
Perceived Symptoms of Depression, Anxiety and Stress amongst Staff in a Malaysian Public University: A Workers Survey

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Setting and Participants
2.2. Sample Size Calculation
2.3. Study Inclusion and Exclusion Criteria
2.4. Study Instrument
2.5. Statistical Analyses
3. Results
3.1. Sample Characteristics
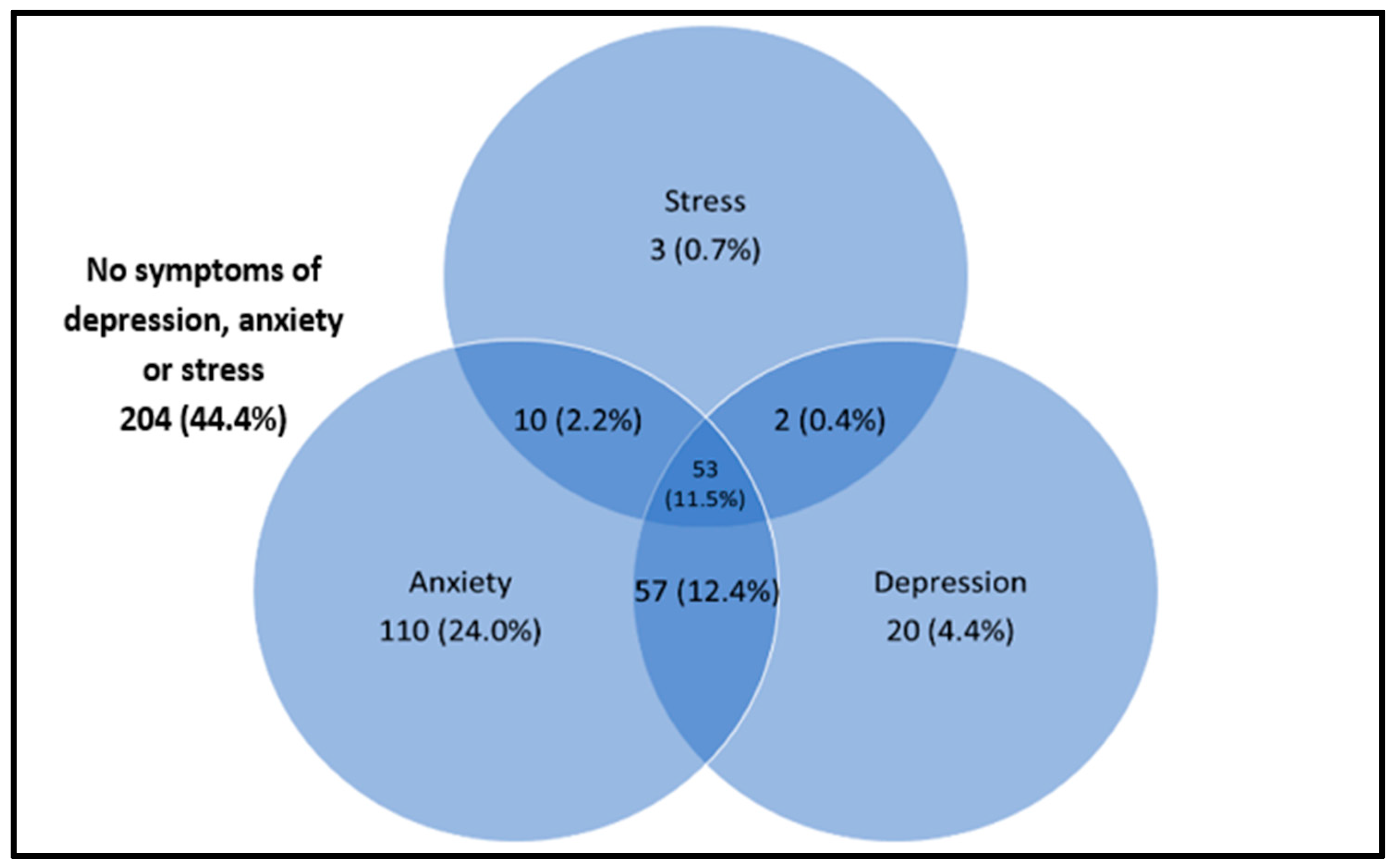
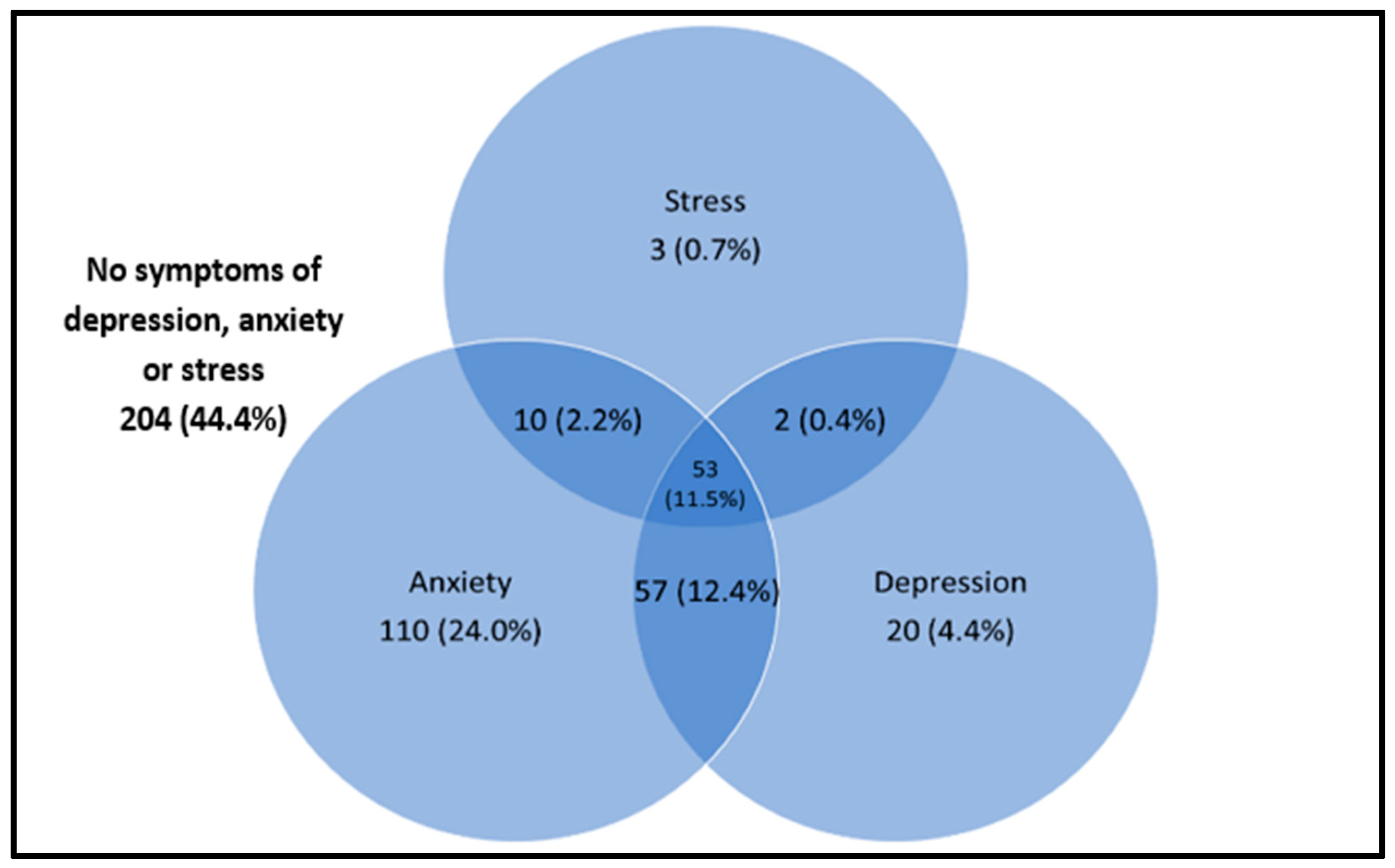
3.2. Prevalence of Depression, Anxiety and Stress
3.3. Factors Associated with Depression, Anxiety and Stress at the Bivariate Level
3.4. Factors Associated with Depression, Anxiety and Stress by Multiple Logistic Regression
4. Discussion
4.1. Core Summary Findings
4.2. Comparisons with Existing Literature
4.3. Study Limitations and Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saraceno, B. The WHO World Health Report 2001 on Mental Health. Epidemiol. Psichiatr. Soc. 2002, 11, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Global Burden of Disease Study 2013 Collaborators. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 301 Acute and Chronic Diseases and Injuries in 188 Countries, 1990–2013: A Systematic Analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [Google Scholar] [CrossRef] [Green Version]
- Steel, Z.; Marnane, C.; Iranpour, C.; Chey, T.; Jackson, J.W.; Patel, V.; Silove, D. The Global Prevalence of Common Mental Disorders: A Systematic Review and Meta-Analysis 1980–2013. Int. J. Epidemiol. 2014, 43, 476–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naveed, S.; Waqas, A.; Chaudhary, A.; Kumar, S.; Abbas, N.; Amin, R.; Jamil, N.; Saleem, S. Prevalence of Common Mental Disorders in South Asia: A Systematic Review and Meta-Regression Analysis. Front. Psychiatry 2020, 11, 573150. [Google Scholar] [CrossRef] [PubMed]
- Institute for Public Health. National Health & Morbidity Survey (NHMS) 2015; Fact Sheet 2015; Institute for Public Health: Kuala Lumpur, Malaysia, 2015. [Google Scholar]
- Teh, C.K.; Ngo, C.W.; Zulkifli, R.A.; Vellasamy, R.; Suresh, K. Depression, Anxiety and Stress among Undergraduate Students: A Cross Sectional Study. Open J. Epidemiol. 2015, 5, 260–268. [Google Scholar] [CrossRef] [Green Version]
- Al-Naggar, R.A.; Al-Naggar, D.H. Prevalence and Associated Factors of Emotional Disorder among Malaysian University Students. Int. J. Collab. Res. Intern. Med. Public Health 2012, 4, 1401–1411. [Google Scholar]
- Whiteford, H.A.; Degenhardt, L.; Rehm, J.; Baxter, A.J.; Ferrari, A.J.; Erskine, H.E.; Charlson, F.J.; Norman, R.E.; Flaxman, A.D.; Johns, N.; et al. Global Burden of Disease Attributable to Mental and Substance Use Disorders: Findings from the Global Burden of Disease Study 2010. Lancet 2013, 382, 1575–1586. [Google Scholar] [CrossRef]
- Mathers, C.D.; Loncar, D. Projections of Global Mortality and Burden of Disease from 2002 to 2030. PLoS Med. 2006, 3, e442. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Disease Burden and Mortality Estimates. Available online: https://www.who.int/healthinfo/global_burden_disease/estimates/en/ (accessed on 28 October 2021).
- Institute for Public Health. National Health and Morbidity Survey (NHMS) 2019: NCDs—Non-Communicable Diseases: Risk Factors and other Health Problems; Institute for Public Health, National Institutes of Health (NIH), Ministry of Health Malaysia: Shah Alam, Malaysia, 2019; Volume 1. [Google Scholar]
- Roser, H.R.; Ritchie, M.H.; Roser, M. Mental Health. Available online: https://ourworldindata.org/mental-health (accessed on 30 August 2021).
- American Psychological Association. What’s the Difference between Stress and Anxiety? Available online: https://www.apa.org/topics/stress/anxiety-difference (accessed on 30 August 2021).
- Patel, V.; Saxena, S.; Lund, C.; Thornicroft, G.; Baingana, F.; Bolton, P.; Chisholm, D.; Collins, P.Y.; Cooper, J.L.; Eaton, J.; et al. The Lancet Commission on Global Mental Health and Sustainable Development. Lancet 2018, 392, 1553–1598. [Google Scholar] [CrossRef] [Green Version]
- Chua, S.N. Workplace Mental Health: The Business Costs. Relate Mental Health Malaysia 2020. Available online: https://relate.com.my/wp-content/uploads/2020/02/WorkplaceMentalHealth_FA_17022020_BW.pdf (accessed on 30 August 2021).
- Loissel, E. Mental Health in Academia a Question of Support. eLife 2019, 8, e52881. [Google Scholar] [CrossRef]
- Guthrie, S.; Lichten, C.A.; Van Belle, J.; Ball, S.; Knack, A.; Hofman, J. Understanding Mental Health in the Research Environment: A Rapid Evidence Assessment. Rand Health Q. 2018, 7, 2. [Google Scholar] [PubMed]
- Tai, K.L.; Ng, Y.G.; Lim, P.Y. Systematic Review on the Prevalence of Illness and Stress and Their Associated Risk Factors among Educators in Malaysia. PLoS ONE 2019, 14, e0217430. [Google Scholar] [CrossRef] [Green Version]
- Lashuel, H.A. Mental Health in Academia: What about Faculty? eLife 2020, 9, e54551. [Google Scholar] [CrossRef] [Green Version]
- Rajgopal, T. Mental Well-Being at the Workplace. Indian J. Occup. Environ. Med. 2010, 14, 63. [Google Scholar] [CrossRef] [Green Version]
- Kish, L. Survey Sampling; John Wiley and Sons, Inc.: New York, NY, USA, 1965; pp. 78–94. [Google Scholar]
- Urbaniak, G.C.; Plous, S. Research Randomizer—Random Sampling and Random Assignment Made Easy. Available online: https://www.randomizer.org/ (accessed on 30 January 2019).
- Department of Statistics Malaysia. Household Income & Basic Amenities Survey Report 2019. 2020. Available online: https://www.dosm.gov.my/v1/index.php?r=column/cthemeByCat&cat=120&bul_id=TU00TmRhQ1N5TUxHVWN0T2VjbXJYZz09&menu_id=amVoWU54UTl0a21NWmdhMjFMMWcyZz09 (accessed on 30 August 2021).
- Xiao, J.; Wu, C.L.; Gao, Y.X.; Wang, S.L.; Wang, L.; Lu, Q.Y.; Wang, X.J.; Hua, T.Q.; Shen, H.; Cai, H. Prevalence of Metabolic Syndrome and Its Risk Factors Among Rural Adults in Nantong, China. Sci. Rep. 2016, 6, 38089. [Google Scholar] [CrossRef] [Green Version]
- Soo, K.L.; Wan Abdul Manan, W.M.; Wan Suriati, W.N. The Bahasa Melayu Version of the Global Physical Activity Questionnaire: Reliability and Validity Study in Malaysia. Asia Pac. J. Public Health 2015, 27, 184–193. [Google Scholar] [CrossRef]
- Roland, J. What Exactly Are METs, and What Should You Know About Them? Available online: https://www.healthline.com/health/what-are-mets (accessed on 30 January 2019).
- World Health Organization. Global Recommendations on Physical Activity for Health 2010. Available online: https://www.who.int/publications/i/item/9789241599979 (accessed on 30 September 2021).
- Musa, R.; Fadzil, M.F.; Zain, Z. Translation, validation and psychometric properties of Bahasa Malaysia version of the Depression, Anxiety and Stress Scale (DASS). ASEAN J. Psychiatry 2007, 8, 82–89. [Google Scholar]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scales; Psychology Foundation of Australia: Sydney, Australia, 1995; p. 56. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows; Version 22.0; IBM Corp: Armonk, NY, USA, 2013. [Google Scholar]
- Meeks, K.; Peak, A.S.; Dreihaus, A. Depression, Anxiety, and Stress among Students, Faculty, and Staff. J. Am. Coll. Health 2021, 1–7. [Google Scholar] [CrossRef]
- Yeshaw, Y.; Mossie, A. Depression, Anxiety, Stress, and Their Associated Factors among Jimma University Staff, Jimma, Southwest Ethiopia, 2016: A Cross-Sectional Study. Neuropsychiatr. Dis. Treat. 2017, 13, 2803–2812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winefield, A.H.; Gillespie, N.; Stough, C.; Dua, J.; Hapuarachchi, J.; Boyd, C. Occupational Stress in Australian University Staff: Results from a National Survey. Int. J. Stress Manag. 2003, 10, 51–63. [Google Scholar] [CrossRef]
- Shen, X.; Yang, Y.L.; Wang, Y.; Liu, L.; Wang, S.; Wang, L. The Association between Occupational Stress and Depressive Symptoms and the Mediating Role of Psychological Capital among Chinese University Teachers: A Cross-Sectional Study. BMC Psychiatry 2014, 14, 329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukosolu, O.; Ibrahim, F.; Rampal, L.; Ibrahim, N. Prevalence of Job Stress and Its Associated Factors among Universiti Putra Malaysia Staff. Malaysian J. Med. Health Sci. 2015, 11, 27–38. [Google Scholar]
- Ismail, N.H.; Noor, A. Occupational Stress and Its Associated Factors among Academician in a Research University, Malaysia. Malays. J. Public Health Med. 2016, 16, 81–91. [Google Scholar]
- Hunter, B.; Fenwick, J.; Sidebotham, D.M.; Henley, D.J. Midwives in the United Kingdom: Levels of Burnout, Depression, Anxiety and Stress and Associated Predictors. Midwifery 2019, 79, 102526. [Google Scholar] [CrossRef]
- Saah, F.I.; Amu, H. Sleep Quality and Its Predictors among Waiters in Upscale Restaurants: A Descriptive Study in the Accra Metropolis. PLoS ONE 2020, 15, e0240599. [Google Scholar] [CrossRef] [PubMed]
- Woon, L.S.C.; Tiong, C.P. Burnout, Mental Health, and Quality of Life among Employees of a Malaysian Hospital: A Cross-sectional Study. Ann. Work Expo. Health 2020, 64, 1007–1019. [Google Scholar] [CrossRef] [PubMed]
- Ghawadra, S.F.; Abdullah, K.L.; Choo, W.Y.; Phang, C.K. Psychological Distress and Its Association with Job Satisfaction among Nurses in a Teaching Hospital. J. Clin. Nurs. 2019, 28, 4087–4097. [Google Scholar] [CrossRef] [PubMed]
- Perales, A.; Chue, H.; Padilla, A.; Barahona, L. Stress, Anxiety and Depression in Magistrates from Lima, Peru. Rev. Peru. Med. Exp. Salud Publica 2011, 28, 581–588. [Google Scholar] [CrossRef]
- Bentley, M.A.; Crawford, J.M.; Wilkins, J.R.; Fernandez, A.R.; Studnek, J.R. An Assessment of Depression, Anxiety, and Stress among Nationally Certified EMS Professionals. Prehospital. Emerg. Care 2013, 17, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Harvey, S.B.; Sellahewa, D.A.; Wang, M.J.; Milligan-Saville, J.; Bryan, B.T.; Henderson, M.; Hatch, S.L.; Mykletun, A. The Role of Job Strain in Understanding Midlife Common Mental Disorder: A National Birth Cohort Study. Lancet Psychiatry 2018, 5, 498–506. [Google Scholar] [CrossRef] [Green Version]
- Kessler, R.C.; Sampson, N.A.; Berglund, P.; Gruber, M.J.; Al-Hamzawi, A.; Andrade, L.; Bunting, B.; Demyttenaere, K.; Florescu, S.; de Girolamo, G.; et al. Anxious and Non-Anxious Major Depressive Disorder in the World Health Organization World Mental Health Surveys. Epidemiol. Psychiatr. Sci. 2015, 24, 210–226. [Google Scholar] [CrossRef] [Green Version]
- Long, E.E.; Young, J.F.; Hankin, B.L. Temporal Dynamics and Longitudinal Co-Occurrence of Depression and Different Anxiety Syndromes in Youth: Evidence for Reciprocal Patterns in a 3-Year Prospective Study. J. Affect. Disord. 2018, 234, 20–27. [Google Scholar] [CrossRef]
- Ferrari, A.J.; Somerville, A.J.; Baxter, A.J.; Norman, R.; Patten, S.B.; Vos, T.; Whiteford, H.A. Global Variation in the Prevalence and Incidence of Major Depressive Disorder: A Systematic Review of the Epidemiological Literature. Psychol. Med. 2013, 43, 471–481. [Google Scholar] [CrossRef]
- Harvard Medical School; National Comorbidity Survey (NCS). Data Table 1: Lifetime Prevalence DSM-IV/WMH-CIDI Disorders by Sex and Cohort, National Comorbidity Survey (NCS), 2007. Available online: https://www.hcp.med.harvard.edu/ncs/index.php(accessed on 30 August 2021).
- Salk, R.H.; Hyde, J.S.; Abramson, L.Y. Gender Differences in Depression in Representative National Samples: Meta-analyses of Diagnoses and Symptoms. Psychol. Bull. 2017, 143, 783–822. [Google Scholar] [CrossRef]
- Rai, D.; Zitko, P.; Jones, K.; Lynch, J.; Araya, R. Country- and Individual-Level Socioeconomic Determinants of Depression: Multilevel Cross-National Comparison. Br. J. Psychiatry 2013, 202, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Breslau, N.; Davis, G.C.; Andreski, P.; Peterson, E.L.; Schultz, L.R. Sex Differences in Posttraumatic Stress Disorder. Arch. Gen. Psychiatry 1997, 54, 1044–1048. [Google Scholar] [CrossRef]
- Karl, M.; Schaber, R.; Kress, V.; Kopp, M.; Martini, J.; Weidner, K.; Garthus-Niegel, S. Precarious Working Conditions and Psychosocial Work Stress Act as a Risk Factor for Symptoms of Postpartum Depression during Maternity Leave: Results from a Longitudinal Cohort Study. BMC Public Health 2020, 20, 1505. [Google Scholar] [CrossRef] [PubMed]
- Akhtar-Danesh, N.; Landeen, J. Relation between Depression and Sociodemographic Factors. Int. J. Ment. Health Syst. 2007, 1, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, R.C.; Birnbaum, H.; Bromet, E.; Hwang, I.; Sampson, N.; Shahly, V. Age Differences in Major Depression: Results from the National Comorbidity Survey Replication (NCS-R). Psychol. Med. 2010, 40, 225–237. [Google Scholar] [CrossRef] [Green Version]
- Ganasegeran, K.; Renganathan, P.; Manaf, R.A.; Al-Dubai, S.A. Factors Associated with Anxiety and Depression Among Type 2 Diabetes Outpatients in Malaysia: A Descriptive Cross-Sectional Single-Centre Study. BMJ Open 2014, 4, e004794. [Google Scholar] [CrossRef]
- Stordal, E.; Mykletun, A.; Dahl, A.A. The Association between Age and Depression in the General Population: A Multivariate Examination. Acta Psychiatr. Scand. 2003, 107, 132–141. [Google Scholar] [CrossRef]
- Kim, Y.M.; Cho, S. Socioeconomic Status, Work-Life Conflict, and Mental Health. Am. J. Ind. Med. 2020, 63, 703–712. [Google Scholar] [CrossRef]
- Stansfeld, S.A.; Rasul, F.R.; Head, J.; Singleton, N. Occupation and Mental Health in a National UK Survey. Soc. Psychiatry Psychiatr. Epidemiol. 2011, 46, 101–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melchior, M.; Caspi, A.; Milne, B.J.; Danese, A.; Poulton, R.; Moffitt, T.E. Work Stress Precipitates Depression and Anxiety in Young, Working Women and Men. Psychol. Med. 2007, 37, 1119–1129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clarke, D.M.; Currie, K.C. Depression, Anxiety and Their Relationship with Chronic Diseases: A Review of the Epidemiology, Risk and Treatment Evidence. Med. J. Aust. 2009, 190, S54–S60. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristics | n (%) | |
|---|---|---|
| Gender | Men | 150 (32.7) |
| Women | 309 (67.3) | |
| Age (years) | Mean (SD) | 43.21 (7.57) |
| Age groups (years) | <40 | 181 (39.4) |
| ≥40 | 278 (60.6) | |
| Marital status | Single | 64 (13.9) |
| Married | 395 (86.1) | |
| Household income classification (n = 417) | B40 | 120 (28.8) |
| M40 | 198 (47.5) | |
| T20 | 99 (23.7) | |
| Education level | Secondary or less | 107 (23.3) |
| Tertiary | 352 (76.7) | |
| Occupation categories | Academic | 104 (22.7) |
| Non-academic professional | 94 (20.5) | |
| Non-academic support | 261 (56.9) | |
| Duration of service years | ≤15 | 225 (49.0) |
| >15 | 234 (51.0) | |
| Smoking status (n = 344) | No | 284 (82.6) |
| Yes | 60 (17.4) | |
| Physical activity level | Active PA | 386 (84.1) |
| Inactive PA | 73 (15.9) | |
| Medical conditions that required hospitalizations | No | 443 (96.5) |
| Yes | 16 (3.5) | |
| Domains | Symptom Severity | Total n (%) | Men n (%) | Women n (%) | p-Value |
|---|---|---|---|---|---|
| Depression | No depression | 327 (71.2) | 118 (78.7) | 209 (67.6) | 0.027 |
| Mild | 69 (15.0) | 14 (9.3) | 55 (17.8) | ||
| Moderate | 54 (11.8) | 18 (12.0) | 36 (11.7) | ||
| Severe | 8 (1.7) | 0 (0) | 8 (2.6) | ||
| Extremely severe | 1 (0.2) | 0 (0) | 1 (0.3) | ||
| Mean (SD) | 6.42 (5.49) | 5.97 (4.95) | 6.64 (5.73) | 0.222 | |
| Anxiety | No anxiety | 229 (49.9) | 78 (52.0) | 151 (48.9) | 0.805 |
| Mild | 59 (12.9) | 19 (12.7) | 40 (12.9) | ||
| Moderate | 136 (29.6) | 44 (29.3) | 92 (29.8) | ||
| Severe | 35 (7.6) | 9 (6.0) | 26 (5.7) | ||
| Extremely severe | 0 (0) | 0 (0) | 0 (0) | ||
| Mean (SD) | 7.67 (5.23) | 7.45 (4.90) | 7.78 (5.40) | 0.531 | |
| Stress | No stress | 391 (85.2) | 133 (88.7) | 258 (83.5) | 0.479 |
| Mild | 45 (9.8) | 11 (7.3) | 34 (11.0) | ||
| Moderate | 22 (4.8) | 6 (4.0) | 16 (5.2) | ||
| Severe | 1 (0.2) | 0 (0) | 1 (0.3) | ||
| Extremely severe | 0 (0) | 0 (0) | 0 (0) | ||
| Mean (SD) | 9.53 (5.64) | 8.73 (5.55) | 9.92 (5.65) | 0.035 |
| Factors | Symptoms of Depression | Symptoms of Anxiety | Symptoms of Stress | |||
|---|---|---|---|---|---|---|
| Bivariate Model cOR (95% CI) | Multivariate Model aOR (95% CI) | Bivariate Model cOR (95% CI) | Multivariate Model aOR (95% CI) | Bivariate Model cOR (95% CI) | Multivariate Model aOR (95% CI) | |
| Gender | ||||||
| Men | 1.00 | 1.00 | 1.00 | 1.00 | ||
| Women | 1.76 (1.12, 2.79) * | 1.62 (1.01, 2.65) | 1.13 (0.77, 1.68) | 1.55 (0.86, 2.78) | ||
| Age groups (years) | ||||||
| <40 | 1.62 (1.07, 2.44) * | 1.58 (1.02, 2.45) * | 1.05 (0.72, 1.53) | 1.12 (0.69, 1.97) | ||
| ≥40 | 1.00 | 1.00 | 1.00 | 1.00 | ||
| Marital status | ||||||
| Single | 1.47 (0.84, 2.57) | 1.07 (0.63, 1.82) | 1.00 | |||
| Married | 1.00 | 1.00 | 1.08 (0.52, 2.23) | |||
| Household income classification | ||||||
| B40 | 2.44 (1.31, 4.55) * | 1.67 (0.98, 2.86) | 1.07 (0.50, 2.28) | |||
| M40 | 1.75 (0.97, 3.13) | 1.50 (0.92, 2.44) | 0.88 (0.43, 1.77) | |||
| T20 | 1.00 | 1.00 | 1.00 | |||
| Education level | ||||||
| Secondary or less | 1.21 (0.76, 1.93) | 1.18 (0.77, 1.82) | 1.69 (0.85, 3.34) | 2.20 (0.90, 5.42) | ||
| Tertiary | 1.00 | 1.00 | 1.00 | 1.00 | ||
| Occupation categories | ||||||
| Academic | 1.53 (0.91, 2.55) | 1.61 (0.91, 2.83) | 1.37 (0.87, 2.17) | 1.64 (0.89, 3.02) | ||
| Non-academic professional | 2.15 (1.21, 3.81) * | 2.04 (1.12, 3.72) * | 1.04 (0.65, 1.67) | 1.31 (0.68, 2.54) | ||
| Non-academic support | 1.00 | 1.00 | 1.00 | 1.00 | ||
| Duration of services (years) | ||||||
| ≤15 | 1.55 (1.03, 2.33) * | 1.20 (0.83, 1.73) | 1.00 | |||
| >15 | 1.00 | 1.00 | 1.38 (0.82, 2.32) | |||
| Smoking status | ||||||
| No | 1.00 | 1.00 | 1.00 | 1.00 | ||
| Yes | 2.00 (0.99, 4.03) | 1.19 (0.68, 2.08) | 2.57 (0.89, 7.44) | 2.56 (0.88, 7.40) | ||
| Physical activity categories | ||||||
| Active PA | 1.00 | 1.00 | 1.00 | |||
| Inactive PA | 1.15 (0.72, 1.82) | 1.15 (0.76, 1.72) | 1.14 (0.64, 2.01) | |||
| Medical conditions that required hospitalizations | ||||||
| No | 1.00 | 1.00 | 1.00 | 1.00 | ||
| Yes | 1.24 (0.62, 2.46) | 2.39 (1.26, 4.52) * | 2.38 (1.24, 4.50) * | 1.17 (0.52, 2.62) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manaf, M.R.A.; Shaharuddin, M.A.-A.; Nawi, A.M.; Tauhid, N.M.; Othman, H.; Rahman, M.R.A.; Yusoff, H.M.; Safian, N.; Ng, P.Y.; Manaf, Z.A.; et al. Perceived Symptoms of Depression, Anxiety and Stress amongst Staff in a Malaysian Public University: A Workers Survey. Int. J. Environ. Res. Public Health 2021, 18, 11874. https://doi.org/10.3390/ijerph182211874
Manaf MRA, Shaharuddin MA-A, Nawi AM, Tauhid NM, Othman H, Rahman MRA, Yusoff HM, Safian N, Ng PY, Manaf ZA, et al. Perceived Symptoms of Depression, Anxiety and Stress amongst Staff in a Malaysian Public University: A Workers Survey. International Journal of Environmental Research and Public Health. 2021; 18(22):11874. https://doi.org/10.3390/ijerph182211874
Chicago/Turabian StyleManaf, Mohd Rizal Abdul, Muhammad Al-Amin Shaharuddin, Azmawati Mohammed Nawi, Noorlaili Mohd Tauhid, Hanita Othman, Mohd Rizam Abdul Rahman, Hanizah Mohd Yusoff, Nazarudin Safian, Pei Yuen Ng, Zahara Abdul Manaf, and et al. 2021. "Perceived Symptoms of Depression, Anxiety and Stress amongst Staff in a Malaysian Public University: A Workers Survey" International Journal of Environmental Research and Public Health 18, no. 22: 11874. https://doi.org/10.3390/ijerph182211874
APA StyleManaf, M. R. A., Shaharuddin, M. A.-A., Nawi, A. M., Tauhid, N. M., Othman, H., Rahman, M. R. A., Yusoff, H. M., Safian, N., Ng, P. Y., Manaf, Z. A., Kadir, N. B. A., Yanasegaran, K., Basir, S. M. A., Ramakrishnappa, S., Ariff, M. I., & Ganasegeran, K. (2021). Perceived Symptoms of Depression, Anxiety and Stress amongst Staff in a Malaysian Public University: A Workers Survey. International Journal of Environmental Research and Public Health, 18(22), 11874. https://doi.org/10.3390/ijerph182211874