
Measuring Electromechanical Coupling in Patients with Coronary Artery Disease and Healthy Subjects


Abstract
:1. Introduction
2. Algorithms of Coupling Measurements
2.1. Linear Measurements
2.1.1. Correlation Coefficient (CC)
2.1.2. Coherence Function (CF)
2.2. Nonlinear Measurements
2.2.1. Mutual Information (MI)
2.2.2. Cross-Conditional Entropy (XCE)
- (1)
- Coarse-grainingThe full range of time series is divided into a fixed number of values labeled from zero to . The coarse-graining resolution thus equals . It renders and sequences of symbols and , .
- (2)
- State space reconstructionForm and by:respectively, where .
- (3)
- EncodingThe vectors and can be codified in decimal format as:thus rendering each sequence of vectors and series of integer numbers and with ranging from zero to , and ranging from zero to .
- (4)
- Probability estimationEstimate the probability of each possible value for and by the corresponding frequency.
- (5)
- XCE calculationDefine XCE by:where calculates the Shannon entropy of a specific distribution, is the percentage of patterns found only once in the data set, is the Shannon entropy of the quantized series .
2.2.3. Cross-Sample Entropy (XSampEn)
- (1)
- State space reconstructionForm and by:respectively, where .
- (2)
- Ranking similar vectorsDefine the distance (d) between two vectors by:where indicates the maximum norm. Then define:where , the Heaviside step function (i.e., if , and otherwise). Define similarly according to steps (1) and (2).
- (3)
- XSampEn calculationDefine XSampEn by:
2.2.4. Cross-Fuzzy Entropy (XFuzzyEn)
2.3. Further Explanation of the Methods Used
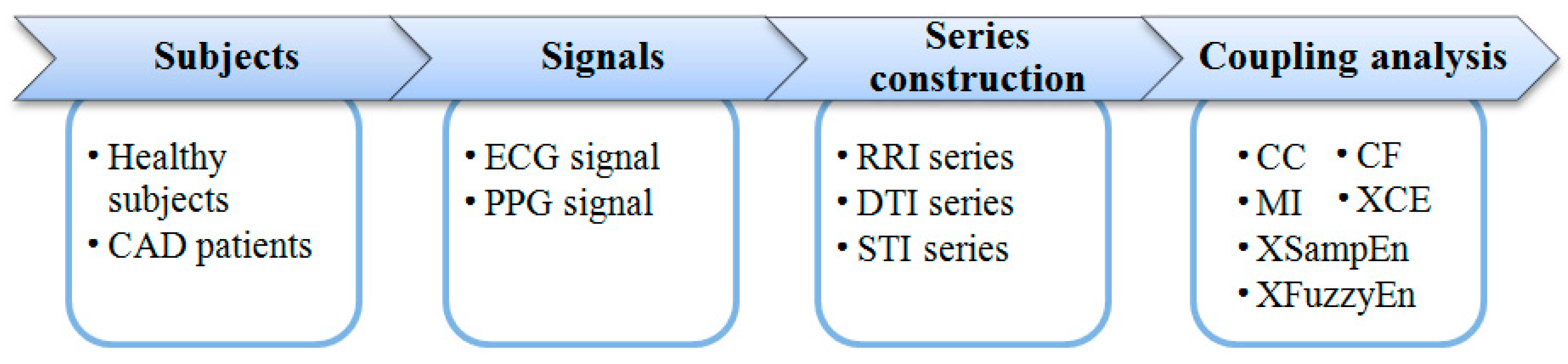
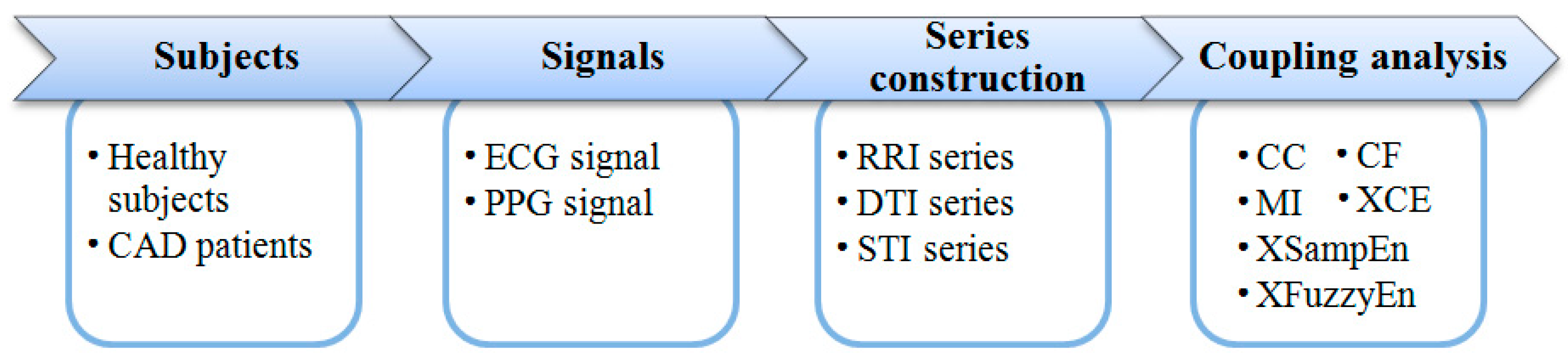
3. Experimental Data and Processing Procedures
3.1. Subjects
3.2. Protocol
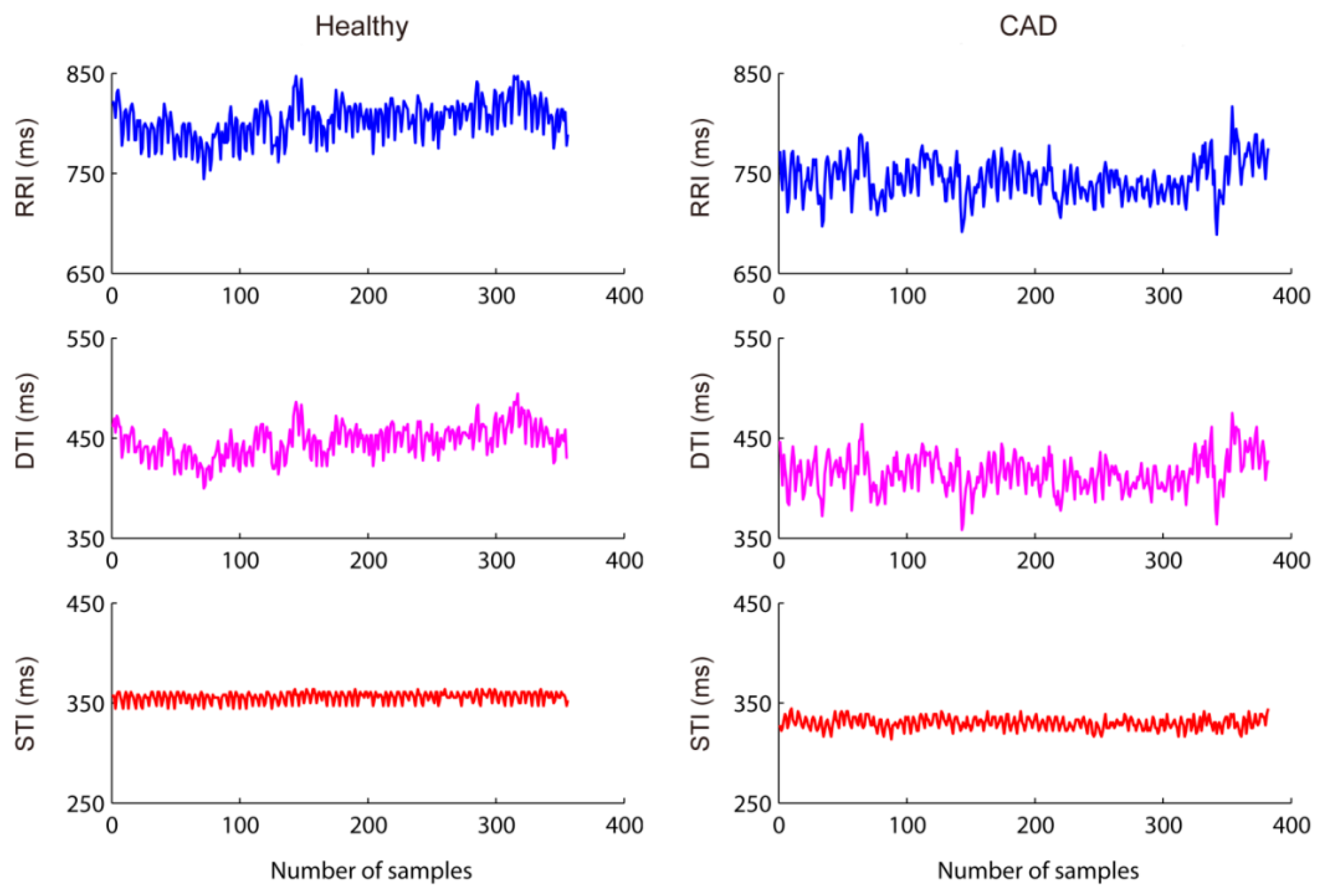
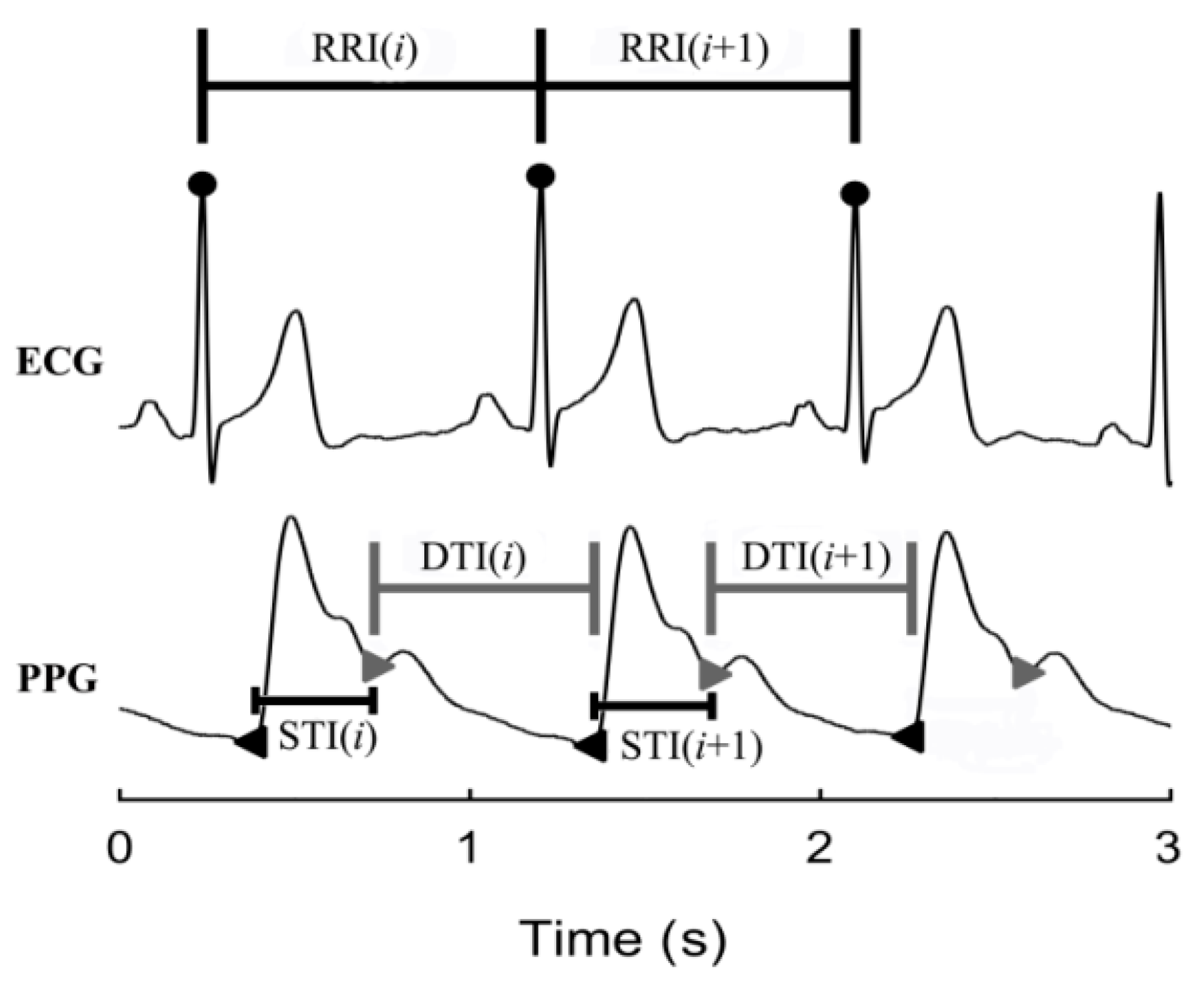
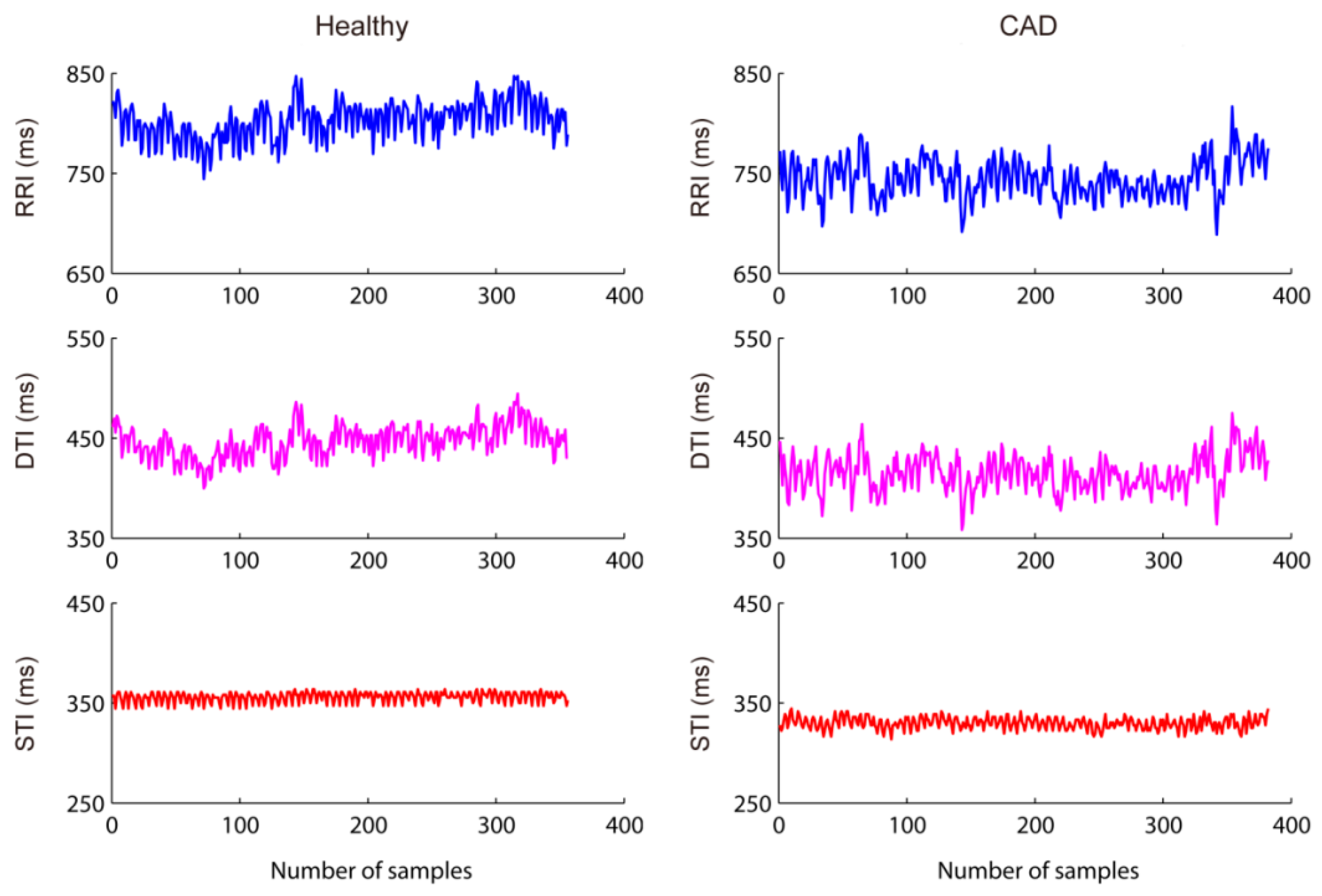
3.3. Construction of RRI, STI, and DTI Time-Series
3.4. RRI-STI, RRI-DTI, and STI-DTI Coupling Analysis
3.5. Statistical Analysis
4. Results
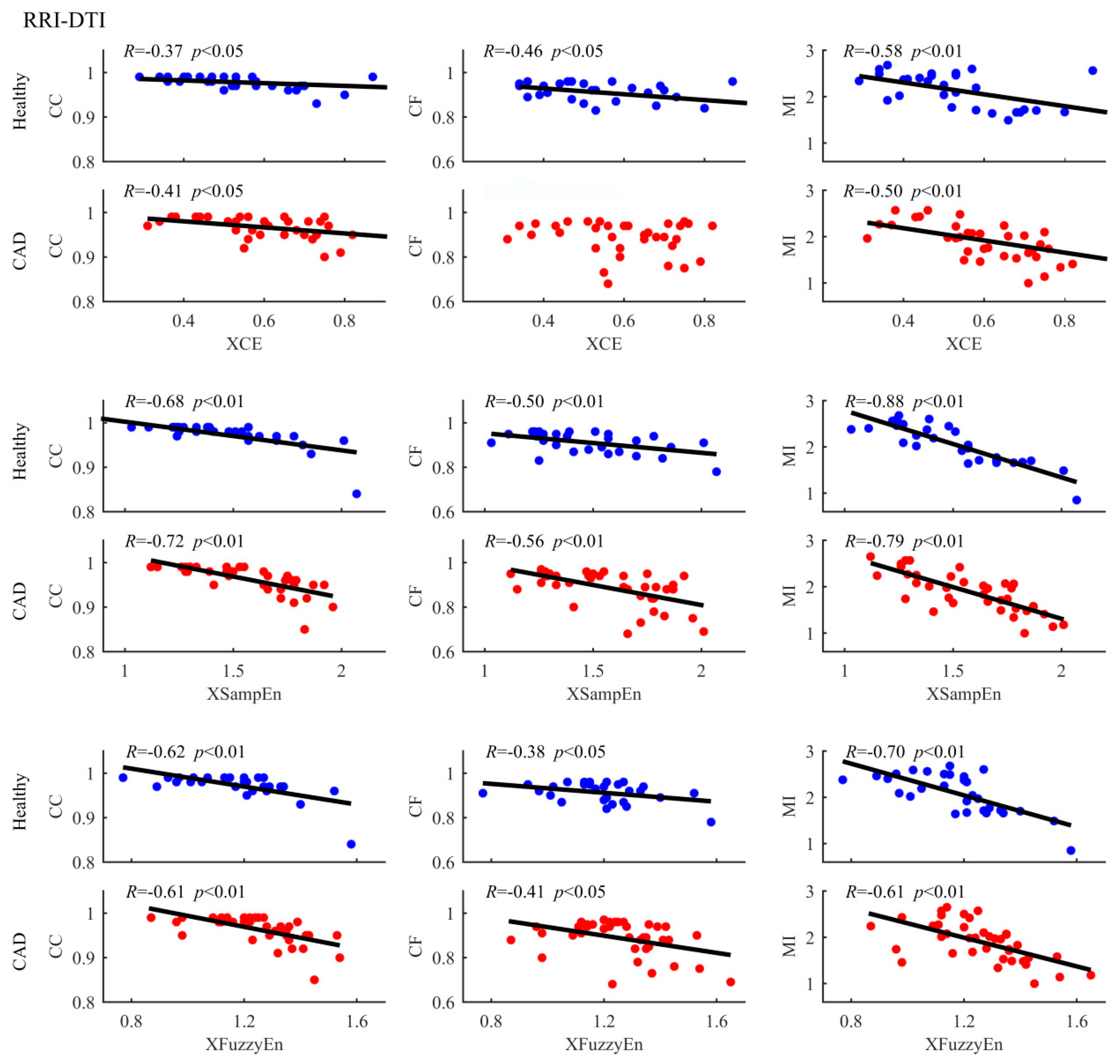
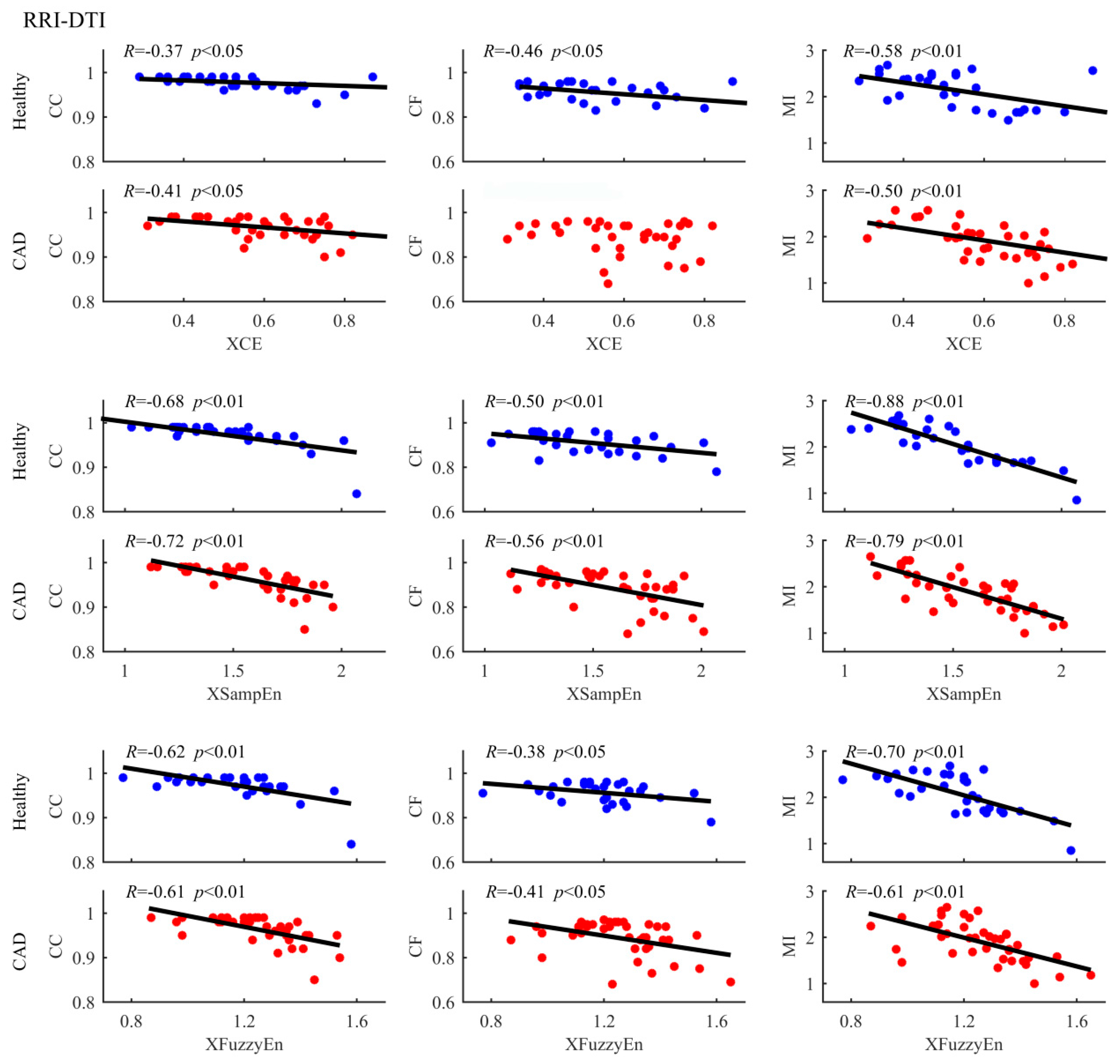
4.1. RRI-DTI Coupling Analysis Results
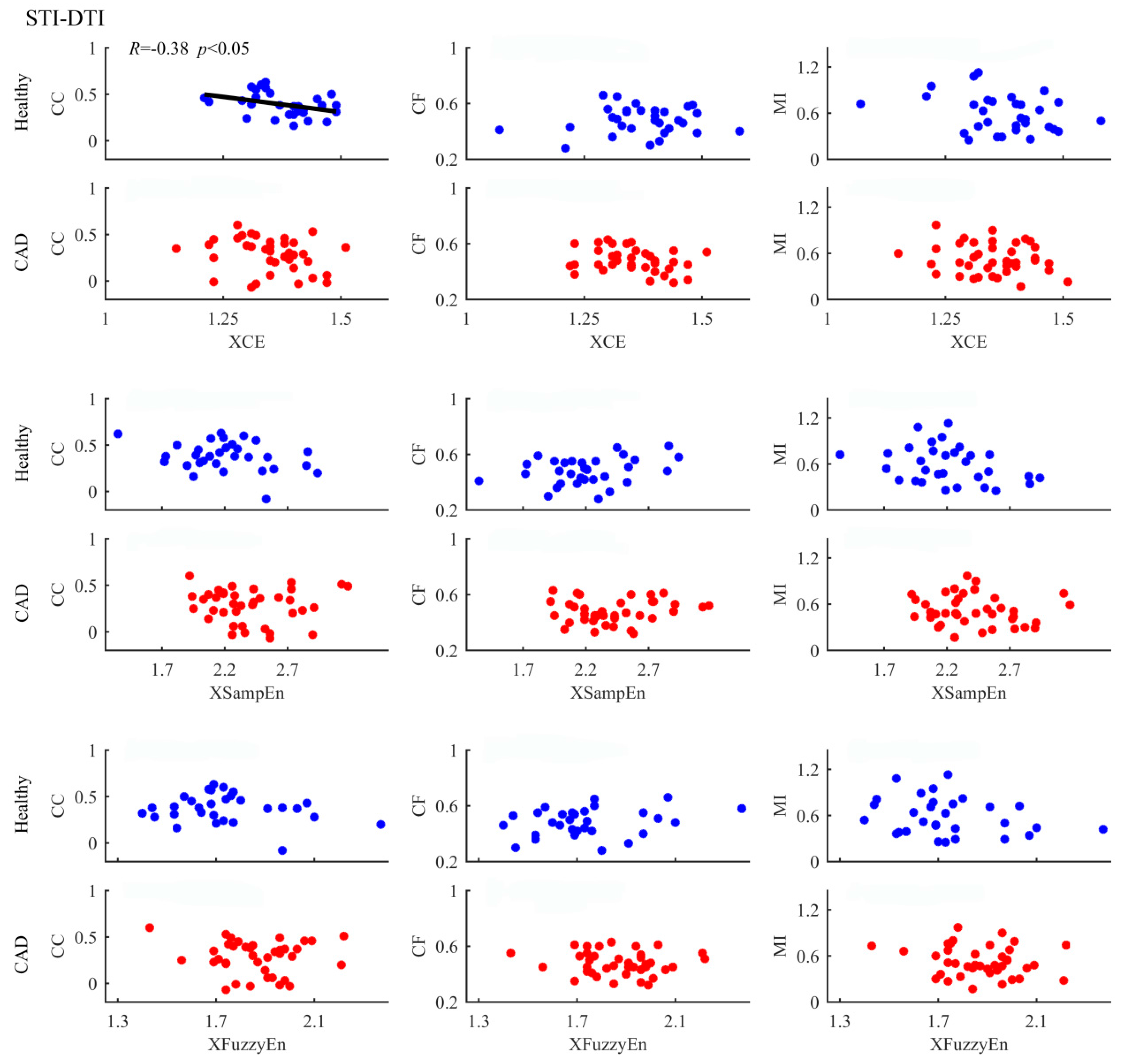
4.2. STI-DTI Coupling Analysis Results
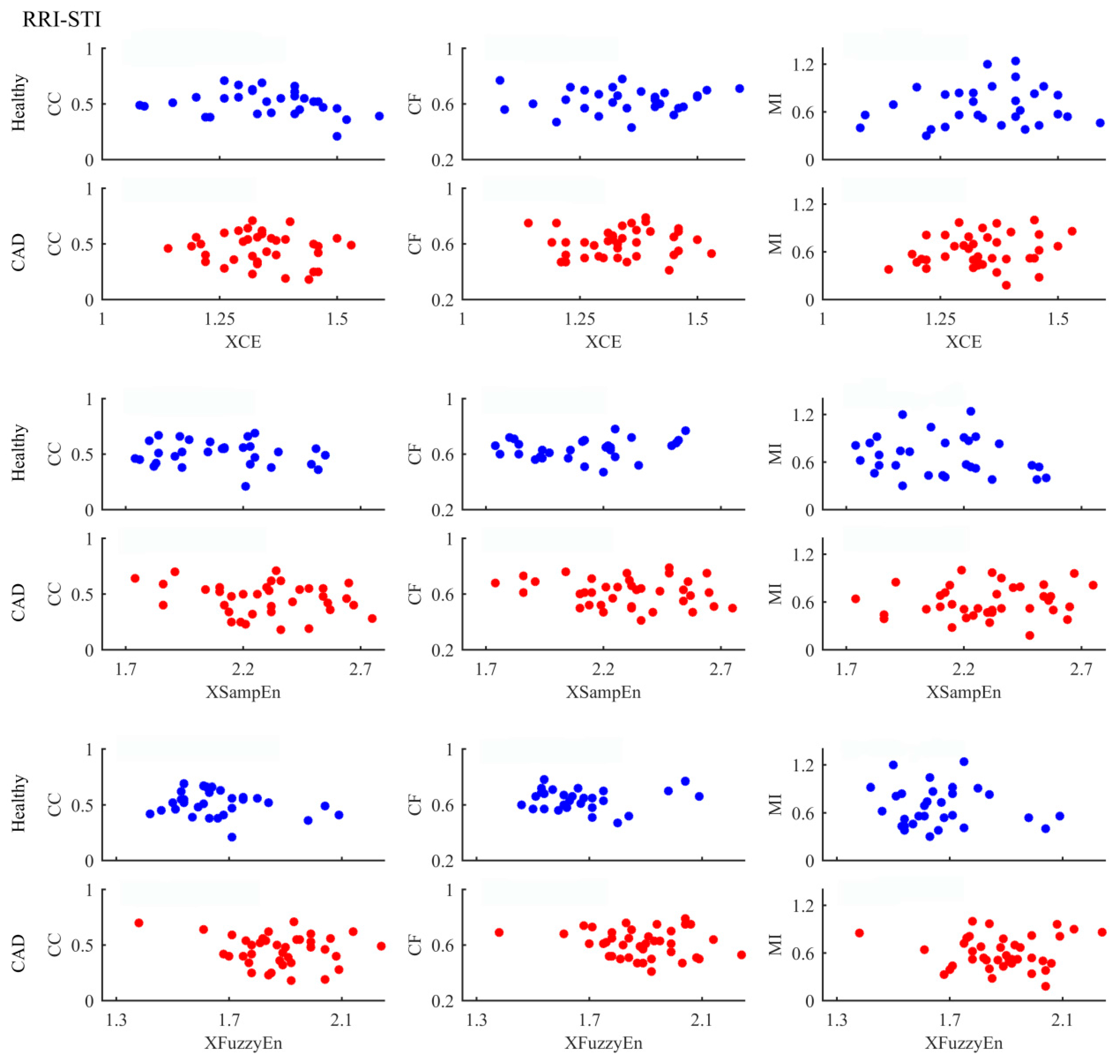
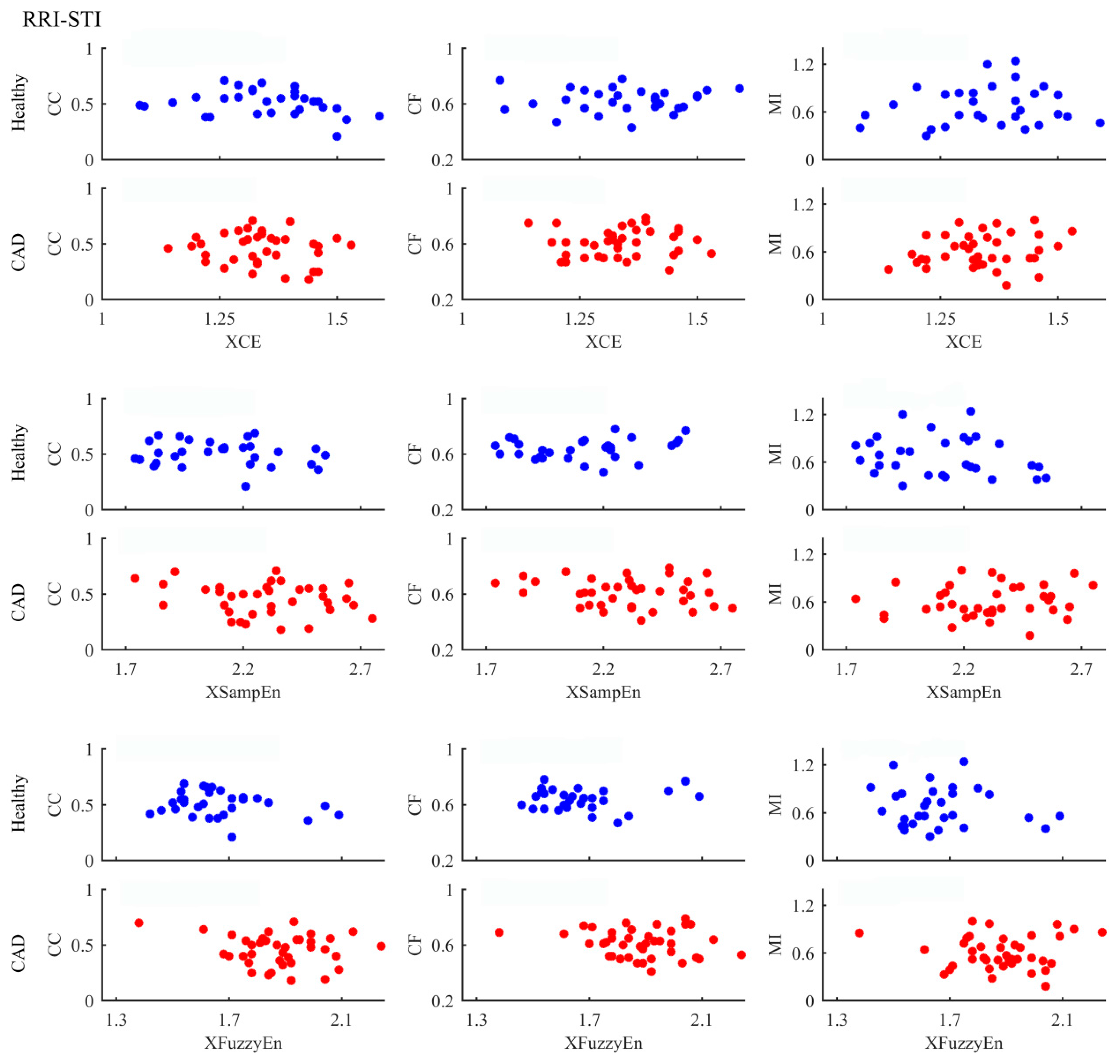
4.3. RRI-STI Coupling Analysis Results
5. Discussion
6. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| CAD | coronary artery disease |
| RRI | heartbeat interval |
| DTI | diastolic time interval |
| STI | systolic time interval |
| ECG | electrocardiograph |
| PPG | photoplethysmography |
| CC | correlation coefficient |
| CF | coherence function |
| MI | mutual information |
| XCE | cross-conditional entropy |
| XSampEn | cross-sample entropy |
| XFuzzyEn | cross-fuzzy entropy |
| RAP | radial artery pressure |
| BMI | body mass index |
| DBP | diastolic blood pressure |
| SBP | systolic blood pressure |
| SD | standard deviation |
References
- Akselrod, S.; Gordon, D.; Ubel, F.A.; Shannon, D.C.; Berger, A.C.; Cohen, R.J. Power spectrum analysis of heart rate fluctuation: A quantitative probe of beat-to-beat cardiovascular control. Science 1981, 213, 220–222. [Google Scholar] [CrossRef] [PubMed]
- Makikallio, T.H.; Hoiber, S.; Kober, L.; Torp-Pedersen, C.; Peng, C.K.; Goldberger, A.L.; Huikuri, H.V. Fractal analysis of heart rate dynamics as a predictor of mortality in patients with depressed left ventricular function after acute myocardial infarction. Am. J. Cardiol. 1999, 83, 836–839. [Google Scholar] [CrossRef]
- Acharya, U.R.; Faust, O.; Sree, V.; Swapna, G.; Martis, R.J.; Kadri, N.A.; Suri, J.S. Linear and nonlinear analysis of normal and CAD-affected heart rate signals. Comput. Meth. Prog. Biomed. 2014, 113, 55–68. [Google Scholar] [CrossRef] [PubMed]
- Giri, D.; Rajendra Acharya, U.; Martis, R.J.; Vinitha Sree, S.; Lim, T.-C.; Ahamed, T.; Suri, J.S. Automated diagnosis of coronary artery disease affected patients using LDA, PCA, ICA and discrete wavelet transform. Knowl. Based Syst. 2013, 37, 274–282. [Google Scholar] [CrossRef]
- Dua, S.; Du, X.; Sree, V.S.; Ahamed, T.V.I. Novel classification of coronary artery disease using heart rate variability analysis. J. Mech. Med. Biol. 2012, 12, 1240017. [Google Scholar] [CrossRef]
- Lee, H.G.; Noh, K.Y.; Ho, K. Mining biosignal data: Coronary artery disease diagnosis using linear and nonlinear features of HRV. Lect. Notes Comput. Sci. 2007, 4819, 218–228. [Google Scholar]
- Ferro, G.; Piscione, F.; Carella, G.; Betocchi, S.; Spinelli, L.; Chiariello, M. Systolic and diastolic time intervals during spontaneous angina. Clin. Cardiol. 1984, 7, 588–592. [Google Scholar] [CrossRef] [PubMed]
- Imam, M.H.; Karmakar, C.K.; Jelinek, H.F.; Palaniswami, M.; Khandoker, A.H. Analyzing systolic-diastolic interval interaction characteristics in diabetic cardiac autonomic neuropathy progression. IEEE JTEHM 2015, 3, 1900510. [Google Scholar] [CrossRef]
- Fossa, A.A.; Zhou, M.J.; Robinson, A.; Purkayastha, J.; Martin, P. Use of ECG restitution (beat-to-beat QT-TQ interval analysis) to assess arrhythmogenic risk of QTc prolongation with guanfacine. Ann. Noninvasive Electrocardiol. 2014, 19, 582–594. [Google Scholar] [CrossRef] [PubMed]
- Ji, L.Z.; Li, P.; Li, K.; Wang, X.P.; Liu, C.C. Analysis of short-term heart rate and diastolic period variability using a refined fuzzy entropy method. Biomed. Eng. Online 2015, 14. [Google Scholar] [CrossRef] [PubMed]
- Hirose, K.; Reed, J.E.; Rumberger, J.A. Serial changes in left and right ventricular systolic and diastolic dynamics during the first year after an index left ventricular Q wave myocardial infarction. J. Am. Coll. Cardiol. 1995, 25, 1097–1104. [Google Scholar] [CrossRef]
- Liu, C.Y.; Liu, C.C.; Li, L.P.; Zhang, Q.G.; Li, B. Systolic and diastolic time interval variability analysis and their relations with heart rate variability. In Proceedings of 3rd International Conference on Bioinformatics and Biomedical Engineering (ICBBE), Beijing, China, 11–13 June 2009; pp. 2609–2612.
- Carrasco-Sosa, S.; Guillen-Mandujano, A. Variability of left ventricular ejection and diastolic times obtained from impedance cardiography: A comparison with heart rate variability. In Proceedings of Computing in Cardiology, Zaragoza, Spain, 22–25 September 2013; pp. 405–408.
- Li, P.; Ji, L.; Yan, C.; Li, K.; Liu, C.; Liu, C. Coupling between short-term heart rate and diastolic period is reduced in heart failure patients as indicated by multivariate entropy analysis. In Proceedings of Computing in Cardiology, Cambridge, UK, 7–10 September 2014; pp. 97–100.
- Li, P.; Liu, C.; Sun, X.; Ren, Y.; Yan, C.; Yu, Z.; Liu, C. Age related changes in variability of short-term heart rate and diastolic period. In Proceedings of Computing in Cardiology, Zaragoza, Spain, 22–25 September 2013; pp. 995–998.
- Li, P.; Karmakar, C.; Liu, C.; Liu, C. Analysing effect of heart rate and age on radial artery pressure derived systolic and diastolic durations in healthy adults. In Proceedings of Computing in Cardiology, Nice, France, 7–9 September 2015; pp. 381–384.
- Fossa, A.A.; Wisialowski, T.; Crimin, K.; Wolfgang, E.; Couderc, J.P.; Hinterseer, M.; Kaab, S.; Zareba, W.; Badilini, F.; Sarapa, N. Analyses of dynamic beat-to-beat QT-TQ interval (ECG restitution) changes in humans under normal sinus rhythm and prior to an event of torsades de pointes during QT prolongation caused by sotalol. Ann. Noninvasive Electrocardiol. 2007, 12, 338–348. [Google Scholar] [CrossRef] [PubMed]
- Dorland. Dorland’s Illustrated Medical Dictionary, 32rd ed.; Saunders: Chicago, IL, USA, 2011. [Google Scholar]
- Franaszczuk, P.J.; Bergey, G.K. An autoregressive method for the measurement of synchronization of interictal and ictal EEG signals. Biol. Cybern. 1999, 81, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Alonso, J.F.; Mananas, M.A.; Romero, S.; Rojas-Martinez, M.; Riba, J. Cross-conditional entropy and coherence analysis of pharmaco-EEG changes induced by alprazolam. Psychopharmacology 2012, 221, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Breakspear, M. “Dynamic” connectivity in neural systems: Theoretical and empirical considerations. Neuroinformatics 2004, 2, 205–226. [Google Scholar] [CrossRef]
- Dauwels, J.; Vialatte, F.; Musha, T.; Cichocki, A. A comparative study of synchrony measures for the early diagnosis of alzheimer’s disease based on EEG. NeuroImage 2010, 49, 668–693. [Google Scholar] [CrossRef] [PubMed]
- Xie, H.B.; Guo, J.Y.; Zheng, Y.P. A comparative study of pattern synchronization detection between neural signals using different cross-entropy measures. Biol. Cybern. 2010, 102, 123–135. [Google Scholar] [CrossRef] [PubMed]
- Grossman, P.; Taylor, E.W. Toward understanding respiratory sinus arrhythmia: Relations to cardiac vagal tone, evolution and biobehavioral functions. Biol. Psychol. 2007, 74, 263–285. [Google Scholar] [CrossRef] [PubMed]
- Ramirez Avila, G.M.; Gapelyuk, A.; Marwan, N.; Walther, T.; Stepan, H.; Kurths, J.; Wessel, N. Classification of cardiovascular time series based on different coupling structures using recurrence networks analysis. Philos. Trans. A Math. Phys. Eng. Sci. 2013, 371, 20110623. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.T.; Liu, C.C.; Lo, M.T.; Hsu, P.C.; Liu, A.B.; Chang, K.Y.; Tang, C.J. Multiscale cross-approximate entropy analysis as a measure of complexity among the aged and diabetic. Comput. Math. Methods Med. 2013, 2013, 324325. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Zhang, C.; Zhang, L.; Zhao, L.; Liu, C.; Wang, H. Measuring synchronization in coupled simulation and coupled cardiovascular time series: A comparison of different cross entropy measures. Biomed. Signal Process. Control 2015, 21, 49–57. [Google Scholar] [CrossRef]
- Kreuz, T.; Mormann, F.; Andrzejak, R.G.; Kraskov, A.; Lehnertz, K.; Grassberger, P. Measuring synchronization in coupled model systems: A comparison of different approaches. Physica D 2007, 225, 29–42. [Google Scholar] [CrossRef]
- Ansari-Asl, K.; Senhadji, L.; Bellanger, J.J.; Wendling, F. Quantitative evaluation of linear and nonlinear methods characterizing interdependencies between brain signals. Phys. Rev. E 2006, 74, 031916. [Google Scholar] [CrossRef] [PubMed]
- Porta, A.; Baselli, G.; Lombardi, F.; Montano, N.; Malliani, A.; Cerutti, S. Conditional entropy approach for the evaluation of the coupling strength. Biol. Cybern. 1999, 81, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Li, K.; Liu, C.; Zheng, D.; Li, Z.-M.; Liu, C. Detection of coupling in short physiological series by a joint distribution entropy method. IEEE Trans. Biomed. Eng. 2016. [Google Scholar] [CrossRef] [PubMed]
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol. Heart Circ. Physiol. 2000, 278, H2039–H2049. [Google Scholar] [PubMed]
- Li, P.; Liu, C.; Wang, X.; Li, B.; Che, W.; Liu, C. Cross-sample entropy and cross-fuzzy entropy for testing pattern synchrony: How results vary with different threshold value r. In Proceedings of the World Congress on Medical Physics and Biomedical Engineering, Beijing, China, 26–31 May 2012; pp. 485–488.
- Li, P.; Liu, C.; Wang, X.; Li, L.; Yang, L.; Chen, Y.; Liu, C. Testing pattern synchronization in coupled systems through different entropy-based measures. Med. Biol. Eng. Comput. 2013, 51, 581–591. [Google Scholar] [CrossRef] [PubMed]
- Xie, H.B.; Zheng, Y.P.; Guo, J.Y.; Chen, X. Cross-fuzzy entropy: A new method to test pattern synchrony of bivariate time series. Inf. Sci. 2010, 180, 1715–1724. [Google Scholar] [CrossRef]
- Feldmann, U.; Bhattacharya, J. Predictability improvement as an asymmetrical measure of interdependence in bivariate time series. Int. J. Bifurc. Chaos 2004, 14, 505–514. [Google Scholar] [CrossRef]
- Palus, M.; Stefanovska, A. Direction of coupling from phases of interacting oscillators: An information-theoretic approach. Phys. Rev. E 2003, 67, 055201. [Google Scholar] [CrossRef] [PubMed]
- Tallon-Baudry, C.; Bertrand, O.; Delpuech, C.; Pernier, J. Stimulus specificity of phase-locked and non-phase-locked 40 Hz visual responses in human. J. Neurosci. 1996, 16, 4240–4249. [Google Scholar] [PubMed]
- Quian Quiroga, R.; Kreuz, T.; Grassberger, P. Event synchronization: A simple and fast method to measure synchronicity and time delay patterns. Phys. Rev. E 2002, 66, 041904. [Google Scholar] [CrossRef] [PubMed]
- Halamek, J.; Jurak, P.; Leinveber, P.; Vondra, V.; Couderc, J.P. Comparing the relationship between QT/RR slope and basal QTc in LQT1 patients and healthy subjects. In Proceedings of Computing in Cardiology, Zaragoza, Spain, 22–25 September 2013; pp. 65–68.
- Nunez, P.L.; Srinivasan, R. Electric Fields of the Brain: The Neurophysics of EEG, 2nd ed.; Oxford University Press: New York, NY, USA, 2006. [Google Scholar]
- Li, P.; Liu, C.; Wang, X.; Zheng, D.; Li, Y.; Liu, C. A low-complexity data-adaptive approach for premature ventricular contraction recognition. Signal Image Video Process. 2014, 8, 111–120. [Google Scholar] [CrossRef]
- Yambe, T.; Shiraishi, Y.; Saijo, Y.; Liu, H.; Nitta, S.; Imachi, K.; Baba, A.; Yamaguchi, T.; Sugawara, S.; Katahira, Y.; et al. Clinical research on the accuracy in determining the pulse wave rising point. Scr. Med. 2009, 82, 164–174. [Google Scholar]
- Liu, C.Y.; Li, L.P.; Zhao, L.N.; Zheng, D.C.; Li, P.; Liu, C.C. A combination method of improved impulse rejection filter and template matching for identification of anomalous intervals in RR sequences. J. Med. Biol. Eng. 2012, 32, 245–249. [Google Scholar] [CrossRef]
- Karimi, M.; Amirfattahi, R.; Sadri, S.; Marvasti, S.A. Noninvasive detection and classification of coronary artery occlusions using wavelet analysis of heart sounds with neural networks. In Proceedings of the 3rd IEE International Seminar on Medical Applications of Signal Processing, London, UK, 3–4 November 2005; pp. 117–120.
- Zhao, Z.; Ma, C. An intelligent system for noninvasive diagnosis of coronary artery disease with EMD-TEO and BP neural network. In Proceedings of the International Workshop on Education Technology and Training (ETT) and on Geoscience and Remote Sensing (GRS), Shanghai, China, 21–22 December 2008; pp. 631–635.
- Babaoğlu, I.; Findik, O.; Bayrak, M. Effects of principle component analysis on assessment of coronary artery diseases using support vector machine. Expert Syst. Appl. 2010, 37, 2182–2185. [Google Scholar] [CrossRef]
- Babaoğlu, I.; Findik, O.; Ülker, E. A comparison of feature selection models utilizing binary particle swarm optimization and genetic algorithm in determining coronary artery disease using support vector machine. Expert Syst. Appl. 2010, 37, 3177–3183. [Google Scholar] [CrossRef]
- Patidar, S.; Pachori, R.B.; Acharya, U.R. Automated diagnosis of coronary artery disease using tunable-Q wavelet transform applied on heart rate signals. Know. Based Syst. 2015, 82, 1–10. [Google Scholar] [CrossRef]
- Wilson, M.F.; Sung, B.H.; Herbst, C.P.; Lee, R.H.; Brackett, D.J. Evaluation of left ventricular contractility indexes for the detection of symptomatic and silent myocardial ischemia. Am. J. Cardiol. 1988, 62, 1176–1179. [Google Scholar] [CrossRef]
- Liou, Y.M.; Hsieh, S.R.; Wu, T.J.; Chen, J.Y. Green tea extract given before regional myocardial ischemia-reperfusion in rats improves myocardial contractility by attenuating calcium overload. Pflug. Arch. Eur. J. Phy. 2010, 460, 1003–1014. [Google Scholar] [CrossRef] [PubMed]
- Cascio, W.E.; Johnson, T.A.; Gettes, L.S. Electrophysiologic changes in ischemic ventricular myocardium: I. Influence of ionic, metabolic, and energetic changes. J. Cardiovasc. Electrophysiol. 1995, 6, 1039–1062. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Yang, Z.; Coote, J.H. Cross-sample entropy statistic as a measure of complexity and regularity of renal sympathetic nerve activity in the rat. Exp. Physiol. 2007, 92, 659–669. [Google Scholar] [CrossRef] [PubMed]
- Kuehl, M.; Stevens, M.J. Cardiovascular autonomic neuropathies as complications of diabetes mellitus. Nat. Rev. Endocrinol. 2012, 8, 405–416. [Google Scholar] [CrossRef] [PubMed]
- Brunner, M.J.; Greene, A.S.; Kallman, C.H.; Shoukas, A.A. Interaction of canine carotid sinus and aortic arch baroreflexes in the control of total peripheral resistance. Circ. Res. 1984, 55, 740–750. [Google Scholar] [CrossRef] [PubMed]
- Pierdomenico, S.D. Left-ventricular hypertrophy and coronary artery disease. Am. J. Hypertens. 2007, 20, 1036–1037. [Google Scholar] [CrossRef] [PubMed]
- Ghali, J.K.; Liao, Y.; Simmons, B.; Castaner, A.; Cao, G.; Cooper, R.S. The prognostic role of left ventricular hypertrophy in patients with or without coronary artery disease. Ann. Intern. Med. 1992, 117, 831–836. [Google Scholar] [CrossRef] [PubMed]
- Wessel, N.; Suhrbier, A.; Riedl, M.; Marwan, N.; Malberg, H.; Bretthauer, G.; Penzel, T.; Kurths, J. Detection of time-delayed interactions in biosignals using symbolic coupling traces. EPL 2009, 87, 10004. [Google Scholar] [CrossRef]
- Suhrbier, A.; Riedl, M.; Malberg, H.; Penzel, T.; Bretthauer, G.; Kurths, J.; Wessel, N. Cardiovascular regulation during sleep quantified by symbolic coupling traces. Chaos 2010, 20, 045124. [Google Scholar] [CrossRef] [PubMed]
- Penzel, T.; Riedl, M.; Gapelyuk, A.; Suhrbier, A.; Bretthauer, G.; Malberg, H.; Schobel, C.; Fietze, I.; Heitmann, J.; Kurths, J.; et al. Effect of CPAP therapy on daytime cardiovascular regulations in patients with obstructive sleep apnea. Comput. Biol. Med. 2012, 42, 328–334. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Healthy Subjects | CAD Patients | p |
|---|---|---|---|
| Age (years) | 57 ± 10 | 59 ± 8 | 0.51 |
| Gender (M/F) | 16/20 | 22/17 | 0.42 |
| HR (beats/min) | 66 ± 6 | 69 ± 7 | 0.08 |
| Height (cm) | 164 ± 7 | 166 ± 9 | 0.20 |
| Weight (kg) | 65.8 ± 6.2 | 68.0 ± 6.4 | 0.21 |
| BMI (kg/m2) | 23.5 ± 2.2 | 24.4 ± 1.6 | 0.12 |
| DBP (mmHg) | 77 ± 8 | 79 ± 9 | 0.29 |
| SBP (mmHg) | 124 ± 10 | 128 ± 10 | 0.15 |
| Measurements | Healthy Subjects | CAD Patients | p |
|---|---|---|---|
| CC | 0.98 (0.97 0.99) | 0.97 (0.95 0.99) | 0.06 |
| CF | 0.92 (0.87 0.95) | 0.91 (0.85 0.95) | 0.82 |
| MI | 2.19 (1.71 2.47) | 1.97 (1.56 2.24) | 0.05 |
| XCE | 0.50 (0.39 0.60) | 0.59 (0.52 0.71) | 0.02 |
| XSampEn | 1.41 (1.25 1.70) | 1.55 (1.33 1.78) | 0.07 |
| XFuzzyEn | 1.20 (1.02 1.27) | 1.27 (1.14 1.36) | 0.03 |
| Measurements | Healthy Subjects | CAD Patients | p |
|---|---|---|---|
| CC | 0.38 (0.29 0.50) | 0.36 (0.26 0.45) | 0.25 |
| CF | 0.49 (0.42 0.55) | 0.46 (0.43 0.54) | 0.55 |
| MI | 0.54 (0.39 0.75) | 0.48 (0.38 0.68) | 0.36 |
| XCE | 1.35 (1.29 1.40) | 1.39 (1.32 1.43) | 0.08 |
| XSampEn | 2.09 (1.95 2.15) | 2.19 (1.99 2.45) | 0.05 |
| XFuzzyEn | 1.61 (1.50 1.68) | 1.69 (1.57 1.80) | <0.008 |
| Measurements | Healthy Subjects | CAD Patients | p |
|---|---|---|---|
| CC | 0.52 (0.42 0.61) | 0.48 (0.36 0.55) | 0.08 |
| CF | 0.63 (0.57 0.69) | 0.61 (0.52 0.69) | 0.54 |
| MI | 0.62 (0.46 0.84) | 0.54 (0.47 0.79) | 0.21 |
| XCE | 1.34 (1.25 1.42) | 1.33 (1.28 1.39) | 0.77 |
| XSampEn | 2.11 (1.89 2.25) | 2.25 (2.11 2.36) | 0.04 |
| XFuzzyEn | 1.62 (1.54 1.71) | 1.84 (1.77 1.92) | < 0.008 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ji, L.; Li, P.; Liu, C.; Wang, X.; Yang, J.; Liu, C. Measuring Electromechanical Coupling in Patients with Coronary Artery Disease and Healthy Subjects. Entropy 2016, 18, 153. https://doi.org/10.3390/e18040153
Ji L, Li P, Liu C, Wang X, Yang J, Liu C. Measuring Electromechanical Coupling in Patients with Coronary Artery Disease and Healthy Subjects. Entropy. 2016; 18(4):153. https://doi.org/10.3390/e18040153
Chicago/Turabian StyleJi, Lizhen, Peng Li, Chengyu Liu, Xinpei Wang, Jing Yang, and Changchun Liu. 2016. "Measuring Electromechanical Coupling in Patients with Coronary Artery Disease and Healthy Subjects" Entropy 18, no. 4: 153. https://doi.org/10.3390/e18040153
APA StyleJi, L., Li, P., Liu, C., Wang, X., Yang, J., & Liu, C. (2016). Measuring Electromechanical Coupling in Patients with Coronary Artery Disease and Healthy Subjects. Entropy, 18(4), 153. https://doi.org/10.3390/e18040153