
Pathophysiology and Molecular Imaging of Diabetic Foot Infections


Abstract
1. Introduction
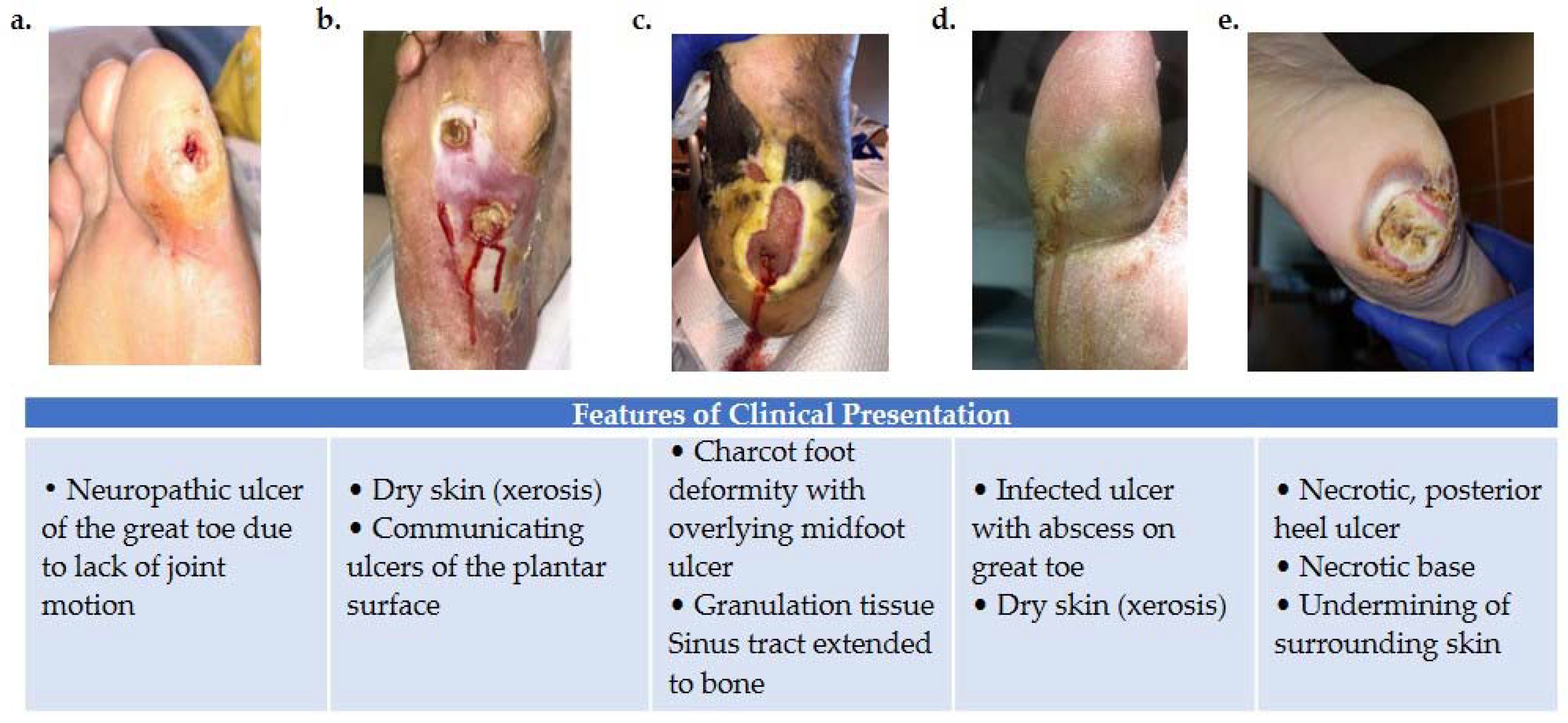
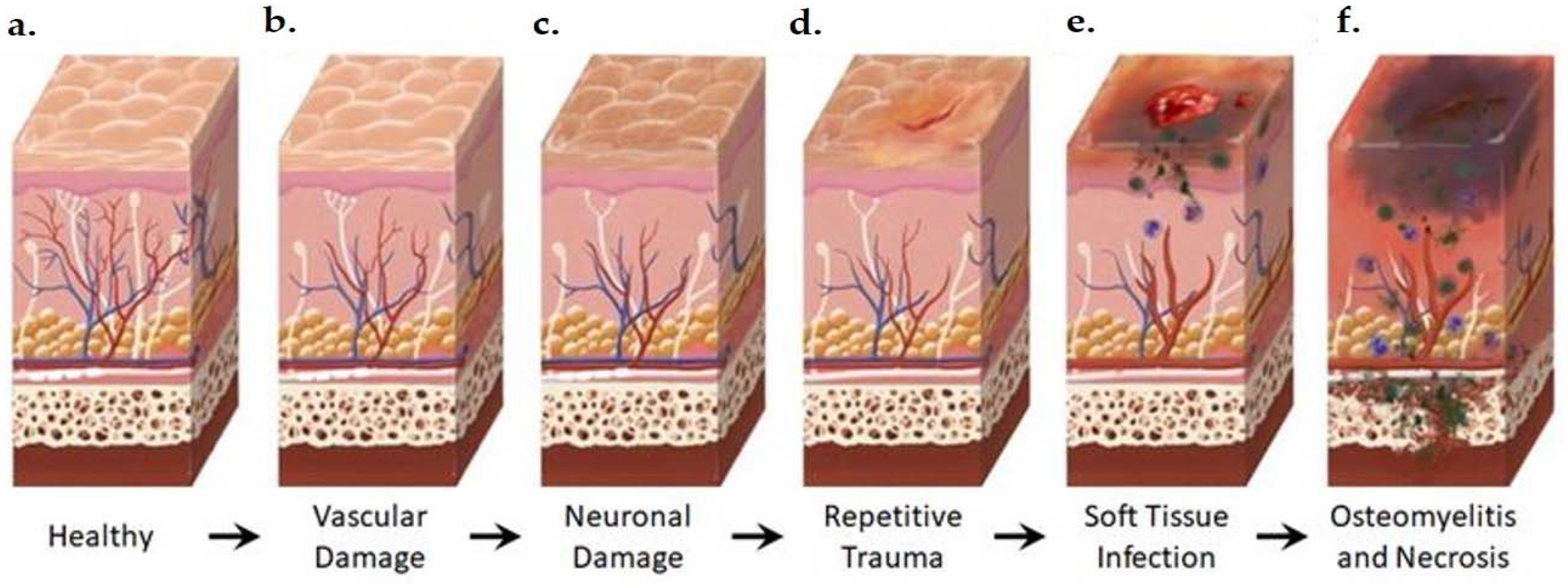
2. Pathophysiology and Clinical Assessment of DFI
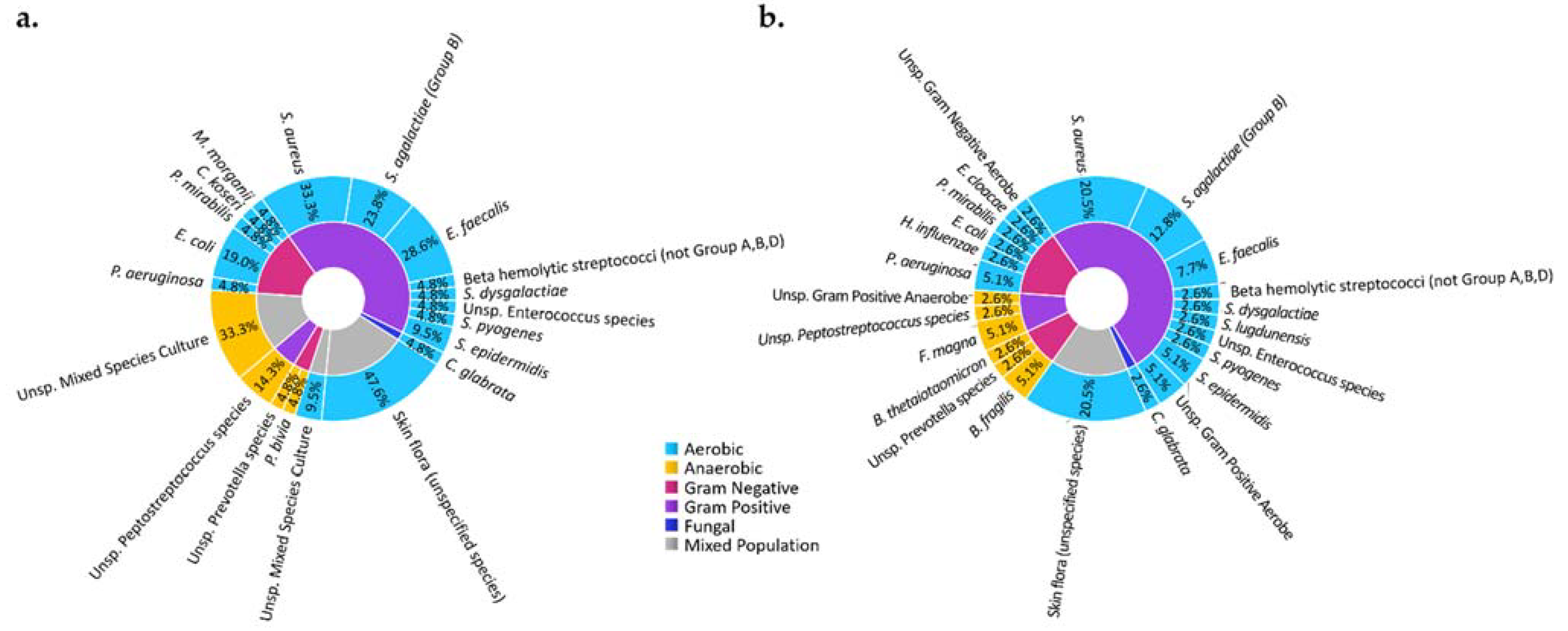
2.1. Diabetic Susceptibility to DFI
2.2. Clinical Diagnostic Tests
2.3. Molecular Mechanisms of DFI Features
3. Imaging Modalities
3.1. Anatomical Modalities
3.1.1. Radiography
3.1.2. Ultrasonography
3.1.3. Computed Tomography (CT)
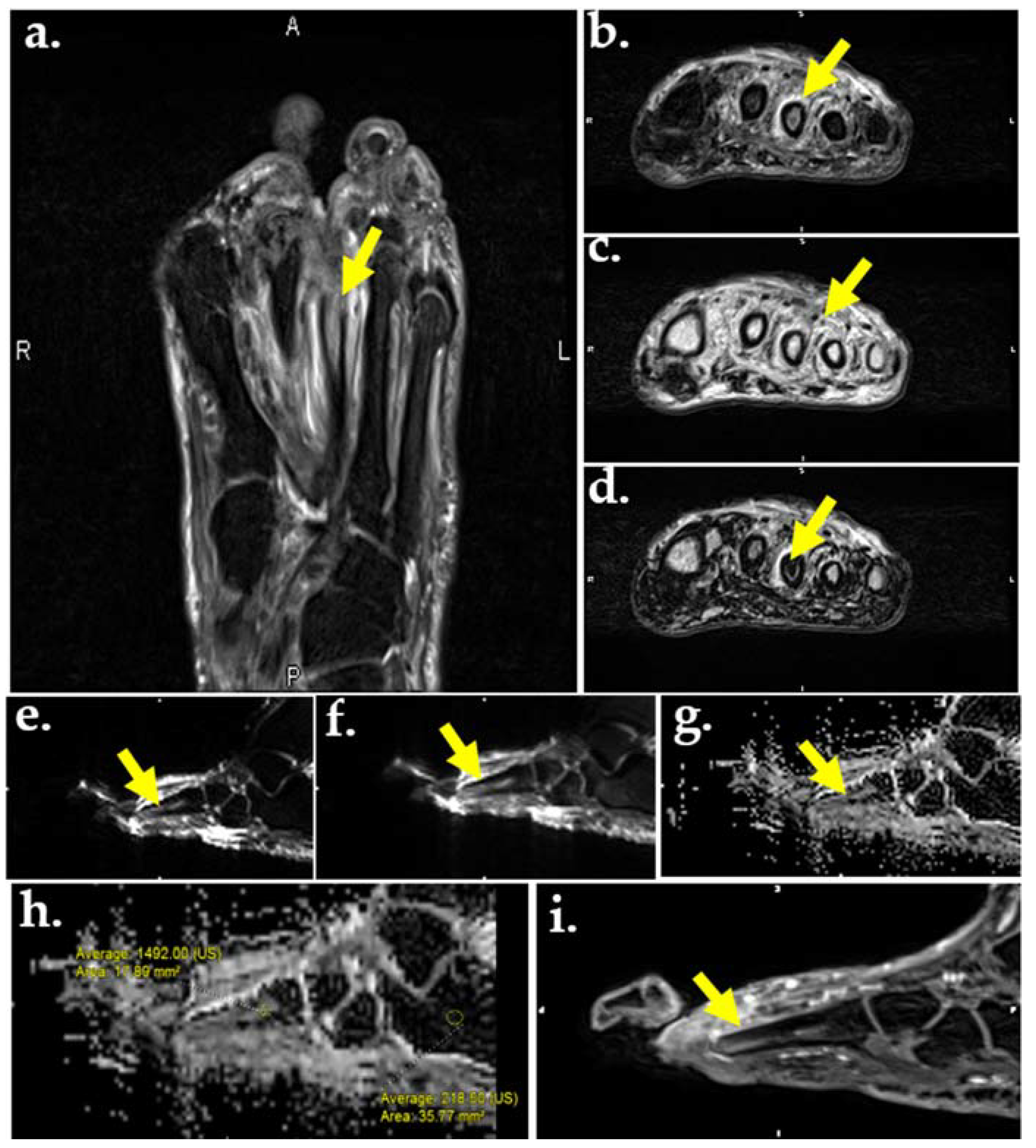
3.1.4. Magnetic Resonance
3.2. Molecular Imaging
3.2.1. Bone Scintigraphy
3.2.2. Radiolabeled WBC and Bone Marrow Planar Scintigraphy, SPECT, and SPECT/CT
3.2.3. 18F-FDG PET and PET/CT
3.2.4. Gallium Scan
4. Emerging Radiotracers in Infection Imaging
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. National Diabetes Statistics Report. 2017. Available online: cdc.gov/media/releases/2017/p0718-diabetes-report.html (accessed on 8 October 2019).
- Frykberg, R.G.; Wittmayer, B.; Zgonis, T. Surgical management of diabetic foot infections and osteomyelitis. Clin. Podiatr. Med. Surg. 2007, 24, 469–482. [Google Scholar] [CrossRef] [PubMed]
- Lipsky, B.A. Bone of contention: Diagnosing diabetic foot osteomyelitis. Clin. Infect. Dis. 2008, 47, 528–530. [Google Scholar] [CrossRef]
- Zhang, P.; Lu, J.; Jing, Y.; Tang, S.; Zhu, D.; Bi, Y. Global epidemiology of diabetic foot ulceration: A systematic review and meta-analysis. Ann. Med. 2017, 49, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.; Sun, X.; Wang, W.; Jiang, K. A study of prognostic factors in Chinese patients with diabetic foot ulcers. Diabet. Foot Ankle 2014, 5, 22936. [Google Scholar] [CrossRef]
- Gilliver, S.C.; Ashcroft, G.S. Sex steroids and cutaneous wound healing: The contrasting influences of estrogens and androgens. Climacteric 2007, 10, 276–288. [Google Scholar] [CrossRef] [PubMed]
- Vuorlaakso, M.; Kiiski, J.; Salonen, T.; Karppelin, M.; Helminen, M.; Kaartinen, I. Major Amputation Profoundly Increases Mortality in Patients with Diabetic Foot Infection. Front. Surg. 2021, 8, 655902. [Google Scholar] [CrossRef] [PubMed]
- Amoah, V.M.K.; Anokye, R.; Acheampong, E.; Dadson, H.R.; Osei, M.; Nadutey, A. The experiences of people with diabetes-related lower limb amputation at the Komfo Anokye Teaching Hospital (KATH) in Ghana. BMC Res. Notes 2018, 11, 66. [Google Scholar] [CrossRef]
- Raghav, A.; Khan, Z.A.; Labala, R.K.; Ahmad, J.; Noor, S.; Mishra, B.K. Financial burden of diabetic foot ulcers to world: A progressive topic to discuss always. Ther. Adv. Endocrinol. Metab. 2018, 9, 29–31. [Google Scholar] [CrossRef] [PubMed]
- Barshes, N.R.; Sigireddi, M.; Wrobel, J.S.; Mahankali, A.; Robbins, J.M.; Kougias, P.; Armstrong, D.G. The system of care for the diabetic foot: Objectives, outcomes, and opportunities. Diabet. Foot Ankle 2013, 4, 21847. [Google Scholar] [CrossRef] [PubMed]
- Hicks, C.W.; Selvarajah, S.; Mathioudakis, N.; Sherman, R.E.; Hines, K.F.; Black, J.H.; Abularrage, C.J. Burden of Infected Diabetic Foot Ulcers on Hospital Admissions and Costs. Ann. Vasc. Surg. 2016, 33, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Lipsky, B.A.; Berendt, A.R.; Deery, H.G.; Embil, J.M.; Joseph, W.S.; Karchmer, A.W.; LeFrock, J.L.; Lew, D.P.; Mader, J.T.; Norden, C.; et al. Diagnosis and treatment of diabetic foot infections. Plast. Reconstr. Surg. 2006, 117, 212S–238S. [Google Scholar] [CrossRef] [PubMed]
- Ponirakis, G.; Elhadd, T.; Chinnaiyan, S.; Dabbous, Z.; Siddiqui, M.; Al-Muhannadi, H.; Petropoulos, I.N.; Khan, A.; Ashawesh, K.A.E.; Dukhan, K.M.O.; et al. Prevalence and management of diabetic neuropathy in secondary care in Qatar. Diabetes Metab. Res. Rev. 2020, 36, e3286. [Google Scholar] [CrossRef] [PubMed]
- Juster-Switlyk, K.; Smith, A.G. Updates in diabetic peripheral neuropathy. F1000Research 2016, 5, 738. [Google Scholar] [CrossRef]
- Gregg, E.W.; Gu, Q.; Williams, D.; de Rekeneire, N.; Cheng, Y.J.; Geiss, L.; Engelgau, M. Prevalence of lower extremity diseases associated with normal glucose levels, impaired fasting glucose, and diabetes among U.S. adults aged 40 or older. Diabetes Res. Clin. Pract. 2007, 77, 485–488. [Google Scholar] [CrossRef]
- Candrilli, S.D.; Davis, K.L.; Kan, H.J.; Lucero, M.A.; Rousculp, M.D. Prevalence and the associated burden of illness of symptoms of diabetic peripheral neuropathy and diabetic retinopathy. J. Diabetes Complicat. 2007, 21, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Bader, M.S. Diabetic foot infection. Am. Fam. Physician 2008, 78, 71–79. [Google Scholar] [PubMed]
- Ababneh, A.; Bakri, F.G.; Khader, Y.; Lazzarini, P.; Ajlouni, K. Prevalence and Associates of Foot Deformities among Patients with Diabetes in Jordan. Curr. Diabetes Rev. 2020, 16, 471–482. [Google Scholar] [CrossRef]
- Lung, C.W.; Wu, F.L.; Zhang, K.; Liau, B.Y.; Townsend, R.; Jan, Y.K. Using elastographic ultrasound to assess plantar tissue stiffness after waking at different speeds and durations. Appl. Sci. 2020, 10, 7498. [Google Scholar] [CrossRef]
- Wanzou, J.P.V.; Sekimpi, P.; Komagum, J.O.; Nakwagala, F.; Mwaka, E.S. Charcot arthropathy of the diabetic foot in a sub-Saharan tertiary hospital: A cross-sectional study. J. Foot Ankle Res. 2019, 12, 33. [Google Scholar] [CrossRef]
- Wukich, D.K.; Sung, W. Charcot arthropathy of the foot and ankle: Modern concepts and management review. J. Diabetes Complicat. 2009, 23, 409–426. [Google Scholar] [CrossRef] [PubMed]
- Bandyk, D.F. The diabetic foot: Pathophysiology, evaluation, and treatment. Semin. Vasc. Surg. 2018, 31, 43–48. [Google Scholar] [CrossRef]
- Boulton, A.J.M. Diabetic neuropathy and foot complications. In Diabetes and the Nervous System; Elsevier: Amsterdam, The Netherlands, 2014; Volume 126, pp. 97–107. ISBN 1612764452. [Google Scholar]
- Giurato, L.; Meloni, M.; Izzo, V.; Uccioli, L. Osteomyelitis in diabetic foot: A comprehensive overview. World J. Diabetes 2017, 8, 135. [Google Scholar] [CrossRef]
- Boulton, A.J.M.; Kirsner, R.S.; Vileikyte, L. Neuropathic diabetic foot ulcers. N. Engl. J. Med. 2004, 351, 48–55. [Google Scholar] [CrossRef]
- Lázaro-Martínez, J.L.; Tardáguila-García, A.; García-Klepzig, J.L. Diagnostic and therapeutic update on diabetic foot osteomyelitis. Endocrinol. Diabetes Nutr. 2017, 64, 100–108. [Google Scholar] [CrossRef]
- Lavery, L.A.; Crisologo, P.A.; La Fontaine, J.; Bhavan, K.; Oz, O.K.; Davis, K.E. Are We Misdiagnosing Diabetic Foot Osteomyelitis? Is the Gold Standard Gold? J. Foot Ankle Surg. 2019, 58, 713–716. [Google Scholar] [CrossRef]
- Lipsky, B.A.; Berendt, A.R.; Cornia, P.B.; Pile, J.C.; Peters, E.J.G.; Armstrong, D.G.; Deery, H.G.; Embil, J.M.; Joseph, W.S.; Karchmer, A.W.; et al. Executive summary: 2012 Infectious Diseases Society of America clinical practice guideline for the diagnosis and treatment of diabetic foot infections. Clin. Infect. Dis. 2012, 54, 1679–1684. [Google Scholar] [CrossRef]
- Lavery, L.A.; Ryan, E.C.; Ahn, J.; Crisologo, P.A.; Oz, O.K.; La Fontaine, J.; Wukich, D.K. The Infected Diabetic Foot: Re-Evaluating the IDSA Diabetic Foot Infection Classification. Clin. Infect. Dis. 2019, 70, 1573–1579. [Google Scholar] [CrossRef]
- Lavery, L.A.; Armstrong, D.G.; Peters, E.J.G.; Lipsky, B.A. Probe-to-bone test for diagnosing diabetic foot osteomyelitis: Reliable or relic? Diabetes Care 2007, 30, 270–274. [Google Scholar] [CrossRef]
- Walton, D.M.; Minton, S.D.; Cook, A.D. The potential of transdermal nitric oxide treatment for diabetic peripheral neuropathy and diabetic foot ulcers. Diabetes Metab. Syndr. 2019, 13, 3053–3056. [Google Scholar] [CrossRef]
- Petrova, N.L.; Petrov, P.K.; Edmonds, M.E.; Shanahan, C.M. Novel use of a Dektak 150 surface profiler unmasks differences in resorption pit profiles between control and Charcot patient osteoclasts. Calcif. Tissue Int. 2014, 94, 403–411. [Google Scholar] [CrossRef]
- Ndip, A.; Williams, A.; Jude, E.B.; Serracino-Inglott, F.; Richardson, S.; Smyth, J.V.; Boulton, A.J.M.; Alexander, M.Y. The RANKL/RANK/OPG signaling pathway mediates medial arterial calcification in diabetic Charcot neuroarthropathy. Diabetes 2011, 60, 2187–2196. [Google Scholar] [CrossRef]
- Rask-Madsen, C.; King, G.L. Vascular complications of diabetes: Mechanisms of injury and protective factors. Cell Metab. 2013, 17, 20–33. [Google Scholar] [CrossRef] [PubMed]
- Burg, M.B.; Kador, P.F. Sorbitol, osmoregulation, and the complications of diabetes. J. Clin. Investig. 1988, 81, 635–640. [Google Scholar] [CrossRef]
- Tanenberg, R.J.; Donofrio, P.D. Neuropathic Problems of the Lower Limbs in Diabetic Patients. In Levin and O’Neal’s The Diabetic Foot; Bowker, J.H., Pfeifer, M.A., Eds.; Elsevier: Amsterdam, The Netherlands, 2007; pp. 33–74. ISBN 9780323041454. [Google Scholar]
- Hobizal, K.B.; Wukich, D.K. Diabetic foot infections: Current concept review. Diabet. Foot Ankle 2012, 3, 1849. [Google Scholar] [CrossRef]
- Insuela, D.; Coutinho, D.; Martins, M.; Ferrero, M.; Carvalho, V. Neutrophil Function Impairment Is a Host Susceptibility Factor to Bacterial Infection in Diabetes. In Cells of the Immune System; IntechOpen: London, UK, 2020. [Google Scholar]
- Demirdal, T.; Sen, P. The significance of neutrophil-lymphocyte ratio, platelet-lymphocyte ratio and lymphocyte-monocyte ratio in predicting peripheral arterial disease, peripheral neuropathy, osteomyelitis and amputation in diabetic foot infection. Diabetes Res. Clin. Pract. 2018, 144, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Charles, J.F.; Nakamura, M.C. Bone and the innate immune system. Curr. Osteoporos. Rep. 2014, 12, 1–8. [Google Scholar] [CrossRef]
- Seth, R.B.; Sun, L.; Ea, C.-K.; Chen, Z.J. Identification and characterization of MAVS, a mitochondrial antiviral signaling protein that activates NF-kappaB and IRF 3. Cell 2005, 122, 669–682. [Google Scholar] [CrossRef]
- Gao, L.; Liesveld, J.; Anolik, J.; Mcdavid, A.; Looney, R.J. IFNβ signaling inhibits osteogenesis in human SLE bone marrow. Lupus 2020, 29, 1040–1049. [Google Scholar] [CrossRef]
- Stacey, H.J.; Clements, C.S.; Welburn, S.C.; Jones, J.D. The prevalence of methicillin-resistant Staphylococcus aureus among diabetic patients: A meta-analysis. Acta Diabetol. 2019, 56, 907–921. [Google Scholar] [CrossRef]
- Lavery, L.A.; La Fontaine, J.; Bhavan, K.; Kim, P.J.; Williams, J.R.; Hunt, N.A. Risk factors for methicillin-resistant Staphylococcus aureus in diabetic foot infections. Diabet. Foot Ankle 2014, 5. [Google Scholar] [CrossRef]
- Saltoglu, N.; Ergonul, O.; Tulek, N.; Yemisen, M.; Kadanali, A.; Karagoz, G.; Batirel, A.; Ak, O.; Sonmezer, C.; Eraksoy, H.; et al. Influence of multidrug resistant organisms on the outcome of diabetic foot infection. Int. J. Infect. Dis. 2018, 70, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Icks, A.; Scheer, M.; Morbach, S.; Genz, J.; Haastert, B.; Giani, G.; Glaeske, G.; Hoffmann, F. Time-dependent impact of diabetes on mortality in patients after major lower extremity amputation: Survival in a population-based 5-year cohort in Germany. Diabetes Care 2011, 34, 1350–1354. [Google Scholar] [CrossRef] [PubMed]
- Kerr, M. Foot Care for People with Diabetes: The Economic Case for Change. In Supporting, Improving, Caring; Insight Health Economics: London, UK, 2012. [Google Scholar]
- Lauri, C.; Leone, A.; Cavallini, M.; Signore, A.; Giurato, L.; Uccioli, L. Diabetic Foot Infections: The Diagnostic Challenges. J. Clin. Med. 2020, 9, 1779. [Google Scholar] [CrossRef] [PubMed]
- Walker, E.A.; Beaman, F.D.; Wessell, D.E.; Cassidy, R.C.; Czuczman, G.J.; Demertzis, J.L.; Lenchik, L.; Motamedi, K.; Pierce, J.L.; Sharma, A.; et al. ACR Appropriateness Criteria® Suspected Osteomyelitis of the Foot in Patients With Diabetes Mellitus. J. Am. Coll. Radiol. 2019, 16, S440–S450. [Google Scholar] [CrossRef]
- Pineda, C.; Espinosa, R.; Pena, A. Radiographic imaging in osteomyelitis: The role of plain radiography, computed tomography, ultrasonography, magnetic resonance imaging, and scintigraphy. Semin. Plast. Surg. 2009, 23, 80–89. [Google Scholar] [CrossRef]
- Álvaro-Afonso, F.J.; Lázaro-Martínez, J.L.; García-Morales, E.; García-Álvarez, Y.; Sanz-Corbalán, I.; Molines-Barroso, R.J. Cortical disruption is the most reliable and accurate plain radiographic sign in the diagnosis of diabetic foot osteomyelitis. Diabet. Med. 2019, 36, 258–259. [Google Scholar] [CrossRef]
- Llewellyn, A.; Kraft, J.; Holton, C.; Harden, M.; Simmonds, M. Imaging for detection of osteomyelitis in people with diabetic foot ulcers: A systematic review and meta-analysis. Eur. J. Radiol. 2020, 131, 109215. [Google Scholar] [CrossRef]
- Llewellyn, A.; Jones-Diette, J.; Kraft, J.; Holton, C.; Harden, M.; Simmonds, M. Imaging tests for the detection of osteomyelitis: A systematic review. Health Technol. Assess. 2019, 23, 1–128. [Google Scholar] [CrossRef]
- Dinh, M.T.; Abad, C.L.; Safdar, N. Diagnostic accuracy of the physical examination and imaging tests for osteomyelitis underlying diabetic foot ulcers: Meta-analysis. Clin. Infect. Dis. 2008, 47, 519–527. [Google Scholar] [CrossRef]
- Termaat, M.F.; Raijmakers, P.G.H.M.; Scholten, H.J.; Bakker, F.C.; Patka, P.; Haarman, H.J.T.M. The accuracy of diagnostic imaging for the assessment of chronic osteomyelitis: A systematic review and meta-analysis. J. Bone Joint Surg. Am. 2005, 87, 2464–2471. [Google Scholar] [CrossRef]
- Enderle, M.D.; Coerper, S.; Schweizer, H.P.; Kopp, A.E.; Thelen, M.H.; Meisner, C.; Pressler, H.; Becker, H.D.; Claussen, C.; Häring, H.U.; et al. Correlation of imaging techniques to histopathology in patients with diabetic foot syndrome and clinical suspicion of chronic osteomyelitis. The role of high-resolution ultrasound. Diabetes Care 1999, 22, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Hoang, D.; Fisher, S.; Oz, O.K.; La Fontaine, J.; Chhabra, A. Percutaneous CT guided bone biopsy for suspected osteomyelitis: Diagnostic yield and impact on patient’s treatment change and recovery. Eur. J. Radiol. 2019, 114, 85–91. [Google Scholar] [CrossRef]
- Lauri, C.; Tamminga, M.; Glaudemans, A.W.J.M.; Juárez Orozco, L.E.; Erba, P.A.; Jutte, P.C.; Lipsky, B.A.; IJzerman, M.J.; Signore, A.; Slart, R.H.J.A. Detection of Osteomyelitis in the Diabetic Foot by Imaging Techniques: A Systematic Review and Meta-analysis Comparing MRI, White Blood Cell Scintigraphy, and FDG-PET. Diabetes Care 2017, 40, 1111–1120. [Google Scholar] [CrossRef] [PubMed]
- Al-Khawari, H.A.; Al-Saeed, O.M.; Jumaa, T.H.; Chishti, F. Evaluating diabetic foot infection with magnetic resonance imaging: Kuwait experience. Med. Princ. Pract. 2005, 14, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Lauri, C.; Glaudemans, A.W.J.M.; Campagna, G.; Keidar, Z.; Muchnik Kurash, M.; Georga, S.; Arsos, G.; Noriega-Álvarez, E.; Argento, G.; Kwee, T.C.; et al. Comparison of White Blood Cell Scintigraphy, FDG PET/CT and MRI in Suspected Diabetic Foot Infection: Results of a Large Retrospective Multicenter Study. J. Clin. Med. 2020, 9, 1645. [Google Scholar] [CrossRef] [PubMed]
- Ledermann, H.P.; Morrison, W.B.; Schweitzer, M.E. MR image analysis of pedal osteomyelitis: Distribution, patterns of spread, and frequency of associated ulceration and septic arthritis. Radiology 2002, 223, 747–755. [Google Scholar] [CrossRef]
- La Fontaine, J.; Bhavan, K.; Lam, K.; Van Asten, S.; Erdman, W.; Lavery, L.A.; Öz, O.K. Comparison Between Tc-99m WBC SPECT/CT and MRI for the Diagnosis of Biopsy-proven Diabetic Foot Osteomyelitis. Wounds Compend. Clin. Res. Pract. 2016, 28, 271–278. [Google Scholar]
- Richter, W.S.; Ivancevic, V.; Meller, J.; Lang, O.; Le Guludec, D.; Szilvazi, I.; Amthauer, H.; Chossat, F.; Dahmane, A.; Schwenke, C.; et al. 99mTc-besilesomab (Scintimun) in peripheral osteomyelitis: Comparison with 99mTc-labelled white blood cells. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 899–910. [Google Scholar] [CrossRef][Green Version]
- Parsons, L.M. Pitfalls in the diagnosis of chronic osteomyelitis in the presence of a contiguous neuropathic ulcer. J. Cutan. Med. Surg. 2009, 13 (Suppl. 1), S35–S37. [Google Scholar] [CrossRef] [PubMed]
- Familiari, D.; Glaudemans, A.W.J.M.; Vitale, V.; Prosperi, D.; Bagni, O.; Lenza, A.; Cavallini, M.; Scopinaro, F.; Signore, A. Can sequential 18F-FDG PET/CT replace WBC imaging in the diabetic foot? J. Nucl. Med. 2011, 52, 1012–1019. [Google Scholar] [CrossRef] [PubMed]
- Vouillarmet, J.; Moret, M.; Morelec, I.; Michon, P.; Dubreuil, J. Application of white blood cell SPECT/CT to predict remission after a 6 or 12 week course of antibiotic treatment for diabetic foot osteomyelitis. Diabetologia 2017, 60, 2486–2494. [Google Scholar] [CrossRef]
- Lazaga, F.; Van Asten, S.A.; Nichols, A.; Bhavan, K.; La Fontaine, J.; Oz, O.K.; Lavery, L.A. Hybrid imaging with 99mTc-WBC SPECT/CT to monitor the effect of therapy in diabetic foot osteomyelitis. Int. Wound J. 2016, 13, 1158–1160. [Google Scholar] [CrossRef]
- Erdman, W.A.; Buethe, J.; Bhore, R.; Ghayee, H.K.; Thompson, C.; Maewal, P.; Anderson, J.; Klemow, S.; Oz, O.K. Indexing severity of diabetic foot infection with 99mTc-WBC SPECT/CT hybrid imaging. Diabetes Care 2012, 35, 1826–1831. [Google Scholar] [CrossRef]
- Przybylski, M.M.; Holloway, S.; Vyce, S.D.; Obando, A. Diagnosing osteomyelitis in the diabetic foot: A pilot study to examine the sensitivity and specificity of Tc(99m) white blood cell-labelled single photon emission computed tomography/computed tomography. Int. Wound J. 2016, 13, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Delcourt, A.; Huglo, D.; Prangere, T.; Benticha, H.; Devemy, F.; Tsirtsikoulou, D.; Lepeut, M.; Fontaine, P.; Steinling, M. Comparison between Leukoscan (Sulesomab) and Gallium-67 for the diagnosis of osteomyelitis in the diabetic foot. Diabetes Metab. 2005, 31, 125–133. [Google Scholar] [CrossRef]
- Loessel, C.; Mai, A.; Starke, M.; Vogt, D.; Stichling, M.; Willy, C. Value of antigranulocyte scintigraphy with Tc-99m-sulesomab in diagnosing combat-related infections of the musculoskeletal system. BMJ Mil. Health 2021, 167, 8–17. [Google Scholar] [CrossRef]
- Wang, G.; Zhao, K.; Liu, Z.; Dong, M.; Yang, S. A meta-analysis of fluorodeoxyglucose-positron emission tomography versus scintigraphy in the evaluation of suspected osteomyelitis. Nucl. Med. Commun. 2011, 32, 1134–1142. [Google Scholar] [CrossRef]
- Nawaz, A.; Torigian, D.A.; Siegelman, E.S.; Basu, S.; Chryssikos, T.; Alavi, A. Diagnostic performance of FDG-PET, MRI, and plain film radiography (PFR) for the diagnosis of osteomyelitis in the diabetic foot. Mol. Imaging Biol. 2010, 12, 335–342. [Google Scholar] [CrossRef]
- Aslangul, E.; M’bemba, J.; Caillat-Vigneron, N.; Coignard, S.; Larger, E.; Boitard, C.; Lipsky, B.A. Diagnosing diabetic foot osteomyelitis in patients without signs of soft tissue infection by coupling hybrid 67Ga SPECT/CT with bedside percutaneous bone puncture. Diabetes Care 2013, 36, 2203–2210. [Google Scholar] [CrossRef] [PubMed]
- Nanni, C.; Errani, C.; Boriani, L.; Fantini, L.; Ambrosini, V.; Boschi, S.; Rubello, D.; Pettinato, C.; Mercuri, M.; Gasbarrini, A.; et al. 68Ga-citrate PET/CT for evaluating patients with infections of the bone: Preliminary results. J. Nucl. Med. 2010, 51, 1932–1936. [Google Scholar] [CrossRef]
- Martín Noguerol, T.; Luna Alcalá, A.; Beltrán, L.S.; Gómez Cabrera, M.; Broncano Cabrero, J.; Vilanova, J.C. Advanced MR Imaging Techniques for Differentiation of Neuropathic Arthropathy and Osteomyelitis in the Diabetic Foot. Radiographics 2017, 37, 1161–1180. [Google Scholar] [CrossRef] [PubMed]
- Fridman, R.; Bar-David, T.; Kamen, S.; Staron, R.B.; Leung, D.K.; Rasiej, M.J. Imaging of diabetic foot infections. Clin. Podiatr. Med. Surg. 2014, 31, 43–56. [Google Scholar] [CrossRef] [PubMed]
- Kavitha, K.V.; Tathare, S.; Kumbhar, V.; Bidaye, A.; Panse, R.; Maheshwari, S.; Gavankar, A.; Unnikrishnan, A.G. Role of Radiology in the Management of Diabetic Foot Infections: A Report of Three Cases. Clin. Res. Foot Ankle 2018, 6, 267. [Google Scholar] [CrossRef]
- Hochman, M.G.; Connolly, C. Imaging of Infection in the Diabetic Foot. In The Diabetic Foot. Contemporary Diabetes; Humana: Cham, Switzerland, 2018; pp. 55–94. ISBN 978-3-319-89868-1. [Google Scholar]
- Commean, P.K.; Kennedy, J.A.; Bahow, K.A.; Hildebolt, C.F.; Liu, L.; Smith, K.E.; Hastings, M.K.; Ju, T.; Prior, F.W.; Sinacore, D.R. Volumetric quantitative computed tomography measurement precision for volumes and densities of tarsal and metatarsal bones. J. Clin. Densitom. 2011, 14, 313–320. [Google Scholar] [CrossRef]
- Fayad, L.M.; Carrino, J.A.; Fishman, E.K. Musculoskeletal infection: Role of CT in the emergency department. Radiographics 2007, 27, 1723–1736. [Google Scholar] [CrossRef]
- Beroukhim, G.; Shah, R.; Bucknor, M.D. Factors Predicting Positive Culture in CT-Guided Bone Biopsy Performed for Suspected Osteomyelitis. Am. J. Roentgenol. 2019, 212, 620–624. [Google Scholar] [CrossRef]
- Lee, H.T.; Sebro, R. Predictors of positive bone cultures from CT-guided bone biopsies performed for suspected osteomyelitis. J. Med. Imaging Radiat. Oncol. 2020, 64, 313–318. [Google Scholar] [CrossRef]
- Ergen, F.B.; Sanverdi, S.E.; Oznur, A. Charcot foot in diabetes and an update on imaging. Diabet. Foot Ankle 2013, 4, 21884. [Google Scholar] [CrossRef]
- Mader, J.T.; Calhoun, J. Bone, Joint, and Necrotizing Soft Tissue Infections, 4th ed.; Baron, S., Ed.; University of Texas Medical Branch at Galveston: Galveston, TX, USA, 1996; ISBN 0963117211. [Google Scholar]
- Patel, S.; Srivastava, S.; Singh, M.R.; Singh, D. Mechanistic insight into diabetic wounds: Pathogenesis, molecular targets and treatment strategies to pace wound healing. Biomed. Pharmacother. 2019, 112, 108615. [Google Scholar] [CrossRef] [PubMed]
- Delikatny, E.J.; Poptani, H. MR techniques for in vivo molecular and cellular imaging. Radiol. Clin. N. Am. 2005, 43, 205–220. [Google Scholar] [CrossRef]
- Ahmadi, M.E.; Morrison, W.B.; Carrino, J.A.; Schweitzer, M.E.; Raikin, S.M.; Ledermann, H.P. Neuropathic arthropathy of the foot with and without superimposed osteomyelitis: MR imaging characteristics. Radiology 2006, 238, 622–631. [Google Scholar] [CrossRef]
- Kumar, Y.; Khaleel, M.; Boothe, E.; Awdeh, H.; Wadhwa, V.; Chhabra, A. Role of Diffusion Weighted Imaging in Musculoskeletal Infections: Current Perspectives. Eur. Radiol. 2017, 27, 414–423. [Google Scholar] [CrossRef]
- Liao, D.; Xie, L.; Han, Y.; Du, S.; Wang, H.; Zeng, C.; Li, Y. Dynamic contrast-enhanced magnetic resonance imaging for differentiating osteomyelitis from acute neuropathic arthropathy in the complicated diabetic foot. Skeletal Radiol. 2018, 47, 1337–1347. [Google Scholar] [CrossRef]
- O’Connor, J.P.B.; Tofts, P.S.; Miles, K.A.; Parkes, L.M.; Thompson, G.; Jackson, A. Dynamic contrast-enhanced imaging techniques: CT and MRI. Br. J. Radiol. 2011, 84, S112–S120. [Google Scholar] [CrossRef] [PubMed]
- Gordon, Y.; Partovi, S.; Müller-Eschner, M.; Amarteifio, E.; Bäuerle, T.; Weber, M.-A.; Kauczor, H.; Rengier, F. Dynamic contrast-enhanced magnetic resonance imaging: Fundamentals and application to the evaluation of the peripheral perfusion. Cardiovasc. Diagn. Ther. 2014, 4, 147–164. [Google Scholar] [CrossRef] [PubMed]
- Abdel Razek, A.A.K.; Samir, S. Diagnostic performance of diffusion-weighted MR imaging in differentiation of diabetic osteoarthropathy and osteomyelitis in diabetic foot. Eur. J. Radiol. 2017, 89, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Padhani, A.R.; van Ree, K.; Collins, D.J.; D’Sa, S.; Makris, A. Assessing the relation between bone marrow signal intensity and apparent diffusion coefficient in diffusion-weighted MRI. Am. J. Roentgenol. 2013, 200, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Mahesh, M. The Essential Physics of Medical Imaging, Third Edition. Med. Phys. 2013, 40, 077301. [Google Scholar] [CrossRef]
- Van Vucht, N.; Santiago, R.; Lottmann, B.; Pressney, I.; Harder, D.; Sheikh, A.; Saifuddin, A. The Dixon technique for MRI of the bone marrow. Skeletal Radiol. 2019, 48, 1861–1874. [Google Scholar] [CrossRef]
- Komarraju, A.; Chhabra, A. Advanced Cross-Sectional Radiology-Ultrasound, Computed Tomography and Magnetic Resonance Imaging of the Diabetic Foot. In The Foot in Diabetes; Wiley: Hoboken, NJ, USA, 2020; pp. 169–185. ISBN 9781119445814. [Google Scholar]
- Donovan, A.; Schweitzer, M.E. Use of MR imaging in diagnosing diabetes-related pedal osteomyelitis. Radiographics 2010, 30, 723–736. [Google Scholar] [CrossRef]
- Tan, P.L.; Teh, J. MRI of the diabetic foot: Differentiation of infection from neuropathic change. Br. J. Radiol. 2007, 80, 939–948. [Google Scholar] [CrossRef]
- Fujii, M.; Armstrong, D.G.; Armsrong, D.G.; Terashi, H. Efficacy of magnetic resonance imaging in diagnosing diabetic foot osteomyelitis in the presence of ischemia. J. Foot Ankle Surg. 2015, 52, 717–723. [Google Scholar] [CrossRef] [PubMed]
- Donovan, A.; Rosenberg, Z.S.; Cavalcanti, C.F. MR imaging of entrapment neuropathies of the lower extremity. Part 2. The knee, leg, ankle, and foot. Radiographics 2010, 30, 1001–1019. [Google Scholar] [CrossRef] [PubMed]
- Thakkar, R.S.; Del Grande, F.; Thawait, G.K.; Andreisek, G.; Carrino, J.A.; Chhabra, A. Spectrum of high-resolution MRI findings in diabetic neuropathy. Am. J. Roentgenol. 2012, 199, 407–412. [Google Scholar] [CrossRef]
- Vaeggemose, M.; Haakma, W.; Pham, M.; Ringgaard, S.; Tankisi, H.; Ejskjaer, N.; Heiland, S.; Poulsen, P.L.; Andersen, H. Diffusion tensor imaging MR Neurography detects polyneuropathy in type 2 diabetes. J. Diabetes Complicat. 2020, 34, 107439. [Google Scholar] [CrossRef]
- Vaeggemose, M.; Pham, M.; Ringgaard, S.; Tankisi, H.; Ejskjaer, N.; Heiland, S.; Poulsen, P.L.; Andersen, H. Diffusion tensor imaging MR neurography for the detection of polyneuropathy in type 1 diabetes. J. Magn. Reson. Imaging 2017, 45, 1125–1134. [Google Scholar] [CrossRef] [PubMed]
- Hlis, R.; Poh, F.; Xi, Y.; Chhabra, A. Diffusion tensor imaging of diabetic amyotrophy. Skeletal Radiol. 2019, 48, 1705–1713. [Google Scholar] [CrossRef]
- Wu, C.; Wang, G.; Zhao, Y.; Hao, W.; Zhao, L.; Zhang, X.; Cao, J.; Wang, S.; Chen, W.; Chan, Q.; et al. Assessment of tibial and common peroneal nerves in diabetic peripheral neuropathy by diffusion tensor imaging: A case control study. Eur. Radiol. 2017, 27, 3523–3531. [Google Scholar] [CrossRef]
- Pham, M.; Oikonomou, D.; Hornung, B.; Weiler, M.; Heiland, S.; Bäumer, P.; Kollmer, J.; Nawroth, P.P.; Bendszus, M. Magnetic resonance neurography detects diabetic neuropathy early and with Proximal Predominance. Ann. Neurol. 2015, 78, 939–948. [Google Scholar] [CrossRef] [PubMed]
- Newhart, H.; Patterson, J.; Gunasekaran, A.; Pandey, T.; Kumar, M.; Kazemi, N. The Incremental Value of Magnetic Resonance Neurography for the Neurosurgeon: Review of the Literature. World Neurosurg. 2019, 122, 331–341. [Google Scholar] [CrossRef]
- Diez, A.I.G.; Fuster, D.; Morata, L.; Torres, F.; Garcia, R.; Poggio, D.; Sotes, S.; Del Amo, M.; Isern-Kebschull, J.; Pomes, J.; et al. Comparison of the diagnostic accuracy of diffusion-weighted and dynamic contrast-enhanced MRI with 18F-FDG PET/CT to differentiate osteomyelitis from Charcot neuro-osteoarthropathy in diabetic foot. Eur. J. Radiol. 2020, 132, 109299. [Google Scholar] [CrossRef]
- Ruiz-Bedoya, C.A.; Gordon, O.; Mota, F.; Abhishek, S.; Tucker, E.W.; Ordonez, A.A.; Jain, S.K. Molecular imaging of diabetic foot infections: New tools for old questions. Int. J. Mol. Sci. 2019, 20, 5984. [Google Scholar] [CrossRef] [PubMed]
- Palestro, C.J. Radionuclide imaging of osteomyelitis. Semin. Nucl. Med. 2015, 45, 32–46. [Google Scholar] [CrossRef]
- Rosales, C.; Lowell, C.A.; Schnoor, M.; Uribe-Querol, E. Neutrophils: Their Role in Innate and Adaptive Immunity 2017. J. Immunol. Res. 2017, 2017, 9748345. [Google Scholar] [CrossRef] [PubMed]
- Censullo, A.; Vijayan, T. Using Nuclear Medicine Imaging Wisely in Diagnosing Infectious Diseases. Open Forum Infect. Dis. 2017, 4, ofx011. [Google Scholar] [CrossRef]
- Meller, J.; Köster, G.; Liersch, T.; Siefker, U.; Lehmann, K.; Meyer, I.; Schreiber, K.; Altenvoerde, G.; Becker, W. Chronic bacterial osteomyelitis: Prospective comparison of 18F-FDG imaging with a dual-head coincidence camera and 111In-labelled autologous leucocyte scintigraphy. Eur. J. Nucl. Med. Mol. Imaging 2002, 29, 53–60. [Google Scholar] [CrossRef]
- PubChem Compound Summary for CID 76957057. Technetium Tc-99M Sulfur Colloid. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Technetium-Tc-99M-sulfur-colloid (accessed on 1 February 2021).
- Heiba, S.; Kolker, D.; Ong, L.; Sharma, S.; Travis, A.; Teodorescu, V.; Ellozy, S.; Kostakoglu, L.; Savitch, I.; Machac, J. Dual-isotope SPECT/CT impact on hospitalized patients with suspected diabetic foot infection: Saving limbs, lives, and resources. Nucl. Med. Commun. 2013, 34, 877–884. [Google Scholar] [CrossRef] [PubMed]
- NDA 21-870: [18F] FDG Injection. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2005/021870lbl.pdf (accessed on 1 February 2021).
- Ruotolo, V.; Di Pietro, B.; Giurato, L.; Masala, S.; Meloni, M.; Schillaci, O.; Bergamini, A.; Uccioli, L. A new natural history of Charcot foot: Clinical evolution and final outcome of stage 0 Charcot neuroarthropathy in a tertiary referral diabetic foot clinic. Clin. Nucl. Med. 2013, 38, 506–509. [Google Scholar] [CrossRef]
- Kwee, T.C.; Kwee, R.M.; Alavi, A. FDG-PET for diagnosing prosthetic joint infection: Systematic review and metaanalysis. Eur. J. Nucl. Med. Mol. Imaging 2008, 35, 2122–2132. [Google Scholar] [CrossRef]
- Shemesh, S.; Kosashvili, Y.; Groshar, D.; Bernstine, H.; Sidon, E.; Cohen, N.; Luria, T.; Velkes, S. The value of 18-FDG PET/CT in the diagnosis and management of implant-related infections of the tibia: A case series. Injury 2015, 46, 1377–1382. [Google Scholar] [CrossRef]
- Lemans, J.V.C.; Hobbelink, M.G.G.; IJpma, F.F.A.; Plate, J.D.J.; van den Kieboom, J.; Bosch, P.; Leenen, L.P.H.; Kruyt, M.C.; Glaudemans, A.W.J.M.; Govaert, G.A.M. The diagnostic accuracy of 18F-FDG PET/CT in diagnosing fracture-related infections. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 999–1008. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Zhuang, H.; Rubello, D.; Alavi, A. Mild-to-moderate hyperglycemia will not decrease the sensitivity of 18F-FDG PET imaging in the detection of pedal osteomyelitis in diabetic patients. Nucl. Med. Commun. 2016, 37, 259–262. [Google Scholar] [CrossRef] [PubMed]
- Kagna, O.; Kurash, M.; Ghanem-Zoubi, N.; Keidar, Z.; Israel, O. Does Antibiotic Treatment Affect the Diagnostic Accuracy of 18F-FDG PET/CT Studies in Patients with Suspected Infectious Processes? J. Nucl. Med. 2017, 58, 1827–1830. [Google Scholar] [CrossRef] [PubMed]
- Vorster, M.; Maes, A.; van de Wiele, C.; Sathekge, M. Gallium-68 PET: A Powerful Generator-based Alternative to Infection and Inflammation Imaging. Semin. Nucl. Med. 2016, 46, 436–447. [Google Scholar] [CrossRef]
- Palestro, C.J. Radionuclide Imaging of Musculoskeletal Infection: A Review. J. Nucl. Med. 2016, 57, 1406–1412. [Google Scholar] [CrossRef]
- Jødal, L.; Jensen, S.B.; Nielsen, O.L.; Afzelius, P.; Borghammer, P.; Alstrup, A.K.O.; Hansen, S.B. Kinetic Modelling of Infection Tracers [18F]FDG, [68Ga]Ga-Citrate, [11C]Methionine, and [11C]Donepezil in a Porcine Osteomyelitis Model. Contrast Media Mol. Imaging 2017, 2017, 9256858. [Google Scholar] [CrossRef]
- Velikyan, I. Prospective of 68Ga Radionuclide Contribution to the Development of Imaging Agents for Infection and Inflammation. Contrast Media Mol. Imaging 2018, 2018, 9713691. [Google Scholar] [CrossRef]
- Salomäki, S.P.; Kemppainen, J.; Hohenthal, U.; Luoto, P.; Eskola, O.; Nuutila, P.; Seppänen, M.; Pirilä, L.; Oksi, J.; Roivainen, A. Head-to-Head Comparison of 68Ga-Citrate and 18F-FDG PET/CT for Detection of Infectious Foci in Patients with Staphylococcus aureus Bacteraemia. Contrast Media Mol. Imaging 2017, 2017, 3179607. [Google Scholar] [CrossRef] [PubMed]
- Uçkay, I.; Aragón-Sánchez, J.; Lew, D.; Lipsky, B.A. Diabetic foot infections: What have we learned in the last 30 years? Int. J. Infect. Dis. 2015, 40, 81–91. [Google Scholar] [CrossRef]
- Signore, A.; Artiko, V.; Conserva, M.; Ferro-Flores, G.; Welling, M.M.; Jain, S.K.; Hess, S.; Sathekge, M. Imaging Bacteria with Radiolabelled Probes: Is It Feasible? J. Clin. Med. 2020, 9, 2372. [Google Scholar] [CrossRef]
- Ankrah, A.O.; Klein, H.C.; Elsinga, P.H. New Imaging Tracers for the Infected Diabetic Foot (Nuclear and Optical Imaging). Curr. Pharm. Des. 2018, 24, 1287–1303. [Google Scholar] [CrossRef]
- Siaens, R.H.; Rennen, H.J.; Boerman, O.C.; Dierckx, R.; Slegers, G. Synthesis and comparison of 99mTc-enrofloxacin and 99mTc-ciprofloxacin. J. Nucl. Med. 2004, 45, 2088–2094. [Google Scholar]
- Malamitsi, J.; Giamarellou, H.; Kanellakopoulou, K.; Dounis, E.; Grecka, V.; Christakopoulos, J.; Koratzanis, G.; Antoniadou, A.; Panoutsopoulos, G.; Batsakis, C.; et al. Infecton: A 99mTc-ciprofloxacin radiopharmaceutical for the detection of bone infection. Clin. Microbiol. Infect. 2003, 9, 101–109. [Google Scholar] [CrossRef][Green Version]
- Britton, K.E.; Wareham, D.W.; Das, S.S.; Solanki, K.K.; Amaral, H.; Bhatnagar, A.; Katamihardja, A.H.S.; Malamitsi, J.; Moustafa, H.M.; Soroa, V.E.; et al. Imaging bacterial infection with (99m)Tc-ciprofloxacin (Infecton). J. Clin. Pathol. 2002, 55, 817–823. [Google Scholar] [CrossRef]
- Sarda, L.; Saleh-Mghir, A.; Peker, C.; Meulemans, A.; Crémieux, A.-C.; Le Guludec, D. Evaluation of (99m)Tc-ciprofloxacin scintigraphy in a rabbit model of Staphylococcus aureus prosthetic joint infection. J. Nucl. Med. 2002, 43, 239–245. [Google Scholar]
- Dutta, P.; Bhansali, A.; Mittal, B.R.; Singh, B.; Masoodi, S.R. Instant 99mTc-ciprofloxacin scintigraphy for the diagnosis of osteomyelitis in the diabetic foot. Foot Ankle Int. 2006, 27, 716–722. [Google Scholar] [CrossRef]
- Vito, A.; Alarabi, H.; Czorny, S.; Beiraghi, O.; Kent, J.; Janzen, N.; Genady, A.R.; Al-Karmi, S.A.; Rathmann, S.; Naperstkow, Z.; et al. A 99mTc-Labelled Tetrazine for Bioorthogonal Chemistry. Synthesis and Biodistribution Studies with Small Molecule trans-Cyclooctene Derivatives. PLoS ONE 2016, 11, e0167425. [Google Scholar] [CrossRef]
- Van Oosten, M.; Schäfer, T.; Gazendam, J.A.C.; Ohlsen, K.; Tsompanidou, E.; de Goffau, M.C.; Harmsen, H.J.M.; Crane, L.M.A.; Lim, E.; Francis, K.P.; et al. Real-time in vivo imaging of invasive- and biomaterial-associated bacterial infections using fluorescently labelled vancomycin. Nat. Commun. 2013, 4, 2584. [Google Scholar] [CrossRef]
- Yang, C.; Ren, C.; Zhou, J.; Liu, J.; Zhang, Y.; Huang, F.; Ding, D.; Xu, B.; Liu, J. Dual Fluorescent- and Isotopic-Labelled Self-Assembling Vancomycin for in vivo Imaging of Bacterial Infections. Angew. Chem. Int. Ed. Engl. 2017, 56, 2356–2360. [Google Scholar] [CrossRef]
- Yao, S.; Xing, H.; Zhu, W.; Wu, Z.; Zhang, Y.; Ma, Y.; Liu, Y.; Huo, L.; Zhu, Z.; Li, Z.; et al. Infection Imaging With 18F-FDS and First-in-Human Evaluation. Nucl. Med. Biol. 2016, 43, 206–214. [Google Scholar] [CrossRef]
- Ordonez, A.A.; Wintaco, L.M.; Mota, F.; Restrepo, A.F.; Ruiz-Bedoya, C.A.; Reyes, C.F.; Uribe, L.G.; Abhishek, S.; D’Alessio, F.R.; Holt, D.P.; et al. Imaging Enterobacterales infections in patients using pathogen-specific positron emission tomography. Sci. Transl. Med. 2021, 13, 1–10. [Google Scholar] [CrossRef]
- Martínez, M.E.; Kiyono, Y.; Noriki, S.; Inai, K.; Mandap, K.S.; Kobayashi, M.; Mori, T.; Tokunaga, Y.; Tiwari, V.N.; Okazawa, H.; et al. New radiosynthesis of 2-deoxy-2-[(18)F]fluoroacetamido-D-glucopyranose and its evaluation as a bacterial infections imaging agent. Nucl. Med. Biol. 2011, 38, 807–817. [Google Scholar] [CrossRef]
- Ning, X.; Seo, W.; Lee, S.; Takemiya, K.; Rafi, M.; Feng, X.; Weiss, D.; Wang, X.; Williams, L.; Camp, V.M.; et al. PET imaging of bacterial infections with fluorine-18-labeled maltohexaose. Angew. Chem. Int. Ed. Engl. 2014, 53, 14096–14101. [Google Scholar] [CrossRef]
- Gowrishankar, G.; Hardy, J.; Wardak, M.; Namavari, M.; Reeves, R.E.; Neofytou, E.; Srinivasan, A.; Wu, J.C.; Contag, C.H.; Gambhir, S.S. Specific Imaging of Bacterial Infection Using 6″-18F-Fluoromaltotriose: A Second-Generation PET Tracer Targeting the Maltodextrin Transporter in Bacteria. J. Nucl. Med. 2017, 58, 1679–1684. [Google Scholar] [CrossRef]
- Gabr, M.T.; Haywood, T.; Gowrishankar, G.; Srinivasan, A.; Gambhir, S.S. New synthesis of 6″-[18F]fluoromaltotriose for positron emission tomography imaging of bacterial infection. J. Label. Compd. Radiopharm. 2020, 63, 466–475. [Google Scholar] [CrossRef]
- Neumann, K.D.; Villanueva-Meyer, J.E.; Mutch, C.A.; Flavell, R.R.; Blecha, J.E.; Kwak, T.; Sriram, R.; VanBrocklin, H.F.; Rosenberg, O.S.; Ohliger, M.A.; et al. Imaging Active Infection in vivo Using D-Amino Acid Derived PET Radiotracers. Sci. Rep. 2017, 7, 7903. [Google Scholar] [CrossRef]
- Stewart, M.N.; Parker, M.F.L.; Jivan, S.; Luu, J.M.; Huynh, T.L.; Schulte, B.; Seo, Y.; Blecha, J.E.; Villanueva-Meyer, J.E.; Flavell, R.R.; et al. High Enantiomeric Excess In-Loop Synthesis of d-[methyl-11C]Methionine for Use as a Diagnostic Positron Emission Tomography Radiotracer in Bacterial Infection. ACS Infect. Dis. 2020, 6, 43–49. [Google Scholar] [CrossRef]
- Renick, P.J.; Mulgaonkar, A.; Co, C.M.; Wu, C.; Zhou, N.; Velazquez, A.; Pennington, J.; Sherwood, A.; Dong, H.; Castellino, L.; et al. Imaging of Actively Proliferating Bacterial Infections by Targeting the Bacterial Metabolic Footprint with d-[5-11C]-Glutamine. ACS Infect. Dis. 2021, 7, 347–361. [Google Scholar] [CrossRef]
- Erba, P.A.; Cataldi, A.G.; Tascini, C.; Leonildi, A.; Manfredi, C.; Mariani, G.; Lazzeri, E. 111In-DTPA-Biotin uptake by Staphylococcus aureus. Nucl. Med. Commun. 2010, 31, 994–997. [Google Scholar] [CrossRef]
- Baldoni, D.; Waibel, R.; Bläuenstein, P.; Galli, F.; Iodice, V.; Signore, A.; Schibli, R.; Trampuz, A. Evaluation of a Novel Tc-99m Labelled Vitamin B12 Derivative for Targeting Escherichia coli and Staphylococcus aureus In Vitro and in an Experimental Foreign-Body Infection Model. Mol. Imaging Biol. 2015, 17, 829–837. [Google Scholar] [CrossRef]
- Ordonez, A.A.; Weinstein, E.A.; Bambarger, L.E.; Saini, V.; Chang, Y.S.; DeMarco, V.P.; Klunk, M.H.; Urbanowski, M.E.; Moulton, K.L.; Murawski, A.M.; et al. A Systematic Approach for Developing Bacteria-Specific Imaging Tracers. J. Nucl. Med. 2017, 58, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Diaz, L.A.; Foss, C.A.; Thornton, K.; Nimmagadda, S.; Endres, C.J.; Uzuner, O.; Seyler, T.M.; Ulrich, S.D.; Conway, J.; Bettegowda, C.; et al. Imaging of musculoskeletal bacterial infections by [124I]FIAU-PET/CT. PLoS ONE 2007, 2, e1007. [Google Scholar] [CrossRef]
- Zhang, X.M.; Zhang, H.H.; McLeroth, P.; Berkowitz, R.D.; Mont, M.A.; Stabin, M.G.; Siegel, B.A.; Alavi, A.; Barnett, T.M.; Gelb, J.; et al. [124I]FIAU: Human dosimetry and infection imaging in patients with suspected prosthetic joint infection. Nucl. Med. Biol. 2016, 43, 273–279. [Google Scholar] [CrossRef]
- Cho, S.Y.; Rowe, S.P.; Jain, S.K.; Schon, L.C.; Yung, R.C.; Nayfeh, T.A.; Bingham, C.O.; Foss, C.A.; Nimmagadda, S.; Pomper, M.G. Evaluation of Musculoskeletal and Pulmonary Bacterial Infections With [124I]FIAU PET/CT. Mol. Imaging 2020, 19, 1536012120936876. [Google Scholar] [CrossRef]
- Ferreira, I.M.; de Sousa Lacerda, C.M.; Dos Santos, S.R.; de Barros, A.L.B.; Fernandes, S.O.; Cardoso, V.N.; de Andrade, A.S.R. Detection of bacterial infection by a technetium-99m-labeled peptidoglycan aptamer. Biomed. Pharmacother. 2017, 93, 931–938. [Google Scholar] [CrossRef]
- Aznar, A.; Dellagi, A. New insights into the role of siderophores as triggers of plant immunity: What can we learn from animals? J. Exp. Bot. 2015, 66, 3001–3010. [Google Scholar] [CrossRef]
- Hilty, J.; George Smulian, A.; Newman, S.L. Histoplasma capsulatum utilizes siderophores for intracellular iron acquisition in macrophages. Med. Mycol. 2011, 49, 633–642. [Google Scholar] [CrossRef]
- Zhi, H.; Behnsen, J.; Aron, A.; Subramanian, V.; Liu, J.Z.; Gerner, R.R.; Petras, D.; Green, K.D.; Price, S.L.; Camacho, J.; et al. Siderophore-Mediated Zinc Acquisition Enhances Enterobacterial Colonization of the Inflamed Gut. Available online: https://www.biorxiv.org/content/10.1101/2020.07.20.212498v1.full (accessed on 17 August 2021).
- Enyedy, É.A.; Pócsi, I.; Farkas, E. Complexation of desferricoprogen with trivalent Fe, Al, Ga, In and divalent Fe, Ni, Cu, Zn metal ions: Effects of the linking chain structure on the metal binding ability of hydroxamate based siderophores. J. Inorg. Biochem. 2004, 98, 1957–1966. [Google Scholar] [CrossRef] [PubMed]
- Petrik, M.; Zhai, C.; Haas, H.; Decristoforo, C. Siderophores for molecular imaging applications. Clin. Transl. Imaging 2017, 5, 15–27. [Google Scholar] [CrossRef]
- Pfister, J.; Lichius, A.; Summer, D.; Haas, H.; Kanagasundaram, T.; Kopka, K.; Decristoforo, C. Live-cell imaging with Aspergillus fumigatus-specific fluorescent siderophore conjugates. Sci. Rep. 2020, 10, 15519. [Google Scholar] [CrossRef] [PubMed]
- Pfister, J.; Bata, R.; Hubmann, I.; Hörmann, A.A.; Gsaller, F.; Haas, H.; Decristoforo, C. Siderophore Scaffold as Carrier for Antifungal Peptides in Therapy of Aspergillus fumigatus Infections. J. Fungi 2020, 6, 367. [Google Scholar] [CrossRef]
- Love, C.; Palestro, C.J. Nuclear medicine imaging of bone infections. Clin. Radiol. 2016, 71, 632–646. [Google Scholar] [CrossRef] [PubMed]
- Wiehr, S.; Warnke, P.; Rolle, A.-M.; Schütz, M.; Oberhettinger, P.; Kohlhofer, U.; Quintanilla-Martinez, L.; Maurer, A.; Thornton, C.; Boschetti, F.; et al. New pathogen-specific immunoPET/MR tracer for molecular imaging of a systemic bacterial infection. Oncotarget 2016, 7, 10990–11001. [Google Scholar] [CrossRef] [PubMed]
- Morad, H.O.J.; Wild, A.-M.; Wiehr, S.; Davies, G.; Maurer, A.; Pichler, B.J.; Thornton, C.R. Pre-clinical Imaging of Invasive Candidiasis Using ImmunoPET/MR. Front. Microbiol. 2018, 9, 1996. [Google Scholar] [CrossRef] [PubMed]
- Pakos, E.E.; Koumoullis, H.D.; Koumoulis, H.D.; Fotopoulos, A.D.; Ioannidis, J.P.A. Osteomyelitis: Antigranulocyte scintigraphy with 99mTC radiolabeled monoclonal antibodies for diagnosis- meta-analysis. Radiology 2007, 245, 732–741. [Google Scholar] [CrossRef]
- Sellmyer, M.A.; Lee, I.; Hou, C.; Weng, C.-C.; Li, S.; Lieberman, B.P.; Zeng, C.; Mankoff, D.A.; Mach, R.H. Bacterial infection imaging with [18F]fluoropropyl-trimethoprim. Proc. Natl. Acad. Sci. USA 2017, 114, 8372–8377. [Google Scholar] [CrossRef]
- Lee, J.T.; Zhang, H.; Moroz, M.A.; Likar, Y.; Shenker, L.; Sumzin, N.; Lobo, J.; Zurita, J.; Collins, J.; van Dam, R.M.; et al. Comparative Analysis of Human Nucleoside Kinase-Based Reporter Systems for PET Imaging. Mol. Imaging Biol. 2017, 19, 100–108. [Google Scholar] [CrossRef]
- Rajamani, S.; Kuszpit, K.; Scarff, J.M.; Lundh, L.; Khan, M.; Brown, J.; Stafford, R.; Cazares, L.H.; Panchal, R.G.; Bocan, T. Bioengineering of bacterial pathogens for noninvasive imaging and in vivo evaluation of therapeutics. Sci. Rep. 2018, 8, 12618. [Google Scholar] [CrossRef]
- Meyr, A.J.; Seo, K.; Khurana, J.S.; Choksi, R.; Chakraborty, B. Level of Agreement With a Multi-Test Approach to the Diagnosis of Diabetic Foot Osteomyelitis. J. Foot Ankle Surg. 2018, 57, 1137–1139. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Imaging Method/Radionuclide | Sensitivity (%) | Specificity (%) | Function | Cost | Accessibility | Radiation | References | |
|---|---|---|---|---|---|---|---|---|
| Radiography | 43–86 | 27–83 | +++ | + | +++++ | ☢ | [50,51,52,53,54] | |
| CT | 67–80 | 50–70 | +++ | +++ | +++ | ☢ | [50,55] | |
| Ultrasound | 79 | 80 | ++ | + | +++++ | O | [56] | |
| MRI | 87–100 | 37–83.8 | ++++ | +++ | +++ | O | [52,53,54,57,58,59,60,61,62] | |
| Planar Bone Scintigraphy | 99mTc-MDP | 81.0–84.2 | 28.0–67.7 | +++ | ++ | ++ | ☢☢☢ | [52,54] |
| Planar WBC Scan | 99mTc-besilesomab | 74.8 | 71.8 | +++ | +++ | ++ | ☢☢☢ | [63] |
| 99mTc-HMPAO | 59.0–91 | 79.5–92 | +++ | ++ | ++ | ☢☢☢ | [63,64] | |
| 99mTc-exametazime | 86.0 | 100 | +++ | ++ | ++ | ☢☢☢ | [65] | |
| WBC SPECT/CT | 99mTc-WBC | 87.5–100 | 35–92 | ++++ | ++++ | + | ☢☢☢☢ | [58,62,66,67,68,69] |
| 99mTc-sulesomab | 67–72.0 | 85–88.0 | +++ | +++ | ++ | ☢☢☢☢ | [70,71] | |
| 111In-WBC | 74–92 | 68–75 | ++++ | ++++ | + | ☢☢☢☢ | [54,58] | |
| PET | 18F-FDG | 81–92.3 | 92.0–93 | +++ | ++++ | + | ☢☢☢ | [72,73] |
| PET/CT | 18F-FDG | 43–89 | 67–100 | ++++ | ++++ | + | ☢☢☢☢ | [58,65] |
| 67Ga-citrate | 44–100 | 45–77 | ++ | ++ | ++ | ☢☢☢ | [70,74] | |
| 68Ga-citrate | 100 | 76 | ++ | ++ | ++ | ☢☢☢ | [75] | |
| MR Technique | Molecular Basis | Demonstrated Imaging Feature of DFI |
|---|---|---|
| Dynamic Contrast Enhancement (DCE) | Contrast agent alters MR signal intensity in a concentration dependent manner | Bone marrow edema Pattern of Soft tissue involvement Joint impairment Vascular involvement |
| Diffusion Weighted Imaging (DWI) | Takes advantage of restricted diffusion in certain anatomical features such as abscesses and compares this to free water to provide an enhanced image with excellent background suppression. | Bone marrow edema Soft tissue involvement Joint impairment Nerve damage |
| Dixon Sequence | Combines in-phase and out-of-phase images produced through chemical-shift with decreased sensitivity to inhomogeneities of B0 and B1, resulting in homogenous fat suppression. Cortical margins and cysts are best seen on out-of-phase image, marrow edema on water-image, muscle fatty replacement and marrow fat replacement on in-phase and fat-images. | Bone marrow edema Bone lesion identification Nerve damage |
| Diffusion Tensor Imaging (DTI) | Uses the sensitivity of DWI to the anisotropic water movement within myelinated axons to generate high resolution images that can provide information regarding myelin sheath and axonal damage | Nerve damage |
| Radiotracer | Imaging Technique | Cellular Parameter | Mechanism of Localization | Strengths | Weaknesses |
|---|---|---|---|---|---|
| 99mTc-MDP | Bone Scintigraphy | Osteoblastic bone formation | Chemiabsorption onto hydroxyapatite crystals of the bone matrix | Inexpensive High sensitivity | Low specificity, dependent on area of exposed bone surface |
| 18F-NaF | Bone Scintigraphy or PET | Osteoblastic bone formation | Binds to and engages exchange reaction with hydroxyapatite crystals to form hydroxyfluoroapatite and fluoroapatite in the bone matrix | Smaller molecule than MDP with faster uptake, fast renal clearance, less background | Dependent on area of exposed bone surface |
| 99mTc-HMPAO | Labeled WBC (in vitro) | WBC migration to site of infection | WBC response to infection | Specificity, same day diagnosis of DFI | Simultaneous dual-tracer approach is not possible. Intensive preparation Expensive |
| 111I-oxine | Labeled WBC (in vitro) | WBC migration to site of infection | WBC response to infection | Simultaneous dual-tracer approach is possible | Intensive preparation Expensive Low image quality |
| 18F-FDG | PET/CT | Glucose uptake and metabolism | Taken up by WBC or immune cells with increased glucose disposal | Sensitivity, inherently tomographic | Specificity, Availability, and cost |
| 67/68Ga-Citrate | Scintigraphy/SPECT/CT (67Ga) or PET/CT (68Ga) | WBC activity at site of infection | Iron mimetic. Binds to transferrin in circulating plasma. Binds to lactoferrin released from dying WBCs and bacterial siderophores at the site of infection | Detects low grade infection Low toxicity, Bone/soft tissue distinction | Delayed imaging High radiation dose, Non-specific accumulation in sterile inflammation or osteoblasts in healing bone |
| Radiotracer | Clinical Trials | Parameter | Mechanism of Localization | Strength/Weakness | References | |
|---|---|---|---|---|---|---|
| Radiolabeled Antibiotics | 99mTc-ciprofloxacin | Yes | Inhibition of DNA Synthesis | Bacterial DNA gyrase | High sensitivity (85.4–97.2%), ciprofloxacin already used in DFI treatment | [133,134,135,136] |
| Low specificity (66.7–81.7%), antibiotic resistant bacteria | ||||||
| 18F-fluoropropyl-trimethoprim | No | Inhibition of Folic Acid Synthesis | Inhibition of thymidine biosynthesis | Low background, high uptake in bacteria, detect inflammation from soft tissue infection vs sterile inflammation | [167] | |
| Antibiotic resistant bacteria | ||||||
| 99mTc-sulfonamides (pertechnetate, sulfadiazine) | No | Inhibition of Folic Acid Synthesis | Broad spectrum antibiotics, uptake in bacterial and fungal infections | [155] | ||
| Antibiotic resistant bacteria | ||||||
| 99mTc-vancomycin | No | Inhibition of bacterial cell wall synthesis | Binds to D-ala-D-ala lipid moiety | Specific for gram positive organisms | [137,138,139] | |
| Not specific for gram negative organisms Antibiotic resistant bacteria | ||||||
| Radiolabeled Sugars | 18F-FDS | Yes | Bacteria-Specific Glucose Sources for Carbohydrate Metabolism | Bacterial Metabolic Substrate | Antibiotic treatment monitoring, used in humans | [140,141] |
| Uptake by Enterobacteriaceae in the human gut | ||||||
| 18F-FAG | No | Sorbitol analogue utilized only by bacteria | Selective accumulation in E. coli, rapid accumulation, can differentiate infection from sterile inflammation, shows promise for monitoring response to treatment, small molecule | [142] | ||
| Not applied clinically | ||||||
| 18F-maltohexose | No | Bacterial-specific maltodextrin transporter | Can discriminate between live bacteria, metabolically inactive bacteria, and sterile inflammation | [143] | ||
| Poor signal-to-noise ratios, Not applied clinically | ||||||
| 6′′-18F-fluoromaltotriose | No | Bacterial-specific maltodextrin transporter | 2nd Gen, improved signal-to-noise ratio, bacterial-selective uptake in vitro and in vivo | [144,145] | ||
| Not applied clinically | ||||||
| Amino Acid Uptake | D-[methyl-11C] methionine | No | Bacterial Cell Wall Synthesis | Incorporation into the peptidoglycan | Distinguish sterile inflammation from infection in both gram—and gram +, broad sensitivity | [146,147] |
| Not applied clinically | ||||||
| D-5-[11C] glutamine | No | Incorporation into the peptidoglycan | Highly specific, high sensitivity for gram +, no uptake in sterile inflammation, fast clearance | [148] | ||
| Corroborating studies needed, not yet applied clinically | ||||||
| Vitamin Uptake | 124I-fialuridine (FIAU) | Yes | Endogenous TK enzyme of pathogenic bacteria | Trapped in the cell after phosphorylation | Reduced uptake in the presence of metal artifacts, | [154,168,169] |
| More clinical studies needed to assess clinical efficacy | ||||||
| 111In-biotin | No | Production of Fatty Acid | Bacterial growth factor | Essential growth factor for S. aureus | [149] | |
| Corroborating in vivo studies needed to assess clinical relevance | ||||||
| 99mTc-PAMA | No | Vitamin B12 Metabolism | Vitamin B12 derivative that accumulates in rapidly proliferating cells | High uptake in Gram + and Gram - | [150] | |
| Not applied clinically | ||||||
| 18F or 3H-PABA | No | Folic Acid Synthesis | Inhibition of Thymidine Synthesis | Accumulation in MRSA and other resistant organisms | [151] | |
| In vivo studies needed | ||||||
| Polyclonal Antibodies | 64Cu-NODAGA | No | Membrane protein binding of polyclonal antibody | Microbe-specific membrane polyclonal antibody binding | Particular to a specific microbe | [164,165] |
| Slow accumulation time | ||||||
| Siderophores | 68Ga-FOXE | No | Iron Transport | Accumulation of Siderophores in the cell | High uptake in S. aureus and fungi | [160,161,162] |
| Not used in DFI model | ||||||
| Immunoscintigraphy | 99mTc-sulesomab | Yes | WBC migration to infectious foci | Binds to antigen-90 on WBC membranes | Ease of preparation? Not sure about this | [63,71] |
| Dependent upon host response, expensive, limited availability | ||||||
| 99mTc-Besilesomab | Binds to antigen-95 on granulocytes and their precursors | Ease of preparation, good sensitivity and specificity | [63] | |||
| Dependent upon host response, expensive, limited availability |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rubitschung, K.; Sherwood, A.; Crisologo, A.P.; Bhavan, K.; Haley, R.W.; Wukich, D.K.; Castellino, L.; Hwang, H.; La Fontaine, J.; Chhabra, A.; et al. Pathophysiology and Molecular Imaging of Diabetic Foot Infections. Int. J. Mol. Sci. 2021, 22, 11552. https://doi.org/10.3390/ijms222111552
Rubitschung K, Sherwood A, Crisologo AP, Bhavan K, Haley RW, Wukich DK, Castellino L, Hwang H, La Fontaine J, Chhabra A, et al. Pathophysiology and Molecular Imaging of Diabetic Foot Infections. International Journal of Molecular Sciences. 2021; 22(21):11552. https://doi.org/10.3390/ijms222111552
Chicago/Turabian StyleRubitschung, Katie, Amber Sherwood, Andrew P. Crisologo, Kavita Bhavan, Robert W. Haley, Dane K. Wukich, Laila Castellino, Helena Hwang, Javier La Fontaine, Avneesh Chhabra, and et al. 2021. "Pathophysiology and Molecular Imaging of Diabetic Foot Infections" International Journal of Molecular Sciences 22, no. 21: 11552. https://doi.org/10.3390/ijms222111552
APA StyleRubitschung, K., Sherwood, A., Crisologo, A. P., Bhavan, K., Haley, R. W., Wukich, D. K., Castellino, L., Hwang, H., La Fontaine, J., Chhabra, A., Lavery, L., & Öz, O. K. (2021). Pathophysiology and Molecular Imaging of Diabetic Foot Infections. International Journal of Molecular Sciences, 22(21), 11552. https://doi.org/10.3390/ijms222111552