
Apricot Kernel Extract and Amygdalin Inhibit Urban Particulate Matter-Induced Keratoconjunctivitis Sicca


 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Results
2.1. HPLC Analysis of AKE
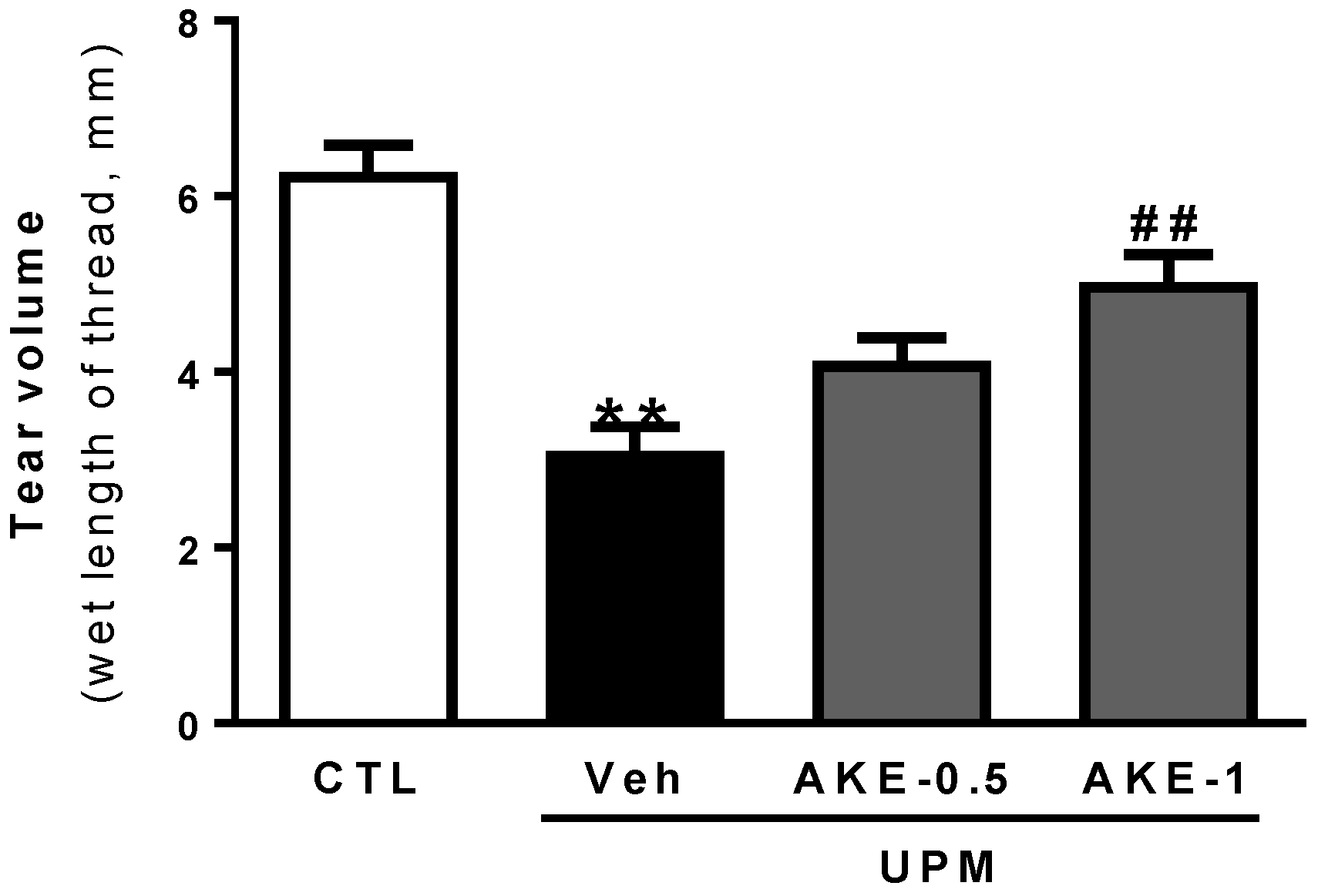
2.2. Effects of AKE on Tear Secretion
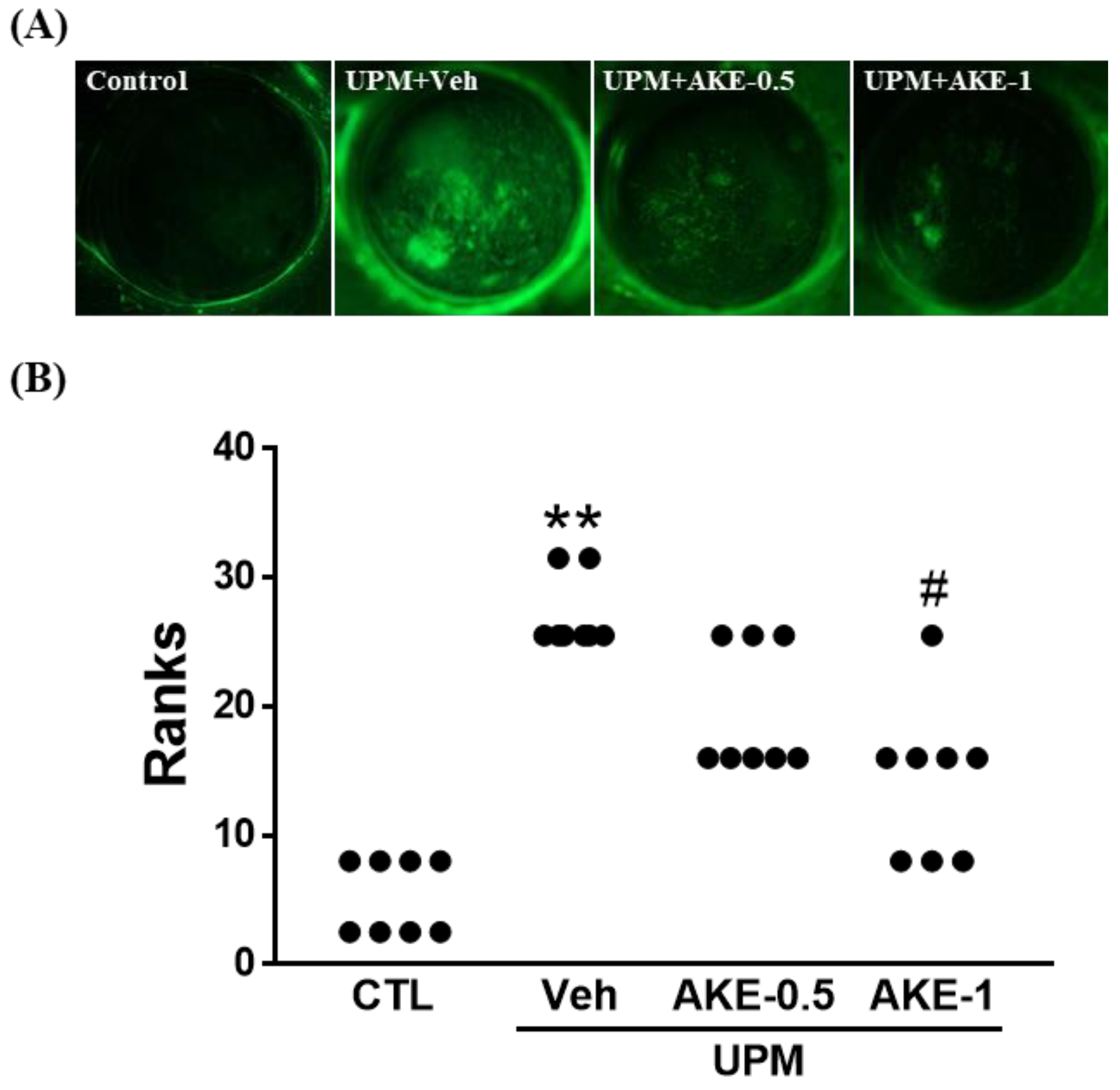
2.3. Effects of AKE on Corneal Epithelial Damage
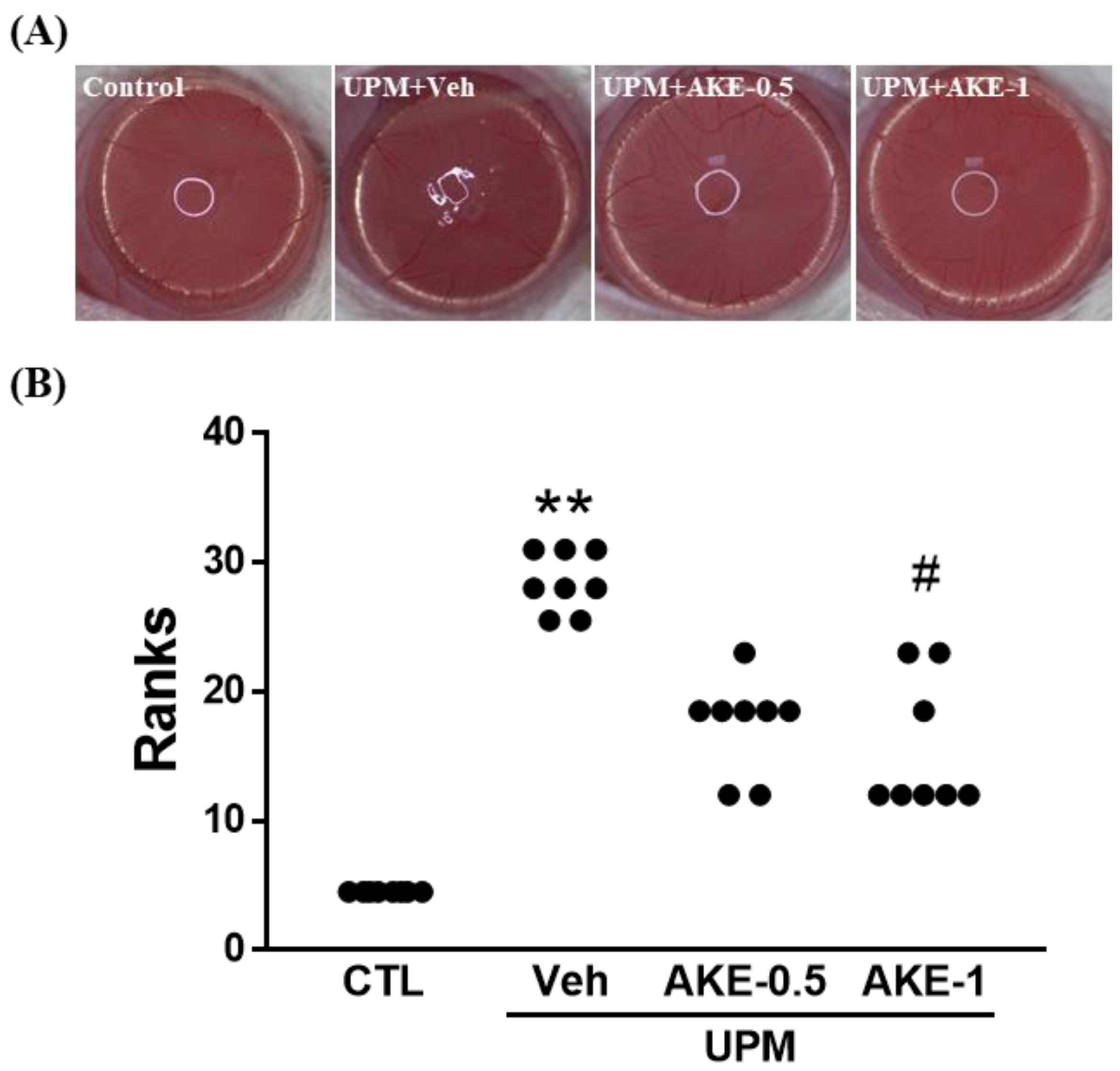
2.4. Effects of AKE on Corneal Irregularity
2.5. Effects of AKE on Mucin Integrity
2.6. Effects of AKE and Amygdalin on Matrix Metalloproteinases (MMP)
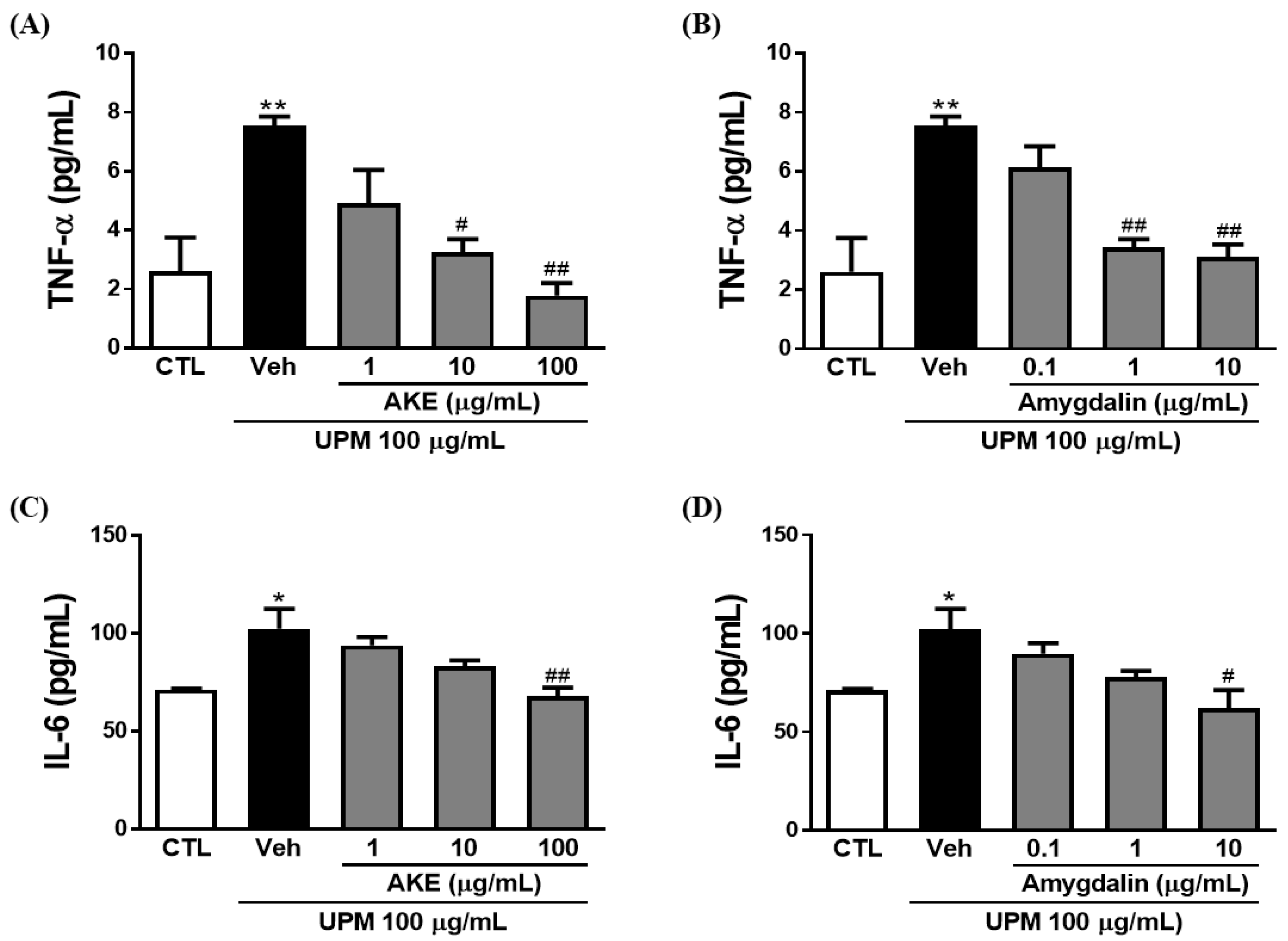
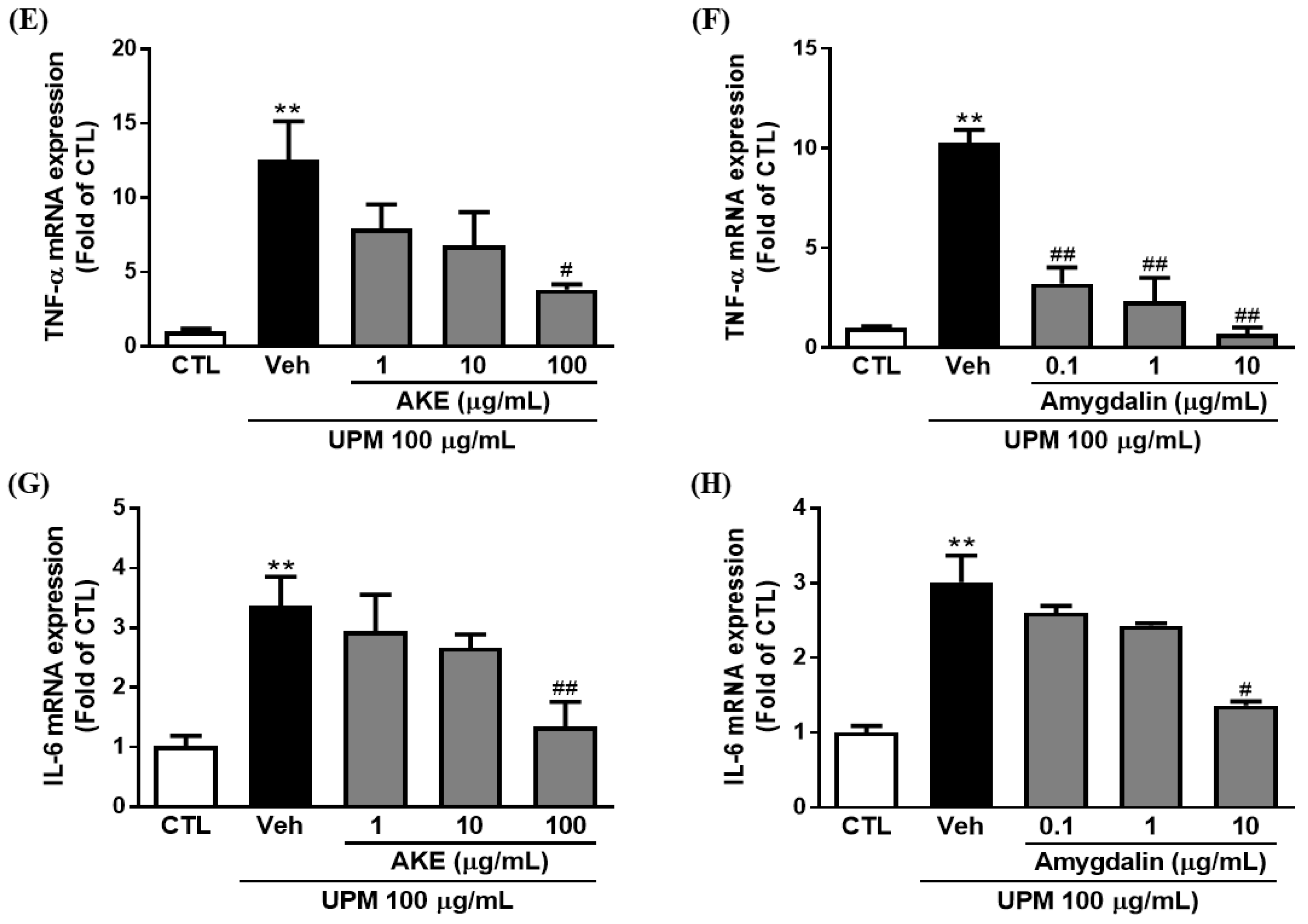
2.7. Effects of AKE and Amygdalin on Inflammation
3. Discussion
4. Materials and Methods
4.1. Materials
4.2. Preparation of AKE
4.3. Animals and Experimental Design
4.4. Phenol Red Thread Tear Test
4.5. Fluorescein Staining Score
4.6. Irregularity Score
4.7. Immunohistochemistry
4.8. Cell Culture
4.9. Detection of MMP Activity
4.10. Detection of Inflammatory Factors
4.11. Quantitative Polymerase Chain Reaction (qPCR)
4.12. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Michael, A.L.; Christophe, B.; Jules, B.; Murat, D.; Gary, N.F.; Shigeru, K.; Peter, L.; James, M.; Juan, M.; Stephen, C.P.; et al. The definition and classification of dry eye disease: Report of the definition and classification subcommittee of the international dry eye workshop (2007). Ocul. Surf. 2007, 5, 75–92. [Google Scholar]
- Yu, G.Y.; Zhu, Z.H.; Mao, C.; Cai, Z.G.; Zou, L.H.; Lu, L.; Zhang, L.; Peng, X.; Li, N.; Huang, Z. Microvascular autologous submandibular gland transfer in severe cases of keratoconjunctivitis sicca. Int. J. Oral Maxillofac. Surg. 2004, 33, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Gipson, I.K. The ocular surface: The challenge to enable and protect vision: The Friedenwald lecture. Invest. Ophthalmol. Vis. Sci. 2007, 48, 4390–4398. [Google Scholar] [CrossRef] [PubMed]
- Janine, A.S.; Julie, A.; Carolyn, B.; Barbara, C.; Kelly, N.; Debra, S.; Oliver, S. The epidemiology of dry eye disease: Report of the epidemiology subcommittee of the international dry eye workshop (2007). Ocul. Surf. 2007, 5, 93–107. [Google Scholar]
- Schwartz, J. Air pollution and daily mortality: A review and meta analysis. Environ. Res. 1994, 64, 36–52. [Google Scholar] [CrossRef] [PubMed]
- Chen, I.C.; Huang, H.H.; Chen, P.F.; Chiang, H.C. Sirtuin 3 protects against urban particulate matter-induced autophagy in human bronchial epithelial cells. Toxicol. Sci. 2016, 152, 113–127. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.C.; Li, Z.; Harder, S.D.; Soukup, J.M. Apoptotic and inflammatory effects induced by different particles in human alveolar macrophages. Inhal. Toxicol. 2004, 16, 863–878. [Google Scholar] [CrossRef] [PubMed]
- Obot, C.J.; Morandi, M.T.; Beebe, T.P.; Hamilton, R.F.; Holian, A. Surface components of airborne particulate matter induce macrophage apoptosis through scavenger receptors. Toxicol. Appl. Pharmacol. 2002, 184, 98–106. [Google Scholar] [CrossRef]
- Soukup, J.M.; Becker, S. Human alveolar macrophage responses to air pollution particulates are associated with insoluble components of coarse material, including particulate endotoxin. Toxicol. Appl. Pharmacol. 2001, 171, 20–26. [Google Scholar] [CrossRef]
- Li, J.; Tan, G.; Ding, X.; Wang, Y.; Wu, A.; Yang, Q.; Ye, L.; Shao, Y. A mouse dry eye model induced by topical administration of the air pollutant particulate matter 10. Biomed. Pharmacother. 2017, 960, 524–534. [Google Scholar] [CrossRef]
- Kim, C.S.; Jo, K.; Lee, I.S.; Kim, J. Topical application of apricot kernel extract improves dry eye symptoms in a unilateral exorbital lacrimal gland excision mouse. Nutrients 2016, 8, 750. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.K.; Yang, H.Y.; Lee, T.H.; Shin, M.C.; Lee, M.H.; Shin, M.S.; Kim, C.J.; Kim, O.J.; Hong, S.P.; Cho, S. Armeniacae semen extract suppresses lipopolysaccharide-induced expressions of cycloosygenase-2 and inducible nitric oxide synthase in mouse BV2 microglial cells. Biol. Pharm. Bull. 2005, 28, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Hwang, D.-R.; Kang, Y.-S.; Kim, S.-S.; Kim, D.-H.; Shin, M.-K.; Song, H.-J. Studies on the allergic asthma effect of semen armeniaceae amarum. Kor. J. Herbology 2003, 18, 201–201. [Google Scholar]
- Zhang, J.; Gu, H.D.; Zhang, L.; Tian, Z.J.; Zhang, Z.Q.; Shi, X.C.; Ma, W.H. Protective effects of apricot kernel oil on myocardium against ischemia-reperfusion injury in rats. Food Chem. Toxicol. 2011, 49, 3136–3141. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.H.; Ahn, J.H.; Kwon, A.R.; Lee, E.S.; Kwak, J.H.; Min, Y.H. Chemical composition and antimicrobial activity of the essential oil of apricot seed. Phytother. Res. 2014, 28, 1867–1872. [Google Scholar] [CrossRef] [PubMed]
- Yigit, D.; Yigit, N.; Mavi, A. Antioxidant and antimicrobial activities of bitter and sweet apricot (Prunus armeniaca L.) kernels. Braz. J. Med. Biol. Res. 2009, 42, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D.; Franklin, B.; Cascio, W.; Hong, Y.; Howard, G.; Lipsett, M.; Luepker, R.; Mittleman, M.; Samet, J.; Smith, S.C.; et al. Air pollution and cardiovascular disease: A statement for healthcare professionals from the Expert Panel on Population and Prevention Science of the American Heart Association. Circulation 2004, 109, 2655–2671. [Google Scholar] [CrossRef]
- Ball, B.R.; Smith, K.R.; Veranth, J.M.; Aust, A.E. Bioavailability of iron from coal fly ash: Mechanisms of mobilization and of biological effects. Inhal. Toxicol. 2000, 12, 209–225. [Google Scholar] [CrossRef]
- Mitkus, R.J.; Powell, J.L.; Zeisler, R.; Squibb, K.S. Comparative physicochemical and biological characterization of NIST Interim Reference Material PM2.5 and SRM 1648 in human A549 and mouse RAW264.7 cells. Toxicol. In Vitro 2013, 27, 2289–2298. [Google Scholar] [CrossRef]
- Smith, K.R.; Aust, A.E. Mobilization of iron from urban particulates leads to generation of reactive oxygen species in vitro and induction of ferritin synthesis in human lung epithelial cells. Chem. Res. Toxicol. 1997, 10, 828–834. [Google Scholar] [CrossRef]
- Shoenfelt, J.; Mitkus, R.J.; Zeisler, R.; Spatz, R.O.; Powell, J.; Fenton, M.J.; Squibb, K.A.; Medvedev, A.E. Involvement of TLR2 and TLR4 in inflammatory immune responses induced by fine and coarse ambient air particulate matter. J. Leukoc. Biol. 2009, 86, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Mantelli, F.; Massaro-Giordano, M.; Macchi, I.; Lambiase, A.; Bonini, S. The cellular mechanisms of dry eye: From pathogenesis to treatment. J. Cell Physiol. 2013, 228, 2253–2256. [Google Scholar] [CrossRef] [PubMed]
- Chotikavanich, S.; de Paiva, C.S.; Li de, Q.; Chen, J.J.; Bian, F.; Farley, W.J.; Pflugfelder, S.C. Production and activity of matrix metalloproteinase-9 on the ocular surface increase in dysfunctional tear syndrome. Invest. Ophthalmol. Vis. Sci. 2009, 50, 3203–3209. [Google Scholar] [CrossRef] [PubMed]
- Pflugfelder, S.C.; Farley, W.; Luo, L.; Chen, L.Z.; de Paiva, C.S.; Olmos, L.C.; Li, D.Q.; Fini, M.E. Matrix metalloproteinase-9 knockout confers resistance to corneal epithelial barrier disruption in experimental dry eye. Am. J. Pathol. 2005, 166, 61–71. [Google Scholar] [CrossRef]
- Park, B.; Lee, I.S.; Hyun, S.W.; Jo, K.; Lee, T.G.; Kim, J.S.; Kim, C.S. The protective effect of polygonum cuspidatum (PCE) aqueous extract in a dry eye model. Nutrients 2018, 10, 1550. [Google Scholar] [CrossRef] [PubMed]
- Dartt, D.A. Regulation of mucin and fluid secretion by conjunctival epithelial cells. Prog. Retin. Eye Res. 2002, 21, 555–576. [Google Scholar] [CrossRef]
- Tsubota, K. Understanding dry eye syndrome. Adv. Exp. Med. Biol. 2002, 506 Pt A, 3–16. [Google Scholar]
- Zhang, X.; M, V.J.; Qu, Y.; He, X.; Ou, S.; Bu, J.; Jia, C.; Wang, J.; Wu, H.; Liu, Z.; et al. Dry eye management: Targeting the ocular surface microenvironment. Int. J. Mol. Sci. 2017, 18, 1398. [Google Scholar] [CrossRef]
- Johnson, M.E.; Murphy, P.J. Changes in the tear film and ocular surface from dry eye syndrome. Prog. Retin. Eye Res. 2004, 23, 449–474. [Google Scholar] [CrossRef]
- Ablamowicz, A.F.; Nichols, J.J. Ocular surface membrane-associated mucins. Ocul. Surf. 2016, 14, 331–341. [Google Scholar] [CrossRef]
- Corrales, R.M.; Narayanan, S.; Fernandez, I.; Mayo, A.; Galarreta, D.J.; Fuentes-Paez, G.; Chaves, F.J.; Herreras, J.M.; Calonge, M. Ocular mucin gene expression levels as biomarkers for the diagnosis of dry eye syndrome. Invest. Ophthalmol. Vis. Sci. 2011, 52, 8363–8369. [Google Scholar] [CrossRef] [PubMed]
- Enriquez-de-Salamanca, A.; Bonini, S.; Calonge, M. Molecular and cellular biomarkers in dry eye disease and ocular allergy. Curr. Opin. Allergy Clin. Immunol. 2012, 12, 523–533. [Google Scholar] [CrossRef] [PubMed]
- Imbert, Y.; Darling, D.S.; Jumblatt, M.M.; Foulks, G.N.; Couzin, E.G.; Steele, P.S.; Young, W.W. MUC1 splice variants in human ocular surface tissues: Possible differences between dry eye patients and normal controls. Exp. Eye Res. 2006, 83, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Gipson, I.K.; Spurr-Michaud, S.J.; Senchyna, M.; Ritter, R.; Schaumberg, D. Comparison of mucin levels at the ocular surface of postmenopausal women with and without a history of dry eye. Cornea 2011, 30, 1346–1352. [Google Scholar] [CrossRef] [PubMed]
- Caffery, B.; Heynen, M.L.; Joyce, E.; Jones, L.; Ritter, R.; Senchyna, M. MUC1 expression in Sjogren’s syndrome, KCS, and control subjects. Mol. Vis. 2010, 16, 1720–1727. [Google Scholar] [PubMed]
- Berry, M.; Pult, H.; Purslow, C.; Murphy, P.J. Mucins and ocular signs in symptomatic and asymptomatic contact lens wear. Optom. Vis. Sci. 2008, 85, E930–E938. [Google Scholar] [CrossRef] [PubMed]
- Dogru, M.; Okada, N.; Asano-Kato, N.; Tanaka, M.; Igarashi, A.; Takano, Y.; Fukagawa, K.; Shimazaki, J.; Tsubota, K.; Fujishima, H. Atopic ocular surface disease: Implications on tear function and ocular surface mucins. Cornea 2005, 24, S18–S23. [Google Scholar] [CrossRef]
- Albertsmeyer, A.C.; Kakkassery, V.; Spurr-Michaud, S.; Beeks, O.; Gipson, I.K. Effect of pro-inflammatory mediators on membrane-associated mucins expressed by human ocular surface epithelial cells. Exp. Eye Res. 2010, 90, 444–451. [Google Scholar] [CrossRef]
- Nabavizadeh, F.; Alizadeh, A.M.; Sadroleslami, Z.; Adeli, S. Gastroprotective effects of amygdalin on experimental gastric ulcer: Role of NO and TNF. J. Med. Plants Res. 2011, 5, 3122–3127. [Google Scholar]
- Capper, R.; Guo, L.; Pearson, J.P.; Birchall, J.P. Effect of nitric oxide donation on mucin production in vitro. Clin. Otolaryngol. Allied Sci. 2003, 28, 51–54. [Google Scholar] [CrossRef]







© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hyun, S.-W.; Kim, J.; Park, B.; Jo, K.; Lee, T.G.; Kim, J.S.; Kim, C.-S. Apricot Kernel Extract and Amygdalin Inhibit Urban Particulate Matter-Induced Keratoconjunctivitis Sicca. Molecules 2019, 24, 650. https://doi.org/10.3390/molecules24030650
Hyun S-W, Kim J, Park B, Jo K, Lee TG, Kim JS, Kim C-S. Apricot Kernel Extract and Amygdalin Inhibit Urban Particulate Matter-Induced Keratoconjunctivitis Sicca. Molecules. 2019; 24(3):650. https://doi.org/10.3390/molecules24030650
Chicago/Turabian StyleHyun, Soo-Wang, Junghyun Kim, Bongkyun Park, Kyuhyung Jo, Tae Gu Lee, Jin Sook Kim, and Chan-Sik Kim. 2019. "Apricot Kernel Extract and Amygdalin Inhibit Urban Particulate Matter-Induced Keratoconjunctivitis Sicca" Molecules 24, no. 3: 650. https://doi.org/10.3390/molecules24030650
APA StyleHyun, S.-W., Kim, J., Park, B., Jo, K., Lee, T. G., Kim, J. S., & Kim, C.-S. (2019). Apricot Kernel Extract and Amygdalin Inhibit Urban Particulate Matter-Induced Keratoconjunctivitis Sicca. Molecules, 24(3), 650. https://doi.org/10.3390/molecules24030650