
Monoclonal Antibodies for Chronic Pain Treatment: Present and Future

 , ,
, ,
Abstract
1. Monoclonal Antibodies
1.1. Classification and Types of mAbs
- Murine: this was the first mAb discovered and reproduced. This type of mAb emerges from a collection of B lymphocytes from the spleen of a mouse, which are then fused with an immortal myeloma cell line. All these mAbs are identified with a name that ends in -omab (e.g., muromonab-CD3, capromab). They are often associated with allergic reactions and the induction of anti-drug antibodies (ADAs) [5,7]. Hybrid mouse/rat antibodies are denoted by the syllable -axo- (e.g., catumaxomab).
- Chimeric: attempting to overcome the inherent immunogenicity and reduced effector function of murine mAbs in human and chimeric mouse–human Abs were developed. They utilize the murine antigen-specific variable region, but the remaining heavy and light chains are human, resulting in mAbs that are approximately 65% human and 35% murine [1]. These mAbs are identified with names ending in -ximab (e.g., rituximab, infliximab) [6]; they exhibit an extended half-life in humans and show reduced immunogenicity, but the propensity to induce ADAs is still considerable [5].
- Humanized: in humanized Abs, only the hypervariable regions of the light and heavy chains are murine [8]; this results in molecules that are approximately 95% human, decreasing the apparition of ADAs. These mAbs are identified with names ending in -zumab (e.g., trastuzumab, alemtuzumab, tanezumab) [5,6].
- Human: the fully human mAbs are created using animals carrying human Ig genes. These transgenes include parts of the variable regions that enable the recombination of the human Abs [5,9]. These mAbs are less antigenic and better tolerated compared to the other classes of mAbs. They are identified with names ending in -umab (e.g., ofatumumab, fulranumab, erenumab) [6].
1.2. Mechanisms of Action and Clinical Applications of mAbs
- Autoinmune diseases: these conditions are characterized by a proliferation, migration, and activation of B and T cells, leading to cytokine and proinflammatory molecule secretion, ensuing cellular damage. Herein, mAbs are in charge of suppressing excessive responses, hence inhibiting cellular recruitment or the interaction of antigen-presenting cells with T cells and blocking the activation and depletion of B and T cells inhibiting the release of proinflammatory cytokines [12].
- Infectious diseases: mAbs may bind viruses, directly inhibiting their replication, or, as in the case of HIV, by binding to CD4 receptors of immune cells, impeding the entrance of the virus inside the host cell [12].
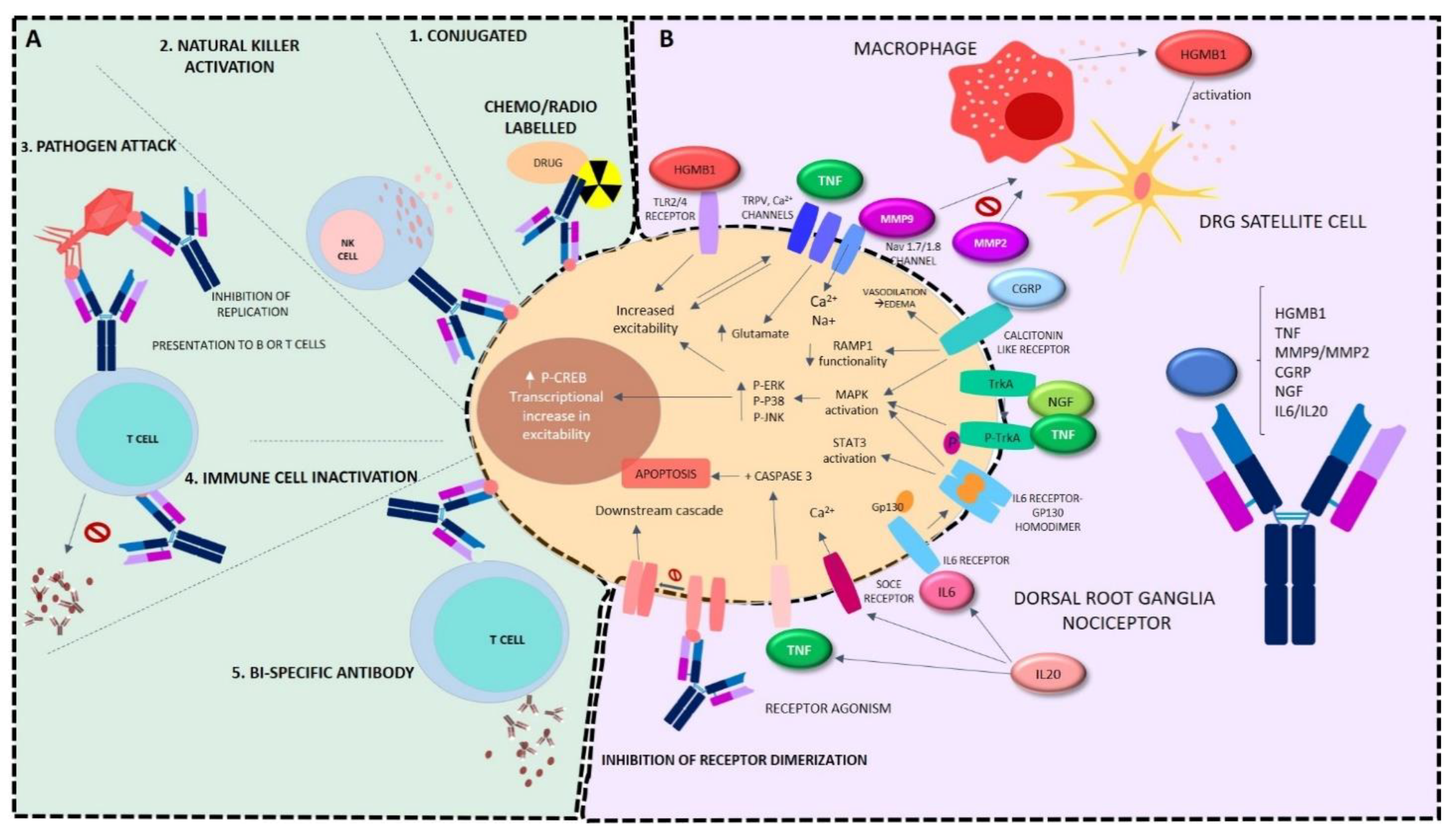
- Oncology: mAbs herein attempt to inhibit tumorigenesis and tumor cell migration through several pathways. The first approach is tumor cell killing. Firstly, conjugated mAbs work as specific treatment carriers to the tumor, herein including drug-conjugated Ab (carrying the drug itself) or radioactively conjugated Ab (carrying radiation to the tumoral cell) [13]. The second approach is by receptor binding, by induction of cellular apoptosis cascade through receptor agonism, or by antagonism-specific receptors inhibiting receptor dimerization or ligand binding, rendering downstream cascades that lead to reduced proliferation or apoptosis.
- Moreover, another strategy resides in the driving of the immune cells to the tumorigenic cells for them to carry out the assault. This process may be carried out by phagocytosis, antibody-dependent cellular cytotoxicity using immune cell effectors such as natural killers, complement mediated cytotoxicity, or by inhibiting the checkpoint escape (inactivation of T cell inhibitory receptors). Tumor cells bind through PD-L1 to PD-1 receptors of T cells to inhibit immune response that would destroy malignant proliferation; hence, the binding of mAbs to PD1 and PD-L1 blocks this inhibition [14]. Moreover, carcinogenic cells may be specifically targeted by vascular and stromal cell ablation by precise toxin delivery, inhibition of agonists in the vasculature, or specific stromal cell inhibition. The last strategy resides in bispecific mAbs, which consist of two arms, with one arm recognizing cancer cells and the other activating antigens on immune effector cells including CD3 [15].
2. Chronic Pain and Possible Usefulness of mAbs in Its Treatment
3. mAbs in Osteoarthritis Pain
3.1. Data from Preclinical Research
3.2. Data from Clinical Research
4. mAbs in Rheumatoid Arthritis
4.1. Data from Preclinical Research
4.2. Data from Clinical Research
5. mAbs in Migraine
5.1. Data from Preclinical Research
5.2. Data from Clinical Research
6. mAbs in Chronic Low Back Pain
7. mAbs in Neuropathic Pain
7.1. Data from Preclinical Research
7.2. Data from Clinical Research
8. Other Clinical Evidence of Use of mAbs in Chronic Pain: Endometriosis and Fibromyalgia
- Endometriosis: deep endometriosis-associated pain is believed to be caused by inflammation. Endometriosis is associated with an inflammatory response in the pelvis, which is mediated by several cytokines including TNF. It has therefore been suggested that the anti-TNF mAb infliximab might relieve pain in affected women. Thus, a phase II clinical trial to study infliximab effect was conducted in women with endometriosis [148], and results indicated that it did not appear to modify pain [149].
- Fibromyalgia: currently, a phase II clinical trial is ongoing to estimate the effect of fremanezumab administered subcutaneously in reducing pain in adult patients with fibromyalgia. Other measures of efficacy will also be studied, such as quality of life, sleep, fatigue, health improvement, physical functioning, and mood, as well as the safety and tolerability of this drug [150]. This study is currently in the recruitment phase.
9. Future Applications of mAbs in Preclinical Development: Cancer Pain and Pain in Bone Fracture
- Bone cancer pain: among other adverse consequences, the tumor formation in bones provokes in many patients a severe pain state (including spontaneous and evoked) that impairs quality of life. This pain state includes several aspects such as nociceptive, inflammatory, and neuropathic effects.
- Pain in bone fracture: the mouse model of painful bone fracture induces a marked reduction in the physical activity of the animal; using this model, in which mice exhibited femur fracture pain, it has been found that the administration of the anti-NGF antibody mAb911 induced an improvement in mice physical activity by blocking the sensitization of nociceptors that innervate the bone [155] (Table 4).

{kind=link}
{kind=link}
| Animal Model | Target | mAb | Method | Species | Pain Assessed | Effect | Reference |
|---|---|---|---|---|---|---|---|
| Osteoarthritis | NGF | GZ389988 | Chemical MIA | Lewis rats | Weigh bearing | Reduction of weight bearing imbalance | [60] |
| Tanezumab | Surgical MMT | Lewis rats | Weigh bearing | Gait deficiency prevention | [58] | ||
| AS2886401-00 | Chemical MIA | Sprague-Dawley rats | Gait analysis | Improvement in gait imbalance, no effect on knee lesion score | [61] | ||
| AR786 | Surgical MNX, Chemical MIA | Sprague-Dawley rats | Mechanical sensitivity, weight-bearing | Reduction of mechanical allodynia, reversal of weight-bearing asymmetry | [66] | ||
| muMab 911 | Chemical MIA | Sprague-Dawley rats | Mechanical sensitivity, weight-bearing | Reduction of mechanical allodynia, reversal of weight-bearing asymmetry | [66] | ||
| WO 2004/058184 A2 | Chemical MIA | Wistar Han rats | Spontaneous locomotor activity | Reverse deficits in burrowing | [62] | ||
| NV-01 | Spontaneous degenerative joint disease | Dogs | Spontaneous activity, pain | Gain mobility, improve pain severity | [67] | ||
| TrkAd5 | Surgical DMM | C57BL/6 mice | Weight-bearing | Improvement of weight bearing deficit | [56] | ||
| Anti-NGF-2.5S | Surgical DMM | PKCδ null mice | Mechanical sensitivity | Reduce mechanical allodynia | [57] | ||
| mAb911 | Surgical arthrotomy | C3H/HeJ mice | Spontaneous locomotor activity | Increase of horizontal activity, vertical rearing, and horizontal velocity | [59] | ||
| L148 M | Chemical MIA | C57BR/J mice | Gait analysis | Improvement of duty cycle, swing speed, and print area | [64] | ||
| Rheumatoid arthritis | IL-6 | HA-AuNP/TCZ, TCZ | CIA | DBA/1j mice | Clinical scores | Improvement in the degree of swelling | [93] |
| TLR4 | TLR4 blocker NI-0101 | CIA | Mice | Inhibition of LPS-induced cytokine release | [94] | ||
| NGF | AR786 | CIA, Carragenan | Sprague-Dawley rats | Mechanical sensitivity, weight-bearing, joint swelling | Reduce mechanical allodynia and weight-bearing asymmetry, inhibit partially knee swelling | [95] | |
| TNF | Infliximab | AIA | Lewis rats | Mechanical and thermal sensitivity, joint swelling | Reduce mechanical hyperalgesia and swelling in inflamed joint | [96] | |
| TNF transgenic | TNF transgenic mice | Clinical scoring | Averted the increase of symptom severity | [97] | |||
| Adalimumab Humira | CFA | Wistar rats | Morphological examination of the metatarsophalangeal joints | Decrease of inflammation signal | [98] | ||
| uPA | Ab anti-uPA mU1 | CIA, AIA | DBA/1 mice | Clinical scores | Inhibition of disease progression | [156] | |
| Adiponectin | mAbs KH7–33 and KH4–8 | CIA | DBA/1 J mice | Arthritis and squeaking index, paw volume | Inhibit arthritic symptoms | [99] | |
| FcγRI | anti-CD64 | AIA | C57BL/6 mice | Mechanical and thermal sensitivity, joint diameter | Reductions in mechanical and thermal hyperalgesia | [100] | |
| Migraine | CGRP | ALD405 | CGRP-induced | CD1 mice | Light aversion and motility assessment | Aversion to light attenuated, reduced motility avoided | [116] |
| Mouse grimace scale | Blockade of facial signs of discomfort | [117] |
| Type of Pain | Target | mAb | Main Findings | Reference |
|---|---|---|---|---|
| Osteoarthritis (hip or knee) | NGF | Tanezumab | Decreases joint pain and improves physical function. Neurosensory and neuromuscular adverse events. Risk of RPOA at high doses. | [49,68,69,70,71,72,76,77,78,79,80,81,82,83,157] |
| Fulranumab | Greater pain relief relative to oxycodone. Arthralgias and risk of RPOA associated to treatment. | [73,74] | ||
| Fasinumab | Decreases joint pain and improves physical function. Arthropathies associated to treatment. | [75] | ||
| Chronic low back pain | NGF | Tanezumab | Improvement in pain, function, and global scores vs. placebo and naproxen. Arthralgias and risk of neurological adverse events. | [131,132,133,134] |
| TNF | Infliximab | No results yet. | [158] | |
| Migraine | CGRP | Erenumab | Migraine prevention in patients with chronic or episodic migraine. Reduction in monthly migraine days. Low adverse event burden. | [109,119,120,123,159,160,161,162,163] |
| Eptinezumab | Reduction in monthly migraine days in chronic migraine. Nasopharyngitis adverse event. | [124,127] | ||
| Fremanezumab | Reduction of headache severity and duration in patients with chronic or episodic migraine. Decrease in consumption of acute migraine medications. | [125,164,165,166,167,168] | ||
| Galcanezumab | Reduction in monthly migraine days in chronic or episodic migraines. Improvement in function. Mild pain and erythema in injection site. | [169,170] | ||
| Rheumatoid arthritis | IL-6 | Sarilumab | Improvement in pain and fatigue. | [86,87,171,172] |
| Tocilizumab | Improvement in signs and symptoms. Greater inhibition of joint damage and improvement in physical function with tocilizumab plus MTX vs. MTX alone. Infections adverse events. | [103,104,173] | ||
| TNF | Adalimumab | Improvement in pain and physical function. Risk of serious infections. | [174,175] | |
| Golimumab | Improvement in signs and symptoms with golimumab plus MTX vs. MTX alone. Infections adverse events. | [176,177] | ||
| Certolizumab | Improvement in signs and symptoms, pain, fatigue, and health-related quality of life. Increased chance of remission of RA and reduced joint damage. Respiratory tract infections. | [178,179] | ||
| Infliximab | Pain relief and inhibition of cartilage destruction. Decrease in the expression of inflammatory cytokines in the synovial fluid and cartilage. | [180,181] | ||
| CD20 in B cells | Rituximab | Improvement in physical function and health-related quality of life with rituximab plus MTX vs. MTX alone. Risk of serious infections. | [108,182] | |
| Neuropathic pain (DPN, PHN) | NGF | Tanezumab | Pain reduction in DPN. Pain reduction in PHN only at the highest dose. | [144,145] |
| Animal Model | Target | mAb | Method | Species | Pain Assessed | Effect | Reference |
|---|---|---|---|---|---|---|---|
| Neuropathic pain | MMP9 | MMP9 mAb clone 6-6B | Chemical paclitaxel | CD1 mice | Mechanical and thermal sensitivity | Reduction and prevention of mechanical allodynia | [30] |
| IL-20 | anti-IL-20 mAb (7E), anti-IL-20R1 mAb (51D) | Chemical paclitaxel | C57BL/6J mice | Mechanical and thermal sensitivity, motor impairment | Attenuation of mechanical allodynia, heat hypoesthesia and defects in motor coordination | [34] | |
| NGF | anti-NGF mAb (clone AS21) | Diabetes development | db/db mice | Mechanical sensitivity | Decrease of mechanical allodynia | [136] | |
| HMGB1 | anti-HMGB1 mAb (#10-22, IgG2a subclass) | Partial sciatic nerve ligation | ddy mice | Mechanical sensitivity | Decrease of mechanical allodynia | [35] | |
| Cancer pain | NGF | mAb911 | Tibial tumor inoculation | C57BL/6 mice | Spontaneous pain behavior | Decrease in guarding and flinching behavior of the affected hind paw | [43] |
| Bone fracture pain | NGF | mAb911 | Femur fracture | C57Bl/6J mice | Spontaneous locomotor activity | Higher horizontal distance travelled, increase of number of rearing episodes and average velocity | [155] |
10. Conclusions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Buss, N.A.P.S.; Henderson, S.J.; McFarlane, M.; Shenton, J.M.; de Haan, L. Monoclonal Antibody Therapeutics: History and Future. Curr. Opin. Pharmacol. 2012, 12, 615–622. [Google Scholar] [CrossRef] [PubMed]
- Parray, H.A.; Shukla, S.; Samal, S.; Shrivastava, T.; Ahmed, S.; Sharma, C.; Kumar, R. Hybridoma Technology a Versatile Method for Isolation of Monoclonal Antibodies, Its Applicability across Species, Limitations, Advancement and Future Perspectives. Int. Immunopharmacol. 2020, 85, 106639. [Google Scholar] [CrossRef]
- Kaunitz, J.D. Development of Monoclonal Antibodies: The Dawn of MAb Rule. Dig. Dis. Sci. 2017, 62, 831–832. [Google Scholar] [CrossRef] [PubMed]
- Parren, P.W.H.I.; Carter, P.J.; Plückthun, A. Changes to International Nonproprietary Names for Antibody Therapeutics 2017 and beyond: Of Mice, Men and More. mAbs 2017, 9, 898–906. [Google Scholar] [CrossRef]
- Bayer, V. An Overview of Monoclonal Antibodies. Semin. Oncol. Nurs. 2019, 35, 150927. [Google Scholar] [CrossRef]
- Jones, T.D.; Carter, P.J.; Plückthun, A.; Vásquez, M.; Holgate, R.G.E.; Hötzel, I.; Popplewell, A.G.; Parren, P.W.H.I.; Enzelberger, M.; Rademaker, H.J.; et al. The INNs and Outs of Antibody Nonproprietary Names. mAbs 2016, 8, 1–9. [Google Scholar] [CrossRef]
- Shepard, H.M.; Phillips, G.L.; Thanos, C.D.; Feldmann, M. Developments in Therapy with Monoclonal Antibodies and Related Proteins. Clin. Med. 2017, 17, 220–232. [Google Scholar] [CrossRef]
- García Merino, A. Monoclonal Antibodies. Basic Features. Neurolia 2011, 26, 301–306. [Google Scholar] [CrossRef]
- Lu, R.-M.; Hwang, Y.-C.; Liu, I.-J.; Lee, C.-C.; Tsai, H.-Z.; Li, H.-J.; Wu, H.-C. Development of Therapeutic Antibodies for the Treatment of Diseases. J. Biomed. Sci. 2020, 27, 1. [Google Scholar] [CrossRef]
- Anonymous. Similar Biological Medicinal Products. Available online: https://www.ema.europa.eu/en/similar-biological-medicinal-products (accessed on 28 July 2021).
- Declerck, P.; Danesi, R.; Petersel, D.; Jacobs, I. The Language of Biosimilars: Clarification, Definitions, and Regulatory Aspects. Drugs 2017, 77, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Castelli, M.S.; McGonigle, P.; Hornby, P.J. The Pharmacology and Therapeutic Applications of Monoclonal Antibodies. Pharmacol. Res. Perspect. 2019, 7, e00535. [Google Scholar] [CrossRef]
- Pandey, M.; Mahadevan, D. Monoclonal Antibodies as Therapeutics in Human Malignancies. Future Oncol. 2014, 10, 609–636. [Google Scholar] [CrossRef]
- Balakrishnan, P.B.; Sweeney, E.E.; Ramanujam, A.S.; Fernandes, R. Photothermal Therapies to Improve Immune Checkpoint Blockade for Cancer. Int. J. Hyperth. 2020, 37, 34–49. [Google Scholar] [CrossRef]
- Charmsaz, S.; Scott, A.M.; Boyd, A.W. Targeted Therapies in Hematological Malignancies Using Therapeutic Monoclonal Antibodies against Eph Family Receptors. Exp. Hematol. 2017, 54, 31–39. [Google Scholar] [CrossRef]
- Raja, S.N.; Carr, D.B.; Cohen, M.; Finnerup, N.B.; Flor, H.; Gibson, S.; Keefe, F.J.; Mogil, J.S.; Ringkamp, M.; Sluka, K.A.; et al. The Revised International Association for the Study of Pain Definition of Pain: Concepts, Challenges, and Compromises. Pain 2020, 161, 1976–1982. [Google Scholar] [CrossRef]
- Yeh, J.-F.; Akinci, A.; Al Shaker, M.; Chang, M.H.; Danilov, A.; Guillen, R.; Johnson, K.W.; Kim, Y.-C.; El-Shafei, A.A.; Skljarevski, V.; et al. Monoclonal Antibodies for Chronic Pain: A Practical Review of Mechanisms and Clinical Applications. Mol. Pain 2017, 13, 174480691774023. [Google Scholar] [CrossRef]
- Heinricher, M.M. Pain Modulation and the Transition from Acute to Chronic Pain. Adv. Exp. Med. Biol. 2016, 904, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Ji, R.-R.; Nackley, A.; Huh, Y.; Terrando, N.; Maixner, W. Neuroinflammation and Central Sensitization in Chronic and Widespread Pain. Anesthesiology 2018, 129, 343–366. [Google Scholar] [CrossRef] [PubMed]
- Haight, E.S.; Forman, T.E.; Cordonnier, S.A.; James, M.L.; Tawfik, V.L. Microglial Modulation as a Target for Chronic Pain: From the Bench to the Bedside and Back. Anesth. Analg. 2019, 128, 737–746. [Google Scholar] [CrossRef] [PubMed]
- Szok, D.; Tajti, J.; Nyári, A.; Vécsei, L. Therapeutic Approaches for Peripheral and Central Neuropathic Pain. Behav. Neurol. 2019, 2019, 8685954. [Google Scholar] [CrossRef]
- Matsuda, M.; Huh, Y.; Ji, R.-R. Roles of Inflammation, Neurogenic Inflammation, and Neuroinflammation in Pain. J. Anesth. 2019, 33, 131–139. [Google Scholar] [CrossRef]
- Bannwarth, B.; Kostine, M. Biologics in the Treatment of Chronic Pain: A New Era of Therapy? Clin. Pharmacol. Ther. 2015, 97, 122–124. [Google Scholar] [CrossRef] [PubMed]
- Mai, L.; Zhu, X.; Huang, F.; He, H.; Fan, W. P38 Mitogen-Activated Protein Kinase and Pain. Life Sci. 2020, 256, 117885. [Google Scholar] [CrossRef] [PubMed]
- Edelmayer, R.M.; Brederson, J.-D.; Jarvis, M.F.; Bitner, R.S. Biochemical and Pharmacological Assessment of MAP-Kinase Signaling along Pain Pathways in Experimental Rodent Models: A Potential Tool for the Discovery of Novel Antinociceptive Therapeutics. Biochem. Pharmacol. 2014, 87, 390–398. [Google Scholar] [CrossRef] [PubMed]
- McKelvey, L.; Shorten, G.D.; O’Keeffe, G.W. Nerve Growth Factor-Mediated Regulation of Pain Signalling and Proposed New Intervention Strategies in Clinical Pain Management. J. Neurochem. 2013, 124, 276–289. [Google Scholar] [CrossRef]
- Kim, S.H.; Nam, J.S.; Choi, D.K.; Koh, W.W.; Suh, J.H.; Song, J.G.; Shin, J.W.; Leem, J.G. Tumor Necrosis Factor-Alpha and Apoptosis Following Spinal Nerve Ligation Injury in Rats. Korean J. Pain 2011, 24, 185–190. [Google Scholar] [CrossRef]
- Kim, Y.; Remacle, A.G.; Chernov, A.V.; Liu, H.; Shubayev, I.; Lai, C.; Dolkas, J.; Shiryaev, S.A.; Golubkov, V.S.; Mizisin, A.P.; et al. The MMP-9/TIMP-1 Axis Controls the Status of Differentiation and Function of Myelin-Forming Schwann Cells in Nerve Regeneration. PLoS ONE 2012, 7, e33664. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, Y.; Xu, Z.-Z.; Wang, X.; Park, J.Y.; Zhuang, Z.-Y.; Tan, P.-H.; Gao, Y.-J.; Roy, K.; Corfas, G.; Lo, E.H.; et al. Distinct Roles of Matrix Metalloproteases in the Early- and Late-Phase Development of Neuropathic Pain. Nat. Med. 2008, 14, 331–336. [Google Scholar] [CrossRef]
- Tonello, R.; Lee, S.H.; Berta, T. Monoclonal Antibody Targeting the Matrix Metalloproteinase 9 Prevents and Reverses Paclitaxel-Induced Peripheral Neuropathy in Mice. J. Pain 2019, 20, 515–527. [Google Scholar] [CrossRef]
- Bigal, M.E.; Walter, S.; Rapoport, A.M. Calcitonin Gene-Related Peptide (CGRP) and Migraine Current Understanding and State of Development. Headache 2013, 53, 1230–1244. [Google Scholar] [CrossRef]
- Sebba, A. Pain: A Review of Interleukin-6 and Its Roles in the Pain of Rheumatoid Arthritis. Open Access Rheumatol. Res. Rev. 2021, 13, 31–43. [Google Scholar] [CrossRef]
- Kang, S.; Tanaka, T.; Kishimoto, T. Therapeutic Uses of Anti-Interleukin-6 Receptor Antibody. Int. Immunol. 2015, 27, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.-H.; Yeh, Y.-M.; Chen, Y.-F.; Hsu, Y.-H.; Wang, H.-H.; Lin, P.-C.; Chang, L.-Y.; Lin, C.-C.K.; Chang, M.-S.; Shen, M.-R. Targeting Interleukin-20 Alleviates Paclitaxel-Induced Peripheral Neuropathy. PAIN 2020, 161, 1237–1254. [Google Scholar] [CrossRef]
- Zhang, F.F.; Morioka, N.; Harano, S.; Nakamura, Y.; Liu, K.; Nishibori, M.; Hisaoka-Nakashima, K.; Nakata, Y. Perineural Expression of High-Mobility Group Box-1 Contributes to Long-Lasting Mechanical Hypersensitivity via Matrix Metalloprotease-9 up-Regulation in Mice with Painful Peripheral Neuropathy. J. Neurochem. 2016, 136, 837–850. [Google Scholar] [CrossRef] [PubMed]
- Maeda, T.; Ozaki, M.; Kobayashi, Y.; Kiguchi, N.; Kishioka, S. HMGB1 as a Potential Therapeutic Target for Neuropathic Pain. J. Pharmacol. Sci. 2013, 123, 301–305. [Google Scholar] [CrossRef]
- Ren, P.-C.; Zhang, Y.; Zhang, X.-D.; An, L.-J.; Lv, H.-G.; He, J.; Gao, C.-J.; Sun, X.-D. High-Mobility Group Box 1 Contributes to Mechanical Allodynia and Spinal Astrocytic Activation in a Mouse Model of Type 2 Diabetes. Brain Res. Bull. 2012, 88, 332–337. [Google Scholar] [CrossRef]
- Tong, W.; Wang, W.; Huang, J.; Ren, N.; Wu, S.-X.; Li, Y.-Q. Spinal High-Mobility Group Box 1 Contributes to Mechanical Allodynia in a Rat Model of Bone Cancer Pain. Biochem. Biophys. Res. Commun. 2010, 395, 572–576. [Google Scholar] [CrossRef]
- Shibasaki, M.; Sasaki, M.; Miura, M.; Mizukoshi, K.; Ueno, H.; Hashimoto, S.; Tanaka, Y.; Amaya, F. Induction of High Mobility Group Box-1 in Dorsal Root Ganglion Contributes to Pain Hypersensitivity after Peripheral Nerve Injury. Pain 2010, 149, 514–521. [Google Scholar] [CrossRef]
- Nakamura, Y.; Morioka, N.; Abe, H.; Zhang, F.F.; Hisaoka-Nakashima, K.; Liu, K.; Nishibori, M.; Nakata, Y. Neuropathic Pain in Rats with a Partial Sciatic Nerve Ligation Is Alleviated by Intravenous Injection of Monoclonal Antibody to High Mobility Group Box-1. PLoS ONE 2013, 8, e73640. [Google Scholar] [CrossRef] [PubMed]
- Kochi, T.; Nakamura, Y.; Ma, S.; Hisaoka-Nakashima, K.; Wang, D.; Liu, K.; Wake, H.; Nishibori, M.; Irifune, M.; Morioka, N. Pretreatment with High Mobility Group Box-1 Monoclonal Antibody Prevents the Onset of Trigeminal Neuropathy in Mice with a Distal Infraorbital Nerve Chronic Constriction Injury. Molecules 2021, 26, 2035. [Google Scholar] [CrossRef]
- Guo, L.-H.; Schluesener, H.J. The Innate Immunity of the Central Nervous System in Chronic Pain: The Role of Toll-like Receptors. Cell. Mol. Life Sci. 2007, 64, 1128–1136. [Google Scholar] [CrossRef]
- Buehlmann, D.; Ielacqua, G.D.; Xandry, J.; Rudin, M. Prospective Administration of Anti-Nerve Growth Factor Treatment Effectively Suppresses Functional Connectivity Alterations after Cancer-Induced Bone Pain in Mice. Pain 2019, 160, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Lotze, M.T.; Tracey, K.J. High-Mobility Group Box 1 Protein (HMGB1): Nuclear Weapon in the Immune Arsenal. Nat. Rev. Immunol. 2005, 5, 331–342. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.P.-C.; Hunter, D.J. Emerging Drugs for the Treatment of Knee Osteoarthritis. Expert Opin. Emerg. Drugs 2015, 20, 361–378. [Google Scholar] [CrossRef] [PubMed]
- Hunter, D.J.; Bierma-Zeinstra, S. Osteoarthritis. Lancet 2019, 393, 1745–1759. [Google Scholar] [CrossRef]
- Schmelz, M.; Mantyh, P.; Malfait, A.-M.; Farrar, J.; Yaksh, T.; Tive, L.; Viktrup, L. Nerve Growth Factor Antibody for the Treatment of Osteoarthritis Pain and Chronic Low-Back Pain: Mechanism of Action in the Context of Efficacy and Safety. Pain 2019, 160, 2210–2220. [Google Scholar] [CrossRef] [PubMed]
- Blikman, T.; Rienstra, W.; van Raay, J.J.A.M.; Dijkstra, B.; Bulstra, S.K.; Stevens, M.; van den Akker-Scheek, I. Neuropathic-like Symptoms and the Association with Joint-Specific Function and Quality of Life in Patients with Hip and Knee Osteoarthritis. PLoS ONE 2018, 13, e0199165. [Google Scholar] [CrossRef] [PubMed]
- Berenbaum, F.; Blanco, F.J.; Guermazi, A.; Miki, K.; Yamabe, T.; Viktrup, L.; Junor, R.; Carey, W.; Brown, M.T.; West, C.R.; et al. Subcutaneous Tanezumab for Osteoarthritis of the Hip or Knee: Efficacy and Safety Results from a 24-Week Randomised Phase III Study with a 24-Week Follow-up Period. Ann. Rheum. Dis. 2020, 79, 800–810. [Google Scholar] [CrossRef]
- Cai, X.; Yuan, S.; Zeng, Y.; Wang, C.; Yu, N.; Ding, C. New Trends in Pharmacological Treatments for Osteoarthritis. Front. Pharmacol. 2021, 12, 645842. [Google Scholar] [CrossRef]
- Wise, B.L.; Seidel, M.F.; Lane, N.E. The Evolution of Nerve Growth Factor Inhibition in Clinical Medicine. Nat. Rev. Rheumatol. 2021, 17, 34–46. [Google Scholar] [CrossRef]
- Ashraf, S.; Mapp, P.I.; Burston, J.; Bennett, A.J.; Chapman, V.; Walsh, D.A. Augmented Pain Behavioural Responses to Intra-Articular Injection of Nerve Growth Factor in Two Animal Models of Osteoarthritis. Ann. Rheum. Dis. 2014, 73, 1710–1718. [Google Scholar] [CrossRef]
- Hoshino, T.; Tsuji, K.; Onuma, H.; Udo, M.; Ueki, H.; Akiyama, M.; Abula, K.; Katagiri, H.; Miyatake, K.; Watanabe, T.; et al. Persistent Synovial Inflammation Plays Important Roles in Persistent Pain Development in the Rat Knee before Cartilage Degradation Reaches the Subchondral Bone. BMC Musculoskelet. Disord. 2018, 19, 291. [Google Scholar] [CrossRef]
- Zhu, S.; Zhu, J.; Zhen, G.; Hu, Y.; An, S.; Li, Y.; Zheng, Q.; Chen, Z.; Yang, Y.; Wan, M.; et al. Subchondral Bone Osteoclasts Induce Sensory Innervation and Osteoarthritis Pain. J. Clin. Investig. 2019, 129, 1076–1093. [Google Scholar] [CrossRef]
- Hong, J.-I.; Park, I.Y.; Kim, H.A. Understanding the Molecular Mechanisms Underlying the Pathogenesis of Arthritis Pain Using Animal Models. Int. J. Mol. Sci. 2020, 21, 533. [Google Scholar] [CrossRef] [PubMed]
- McNamee, K.E.; Burleigh, A.; Gompels, L.L.; Feldmann, M.; Allen, S.J.; Williams, R.O.; Dawbarn, D.; Vincent, T.L.; Inglis, J.J. Treatment of Murine Osteoarthritis with TrkAd5 Reveals a Pivotal Role for Nerve Growth Factor in Non-Inflammatory Joint Pain. Pain 2010, 149, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Kc, R.; Li, X.; Kroin, J.S.; Liu, Z.; Chen, D.; Xiao, G.; Levine, B.; Li, J.; Hamilton, J.L.; van Wijnen, A.J.; et al. PKCδ Null Mutations in a Mouse Model of Osteoarthritis Alter Osteoarthritic Pain Independently of Joint Pathology by Augmenting NGF/TrkA-Induced Axonal Outgrowth. Ann. Rheum. Dis. 2016, 75, 2133–2141. [Google Scholar] [CrossRef]
- LaBranche, T.P.; Bendele, A.M.; Omura, B.C.; Gropp, K.E.; Hurst, S.I.; Bagi, C.M.; Cummings, T.R.; Grantham, L.E.; Shelton, D.L.; Zorbas, M.A. Nerve Growth Factor Inhibition with Tanezumab Influences Weight-Bearing and Subsequent Cartilage Damage in the Rat Medial Meniscal Tear Model. Ann. Rheum. Dis. 2017, 76, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Majuta, L.A.; Guedon, J.-M.G.; Mitchell, S.A.T.; Ossipov, M.H.; Mantyh, P.W. Anti-Nerve Growth Factor Therapy Increases Spontaneous Day/Night Activity in Mice with Orthopedic Surgery-Induced Pain. Pain 2017, 158, 605–617. [Google Scholar] [CrossRef] [PubMed]
- Flannery, C.R.; Moran, N.; Blasioli, D.; Donahue, K.; Kane, J.; Gladysheva, T.; Dagher, R.; Fang, R.; Vardanyan, A.; Bangari, D.; et al. Efficacy of a Novel, Locally Delivered TrkA Inhibitor in Preclinical Models of OA and Joint Pain. Osteoarthr. Cartil. 2015, 23, A45–A46. [Google Scholar] [CrossRef][Green Version]
- Ishikawa, G.; Koya, Y.; Tanaka, H.; Nagakura, Y. Long-Term Analgesic Effect of a Single Dose of Anti-NGF Antibody on Pain during Motion without Notable Suppression of Joint Edema and Lesion in a Rat Model of Osteoarthritis. Osteoarthr. Cartil. 2015, 23, 925–932. [Google Scholar] [CrossRef]
- Bryden, L.A.; Nicholson, J.R.; Doods, H.; Pekcec, A. Deficits in Spontaneous Burrowing Behavior in the Rat Bilateral Monosodium Iodoacetate Model of Osteoarthritis: An Objective Measure of Pain-Related Behavior and Analgesic Efficacy. Osteoarthr. Cartil. 2015, 23, 1605–1612. [Google Scholar] [CrossRef]
- Xu, L.; Nwosu, L.N.; Burston, J.J.; Millns, P.J.; Sagar, D.R.; Mapp, P.I.; Meesawatsom, P.; Li, L.; Bennett, A.J.; Walsh, D.A.; et al. The Anti-NGF Antibody MuMab 911 Both Prevents and Reverses Pain Behaviour and Subchondral Osteoclast Numbers in a Rat Model of Osteoarthritis Pain. Osteoarthr. Cartil. 2016, 24, 1587–1595. [Google Scholar] [CrossRef]
- Miyagi, M.; Ishikawa, T.; Kamoda, H.; Suzuki, M.; Inoue, G.; Sakuma, Y.; Oikawa, Y.; Orita, S.; Uchida, K.; Takahashi, K.; et al. Efficacy of Nerve Growth Factor Antibody in a Knee Osteoarthritis Pain Model in Mice. BMC Musculoskelet. Disord. 2017, 18, 428. [Google Scholar] [CrossRef]
- Larkin, J.; Lohr, T.A.; Elefante, L.; Shearin, J.; Matico, R.; Su, J.-L.; Xue, Y.; Liu, F.; Genell, C.; Miller, R.E.; et al. Translational Development of an ADAMTS-5 Antibody for Osteoarthritis Disease Modification. Osteoarthr. Cartil. 2015, 23, 1254–1266. [Google Scholar] [CrossRef] [PubMed]
- Nwosu, L.N.; Mapp, P.I.; Chapman, V.; Walsh, D.A. Blocking the Tropomyosin Receptor Kinase A (TrkA) Receptor Inhibits Pain Behaviour in Two Rat Models of Osteoarthritis. Ann. Rheum. Dis. 2016, 75, 1246–1254. [Google Scholar] [CrossRef] [PubMed]
- Lascelles, B.D.X.; Knazovicky, D.; Case, B.; Freire, M.; Innes, J.F.; Drew, A.C.; Gearing, D.P. A Canine-Specific Anti-Nerve Growth Factor Antibody Alleviates Pain and Improves Mobility and Function in Dogs with Degenerative Joint Disease-Associated Pain. BMC Vet. Res. 2015, 11, 101. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.T.; Murphy, F.T.; Radin, D.M.; Davignon, I.; Smith, M.D.; West, C.R. Tanezumab Reduces Osteoarthritic Knee Pain: Results of a Randomized, Double-Blind, Placebo-Controlled Phase III Trial. J. Pain 2012, 13, 790–798. [Google Scholar] [CrossRef]
- Ekman, E.F.; Gimbel, J.S.; Bello, A.E.; Smith, M.D.; Keller, D.S.; Annis, K.M.; Brown, M.T.; West, C.R.; Verburg, K.M. Efficacy and Safety of Intravenous Tanezumab for the Symptomatic Treatment of Osteoarthritis: 2 Randomized Controlled Trials versus Naproxen. J. Rheumatol. 2014, 41, 2249–2259. [Google Scholar] [CrossRef] [PubMed]
- Birbara, C.; Dabezies, E.J.; Burr, A.M.; Fountaine, R.J.; Smith, M.D.; Brown, M.T.; West, C.R.; Arends, R.H.; Verburg, K.M. Safety and Efficacy of Subcutaneous Tanezumab in Patients with Knee or Hip Osteoarthritis. J. Pain Res. 2018, 11, 151–164. [Google Scholar] [CrossRef]
- Schnitzer, T.J.; Khan, A.; Bessette, L.; Davignon, I.; Brown, M.T.; Pixton, G.; Prucka, W.R.; Tive, L.; Viktrup, L.; West, C.R. Onset and Maintenance of Efficacy of Subcutaneous Tanezumab in Patients with Moderate to Severe Osteoarthritis of the Knee or Hip: A 16-Week Dose-Titration Study. Semin. Arthritis Rheum. 2020, 50, 387–393. [Google Scholar] [CrossRef]
- Tive, L.; Bello, A.E.; Radin, D.; Schnitzer, T.J.; Nguyen, H.; Brown, M.T.; West, C.R. Pooled Analysis of Tanezumab Efficacy and Safety with Subgroup Analyses of Phase III Clinical Trials in Patients with Osteoarthritis Pain of the Knee or Hip. J. Pain Res. 2019, 12, 975–995. [Google Scholar] [CrossRef]
- Mayorga, A.J.; Wang, S.; Kelly, K.M.; Thipphawong, J. Efficacy and Safety of Fulranumab as Monotherapy in Patients with Moderate to Severe, Chronic Knee Pain of Primary Osteoarthritis: A Randomised, Placebo- and Active-Controlled Trial. Int. J. Clin. Pract. 2016, 70, 493–505. [Google Scholar] [CrossRef]
- Sanga, P.; Katz, N.; Polverejan, E.; Wang, S.; Kelly, K.M.; Haeussler, J.; Thipphawong, J. Long-Term Safety and Efficacy of Fulranumab in Patients with Moderate-to-Severe Osteoarthritis Pain: A Phase II Randomized, Double-Blind, Placebo-Controlled Extension Study. Arthritis Rheumatol. 2017, 69, 763–773. [Google Scholar] [CrossRef] [PubMed]
- Dakin, P.; DiMartino, S.J.; Gao, H.; Maloney, J.; Kivitz, A.J.; Schnitzer, T.J.; Stahl, N.; Yancopoulos, G.D.; Geba, G.P. The Efficacy, Tolerability, and Joint Safety of Fasinumab in Osteoarthritis Pain: A Phase IIb/III Double-Blind, Placebo-Controlled, Randomized Clinical Trial. Arthritis Rheumatol. 2019, 71, 1824–1834. [Google Scholar] [CrossRef]
- Balanescu, A.R.; Feist, E.; Wolfram, G.; Davignon, I.; Smith, M.D.; Brown, M.T.; West, C.R. Efficacy and Safety of Tanezumab Added on to Diclofenac Sustained Release in Patients with Knee or Hip Osteoarthritis: A Double-Blind, Placebo-Controlled, Parallel-Group, Multicentre Phase III Randomised Clinical Trial. Ann. Rheum. Dis. 2014, 73, 1665–1672. [Google Scholar] [CrossRef] [PubMed]
- Schnitzer, T.J.; Ekman, E.F.; Spierings, E.L.H.; Greenberg, H.S.; Smith, M.D.; Brown, M.T.; West, C.R.; Verburg, K.M. Efficacy and Safety of Tanezumab Monotherapy or Combined with Non-Steroidal Anti-Inflammatory Drugs in the Treatment of Knee or Hip Osteoarthritis Pain. Ann. Rheum. Dis. 2015, 74, 1202–1211. [Google Scholar] [CrossRef] [PubMed]
- Hochberg, M.C.; Carrino, J.A.; Schnitzer, T.J.; Guermazi, A.; Walsh, D.A.; White, A.; Nakajo, S.; Fountaine, R.J.; Hickman, A.; Pixton, G.; et al. Long-Term Safety and Efficacy of Subcutaneous Tanezumab Versus Nonsteroidal Antiinflammatory Drugs for Hip or Knee Osteoarthritis: A Randomized Trial. Arthritis Rheumatol. 2021, 73, 1167–1177. [Google Scholar] [CrossRef]
- Spierings, E.L.H.; Fidelholtz, J.; Wolfram, G.; Smith, M.D.; Brown, M.T.; West, C.R. A Phase III Placebo- and Oxycodone-Controlled Study of Tanezumab in Adults with Osteoarthritis Pain of the Hip or Knee. Pain 2013, 154, 1603–1612. [Google Scholar] [CrossRef]
- Brown, M.T.; Murphy, F.T.; Radin, D.M.; Davignon, I.; Smith, M.D.; West, C.R. Tanezumab Reduces Osteoarthritic Hip Pain: Results of a Randomized, Double-Blind, Placebo-Controlled Phase III Trial. Arthritis Rheum. 2013, 65, 1795–1803. [Google Scholar] [CrossRef]
- Lane, N.E.; Schnitzer, T.J.; Birbara, C.A.; Mokhtarani, M.; Shelton, D.L.; Smith, M.D.; Brown, M.T. Tanezumab for the Treatment of Pain from Osteoarthritis of the Knee. N. Engl. J. Med. 2010, 363, 1521–1531. [Google Scholar] [CrossRef]
- Berenbaum, F.; Langford, R.; Perrot, S.; Miki, K.; Blanco, F.J.; Yamabe, T.; Isogawa, N.; Junor, R.; Carey, W.; Viktrup, L.; et al. Subcutaneous Tanezumab for Osteoarthritis: Is the Early Improvement in Pain and Function Meaningful and Sustained? Eur. J. Pain 2021, 1525–1539. [Google Scholar] [CrossRef]
- Schnitzer, T.J.; Easton, R.; Pang, S.; Levinson, D.J.; Pixton, G.; Viktrup, L.; Davignon, I.; Brown, M.T.; West, C.R.; Verburg, K.M. Effect of Tanezumab on Joint Pain, Physical Function, and Patient Global Assessment of Osteoarthritis Among Patients with Osteoarthritis of the Hip or Knee: A Randomized Clinical Trial. JAMA 2019, 322, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Bimonte, S.; Cascella, M.; Forte, C.A.; Esposito, G.; Cuomo, A. The Role of Anti-Nerve Growth Factor Monoclonal Antibodies in the Control of Chronic Cancer and Non-Cancer Pain. J. Pain Res. 2021, 14, 1959–1967. [Google Scholar] [CrossRef] [PubMed]
- Sparks, J.A. Rheumatoid Arthritis. Ann. Intern. Med. 2019, 170, ITC1–ITC16. [Google Scholar] [CrossRef] [PubMed]
- Atzeni, F.; Nucera, V.; Masala, I.F.; Sarzi-Puttini, P.; Bonitta, G. Il-6 Involvement in Pain, Fatigue and Mood Disorders in Rheumatoid Arthritis and the Effects of Il-6 Inhibitor Sarilumab. Pharmacol. Res. 2019, 149, 104402. [Google Scholar] [CrossRef]
- Crotti, C.; Biggioggero, M.; Becciolini, A.; Favalli, E.G. Sarilumab: Patient-Reported Outcomes in Rheumatoid Arthritis. Patient Relat. Outcome Meas. 2018, 9, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, J.E.; Santos, M.J.; Canhão, H.; Choy, E. Interleukin-6 as a Key Player in Systemic Inflammation and Joint Destruction. Autoimmun. Rev. 2009, 8, 538–542. [Google Scholar] [CrossRef]
- Song, S.-N.J.; Tomosugi, N.; Kawabata, H.; Ishikawa, T.; Nishikawa, T.; Yoshizaki, K. Down-Regulation of Hepcidin Resulting from Long-Term Treatment with an Anti-IL-6 Receptor Antibody (Tocilizumab) Improves Anemia of Inflammation in Multicentric Castleman Disease. Blood 2010, 116, 3627–3634. [Google Scholar] [CrossRef]
- Bullock, J.; Rizvi, S.A.A.; Saleh, A.M.; Ahmed, S.S.; Do, D.P.; Ansari, R.A.; Ahmed, J. Rheumatoid Arthritis: A Brief Overview of the Treatment. Med. Princ. Pract. 2019, 27, 501–507. [Google Scholar] [CrossRef]
- Mahmood, Z.; Schmalzing, M.; Dörner, T.; Tony, H.-P.; Muhammad, K. Therapeutic Cytokine Inhibition Modulates Activation and Homing Receptors of Peripheral Memory B Cell Subsets in Rheumatoid Arthritis Patients. Front. Immunol. 2020, 11, 572475. [Google Scholar] [CrossRef]
- Zhang, A.; Lee, Y.C. Mechanisms for Joint Pain in Rheumatoid Arthritis (RA): From Cytokines to Central Sensitization. Curr. Osteoporos. Rep. 2018, 16, 603–610. [Google Scholar] [CrossRef]
- Lee, H.; Lee, M.-Y.; Bhang, S.H.; Kim, B.-S.; Kim, Y.S.; Ju, J.H.; Kim, K.S.; Hahn, S.K. Hyaluronate-Gold Nanoparticle/Tocilizumab Complex for the Treatment of Rheumatoid Arthritis. ACS Nano 2014, 8, 4790–4798. [Google Scholar] [CrossRef]
- Monnet, E.; Shang, L.; Lapeyre, G.; deGraaf, K.; Hatterer, E.; Buatois, V.; Elson, G.; Ferlin, W.; Gabay, C.; Sokolove, J.; et al. AB0451 NI-0101, a Monoclonal Antibody Targeting Toll Like Receptor 4 (TLR4) Being Developed for Rheumatoid Arthritis (RA) Treatment with a Potential for Personalized Medicine. Ann. Rheum. Dis. 2015, 74, 1046. [Google Scholar] [CrossRef]
- Ashraf, S.; Bouhana, K.S.; Pheneger, J.; Andrews, S.W.; Walsh, D.A. Selective Inhibition of Tropomyosin-Receptor-Kinase A (TrkA) Reduces Pain and Joint Damage in Two Rat Models of Inflammatory Arthritis. Arthritis Res. Ther. 2016, 18, 97. [Google Scholar] [CrossRef]
- Segond von Banchet, G.; König, C.; Patzer, J.; Eitner, A.; Leuchtweis, J.; Ebbinghaus, M.; Boettger, M.K.; Schaible, H.-G. Long-Lasting Activation of the Transcription Factor CREB in Sensory Neurons by Interleukin-1β During Antigen-Induced Arthritis in Rats: A Mechanism of Persistent Arthritis Pain? Arthritis Rheumatol. 2016, 68, 532–541. [Google Scholar] [CrossRef] [PubMed]
- Bonetti, N.R.; Diaz-Cañestro, C.; Liberale, L.; Crucet, M.; Akhmedov, A.; Merlini, M.; Reiner, M.F.; Gobbato, S.; Stivala, S.; Kollias, G.; et al. Tumour Necrosis Factor-α Inhibition Improves Stroke Outcome in a Mouse Model of Rheumatoid Arthritis. Sci. Rep. 2019, 9, 2173. [Google Scholar] [CrossRef] [PubMed]
- Makalish, T.P.; Golovkin, I.O.; Oberemok, V.V.; Laikova, K.V.; Temirova, Z.Z.; Serdyukova, O.A.; Novikov, I.A.; Rosovskyi, R.A.; Gordienko, A.I.; Zyablitskaya, E.Y.; et al. Anti-Rheumatic Effect of Antisense Oligonucleotide Cytos-11 Targeting TNF-α Expression. Int. J. Mol. Sci. 2021, 22, 1022. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-A.; Hahm, D.-H.; Kim, J.Y.; Sur, B.; Lee, H.M.; Ryu, C.J.; Yang, H.-I.; Kim, K.S. Potential Therapeutic Antibodies Targeting Specific Adiponectin Isoforms in Rheumatoid Arthritis. Arthritis Res. Ther. 2018, 20, 245. [Google Scholar] [CrossRef]
- Wang, L.; Jiang, X.; Zheng, Q.; Jeon, S.-M.; Chen, T.; Liu, Y.; Kulaga, H.; Reed, R.; Dong, X.; Caterina, M.J.; et al. Neuronal FcγRI Mediates Acute and Chronic Joint Pain. J. Clin. Investig. 2019, 129, 3754–3769. [Google Scholar] [CrossRef] [PubMed]
- Lamb, Y.N.; Deeks, E.D. Sarilumab: A Review in Moderate to Severe Rheumatoid Arthritis. Drugs 2018, 78, 929–940. [Google Scholar] [CrossRef]
- Chen, Y.-F.; Jobanputra, P.; Barton, P.; Jowett, S.; Bryan, S.; Clark, W.; Fry-Smith, A.; Burls, A. A Systematic Review of the Effectiveness of Adalimumab, Etanercept and Infliximab for the Treatment of Rheumatoid Arthritis in Adults and an Economic Evaluation of Their Cost-Effectiveness. Health Technol. Assess. 2006, 10. [Google Scholar] [CrossRef]
- Smolen, J.S.; Beaulieu, A.; Rubbert-Roth, A.; Ramos-Remus, C.; Rovensky, J.; Alecock, E.; Woodworth, T.; Alten, R. OPTION Investigators Effect of Interleukin-6 Receptor Inhibition with Tocilizumab in Patients with Rheumatoid Arthritis (OPTION Study): A Double-Blind, Placebo-Controlled, Randomised Trial. Lancet 2008, 371, 987–997. [Google Scholar] [CrossRef]
- Kremer, J.M.; Blanco, R.; Brzosko, M.; Burgos-Vargas, R.; Halland, A.-M.; Vernon, E.; Ambs, P.; Fleischmann, R. Tocilizumab Inhibits Structural Joint Damage in Rheumatoid Arthritis Patients with Inadequate Responses to Methotrexate: Results from the Double-Blind Treatment Phase of a Randomized Placebo-Controlled Trial of Tocilizumab Safety and Prevention of Structural Joint Damage at One Year. Arthritis Rheum. 2011, 63, 609–621. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, R.M.; Halland, A.-M.; Brzosko, M.; Burgos-Vargas, R.; Mela, C.; Vernon, E.; Kremer, J.M. Tocilizumab Inhibits Structural Joint Damage and Improves Physical Function in Patients with Rheumatoid Arthritis and Inadequate Responses to Methotrexate: LITHE Study 2-Year Results. J. Rheumatol. 2013, 40, 113–126. [Google Scholar] [CrossRef]
- Almeida, C.; Choy, E.H.S.; Hewlett, S.; Kirwan, J.R.; Cramp, F.; Chalder, T.; Pollock, J.; Christensen, R. Biologic Interventions for Fatigue in Rheumatoid Arthritis. Cochrane Database Syst. Rev. 2016, CD008334. [Google Scholar] [CrossRef] [PubMed]
- Tumor Necrosis Factor Antagonists. LiverTox: Clinical and Research Information on Drug-Induced Liver Injury; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2012.
- Mok, C.C. Rituximab for the Treatment of Rheumatoid Arthritis: An Update. Drug Des. Devel. Ther. 2013, 8, 87–100. [Google Scholar] [CrossRef]
- Sacco, S.; Bendtsen, L.; Ashina, M.; Reuter, U.; Terwindt, G.; Mitsikostas, D.-D.; Martelletti, P. European Headache Federation Guideline on the Use of Monoclonal Antibodies Acting on the Calcitonin Gene Related Peptide or Its Receptor for Migraine Prevention. J. Headache Pain 2019, 20, 6. [Google Scholar] [CrossRef]
- Charles, A.; Pozo-Rosich, P. Targeting Calcitonin Gene-Related Peptide: A New Era in Migraine Therapy. Lancet 2019, 394, 1765–1774. [Google Scholar] [CrossRef]
- Yuan, H.; Lauritsen, C.G.; Kaiser, E.A.; Silberstein, S.D. CGRP Monoclonal Antibodies for Migraine: Rationale and Progress. BioDrugs 2017, 31, 487–501. [Google Scholar] [CrossRef]
- Hansen, J.M.; Hauge, A.W.; Olesen, J.; Ashina, M. Calcitonin Gene-Related Peptide Triggers Migraine-like Attacks in Patients with Migraine with Aura. Cephalalgia 2010, 30, 1179–1186. [Google Scholar] [CrossRef] [PubMed]
- Raddant, A.C.; Russo, A.F. Calcitonin Gene-Related Peptide in Migraine: Intersection of Peripheral Inflammation and Central Modulation. Expert Rev. Mol. Med. 2011, 13, e36. [Google Scholar] [CrossRef] [PubMed]
- Iyengar, S.; Ossipov, M.H.; Johnson, K.W. The Role of Calcitonin Gene-Related Peptide in Peripheral and Central Pain Mechanisms Including Migraine. Pain 2017, 158, 543–559. [Google Scholar] [CrossRef]
- Wattiez, A.-S.; Wang, M.; Russo, A.F. CGRP in Animal Models of Migraine. Handb. Exp. Pharmacol. 2019, 255, 85–107. [Google Scholar] [CrossRef] [PubMed]
- Mason, B.N.; Kaiser, E.A.; Kuburas, A.; Loomis, M.-C.M.; Latham, J.A.; Garcia-Martinez, L.F.; Russo, A.F. Induction of Migraine-Like Photophobic Behavior in Mice by Both Peripheral and Central CGRP Mechanisms. J. Neurosci. 2017, 37, 204–216. [Google Scholar] [CrossRef]
- Rea, B.J.; Wattiez, A.-S.; Waite, J.S.; Castonguay, W.C.; Schmidt, C.M.; Fairbanks, A.M.; Robertson, B.R.; Brown, C.J.; Mason, B.N.; Moldovan-Loomis, M.-C.; et al. Peripherally Administered Calcitonin Gene-Related Peptide Induces Spontaneous Pain in Mice: Implications for Migraine. Pain 2018, 159, 2306–2317. [Google Scholar] [CrossRef]
- Wattiez, A.-S.; Sowers, L.P.; Russo, A.F. Calcitonin Gene-Related Peptide (CGRP): Role in Migraine Pathophysiology and Therapeutic Targeting. Expert Opin. Ther. Targets 2020, 24, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Dodick, D.W.; Ashina, M.; Brandes, J.L.; Kudrow, D.; Lanteri-Minet, M.; Osipova, V.; Palmer, K.; Picard, H.; Mikol, D.D.; Lenz, R.A. ARISE: A Phase 3 Randomized Trial of Erenumab for Episodic Migraine. Cephalalgia 2018, 38, 1026–1037. [Google Scholar] [CrossRef]
- Sun, H.; Dodick, D.W.; Silberstein, S.; Goadsby, P.J.; Reuter, U.; Ashina, M.; Saper, J.; Cady, R.; Chon, Y.; Dietrich, J.; et al. Safety and Efficacy of AMG 334 for Prevention of Episodic Migraine: A Randomised, Double-Blind, Placebo-Controlled, Phase 2 Trial. Lancet Neurol. 2016, 15, 382–390. [Google Scholar] [CrossRef]
- Ashina, M.; Saper, J.; Cady, R.; Schaeffler, B.A.; Biondi, D.M.; Hirman, J.; Pederson, S.; Allan, B.; Smith, J. Eptinezumab in Episodic Migraine: A Randomized, Double-Blind, Placebo-Controlled Study (PROMISE-1). Cephalalgia 2020, 40, 241–254. [Google Scholar] [CrossRef]
- Smith, T.R.; Janelidze, M.; Chakhava, G.; Cady, R.; Hirman, J.; Allan, B.; Pederson, S.; Smith, J.; Schaeffler, B. Eptinezumab for the Prevention of Episodic Migraine: Sustained Effect Through 1 Year of Treatment in the PROMISE-1 Study. Clin. Ther. 2020, 42, 2254–2265.e3. [Google Scholar] [CrossRef]
- Tepper, S.; Ashina, M.; Reuter, U.; Brandes, J.L.; Doležil, D.; Silberstein, S.; Winner, P.; Leonardi, D.; Mikol, D.; Lenz, R. Safety and Efficacy of Erenumab for Preventive Treatment of Chronic Migraine: A Randomised, Double-Blind, Placebo-Controlled Phase 2 Trial. Lancet Neurol. 2017, 16, 425–434. [Google Scholar] [CrossRef]
- Lipton, R.B.; Goadsby, P.J.; Smith, J.; Schaeffler, B.A.; Biondi, D.M.; Hirman, J.; Pederson, S.; Allan, B.; Cady, R. Efficacy and Safety of Eptinezumab in Patients with Chronic Migraine: PROMISE-2. Neurology 2020, 94, e1365–e1377. [Google Scholar] [CrossRef] [PubMed]
- Bigal, M.E.; Edvinsson, L.; Rapoport, A.M.; Lipton, R.B.; Spierings, E.L.H.; Diener, H.-C.; Burstein, R.; Loupe, P.S.; Ma, Y.; Yang, R.; et al. Safety, Tolerability, and Efficacy of TEV-48125 for Preventive Treatment of Chronic Migraine: A Multicentre, Randomised, Double-Blind, Placebo-Controlled, Phase 2b Study. Lancet Neurol. 2015, 14, 1091–1100. [Google Scholar] [CrossRef]
- Silberstein, S.; Diamond, M.; Hindiyeh, N.A.; Biondi, D.M.; Cady, R.; Hirman, J.; Allan, B.; Pederson, S.; Schaeffler, B.; Smith, J. Eptinezumab for the Prevention of Chronic Migraine: Efficacy and Safety through 24 Weeks of Treatment in the Phase 3 PROMISE-2 (Prevention of Migraine via Intravenous ALD403 Safety and Efficacy-2) Study. J. Headache Pain 2020, 21, 120. [Google Scholar] [CrossRef] [PubMed]
- Villar-Martínez, M.D.; Moreno-Ajona, D.; Goadsby, P.J. Eptinezumab for the Preventive Treatment of Migraine. Pain Manag. 2021, 11, 113–121. [Google Scholar] [CrossRef]
- Dimitroulas, T.; Lambe, T.; Raphael, J.H.; Kitas, G.D.; Duarte, R.V. Biologic Drugs as Analgesics for the Management of Low Back Pain and Sciatica. Pain Med. 2019, 20, 1678–1686. [Google Scholar] [CrossRef]
- Williams, N.H.; Lewis, R.; Din, N.U.; Matar, H.E.; Fitzsimmons, D.; Phillips, C.J.; Sutton, A.; Burton, K.; Hendry, M.; Nafees, S.; et al. A Systematic Review and Meta-Analysis of Biological Treatments Targeting Tumour Necrosis Factor α for Sciatica. Eur. Spine J. 2013, 22, 1921–1935. [Google Scholar] [CrossRef]
- Wang, Y.F.; Chen, P.Y.; Chang, W.; Zhu, F.Q.; Xu, L.L.; Wang, S.L.; Chang, L.Y.; Luo, J.; Liu, G.J. Clinical Significance of Tumor Necrosis Factor-α Inhibitors in the Treatment of Sciatica: A Systematic Review and Meta-Analysis. PLoS ONE 2014, 9, e103147. [Google Scholar] [CrossRef] [PubMed]
- Leite, V.F.; Buehler, A.M.; El Abd, O.; Benyamin, R.M.; Pimentel, D.C.; Chen, J.; Hsing, W.T.; Mazloomdoost, D.; Amadera, J.E.D. Anti-Nerve Growth Factor in the Treatment of Low Back Pain and Radiculopathy: A Systematic Review and a Meta-Analysis. Pain Physician 2014, 17, E45–E60. [Google Scholar]
- Markman, J.D.; Bolash, R.B.; McAlindon, T.E.; Kivitz, A.J.; Pombo-Suarez, M.; Ohtori, S.; Roemer, F.W.; Li, D.J.; Viktrup, L.; Bramson, C.; et al. Tanezumab for Chronic Low Back Pain: A Randomized, Double-Blind, Placebo- and Active-Controlled, Phase 3 Study of Efficacy and Safety. Pain 2020, 161, 2068–2078. [Google Scholar] [CrossRef]
- Kivitz, A.J.; Gimbel, J.S.; Bramson, C.; Nemeth, M.A.; Keller, D.S.; Brown, M.T.; West, C.R.; Verburg, K.M. Efficacy and Safety of Tanezumab versus Naproxen in the Treatment of Chronic Low Back Pain. Pain 2013, 154, 1009–1021. [Google Scholar] [CrossRef]
- Gimbel, J.S.; Kivitz, A.J.; Bramson, C.; Nemeth, M.A.; Keller, D.S.; Brown, M.T.; West, C.R.; Verburg, K.M. Long-Term Safety and Effectiveness of Tanezumab as Treatment for Chronic Low Back Pain. Pain 2014, 155, 1793–1801. [Google Scholar] [CrossRef]
- Montague, K.; Malcangio, M. The Therapeutic Potential of Monocyte/Macrophage Manipulation in the Treatment of Chemotherapy-Induced Painful Neuropathy. Front. Mol. Neurosci. 2017, 10, 397. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.T.; Dauch, J.R.; Hayes, J.M.; Yanik, B.M.; Feldman, E.L. Nerve Growth Factor/P38 Signaling Increases Intraepidermal Nerve Fiber Densities in Painful Neuropathy of Type 2 Diabetes. Neurobiol. Dis. 2012, 45, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Mathews, J.A.; Krishnamoorthy, N.; Kasahara, D.I.; Hutchinson, J.; Cho, Y.; Brand, J.D.; Williams, A.S.; Wurmbrand, A.P.; Ribeiro, L.; Cuttitta, F.; et al. Augmented Responses to Ozone in Obese Mice Require IL-17A and Gastrin-Releasing Peptide. Am. J. Respir. Cell Mol. Biol. 2018, 58, 341–351. [Google Scholar] [CrossRef] [PubMed]
- Banach, M.; Juranek, J.K.; Zygulska, A.L. Chemotherapy-Induced Neuropathies-a Growing Problem for Patients and Health Care Providers. Brain Behav. 2017, 7, e00558. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.-Y.; Mi, W.-L.; Wu, G.-C.; Wang, Y.-Q.; Mao-Ying, Q.-L. Prevention and Treatment for Chemotherapy-Induced Peripheral Neuropathy: Therapies Based on CIPN Mechanisms. Curr. Neuropharmacol. 2019, 17, 184–196. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, L.A.; Duggett, N.A.; Pitcher, A.L.; Flatters, S.J.L. Evoked and Ongoing Pain-Like Behaviours in a Rat Model of Paclitaxel-Induced Peripheral Neuropathy. Pain Res. Manag. 2018, 2018, 8217613. [Google Scholar] [CrossRef] [PubMed]
- Kiguchi, N.; Kobayashi, Y.; Maeda, T.; Fukazawa, Y.; Tohya, K.; Kimura, M.; Kishioka, S. Epigenetic Augmentation of the Macrophage Inflammatory Protein 2/C-X-C Chemokine Receptor Type 2 Axis through Histone H3 Acetylation in Injured Peripheral Nerves Elicits Neuropathic Pain. J. Pharmacol. Exp. Ther. 2012, 340, 577–587. [Google Scholar] [CrossRef] [PubMed]
- Wild, K.D.; Bian, D.; Zhu, D.; Davis, J.; Bannon, A.W.; Zhang, T.J.; Louis, J.-C. Antibodies to Nerve Growth Factor Reverse Established Tactile Allodynia in Rodent Models of Neuropathic Pain without Tolerance. J. Pharmacol. Exp. Ther. 2007, 322, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Gwak, Y.S.; Nam, T.S.; Paik, K.S.; Hulsebosch, C.E.; Leem, J.W. Attenuation of Mechanical Hyperalgesia Following Spinal Cord Injury by Administration of Antibodies to Nerve Growth Factor in the Rat. Neurosci. Lett. 2003, 336, 117–120. [Google Scholar] [CrossRef]
- Pfizer. A Phase II Randomized, Double-Blind, Placebo-Controlled, Multicenter, Parallel Group, Proof of Concept Study of the Analgesic Effects of rn624 in Adult Patients with Post-Herpetic Neuralgia. 2021. Available online: https://clinicaltrials.gov/ct2/show/NCT00568321 (accessed on 15 July 2021).
- Bramson, C.; Herrmann, D.N.; Carey, W.; Keller, D.; Brown, M.T.; West, C.R.; Verburg, K.M.; Dyck, P.J. Exploring the Role of Tanezumab as a Novel Treatment for the Relief of Neuropathic Pain. Pain Med. 2015, 16, 1163–1176. [Google Scholar] [CrossRef]
- NCIC Clinical Trials Group. A Multi-Centre Phase II Trial Investigating the Efficacy and Tolerability of Bortezomib Added to Cyclophosphamide, Vincristine, Prednisone, and Rituximab (BCVP-R) for Patients with Advanced Stage Follicular Non-Hodgkin’s Lymphoma Requiring Systemic First-Line Treatment. 2012. Available online: https://clinicaltrials.gov/ct2/show/NCT00428142 (accessed on 15 July 2021).
- Northwestern University. A Phase I/II Trial of Combined Weekly Bortezomib (VELCADE®) and Y-90-Ibritumomab Tiuxetan (Zevalin) in Patients with Relapsed or Refractory Follicular Lymphoma and Transformed Non-Hodgkin’s Lymphoma. 2019. Available online: https://clinicaltrials.gov/ct2/show/NCT00372905 (accessed on 15 July 2021).
- KU. Leuven Anti TNFa Treatment for Deep Endometriosis Associated Pain: A Randomised Placebo Controlled Trial. 2008. Available online: https://clinicaltrials.gov/ct2/show/NCT00604864 (accessed on 16 July 2021).
- Koninckx, P.R.; Craessaerts, M.; Timmerman, D.; Cornillie, F.; Kennedy, S. Anti-TNF-α Treatment for Deep Endometriosis-Associated Pain: A Randomized Placebo-Controlled Trial. Hum. Reprod. 2008, 23, 2017–2023. [Google Scholar] [CrossRef]
- Teva Branded Pharmaceutical Products R & D, Inc. A Multicenter, Randomized, Double-Blind, Placebo-Controlled, Proof of Concept Study of the Efficacy and Safety of Fremanezumab for Treatment of Patients with Fibromyalgia. 2021. Available online: https://clinicaltrials.gov/ct2/show/NCT03965091 (accessed on 16 July 2021).
- Jimenez-Andrade, J.M.; Ghilardi, J.R.; Castañeda-Corral, G.; Kuskowski, M.A.; Mantyh, P.W. Preventive or Late Administration of Anti-NGF Therapy Attenuates Tumor-Induced Nerve Sprouting, Neuroma Formation, and Cancer Pain. Pain 2011, 152, 2564–2574. [Google Scholar] [CrossRef]
- Currie, G.L.; Delaney, A.; Bennett, M.I.; Dickenson, A.H.; Egan, K.J.; Vesterinen, H.M.; Sena, E.S.; Macleod, M.R.; Colvin, L.A.; Fallon, M.T. Animal Models of Bone Cancer Pain: Systematic Review and Meta-Analyses. Pain 2013, 154, 917–926. [Google Scholar] [CrossRef]
- Mantyh, P.W.; Koltzenburg, M.; Mendell, L.M.; Tive, L.; Shelton, D.L. Antagonism of Nerve Growth Factor-TrkA Signaling and the Relief of Pain. Anesthesiology 2011, 115, 189–204. [Google Scholar] [CrossRef] [PubMed]
- Sevcik, M.A.; Ghilardi, J.R.; Peters, C.M.; Lindsay, T.H.; Halvorson, K.G.; Jonas, B.M.; Kubota, K.; Kuskowski, M.A.; Boustany, L.; Shelton, D.L.; et al. Anti-NGF Therapy Profoundly Reduces Bone Cancer Pain and the Accompanying Increase in Markers of Peripheral and Central Sensitization. Pain 2005, 115, 128–141. [Google Scholar] [CrossRef]
- Majuta, L.A.; Mitchell, S.A.T.; Kuskowski, M.A.; Mantyh, P.W. Anti-Nerve Growth Factor Does Not Change Physical Activity in Normal Young or Aging Mice but Does Increase Activity in Mice with Skeletal Pain. Pain 2018, 159, 2285–2295. [Google Scholar] [CrossRef]
- Almholt, K.; Hebsgaard, J.B.; Nansen, A.; Andersson, C.; Pass, J.; Rønø, B.; Thygesen, P.; Pelzer, H.; Loftager, M.; Lund, I.K.; et al. Antibody-Mediated Neutralization of UPA Proteolytic Function Reduces Disease Progression in Mouse Arthritis Models. J. Immunol. 2018, 200, 957–965. [Google Scholar] [CrossRef] [PubMed]
- Hu, R.; Song, Y.-F.; Yang, Z.-Y.; Zhang, C.; Tan, B. Clinical Outcomes of Tanezumab with Different Dosages for Patient with Osteoarthritis: Network Meta-Analysis. Front. Pharmacol. 2021, 12, 614753. [Google Scholar] [CrossRef] [PubMed]
- Gjefsen, E.; Bråten, L.C.H.; Goll, G.L.; Wigemyr, M.; Bolstad, N.; Valberg, M.; Schistad, E.I.; Marchand, G.H.; Granviken, F.; Selmer, K.K.; et al. The Effect of Infliximab in Patients with Chronic Low Back Pain and Modic Changes (the BackToBasic Study): Study Protocol of a Randomized, Double Blind, Placebo-Controlled, Multicenter Trial. BMC Musculoskelet. Disord. 2020, 21, 698. [Google Scholar] [CrossRef] [PubMed]
- Tepper, S.J.; Diener, H.-C.; Ashina, M.; Brandes, J.L.; Friedman, D.I.; Reuter, U.; Cheng, S.; Nilsen, J.; Leonardi, D.K.; Lenz, R.A.; et al. Erenumab in Chronic Migraine with Medication Overuse: Subgroup Analysis of a Randomized Trial. Neurology 2019, 92, e2309–e2320. [Google Scholar] [CrossRef] [PubMed]
- Tepper, S.J.; Ashina, M.; Reuter, U.; Brandes, J.L.; Doležil, D.; Silberstein, S.D.; Winner, P.; Zhang, F.; Cheng, S.; Mikol, D.D. Long-Term Safety and Efficacy of Erenumab in Patients with Chronic Migraine: Results from a 52-Week, Open-Label Extension Study. Cephalalgia Int. J. Headache 2020, 40, 543–553. [Google Scholar] [CrossRef] [PubMed]
- Overeem, L.H.; Neeb, L.; Reuter, U. Erenumab for Episodic Migraine Prophylaxis. Expert Rev. Neurother. 2019, 19, 751–757. [Google Scholar] [CrossRef] [PubMed]
- Garland, S.G.; Smith, S.M.; Gums, J.G. Erenumab: A First-in-Class Monoclonal Antibody for Migraine Prevention. Ann. Pharmacother. 2019, 53, 933–939. [Google Scholar] [CrossRef]
- Ornello, R.; Tiseo, C.; Frattale, I.; Perrotta, G.; Marini, C.; Pistoia, F.; Sacco, S. The Appropriate Dosing of Erenumab for Migraine Prevention after Multiple Preventive Treatment Failures: A Critical Appraisal. J. Headache Pain 2019, 20, 99. [Google Scholar] [CrossRef]
- Ashina, M.; Cohen, J.M.; Gandhi, S.K.; Du, E. Reduction in the Severity and Duration of Headache Following Fremanezumab Treatment in Patients with Episodic and Chronic Migraine. Headache 2021, 61, 916–926. [Google Scholar] [CrossRef]
- Cohen, J.M.; Dodick, D.W.; Yang, R.; Newman, L.C.; Li, T.; Aycardi, E.; Bigal, M.E. Fremanezumab as Add-On Treatment for Patients Treated with Other Migraine Preventive Medicines. Headache 2017, 57, 1375–1384. [Google Scholar] [CrossRef]
- Halker Singh, R.B.; Aycardi, E.; Bigal, M.E.; Loupe, P.S.; McDonald, M.; Dodick, D.W. Sustained Reductions in Migraine Days, Moderate-to-Severe Headache Days and Days with Acute Medication Use for HFEM and CM Patients Taking Fremanezumab: Post-Hoc Analyses from Phase 2 Trials. Cephalalgia 2019, 39, 52–60. [Google Scholar] [CrossRef]
- Silberstein, S.D.; Rapoport, A.M.; Loupe, P.S.; Aycardi, E.; McDonald, M.; Yang, R.; Bigal, M.E. The Effect of Beginning Treatment with Fremanezumab on Headache and Associated Symptoms in the Randomized Phase 2 Study of High Frequency Episodic Migraine: Post-Hoc Analyses on the First 3 Weeks of Treatment. Headache 2019, 59, 383–393. [Google Scholar] [CrossRef]
- Silberstein, S.D.; Cohen, J.M.; Yang, R.; Gandhi, S.K.; Du, E.; Jann, A.E.; Marmura, M.J. Treatment Benefit among Migraine Patients Taking Fremanezumab: Results from a Post Hoc Responder Analysis of Two Placebo-Controlled Trials. J. Headache Pain 2021, 22, 2. [Google Scholar] [CrossRef]
- Martin, V.; Samaan, K.H.; Aurora, S.; Pearlman, E.M.; Zhou, C.; Li, X.; Pallay, R. Efficacy and Safety of Galcanezumab for the Preventive Treatment of Migraine: A Narrative Review. Adv. Ther. 2020, 37, 2034–2049. [Google Scholar] [CrossRef] [PubMed]
- Dodick, D.W.; Goadsby, P.J.; Spierings, E.L.H.; Scherer, J.C.; Sweeney, S.P.; Grayzel, D.S. Safety and Efficacy of LY2951742, a Monoclonal Antibody to Calcitonin Gene-Related Peptide, for the Prevention of Migraine: A Phase 2, Randomised, Double-Blind, Placebo-Controlled Study. Lancet Neurol. 2014, 13, 885–892. [Google Scholar] [CrossRef]
- Sanofi. A Randomized, Double-Blind, Placebo-Controlled, Multicenter, Two-Part, Dose Ranging and Confirmatory Study with an Operationally Seamless Design, Evaluating Efficacy and Safety of SAR153191 on Top of Methotrexate (MTX) in Patients with Active Rheumatoid Arthritis Who Are Inadequate Responders to MTX Therapy. 2017. Available online: https://www.clinicaltrials.gov/ct2/show/NCT01061736 (accessed on 15 July 2021).
- Strand, V.; Kosinski, M.; Chen, C.-I.; Joseph, G.; Rendas-Baum, R.; Graham, N.M.H.; van Hoogstraten, H.; Bayliss, M.; Fan, C.; Huizinga, T.; et al. Sarilumab plus Methotrexate Improves Patient-Reported Outcomes in Patients with Active Rheumatoid Arthritis and Inadequate Responses to Methotrexate: Results of a Phase III Trial. Arthritis Res. Ther. 2016, 18, 198. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann-La Roche. A Randomized, Double-Blind Study of Safety and Prevention of Structural Joint Damage During Treatment with Tocilizumab Versus Placebo, in Combination with Methotrexate, in Patients with Moderate to Severe Rheumatoid Arthritis. 2013. Available online: https://clinicaltrials.gov/ct2/show/NCT00106535 (accessed on 15 July 2021).
- Burmester, G.R.; Landewé, R.; Genovese, M.C.; Friedman, A.W.; Pfeifer, N.D.; Varothai, N.A.; Lacerda, A.P. Adalimumab Long-Term Safety: Infections, Vaccination Response and Pregnancy Outcomes in Patients with Rheumatoid Arthritis. Ann. Rheum. Dis. 2017, 76, 414–417. [Google Scholar] [CrossRef]
- Fautrel, B.; Kirkham, B.; Pope, J.E.; Takeuchi, T.; Gaich, C.; Quebe, A.; Zhu, B.; de la Torre, I.; De Leonardis, F.; Taylor, P.C. Effect of Baricitinib and Adalimumab in Reducing Pain and Improving Function in Patients with Rheumatoid Arthritis in Low Disease Activity: Exploratory Analyses from RA-BEAM. J. Clin. Med. 2019, 8, 1394. [Google Scholar] [CrossRef]
- Kremer, J.; Ritchlin, C.; Mendelsohn, A.; Baker, D.; Kim, L.; Xu, Z.; Han, J.; Taylor, P. Golimumab, a New Human Anti-Tumor Necrosis Factor Alpha Antibody, Administered Intravenously in Patients with Active Rheumatoid Arthritis: Forty-Eight-Week Efficacy and Safety Results of a Phase III Randomized, Double-Blind, Placebo-Controlled Study. Arthritis Rheum. 2010, 62, 917–928. [Google Scholar] [CrossRef]
- Li, Z.; Zhang, F.; Kay, J.; Fei, K.; Han, C.; Zhuang, Y.; Wu, Z.; Hsia, E.C. Efficacy and Safety Results from a Phase 3, Randomized, Placebo-Controlled Trial of Subcutaneous Golimumab in Chinese Patients with Active Rheumatoid Arthritis despite Methotrexate Therapy. Int. J. Rheum. Dis. 2016, 19, 1143–1156. [Google Scholar] [CrossRef]
- Ruiz Garcia, V.; Burls, A.; Cabello, J.B.; Vela Casasempere, P.; Bort-Marti, S.; Bernal, J.A. Certolizumab Pegol (CDP870) for Rheumatoid Arthritis in Adults. Cochrane Database Syst. Rev. 2017, 2017, CD007649. [Google Scholar] [CrossRef]
- Bessette, L.; Haraoui, B.; Chow, A.; Fortin, I.; Dixit, S.; Khraishi, M.; Haaland, D.; Elmoufti, S.; Staelens, F.; Bogatyreva, I.; et al. Effectiveness and Safety of Certolizumab Pegol in Rheumatoid Arthritis Patients in Canadian Practice: 2-Year Results from the Observational FαsT-CAN Study. Ther. Adv. Musculoskelet. Dis. 2019, 11, 1759720. [Google Scholar] [CrossRef]
- Chen, W.; Li, Z.; Wang, Z.; Gao, H.; Ding, J.; He, Z. Intraarticular Injection of Infliximab-Loaded Thermosensitive Hydrogel Alleviates Pain and Protects Cartilage in Rheumatoid Arthritis. J. Pain Res. 2020, 13, 3315–3329. [Google Scholar] [CrossRef] [PubMed]
- Thorne, C.; Bensen, W.G.; Choquette, D.; Chow, A.; Khraishi, M.; Atkins, C.J.; Kelsall, J.T.; Lehman, A.J.; Shawi, M.; Khalil, H.; et al. Effectiveness and Safety of Infliximab in Rheumatoid Arthritis: Analysis from a Canadian Multicenter Prospective Observational Registry. Arthritis Care Res. 2014, 66, 1142–1151. [Google Scholar] [CrossRef] [PubMed]
- Rigby, W.; Ferraccioli, G.; Greenwald, M.; Zazueta-Montiel, B.; Fleischmann, R.; Wassenberg, S.; Ogale, S.; Armstrong, G.; Jahreis, A.; Burke, L.; et al. Effect of Rituximab on Physical Function and Quality of Life in Patients with Rheumatoid Arthritis Previously Untreated with Methotrexate. Arthritis Care Res. 2011, 63, 711–720. [Google Scholar] [CrossRef] [PubMed]


| Monoclonal Antibodies | Classic Drugs |
|---|---|
| Very high selectivity (few side effects) | Good selectivity (dose-related) |
| Parenteral administration | Multiple routes of administration |
| PK: elimination by either excretion or catabolism | PK: classic metabolism and excretion (liver, kidney, etc.) |
| PK and PD interactions almost excluded | PK and PD interactions |
| Prolonged half-life | Shorter half-life |
| Produced by genetic engineering | Chemical synthesis or natural purification |
| Do not cross BBB | Can cross BBB |
| Can produce immunogenicity | Poorly immunogenic |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Robles, E.M.; Girón, R.; Paniagua, N.; Rodríguez-Rivera, C.; Pascual, D.; Goicoechea, C. Monoclonal Antibodies for Chronic Pain Treatment: Present and Future. Int. J. Mol. Sci. 2021, 22, 10325. https://doi.org/10.3390/ijms221910325
Sánchez-Robles EM, Girón R, Paniagua N, Rodríguez-Rivera C, Pascual D, Goicoechea C. Monoclonal Antibodies for Chronic Pain Treatment: Present and Future. International Journal of Molecular Sciences. 2021; 22(19):10325. https://doi.org/10.3390/ijms221910325
Chicago/Turabian StyleSánchez-Robles, Eva M., Rocío Girón, Nancy Paniagua, Carmen Rodríguez-Rivera, David Pascual, and Carlos Goicoechea. 2021. "Monoclonal Antibodies for Chronic Pain Treatment: Present and Future" International Journal of Molecular Sciences 22, no. 19: 10325. https://doi.org/10.3390/ijms221910325
APA StyleSánchez-Robles, E. M., Girón, R., Paniagua, N., Rodríguez-Rivera, C., Pascual, D., & Goicoechea, C. (2021). Monoclonal Antibodies for Chronic Pain Treatment: Present and Future. International Journal of Molecular Sciences, 22(19), 10325. https://doi.org/10.3390/ijms221910325