
Prosthetic Rehabilitation of an Unusually Self-Obturated Cleft Palate Defect in an Adult Edentulous Patient Living in a Remote Rural Area. A Clinical Report


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
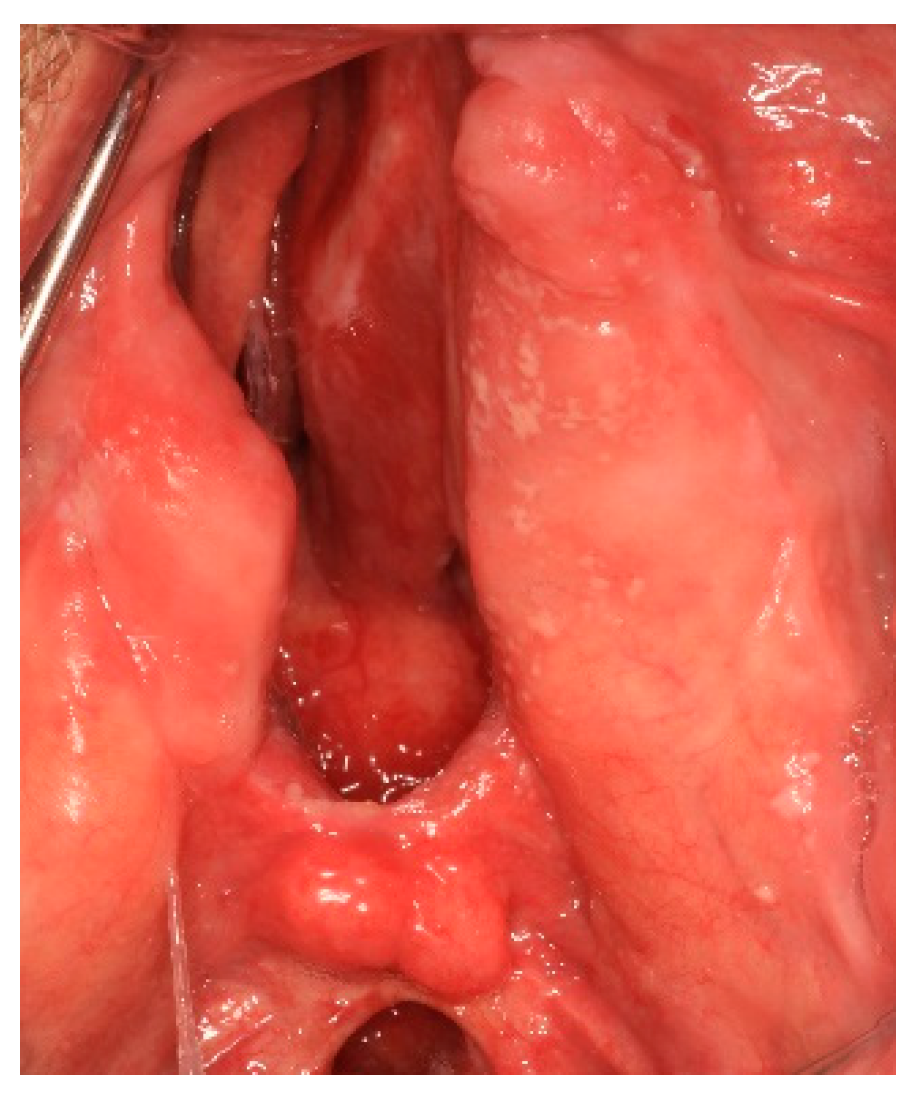
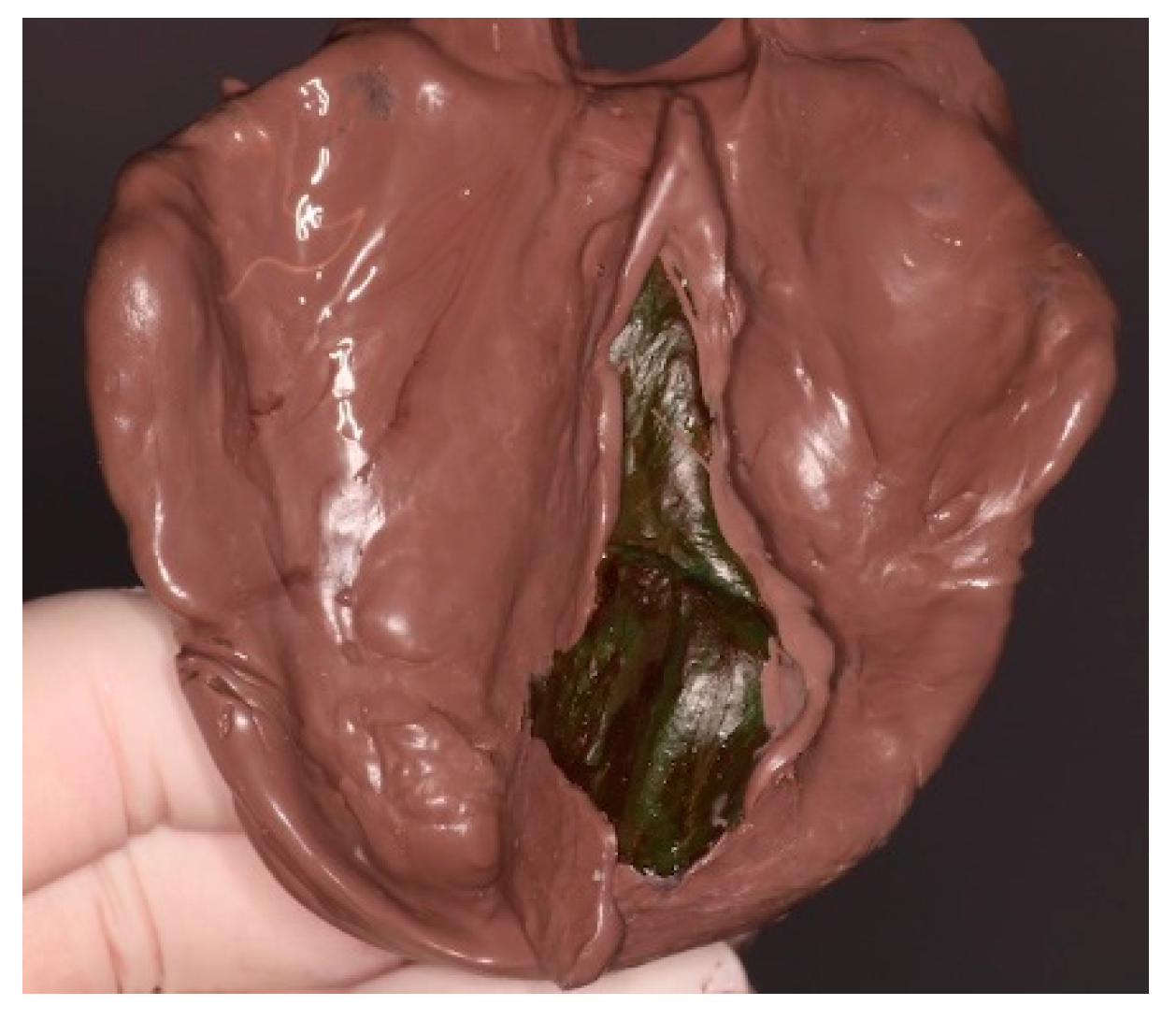
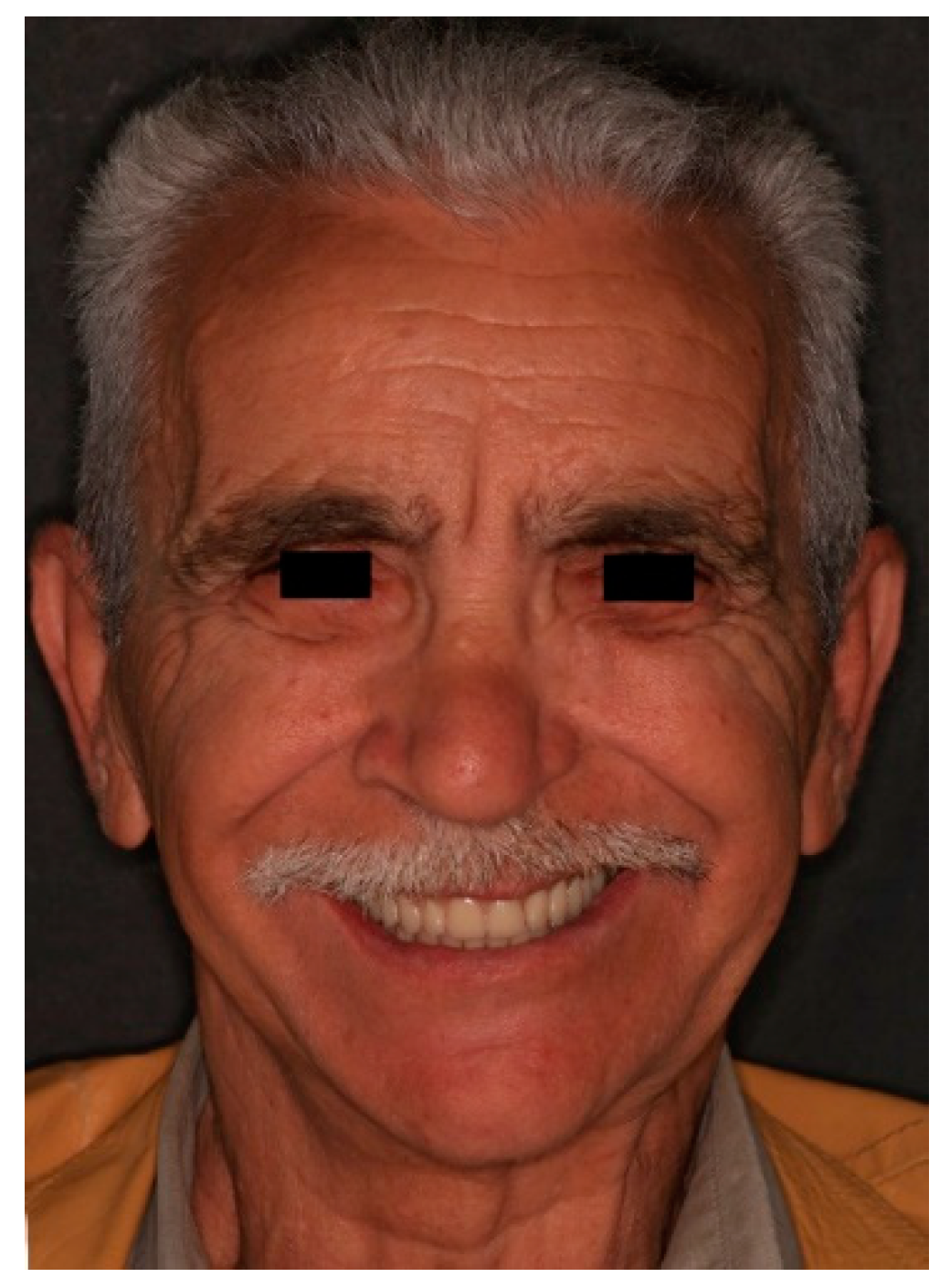
2. Case Report
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferro, K.J.; Morgano, S.M.; Driscoll, C.F.; Freilich, M.A.; Guckes, A.D.; Knoernschild, K.L. The Glossary of Prosthodontic Terms. J. Prosthet. Dent. 2017, 117, C1–e105. [Google Scholar] [CrossRef] [Green Version]
- Aramany, M.A. A history of prosthetic management of cleft palate: Pare to Suerson. Cleft Palate J. 1971, 8, 415–430. [Google Scholar] [PubMed]
- Beumer, J.; Curtis, T.A.; Marunick, M.T. Maxillofacial Rehabilitation: Prosthodontic and Surgical Management of Cancer-Related, Acquired, and Congenital Defects of the Head and Neck, 3rd ed.; Quintessence Pub: Hanover Park, IL, USA, 2011; pp. 315–355. [Google Scholar]
- Güven, O.; Gürbüz, A.; Baltali, E.; Yilmez, B.; Hatipoglou, M. Surgical and Prosthetic Rehabilitation of Edentulous Adult Cleft Palate Patients by Dental Implants. J. Craniofac. Surg. 2010, 21, 1538–1541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosalen, N.P.; Muniz, F.W.; Scalo, N.R.; Dezingrini, K.S.; Colussi, E.L.; Pires, A.L.; Colussi, P.R.G. What variables are associated with use of and need for dental prosthesis? A cross-sectional study. Gerodontology 2021. Early View. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.-C.; Park, J.-H.; Seok, H.; Baek, J.-A.; Kim, D.-W.; Ko, S.-O. Speech-aid prosthesis in velopharyngeal incompetency patient with cleft palate: Can speech aids be applicable for adult patient? Maxillofac. Plast. Reconstr. Surg. 2021, 43, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Markus, A.F.; Watts, R. Cleft palate speech. Dent Clin. North Am. 2000, 12, 481–498. [Google Scholar] [CrossRef]
- Hardwick, C.; Puryer, J. A palatal speech bulb-A case study. Reports 2019, 2, 5. [Google Scholar] [CrossRef] [Green Version]
- Harrison, J.W. Dental Implants to Rehabilitate a Patient with an Unrepaired Complete Cleft of the Hard and Soft Palate: A Clinical Report. Cleft Palate-Craniofacial J. 1992, 29, 485–488. [Google Scholar] [CrossRef] [PubMed]
- Banett, T.; Hoag, H.; Stuart, J.; Crocombe, L. The relationship of primary care providers to dental practitioners in rural and re-mote Australia. BMC Health Serv. Res. 2017, 17, 515–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Artopoulou, I.I.; Salia, A.; Polyzois, G. Prosthetic Rehabilitation of an Unusually Self-Obturated Cleft Palate Defect in an Adult Edentulous Patient Living in a Remote Rural Area. A Clinical Report. Prosthesis 2021, 3, 388-393. https://doi.org/10.3390/prosthesis3040034
Artopoulou II, Salia A, Polyzois G. Prosthetic Rehabilitation of an Unusually Self-Obturated Cleft Palate Defect in an Adult Edentulous Patient Living in a Remote Rural Area. A Clinical Report. Prosthesis. 2021; 3(4):388-393. https://doi.org/10.3390/prosthesis3040034
Chicago/Turabian StyleArtopoulou, Ioli Ioanna, Andromachi Salia, and Gregory Polyzois. 2021. "Prosthetic Rehabilitation of an Unusually Self-Obturated Cleft Palate Defect in an Adult Edentulous Patient Living in a Remote Rural Area. A Clinical Report" Prosthesis 3, no. 4: 388-393. https://doi.org/10.3390/prosthesis3040034