
Partial Decellularized Scaffold Combined with Autologous Nasal Epithelial Cell Sheet for Tracheal Tissue Engineering

 ,
,  ,
,  , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
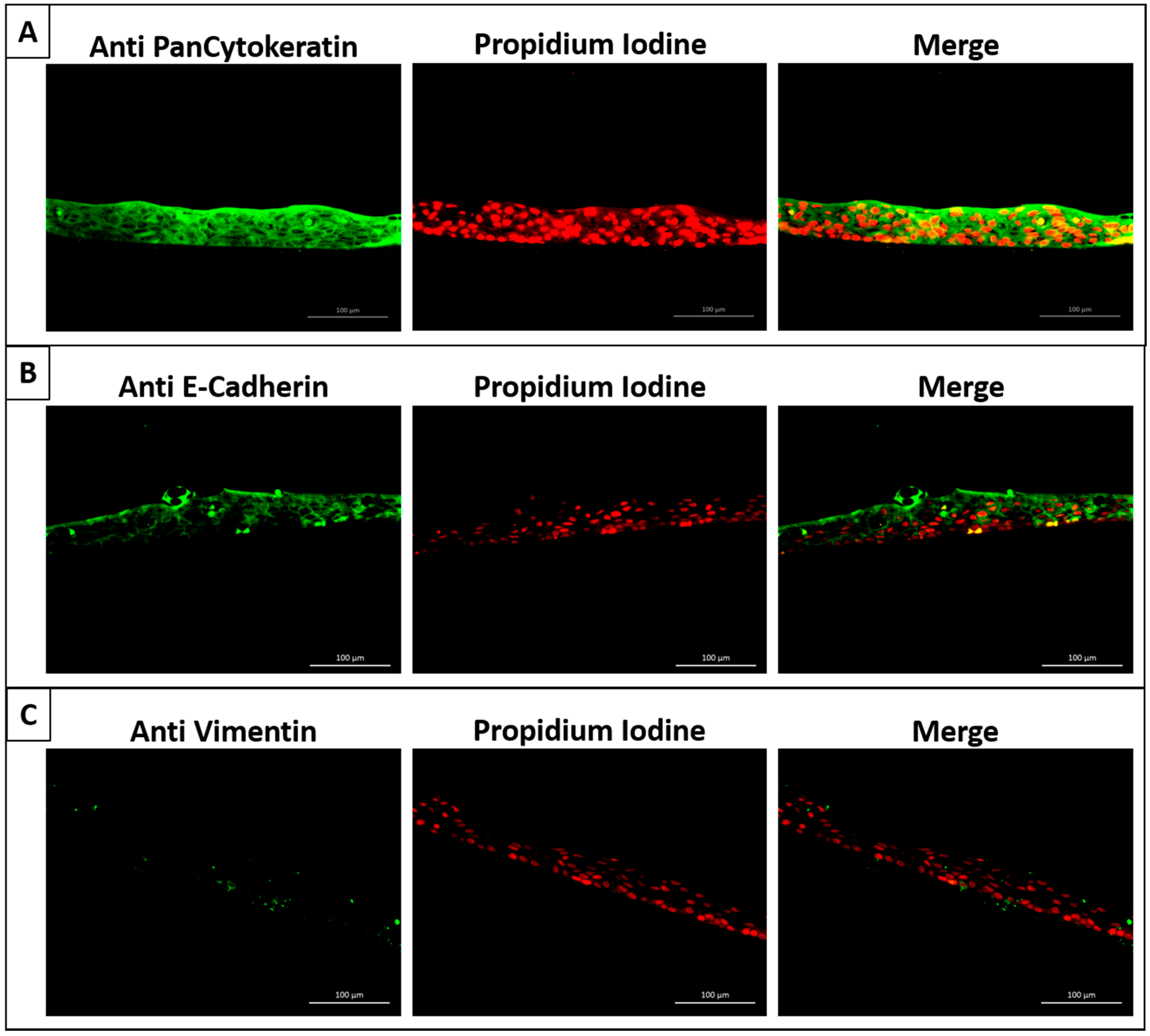
2.1. Successful Generation of Autologous Nasal Epithelial Cell Sheets Using Our Novel Cell Sheet Method
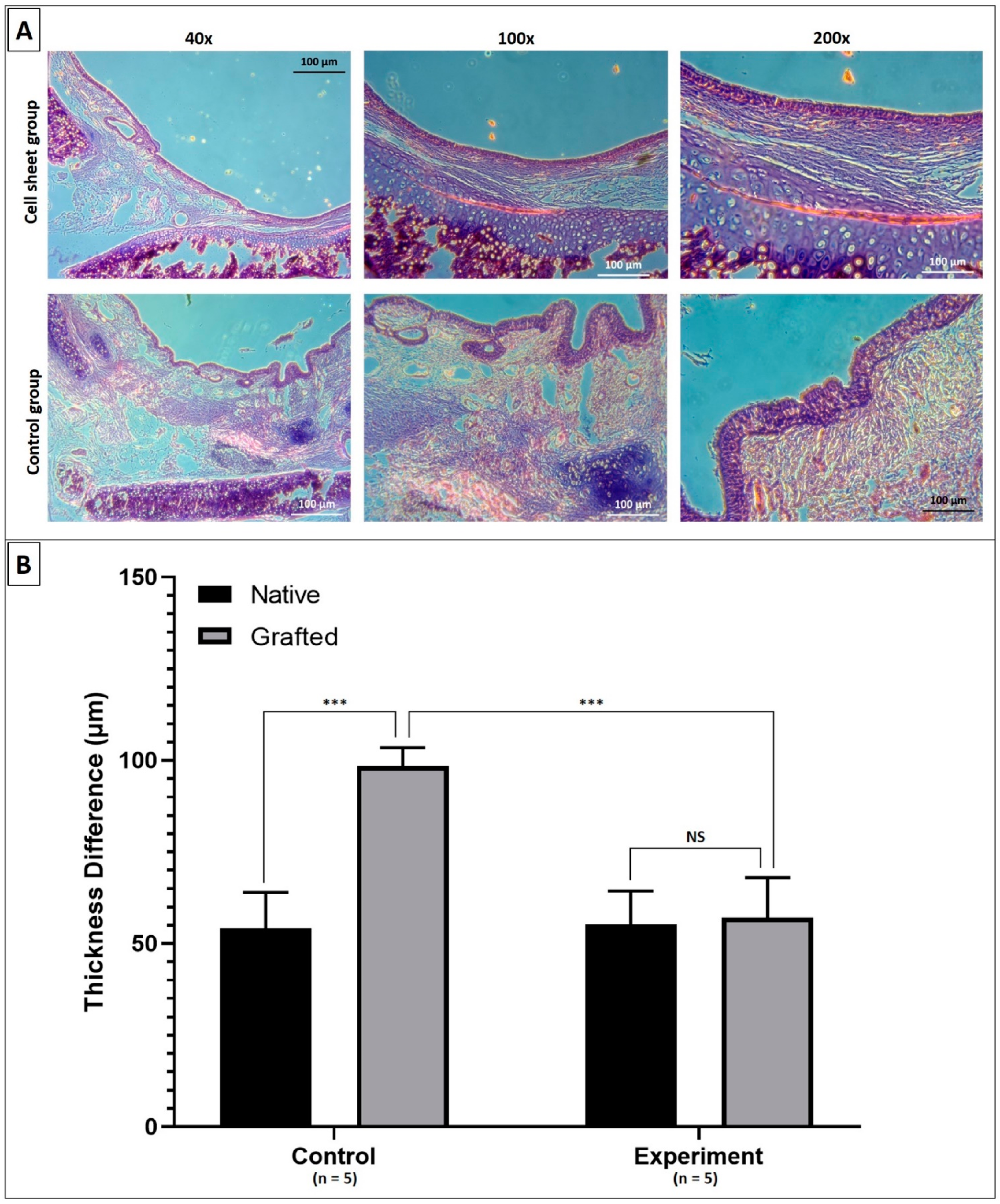
2.2. Results of Surgical Transplantations in Rabbit Groups Using Decellularized Tracheal Grafts with Cell Sheets Applied onto the Luminal Surface
3. Discussion
4. Materials and Methods
4.1. Fabrication of Nasal Epithelial Cell Sheets and Pretransplantation Evaluations
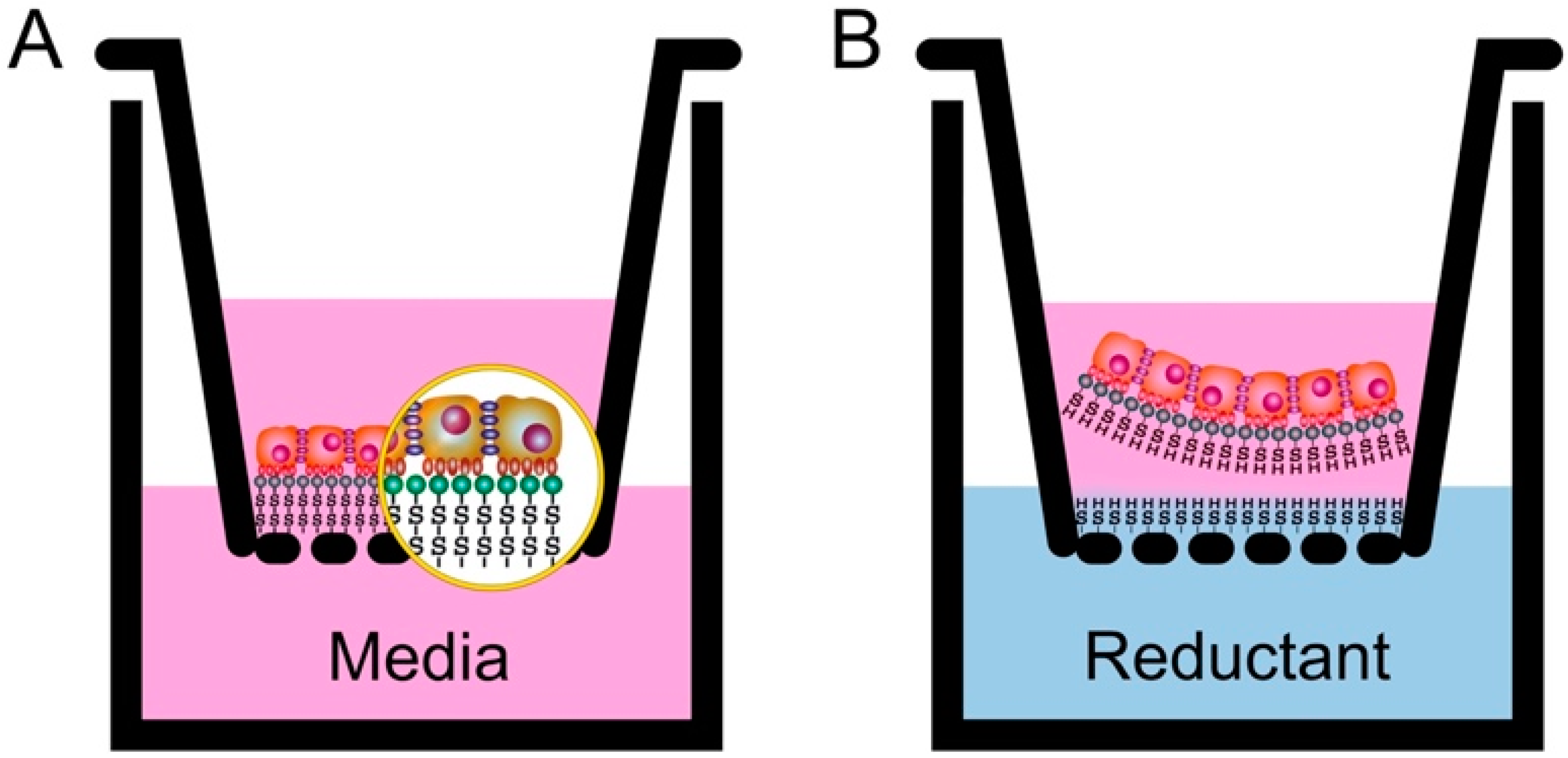
4.1.1. Fabrication of Nasal Epithelial Cell Sheets
Preparation of Our Cell Culture Inserts
Culture of Rabbit Nasal Epithelial Cell Sheets
4.1.2. Pretransplantation Evaluations of the Nasal Epithelial Cell Sheets
Vital Staining Assay
Histological and Immunohistochemical Analyses
4.2. Autograft Tracheal Patch Transplantation
4.2.1. Partial Decellularization of the Rabbit Tracheal Patch
4.2.2. Surgical Transplantation of Autologous Nasal Epithelial Cell Sheets in Autograft Tracheal Patch Transplantation
4.3. Endoscopic and Histological Analyses after Transplantation
4.4. Statistical Analysis
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Etienne, H.; Fabre, D.; Caro, A.G.; Kolb, F.; Mussot, S.; Mercier, O.; Mitilian, D.; Stephan, F.; Fadel, E.; Dartevelle, P. Tracheal replacement. Eur. Respir. J. 2018, 51, 1702211. [Google Scholar] [CrossRef] [PubMed]
- Udelsman, B.; Mathisen, D.J.; Ott, H.C. A reassessment of tracheal substitutes—A systematic review. Ann. Cardiothorac. Surg. 2018, 7, 175–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Law, J.X.; Liau, L.L.; Aminuddin, B.S.; Ruszymah, B.H.I. Tissue-engineered trachea: A review. Int. J. Pediatr. Otorhinolaryngol. 2016, 91, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Rajab, T.K.; O’Malley, T.J.; Tchantchaleishvili, V. Decellularized scaffolds for tissue engineering: Current status and future perspective. Artif. Organs 2020, 44, 1031–1043. [Google Scholar] [CrossRef] [PubMed]
- Molins, L. Patient follow-up after tissue-engineered airway transplantation. Lancet 2019, 393, 1099. [Google Scholar] [CrossRef] [Green Version]
- Hung, S.H.; Su, C.H.; Lin, S.E.; Tseng, H. Preliminary experiences in trachea scaffold tissue engineering with segmental organ decellularization. Laryngoscope 2016, 126, 2520–2527. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Dharmadhikari, S.; Shontz, K.M.; Tan, Z.H.; Spector, B.M.; Stephens, B.; Bergman, M.; Manning, A.; Zhao, K.; Reynolds, S.D.; et al. Regeneration of partially decellularized tracheal scaffolds in a mouse model of orthotopic tracheal replacement. J. Tissue Eng. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Aoki, F.G.; Varma, R.; Marin-Araujo, A.E.; Lee, H.; Soleas, J.P.; Li, A.H.; Soon, K.; Romero, D.; Moriya, H.T.; Haykal, S.; et al. De-epithelialization of porcine tracheal allografts as an approach for tracheal tissue engineering. Sci. Rep. 2019, 9, 12034. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhang, H.; Sun, Y.; Liu, P.; Li, S.; Cui, P. Mechanical properties of de-epithelialized tracheal allografts. J. Thorac. Dis. 2021, 13, 1066–1074. [Google Scholar] [CrossRef] [PubMed]
- Dang, L.H.; Tseng, Y.; Tseng, H.; Hung, S.H. Partial decellularization for segmental tracheal scaffold tissue engineering: A preliminary study in rabbits. Biomolecules 2021, 11, 866. [Google Scholar] [CrossRef] [PubMed]
- Kanzaki, M.; Yamato, M.; Hatakeyama, H.; Kohno, C.; Yang, J.; Umemoto, T.; Kikuchi, A.; Okano, T.; Onuki, T. Tissue engineered epithelial cell sheets for the creation of a bioartificial trachea. Tissue Eng. 2006, 12, 1275–1283. [Google Scholar] [CrossRef] [PubMed]
- Maughan, E.F.; Hynds, R.E.; Proctor, T.J.; Janes, S.M.; Elliott, M.; Birchall, M.A.; Lowdell, M.W.; De Coppi, P. Autologous Cell Seeding in Tracheal Tissue Engineering. Curr. Stem Cell Rep. 2017, 3, 279–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brewington, J.J.; Filbrandt, E.T.; LaRosa, F.J.; Moncivaiz, J.D.; Ostmann, A.J.; Strecker, L.M.; Clancy, J.P. Brushed nasal epithelial cells are a surrogate for bronchial epithelial CFTR studies. JCI Insight 2018, 3, e99385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDougall, C.M.; Blaylock, M.G.; Douglas, J.G.; Brooker, R.J.; Helms, P.J.; Walsh, G.M. Nasal epithelial cells as surrogates for bronchial epithelial cells in airway inflammation studies. Am. J. Respir. Cell Mol. Biol. 2008, 39, 560–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koo, J.P.; Kim, C.H.; Lee, J.G.; Kim, K.S.; Yoon, J.H. Airway reconstruction with carrier-free cell sheets composed of autologous nasal squamous epithelium. Laryngoscope 2007, 117, 1750–1755. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, N.J.; Kanani, M.; Roebuck, D.J.; Hewitt, R.J.; Cetto, R.; Culme-Seymour, E.J.; Toll, E.; Bates, A.J.; Comerford, A.P.; McLaren, C.A.; et al. Tissue-Engineered Tracheal Replacement in a Child: A 4-Year Follow-Up Study. Am. J. Transplant. 2015, 15, 2750–2757. [Google Scholar] [CrossRef] [PubMed]
- Sueyoshi, S.; Chitose, S.I.; Sato, K.; Fukahori, M.; Kurita, T.; Umeno, H. Stable Tracheal Regeneration Using Organotypically Cultured Tissue Composed of Autologous Chondrocytes and Epithelial Cells in Beagles. Ann. Otol. Rhinol. Laryngol. 2019, 128, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Kim, I.G.; Park, S.A.; Lee, S.H.; Choi, J.S.; Cho, H.; Lee, S.J.; Kwon, Y.W.; Kwon, S.K. Transplantation of a 3D-printed tracheal graft combined with iPS cell-derived MSCs and chondrocytes. Sci. Rep. 2020, 10, 4326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanai, N.; Kobayashi, S.; Yamato, M.; Ohki, T.; Yamamoto, M.; Okano, T. 360 Development of Novel Endoscopic Delivery Devices for Cell Sheets Transplantation. Gastrointest. Endosc. 2013, 77, AB147. [Google Scholar] [CrossRef]
- Tseng, H.; Tsai, J.-K.; Ou, K.-L.; Chen, P.-N. Supports for Cell Culture and Cell Sheet Detachment and Methods for Cell, Sheet Detachment. U.S. Patent 9,546,349, 17 January 2017. [Google Scholar]
- Yamamoto, K.; Hama, T.; Yamato, M.; Uchimizu, H.; Sugiyama, H.; Takagi, R.; Yaguchi, Y.; Okano, T.; Kojima, H. The effect of transplantation of nasal mucosal epithelial cell sheets after middle ear surgery in a rabbit model. Biomaterials 2015, 42, 87–93. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dang, L.H.; Hung, S.-H.; Tseng, Y.; Quang, L.X.; Le, N.T.N.; Fang, C.-L.; Tseng, H. Partial Decellularized Scaffold Combined with Autologous Nasal Epithelial Cell Sheet for Tracheal Tissue Engineering. Int. J. Mol. Sci. 2021, 22, 10322. https://doi.org/10.3390/ijms221910322
Dang LH, Hung S-H, Tseng Y, Quang LX, Le NTN, Fang C-L, Tseng H. Partial Decellularized Scaffold Combined with Autologous Nasal Epithelial Cell Sheet for Tracheal Tissue Engineering. International Journal of Molecular Sciences. 2021; 22(19):10322. https://doi.org/10.3390/ijms221910322
Chicago/Turabian StyleDang, Luong Huu, Shih-Han Hung, Yuan Tseng, Ly Xuan Quang, Nhi Thao Ngoc Le, Chia-Lang Fang, and How Tseng. 2021. "Partial Decellularized Scaffold Combined with Autologous Nasal Epithelial Cell Sheet for Tracheal Tissue Engineering" International Journal of Molecular Sciences 22, no. 19: 10322. https://doi.org/10.3390/ijms221910322
APA StyleDang, L. H., Hung, S.-H., Tseng, Y., Quang, L. X., Le, N. T. N., Fang, C.-L., & Tseng, H. (2021). Partial Decellularized Scaffold Combined with Autologous Nasal Epithelial Cell Sheet for Tracheal Tissue Engineering. International Journal of Molecular Sciences, 22(19), 10322. https://doi.org/10.3390/ijms221910322