Ivabradine: An Intelligent Drug for the Treatment of Ischemic Heart Disease

{kind=link}
Abstract
:List of Abbreviations
| CSAP | Chronic stable angina pectoris |
| HR | Heart rate |
| BP | Blood pressure |
| CBF | Coronary blood flow |
| CVD | Cardiovascular disease |
| CAD | Coronary artery disease |
| SAN | Sino atrial node |
| LVEF | Left ventricular ejection fraction |
| CHF | Chronic heart failure |
| IVA | Ivabradine |
1. Introduction
2. Generation of Electrical Impulse and Role of If Current
3. Pharmacokinetics and Pharmacodynamics of Ivabradine
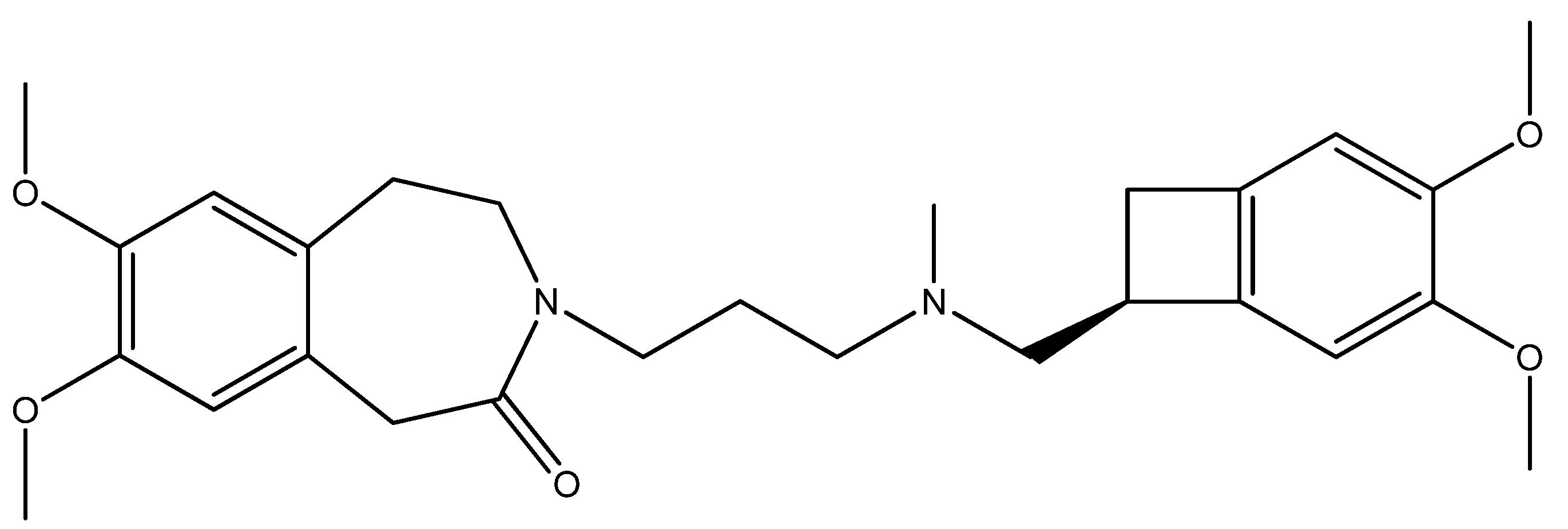
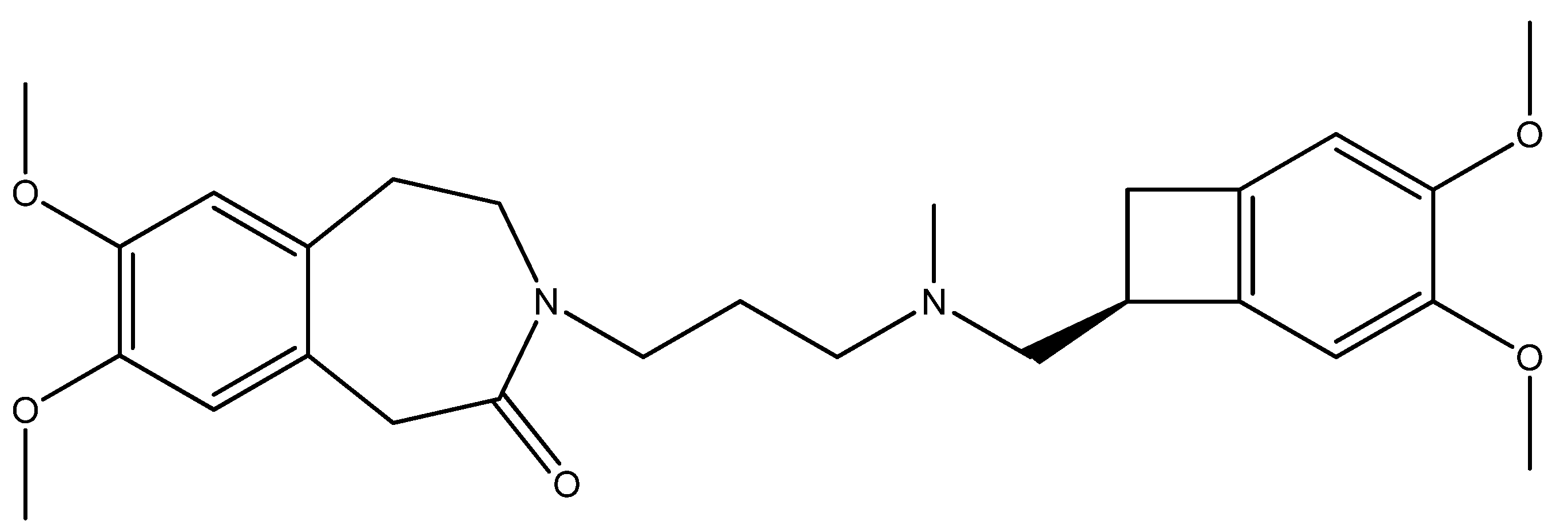
3.1. Chemical Structure
3.2. Activity
3.3. Relationship
4. Safety and Tolerability
4.1. Phosphenes
4.2. Bradycardia and Conduction/Rhythm Disturbances
4.3. QT Interval
4.4. Interactions with Other Drugs
5. Antianginal and Antischemic Effects
6. HR Control in Myocardial Infarction and Cardiogenic Shock
7. Conclusions
Conflict of Interest
References
- Morrow, D.A.; Gersh, B.E.; Braunwald, E. Braunwald’s Heart Disease, 7th ed; Elsevier Saunders: Philadelphia, PA, USA, 2005; pp. 1281–1282. [Google Scholar]
- O’Rourke, R.A.; O’Gara, P.; Douglas, J.S. Diagnosis and Management of Patients with Chronic Ischemic Heart Disease. In Hurst’s The Heart, 11th ed; McGraw Hill Medical Publishing Division: New York, NY, USA, 2004; pp. 1465–1472. [Google Scholar]
- Kones, R.A. Recent advances in the management of chronic stable angina I: Approach to the patients, diagnosis, pathophysiology, risk stratification and gender disparities. Vasc. Health Risk Manag. 2010, 6, 635–656. [Google Scholar] [CrossRef]
- Kaski, J.C.; Arrebola-Moreno, A.; Dungu, J. Treatment strategies for chronic stable angina. Expert Opin. Pharmacother. 2011, 12, 2833–2844. [Google Scholar] [CrossRef]
- Barbuti, A.; Baruscotti, M.; DiFrancesco, D. The pacemaker current: From basics to the clinics. J. Cardiovasc. Electrophysiol. 2007, 18, 342–347. [Google Scholar] [CrossRef]
- Postea, O.; Biel, M. Exploring HCNchannels as novel drug targets. Nat. Rev. Drug Discov. 2011, 10, 903–914. [Google Scholar]
- Biel, M.; Schneider, A.; Wahl, C. Cardiac HCN channels: Structure, function, and modulation. Trends Cardiovasc. Med. 2002, 12, 206–212. [Google Scholar] [CrossRef]
- Reid, C.A.; Phillips, A.M.; Petrou, S. HCN channelopathies: Pathophysiology in genetic epilepsy and therapeutic implications. Br. J. Pharmacol. 2012, 165, 49–56. [Google Scholar] [CrossRef]
- DiFrancesco, D. The role of the funny current in pacemaker activity. Circ. Res. 2010, 106, 434–446. [Google Scholar] [CrossRef]
- DiFrancesco, D. Funny channel-based pacemaking. Heart Rhythm 2010, 7, 276–279. [Google Scholar] [CrossRef]
- Baruscotti, M.; Barbuti, A.; Bucchi, A. The cardiac pacemaker current. J. Mol. Cell. Cardiol. 2010, 48, 55–64. [Google Scholar] [CrossRef]
- DiFrancesco, D.; Borer, J.S. The funny current: Cellular basis for the control of heart rate. Drugs 2007, 67, 15–24. [Google Scholar] [CrossRef]
- Thollon, C.; Bedut, S.; Villeneuve, N. Use-dependent inhibition of hHCN4 by ivabradine and relationship with reduction in pacemaker activity. Br. J. Pharmacol. 2007, 150, 37–46. [Google Scholar]
- Baruscotti, M.; Bottelli, G.; Milanesi, R.; DiFrancesco, J.C.; DiFrancesco, D. HCN-related channelopathies. Pflug. Arch. Eur. J. Physiol. 2010, 460, 405–415. [Google Scholar] [CrossRef]
- Biel, M.; Wahl-Schott, C.; Michalakis, S.; Zong, X. Hyperpolarization-activated cation channels: From genes to function. Physiol. Rev. 2009, 89, 847–885. [Google Scholar] [CrossRef]
- Wahl-Schott, C.; Biel, M. HCN channels: Structure, cellular regulation and physiological function. Cell. Mol. Life Sci. 2009, 66, 470–494. [Google Scholar] [CrossRef]
- Scicchitano, P.; Carbonara, S.; Ricci, G.; Mandurino, C.; Locorotondo, M.; Bulzis, G.; Gesualdo, M.; Zito, A.; Carbonara, R.; Dentamaro, I.; et al. HCN channels and heart rate. Molecules 2012, 17, 4225–4235. [Google Scholar] [CrossRef]
- DiFrancesco, D.; Tromba, C. Acetylcholine inhibits activation of the cardiac hyperpolarizing-activated current If. Pflug. Arch. Eur. J. Physiol. 1998, 410, 139–142. [Google Scholar] [CrossRef]
- DiFrancesco, D.; Tromba, C. Muscarinic control of the hyperpolarization-activated current (If) in rabbit sino-atrial node myocytes. J. Physiol. 1988, 405, 493–510. [Google Scholar]
- Summary of Product Characteristics. Procoralan™ (ivabradine hydrochloride). Servier Laboratories Ltd.: Cedex, France, October 2005. Available online: http://emc.medicines.org.uk (accessed on 27 November 2005).
- European Public Assessment Report (EPAR): Scientific discussion for Procoralan. EMEA, London, UK, 17 November 2005; Available online: http://www.emea.eu.int (accessed on 18 November 2005).
- Simon, L.; Ghaleh, B.; Puybasset, L.; Giudicelli, J.F.; Berdeaux, A. Coronary and haemodynamic effects of S16257, a new bradycardic agents, in resting and exercising conscious dogs. J. Pharmacol. Exp. Ther. 1995, 275, 579–586. [Google Scholar]
- Ragueneau, I.; Laveillem, C.; Jochemsen, R.; Resplandy, G.; Funck-Brentano, C.; Jaillon, P. Pharmacokinetic—pharmacodynamic modelling of the effects of ivabradine, a direct sinus node inhibitor, on heart rate in healthy volunteers. Clin. Pharmacol. Ther. 1998, 64, 192–203. [Google Scholar] [CrossRef]
- DiFrancesco, D. The contribution of pacemaker current (if) to generation of spontaneous activity in rabbit sino-atrial node myocytes. J. Physiol. 1991, 34, 23–40. [Google Scholar]
- DiFrancesco, D. If inhibition: A novel mechanism of action. Eur. Heart J. Suppl. 2003, 5, 19–25. [Google Scholar] [CrossRef]
- Tardif, J.C.; O’Meara, E.; Komajda, M.; Böhm, M.; Borer, J.S.; Ford, I.; Tavazzi, L.; Swedberg, K. SHIFT Investigators. Effects of selective heart rate reduction with ivabradine on left ventricular remodelling and function: Results from the SHIFT echocardiography substudy. Eur. Heart J. Suppl. 2011, 32, 2507–2515. [Google Scholar]
- Brown, H.F.; DiFrancesco, D.; Noble, S.J. How does adrenaline accelerate the heart? Nature 1979, 280, 235–236. [Google Scholar]
- VanBogaert, P.P.; Goethals, M.; Simoens, C. Use and frequency-dependent blockade by UL-FS 49 of the I(f) pacemaker current in sheep cardiac Purkinie fibres. Eur. J. Pharmacol. 1990, 187, 241–256. [Google Scholar] [CrossRef]
- Franke, H.; Su, C.A.; Schumacher, K.; Seiberling, M. Clinical pharmacology of two specific bradycardiac agents. Eur. Heart J. 1987, 8, 91–98. [Google Scholar]
- Kobinger, W.; Lillie, C.; Pichler, L. N-allyl-derivative of clonidine, a substance with specific bradycardic action at a cardiac site. Naunyn Schmiedebergs Arch. Pharmacol. 1979, 306, 255–262. [Google Scholar] [CrossRef]
- BoSmith, R.E.; Briggs, I.; Sturgess, N.C. Inhibitory actions of ZENECA ZD7288 on whole-cell hyperpolarization activated inward current (If) in guinea-pig dissociated sinoatrial node cells. Br. J. Pharmacol. 1993, 110, 343–349. [Google Scholar] [CrossRef]
- Savelieva, I.; Camm, A.J. If inhibition with ivabradine: Electrophysiological effects and safety. Drug Saf. 2008, 31, 95–107. [Google Scholar] [CrossRef]
- Koester, R.; Kaehler, J.; Meinertz, T. Ivabradine for the treatment of stable angina pectoris in octogenarians. Clin. Res. Cardiol. 2011, 100, 121–128. [Google Scholar] [CrossRef]
- Riccioni, G. Ivabradine: Recent and potential applications in clinical practice. Expert Opin. Pharmacother. 2011, 12, 443–450. [Google Scholar] [CrossRef]
- Savalieva, I.; Camm, A.J. Novel If current inhibitor ivabradine: Safety considerations. Adv.Cardiol. 2006, 43, 79–96. [Google Scholar]
- Swedberg, K.; Komajda, M.; Böhm, M.; Borer, J.S.; Ford, I.; Dubost-Brama, A.; Lerebours, G.; Tavazzi, L. SHIFT Investigators. Ivabradine and outcomes in chronic heart failure (SHIFT): A randomised placebo-controlled study. Lancet 2010, 376, 875–885. [Google Scholar]
- Riccioni, G. Focus on ivabradine. Expert Rev. Cardiovasc. Ther. 2009, 7, 107–113. [Google Scholar] [CrossRef]
- Cervetto, L.; Demontis, G.C.; Gargini, C. Cellular mechanisms underlying the pharmacological induction of phosphenes. Br. J. Pharmacol. 2007, 150, 383–390. [Google Scholar]
- Canet, E.; Lerebours, G.; Vilaine, J.P. Innovation in coronary artery disease and heart failure: Clinical benefits of pure heart rate reduction with ivabradine. Ann. N. Y. Acad. Sci. 2011, 1222, 90–99. [Google Scholar] [CrossRef]
- Tendera, M.; Talajic, M.; Robertson, M.; Tardif, J.C.; Ferrari, R.; Ford, I.; Steg, P.G.; Fox, K. BEAUTIFUL Investigators. Safety of ivabradine in patients with coronary artery disease and left ventricular systolic dysfunction (from the BEAUTIFUL Holter Substudy). Am. J. Cardiol. 2011, 107, 805–811. [Google Scholar]
- Guaricci, A.I.; Schuijf, J.D.; Cademartiri, F.; Brunetti, N.D.; Montrone, D.; Maffei, E.; Tedeschi, C.; Ieva, R.; di Biase, L.; Midiri, M.; et al. Incremental value and safety of oral ivabradine for heart rate reduction in computed tomography coronary angiography. Int. J. Cardiol. 2012, 156, 28–33. [Google Scholar] [CrossRef]
- Calò, L.; Rebecchi, M.; Sette, A.; Martino, A.; de Ruvo, E.; Sciarra, L.; de Luca, L.; Zuccaro, L.M.; Giunta, G.; Ciccaglioni, A.; et al. Efficacy of ivabradine administration in patients affected by inappropriate sinus tachycardia. Heart Rhythm 2010, 7, 1318–1323. [Google Scholar] [CrossRef]
- Borer, J.S.; Tardif, J.C. Efficacy of ivabradine, a selective I(f) inhibitor, in patients with chronic stable angina pectoris and diabetes mellitus. Am. J. Cardiol. 2010, 105, 29–35. [Google Scholar] [CrossRef]
- Lage-Gallé, E.; Romero-Rodríguez, N.; Nevado-Portero, J.; Guisado-Rasco, A.; Sobrino-Márquez, M.; Machuca, M.G.; Fernández-Quero, M.; Campos-Pareja, A.; Ballesteros-Pradas, S.; Martínez-Martínez, A. Safety and effectiveness of ivabradine after cardiac transplantation. Transplant. Proc. 2010, 42, 3191–3192. [Google Scholar]
- Camm, A.J.; Lau, C.P. Electrophysiological effects of a single intravenous administration of ivabradine (S 16257) in adult patients with normal baseline electrophysiology. Drugs R. D. 2003, 4, 83–89. [Google Scholar] [CrossRef]
- Kmecova, J.; Klimas, J. Heart rate correction of the QT duration in rats. Eur. J. Pharmacol. 2010, 641, 187–192. [Google Scholar] [CrossRef]
- Milliez, P.; Messaoudi, S.; Nehme, J.; Rodriguez, C.; Samuel, J.L.; Delcayre, C. Beneficial effects of delayed ivabradine treatment on cardiac anatomical and electrical remodeling in rat severe chronic heart failure. Am. J. Physiol. Heart Circ. Physiol. 2009, 296, 435–441. [Google Scholar]
- Summary of Product Characteristics (last update 16 February 2012). Available online: http://www.medicines.org.uk/EMC/medicine/17188/SPC/Procoralan/ (accessed on 18 June 2012).
- Portolés, A.; Terleira, A.; Calvo, A.; Martínez, I.; Resplandy, G. Effects of Hypericum perforatum on ivabradine pharmacokinetics in healthy volunteers: An open-label, pharmacokinetic interaction clinical trial. J. Clin. Pharmacol. 2006, 46, 1188–1194. [Google Scholar] [CrossRef]
- Vlase, L.; Neag, M.; Popa, A.; Muntean, D.; Bâldea, I.; Leucuta, S.E. Pharmacokinetic interaction between ivabradine and carbamazepine in healthy volunteers. J. Clin. Pharm. Ther. 2011, 36, 225–229. [Google Scholar] [CrossRef]
- Aboyans, V.; Criqui, M.H. Can we improve cardiovascular risk prediction beyond risk equations in the physician’s office? J. Clin. Epidemiol. 2006, 59, 547–558. [Google Scholar] [CrossRef]
- Diaz, A.; Bourassa, M.G.; Guertin, M.C.; Tardif, J.C. Long term prognostic value of resting heart rate in patients with suspected or proven coronary artery disease. Eur. Heart J. 2005, 26, 967–974. [Google Scholar] [CrossRef]
- Fox, K.; Ford, I.; Steg, P.G.; Tendera, M.; Robertson, M.; Ferrari, R. Heart rate as a prognostic risk factors in patients with coronary artery diasease and left-ventricular systolic dysfuunction (BEAUTIFUL): A subgoup analysis of a randomised controlled trial. Lancet 2008, 372, 817–821. [Google Scholar]
- Fox, K.; Borer, J.S.; Camm, A.J.; Danchin, N.; Ferrari, R.; Lopez-Sendon, J.L.; Steg, P.G.; Tardif, J.C.; Tavazzi, L.; Tendera, M.; et al. Resting heart rate in cardiovascular disease. J. Am. Coll. Cardiol. 2007, 50, 823–830. [Google Scholar] [CrossRef]
- Manz, M.; Reuter, M.; Lauck, G.; Omran, H.; Jung, W. A single dose of ivabradine, a novel If inhibitor, lowers heart rate but does not depress left ventricular function in patients with left ventricular dysfunction. Cardiology 2003, 100, 149–155. [Google Scholar] [CrossRef]
- De Ferrari, G.M.; Mazzuero, A.; Agnesina, L.; Bertoletti, A.; Lettino, M.; Campana, C.; Schwartz, P.J.; Tavazzi, L. Favourable effects of heart rate reduction with intravenous administration of ivabradine in patients with advanced heart failure. Eur. J. Heart Fail. 2008, 10, 550–555. [Google Scholar] [CrossRef]
- Portolés, A.; Calvo, A.; Terleira, A.; Laredo, L.; Resplandy, G.; Gorostiaga, C.; Moreno, A. Lack of pharmacokinetic interaction between omeprazole or lansoprazole and ivabradine in healthy volunteers: An open-label, randomized, crossover, pharmacokinetic interaction clinical trial. J. Clin. Pharmacol. 2006, 46, 1195–1203. [Google Scholar] [CrossRef]
- Tardif, J.C.; Ford, I.; Tendera, M.; Bourassa, M.G.; Fox, K. Efficacy of ivabradine, a new selective If inhibitor, compared with atenolol in patients with chronic stable angina. Eur. Heart J. 2005, 26, 2529–2536. [Google Scholar] [CrossRef]
- Tardif, J.C. Ivabradine: I(f) inhibition in the management of stable angina pectoris and other cardiovascular diseases. Drugs Today 2008, 44, 171–181. [Google Scholar] [CrossRef]
- Tardif, J.-C.; Ponikowski, P.; Kahan, T. Efficacy of If current inhibitor ivabradine in patients with chronic stable angina receiving beta-blockers therapy: A 4-month, randomized, placebo-controlled trial. Eur. Heart J. 2009, 30, 540–548. [Google Scholar] [CrossRef]
- Amosova, E.; Andrejev, E.; Zaderey, I.; Rudenko, U.; Ceconi, C.; Ferrari, R. Efficacy of ivabradine in combination with beta-blocker versus up titration of beta-blocker in patients with stable angina. Cardiovasc. Drugs Ther. 2011, 25, 531–537. [Google Scholar] [CrossRef]
- Werdan, K.; Ebelt, H.; Nuding, S.; Höpfner, F.; Hack, G.; Müller-Werdan, U. Ivabradine in combination with beta-blocker improves symptoms and quality of life in patients with stable angina pectoris: Results from the ADDITIONS study. Clin. Res. Cardiol. 2012, 101, 365–373. [Google Scholar] [CrossRef]
- Riccioni, G.; Prencipe, G.A.; Benvenuto, A.; Masciocco, L.; Ventra, S.; Rizzo, U.; Russi, C.; Speziale, G. Ivabradine Improves All Aspects of Quality of Life Assessed with the 36-Item Short Form Health Survey in Subjects with Chronic Ischemic Heart Disease Compared with Beta-Blockers. Pharmacology 2012. [Google Scholar] [CrossRef]
- Fasullo, S.; Cannizzaro, S.; Maringhini, G.; Ganci, F.; Migliore, G.; Torres, D.; Sarullo, F.M.; Paterna, S.; di Pasquale, P. Comparison of ivabradine versus metoprolol in early phases of reperfused anterior myocardial infarction with impaired left ventricular function: Preliminary findings. J. Card. Fail. 2009, 15, 856–863. [Google Scholar] [CrossRef]
- Post, F.; Münzel, T. Ivabradine—A new therapeutic option for cardiogenic shock? Herz 2009, 34, 224–229. [Google Scholar]
- Nuding, S.; Enelt, H.; Hoke, R.S.; Krummenerl, A.; Wiemke, A.; Muller-Werdan, U.; Werdan, K. Reducing elevated heart rate in patients with multiple organ dysfunction syndrome by the I(f) (funny channel current) inhibitor ivabradine. MODI(f)Y trial. Clin. Res. Cardiol. 2011, 100, 915–923. [Google Scholar]
- Heusch, G. Pleiotropic action(s) of the bradycardic agent ivabradine: Cardiovascular protection beyond heart rate reduction. Br. J. Pharmacol. 2008, 155, 970–971. [Google Scholar] [CrossRef]
- Heusch, G.; Skyschally, A.; Gres, P.; van Caster, P.; Schilawa, D.; Schulz, R. Improvement of regional myocardial blood flow and function and reduction of infarct size with ivabradine: Protection beyond heart rate reduction. Eur. Heart J. 2008, 29, 2265–2275. [Google Scholar] [CrossRef]
- Riccioni, G. Ivabradine: from molecular basis to clinical effectiveness. Adv. Ther. 2010, 27, 160–167. [Google Scholar]
- Speranza, L.; Franceschelli, S.; Riccioni, G. The biological effects of ivabradine in cardiovascular disease. Molecules 2012, 17, 4924–4935. [Google Scholar] [CrossRef]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Riccioni, G. Ivabradine: An Intelligent Drug for the Treatment of Ischemic Heart Disease. Molecules 2012, 17, 13592-13604. https://doi.org/10.3390/molecules171113592
Riccioni G. Ivabradine: An Intelligent Drug for the Treatment of Ischemic Heart Disease. Molecules. 2012; 17(11):13592-13604. https://doi.org/10.3390/molecules171113592
Chicago/Turabian StyleRiccioni, Graziano. 2012. "Ivabradine: An Intelligent Drug for the Treatment of Ischemic Heart Disease" Molecules 17, no. 11: 13592-13604. https://doi.org/10.3390/molecules171113592
APA StyleRiccioni, G. (2012). Ivabradine: An Intelligent Drug for the Treatment of Ischemic Heart Disease. Molecules, 17(11), 13592-13604. https://doi.org/10.3390/molecules171113592