
Pharmacokinetics, Tissue Distribution and Excretion of Demethyleneberberine, a Metabolite of Berberine, in Rats and Mice
Abstract
:
1. Introduction
2. Results and Discussion
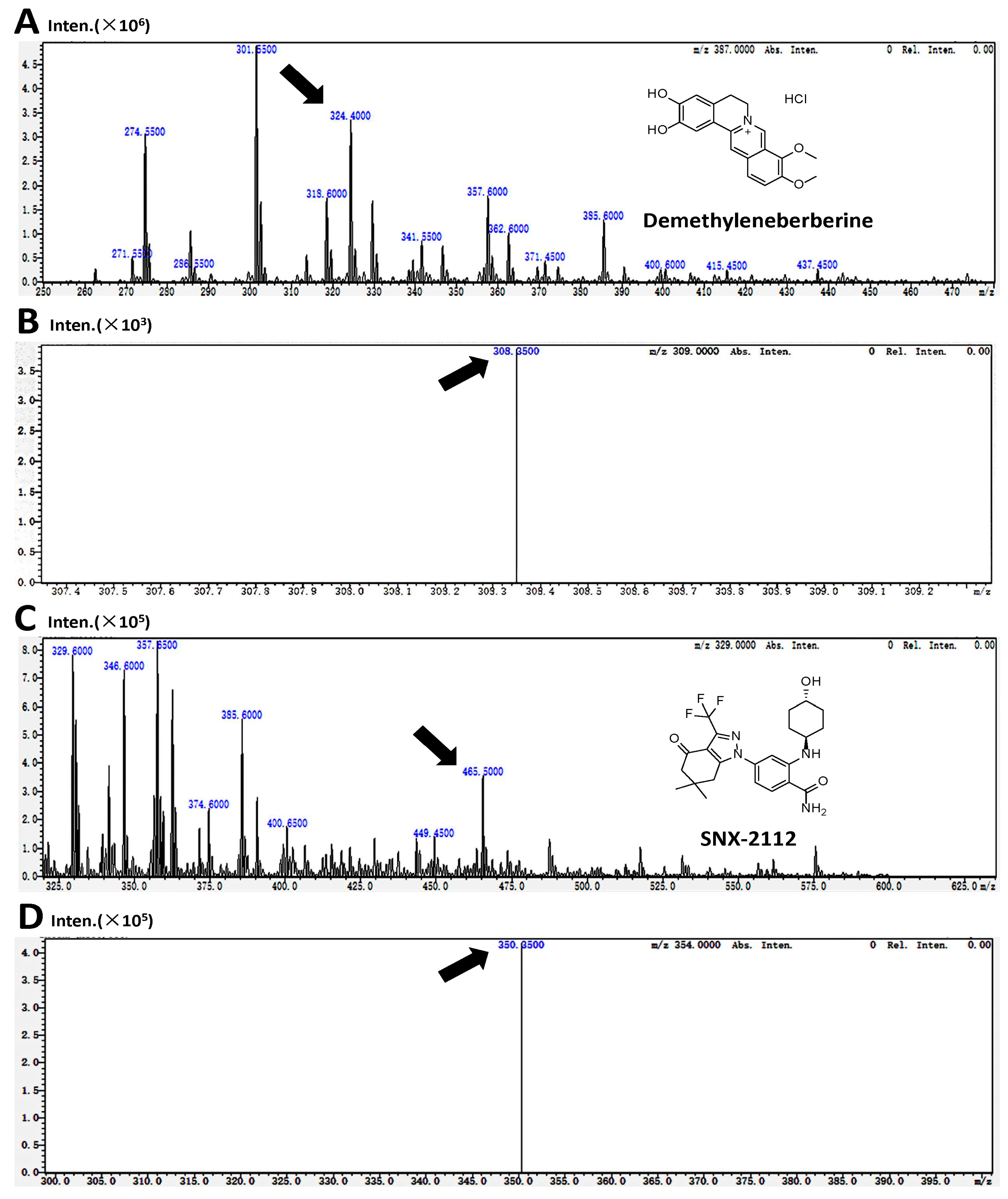
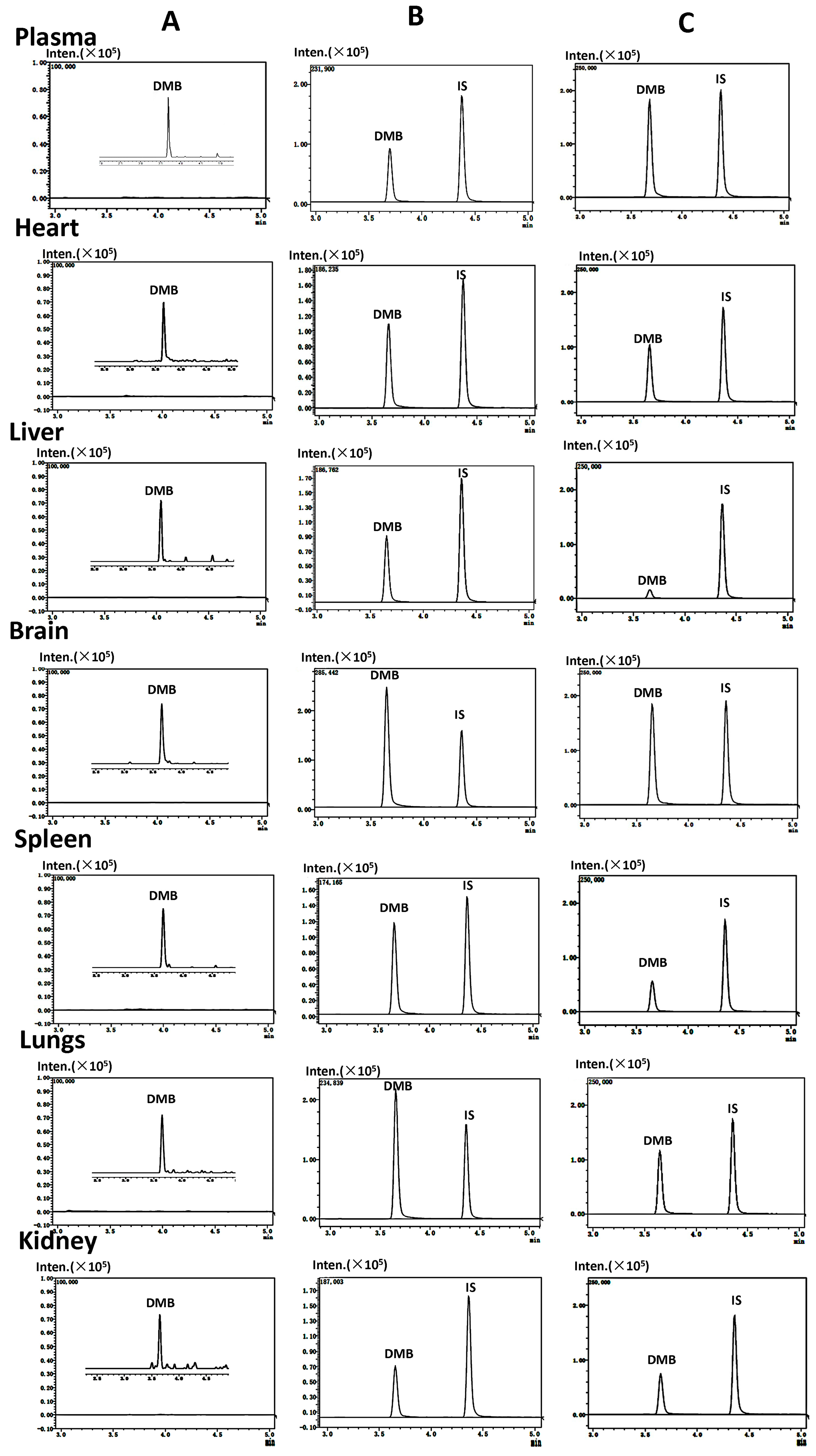
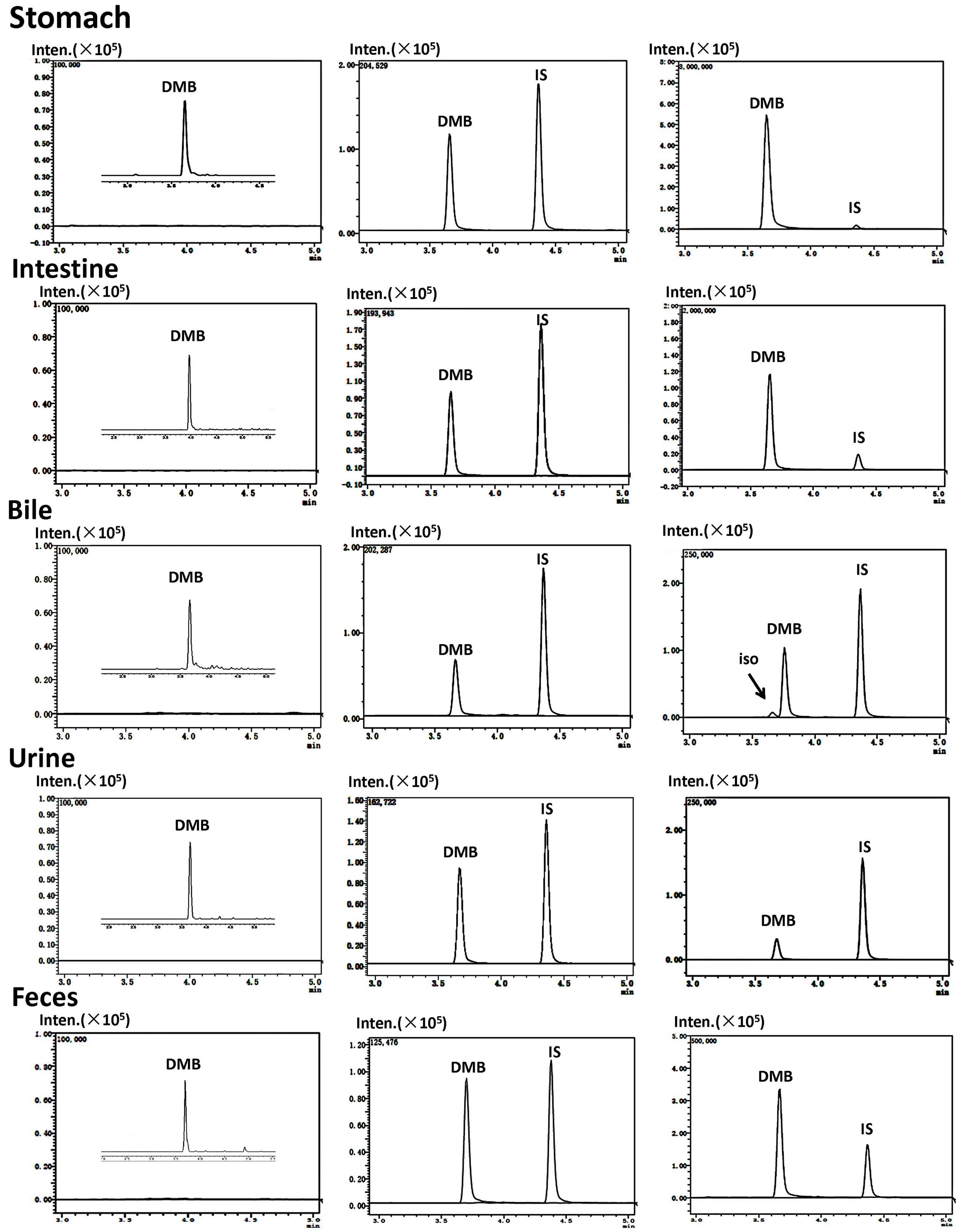
2.1. Validation of Method
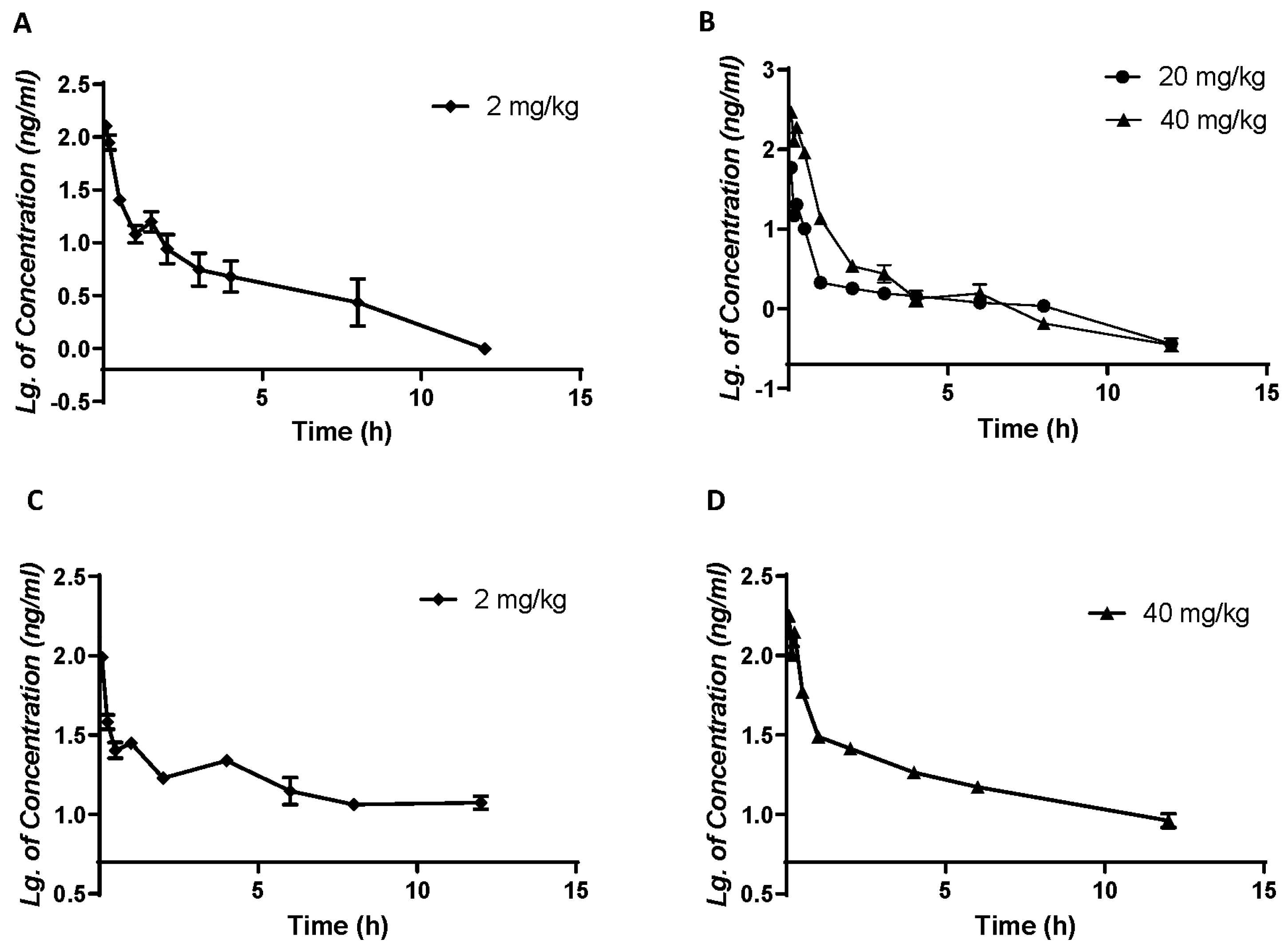
2.2. Pharmacokinetic Parameters and Bioavailability
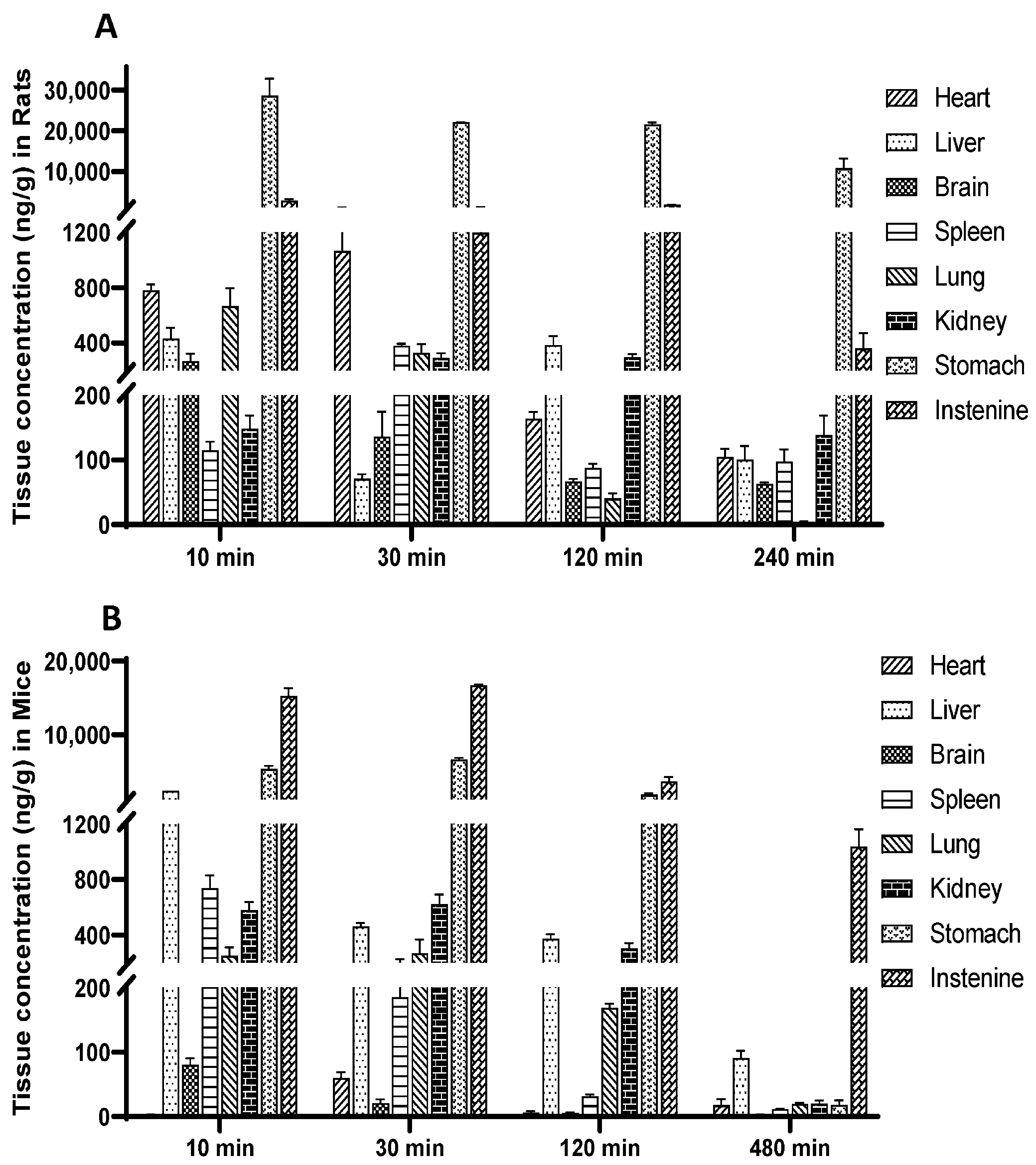
2.3. Tissue Distribution Study
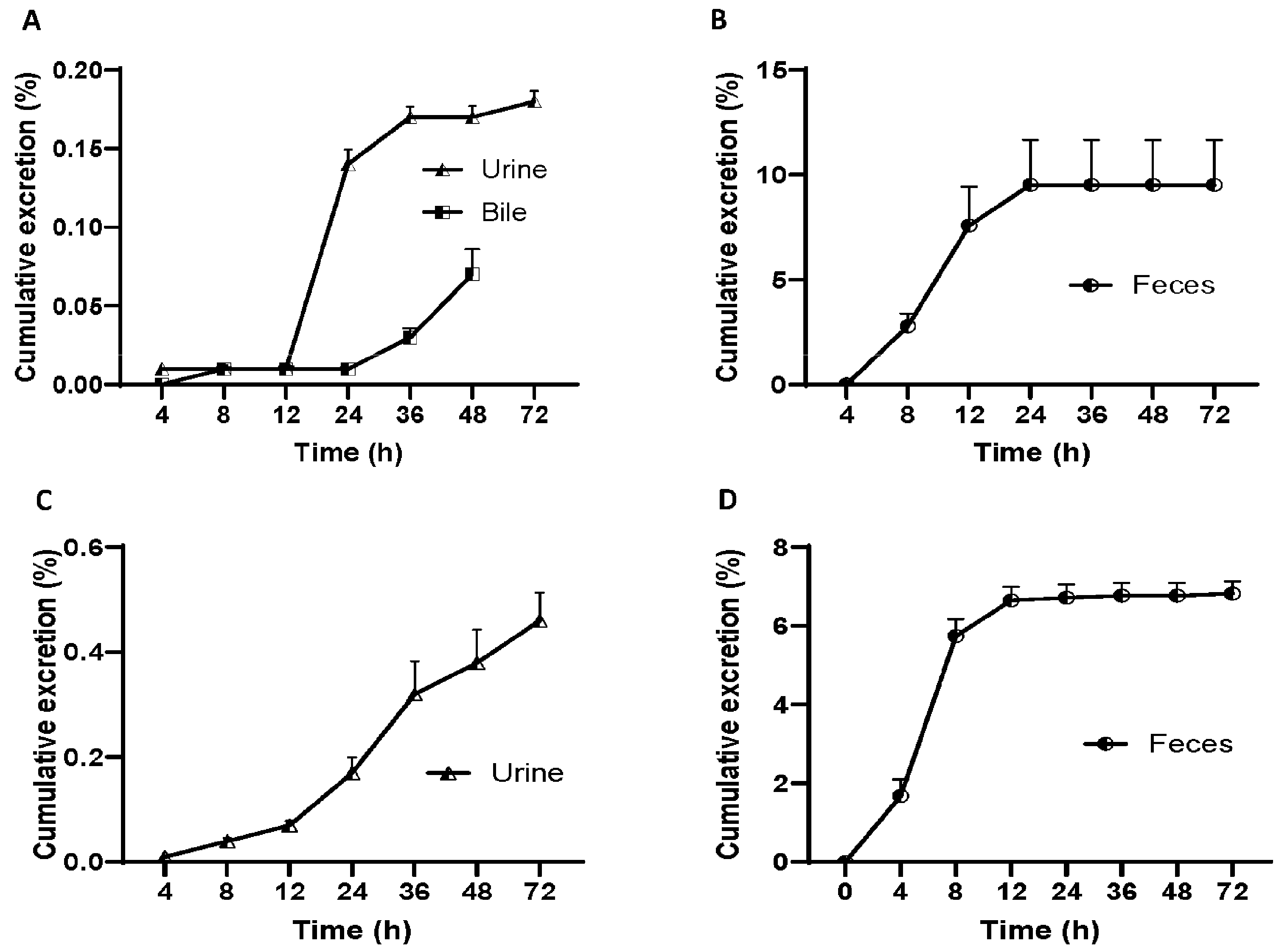
2.4. Excretion Study
3. Materials and Methods
3.1. Chemicals and Reagents
3.2. Animals
3.3. Instruments and Analytical Conditions
3.4. Standard and Sample Preparation
3.4.1. Preparation of Stock and Working Solutions
3.4.2. Preparation of Standard and Quality Control (QC) Samples
3.5. Validation of Methodology
3.6. Experiment
3.6.1. Pharmacokinetics and Bioavailability
3.6.2. Distribution Experiment
3.6.3. Excretion Experiments
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Zuo, F.; Nakamura, N.; Akao, T.; Hattori, M. Pharmacokinetics of berberine and its main metabolites in conventional and pseudo germ-free rats determined by liquid chromatography/ion trap mass spectrometry. Drug Metab. Dispos. Biol. Fate Chem. 2006, 34, 2064–2072. [Google Scholar] [CrossRef]
- Xiao, X.; Zhu, J.X.; Luo, G.M.; Li, L.; Zhu, Y.Y.; Zeng, J.X.; Wang, X.Y.; Wu, B. Study on the liver-protective and choleretic effect of zhizi baipi soup and its disassembled prescription. Zhong Yao Cai = Zhongyaocai = J. Chin. Med. Mater. 2013, 36, 1132–1135. [Google Scholar]
- Xu, B.; Yan, Y.; Huang, J.; Yin, B.; Pan, Y.; Ma, L. Cortex Phellodendri extract’s anti-diarrhea effect in mice related to its modification of gut microbiota. Biomed. Pharmacother. = Biomed. Pharmacother. 2020, 123, 109720. [Google Scholar] [CrossRef]
- Yin, M.C.; Chang, C.H.; Su, C.H.; Yu, B.; Hsu, Y.M. Pteris multifida, Cortex phellodendri, and probiotics attenuated inflammatory status and immunity in mice with a Salmonella enterica serovar Typhimurium infection. Biosci. Biotechnol. Biochem. 2018, 82, 836–847. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.Y.; Kim, M.H.; Han, J.M.; Hong, J.; Lee, T.H.; Kim, S.H.; Yang, W.M. The anti-inflammatory potential of Cortex Phellodendron in vivo and in vitro: Down-regulation of NO and iNOS through suppression of NF-κB and MAPK activation. Int. Immunopharmacol. 2014, 19, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zhang, S.; Wang, W.; Wang, Q.; Kuang, H.; Wang, Q. Characterizing metabolites and potential metabolic pathways changes to understanding the mechanism of medicinal plant Phellodendri Amurensis cortex against doxorubicin-induced nephritis rats using UPLC-Q/TOF-MS metabolomics. J. Pharm. Biomed. Anal. 2020, 188, 113336. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.W.; Kim, K.H.; Park, Y.K. Inhibitory effect of the extract of Phellodendron amurense ruprecht root on collagen-induced arthritis in mice. Chin. J. Integr. Med. 2017, 23, 755–762. [Google Scholar] [CrossRef]
- Kim, H.J.; Kong, M.K.; Kim, Y.C. Beneficial effects of Phellodendri Cortex extract on hyperglycemia and diabetic nephropathy in streptozotocin-induced diabetic rats. BMB Rep. 2008, 41, 710–715. [Google Scholar] [CrossRef]
- Wang, L.; Wang, X.; Zhu, X.M.; Liu, Y.Q.; Du, W.J.; Ji, J.; He, X.; Zhang, C.F.; Li, F.; Guo, C.R.; et al. Gastroprotective Effect of Alkaloids from Cortex Phellodendri on Gastric Ulcers in Rats through Neurohumoral Regulation. Planta Medica 2017, 83, 277–284. [Google Scholar] [CrossRef]
- Petronio Petronio, G.; Cutuli, M.A.; Magnifico, I.; Venditti, N.; Pietrangelo, L.; Vergalito, F.; Pane, A.; Scapagnini, G.; Di Marco, R. In Vitro and In Vivo Biological Activity of Berberine Chloride against Uropathogenic E. coli Strains Using Galleria mellonella as a Host Model. Molecules 2020, 25, 5010. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Huang, J.; Zhang, Y.; Huang, Z.; Yan, W.; Zhou, T.; Wang, Z.; Liao, L.; Cao, H.; Tan, B. Therapeutic Effects of Berberine Hydrochloride on Stress-Induced Diarrhea-Predominant Irritable Bowel Syndrome Rats by Inhibiting Neurotransmission in Colonic Smooth Muscle. Front. Pharmacol. 2021, 12, 596686. [Google Scholar] [CrossRef] [PubMed]
- Wei, W.; Zeng, Q.; Wang, Y.; Guo, X.; Fan, T.; Li, Y.; Deng, H.; Zhao, L.; Zhang, X.; Liu, Y.; et al. Discovery and identification of EIF2AK2 as a direct key target of berberine for anti-inflammatory effects. Acta Pharm. Sin. B 2023, 13, 2138–2151. [Google Scholar] [CrossRef] [PubMed]
- Gu, S.; Cao, B.; Sun, R.; Tang, Y.; Paletta, J.L.; Wu, X.; Liu, L.; Zha, W.; Zhao, C.; Li, Y.; et al. A metabolomic and pharmacokinetic study on the mechanism underlying the lipid-lowering effect of orally administered berberine. Mol. Biosyst. 2015, 11, 463–474. [Google Scholar] [CrossRef]
- Qing, Y.; Dong, X.; Hongli, L.; Yanhui, L. Berberine promoted myocardial protection of postoperative patients through regulating myocardial autophagy. Biomed. Pharmacother. 2018, 105, 1050–1053. [Google Scholar] [CrossRef] [PubMed]
- Song, T.; Chen, W.D. Berberine inhibited carotid atherosclerosis through PI3K/AKTmTOR signaling pathway. Bioengineered 2021, 12, 8135–8146. [Google Scholar] [CrossRef]
- Zhu, L.; Zhang, D.; Zhu, H.; Zhu, J.; Weng, S.; Dong, L.; Liu, T.; Hu, Y.; Shen, X. Berberine treatment increases Akkermansia in the gut and improves high-fat diet-induced atherosclerosis in Apoe(-/-) mice. Atherosclerosis 2018, 268, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Li, M.; Qin, Z.; Ma, X.; Huang, R.; Liu, Y.; Xie, J.; Zeng, H.; Zhan, R.; Su, Z. Intestines-erythrocytes-mediated bio-disposition deciphers the hypolipidemic effect of berberine from Rhizoma Coptidis: A neglected insight. J. Ethnopharmacol. 2023, 314, 116600. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Zhao, Y.; Zhang, Y.; Yang, Y.; Su, W.; Yang, Y.; Sun, L.; Zhang, F.; Yu, J.; Wang, Y.; et al. Gut microbiota specifically mediates the anti-hypercholesterolemic effect of berberine (BBR) and facilitates to predict BBR’s cholesterol-decreasing efficacy in patients. J. Adv. Res. 2022, 37, 197–208. [Google Scholar] [CrossRef]
- Ma, S.R.; Tong, Q.; Lin, Y.; Pan, L.B.; Fu, J.; Peng, R.; Zhang, X.F.; Zhao, Z.X.; Li, Y.; Yu, J.B.; et al. Berberine treats atherosclerosis via a vitamine-like effect down-regulating Choline-TMA-TMAO production pathway in gut microbiota. Signal Transduct. Target. Ther. 2022, 7, 207. [Google Scholar] [CrossRef]
- Zhao, Z.; Meng, M.; Yao, J.; Zhou, H.; Chen, Y.; Liu, J.; Wang, J.; Liu, Y.; Qiao, Y.; Zhang, M.; et al. The long non-coding RNA keratin-7 antisense acts as a new tumor suppressor to inhibit tumorigenesis and enhance apoptosis in lung and breast cancers. Cell Death Dis. 2023, 14, 293. [Google Scholar] [CrossRef]
- Chen, H.; Ye, C.; Wu, C.; Zhang, J.; Xu, L.; Wang, X.; Xu, C.; Zhang, J.; Guo, Y.; Yao, Q. Berberine inhibits high fat diet-associated colorectal cancer through modulation of the gut microbiota-mediated lysophosphatidylcholine. Int. J. Biol. Sci. 2023, 19, 2097–2113. [Google Scholar] [CrossRef]
- Xiong, R.G.; Huang, S.Y.; Wu, S.X.; Zhou, D.D.; Yang, Z.J.; Saimaiti, A.; Zhao, C.N.; Shang, A.; Zhang, Y.J.; Gan, R.Y.; et al. Anticancer Effects and Mechanisms of Berberine from Medicinal Herbs: An Update Review. Molecules 2022, 27, 4523. [Google Scholar] [CrossRef] [PubMed]
- He, Q.; Dong, H.; Guo, Y.; Gong, M.; Xia, Q.; Lu, F.; Wang, D. Multi-target regulation of intestinal microbiota by berberine to improve type 2 diabetes mellitus. Front. Endocrinol. 2022, 13, 1074348. [Google Scholar] [CrossRef]
- Guo, H.H.; Shen, H.R.; Wang, L.L.; Luo, Z.G.; Zhang, J.L.; Zhang, H.J.; Gao, T.L.; Han, Y.X.; Jiang, J.D. Berberine is a potential alternative for metformin with good regulatory effect on lipids in treating metabolic diseases. Biomed. Pharmacother. 2023, 163, 114754. [Google Scholar] [CrossRef]
- Ren, G.; Ding, Y.W.; Wang, L.L.; Jiang, J.D. Berberine stimulates lysosomal AMPK independent of PEN2 and maintains cellular AMPK activity through inhibiting the dephosphorylation regulator UHRF1. Front. Pharmacol. 2023, 14, 1148611. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Chen, M.; Wang, Z.; Fan, Q.; Lin, Z.; Tao, X.; Wu, J.; Liu, Z.; Lin, R.; Zhao, C. Berberine inhibits RA-FLS cell proliferation and adhesion by regulating RAS/MAPK/FOXO/HIF-1 signal pathway in the treatment of rheumatoid arthritis. Bone Jt. Res. 2023, 12, 91–102. [Google Scholar] [CrossRef]
- Li, C.; Leng, Q.; Li, L.; Hu, F.; Xu, Y.; Gong, S.; Yang, Y.; Zhang, H.; Li, X. Berberine Ameliorates Obesity by Inducing GDF15 Secretion by Brown Adipocytes. Endocrinology 2023, 164, bqad035. [Google Scholar] [CrossRef] [PubMed]
- Rong, Q.; Han, B.; Li, Y.; Yin, H.; Li, J.; Hou, Y. Berberine Reduces Lipid Accumulation by Promoting Fatty Acid Oxidation in Renal Tubular Epithelial Cells of the Diabetic Kidney. Front. Pharmacol. 2021, 12, 729384. [Google Scholar] [CrossRef]
- Liu, M.; Xu, Z. Berberine Promotes the Proliferation and Osteogenic Differentiation of Alveolar Osteoblasts through Regulating the Expression of miR-214. Pharmacology 2021, 106, 70–78. [Google Scholar] [CrossRef]
- Chen, Q.C.; Pu, Y.L.; Bi, J.; Zhang, Y. Protective effects of berberine on senile osteoporosis in mice. J. Bone Miner. Metab. 2021, 39, 748–756. [Google Scholar] [CrossRef]
- Zhu, L.; Xu, J.J.; Li, H.D.; Li, J.J.; Cheng, M.; Niu, X.N.; Jia, P.C.; Liu, J.Y.; Huang, C.; Lv, X.W.; et al. Berberine Ameliorates Abnormal Lipid Metabolism via the Adenosine Monophosphate-Activated Protein Kinase/Sirtuin 1 Pathway in Alcohol-Related Liver Disease. Lab. Investig. A J. Tech. Methods Pathol. 2023, 103, 100041. [Google Scholar] [CrossRef] [PubMed]
- Ye, C.; Zhang, Y.; Lin, S.; Chen, Y.; Wang, Z.; Feng, H.; Fang, G.; Quan, S. Berberine Ameliorates Metabolic-Associated Fatty Liver Disease Mediated Metabolism Disorder and Redox Homeostasis by Upregulating Clock Genes: Clock and Bmal1 Expressions. Molecules 2023, 28, 1874. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Liu, X.; Wang, X.; Lu, Z.; Ye, Y. Berberine Alleviates Acute Lung Injury in Septic Mice by Modulating Treg/Th17 Homeostasis and Downregulating NF-κB Signaling. Drug Des. Dev. Ther. 2023, 17, 1139–1151. [Google Scholar] [CrossRef]
- Ahmedy, O.A.; Kamel, M.W.; Abouelfadl, D.M.; Shabana, M.E.; Sayed, R.H. Berberine attenuates epithelial mesenchymal transition in bleomycin-induced pulmonary fibrosis in mice via activating A(2a)R and mitigating the SDF-1/CXCR4 signaling. Life Sci. 2023, 322, 121665. [Google Scholar] [CrossRef]
- Ding, W.; Gu, Q.; Liu, M.; Zou, J.; Sun, J.; Zhu, J. Astrocytes-derived exosomes pre-treated by berberine inhibit neuroinflammation after stroke via miR-182-5p/Rac1 pathway. Int. Immunopharmacol. 2023, 118, 110047. [Google Scholar] [CrossRef]
- Zhang, R.L.; Lei, B.X.; Wu, G.Y.; Wang, Y.Y.; Huang, Q.H. Protective effects of berberine against β-amyloid-induced neurotoxicity in HT22 cells via the Nrf2/HO-1 pathway. Bioorganic Chem. 2023, 133, 106210. [Google Scholar] [CrossRef]
- Feng, X.; Wang, K.; Cao, S.; Ding, L.; Qiu, F. Pharmacokinetics and Excretion of Berberine and Its Nine Metabolites in Rats. Front. Pharmacol. 2020, 11, 594852. [Google Scholar] [CrossRef]
- Chen, W.; Miao, Y.Q.; Fan, D.J.; Yang, S.S.; Lin, X.; Meng, L.K.; Tang, X. Bioavailability study of berberine and the enhancing effects of TPGS on intestinal absorption in rats. AAPS PharmSciTech 2011, 12, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.T.; Hao, H.P.; Xie, H.G.; Lai, L.; Wang, Q.; Liu, C.X.; Wang, G.J. Extensive intestinal first-pass elimination and predominant hepatic distribution of berberine explain its low plasma levels in rats. Drug Metab. Dispos. Biol. Fate Chem. 2010, 38, 1779–1784. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.Y.; Li, R.Y.; Shi, M.J.; Zhao, Y.X.; Yan, Y.; Xu, X.X.; Zhang, M.; Zhao, X.T.; Zhang, Y.B. Demethyleneberberine alleviates inflammatory bowel disease in mice through regulating NF-κB signaling and T-helper cell homeostasis. Res. Soc. 2017, 66, 187–196. [Google Scholar] [CrossRef]
- Zhao, Y.; Liu, P.; Luan, H.; Jiang, H.; Xu, Y.; Zhang, Y.; Zhang, Y.; Li, R. Demethyleneberberine alleviated the inflammatory response by targeting MD-2 to inhibit the TLR4 signaling. Front. Immunol. 2023, 14, 1130404. [Google Scholar] [CrossRef]
- Zhao, Y.; Liu, P.; Zhang, Y.; Jiang, H.; Luan, H.; Xu, Y.; Zhang, Y.; Li, R. Demethyleneberberine blocked the maturation of IL-1β in inflammation by inhibiting TLR4-mitochondria signaling. Int. Immunopharmacol. 2022, 113 Pt A, 109319. [Google Scholar] [CrossRef]
- Wang, Y.; Zhao, Z.; Yan, Y.; Qiang, X.; Zhou, C.; Li, R.; Chen, H.; Zhang, Y. Demethyleneberberine Protects against Hepatic Fibrosis in Mice by Modulating NF-κB Signaling. Int. J. Mol. Sci. 2016, 17, 1036. [Google Scholar] [CrossRef]
- Zhang, M.; Li, Q.; Zhou, C.; Zhao, Y.; Li, R.; Zhang, Y. Demethyleneberberine attenuates concanavalin A-induced autoimmune hepatitis in mice through inhibition of NF-κB and MAPK signaling. Int. Immunopharmacol. 2020, 80, 106137. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Qiang, X.; Zhang, M.; Ma, D.; Zhao, Z.; Zhou, C.; Liu, X.; Li, R.; Chen, H.; Zhang, Y. Demethyleneberberine, a natural mitochondria-targeted antioxidant, inhibits mitochondrial dysfunction, oxidative stress, and steatosis in alcoholic liver disease mouse model. J. Pharmacol. Exp. Ther. 2015, 352, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Ge, C.; Han, Y. To methylene berberine hydrochloride in the preparation of the application of the treatment of pulmonary fibrosis drug. CN115192573A, 18 October 2022. [Google Scholar]
- Liu, J.; Huang, X.; Liu, D.; Ji, K.; Tao, C.; Zhang, R.; Chen, J. Demethyleneberberine induces cell cycle arrest and cellular senescence of NSCLC cells via c-Myc/HIF-1α pathway. Phytomedicine Int. J. Phytother. Phytopharm. 2021, 91, 153678. [Google Scholar] [CrossRef]
- Wang, Z.; Wang, L.; Shi, B.; Sun, X.; Xie, Y.; Yang, H.; Zi, C.; Wang, X.; Sheng, J. Demethyleneberberine promotes apoptosis and suppresses TGF-β/Smads induced EMT in the colon cancer cells HCT-116. Cell Biochem. Funct. 2021, 39, 763–770. [Google Scholar] [CrossRef]
- Wang, S.; Lee, D.Y.; Shang, Y.; Liao, J.; Cao, X.; Xie, L.; Zhang, T.; Liu, J.; Dai, R. The bioactive alkaloids identified from Cortex Phellodendri ameliorate benign prostatic hyperplasia via LOX-5/COX-2 pathways. Phytomedicine Int. J. Phytother. Phytopharm. 2021, 93, 153813. [Google Scholar] [CrossRef]
- Cao, S.; Zhou, Y.; Xu, P.; Wang, Y.; Yan, J.; Bin, W.; Qiu, F.; Kang, N. Berberine metabolites exhibit triglyceride-lowering effects via activation of AMP-activated protein kinase in Hep G2 cells. J. Ethnopharmacol. 2013, 149, 576–582. [Google Scholar] [CrossRef]
- Zhou, Y.; Cao, S.; Wang, Y.; Xu, P.; Yan, J.; Bin, W.; Qiu, F.; Kang, N. Berberine metabolites could induce low density lipoprotein receptor up-regulation to exert lipid-lowering effects in human hepatoma cells. Fitoterapia 2014, 92, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Qiang, X.; Xu, L.; Zhang, M.; Zhang, P.; Wang, Y.; Wang, Y.; Zhao, Z.; Chen, H.; Liu, X.; Zhang, Y. Demethyleneberberine attenuates non-alcoholic fatty liver disease with activation of AMPK and inhibition of oxidative stress. Biochem. Biophys. Res. Commun. 2016, 472, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Saklani, P.; Khan, H.; Singh, T.G.; Gupta, S.; Grewal, A.K. Demethyleneberberine, a potential therapeutic agent in neurodegenerative disorders: A proposed mechanistic insight. Mol. Biol. Rep. 2022, 49, 10101–10113. [Google Scholar] [CrossRef] [PubMed]
- Tao, C.; Hu, S.Q.; Chen, J.; Chen, Y.J.; Sun, K.H.; Cui, G.Z.; Ma, M.; Wu, Z.Z. Highly efficient synthesis and monoamine oxidase B inhibitory profile of demethyleneberberine, columbamine and palmatine. Neurochem. Int. 2020, 139, 104807. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food, Drug Administration. Bioanalytical Method Validation Guidance for Industry. 2018. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/bioanalytical-method-validation-guidance-industry (accessed on 31 May 2018).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Matrix | Regression Equations | Correlation Coefficient (r2) | Linear Range (ng/mL) |
|---|---|---|---|
| Plasma | Y = 227.71 X + 9.788 | 0.9984 | 0.5–1000 |
| Heart | Y = 867.95 X + 15.193 | 0.9994 | 1–1000 |
| Liver | Y = 770.17 X + 6.9004 | 0.9998 | 1–1000 |
| Spleen | Y = 271.01 X + 16.991 | 0.9940 | 1–1000 |
| Lung | Y = 239.7 X − 6.2526 | 0.9983 | 1–1000 |
| Kidney | Y = 560.53 X + 13.146 | 0.9964 | 1–1000 |
| Brain | Y = 198.63 X + 17.806 | 0.9948 | 1–1000 |
| Stomach | Y = 418.44 X − 26.683 | 0.9976 | 3–3000 |
| Intestine | Y = 1379.2 X + 9.7943 | 0.9961 | 1–3000 |
| Urine | Y = 363.85 X + 12.913 | 0.9998 | 1–3000 |
| Feces | Y = 605.06 X − 61.477 | 0.9930 | 3–5000 |
| Bile | Y = 716.2 X − 18.949 | 0.9911 | 3–5000 |
| Sample | Analyte Concentration(ng/mL) | Precision RSD (%) | Accuracy (%) | ||
|---|---|---|---|---|---|
| Intra-Day | Inter-Day | Intra-Day | Inter-Day | ||
| Plasma | 0.5 (LLOQ) | 4.25 | 8.67 | 104.91 | 114.73 |
| 10 | 2.57 | 2.58 | 103.11 | 113.43 | |
| 200 | 1.34 | 0.99 | 100.90 | 108.32 | |
| 800 | 0.63 | 0.50 | 102.76 | 102.75 | |
| Heart | 1 (LLOQ) | 6.67 | 12.30 | 81.60 | 85.70 |
| 10 | 5.50 | 14.74 | 102.58 | 89.73 | |
| 200 | 8.90 | 2.23 | 102.92 | 114.71 | |
| 800 | 0.10 | 5.73 | 93.65 | 89.94 | |
| Liver | 1 (LLOQ) | 4.67 | 13.97 | 80.02 | 89.75 |
| 10 | 1.91 | 6.09 | 90.37 | 91.14 | |
| 200 | 3.21 | 0.87 | 106.93 | 104.87 | |
| 800 | 1.63 | 1.62 | 102.44 | 92.49 | |
| Brain | 1 (LLOQ) | 5.80 | 5.26 | 83.55 | 85.83 |
| 10 | 13.15 | 10.26 | 91.59 | 87.16 | |
| 200 | 7.74 | 1.82 | 109.08 | 101.39 | |
| 800 | 1.86 | 0.08 | 100.83 | 99.22 | |
| Spleen | 1 (LLOQ) | 7.75 | 5.72 | 80.13 | 100.28 |
| 10 | 2.36 | 8.68 | 106.79 | 115.18 | |
| 200 | 1.57 | 7.17 | 109.16 | 104.90 | |
| 800 | 3.55 | 2.69 | 101.39 | 107.88 | |
| Lungs | 1 (LLOQ) | 10.80 | 11.53 | 115.04 | 101.50 |
| 10 | 1.69 | 2.56 | 87.57 | 91.21 | |
| 200 | 0.29 | 3.20 | 105.11 | 109.10 | |
| 800 | 6.99 | 10.62 | 113.73 | 94.75 | |
| Kidney | 1 (LLOQ) | 1.80 | 2.75 | 89.25 | 81.70 |
| 10 | 4.84 | 3.28 | 110.85 | 85.41 | |
| 200 | 6.13 | 4.51 | 105.01 | 102.76 | |
| 800 | 0.44 | 1.92 | 96.11 | 92.05 | |
| Stomach | 3 (LLOQ) | 2.30 | 12.65 | 104.21 | 89.98 |
| 10 | 8.74 | 9.00 | 115.25 | 90.55 | |
| 200 | 0.82 | 13.75 | 106.09 | 104.61 | |
| 800 | 1.34 | 8.31 | 108.20 | 85.88 | |
| Intestine | 1 (LLOQ) | 5.63 | 13.69 | 83.16 | 86.80 |
| 10 | 3.56 | 2.93 | 111.16 | 102.14 | |
| 200 | 1.62 | 1.29 | 92.58 | 99.45 | |
| 800 | 0.49 | 0.96 | 113.87 | 109.00 | |
| Bile | 3 (LLOQ) | 2.95 | 14.14 | 115.01 | 114.64 |
| 10 | 8.94 | 4.27 | 101.63 | 94.98 | |
| 200 | 2.54 | 6.25 | 87.42 | 88.67 | |
| 800 | 3.10 | 2.85 | 89.83 | 94.15 | |
| Urine | 1 (LLOQ) | 13.26 | 4.59 | 94.24 | 114.01 |
| 10 | 4.89 | 7.98 | 114.91 | 110.41 | |
| 200 | 2.39 | 2.31 | 102.32 | 97.55 | |
| 800 | 0.76 | 0.79 | 109.88 | 109.23 | |
| Feces | 3 (LLOQ) | 9.87 | 12.23 | 111.99 | 119.44 |
| 10 | 10.39 | 14.19 | 100.57 | 92.30 | |
| 200 | 3.91 | 0.77 | 113.28 | 90.34 | |
| 800 | 1.29 | 3.81 | 91.85 | 114.27 | |
| Sample | Analyte Concentration (ng/mL) | Extract Recovery (Mean ± SD, %) | Matrix Effect (Mean ± SD, %) |
|---|---|---|---|
| Plasma | 10 | 83.17 ± 7.16 | 113.51 ± 0.33 |
| 200 | 84.46 ± 2.06 | 108.25 ± 3.17 | |
| 800 | 82.77 ± 2.30 | 89.22 ± 1.02 | |
| Heart | 10 | 101.41 ± 5.11 | 94.47 ± 3.01 |
| 200 | 89.46 ± 11.58 | 103.68 ± 1.65 | |
| 800 | 84.14 ± 0.77 | 82.27 ± 2.47 | |
| Liver | 10 | 91.87 ± 8.39 | 90.01 ± 9.78 |
| 200 | 94.43 ± 0.41 | 108.25 ± 0.61 | |
| 800 | 102.52 ± 0.11 | 113.83 ± 0.11 | |
| Brain | 10 | 101.95 ± 5.92 | 113.36 ± 10.55 |
| 200 | 94.51 ± 0.76 | 98.48 ± 0.92 | |
| 800 | 97.54 ± 3.10 | 100.18 ± 0.37 | |
| Spleen | 10 | 84.67 ± 1.12 | 84.13 ± 1.99 |
| 200 | 91.93 ± 8.83 | 115.10 ± 9.42 | |
| 800 | 91.21 ±1.44 | 91.79 ± 1.46 | |
| Lung | 10 | 98.78 ± 9.37 | 83.71 ± 5.63 |
| 200 | 98.81 ± 1.07 | 88.23 ± 3.25 | |
| 800 | 106.93 ± 6.57 | 86.77 ± 4.05 | |
| Kidney | 10 | 94.31 ± 7.53 | 85.78 ± 6.13 |
| 200 | 101.43 ± 4.12 | 106.40 ± 4.32 | |
| 800 | 97.37 ± 0.06 | 97.22 ± 0.06 | |
| Stomach | 10 | 95.23 ± 6.38 | 104.73 ± 4.88 |
| 200 | 95.80 ± 1.00 | 110.74 ± 1.15 | |
| 800 | 100.02 ± 2.31 | 114.25 ± 2.68 | |
| Intestine | 10 | 80.81 ± 4.82 | 90.91 ± 0.83 |
| 200 | 91.90 ± 2.06 | 94.27 ± 4.45 | |
| 800 | 82.95 ± 0.61 | 98.07 ± 3.48 | |
| Bile | 10 | 78.92 ± 7.15 | 42.86 ± 2.43 |
| 200 | 75.52 ± 5.12 | 41.36 ± 0.87 | |
| 800 | 76.98 ± 5.21 | 39.73 ± 7.19 | |
| Urine | 10 | 90.42 ± 7.60 | 85.86 ± 6.40 |
| 200 | 86.15 ± 1.34 | 83.17 ± 1.76 | |
| 800 | 96.66 ± 3.30 | 82.95 ± 1.05 | |
| Feces | 10 | 94.82 ± 2.46 | 104.27 ± 3.82 |
| 200 | 98.97 ± 3.65 | 98.62 ± 2.83 | |
| 800 | 97.74 ± 5.69 | 100.37 ± 9.68 |
| Sample | Analyte Concentration (ng/mL) | Autosampler (12 h, 20 °C, Mean ± SD, %) | Room Temperature (4 h, mean ± SD, %) # | Three Freeze/ Thaw Cycles (Mean ± SD, %) # | Long-Term (30 Days, −80 °C, Mean ± SD, %) # |
|---|---|---|---|---|---|
| Plasma | 10 | 90.18 ± 6.86 | 106.98 ± 2.86 | 105.96 ± 3.61 | 101.04 ± 6.64 |
| 200 | 95.39 ± 7.51 | 112.08 ± 0.90 | 109.78 ± 4.25 | 111.33 ± 2.91 | |
| 800 | 96.21 ± 6.64 | 90.91 ± 2.29 | 102.05 ± 3.01 | 97.89 ± 1.67 | |
| Heart | 10 | 87.65 ± 6.72 | 91.82 ± 1.13 a | 86.38 ± 1.20 | 103.89 ± 1.96 |
| 200 | 93.75 ± 1.08 | 86.73 ± 19.03 a | 105.75 ± 6.15 | 110.35 ± 3.29 | |
| 800 | 108.92 ± 0.51 | 87.81 ± 1.19 a | 97.80 ± 0.54 | 98.17 ± 0.42 | |
| Liver | 10 | 100.21 ± 9.65 | 102.35 ± 24.01 b | 90.44 ± 10.00 | 103.27 ± 2.04 |
| 200 | 98.76 ± 1.48 | 98.35 ± 0.13 b | 101.54 ± 0.36 | 94.91 ± 2.41 | |
| 800 | 85.58 ± 3.80 | 99.45 ± 7.97 b | 92.32 ± 5.20 | 86.91 ± 1.67 | |
| Brain | 10 | 86.65 ± 0.65 | 86.85 ± 4.01 | 87.34 ± 9.15 | 90.55 ± 9.21 |
| 200 | 108.93 ± 2.64 | 99.83 ± 0.89 | 113.68 ± 0.54 | 110.96 ± 1.63 | |
| 800 | 103.42 ± 1.09 | 98.50 ± 3.54 | 103.28 ± 3.76 | 103.52 ± 1.07 | |
| Spleen | 10 | 111.72 ± 7.09 | 92.13 ± 9.72 b | 106.22 ± 4.62 | 100.58 ± 4.46 |
| 200 | 94.37 ± 1.20 | 98.17 ± 4.63 b | 101.32 ± 0.89 | 102.60 ± 1.34 | |
| 800 | 102.59 ± 3.48 | 96.85 ± 1.65 b | 98.89 ± 3.23 | 102.10 ± 1.26 | |
| Lungs | 10 | 104.85 ± 4.39 | 89.86 ± 1.96 b | 99.66 ± 13.91 | 86.66 ± 10.88 |
| 200 | 102.64 ± 3.69 | 87.24 ± 1.24 b | 96.43 ± 4.28 | 94.10 ± 2.16 | |
| 800 | 90.34 ± 0.78 | 86.51 ± 3.78 b | 91.69 ± 0.80 | 88.74 ± 0.84 | |
| Kidney | 10 | 85.46 ± 1.56 | 92.72 ± 2.23 a | 91.72 ± 10.85 | 95.12 ± 6.87 |
| 200 | 101.37 ± 0.45 | 94.73 ± 1.85 a | 102.64 ± 2.14 | 93.83 ± 1.46 | |
| 800 | 96.69 ± 0.92 | 86.85 ± 0.53 a | 97.67 ± 1.37 | 95.22 ± 0.74 | |
| Stomach | 10 | 100.23 ± 0.32 | 86.21 ± 3.67 a | 85.03 ± 2.29 | 86.16 ± 5.14 |
| 200 | 105.21 ± 1.69 | 86.08 ± 9.96 a | 99.07 ± 3.83 | 85.53 ± 3.05 | |
| 800 | 88.90 ± 0.75 | 85.46 ± 8.89 a | 90.66 ± 1.24 | 96.97 ± 5.77 | |
| Intestine | 10 | 98.57 ± 2.18 | 101.25 ± 9.02 a | 104.14 ± 3.61 | 94.96 ± 3.47 |
| 200 | 104.19 ± 1.17 | 98.90 ± 1.51 a | 92.55 ± 1.47 | 99.91 ± 1.46 | |
| 800 | 101.13 ± 1.06 | 89.16 ± 2.78 a | 95.55 ± 0.51 | 99.35 ± 1.28 | |
| Bile | 10 | 88.51 ± 3.93 | 89.00 ± 7.70 | 92.34 ± 12.00 | 85.61 ± 5.23 |
| 200 | 98.53 ± 1.23 | 105.37 ± 4.67 | 88.76 ± 1.43 | 104.95 ± 2.91 | |
| 800 | 87.08 ± 1.72 | 87.13 ± 3.38 | 89.22 ± 2.85 | 96.97 ± 2.09 | |
| Urine | 10 | 86.36 ± 4.20 | 89.14 ± 11.04 a | 103.46 ± 4.15 | 95.21 ± 3.14 |
| 200 | 85.93 ± 1.33 | 100.78 ± 2.01 a | 95.55 ± 1.38 | 85.15 ± 1.25 | |
| 800 | 95.12 ± 0.76 | 87.80 ± 9.98 a | 91.00 ± 0.13 | 107.43 ± 0.64 | |
| Feces | 10 | 95.15 ± 6.64 | 95.79 ± 12.71 b | 94.65 ± 6.23 | 113.83 ± 4.19 |
| 200 | 99.11 ± 1.28 | 94.84 ± 4.27 b | 114.04 ± 13.81 | 85.20 ± 4.47 | |
| 800 | 93.67 ± 2.55 | 90.58 ± 1.03 b | 97.56 ± 3.69 | 93.90 ± 0.97 |
| PK Parameters | Unit | i.v. (mg/kg) | i.g. (mg/kg) | |
|---|---|---|---|---|
| 2 | 20 | 40 | ||
| AUC0–t | h·ng/mL | 111.13 ± 39.71 | 27.14 ± 2.02 | 131.60 ± 33.12 |
| AUC0–∞ | h·ng/mL | 158.75 ± 95.78 | 29.83 ± 2.14 | 133.36 ± 33.20 |
| Cmax | ng/mL | 128.24 ± 15.32 | 60.22 ± 12.53 | 308.25 ± 103.86 |
| Tmax | h | 0.08 ± 0.00 | 0.08 ± 0.00 | 0.08 ± 0.00 |
| t1/2 | h | 5.57 ± 0.83 | 4.26 ± 1.48 | 3.14 ± 0.42 |
| MRT0–∞ | h | 5.13 ± 2.91 | 4.13 ± 1.35 | 1.13 ± 0.40 |
| Bioavailability | % | - | 2.44 | 5.92 |
| PK Parameters | Unit | i.v. (mg/kg) | i.g. (mg/kg) |
|---|---|---|---|
| 2 | 40 | ||
| AUC0–t | h·ng/mL | 226.16 ± 28.25 | 202.26 ± 14.02 |
| AUC0–∞ | h·ng/mL | 343.51 ± 34.15 | 264.61 ± 25.01 |
| Cmax | ng/mL | 94.50 ± 17.45 | 177.15 ± 11.73 |
| Tmax | h | 0.08 ± 0.00 | 0.08 ± 0.00 |
| t1/2 | h | 6.80 ± 1.31 | 4.10 ± 0.81 |
| MRT0–∞ | h | 10.54 ± 2.15 | 5.29 ± 1.30 |
| Bioavailability | % | - | 4.47 |
| Matrix | Rats (t = 240 min) | Mice (t = 480 min) |
|---|---|---|
| Heart | 12.65 | 0.74 |
| Liver | 7.66 | 15.17 |
| Brain | 3.00 | 0.39 |
| Spleen | 5.07 | 2.87 |
| Lung | 4.37 | 5.65 |
| Kidney | 7.76 | 10.66 |
| Stomach | 612.73 | 81.00 |
| Intestine | 43.36 | 202.98 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, J.; Zhang, Q.; Chen, Y.; Lu, C.; Tong, Y. Pharmacokinetics, Tissue Distribution and Excretion of Demethyleneberberine, a Metabolite of Berberine, in Rats and Mice. Molecules 2023, 28, 7725. https://doi.org/10.3390/molecules28237725
Li J, Zhang Q, Chen Y, Lu C, Tong Y. Pharmacokinetics, Tissue Distribution and Excretion of Demethyleneberberine, a Metabolite of Berberine, in Rats and Mice. Molecules. 2023; 28(23):7725. https://doi.org/10.3390/molecules28237725
Chicago/Turabian StyleLi, Jingqi, Qi Zhang, Yutong Chen, Chengyu Lu, and Yongbin Tong. 2023. "Pharmacokinetics, Tissue Distribution and Excretion of Demethyleneberberine, a Metabolite of Berberine, in Rats and Mice" Molecules 28, no. 23: 7725. https://doi.org/10.3390/molecules28237725
APA StyleLi, J., Zhang, Q., Chen, Y., Lu, C., & Tong, Y. (2023). Pharmacokinetics, Tissue Distribution and Excretion of Demethyleneberberine, a Metabolite of Berberine, in Rats and Mice. Molecules, 28(23), 7725. https://doi.org/10.3390/molecules28237725