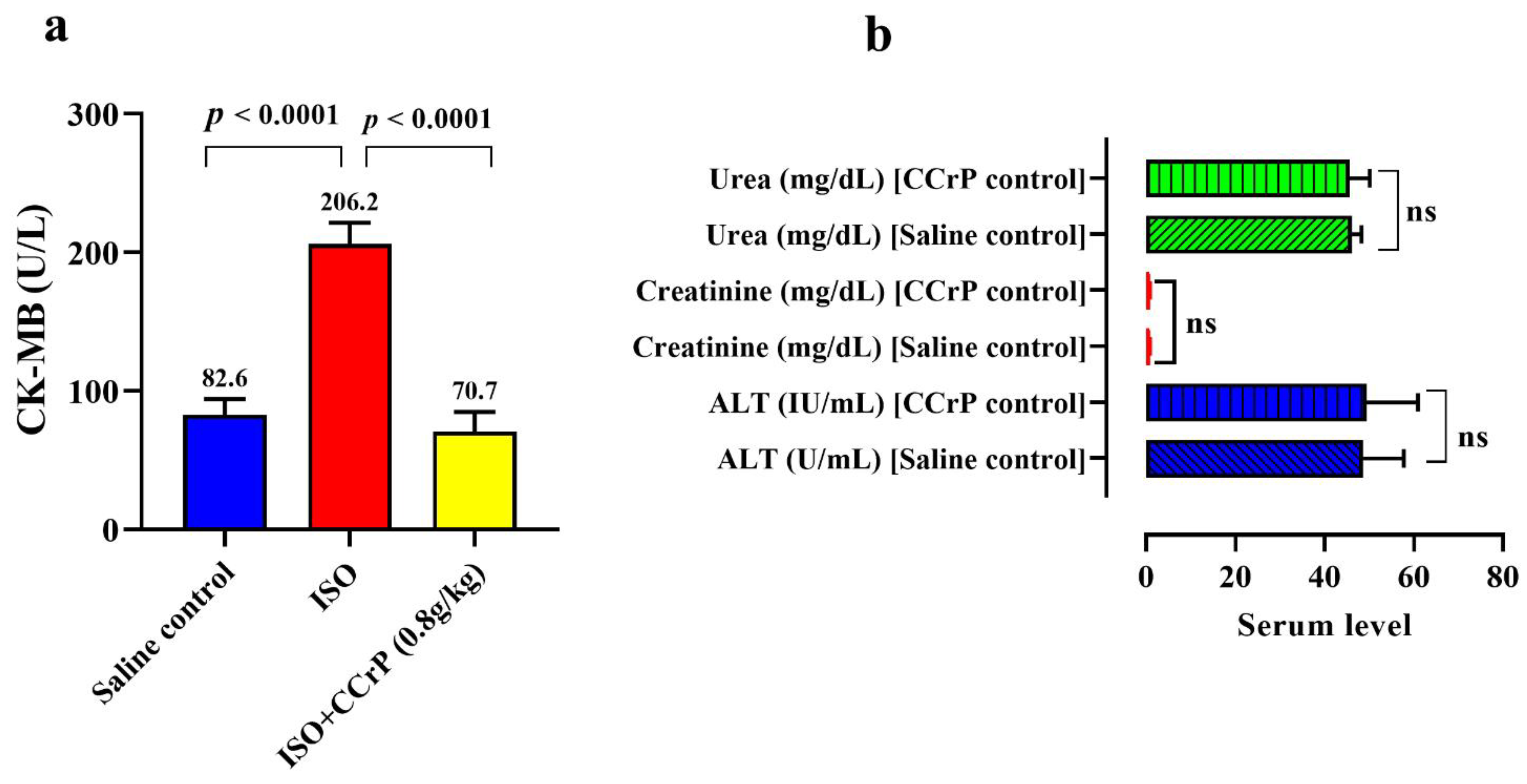
2.1. Cyclocreatine Phosphate Prevents Myocardial Ischemic Injury and Safety Studies
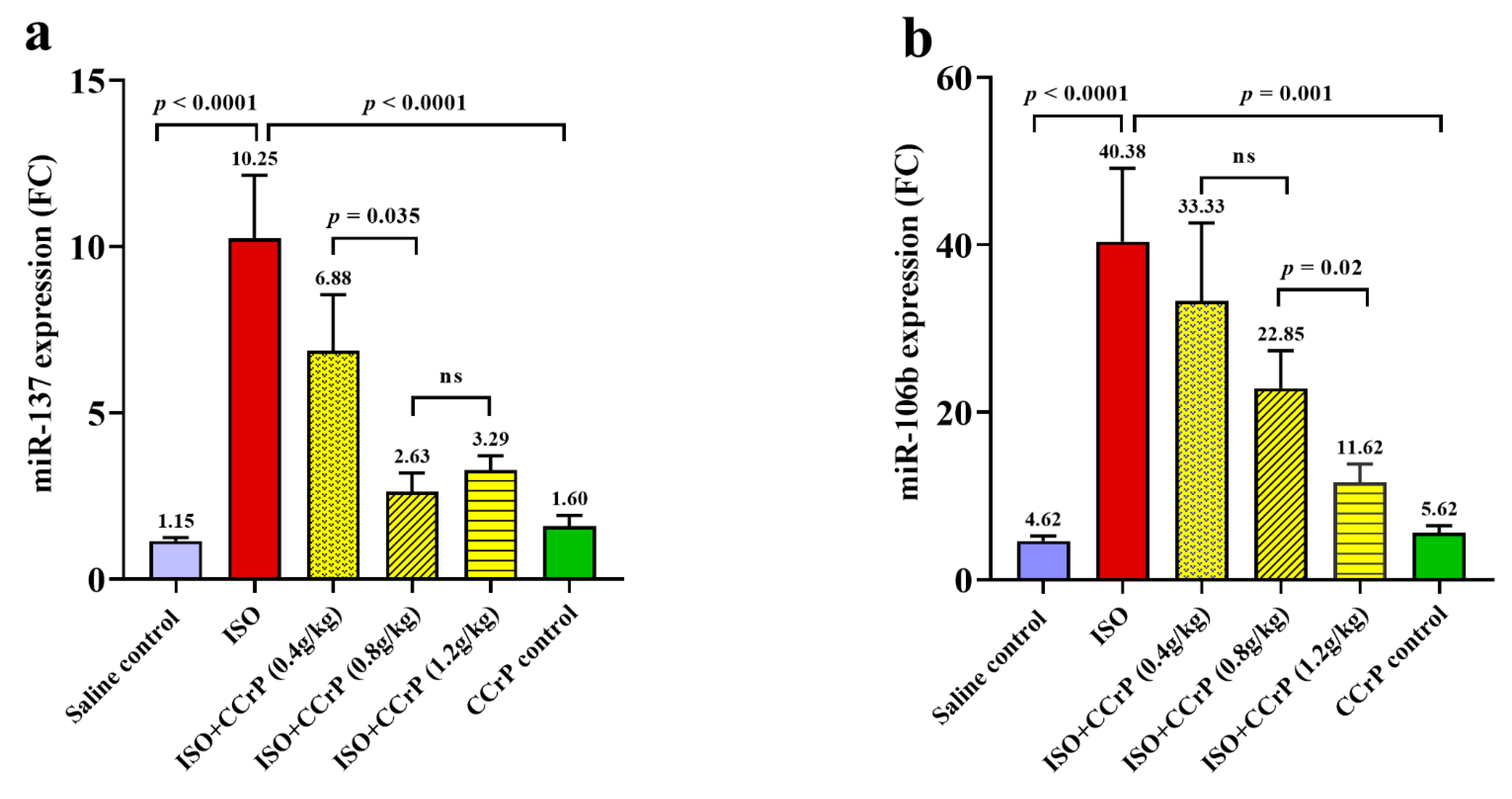
2.2. Gene Expression Levels of Nourin-Associated miR-137 and miR-106b-5b
2.3. Effect of Cyclocreatine Phosphate on Nourin-Associated miR-137 and miR-106b-5p
3. Discussion
4. Materials and Methods
4.1. Bioinformatics Analysis
4.2. Experimental ISO Rat Model (ISO/Saline “HF Rats” and ISO/CCrP “Non-HF Rats”)
4.3. Biochemical Assessment
4.4. Molecular Assessment of Nourin-Associated miR-137 and miR-106b-5p
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AMI | acute myocardial infarction |
| ACT | alpha 1-antichymotrypsin |
| ALT | alanine transaminases |
| CK-MB | creatine kinase-myocardial band |
| CCr | cyclocreatine |
| CCrP | cyclocreatine phosphate |
| EF | ejection fraction |
| DEGs | differentially expressed genes |
| ELAM-1 | endothelial cell leukocyte adhesion molecule-1 |
| GO | gene ontology |
| HF | heart failure |
| HRM | High resolution melting |
| ICAM-1 | intercellular adhesion molecule 1 |
| IL-6 | interleukin 6 |
| IL-8 | interleukin 8 |
| IL-1β | interleukin 1β |
| ISO | isoproterenol |
| KEGG | Kyoto Encyclopedia of Genes and Genomes |
| LECAM-1 | leukocyte-endothelial cell adhesion molecule 1 |
| LV | left ventricular |
| miR | microRNA |
| MI | myocardial injury |
| STEMI | ST elevation myocardial infarction |
| TNF-α | tumor necrosis factor alpha |
| UA | unstable angina |
| VECs | vascular endothelial cells |
| LFA-1 | lymphocyte function-associated antigen |
References
- Reed, G.W.; Rossi, J.E.; Cannon, C.P. Acute myocardial infarction. Lancet 2017, 389, 197–210. [Google Scholar] [CrossRef]
- Von Haehling, S.; Jankowska, E.A.; Anker, S.D. Tumour necrosis factor-alpha and the failing heart--pathophysiology and therapeutic implications. Basic Res. Cardiol. 2004, 99, 18–28. [Google Scholar] [CrossRef]
- Rauchhaus, M.; Doehner, W.; Francis, D.P.; Davos, C.; Kemp, M.; Liebenthal, C.; Niebauer, J.; Hooper, J.; Volk, H.D.; Coats, A.J.; et al. Plasma cytokine parameters and mortality in patients with chronic heart failure. Circulation 2001, 3, 54–55. [Google Scholar]
- Anker, S.D.; Von Haehling, S. Inflammatory mediators in chronic heart failure: An overview. Heart 2004, 90, 464–470. [Google Scholar] [CrossRef]
- Azzam, Z.S.; Kinaneh, S.; Bahouth, F.; Ismael-Badarneh, R.; Khoury, E.; Abassi, Z. Involvement of Cytokines in the Path-ogenesis of Salt and Water Imbalance in Congestive Heart Failure. Front. Immunol. Hypothesis Theory 2017, 8, 716. [Google Scholar] [CrossRef]
- Elgebaly, S.A.; Poston, R.; Todd, R.; Helmy, T.; Almaghraby, A.M.; Elbayoumi, T.; Kreutzer, D.L.; Taegtmeyer, H.; Elgebaly, S. Cyclocreatine protects against ischemic injury and enhances cardiac recovery during early reperfusion. Expert Rev. Cardiovasc. 2019, 17, 683–697. [Google Scholar] [CrossRef]
- Elgebaly, S.A.; Hashmi, F.H.; Houser, S.L.; Allam, M.E.; Doyle, K. Cardiac-derived neutrophil chemotactic factors: De-tection in coronary sinus effluents of patients undergoing myocardial revascularization. J. Thorac. Cardiovasc. Surg. 1992, 103, 952–959. [Google Scholar] [CrossRef]
- Elgebaly, S.A.; Masetti, P.; Allam, M.; Forouhar, F. Cardiac derived neutrophil chemotactic factors; preliminary bio-chemical characterization. J. Mol. Cell. Cardiol. 1989, 21, 585–593. [Google Scholar] [CrossRef]
- Elgebaly, S.A.; Van Buren, C.; Todd, R.; Poston, R.; Rabie, M.A.; Mohamed, A.F.; Ahmed, L.A.; El Sayed, N.S. Cyclocreatine Phosphate: A Novel Mechanism for Preventing De-velopment of Heart Failure. Circulation 2020, 142, A13311. [Google Scholar]
- Elgebaly, S.A.; Christenson, R.H.; Kandil, H.; El-Khazragy, N.; Rashed, L.; Yacoub, B.; Sharafieh, R.; Klueh, U.; Kreutzer, D.L. Abstract 13051: Nourin-dependent Mirna-137: A Novel Early Diagnostic Biomarker for Unstable Angina Patients. Circulation 2020, 142, A13051. [Google Scholar] [CrossRef]
- Elgebaly, S.A.; Christenson, R.H.; Kandil, H.; El-Khazragy, N.; Rashed, L.; Yacoub, B.; Sharafieh, R.; Klueh, U.; Kreutzer, D.L. Nourin-dependent Mirna-106b: A Novel Early Inflammatory Diagnostic Biomarker for Cardiac Injury. Circulation 2020, 142, A13103. [Google Scholar] [CrossRef]
- Elgebaly, S.A. Nourexal: A Novel Anti-inflammatory/Antiapoptotic Therapy against Reperfusion Injury. J. Clin. Exp. Cardiol. 2016, 7, 33. [Google Scholar]
- Elgebaly, S.; Christenson, R.; Schiffmann, E.; Yi, Q.; Kreutzer, D. Early identification of cardiac ischemia patients in the emergency de-partment. Catheter. Cardiovasc. Interv. 2013, 81, S2–S3. [Google Scholar]
- Elgebaly, S.A.; Christenson, R.H.; Kandil, H.; El-Khazragy, N.; Rashed, L.; Yacoub, B.; Eldeeb, H.; Ali, M.; Sharafieh, R.; Klueh, U.; et al. Nourin-Dependent miR-137 and miR-106b: Novel Early Inflammatory Diagnostic Biomarkers for Unstable Angina Patients. Biomolecules 2021, 11, 368. [Google Scholar] [CrossRef] [PubMed]
- Guzun, R.; Timohhina, N.; Tepp, K.; Gonzalez-Granillo, M.; Shevchuk, I.; Chekulayev, V.; Kuznetsov, A.V.; Kaambre, T.; Saks, V. Systems bioenergetics of creatine kinase networks: Physiological roles of creatine and phosphocreatine in regulation of cardiac cell function. Amino Acids 2011, 40, 1333–1348. [Google Scholar] [CrossRef] [PubMed]
- Mayr, B.; Niebauer, J.; Breitenbach-Koller, H. Circulating miRNAs as predictors for morbidity and mortality in coronary artery disease. Mol. Biol. Rep. 2019, 46, 5661–5665. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Tong, Z.; Chen, K.; Hu, X.; Jin, H.; Hou, M. The Role of miRNA-132 against Apoptosis and Oxidative Stress in Heart Failure. BioMed Res. Int. 2018, 2018, 3452748. [Google Scholar] [CrossRef] [PubMed]
- Neupane, B.; Zhou, Q.; Gawaz, M.; Gramlich, M. Personalized medicine in inflammatory cardiomyopathy. Pers. Med. 2018, 15, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Li, W.; Wu, J.; Han, M.; Li, B. The diagnostic value of circulating microRNAs in heart failure (Review). Exp. Med. 2019, 17, 1985–2003. [Google Scholar] [CrossRef] [PubMed]
- Sassi, Y.; Avramopoulos, P.; Ramanujam, D.; Grüter, L.; Werfel, S.; Giosele, S.; Brunner, A.-D.; Esfandyari, D.; Papadopoulou, A.S.; De Strooper, B.; et al. Cardiac myocyte miR-29 promotes pathological remodeling of the heart by activating Wnt signaling. Nat. Commun. 2017, 8, 1614. [Google Scholar] [CrossRef]
- Sheikh, S.A.; Salma, U.; Zhang, B.; Chen, J.; Zhuang, J.; Ping, Z. Diagnostic, Prognostic, and Therapeutic Value of Circulating miRNAs in Heart Failure Patients Associated with Oxidative Stress. Oxid. Med. Cell. Longev. 2016, 2016, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Patrick, D.M.; Montgomery, R.L.; Qi, X.; Obad, S.; Kauppinen, S.; Hill, J.A.; Van Rooij, E.; Olson, E.N. Stress-dependent cardiac remodeling occurs in the absence of microRNA-21 in mice. J. Clin. Investig. 2010, 120, 3912–3916. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, B.A.; Semus, H.M.; Montgomery, R.L.; Stack, C.; Latimer, P.A.; Lewton, S.M.; Lynch, J.M.; Hullinger, T.G.; Seto, A.G.; van Rooij, E. Plasma microRNAs serve as biomarkers of therapeutic efficacy and disease progression in hypertension-induced heart failure. Eur. J. Heart Fail. 2013, 15, 650–659. [Google Scholar] [CrossRef] [PubMed]
- Lok, S.; Van Mil, A.; Bovenschen, N.; Van Der Weide, P.; Van Kuik, J.; Van Wichen, D.; Peeters, T.; Siera, E.; Winkens, B.; Sluijter, J.; et al. Post-Transcriptional Regulation of alpha-1-Antichymotrypsin by miR-137 in Chronic Heart Failure and Mechanical Support. J. Heart Lung Transplant. 2013, 32, S96–S97. [Google Scholar] [CrossRef]
- Chen, C.; Ponnusamy, M.; Liu, C.; Gao, J.; Wang, K.; Li, P. MicroRNA as a Therapeutic Target in Cardiac Remodeling. BioMed Res. Int. 2017, 2017, 1278436. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Azhar, G.; Williams, E.D.; Rogers, S.C.; Wei, J.Y. MicroRNA Clusters in the Adult Mouse Heart: Age-Associated Changes. BioMed Res. Int. 2015, 2015, 732397. [Google Scholar] [CrossRef]
- Slenter, D.N.; Kutmon, M.; Hanspers, K.; Riutta, A.; Windsor, J.; Nunes, N.; Mélius, J.; Cirillo, E.; Coort, S.L.; Digles, D.; et al. WikiPathways: A multifaceted pathway database bridging metabolomics to other omics research. Nucleic Acids Res. 2018, 46, D661–D667. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.V.; Rong, J.; Larson, M.G.; Yeri, A.; Ziegler, O.; Tanriverdi, K.; Murthy, V.; Liu, X.; Xiao, C.; Pico, A.R.; et al. Associations of Circulating Extracellular RNAs With Myocardial Remodeling and Heart Failure. JAMA Cardiol. 2018, 3, 871–876. [Google Scholar] [CrossRef] [PubMed]
- Khan, V.; Sharma, S.; Bhandari, U.; Ali, S.M.; Haque, S.E. Raspberry ketone protects against isoproterenol-induced myocardial infarction in rats. Life Sci. 2018, 194, 205–212. [Google Scholar] [CrossRef]
- Fan, C.; Tang, X.; Ye, M.; Zhu, G.; Dai, Y.; Yao, Z.; Yao, X. Qi-Li-Qiang-Xin Alleviates Isoproterenol-Induced Myocardial Injury by Inhibiting Excessive Autophagy via Activating AKT/mTOR Pathway. Front. Pharm. 2019, 10, 1329. [Google Scholar] [CrossRef]
- Chen, Z.; Li, C.; Lin, K.; Zhang, Q.; Chen, Y.; Rao, L. MicroRNAs in acute myocardial infarction: Evident value as novel biomarkers? Anatol. J. Cardiol. 2018, 19, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, M.S.A. Diagnostic Role of Plasma MicroRNA-21 in Stable and Unstable Angina Patients and Association with Aging. Cardiol. Res. Pract. 2020, 2020, 9093151. [Google Scholar]
- Zhang, Y.; Liu, Y.-J.; Liu, T.; Zhang, H.; Yang, S.-J. Plasma microRNA-21 is a potential diagnostic biomarker of acute myocardial infarction. Eur. Rev. Med. Pharm. Sci. 2016, 20, 323–329. [Google Scholar]
- Mohamed, S.S.; Ahmed, L.A.; Attia, W.A.; Khattab, M.M. Nicorandil enhances the efficacy of mesenchymal stem cell therapy in iso-proterenol-induced heart failure in rats. Biochem. Pharm. 2015, 98, 403–411. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elgebaly, S.A.; Todd, R.; Kreutzer, D.L.; Christenson, R.; El-Khazragy, N.; Arafa, R.K.; Rabie, M.A.; Mohamed, A.F.; Ahmed, L.A.; El Sayed, N.S. Nourin-Associated miRNAs: Novel Inflammatory Monitoring Markers for Cyclocreatine Phosphate Therapy in Heart Failure. Int. J. Mol. Sci. 2021, 22, 3575. https://doi.org/10.3390/ijms22073575
Elgebaly SA, Todd R, Kreutzer DL, Christenson R, El-Khazragy N, Arafa RK, Rabie MA, Mohamed AF, Ahmed LA, El Sayed NS. Nourin-Associated miRNAs: Novel Inflammatory Monitoring Markers for Cyclocreatine Phosphate Therapy in Heart Failure. International Journal of Molecular Sciences. 2021; 22(7):3575. https://doi.org/10.3390/ijms22073575
Chicago/Turabian StyleElgebaly, Salwa A., Robert Todd, Donald L. Kreutzer, Robert Christenson, Nashwa El-Khazragy, Reem K. Arafa, Mostafa A. Rabie, Ahmed F. Mohamed, Lamiaa A. Ahmed, and Nesrine S. El Sayed. 2021. "Nourin-Associated miRNAs: Novel Inflammatory Monitoring Markers for Cyclocreatine Phosphate Therapy in Heart Failure" International Journal of Molecular Sciences 22, no. 7: 3575. https://doi.org/10.3390/ijms22073575
APA StyleElgebaly, S. A., Todd, R., Kreutzer, D. L., Christenson, R., El-Khazragy, N., Arafa, R. K., Rabie, M. A., Mohamed, A. F., Ahmed, L. A., & El Sayed, N. S. (2021). Nourin-Associated miRNAs: Novel Inflammatory Monitoring Markers for Cyclocreatine Phosphate Therapy in Heart Failure. International Journal of Molecular Sciences, 22(7), 3575. https://doi.org/10.3390/ijms22073575