
Augmented Reality-Assisted Craniotomy for Parasagittal and Convexity En Plaque Meningiomas and Custom-Made Cranio-Plasty: A Preliminary Laboratory Report

 , , and
, , and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
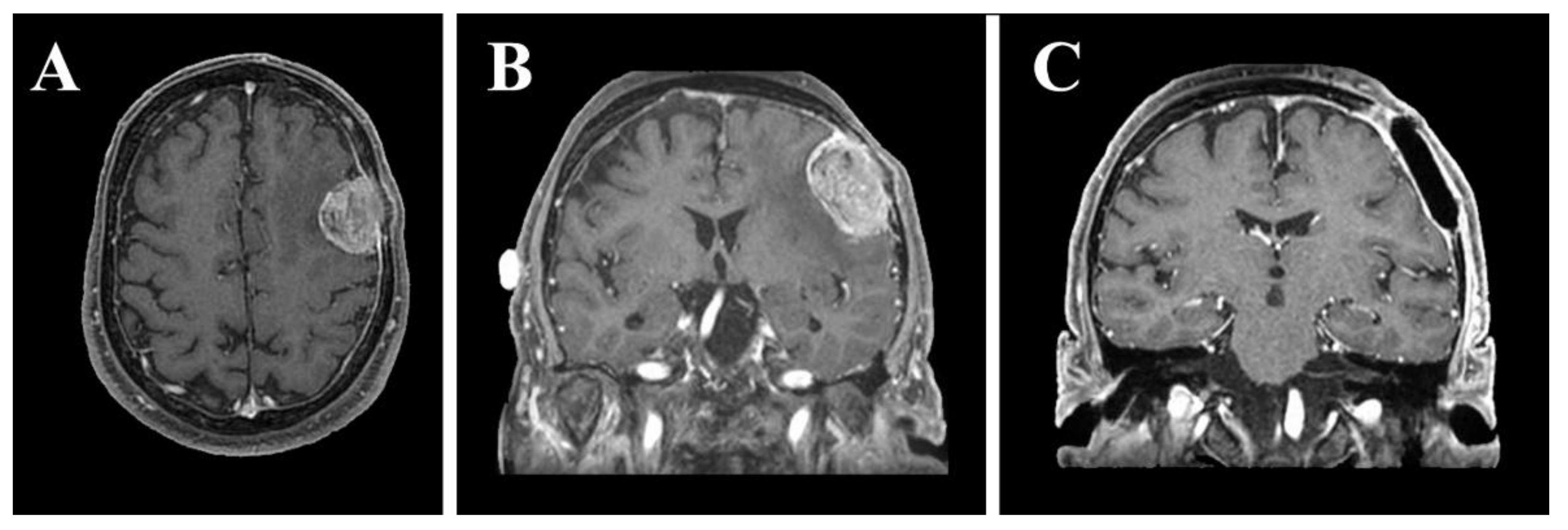
2.1. Case Description
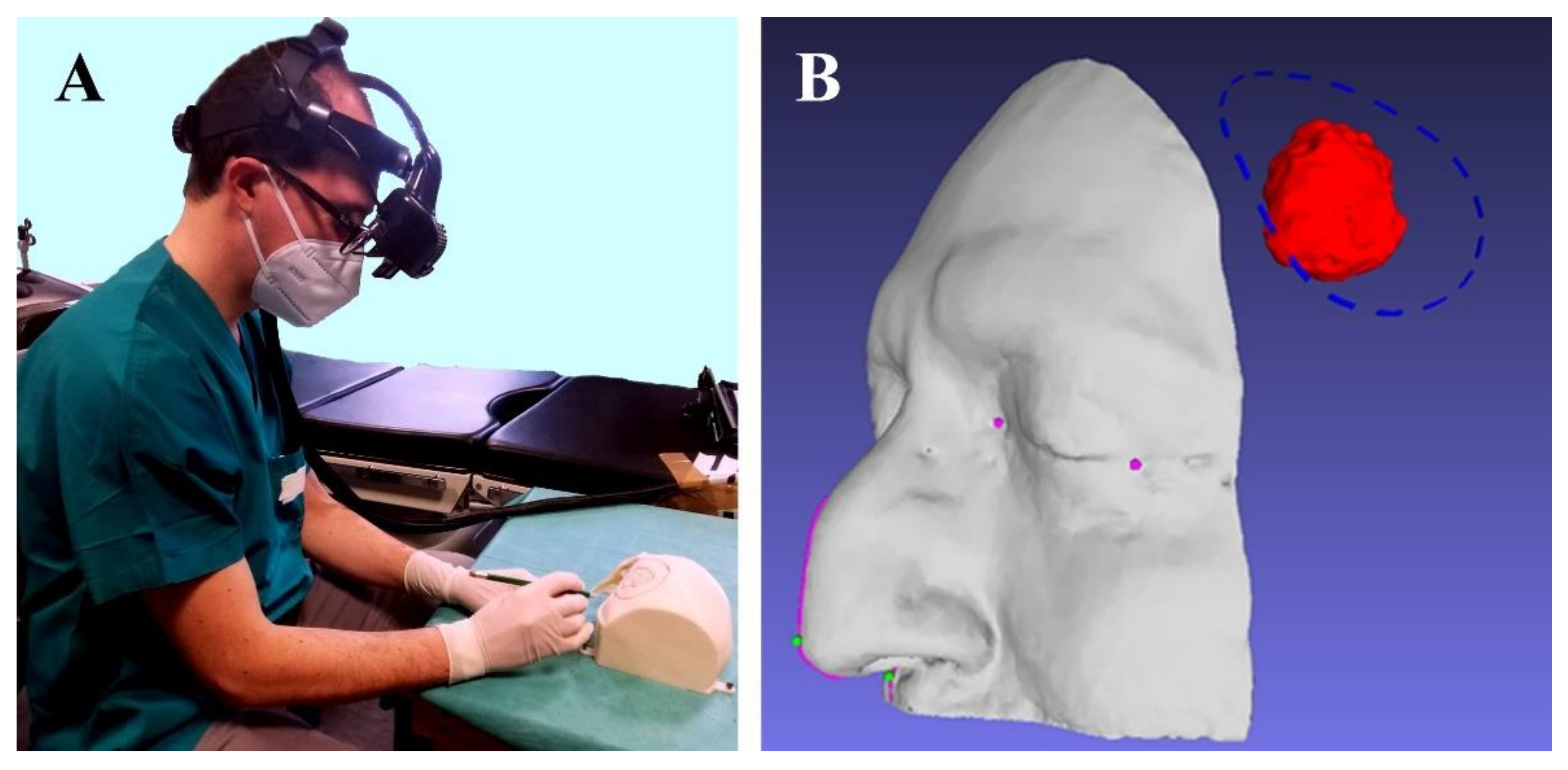
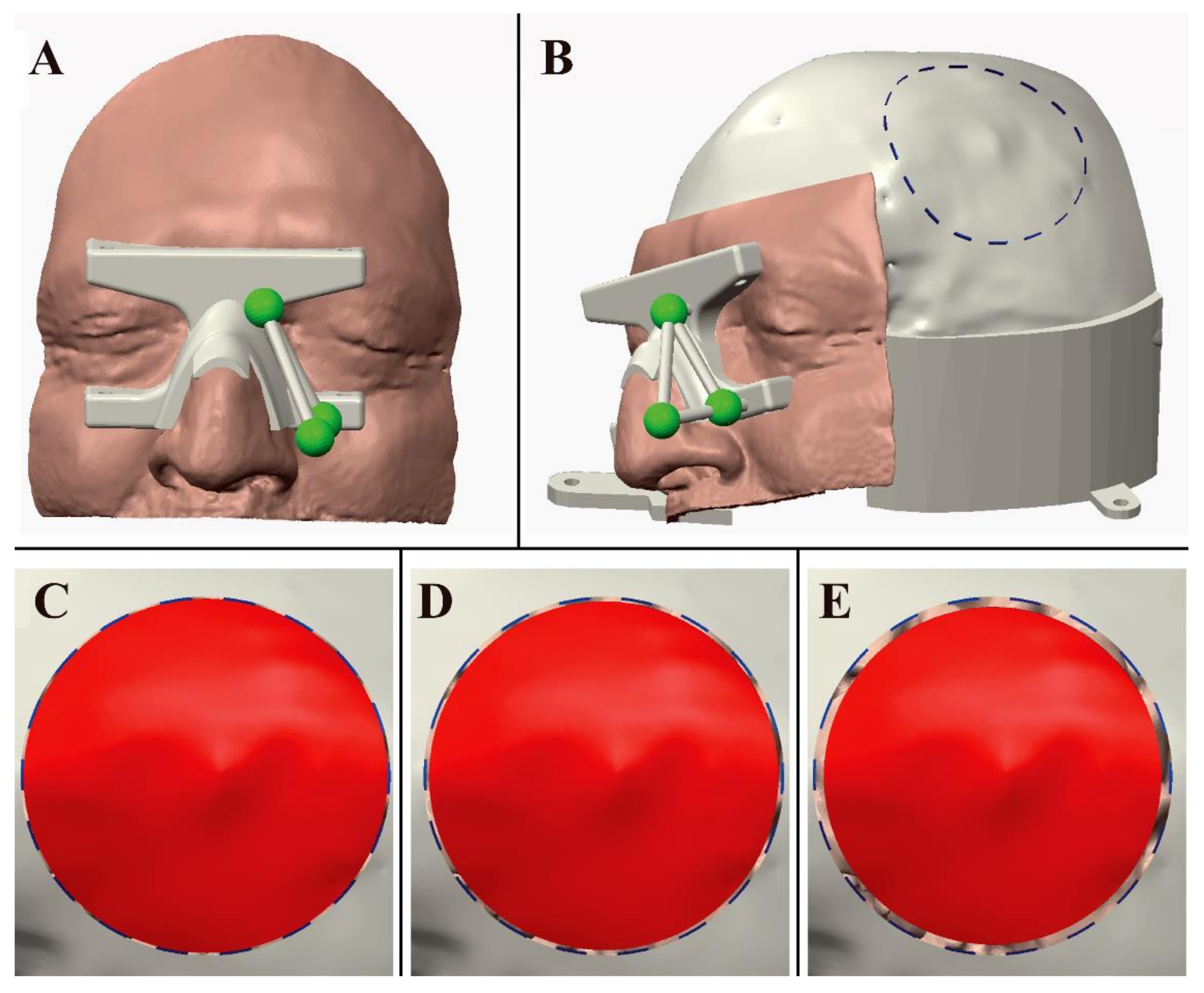
2.2. VOSTARS HMD-Based Surgical Navigation Platform and Template-Based Registration
2.3. AR Visualization Modalities


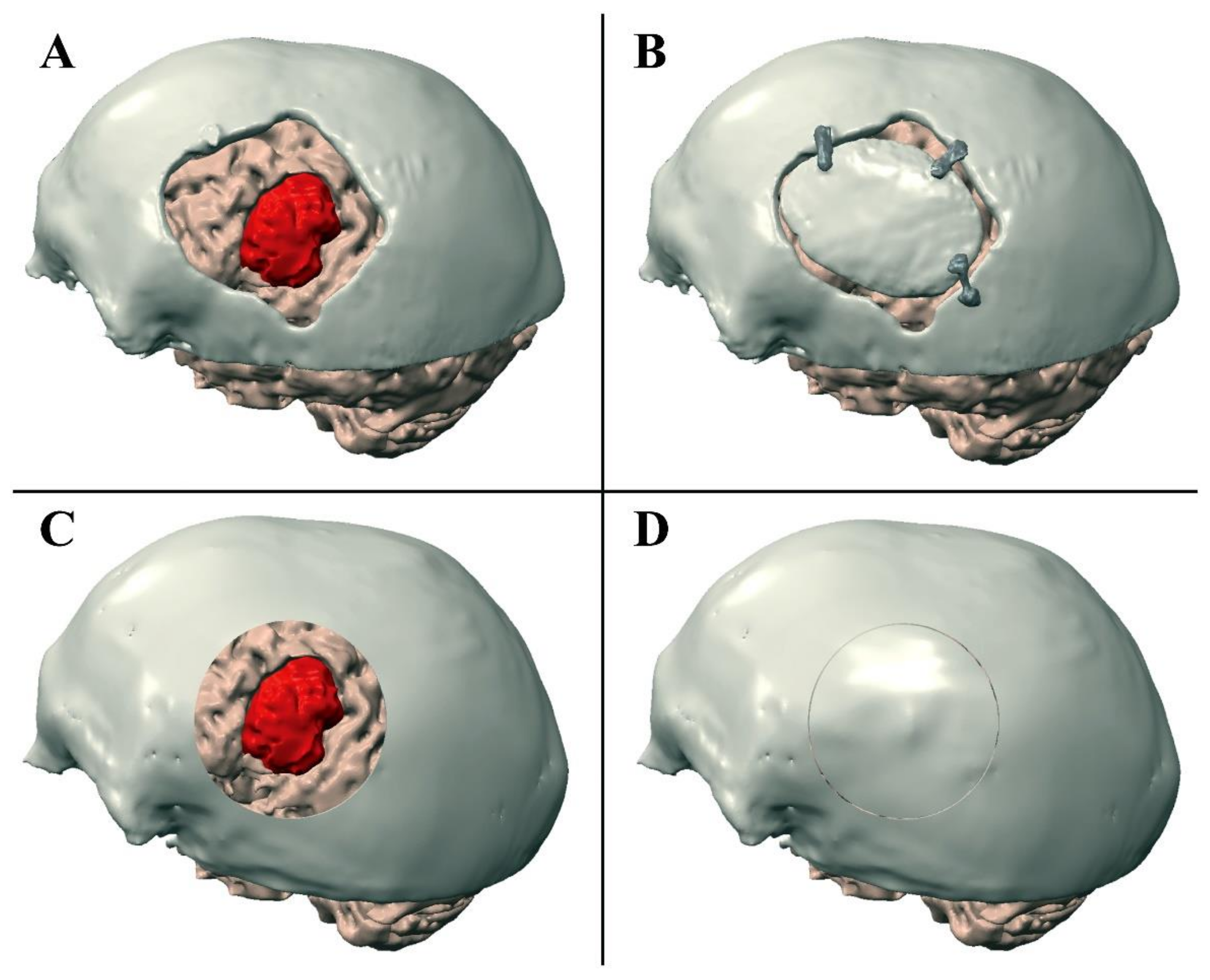
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maruyama, K.; Watanabe, E.; Kin, T.; Saito, K.; Kumakiri, A.; Noguchi, A.; Nagane, M.; Shiokawa, Y. Smart Glasses for Neurosurgical Navigation by Augmented Reality. Oper. Neurosurg. 2018, 15, 551–556. [Google Scholar] [CrossRef]
- Rolland, J.P.; Fuchs, H. Optical versus video see-through head-mounted displays in medical visualization. Presence 2000, 9, 287–309. [Google Scholar] [CrossRef]
- Cutolo, F.; Meola, A.; Carbone, M.; Sinceri, S.; Cagnazzo, F.; Denaro, E.; Esposito, N.; Ferrari, M.; Ferrari, V. A new head-mounted display-based augmented reality system in neurosurgical oncology: A study on phantom. Comput. Assist. Surg. 2017, 22, 39–53. [Google Scholar] [CrossRef]
- Léger, É.; Reyes, J.; Drouin, S.; Popa, T.; Hall, J.A.; Collins, D.L.; Kersten-Oertel, M. MARIN: An open-source mobile augmented reality interactive neuronavigation system. Int. J. Comput. Assist. Radiol. Surg. 2020, 15, 1013–1021. [Google Scholar] [CrossRef] [PubMed]
- Lavé, A.; Meling, T.R.; Schaller, K.; Corniola, M.V. Augmented reality in intracranial meningioma surgery: Report of a case and systematic review. J. Neurosurg. Sci. 2020, 64, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Jean, W.C. Mini-Pterional Craniotomy and Extradural Clinoidectomy for Clinoid Meningioma: Optimization of Exposure Using Augmented Reality Template: 2-Dimensional Operative Video. Oper. Neurosurg. 2020, 28, opaa238. [Google Scholar]
- Hou, X.; Yang, D.; Li, D.; Liu, M.; Zhou, Y.; Shi, M. A new simple brain segmentation method for extracerebral intracranial tumors. PLoS ONE 2020, 15, e0230754. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, E.; Satoh, M.; Konno, T.; Hirai, M.; Yamaguchi, T. The Trans-Visible Navigator: A See-Through Neuronavigation System Using Augmented Reality. World Neurosurg. 2016, 87, 399–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mascitelli, J.R.; Schlachter, L.; Chartrain, A.G.; Oemke, H.; Gilligan, J.; Costa, A.B.; Shrivastava, R.K.; Bederson, J.B. Navigation-Linked Heads-Up Display in Intracranial Surgery: Early Experience. Oper Neurosurg 2018, 15, 184–193. [Google Scholar] [CrossRef] [Green Version]
- Montemurro, N.; Perrini, P.; Rapone, B. Clinical Risk and Overall Survival in Patients with Diabetes Mellitus, Hyperglycemia and Glioblastoma Multiforme. A Review of the Current Literature. Int. J. Environ. Res. Public Health 2020, 17, 8501. [Google Scholar] [CrossRef]
- Karmonik, C.; Elias, S.N.; Zhang, J.Y.; Diaz, O.; Klucznik, R.P.; Grossman, R.G.; Britz, G.W. Augmented Reality with Virtual Cerebral Aneurysms: A Feasibility Study. World Neurosurg. 2018, 119, e617–e622. [Google Scholar] [CrossRef] [PubMed]
- Montemurro, N.; Fanelli, G.N.; Scatena, C.; Ortenzi, V.; Pasqualetti, F.; Mazzanti, C.M.; Morganti, R.; Paiar, F.; Naccarato, A.G.; Perrini, P. Surgical outcome and molecular pattern characterization of recurrent glioblastoma multiforme: A single-center retrospective series. Clin. Neurol. Neurosurg. 2021, 207, 106735. [Google Scholar] [CrossRef]
- Low, D.; Lee, C.K.; Dip, L.L.; Ng, W.H.; Ang, B.T.; Ng, I. Augmented reality neurosurgical planning and navigation for surgical excision of parasagittal, falcine and convexity meningiomas. Br. J. Neurosurg. 2010, 24, 69–74. [Google Scholar] [CrossRef]
- Montemurro, N. Intracranial hemorrhage and COVID-19, but please do not forget “old diseases” and elective surgery. Brain Behav. Immun. 2021, 92, 207–208. [Google Scholar] [CrossRef] [PubMed]
- Haridas, A.; Miller, M. Middle Cerebral Artery Aneurysm Clipping With Immersive 360° Virtual Reality Model: 2-Dimensional Operative Video. Oper. Neurosurg. 2021, 20, E314. [Google Scholar] [CrossRef] [PubMed]
- Corniola, M.V.; Lemée, J.M.; Schaller, K.; Meling, T.R. Lateral sphenoid wing meningiomas without bone invasion-still skull base surgery? Neurosurg. Rev. 2020, 43, 1547–1553. [Google Scholar] [CrossRef]
- Jang, S.Y.; Kim, C.H.; Cheong, J.H.; Kim, J.M. Extracranial extension of intracranial atypical meningioma en plaque with osteoblastic change of the skull. J. Korean Neurosurg. Soc. 2014, 55, 205–207. [Google Scholar] [CrossRef]
- Lin, D.D.; Lin, J.L.; Deng, X.Y.; Li, W.; Li, D.D.; Yin, B.; Lin, J.; Zhang, N.; Sheng, H.S. Trends in intracranial meningioma incidence in the United States, 2004–2015. Cancer Med. 2019, 8, 6458–6467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasseleid, B.F.; Meling, T.R.; Rønning, P.; Scheie, D.; Helseth, E. Surgery for convexity meningioma: Simpson Grade I resection as the goal: Clinical article. J. Neurosurg. 2012, 117, 999–1006. [Google Scholar] [CrossRef] [PubMed]
- Lemée, J.M.; Corniola, M.V.; Da Broi, M.; Joswig, H.; Scheie, D.; Schaller, K.; Helseth, E.; Meling, T.R. Extent of Resection in Meningioma: Predictive Factors and Clinical Implications. Sci. Rep. 2019, 9, 5944. [Google Scholar] [CrossRef]
- Simpson, D. The recurrence of intracranial meningiomas after surgical treatment. J. Neurol. Neurosurg. Psychiatry 1957, 20, 22–39. [Google Scholar] [CrossRef] [Green Version]
- Samadian, M.; Sharifi, G.; Mousavinejad, S.A.; Amin, A.A.; Ebrahimzadeh, K.; Tavassol, H.H.; Borghei-Razavi, H.; Rezaei, O. Surgical Outcomes of Sphenoorbital En Plaque Meningioma: A 10-Year Experience in 57 Consecutive Cases. World Neurosurg. 2020, 144, e576–e581. [Google Scholar] [CrossRef]
- Honeybul, S.; Neil-Dwyer, G.; Lang, D.A.; Evans, B.T.; Ellison, D.W.; Evans, B.T.; Ellison, D.W. Sphenoid wing meningioma en plaque: A clinical review. Acta Neurochir. 2001, 143, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Oishi, T.; Sameshima, T.; Totsuka, T.; Yamasaki, T.; Koizumi, S.; Namba, H. Cosmetic and Neuroprotective Placement of Custom-Made Ultra-High-Molecular-Weight Polyethylene Cranial Plate (SKULPIO) in Single-Step Surgery: Technical Note and Case Report. World Neurosurg. 2019, 130, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Fricia, M.; Nicolosi, F.; Ganau, M.; Cebula, H.; Todeschi, J.; Santin, M.D.N.; Nannavecchia, B.; Morselli, C.; Chibbaro, S. Cranioplasty with Porous Hydroxyapatite Custom-Made Bone Flap: Results from a Multicenter Study Enrolling 149 Patients Over 15 Years. World Neurosurg. 2019, 121, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Condino, S.; Montemurro, N.; Cattari, N.; D’Amato, R.; Thomale, U.; Ferrari, V.; Cutolo, F. Evaluation of a Wearable AR Platform for Guiding Complex Craniotomies in Neurosurgery. Ann. Biomed. Eng. 2021. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef] [PubMed]
- Cutolo, F.; Fida, B.; Cattari, N.; Ferrari, V. Software framework for customized augmented reality headsets in medicine. IEEE Access 2020, 8, 706–720. [Google Scholar] [CrossRef]
- Condino, S.; Fida, B.; Carbone, M.; Cercenelli, L.; Badiali, G.; Ferrari, V.; Cutolo, F. Wearable Augmented Reality Platform for Aiding Complex 3D Trajectory Tracing. Sensors 2020, 20, 1612. [Google Scholar] [CrossRef] [Green Version]
- Schwam, Z.G.; Kaul, V.F.; Bu, D.D.; Iloreta, A.C.; Bederson, J.B.; Perez, E.; Cosetti, M.K.; Wanna, G.B. The utility of augmented reality in lateral skull base surgery: A preliminary report. Am. J. Otolaryngol. 2021, 42, 102942. [Google Scholar] [CrossRef]
- Meola, A.; Cutolo, F.; Carbone, M.; Cagnazzo, F.; Ferrari, M.; Ferrari, V. Augmented reality in neurosurgery: A systematic review. Neurosurg. Rev. 2017, 40, 537–548. [Google Scholar] [CrossRef] [PubMed]
- Roberts, D.W.; Strohbehn, J.W.; Hatch, J.F.; Murray, W.; Kettenberger, H. A frameless stereotaxic integration of computerized tomographic imaging and the operating microscope. J. Neurosurg. 1986, 65, 545–549. [Google Scholar] [CrossRef] [PubMed]
- Henn, J.S.; Lemole, G.M., Jr.; Ferreira, M.A.; Gonzalez, L.F.; Schornak, M.; Preul, M.C.; Spetzler, R. Interactive stereoscopic virtual reality: A new tool for neurosurgical education. Technical note. J. Neurosurg. 2002, 96, 144–149. [Google Scholar] [CrossRef]
- Perin, A.; Galbiati, T.F.; Ayadi, R.; Gambatesa, E.; Orena, E.F.; Riker, N.I.; Silberberg, H.; Sgubin, D.; Meling, T.R.; DiMeco, F. Informed consent through 3D virtual reality: A randomized clinical trial. Acta Neurochir. 2021, 163, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Perin, A.; Galbiati, T.F.; Gambatesa, E.; Ayadi, R.; Orena, E.F.; Cuomo, V.; Riker, N.I.; Falsitta, L.V.; Schembari, S.; Rizzo, S.; et al. Filling the gap between the OR and virtual simulation: A European study on a basic neurosurgical procedure. Acta Neurochir. 2018, 160, 2087–2097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montemurro, N.; Santoro, G.; Marani, W.; Petrella, G. Posttraumatic synchronous double acute epidural hematomas: Two craniotomies, single skin incision. Surg. Neurol. Int. 2020, 11, 435. [Google Scholar] [CrossRef] [PubMed]
- Pelargos, P.E.; Nagasawa, D.T.; Lagman, C.; Tenn, S.; Demos, J.V.; Lee, S.J.; Bui, T.T.; Barnette, N.E.; Bhatt, N.S.; Ung, N.; et al. Utilizing virtual and augmented reality for educational and clinical enhancements in neurosurgery. J. Clin. Neurosci. 2017, 35, 1–4. [Google Scholar] [CrossRef]
- Liu, W.P.; Azizian, M.; Sorger, J.; Taylor, R.H.; Reilly, B.K.; Cleary, K.; Preciado, D. Cadaveric feasibility study of da Vinci Si-assisted cochlear implant with augmented visual navigation for otologic surgery. JAMA Otolaryngol. Head Neck Surg. 2014, 140, 208–214. [Google Scholar] [CrossRef]
- Citardi, M.J.; Agbetoba, A.; Bigcas, J.L.; Luong, A. Augmented reality for endoscopic sinus surgery with surgical navigation: A cadaver study. Int. Forum. Allergy Rhinol. 2016, 6, 523–528. [Google Scholar] [CrossRef]
- Li, L.; Yang, J.; Chu, Y.; Wu, W.; Xue, J.; Liang, P.; Chen, L. A Novel Augmented Reality Navigation System for Endoscopic Sinus and Skull Base Surgery: A Feasibility Study. PLoS ONE 2016, 11, e0146996. [Google Scholar] [CrossRef]
- Besharati Tabrizi, L.; Mahvash, M. Augmented reality-guided neurosurgery: Accuracy and intraoperative application of an image projection technique. J. Neurosurg. 2015, 123, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Mahvash, M.; Besharati Tabrizi, L. A novel augmented reality system of image projection for image-guided neurosurgery. Acta Neurochir. 2013, 155, 943–947. [Google Scholar] [CrossRef]
- Barsom, E.Z.; Graafland, M.; Schijven, M.P. Systematic review on the effectiveness of augmented reality applications in medical training. Surg. Endosc. 2016, 30, 4174–4183. [Google Scholar] [CrossRef] [Green Version]
- Dodier, P.; Winter, F.; Auzinger, T.; Mistelbauer, G.; Frischer, J.M.; Wang, W.T.; Mallouhi, A.; Marik, W.; Wolfsberger, S.; Reissig, L.; et al. Single-stage bone resection and cranioplastic reconstruction: Comparison of a novel software-derived PEEK workflow with the standard reconstructive method. Int. J. Oral Maxillofac. Surg. 2020, 49, 1007–1015. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.; Joldes, G.R.; Bourantas, G.; Warfield, S.K.; Hyde, D.E.; Kikinis, R.; Wittek, A. Biomechanical modeling and computer simulation of the brain during neurosurgery. Int. J. Numer. Method Biomed. Eng. 2019, 35, e3250. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Zhong, Y.; Gu, C. Deformable Models for Surgical Simulation: A Survey. IEEE Rev. Biomed. Eng. 2018, 11, 143–164. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J. A direct Jacobian total Lagrangian explicit dynamics finite element algorithm for real-time simulation of hyperelastic materials. Int. J. Numer. Methods Eng. 2021. [Google Scholar] [CrossRef]
- Fick, T.; van Doormaal, J.A.M.; Hoving, E.W.; Willems, P.W.A.; van Doormaal, T.P.C. Current Accuracy of Augmented Reality Neuronavigation Systems: Systematic Review and Meta-Analysis. World Neurosurg. 2021, 146, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Elmi-Terander, A.; Burström, G.; Nachabé, R.; Fagerlund, M.; Ståhl, F.; Charalampidis, A.; Edström, E.; Gerdhem, P. Augmented reality navigation with intraoperative 3D imaging vs fluoroscopy-assisted free-hand surgery for spine fixation surgery: A matched-control study comparing accuracy. Sci. Rep. 2020, 10, 707. [Google Scholar] [CrossRef] [Green Version]
- Kin, T.; Nakatomi, H.; Shono, N.; Nomura, S.; Saito, T.; Oyama, H.; Saito, N. Neurosurgical Virtual Reality Simulation for Brain Tumor Using High-definition Computer Graphics: A Review of the Literature. Neurol. Med. Chir. 2017, 57, 513–520. [Google Scholar] [CrossRef] [Green Version]
- Mikhail, M.; Mithani, K.; Ibrahim, G.M. Presurgical and Intraoperative Augmented Reality in Neuro-Oncologic Surgery: Clinical Experiences and Limitations. World Neurosurg. 2019, 128, 268–276. [Google Scholar] [CrossRef] [PubMed]
- Canseco, J.A.; Schroeder, G.D.; Patel, P.D.; Grasso, G.; Chang, M.; Kandziora, F.; Vialle, E.N.; Oner, F.C.; Schnake, K.J.; Dvorak, M.F.; et al. Regional and experiential differences in surgeon preference for the treatment of cervical facet injuries: A case study survey with the AO Spine Cervical Classification Validation Group. Eur. Spine J. 2021, 30, 517–523. [Google Scholar] [CrossRef]
- Alfonso-Garcia, A.; Bec, J.; Sridharan Weaver, S.; Hartl, B.; Unger, J.; Bobinski, M.; Lechpammer, M.; Girgis, F.; Boggan, J.; Marcu, L.; et al. Real-time augmented reality for delineation of surgical margins during neurosurgery using autofluorescence lifetime contrast. J. Biophotonics 2020, 13, e201900108. [Google Scholar] [CrossRef] [PubMed]
- Van Doormaal, T.P.C.; van Doormaal, J.A.M.; Mensink, T. Clinical Accuracy of Holographic Navigation Using Point-Based Registration on Augmented-Reality Glasses. Oper. Neurosurg. 2019, 17, 588–593. [Google Scholar] [CrossRef] [Green Version]
- Cho, J.; Rahimpour, S.; Cutler, A.; Goodwin, C.R.; Lad, S.P.; Codd, P. Enhancing Reality: A Systematic Review of Augmented Reality in Neuronavigation and Education. World Neurosurg. 2020, 139, 186–195. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montemurro, N.; Condino, S.; Cattari, N.; D’Amato, R.; Ferrari, V.; Cutolo, F. Augmented Reality-Assisted Craniotomy for Parasagittal and Convexity En Plaque Meningiomas and Custom-Made Cranio-Plasty: A Preliminary Laboratory Report. Int. J. Environ. Res. Public Health 2021, 18, 9955. https://doi.org/10.3390/ijerph18199955
Montemurro N, Condino S, Cattari N, D’Amato R, Ferrari V, Cutolo F. Augmented Reality-Assisted Craniotomy for Parasagittal and Convexity En Plaque Meningiomas and Custom-Made Cranio-Plasty: A Preliminary Laboratory Report. International Journal of Environmental Research and Public Health. 2021; 18(19):9955. https://doi.org/10.3390/ijerph18199955
Chicago/Turabian StyleMontemurro, Nicola, Sara Condino, Nadia Cattari, Renzo D’Amato, Vincenzo Ferrari, and Fabrizio Cutolo. 2021. "Augmented Reality-Assisted Craniotomy for Parasagittal and Convexity En Plaque Meningiomas and Custom-Made Cranio-Plasty: A Preliminary Laboratory Report" International Journal of Environmental Research and Public Health 18, no. 19: 9955. https://doi.org/10.3390/ijerph18199955