
Protective Effect of Water-Soluble C60 Fullerene Nanoparticles on the Ischemia-Reperfusion Injury of the Muscle Soleus in Rats


 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results and Discussion
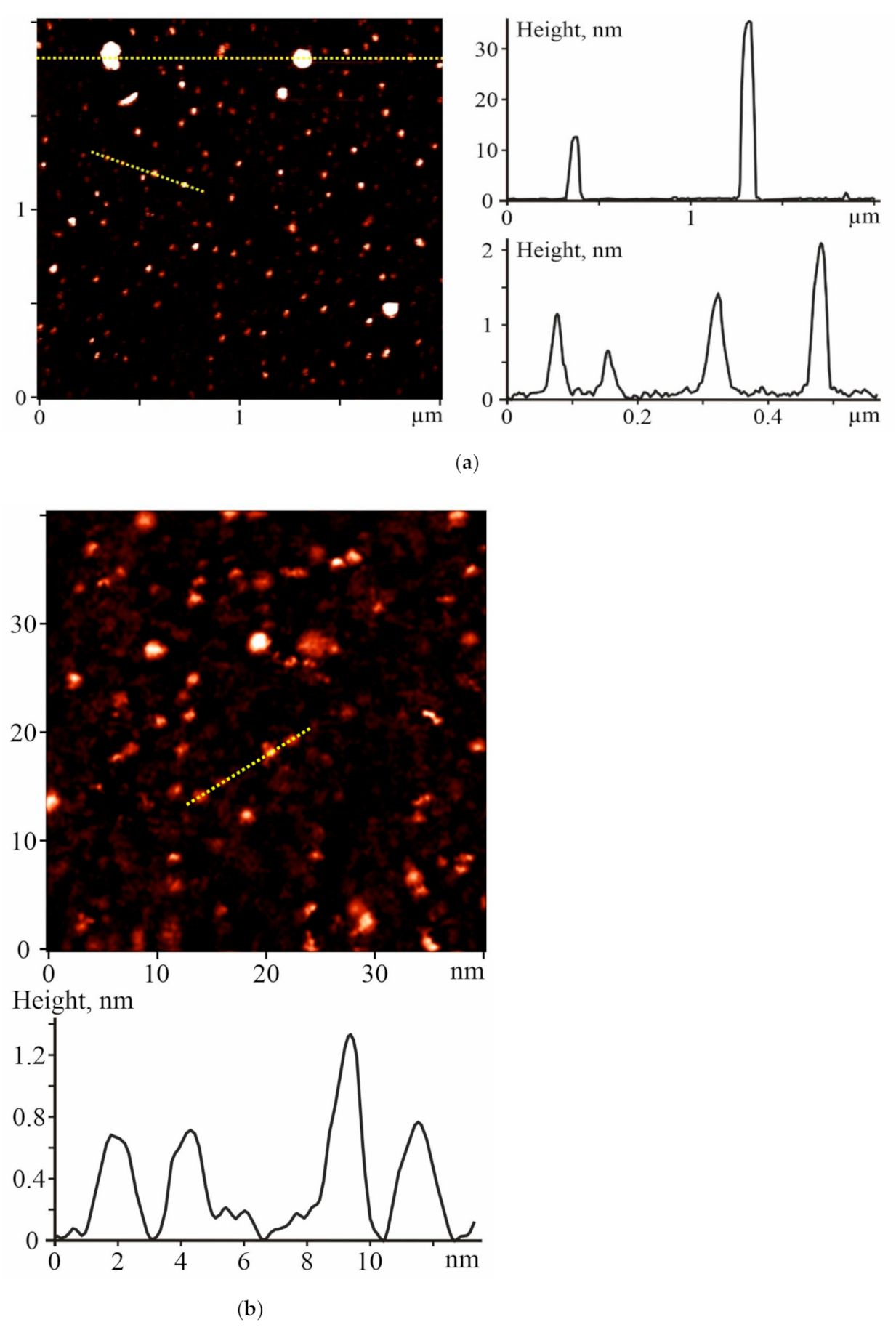
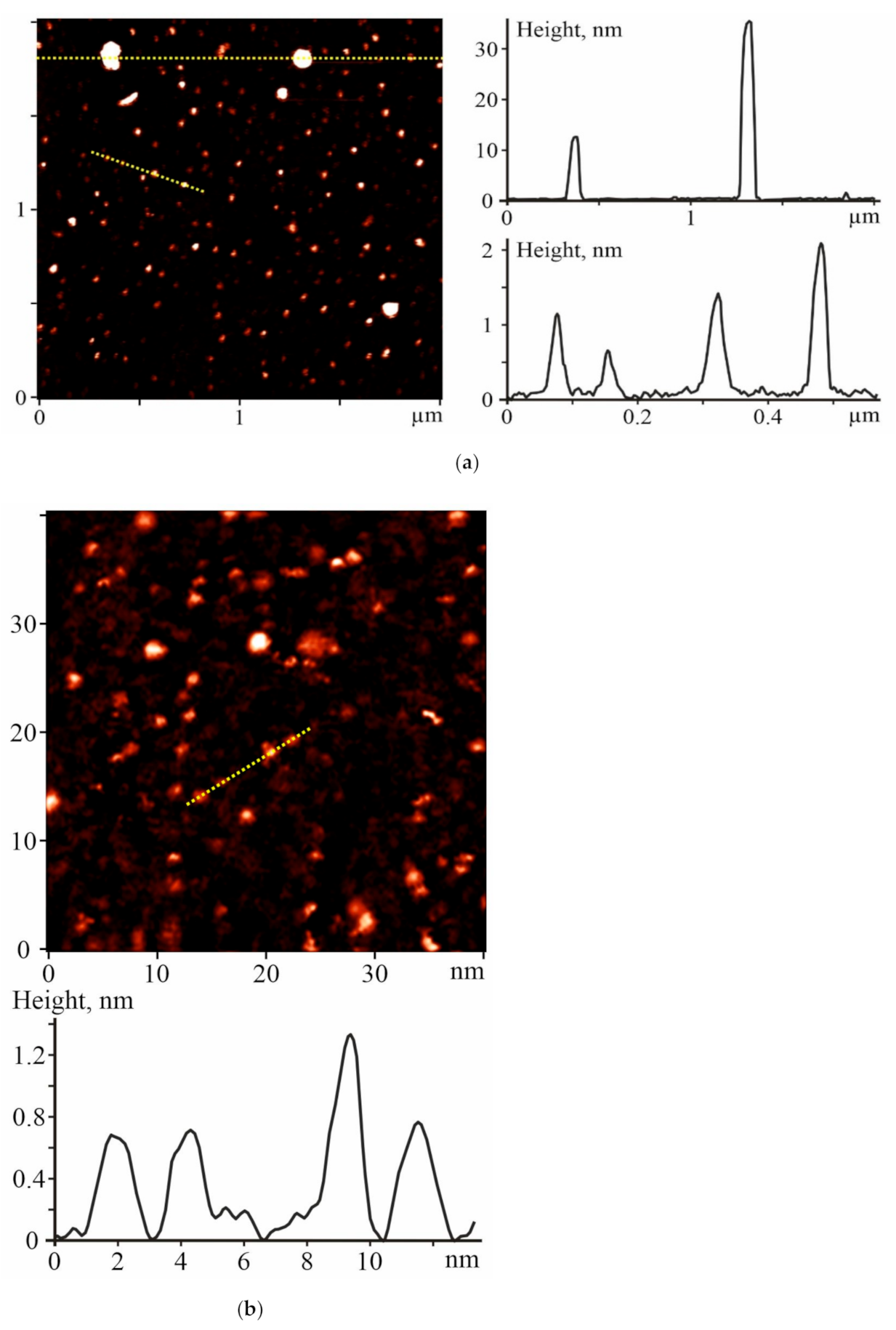
2.1. Characterization of C60FAS
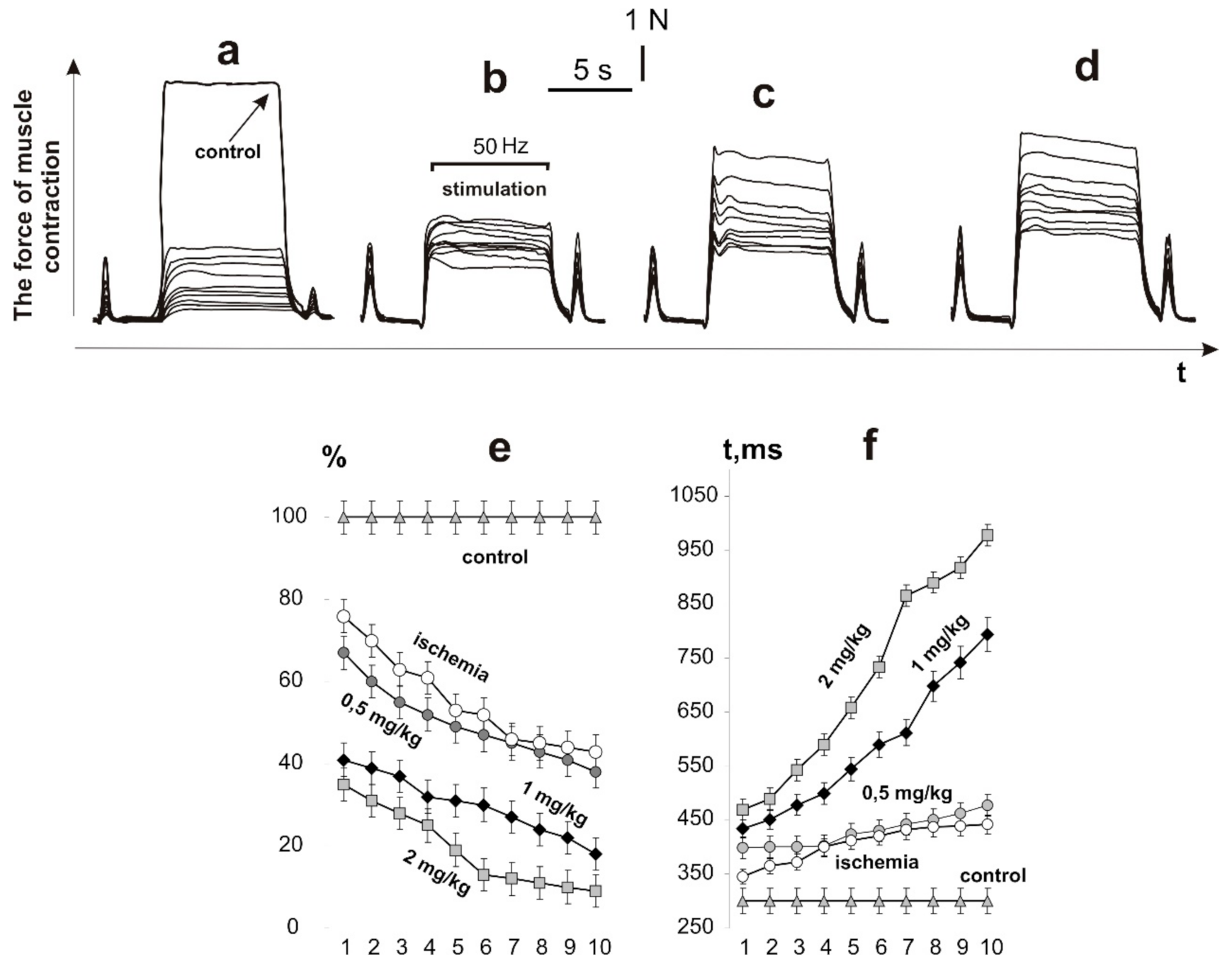
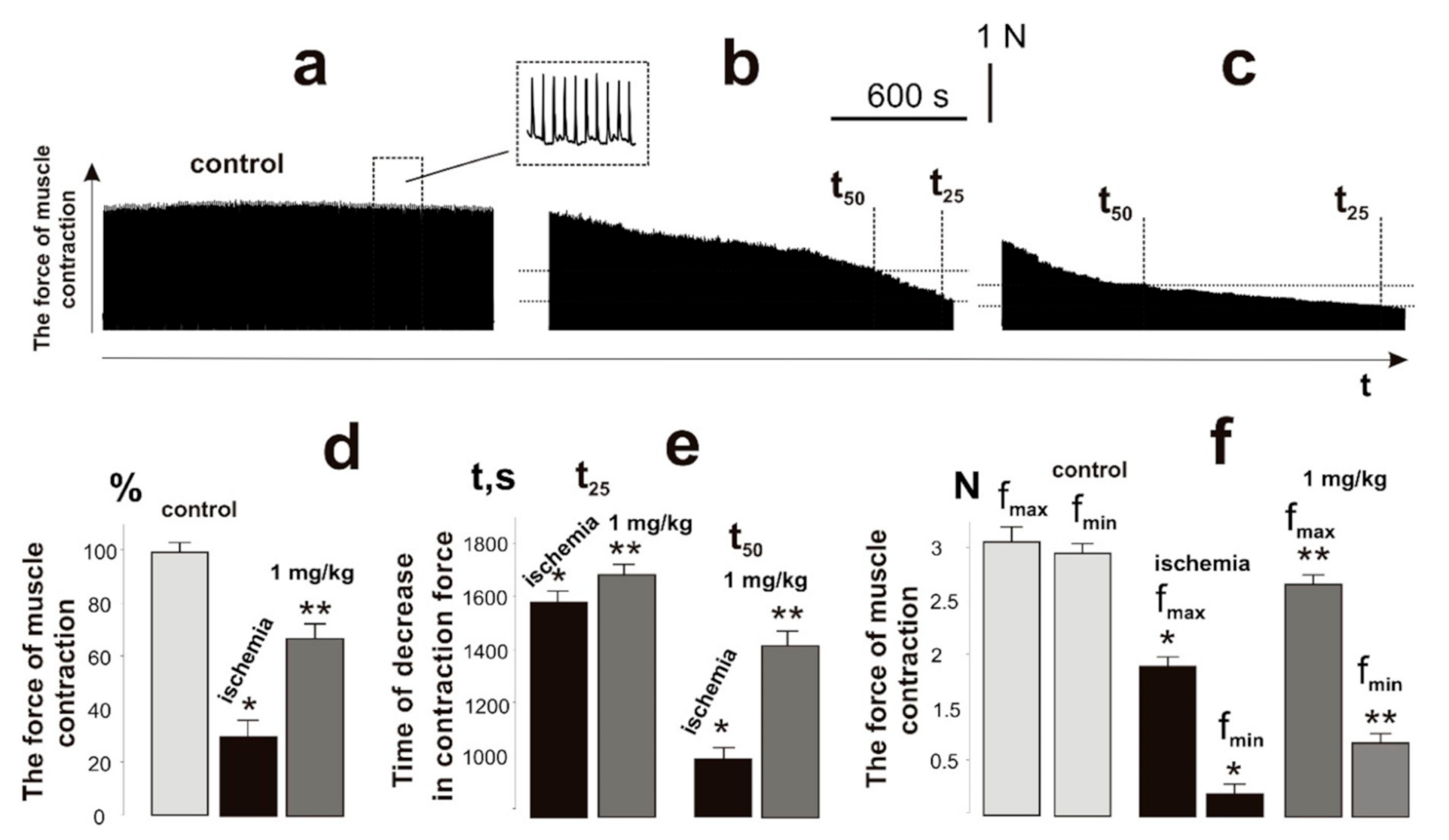
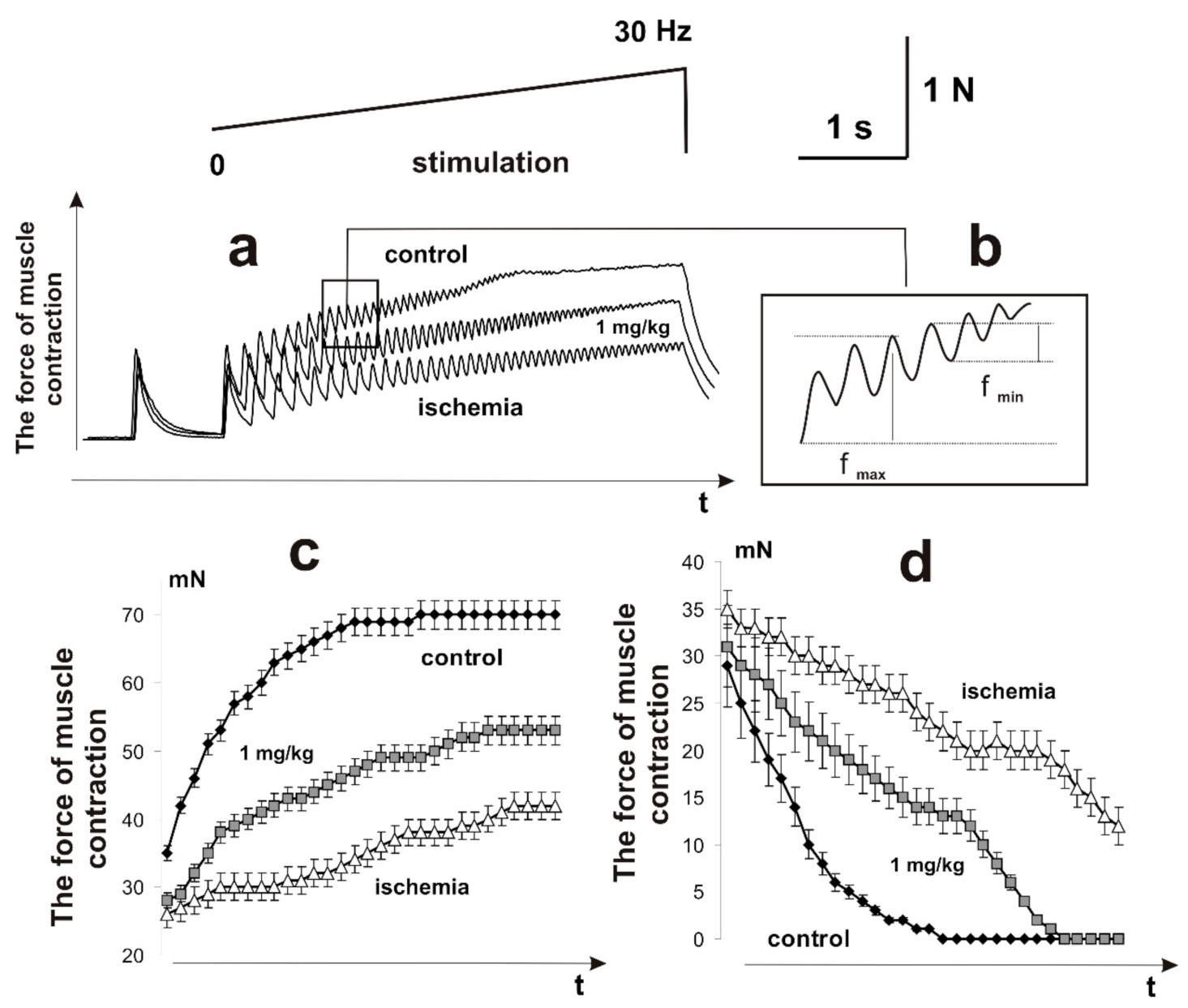
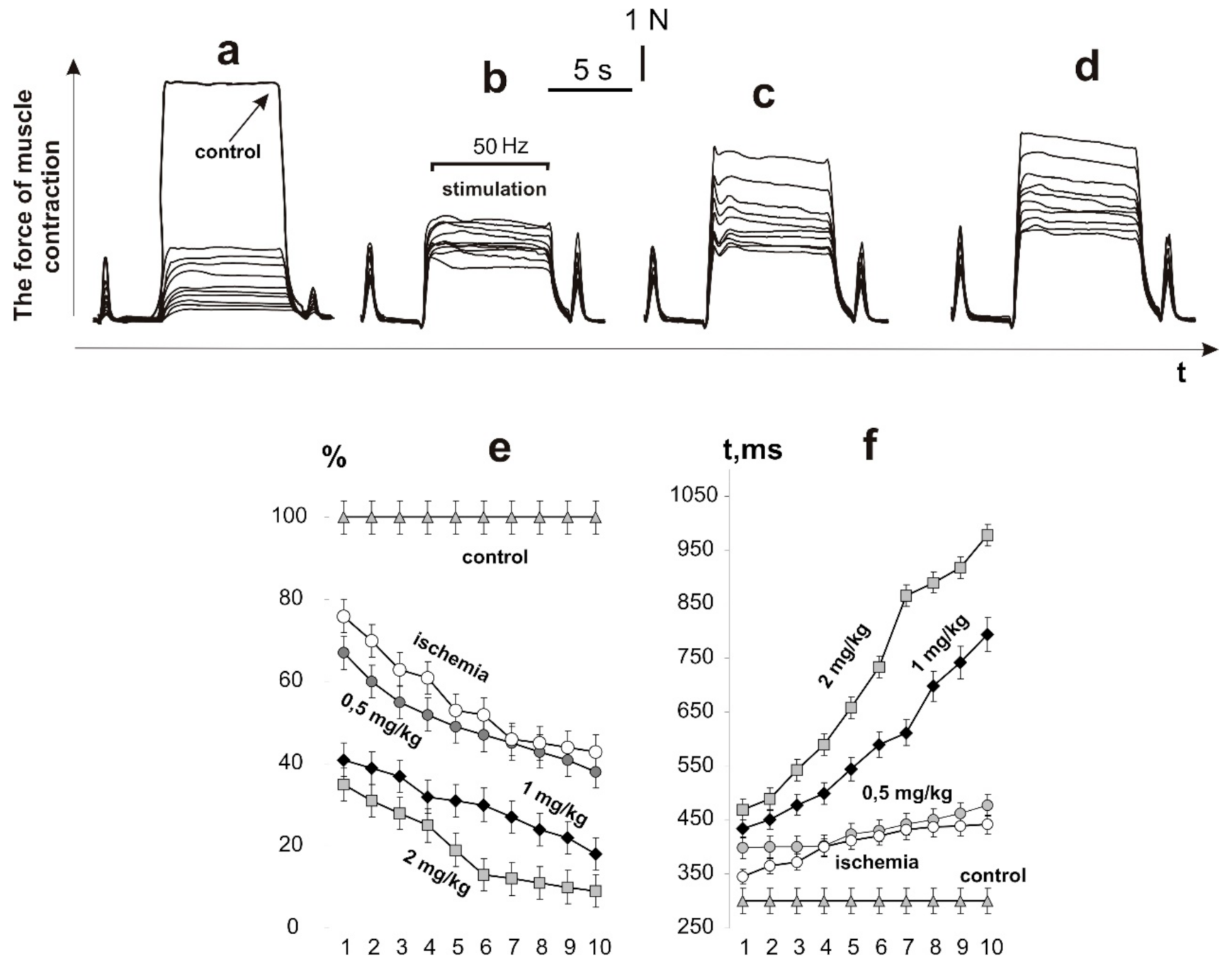
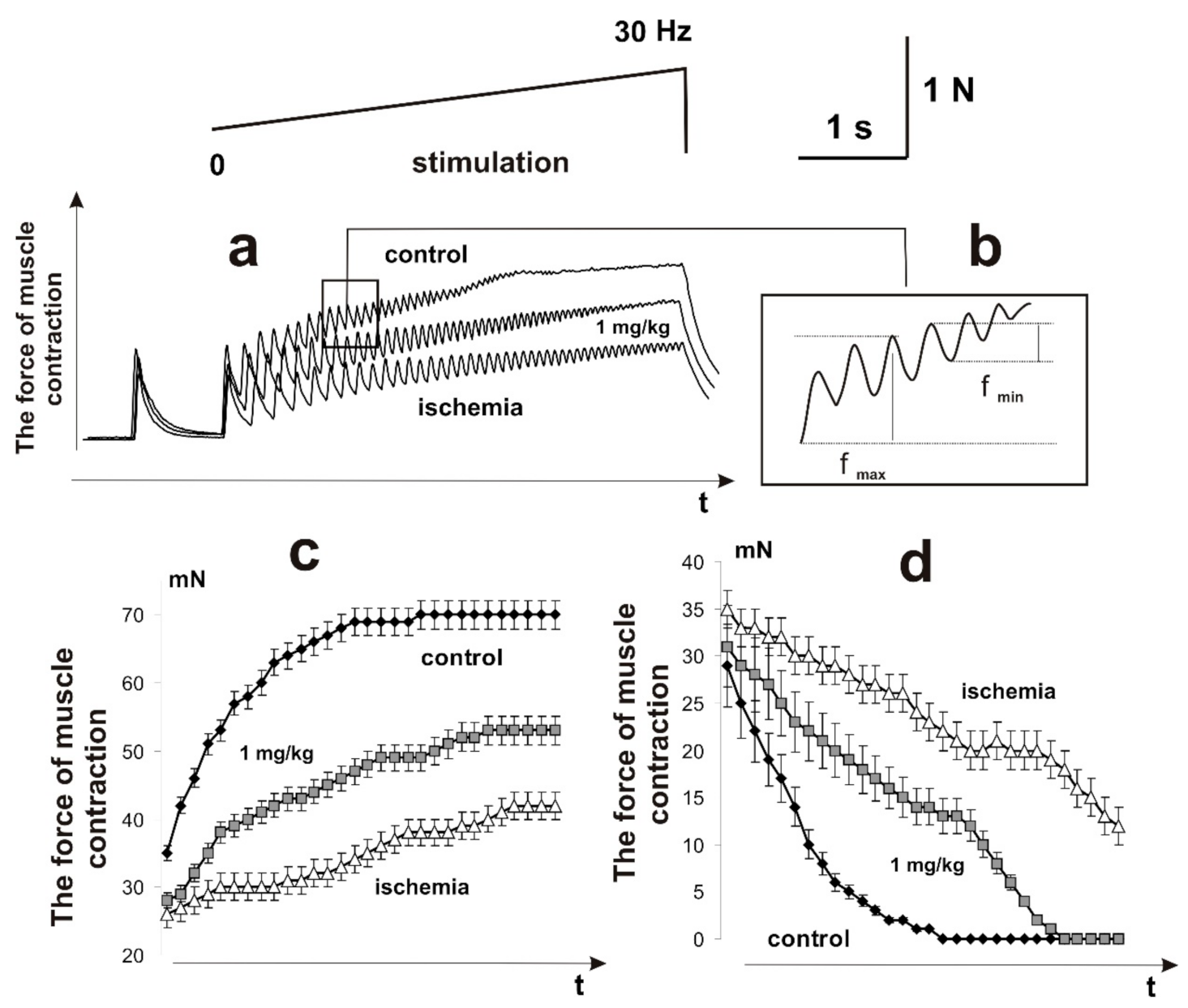
2.2. Biomechanics of Injured Muscle Contractions
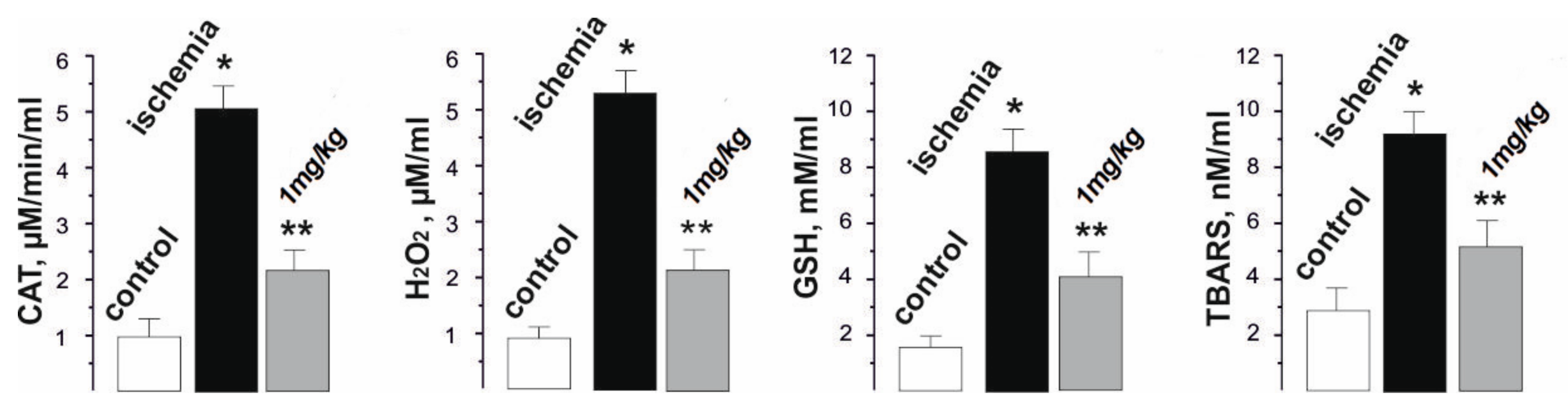
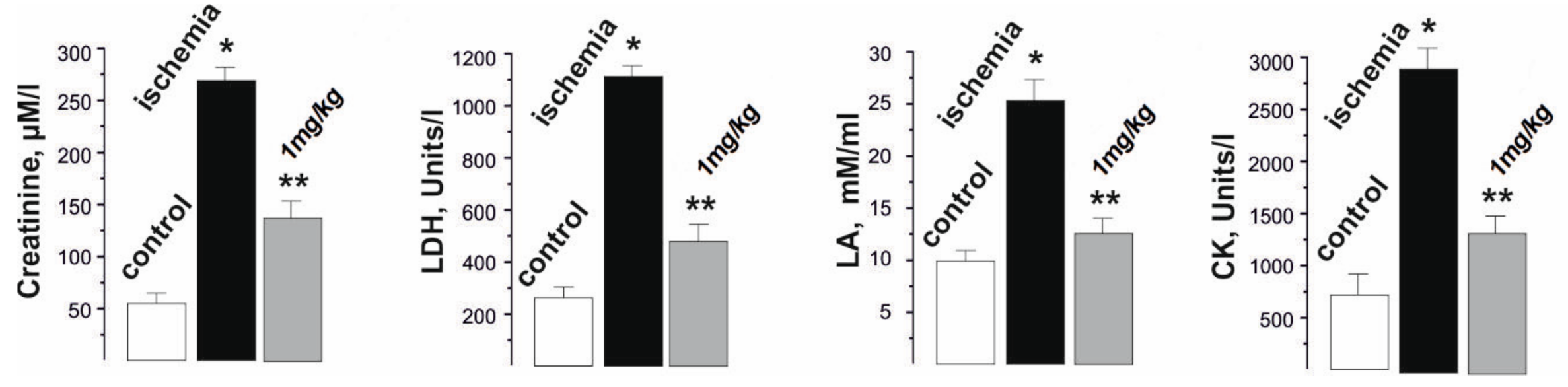
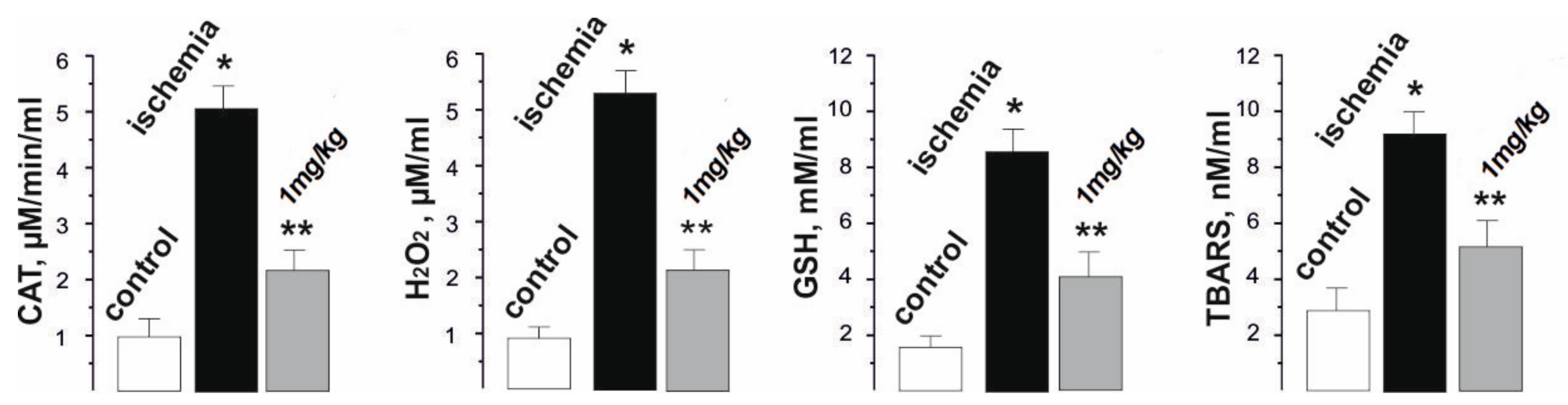
2.3. Blood Biochemical Indicators of Rats with Injured Muscle
3. Materials and Methods
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Erkut, B.; Özyazıcıoğlu, A.; Karapolat, B.S.; Koçoğulları, C.U.; Keles, S.; Ateş, A.; Gundogdu, C.; Kocaket, H. Effects of ascorbic acid, alpha-tocopherol and allopuri, nol on ischemia-reperfusion injury in rabbit skeletal muscle: An experimental study. Drug Target Insights 2007, 2, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Murdock, M.; Murdoch, M.M. Compartment Syndrome: A Review of the Literature. Clin. Podiatr. Med. Surg. 2012, 29, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Vignaud, A.; Hourdé, C.; Medja, F.; Agbulut, O.; Butler-Browne, G.; Ferry, A. Impaired Skeletal Muscle Repair after Ischemia-Reperfusion Injury in Mice. J. Biomed. Biotechnol. 2010, 2010, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korthals, J.K.; Maki, T.; Gieron, M.A. Nerve and muscle vulnerability to ischemia. J. Neurol. Sci. 1985, 71, 283–290. [Google Scholar] [CrossRef]
- Bortolotto, S.K.; Morrison, W.A.; Messina, A. The role of mast cells and fibre type in ischaemia reperfusion injury of murine skeletal muscles. J. Inflamm. 2004, 1, 2. [Google Scholar] [CrossRef] [Green Version]
- Rácz, I.; Illyés, G.; Sarkadi, L.; Hamar, J. The Functional and Morphological Damage of Ischemic Reperfused Skeletal Muscle. Eur. Surg. Res. 1997, 29, 254–263. [Google Scholar] [CrossRef]
- Turóczi, Z.; Arányi, P.; Lukáts, Á.; Garbaisz, D.; Lotz, G.; Harsanyi, L.; Szijártó, A. Muscle Fiber Viability, a Novel Method for the Fast Detection of Ischemic Muscle Injury in Rats. PLoS ONE 2014, 9, e84783. [Google Scholar] [CrossRef] [Green Version]
- Cuzzocrea, S.; Riley, D.P.; Caputi, A.P.; Salvemini, D. Antioxidant therapy: A new pharmacological approach in shock, inflammation, and ischemia/reperfusion injury. Pharmacol. Rev. 2001, 53, 135–159. [Google Scholar]
- Amani, H.; Habibey, R.; Hajmiresmail, S.J.; Latifi, S.; Pazoki-Toroudi, H.; Akhavan, O. Antioxidant nanomaterials in advanced diagnoses and treatments of ischemia reperfusion injuries. J. Mater. Chem. B 2017, 5, 9452–9476. [Google Scholar] [CrossRef]
- Eswaran, S.V. Water Soluble Nanocarbon Materials:A Panacea for All? Curr. Sci. 2018, 114, 1846–1850. [Google Scholar] [CrossRef]
- Ferreira, C.A.; Ni, D.; Rosenkrans, Z.T.; Cai, W. Scavenging of reactive oxygen and nitrogen species with nanomaterials. Nano Res. 2018, 11, 4955–4984. [Google Scholar] [CrossRef]
- Vereshchaka, I.V.; Bulgakova, N.; Maznychenko, A.; Gonchar, O.; Prylutskyy, Y.; Ritter, U.; Moska, W.; Tomiak, T.; Nozdrenko, D.M.; Mishchenko, I.V.; et al. C60 Fullerenes Diminish Muscle Fatigue in Rats Comparable to N-acetylcysteine or β-Alanine. Front. Physiol. 2018, 9, 517. [Google Scholar] [CrossRef]
- Krusic, P.J.; Wasserman, E.; Keizer, P.N.; Morton, J.R.; Preston, K.F. Radical Reactions of C60. Science 1991, 254, 1183–1185. [Google Scholar] [CrossRef]
- Halenova, T.; Raksha, N.; Savchuk, O.; Ostapchenko, L.; Prylutskyy, Y.; Ritter, U.; Scharff, P. Evaluation of the Biocompatibility of Water-Soluble Pristine С60 Fullerenes in Rabbit. BioNanoScience 2020, 10, 721–730. [Google Scholar] [CrossRef]
- Nozdrenko, D.M.; Zavodovskyi, D.O.; Matvienko, T.Y.; Zay, S.Y.; Bogutska, K.I.; Prylutskyy, Y.I.; Ritter, U.; Scharff, P. C60 Fullerene as Promising Therapeutic Agent for the Prevention and Correction of Skeletal Muscle Functioning at Ischemic Injury. Nanoscale Res. Lett. 2017, 12, 115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tidball, J.G. Mechanisms of Muscle Injury, Repair, and Regeneration. Compr. Physiol. 2011, 1, 2029–2062. [Google Scholar] [CrossRef] [PubMed]
- Prylutska, S.; Politenkova, S.; Afanasieva, K.; Korolovych, V.; Bogutska, K.; Sivolob, A.; Skivka, L.; Evstigneev, M.; Kostjukov, V.; Prylutskyy, Y.; et al. A nanocomplex of C60 fullerene with cisplatin: Design, characterization and toxicity. Beilstein J. Nanotechnol. 2017, 8, 1494–1501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraemer, Â.B.; Parfitt, G.M.; Acosta, D.D.S.; Bruch, G.E.; Cordeiro, M.F.; Marins, L.; Ventura-Lima, J.; Monserrat, J.; Barros, D.M. Fullerene (C60) particle size implications in neurotoxicity following infusion into the hippocampi of Wistar rats. Toxicol. Appl. Pharmacol. 2018, 338, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Dryn, D.O.; Melnyk, M.I.; Al Kury, L.T.; Prylutskyy, Y.; Ritter, U.; Zholos, A.V. C 60 fullerenes disrupt cellular signalling leading to TRPC4 and TRPC6 channels opening by the activation of muscarinic receptors and G-proteins in small intestinal smooth muscles. Cell. Signal. 2018, 43, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Singla, R.; Sharma, C.; Shukla, A.K.; Acharya, A. Toxicity Concerns of Therapeutic Nanomaterials. J. Nanosci. Nanotechnol. 2019, 19, 1889–1907. [Google Scholar] [CrossRef]
- Prilutski, Y.; Durov, S.; Yashchuk, V.; Ogul’Chansky, T.; Pogorelov, V.; Astashkin, Y.; Buzaneva, E.; Kirghisov, Y.; Andrievsky, G.; Scharff, P. Theoretical predictions and experimental studies of self-organized C60 nanoparticles in water solution and on the support. Eur. Phys. J. D 1999, 9, 341–343. [Google Scholar] [CrossRef]
- Prylutska, S.V.; Grebinyk, A.G.; Lynchak, O.V.; Byelinska, I.V.; Cherepanov, V.V.; Tauscher, E.; Matyshevska, O.P.; Prylutskyy, Y.I.; Rybalchenko, V.K.; Ritter, U.; et al. In vitro and in vivo toxicity of pristine C60 fullerene aqueous colloid solution. Fuller. Nanotub. Carbon Nanostruct. 2019, 27, 715–728. [Google Scholar] [CrossRef]
- Grace, P.A. Ischaemia-reperfusion injury. BJS 1994, 81, 637–647. [Google Scholar] [CrossRef]
- Carvalho, A.; Hollett, P.; McKee, N. Recovery of Synergistic Skeletal Muscle Function Following Ischemia. J. Surg. Res. 1995, 59, 527–533. [Google Scholar] [CrossRef]
- Kanda, K.; Hashizume, K. Factors causing difference in force output among motor units in the rat medial gastrocnemius muscle. J. Physiol. 1992, 448, 677–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khoma, O.; Zavodovs’Kyĭ, D.; Nozdrenko, D.; Dolhopolov, O.; Miroshnychenko, M.; Motuziuk, O. Dynamics of ischemic skeletal soleus muscle contraction in rats. Fiziol. Zh. 2014, 60, 34–40. [Google Scholar] [CrossRef]
- Grottel, K.; Celichowski, J. Division of motor units in medial gastrocnemius muscle of the rat in the light of variability of their principal properties. Acta Neurobiol. Exp. 1990, 50, 571–587. [Google Scholar]
- Nozdrenko, D.M.; Abramchuk, O.M.; Soroca, V.M.; Miroshnichenko, N.S. Aluminum chloride effect on Ca(2+),Mg(2+)-ATPase activity and dynamic parameters of skeletal muscle contraction. Ukr. Biochem. J. 2015, 87, 38–45. [Google Scholar] [CrossRef] [Green Version]
- Pettersson, J.; Hindorf, U.; Persson, P.; Bengtsson, T.; Malmqvist, U.; Werkström, V.; Ekelund, M. Muscular exercise can cause highly pathological liver function tests in healthy men. Br. J. Clin. Pharmacol. 2008, 65, 253–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chamorro, Á.; Dirnagl, U.; Urra, X.; Planas, A.M. Neuroprotection in acute stroke: Targeting excitotoxicity, oxidative and nitrosative stress, and inflammation. Lancet Neurol. 2016, 15, 869–881. [Google Scholar] [CrossRef]
- Birben, E.; Sahiner, U.M.; Sackesen, C.; Erzurum, S.; Kalayci, O. Oxidative Stress and Antioxidant Defense. World Allergy Organ. J. 2012, 5, 9–19. [Google Scholar] [CrossRef] [Green Version]
- Bakry, R.; Vallant, R.M.; Najam-ul-Haq, M.; Rainer, M.; Szabo, Z.; Huck, C.W.; Bonn, G.K. Medicinal applications of fullerenes. Int. J. Nanomed. 2007, 2, 639–649. [Google Scholar]
- Ryan, J.J.; Bateman, H.R.; Stover, A.; Gomez, G.; Norton, S.K.; Zhao, W.; Schwartz, L.B.; Lenk, R.; Kepley, C.L. Fullerene nanomaterials inhibit the allergic response. J. Immunol. 2007, 179, 665–672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srđenović, B.U.; Slavić, M.N.; Stankov, K.M.; Kladar, N.V.; Jović, D.S.; Seke, M.N.; Bogdanović, V.V. Size distribution of fullerenol nanoparticles in cell culture medium and their influence on antioxidative enzymes in Chinese hamster ovary cells. Chem. Ind. 2015, 69, 425–431. [Google Scholar] [CrossRef] [Green Version]
- Prylutska, S.V.; Grynyuk, I.I.; Matyshevska, O.P.; Prylutskyy, Y.I.; Ritter, U.; Scharff, P. Anti-oxidant Properties of C60Fullerenesin vitro. Fuller. Nanotub. Carbon Nanostruct. 2008, 16, 698–705. [Google Scholar] [CrossRef]
- Foley, S.; Crowley, C.; Smaihi, M.; Bonfils, C.; Erlanger, B.F.; Seta, P.; Larroque, C. Cellular localisation of a water-soluble fullerene derivative. Biochem. Biophys. Res. Commun. 2002, 294, 116–119. [Google Scholar] [CrossRef]
- Grebinyk, A.; Prylutska, S.; Chepurna, O.; Grebinyk, S.; Prylutskyy, Y.; Ritter, U.; Ohulchanskyy, T.Y.; Matyshevska, O.; Dandekar, T.; Frohme, M. Synergy of Chemo- and Photodynamic Therapies with C60 Fullerene-Doxorubicin Nanocomplex. Nanomaterials 2019, 9, 1540. [Google Scholar] [CrossRef] [Green Version]
- Halenova, T.I.; Vareniuk, I.M.; Roslova, N.M.; Dzerzhynsky, M.E.; Savchuk, O.; Ostapchenko, L.; Prylutskyy, Y.I.; Ritter, U.; Scharff, P. Hepatoprotective effect of orally applied water-soluble pristine C60 fullerene against CCl4-induced acute liver injury in rats. RSC Adv. 2016, 6, 100046–100055. [Google Scholar] [CrossRef]
- Prylutskyy, Y.I.; Vereshchaka, I.V.; Maznychenko, A.V.; Bulgakova, N.V.; Gonchar, O.O.; Kyzyma, O.A.; Ritter, U.; Scharff, P.; Tomiak, T.; Nozdrenko, D.M.; et al. C60 fullerene as promising therapeutic agent for correcting and preventing skeletal muscle fatigue. J. Nanobiotechnol. 2017, 15, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Kartal, H.; Küçük, A.; Kiliçarslan, A.; Polat, Y.; Süngü, N.; Kip, G.; Arslan, M. The effect of fullerenol C60 on skeletal muscle after lower limb ischemia reperfusion injury in streptozotocin-induced diabetic rats. J. Surg. Med. 2020, 4, 451–455. [Google Scholar] [CrossRef]
- Kuznietsova, H.; Dziubenko, N.; Hurmach, V.; Chereschuk, I.; Motuziuk, O.; Ogloblya, O.; Prylutskyy, Y. Water-Soluble Pristine C60 Fullerenes Inhibit Liver Fibrotic Alteration and Prevent Liver Cirrhosis in Rats. Oxidative Med. Cell. Longev. 2020, 2020, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Prylutskyy, Y.; Yashchuk, V.; Kushnir, K.; Golub, A.; Kudrenko, V.; Prylutska, S.; Grynyuk, I.; Buzaneva, E.; Scharff, P.; Braun, T.; et al. Biophysical studies of fullerene-based composite for bio-nanotechnology. Mater. Sci. Eng. C 2003, 23, 109–111. [Google Scholar] [CrossRef]
- Ritter, U.; Prylutskyy, Y.; Evstigneev, M.P.; Davidenko, N.A.; Cherepanov, V.V.; Senenko, A.I.; Marchenko, A.; Naumovets, A.G. Structural Features of Highly Stable Reproducible C60Fullerene Aqueous Colloid Solution Probed by Various Techniques. Fuller. Nanotub. Carbon Nanostruct. 2015, 23, 530–534. [Google Scholar] [CrossRef]
- Nozdrenko, D.N.; Berehovyi, S.M.; Nikitina, N.S.; Stepanova, L.I.; Beregova, T.V.; Ostapchenko, L.I. The influence of complex drug cocarnit on the nerve conduction velocity in nerve tibialis of rats with diabetic polyneuropathy. Biomed. Res. 2018, 29, 3629. [Google Scholar] [CrossRef] [Green Version]
- Brancaccio, P.; Lippi, G.; Maffulli, N. Biochemical markers of muscular damage. Clin. Chem. Lab. Med. 2010, 48, 757–767. [Google Scholar] [CrossRef]
- Gonchar, O.O.; Maznychenko, A.V.; Bulgakova, N.V.; Vereshchaka, I.V.; Tomiak, T.; Ritter, U.; Prylutskyy, Y.I.; Mankovska, I.M.; Kostyukov, A.I. C60 Fullerene Prevents Restraint Stress-Induced Oxidative Disorders in Rat Tissues: Possible Involvement of the Nrf2/ARE-Antioxidant Pathway. Oxidative Med. Cell. Longev. 2018, 2018, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nozdrenko, D.; Matvienko, T.; Vygovska, O.; Bogutska, K.; Motuziuk, O.; Nurishchenko, N.; Prylutskyy, Y.; Scharff, P.; Ritter, U. Protective Effect of Water-Soluble C60 Fullerene Nanoparticles on the Ischemia-Reperfusion Injury of the Muscle Soleus in Rats. Int. J. Mol. Sci. 2021, 22, 6812. https://doi.org/10.3390/ijms22136812
Nozdrenko D, Matvienko T, Vygovska O, Bogutska K, Motuziuk O, Nurishchenko N, Prylutskyy Y, Scharff P, Ritter U. Protective Effect of Water-Soluble C60 Fullerene Nanoparticles on the Ischemia-Reperfusion Injury of the Muscle Soleus in Rats. International Journal of Molecular Sciences. 2021; 22(13):6812. https://doi.org/10.3390/ijms22136812
Chicago/Turabian StyleNozdrenko, Dmytro, Tetiana Matvienko, Oksana Vygovska, Kateryna Bogutska, Olexandr Motuziuk, Natalia Nurishchenko, Yuriy Prylutskyy, Peter Scharff, and Uwe Ritter. 2021. "Protective Effect of Water-Soluble C60 Fullerene Nanoparticles on the Ischemia-Reperfusion Injury of the Muscle Soleus in Rats" International Journal of Molecular Sciences 22, no. 13: 6812. https://doi.org/10.3390/ijms22136812
APA StyleNozdrenko, D., Matvienko, T., Vygovska, O., Bogutska, K., Motuziuk, O., Nurishchenko, N., Prylutskyy, Y., Scharff, P., & Ritter, U. (2021). Protective Effect of Water-Soluble C60 Fullerene Nanoparticles on the Ischemia-Reperfusion Injury of the Muscle Soleus in Rats. International Journal of Molecular Sciences, 22(13), 6812. https://doi.org/10.3390/ijms22136812