
Occurrence of Mental Illness and Mental Health Risks among the Self-Employed: A Systematic Review

 , , , ,
, , , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
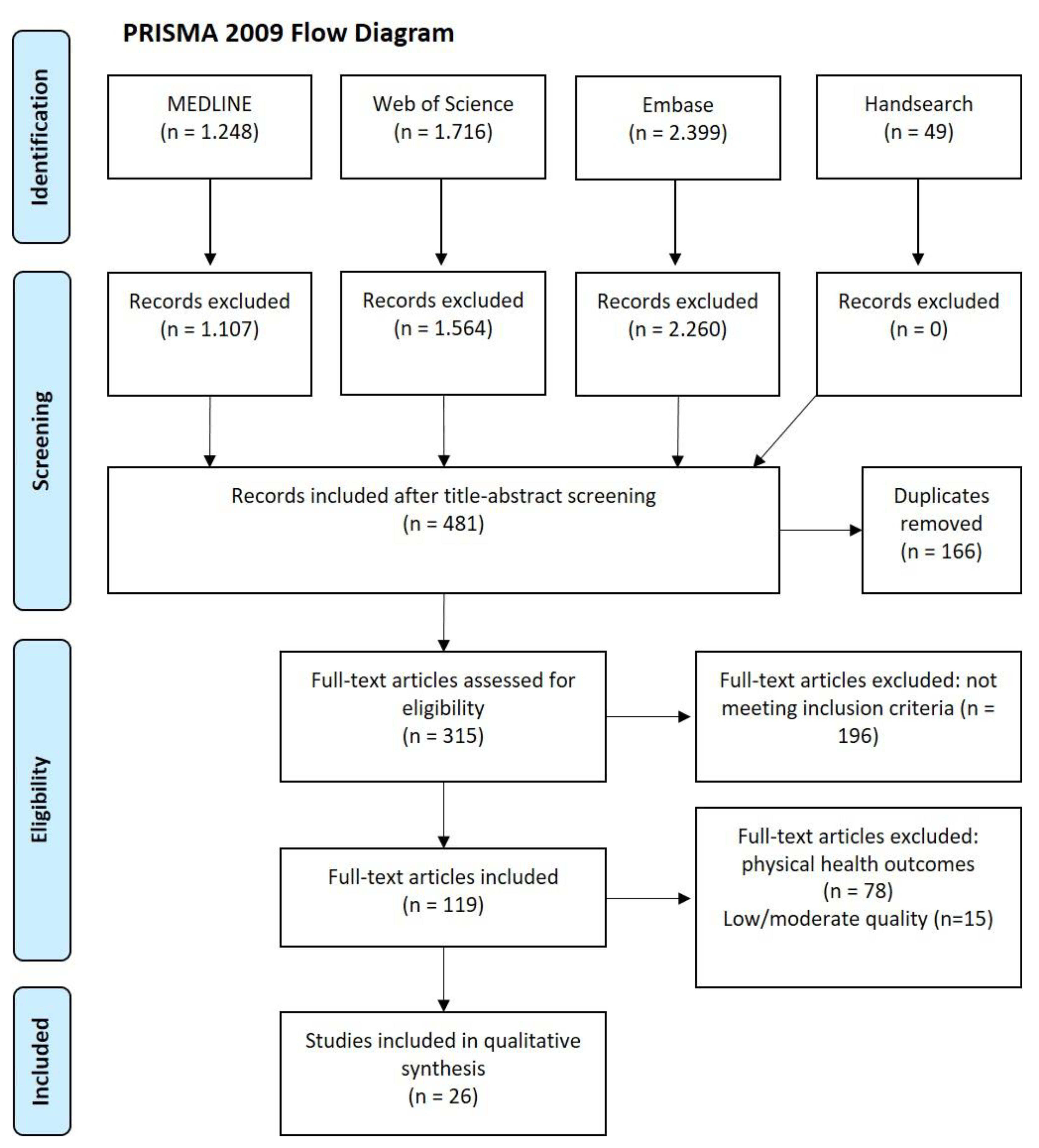
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Assessment of Studies
2.4. Quality Assessment
3. Results
3.1. General Study Characteristics
3.2. Study Population Characteristics
3.3. Assessment of Employment Categories
3.4. Outcome Measures
3.5. Incidence of Mental Disorders in Longitudinal Studies
3.6. Prevalence of Mental Disorders in Cross-Sectional Studies
3.6.1. Mental Illness (at Least One)
3.6.2. Depression
3.6.3. Suicidal Thoughts
3.6.4. Anxiety
3.6.5. Stress, Exhaustion, Burnout
3.6.6. Self-Rated Poor General Mental Health
4. Discussion
4.1. Main Findings
4.2. Comparison of Studies
4.2.1. Longitudinal Studies
4.2.2. Cross-Sectional Studies
4.3. Strengths and Potential Limitations
4.4. Implications and Outlook
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Labour Organization. ILOSTAT Database. 2020; Available online: https://data.worldbank.org/indicator/SL.EMP.SELF.ZS (accessed on 28 April 2020).
- OECD. Self-Employment-Rate (indicator)//Employment. 2020; Available online: https://data.oecd.org/emp/self-employment-rate.htm (accessed on 28 April 2020).
- Schonfeld, I.S.; Mazzola, J.J. A qualitative study of stress in individuals self-employed in solo businesses. J. Occup. Health Psychol. 2015, 20, 501–513. [Google Scholar] [CrossRef] [PubMed]
- Sewdas, R.; Tamminga, S.J.; Boot, C.R.L.; van den Heuvel, S.G.; de Boer, A.G.; van der Beek, A.J. Differences in self-rated health and work ability between self-employed workers and employees: Results from a prospective cohort study in the Netherlands. PLoS ONE 2018, 13, e0206618. [Google Scholar] [CrossRef] [PubMed]
- Oren, L. Job stress and coping: Self-employed versus organizationally employed professionals. Stress Health J. Int. Soc. Investig. Stress 2012, 28, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Aronsson, G. Sick but yet at work. An empirical study of sickness presenteeism. J. Epidemiol. Community Health 2000, 54, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Cocker, F.; Martin, A.; Scott, J.; Venn, A.; Sanderson, K. Psychological distress, related work attendance, and productivity loss in small-to-medium enterprise owner/managers. Int. J. Environ. Res. Public Health 2013, 10, 5062–5082. [Google Scholar] [CrossRef]
- Leignel, S.; Schuster, J.-P.; Hoertel, N.; Poulain, X.; Limosin, F. Mental health and substance use among self-employed lawyers and pharmacists. Occup. Med. 2014, 64, 166–171. [Google Scholar] [CrossRef]
- Chin, B.; Slutsky, J.; Raye, J.; Creswell, J.D. Mindfulness Training Reduces Stress At Work: A Randomized Controlled Trial. Mindfulness 2019, 10, 627–638. [Google Scholar] [CrossRef]
- Plaisier, I.; de Graaf, R.; de Bruijn, J.; Smit, J.; van Dyck, R.; Beekman, A.; Penninx, B. Depressive and anxiety disorders on-the-job: The importance of job characteristics for good work functioning in persons with depressive and anxiety disorders. Psychiatry Res. 2012, 200, 382–388. [Google Scholar] [CrossRef]
- Cardon, M.S.; Patel, P.C. Is Stress Worth it? Stress-Related Health and Wealth Trade-Offs for Entrepreneurs. Appl. Psychol. 2015, 64, 379–420. [Google Scholar] [CrossRef]
- Grégoris, M.; Deschamps, F.; Salles, J.; Sanchez, S. Health assessment of self-employed in the food service industry. Int. J. Occup. Environ. Health 2017, 23, 234–242. [Google Scholar] [CrossRef] [PubMed]
- Gehring, T.M.; Aubert, L.; Padlina, O.; Martin-Diener, E.; Somaini, B. Perceived stress and health-related outcomes in a Swiss population sample. Swiss J. Psychol. 2001, 60, 27–34. [Google Scholar] [CrossRef]
- Benavides, F.G.; Benach, J.; Diez-Roux, A.V.; Roman, C. How do types of employment relate to health indicators? Findings from the Second European Survey on Working Conditions. J. Epidemiol Community Health 2000, 54, 494–501. [Google Scholar] [CrossRef]
- Stahmeyer, J.T.; Kuhlmann, K.; Eberhard, S. Die Häufigkeit von Depressionsdiagnosen nach Versichertengruppen im Zeitverlauf—Eine Routinedatenanalyse der Jahre 2006–2015. Psychother. Psychosom. Med. Psychol. 2019, 69, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Samuelsson, Å.; Alexanderson, K.; Ropponen, A.; Lichtenstein, P.; Svedberg, P. Incidence of disability pension and associations with socio-demographic factors in a Swedish twin cohort. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 47, 1999–2009. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-J.; Min, J.-Y.; Min, K.-B. Physical and mental health problems of self-employed small business owners in South Korea. Am. J. Ind. Med. 2019, 62, 783–790. [Google Scholar] [CrossRef]
- Kim, T.; Kang, M.-Y.; Yoo, M.-S.; Lee, D.; Hong, Y.-C. Computer use at work is associated with self-reported depressive and anxiety disorder. Ann. Occup. Environ. Med. 2016, 28, 57. [Google Scholar] [CrossRef]
- Sakisaka, K. Identification of high risk groups with shorter survival times after onset of the main reason for suicide: Findings from interviews with the bereaved in Japan. BMC Res. Notes 2018, 11, 553. [Google Scholar] [CrossRef] [PubMed]
- Mofidi, N.; Ghazinour, M.; Araste, M.; Jacobsson, L.; Richter, J. General mental health, quality of life and suicide-related attitudes among Kurdish people in Iran. Int. J. Soc. Psychiatry 2008, 54, 457–468. [Google Scholar] [CrossRef]
- Hounsome, B.; Edwards, R.T.; Hounsome, N.; Edwards-Jones, G. Psychological morbidity of farmers and non-farming population: Results from a UK survey. Community Ment. Health J. 2012, 48, 503–510. [Google Scholar] [CrossRef]
- Kameyama, A.; Matsumoto, T.; Katsumata, Y.; Akazawa, M.; Kitani, M.; Hirokawa, S.; Takeshima, T. Psychosocial and psychiatric aspects of suicide completers with unmanageable debt: A psychological autopsy study. Psychiatry Clin. Neurosci. 2011, 65, 592–595. [Google Scholar] [CrossRef]
- Min, J.-Y.; Kim, H.; Park, S.-G.; Hwang, S.H.; Min, K.-B. Differences in suicidal behaviors between self-employed and standardly employed workers. Am. J. Ind. Med. 2019, 62, 1144–1151. [Google Scholar] [CrossRef]
- Yoon, C.-G.; Bae, K.-J.; Kang, M.-Y.; Yoon, J.-H. Is suicidal ideation linked to working hours and shift work in Korea? J. Occup. Health 2015, 57, 222–229. [Google Scholar] [CrossRef]
- Stephan, U.; Roesler, U. Health of entrepreneurs versus employees in a national representative sample. J. Occup. Organ. Psychol. 2010, 83, 717–738. [Google Scholar] [CrossRef]
- International Labour Office. Universal Social Protection to Achieve the Sustainable Development Goals; International Labour Office: Geneva, Switzerland, 2017. [Google Scholar]
- Higgins, J.; Thomas, J. Cochrane Handbook for Systematic Reviews of Interventions, Version 6; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2019; Available online: https://training.cochrane.org/handbook/current (accessed on 4 May 2020).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Available online: http://www.prisma-statement.org/ (accessed on 4 May 2020).
- Hoy, D.; Brooks, P.; Woolf, A.; Blyth, F.; March, L.; Bain, C.; Baker, P.; Smith, E.; Buchbinder, R. Assessing risk of bias in prevalence studies: Modification of an existing tool and evidence of interrater agreement. J. Clin. Epidemiol. 2012, 65, 934–939. [Google Scholar] [CrossRef]
- Tiikkaja, S.; Sandin, S.; Malki, N.; Modin, B.; Sparén, P.; Hultman, C.M. Social class, social mobility and risk of psychiatric disorder—A population-based longitudinal study. PLoS ONE 2013, 8, e77975. [Google Scholar] [CrossRef]
- Jang, S.-Y.; Jang, S.-I.; Bae, H.-C.; Shin, J.; Park, E.-C. Precarious employment and new-onset severe depressive symptoms: A population-based prospective study in South Korea. Scand. J. Work. Environ. Health 2015, 41, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Cambois, E.; Garrouste, C.; Pailhé, A. Gender career divide and women’s disadvantage in depressive symptoms and physical limitations in France. SSM Popul. Health 2017, 3, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Rosta, J.; Tellnes, G.; Aasland, O.G. Differences in sickness absence between self-employed and employed doctors: A cross-sectional study on national sample of Norwegian doctors in 2010. BMC health Serv. Res. 2014, 14, 199. [Google Scholar] [CrossRef] [PubMed]
- Lindström, M.; Ali, S.M.; Rosvall, M. Socioeconomic status, labour market connection, and self-rated psychological health: The role of social capital and economic stress. Scand. J. Public Health 2012, 40, 51–60. [Google Scholar] [CrossRef]
- Samuelsson, Å.; Houkes, I.; Verdonk, P.; Hammarström, A. Types of employment and their associations with work characteristics and health in Swedish women and men. Scand. J. Public Health 2012, 40, 183–190. [Google Scholar] [CrossRef]
- Heinke, W.; Dunkel, P.; Brähler, E.; Nübling, M.; Riedel-Heller, S.; Kaisers, U.X. Burn-out in der Anästhesie und Intensivmedizin: Gibt es ein Problem in Deutschland? Anaesthesist 2011, 60, 1109–1118. [Google Scholar] [CrossRef]
- Saarni, S.I.; Saarni, E.S.; Saarni, H. Quality of life, work ability, and self employment: A population survey of entrepreneurs, farmers, and salary earners. Occup. Environ. Med. 2008, 65, 98–103. [Google Scholar] [CrossRef]
- Muntaner, C.; Borrell, C.; Benach, J.; Pasarín, M.I.; Fernandez, E. The associations of social class and social stratification with patterns of general and mental health in a Spanish population. Int. J. Epidemiol. 2003, 32, 950–958. [Google Scholar] [CrossRef]
- Park, J.; Han, B.; Kim, Y. Comparison of occupational health problems of employees and self-employed individuals who work in different fields. Arch. Environ. Occup. Health 2019, 75, 98–111. [Google Scholar] [CrossRef]
- Yoon, J.-H.; Jeung, D.; Chang, S.-J. Does High Emotional Demand with Low Job Control Relate to Suicidal Ideation among Service and Sales Workers in Korea? J. Korean Med. Sci. 2016, 31, 1042–1048. [Google Scholar] [CrossRef] [PubMed]
- López-Ruiz, M.; Artazcoz, L.; Martínez, J.M.; Rojas, M.; Benavides, F.G. Informal employment and health status in Central America. BMC Public Health 2015, 15, 698. [Google Scholar] [CrossRef]
- Rietveld, C.A.; van Kippersluis, H.; Thurik, A.R. Self-Employment and Health: Barriers or Benefits? Health Econ. 2015, 24, 1302–1313. [Google Scholar] [CrossRef]
- Merchant, J.A.; Kelly, K.M.; Burmeister, L.F.; Lozier, M.J.; Amendola, A.; Lind, D.P.; KcKeen, A.; Slater, T.; Hall, J.L.; Rohlman, D.S.; et al. Employment status matters: A statewide survey of quality-of-life, prevention behaviors, and absenteeism and presenteeism. J. Occup. Environ. Med. 2014, 56, 686–698. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.; Bernell, S.L. The effect of self-employment on health, access to care, and health behavior. Health 2013, 5, 2116–2127. [Google Scholar] [CrossRef]
- Hessels, J.; Rietveld, C.A.; van der Zwan, P. Self-employment and work-related stress: The mediating role of job control and job demand. J. Bus. Ventur. 2017, 32, 178–196. [Google Scholar] [CrossRef]
- Parslow, R.A.; Jorm, A.F.; Christensen, H.; Rodgers, B.; Strazdins, L.; D’Souza, R.M. The associations between work stress and mental health: A comparison of organizationally employed and self-employed workers. Work Stress 2004, 18, 231–244. [Google Scholar] [CrossRef]
- Sevä, I.J.; Larsson, D. Are the self-employed really that poor? Income poverty and living standard among self-employed in Sweden. Soc. Health Vulnerability 2015, 6, 26148. [Google Scholar] [CrossRef]
- Europäische Kommission. Bericht des Europäischen Beschäftigungsobservatoriums: Selbstständige Erwerbstätigkeit in Europa 2010; Generaldirektion Beschäftigung, Soziales und Chancengleichheit: Brussels, Belgium, 2010. [Google Scholar]
- Andersson, L.; Nyman, C.S.; Spak, F.; Hensing, G. High incidence of disability pensionwith a psychiatric diagnosis in western Sweden. A population-based study from 1980 to 1998. Work 2006, 26, 343–353. [Google Scholar] [PubMed]
- Andersson, L.; Wiles, N.; Lewis, G.; Brage, S.; Hensing, G. Can access to psychiatric health care explain regional differences in disability pension with psychiatric disorders? Soc. Psychiatry Psychiatr. Epidemiol. 2007, 42, 366–371. [Google Scholar] [CrossRef]
- Österberg, T.; Gustafsson, B. Disability pension among immigrants in Sweden. Soc. Sci. Med. 2006, 63, 805–816. [Google Scholar] [CrossRef]
- Beckman, A.; Hakansson, A.; Rastam, L.; Lithman, T.; Merlo, J. The role country of birth plays in receiving disability pensions in relation to patterns of health care utilisation and socioeconomic differences: A multilevel analysis of Malmo, Sweden. BMC Public Health 2006, 6, 71. [Google Scholar] [CrossRef]
- Cho, M.J.; Kim, K.H. Use of the Center for Epidemiologic Studies Depression (CES-D) Scale in Korea. J. Nerv. Ment. Dis. 1998, 186, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Lenore Sawyer Radloff. The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Eurofoun. Exploring Self-Employment in the European Union; Publications Office of the European Union: Luxembourg, 2017. [Google Scholar]
- § 57 SGB III durch Artikel 1 Nr. 3 Gesetz zur Verbesserung der Eingliederungschancen am Arbeitsmarkt. Available online: https://www.sozialgesetzbuch-sgb.de/sgbiii/443.html (accessed on 4 May 2020).
- Lee, S. Social Security System of South Korea; Inter American Development Bank, Social Protection and Health Division: Washington, DC, USA, 2015. [Google Scholar]
- Social Security Administration. Social Security Programs throughout the World: Asia and the Pacific; Social Securtiy Administration: Woodlawn, MD, USA, 2014. [Google Scholar]
- Selbstständigkeit. Available online: https://www.infobest.eu/de/themengebiete/artikel?tx_infobestfaq_faq%5Baction%5D=list&tx_infobestfaq_faq%5Bcontroller%5D=Article&tx_infobestfaq_faq%5Btag%5D=106&cHash=7631bb277636120b01c384809aaca903 (accessed on 29 July 2021).
- Self-Employed in Crisis. Available online: http://www.koreaherald.com/view.php?ud=20200910000635# (accessed on 9 August 2021).
- Kim, D.I. The Korean labor market: The Crisis and After. Int. Monet. Fund 2002, 8, 261–292. [Google Scholar]
- World Employment and Social Outlook-Trends 2020. Available online: http://www.ilo.org (accessed on 5 August 2021).
- Benzing, C.; Chu, H.M. A comparison of the motivations of small business owners in Africa. J. Small Bus. Enterp. Dev. 2009, 16, 60–77. [Google Scholar] [CrossRef]
- Reinhardt, U.E. Much ado about nothing: The US Supreme Court’s rules on health reform. Health Econ. Policy Low 2013, 8, 125–132. [Google Scholar] [CrossRef]
- Whiteford, P.; Heron, A. Dealing with Non-Standard Work in a General Revenue Financed Social Protection System—The Case of Australia: The Future of Social Protection: What Works for Non-Standard Workers? OECD Publishing: Paris, France, 2018. [Google Scholar]
- Hamilton, B.H. Does entrepreneurship pay? An empirical analyses of the returns to self-employment. J. Polit. Econ. 2000, 108, 604–631. [Google Scholar] [CrossRef]
- Schafstein, S. Money and mental Health. Psychiatr. Serv. 2015, 66, 1257. [Google Scholar] [CrossRef]
- Kawakami, N.; Iwata, N.; Tanigawa, T.; Oga, H.; Araki, S.; Fujihara, S.; Kitamura, T. Prevalence of mood and Anxiety Disorders in a Working Population in Japan. JOEM 1996, 38, 899–905. [Google Scholar] [CrossRef] [PubMed]
- Eurofound and International Labor Organization. Working Conditions in a Global Perspective; Publications Office of the European Union: Luxembourg; Interantional Labour Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Toivanen, S.; Mellner, C.; Vinberg, S. Selfemployed persons in Sweden—Mortality differentials by industrial sector and enterprise legal form: A five-year follow-up study. Am. J. Ind. Med. 2015, 58, 21–32. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.-K.; Lee, C.-H.; pan, C.-H.; Hu, W.-H. Comparison of the prevalence of substance use and psychiatric disorders between government- and self-employed commercial drivers. Psychiatry Clin. Neurosci. 2003, 57, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Sônego, M.; Meller, M.; Massuti, R.; Campani, F.; Amaro, J.; Barbosa, C.; Rohde, L.A. Exploring the association between attention-deficit/hyperactivity disorder and entrepreneurship. Rev. Bras. Psiquiatr. 2020, 43, 174–180. [Google Scholar] [CrossRef]
- Peltonen, J.; Johansson, E.; Wincent, J. Does attention-deficit hyperactivity disorder medication reduce entrepreneurship? Health Econ. 2020, 29, 1071–1077. [Google Scholar] [CrossRef]
- Verheul, I.; Rietdijk, W.; Block, J.; Franken, I.; Larsson, H.; Thurik, R. The association between attention-deficit/hyperactivity (ADHD) symptoms and self-employment. Eur. J. Epidemiol. 2016, 31, 793–801. [Google Scholar] [CrossRef]
- Anker, E.; Halmøy, A.; Heir, T. Work participation in ADHD and associations with social characteristics, education, lifetime depression, and ADHD symptom severity. Atten. Deficit Hyperact. Disord. 2019, 11, 159–165. [Google Scholar] [CrossRef]
- René Böheim, U.M. Dependent Forms of Self-employment in the UK: Identifying Workers on the Border between Employment and Self-employment. J. Labour Mark. Res. 2009, 42, 182–195. [Google Scholar] [CrossRef]
- Westerveld, M. The ‘New’ Self-Employed: An Issue for Social Policy? Eur. J. Soc. Secur. 2012, 14, 156–173. [Google Scholar] [CrossRef]
- Horemans, J.; Marx, I. Poverty and Material Deprivation among the Self-Employed in Europe: An Exploration of a Relatively Uncharted Landscape; IZA Institute of Labor Economics: Bonn, Germany, 2017. [Google Scholar]
- Graeber, D.; Kritikos, A.S.; Seebauer, J. COVID-19: A crisis of the female self-employed. J. Popul. Econ. 2021, 34, 1141–1187. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Risk of Bias Items | Quality Assessment of The Included Studies 0 = Yes (Low Risk of Bias) 1 = No (High Risk of Bias) | |||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tiikkaja 2013 [30] | Samuelsson 2012b [16] | Jang 2015 [31] | Stahmeyer 2019 [15] | Combois 2017 [32] | Rosta 2014 [33] | Lindström 2012 [34] | Samuelsson 2012a [35] | Heinke 2011 [36] | Stephan 2010 [25] | Saarni 2007 [37] | Muntaner 2003 [38] | Gehring 2001 [13] | Benavides 2000 [14] | Kim 2019 [17] | Park 2019 [39] | Kim 2016 [18] | Yoon 2016 [40] | Yoon 2015 [24] | Cardon 2015 [11] | Lopez-Ruiz 2015 [41] | Rietveld 2015 [42] | Merchant 2014 [43] | Yoon 2013 [44] | Hessels 2016 [45] | Parslow 2014 [46] | |
| 1. The study’s target population was a close representation of the national population. | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 1 |
| 2. The sampling frame was a true or close representation of the target population. | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 3. A census was undertaken, OR, some form of random selection was used to select the sample. | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 0 | 0 |
| 4. Was the likelihood of non-response bias minimal (response rate ≥ 75%)? | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| 5. All data were collected directly from the subjects. | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 6. An acceptable case definition was used. | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 0 |
| 7. The study instrument had been shown to have reliability and validity. | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 |
| 8. The same mode of data collection was used for all subjects. | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 9. Were the numerator(s) and denominator(s) for the parameter of interest appropriate? (* = not applicable) | * | 0 | * | 1 | * | * | * | * | 0 | * | * | 0 | 0 | 0 | 1 | 1 | 0 | 0 | * | 0 | 0 | * | 0 | * | * | * |
| Summary 0–3: low risk of bias for studies that reported prevalence estimates; 0–2: low risk of bias for studies that did not report prevalence estimates (assessed by question 9) | 0 | 3 | 2 | 2 | 1 | 2 | 1 | 1 | 1 | 1 | 1 | 2 | 2 | 3 | 3 | 2 | 3 | 3 | 2 | 3 | 2 | 2 | 3 | 2 | 2 | 2 |
| Author, Publication Year [Reference] | Study Design, Country, Recruitment Year | Baseline Number, Age, Females | Follow-Up Length, Last Response | Source Population | Mental Health Outcome Definition | Results |
|---|---|---|---|---|---|---|
| EUROPE | ||||||
| Tiikkaja 2013 [30] | Historic cohort study, Sweden 1980 | n = 1,016,276 range 21–31 y 38% | 25 y, 99% (census 1980), 98% (census 1990) | Censuses data from 1980 & 1990, National Patient and other registers used to identify all working individuals without psychiatric diagnoses in Sweden before 1980 | First hospitalization for a severe psychiatric disorder such as: schizophrenia, alcoholism, drug dependency, affective psychosis, neurosis, or personality disorder | Severe psychiatric disorder (first hospitalization) aRR Empl (high white-collar): 1.0 (ref.-categ.) Empl (low white-collar): 1.34 (95%-CI 1.29–1.40) S-empl: 1.55 (95%-CI 1.47–1.64) Empl (high blue-collar): 1.60 (95%-CI 1.54–1.67) Empl (low blue-collar): 1.98 (95%-CI 1.91–2.05) Incidence rates Empl (high white-collar): 90/100,000 person-years Empl (low white-collar): 121/100,000 person-years S-empl: 152/100,000 person-years Empl (high blue-collar): 165/100,000 person-years Empl (low blue-collar): 189/100,000 person-years |
| Samuelsson 2012b [16] | Register cohort study, Sweden 1993 | n = 52,509 mean 47.8 y 51% | 15 y, 95% | Swedish Twin Registry, Swedish National Social Insurance Agency, Causes of Death Registry | Disability pension due to a mental diagnosis: ICD10: F00–F99 | Mental illness (reason for disability pension) HR adjusted for age only Empl (high white-collar): 0.97 (95%-CI 0.85–1.17) Empl (middle white-collar): 1.0 (ref.-categ.) Empl (low white-collar): 0.89 (95%-CI 0.73–1.09) S-empl: 0.48 (95%-CI 0.35–0.65) Empl (skilled blue-collar): 0.71 (95%-CI 0.57–0.87) Empl (unskilled blue-collar):1.10 (95%-CI 0.93–1.29) Incidence: males 3.3% vs. 12.4%, females 1.5% vs. 19.8% |
| ASIA | ||||||
| Jang 2015 [31] | Cohort study South Korea, 2007 | n = 3981 range 20 y–59 y 45% | 6 y, 77–79% | Korean Welfare Panel Study (KOWEPS) 2007–2013: nationally representative sample | The Center for Epidemiological Studies Depression Scale (South Korean version) | S-empl vs. full time permanently empl (ref.-categ.): Severe depressive symptoms Males aOR: 1.09 (95%-CI 0.71–1.66) Incidence in males: 1.8% vs. 1.5% Females aOR: 1.21 (95%-CI 0.69–2.11) Incidence in females: 3.0% vs. 1.9% |
| Author, Publication Date [Reference] | Country/Region of Study | Sample size, Female | Age [Mean (SD) or Range] | Source Population | Occupational Groups | Disease Outcomes: Assessment Tools |
|---|---|---|---|---|---|---|
| EUROPE | ||||||
| Stahmeyer 2019 [15] | Germany/Lower Saxony (federal state in Northern Germany) | 1,838,965 (2015), 1,667,495 (2006), 52.3% | 43.8 (19.2) y (2015), n.r. (2006) | Largest statutory health insurance company in federal state Lower Saxony: routine care data | s-empl vs. empl | Depressive episode/Depressive disease (physician’s diagnosis): ICD-10: F32, F33 |
| Cambois 2017 [32] | France | 7537, 53% | 45–74 y | French Population Survey 2006 | s-empl (farm/business owner) vs. empl (low-skilled clerical) vs. empl (unskilled clerical) vs. empl (manual workers) | Depressive symptoms: Mini International Neuropsychiatric Interview (MINI) |
| Rosta 2014 [33] | Norway | 834, 23.8% (s-empl) 43.0% (empl) | 29–67 y | Research Institute of the Norwegian Medical Association: Active Norwegian doctors | s-empl (doctors) vs. empl (doctors) | Psychological stress at work: short form of the effort-reward questionnaire (ERI) |
| Lindström 2012 [34] | Sweden | 28,198, 54.9% | 18–80 y | Public health survey in Skane 2008: randomly selected from the official population registers of people living in Skane | s-empl vs. empl (high non-manual worker) | Self-rated mental health: 12-Item General Health Questionnaire (GHQ-12) |
| Samuelsson 2012a [35] | Sweden | 877, 46% | 42 y | School leavers in Lulea City | s-empl vs. empl (temporary) vs. empl (permanent) | Exhaustion: Subscale of the Swedish Maslach Burnout Inventory |
| Heinke 2011 [36] | Germany | 3541, 32.7% | 44 (8.5) y | Professional Association of German Anaesthetists and German Society for Anaesthesiology and Intensive Care (DGAI) | s-empl (anaesthetists) vs. empl (anaesthetists) | Burn-Out-Syndrome: BOS-Sum-Score (Copenhagen Psychosocial Questionnaire CAPSOQ) |
| Stephan 2010 [25] | Germany | 298, 26.5% | 46.2 (8.7) y | Matched case-control design with participants from German National Health Survey 1998 | s-empl vs. empl | 1. Somatic diseases: ICD-10 2. Mental disorders: DIA-X-Munich Composite International Diagnostic Interview (DIA-X-M-CIDI) |
| Saarni 2007 [37] | Finland | 5184, 50% | 46 (38–53) y | Health 2000 survey: two stage stratified cluster sampling | s-empl (without personnel) vs. s-empl (with personnel) vs. empl | 1. Mental function, depression, distress: 15D 2. Anxiety and or depression: EQ-5D |
| Muntaner 2003 [38] | Spain | 4219, 44.4% | 16–64 y | Non-institutionalised population of Barcelona City in 2000 | s-empl (small enterprise) vs. empl (organizational non-managerial supervisors) | Self-rated mental health: 12-Item General Health Questionnaire (GHQ-12) |
| Gehring 2001 [13] | Switzerland | 1200, 60% | 15–74 y | Random sample of native speakers drawn from the Swiss telephone directory | s-empl vs. empl (with low responsibilities) | Perceived stress: “yes/no”—question |
| Benavides 2000 [14] | Spain | 15,146, n.r. | >15 y | Multi-stage random sample of the working population of 15 EU-countries (1000 cases per country) | s-empl (without personnel) vs. s-empl (with personnel) vs. empl (permanent) | Stress, fatigue: New questionnaire developed for the study |
| ASIA | ||||||
| Kim 2019 [17] | South Korea | 32,630, 40.5% | 20–59 y | Third Korean Working conditions Survey (KWCS, 2011) | s-empl (small business owners) vs. empl (full-time) | Mental well-being: WHO-5 well-being index |
| Park 2019 [39] | South Korea | 44,266, 48.1% | n.r. | Fourth Korean Working conditions Survey (KWCS, 2014) | s-empl vs. empl (mental vs. emotional vs. physical work) | Mental well-being: WHO-5 well-being index |
| Kim 2016 [18] | South Korea | 48,850, 42.2% | 45.8 (13.1) y | Third Korean Working conditions Survey (KWCS, 2011) | s-empl vs. empl (full-time) | Depressive and anxiety disorder: “yes/no”-question |
| Yoon 2016 [40] | South Korea | 1995, 58.7% | n.r. | 4th Korea National Health and Nutrition Examination Survey (KNHANES) | s-empl vs. empl | Suicidal ideation: “yes/no”-question |
| Yoon 2015 [24] | South Korea | 67,471, 35.5% | n.r. | 2008 CHS conducted by the Korea Center for Disease Control and Prevention (KCDC) | s-empl vs. empl | Suicidal ideation: “yes/no”-question |
| NORTH and CENTRAL AMERICA | ||||||
| Cardon 2015 [11] | USA (New York, Indiana) | 1376, n.r. | 25–74 y | NHANES I Epidemiologic Follow-up Study (NHEFS) | s-empl vs. empl | Stress: (a) General Well-Being Schedule, (b) Centre for Epidemiological Studies-Depression Scale (CES-D) |
| Lopez-Ruiz 2015 [41] | Central America (Authors: Spain) | 8823, 48.5% | >18 y | First Central American Survey of Working Conditions and Health (Spanish acronym: ECCTS) | s-empl (without personnel) vs. s-empl (<5 employees) vs. empl | Mental health: 12-Item General Health Questionnaire (GHQ-12) |
| Rietveld 2015 [42] | USA (Authors: Netherlands) | 30,671, 58% | 56.7 (5.0) y (s-empl) 55.9 (5.2) y (empl) | US Health and Retirement study (HRS): representative sample of Americans over 50 years | s-empl vs. empl | Depression: Center for Epidemiologic Studies Depression Scale (CES-D) from 0 (absence of depression symptoms) to 8 (presence of all measured depression symptoms) |
| Merchant 2014 [43] | USA (Iowa) | 1271, 53.4% (s-empl) 66.2% (empl) | 18–68 y | 2010 Iowa Voter Registration database | s-empl vs. empl (organizational) | Quality of Life: Real Iowans Health Survey Questionnaire |
| Yoon 2013 [44] | USA (Oregon) | 13,435, n.r. | 45.1 (10.8) y (s-empl) 39.6 (12.2) y (empl) | 2007 Survey MEPS | s-empl vs. empl | 1. Mental health: Mental Health Composite Score, 2. Stress: Kessler Psychological Distress Scale (K10) |
| AUSTRALIA | ||||||
| Hessels 2016 [45] | Australia | 68,264, 63% (s-empl) 50% (empl) | 18–64 y | HILDA (Household, Income and Labour Dynamics in Australia) survey: working individuals | s-empl (without employees) vs. s-empl (with employees) vs. empl | Work-related stress: 2-item 7-point Likert scale |
| Parslow 2014 [46] | Australia (Author: United Kingdom) | 2530, n.r. | 40–44 y | Australian Electoral Rolls for Canberra in the Australian Capital Territory and adjacent town of Queanbeyan in New South Wales | s-empl (without personnel) vs. s-empl (with personnel) vs. empl (organizational) | Depression and/or anxiety: Goldberg’s depression and anxiety scale |
| Study Design | Author/ Publication Date [Reference] | Mental Illness (at Least One) | Depression or Suicidal Thoughts | Anxiety | Stress or Exhaustion or Burnout | Self-Rated Poor General Mental Health | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Longitudinal | EUROPE | |||||||||||
| Tiikkaja 2013 [30] | vs blue-collar | vs white- collar | ||||||||||
| Samuelsson 2012b [16] | vs blue -collar | vs white-collar | ||||||||||
| ASIA | ||||||||||||
| Jang 2015 [31] | ||||||||||||
| Cross-sectional | EUROPE | |||||||||||
| Stahmeyer 2019 (data 2015) [15] | female | male | ||||||||||
| Cambois 2017 [32] | female | male | ||||||||||
| Rosta 2014 [33] | ||||||||||||
| Lindström 2012 [34] | ||||||||||||
| Samuelsson 2012a [35] | Exhaust. (female) | Exhaust. (male) | ||||||||||
| Heinke 2011 [36] | Burnout | |||||||||||
| Stephan 2010 [25] | ||||||||||||
| Saarni 2007 [37] | sole | non-sole | farm | |||||||||
| Stahmeyer 2019 (data 2006) [15] | female | male | ||||||||||
| Muntaner 2003 [38] | ||||||||||||
| Gehring 2001 [13] | ||||||||||||
| Benavides 2000 [14] | sole | non- sole | ||||||||||
| ASIA | ||||||||||||
| Kim 2019 [17] | ||||||||||||
| Park 2019 [39] | ||||||||||||
| Kim 2016 [18] | ||||||||||||
| Yoon 2016 [40] | Suicidal thoughts | |||||||||||
| Yoon 2015 [24] | Suicidal thoughts | |||||||||||
| NORTH and CENTRAL AMERICA | ||||||||||||
| Cardon 2015 [11] | ||||||||||||
| Lopez-Ruiz 2015 [41] | ||||||||||||
| Rietveld 2015 [42] | ||||||||||||
| Merchant 2014 [43] | ||||||||||||
| Yoon 2013 [44] | ||||||||||||
| AUSTRALIA | ||||||||||||
| Hessels 2016 [45] | sole | non- sole | ||||||||||
| Parslow 2014 [46] | sole | non- sole | sole | non- sole | ||||||||
 = significantly lower occurrence;
= significantly lower occurrence;  = lower occurrence;
= lower occurrence;  = no difference;
= no difference;  = higher occurrence;
= higher occurrence;  = significantly higher occurrence, compared to the employed. Self-employment subgroups: “sole” = sole proprietorship (vs the employed); “non-sole” = employing others (vs the employed); “farm” = farm workers.
= significantly higher occurrence, compared to the employed. Self-employment subgroups: “sole” = sole proprietorship (vs the employed); “non-sole” = employing others (vs the employed); “farm” = farm workers.| Author, Publication Date [Reference] | Results |
|---|---|
| Stephan 2010 [25] | 1. Mental disorders s-empl vs. empl (ref.): OR 0.58 (95%-CI 0.36–0.93) * 2. Somatoform disorders s-empl vs. empl (ref.): OR 0.29 (95%-CI 0.11–0.75) * 3. Affective disorders s-empl vs. empl (ref.): OR 0.96 (95%-CI 0.47–1.94) 4. Substance abuse/dependence s-empl vs. empl (ref.): OR 1.08 (95%-CI 0.35–3.31) |
| Author, Publication Date [Reference] | Results |
|---|---|
| Kim 2019 [17] | Depression s-empl vs. empl (ref.): 15.9% vs. 12.1%, OR 1.20 (95%-CI 1.09–1.32) * |
| Stahmeyer 2019 [15] | Depression s-empl vs. empl: Male (2006): 4.5% vs. 3.8%; Female (2006): 11.1% vs. 10.9% Male (2015): 5.1% vs. 5.9%; Female (2015): 13.6% vs. 15.2% |
| Cambois 2017 [32] | Major depressive episodes s-empl vs. empl (ref.): male: OR 0.47; female: OR 1.76 |
| Rietveld 2015 [42] | Depression symptoms s-empl vs. empl [0 (absence of depression symptoms) to 8 (presence of all measured depression symptoms)] Mean 0.56 (SD 0.50) vs. Mean 0.54 (SD 0.50) |
| Parslow 2014 [46] | Depression s-empl (without personnel) vs. s-empl (with personnel) vs. empl (ref.): male [Mean(β)]: 2.09 (−0.261) vs. 2.27 (−0.295) vs. 2.21, female [Mean(β)]: 2.61 (0.271) vs. 2.5 (0.216) vs. 2.44 |
| Author, Publication Date [Reference] | Results |
|---|---|
| Yoon J-H 2016 [40] | Suicidal ideation s-empl vs. empl: male: 8.7% vs. 10.9% female: 18.1% vs. 22.1% |
| Yoon C-G 2015 [24] | Suicidal ideation s-empl vs. empl: male: 5.4% vs. 3.7% * female: 11.3% vs. 8.3% * |
| Author, Publication Date [Reference] | Results |
|---|---|
| Stephan 2010 [25] | Anxiety disorders s-empl vs. empl (ref.): OR 0.92 (95%-CI 0.43–1.97) |
| Parslow 2004 [46] | Anxiety s-empl (without personnel) vs. s-empl (with personnel) vs. empl (ref.): male [Mean(β)]: 3.25 (−0.276) vs. 2.89 (−0.310) vs. 3.21, female [Mean(β)]: 3.84 (0.105) vs. 3.63 (0.069) vs. 3.60 |
| Author, Publication Date [Reference] | Results |
|---|---|
| Hessels 2016 [45] | Work-related stress s-empl (without personnel) and s-empl (with personnel) vs. empl [Mean(SD); 7-point Likert scale (1 = no stress; 7 = extreme stress)]: 2.49 (1.38) * and 2.91 (1.47) vs. 2.78 (1.45) |
| Cardon 2015 [11] | Stress level (subjective) s-empl vs. empl (ref.) (data from 1987): 0.136 |
| Rosta 2014 [33] | High levels of psychosocial work stress s-empl vs. empl: 11.4% vs. 24.3% * |
| Yoon 2013 [44] | Psychological distress s-empl vs. empl (ref.) [Mean(SD); logarithm of Kessler Psychological Distress Scale (10 = no distress; 50 = extreme distress)]: 0.97 (0.80) vs. 0.99 (0.83) |
| Samuelsson 2012a [35] | Exhaustion s-empl vs. empl (temporary) vs. empl (permanent) [Mean; subscale of the Swedish Maslach Burnout Inventory (1 = no exhaustion; 6 = extreme exhaustion)]: male: 1.95 vs. 2.06 vs. 2.09 female: 2.28 vs. 2.26 vs. 2.32 |
| Heinke 2011 [36] | Burn-Out-Symptom s-empl (physician) vs. empl (physician) [Mean(SD); Personal Burnout Scale of the Copenhagen Burnout Inventory (12 = no burn-out symptom; 60 = extreme burn-out symptom)]: 38.1 (20.5) * vs. 43.0 (19.2) Burn-Out-Symptom s-empl (free-lance/established doctor) vs. empl (private/public/university hospital): 30.5%/33.2% vs. 40.8%/40.9%/42.8% |
| Gehring 2001 [13] | Perceived stress s-empl vs. empl (ref.): 47.1% vs. 35.7%; OR 2.10 (95%-CI 1.30–3.41) * |
| Benavides 2000 [14] | Stress s-empl without and with personnel vs. empl (full-time, ref.): 32.3% and 34.3% * vs. 29.5% |
| Author, Publication Date [Reference] | Results |
|---|---|
| Park 2019 [39] | Self-rated poor general mental health s-empl vs. empl: male non-manual workers with cognitive demands: 36.0% vs. 31.0% *, female non-manual workers with cognitive demands: 33.1% vs. 31.0% male service and sales workers: 44.0% vs. 36.0% *, female service and sales workers: 45.7% vs. 40.3% * male manual workers: 53.2% vs. 47.0% *, female manual workers: 59.9% vs. 52.9% * |
| Kim 2016 [18] | Depression and anxiety disorder s-empl vs. empl: 1.69% vs. 1.25% * |
| Lopez-Ruiz 2015 [41] | Self-rated poor general mental health s-empl (without personnel) and s-empl (<5 employees) vs. empl (ref.) (women/men): 34%/29%; 28%/27%; 27%/24%; aOR 1.27 (95%-CI 1.05–1.54) and aOR 1.33 (1.07–1.65) vs. OR 1.00 (ref.) |
| Merchant 2014 [43] | No days with mental health problems (last 4 months) s-empl vs. empl (organizational): 68.1% vs. 65.3% No days with sad feelings (last 4 months) s-empl vs. empl (organizational): 67.4% vs. 64.9% No days with worries/tension (last 4 months) s-empl vs. empl (organizational): 43.5% vs. 39.9% |
| Yoon 2013 [44] | Perceived mental health s-empl vs. empl (ref.) [Mean(SD); 5-point Likert scale (1 = worst mental health; 5 = good mental health)]: 4.11 (0.90) vs. 4.04 (0.20); effect size (aSE) 0.176 (0.097) |
| Lindström 2012 [34] | Self-rated poor general mental health s-empl vs. empl (high-level white-collar = ref.): men: 11.5% vs. 13.1%; aOR 0.75 (95%-CI 0.56–0.99) women: 15.0% vs. 16.7%; aOR 0.77 (95%-CI 0.57–1.06) |
| Saarni 2007 [37] | Self-reported anxiety and/or depression s-empl (without personnel), s-empl (with personnel) and farmers vs. empl (ref.): OR 1.39 (95%-CI 0.75–0.56), OR 0.67 (0.35–1.28) and OR 1.05 (0.51–2.16) vs. OR 1.00 (ref.) |
| Muntaner 2003 [38] | Self-rated poor general mental health s-empl (of small enterprise) vs. empl (skilled supervisors = ref.): men: 10.1% vs. 6.6%; aOR 1.98 (95%-CI 0.83–4.73) women: 15.0% vs. 8.2%; aOR 2.51 (95%-CI 0.88–7.17) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Willeke, K.; Janson, P.; Zink, K.; Stupp, C.; Kittel-Schneider, S.; Berghöfer, A.; Ewert, T.; King, R.; Heuschmann, P.U.; Zapf, A.; et al. Occurrence of Mental Illness and Mental Health Risks among the Self-Employed: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 8617. https://doi.org/10.3390/ijerph18168617
Willeke K, Janson P, Zink K, Stupp C, Kittel-Schneider S, Berghöfer A, Ewert T, King R, Heuschmann PU, Zapf A, et al. Occurrence of Mental Illness and Mental Health Risks among the Self-Employed: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(16):8617. https://doi.org/10.3390/ijerph18168617
Chicago/Turabian StyleWilleke, Kristina, Patrick Janson, Katharina Zink, Carolin Stupp, Sarah Kittel-Schneider, Anne Berghöfer, Thomas Ewert, Ryan King, Peter U. Heuschmann, Andreas Zapf, and et al. 2021. "Occurrence of Mental Illness and Mental Health Risks among the Self-Employed: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 16: 8617. https://doi.org/10.3390/ijerph18168617
APA StyleWilleke, K., Janson, P., Zink, K., Stupp, C., Kittel-Schneider, S., Berghöfer, A., Ewert, T., King, R., Heuschmann, P. U., Zapf, A., Wildner, M., & Keil, T. (2021). Occurrence of Mental Illness and Mental Health Risks among the Self-Employed: A Systematic Review. International Journal of Environmental Research and Public Health, 18(16), 8617. https://doi.org/10.3390/ijerph18168617