
Impact of the 2019 Coronavirus Disease Pandemic on Health-Related Quality of Life and Psychological Status: The Role of Physical Activity

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Descriptive Statistics
2.3. Survey Development and Instruments
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef]
- Summary of Probable SARS Cases with Onset of Illness from 1 November 2002 to 31 July 2003. Available online: https://www.who.int/csr/sars/country/table2004_04_21/en/ (accessed on 19 July 2020).
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus Disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. China coronavirus: WHO declares international emergency as death toll exceeds 200. BMJ 2020, 368, m408. [Google Scholar] [CrossRef]
- Parnell, D.; Widdop, P.; Bond, A.; Wilson, R. COVID-19, networks and sport. Manag. Sport Leis. 2020, 1, 1–7. [Google Scholar] [CrossRef]
- Yezli, S.; Khan, A. COVID-19 social distancing in the Kingdom of Saudi Arabia: Bold measures in the face of political, economic, social and religious challenges. Travel Med. Infect. Dis. 2020, 37, 101692. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health in Kingdom of Saudi Arabia. Available online: https://www.moh.gov.sa/en/Pages/default.aspx (accessed on 30 June 2020).
- Lesser, I.A.; Nienhuis, C.P. The impact of COVID-19 on physical activity behavior and well-being of Canadians. Int. J. Environ. Res. Public Health 2020, 17, 3899. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.W.; Balluz, L.S.; Heath, G.W.; Moriarty, D.G.; Ford, E.S.; Giles, W.H.; Mokdad, A.H. Associations between recommended levels of physical activity and health-related quality of life. Findings from the 2001 Behavioral Risk Factor Surveillance System (BRFSS) survey. Prev. Med. 2003, 37, 520–528. [Google Scholar] [CrossRef]
- Centers for Disease Control. Prevention: Measuring Healthy Days: Population Assessment of Health-Related Quality of Life; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2000. [Google Scholar]
- Algahtani, F.; Hassan, S.-U.-N.; Alsaif, B.; Zrieq, R. Assessment of the Quality of Life during COVID-19 Pandemic: A Cross-Sectional Survey from the Kingdom of Saudi Arabia. Int. J. Environ. Res. Public Health 2021, 18, 847. [Google Scholar] [CrossRef]
- BinDhim, N.; Althumiri, N.; Basyouni, M.; Alageel, A.; Alghnam, S.; Al-Qunaibet, A.; Almubarak, R.; Aldhukair, S.; Ad-Dab’bagh, Y. Saudi Arabia Mental Health Surveillance System (MHSS): Mental health trends amid COVID-19 and comparison with pre-COVID-19 trends. Eur. J. Psychotraumatol. 2021, 12, 1875642. [Google Scholar] [CrossRef]
- Saarni, S.I.; Suvisaari, J.; Sintonen, H.; Pirkola, S.; Koskinen, S.; Aromaa, A.; Lönnqvist, J. Impact of psychiatric disorders on health-related quality of life: General population survey. Br. J. Psychiatry 2007, 190, 326–332. [Google Scholar] [CrossRef]
- Johansson, R.; Carlbring, P.; Heedman, Å.; Paxling, B.; Andersson, G.J.P. Depression, anxiety and their comorbidity in the Swedish general population: Point prevalence and the effect on health-related quality of life. PeerJ 2013, 1, e98. [Google Scholar] [CrossRef]
- Brown, D.S.; Thompson, W.W.; Zack, M.M.; Arnold, S.E.; Barile, J.P. Associations between health-related quality of life and mortality in older adults. Prev. Sci. 2015, 16, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Landman, G.W.D.; van Hateren, K.J.J.; Kleefstra, N.; Groenier, K.H.; Gans, R.O.B.; Bilo, H.J.G. Health-related quality of life and mortality in a general and elderly population of patients with type 2 diabetes (ZODIAC-18). Diabetes Care 2010, 33, 2378–2382. [Google Scholar] [CrossRef]
- Sim, K.; Huak Chan, Y.; Chong, P.N.; Chua, H.C.; Wen Soon, S. Psychosocial and coping responses within the community health care setting towards a national outbreak of an infectious disease. J. Psychosom. Res. 2010, 68, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Chew, Q.H.; Wei, K.C.; Vasoo, S.; Chua, H.C.; Sim, K. Narrative synthesis of psychological and coping responses towards emerging infectious disease outbreaks in the general population: Practical considerations for the COVID-19 pandemic. Singap. Med. J. 2020, 61, 350–356. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef]
- Alkhamees, A.A.; Alrashed, S.A.; Alzunaydi, A.A.; Almohimeed, A.S.; Aljohani, M.S. The psychological impact of COVID-19 pandemic on the general population of Saudi Arabia. Compr. Psychiatry 2020, 102, 152192. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Bize, R.; Johnson, J.A.; Plotnikoff, R.C. Physical activity level and health-related quality of life in the general adult population: A systematic review. Prev. Med. 2007, 45, 401–415. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour: At a Glance; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The posttraumatic stress disorder checklist for DSM-5 (PCL-5): Development and initial psychometric evaluation. J. Trauma. Stress 2015, 28, 489–498. [Google Scholar] [CrossRef]
- Weathers, F.W.; Litz, B.T.; Keane, T.M.; Palmieri, P.A.; Marx, B.P.; Schnurr, P.P.J. The PTSD Checklist for DSM-5 (pcl-5); National Center for PTSD: Boston, MA, USA, 2013; Volume 10. [Google Scholar]
- Ibrahim, H.; Ertl, V.; Catani, C.; Ismail, A.A.; Neuner, F. The validity of Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5) as screening instrument with Kurdish and Arab displaced populations living in the Kurdistan region of Iraq. BMC Psychiatry 2018, 18, 259. [Google Scholar] [CrossRef] [PubMed]
- Yiengprugsawan, V.; Kelly, M.; Tawatsupa, B. SF-8TM health survey. In Encyclopedia of Quality of Life and Well-Being Research; Michalos, A.C., Ed.; Springer: Dordrecht, The Netherlands, 2014; pp. 5940–5942. [Google Scholar]
- Hooker, S.A. SF-36. In Encyclopedia of Behavioral Medicine; Gellman, M.D., Turner, J.R., Eds.; Springer: New York, NY, USA, 2013; pp. 1784–1786. [Google Scholar]
- Coons, S.J.; Alabdulmohsin, S.A.; Draugalis, J.R.; Hays, R.D. Reliability of an Arabic version of the RAND-36 health survey and its equivalence to the US-English version. Med. Care 1998, 36, 428–432. [Google Scholar] [CrossRef] [PubMed]
- Tokuda, Y.; Okubo, T.; Ohde, S.; Jacobs, J.; Takahashi, O.; Omata, F.; Yanai, H.; Hinohara, S.; Fukui, T. Assessing Items on the SF-8 Japanese Version for Health-Related Quality of Life: A Psychometric Analysis Based on the Nominal Categories Model of Item Response Theory. Value Health J. Int. Soc. Pharm. Outcomes Res. 2008, 12, 568–573. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E.; Kosinski, M.; Dewey, J.E.; Gandek, B. How to score and interpret single-item health status measures: A manual for users of the SF-8 health survey. Linc. RI Qual. Inc. 2001, 15, 5. [Google Scholar]
- Kyriazos, T.A.; Stalikas, A.; Prassa, K.; Yotsidi, V. Can the depression anxiety stress Scales short be shorter? Factor structure and measurement invariance of DASS-21 and DASS-9 in a Greek, non-clinical sample. Psychology 2018, 9, 1095–1127. [Google Scholar] [CrossRef]
- Yusoff, M.S.B. Psychometric properties of the depression anxiety stress scale in a sample of medical degree applicants. Int. Med. J. 1994 2013, 20, 295–300. [Google Scholar]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scales; Psychology Foundation of Australia: Sydney, Australia, 1996. [Google Scholar]
- Antony, M.M.; Bieling, P.J.; Cox, B.J.; Enns, M.W.; Swinson, R.P. Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales in clinical groups and a community sample. Psychol. Assess. 1998, 10, 176–181. [Google Scholar] [CrossRef]
- Moussa, M.T.; Lovibond, P.; Laube, R.; Megahead, H.A. Psychometric properties of an Arabic version of the depression anxiety stress Scales (DASS). Res. Soc. Work Pract. 2017, 27, 375–386. [Google Scholar] [CrossRef]
- Scholz, U.; Doña, B.G.; Sud, S.; Schwarzer, R.J. Is general self-efficacy a universal construct? Psychometric findings from 25 countries. Eur. J. Psychol. Assess. 2002, 18, 242. [Google Scholar] [CrossRef]
- Taouk, M.; Lovibond, P.; Laube, R. Psychometric Properties of an Arabic Version of the Depression Anxiety Stress Scales (DASS21); Report for New South; Wales Transcultural Mental Health Centre, Cumberland Hospital: Sydney, Australia, 2001. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-Country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Helou, K.; El Helou, N.; Mahfouz, M.; Mahfouz, Y.; Salameh, P.; Harmouche Karaki, M. Validity and reliability of an adapted Arabic version of the long international physical activity questionnaire. BMC Public Health 2017, 18. [Google Scholar] [CrossRef] [PubMed]
- Haskell, W.L.; Lee, I.M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1423–1434. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Psychology Press, Taylor & Francis Group: New York, NY, USA, 1988. [Google Scholar] [CrossRef]
- Nguyen, H.C.; Nguyen, M.H.; Do, B.N.; Tran, C.Q.; Nguyen, T.T.P.; Pham, K.M.; Pham, L.V.; Tran, K.V.; Duong, T.T.; Tran, T.V.; et al. People with suspected COVID-19 symptoms were more likely depressed and had lower health-related quality of life: The potential benefit of health literacy. J. Clin. Med. 2020, 9, 965. [Google Scholar] [CrossRef]
- Solomou, I.; Constantinidou, F. Prevalence and predictors of anxiety and depression symptoms during the COVID-19 pandemic and compliance with precautionary measures: Age and sex matter. Int. J. Environ. Res. Public Health 2020, 17, 4924. [Google Scholar] [CrossRef] [PubMed]
- Satici, B.; Gocet-Tekin, E.; Deniz, M.E.; Satici, S.A. Adaptation of the Fear of COVID-19 Scale: Its association with psychological distress and life satisfaction in Turkey. Int. J. Ment. Health Addict. 2020, 1, 1–9. [Google Scholar] [CrossRef]
- Yan, S.; Xu, R.; Stratton, T.D.; Kavcic, V.; Luo, D.; Hou, F.; Bi, F.; Jiao, R.; Song, K.; Jiang, Y. Sex differences and psychological stress: Responses to the COVID-19 pandemic in China. BMC Public Health 2021, 21, 79. [Google Scholar] [CrossRef]
- Xue, B.; McMunn, A. Gender differences in unpaid care work and psychological distress in the UK Covid-19 lockdown. PLoS ONE 2021, 16, e0247959. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Lei, S.M.; Le, S.; Yang, Y.; Zhang, B.; Yao, W.; Gao, Z.; Cheng, S. Bidirectional influence of the COVID-19 pandemic lockdowns on health behaviors and quality of life among Chinese adults. Int. J. Environ. Res. Public Health 2020, 17, 5575. [Google Scholar] [CrossRef]
- Ge, Y.; Xin, S.; Luan, D.; Zou, Z.; Liu, M.; Bai, X.; Gao, Q. Association of physical activity, sedentary time, and sleep duration on the health-related quality of life of college students in Northeast China. Health Qual. Life Outcomes 2019, 17, 124. [Google Scholar] [CrossRef]
- Esain, I.; Gil, S.M.; Bidaurrazaga-Letona, I.; Rodriguez-Larrad, A. Effects of 3 months of detraining on functional fitness and quality of life in older adults who regularly exercise. Aging Clin. Exp. Res. 2019, 31, 503–510. [Google Scholar] [CrossRef]
- Nayak, P.; Kumaran, S.D.; Babu, A.S.; Maiya, A.G.; Solomon, J.M. Levels of physical activity and quality of life among community-dwelling adults with stroke in a developing country. Eur. J. Physiother. 2019, 1–6. [Google Scholar] [CrossRef]
- Pieh, C.; Budimir, S.; Probst, T. The effect of age, gender, income, work, and physical activity on mental health during coronavirus disease (COVID-19) lockdown in Austria. J. Psychosom. Res. 2020, 136, 110186. [Google Scholar] [CrossRef] [PubMed]
- Bowler, D.E.; Buyung-Ali, L.M.; Knight, T.M.; Pullin, A.S. A systematic review of evidence for the added benefits to health of exposure to natural environments. BMC Public Health 2010, 10, 456. [Google Scholar] [CrossRef]
- Nguyen, J.; Brymer, E. Nature-based guided imagery as an intervention for state anxiety. Front. Psychol. 2018, 9, 1858. [Google Scholar] [CrossRef] [PubMed]
- Kremer, E.F.; Block, A.; Gaylor, M.S. Behavioral approaches to treatment of chronic pain: The inaccuracy of patient self-report measures. Arch. Phys. Med. Rehabil. 1981, 62, 188–191. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Characteristics | All Participants (n = 518) | Physical Activity (MET-Min/Week) | |||
|---|---|---|---|---|---|
| Inactive (n = 149) | Sufficiently Active (n = 227) | Very Active (n = 142) | p Value * | ||
| No. (%) | % | % | % | ||
| Age (years), mean (SD) | 37.3 (14.3) | 37.4 (14.3) | 38.2 (14.7) | 35.7 (13.6) | 0.023 |
| Sex | 0.161 | ||||
| Male | 349 (67.4) | 72.5 | 67.4 | 62.0 | |
| Female | 169 (32.6) | 27.5 | 32.6 | 38.0 | |
| Ethnicity | 0.538 | ||||
| Saudi | 506 (97.7) | 96.6 | 97.8 | 98.6 | |
| Non-Saudi | 12 (2.3) | 3.4 | 2.2 | 1.4 | |
| BMI, kg/m2 | 0.092 | ||||
| Underweight (<18.5) | 36 (6.9) | 11.4 | 6.2 | 3.5 | |
| Normal (18.5 to 24.9) | 165 (31.9) | 26.2 | 32.2 | 37.3 | |
| Overweight (25 to 30) | 165 (31.9) | 30.2 | 33.9 | 30.3 | |
| Obese (≥30) | 152 (29.3) | 32.2 | 27.8 | 28.9 | |
| Smoking status | 0.342 | ||||
| Never smoker | 373 (72.0) | 69.8 | 75.8 | 68.3 | |
| Previous smoker | 48 (9.3) | 8.7 | 7.5 | 12.7 | |
| Current smoker | 97 (18.7) | 21.5 | 16.7 | 19.0 | |
| Highest level of education | 0.410 | ||||
| High school or below | 490 (94.6) | 94.0 | 96.0 | 93.0 | |
| Bachelor or above | 28 (5.4) | 6.0 | 4.0 | 7.0 | |
| Employment status | 0.170 | ||||
| Currently employed | 222 (42.9) | 49.0 | 39.2 | 42.3 | |
| Not employed | 296 (57.1) | 51.0 | 60.8 | 57.7 | |
| Social status | 0.048 | ||||
| Single | 188 (36.3) | 32.9 | 35.7 | 40.8 | |
| Married | 319 (61.6) | 67.1 | 60.4 | 57.7 | |
| Widow/divorced | 11 (2.1) | 0.0 | 4.0 | 1.4 | |
| Monthly income | <0.001 | ||||
| None | 101 (19.5) | 14.1 | 17.2 | 28.9 | |
| <6000 | 123 (23.7) | 27.5 | 24.2 | 19.0 | |
| 6000–10,000 | 55 (10.6) | 4.7 | 14.5 | 10.6 | |
| 10,000–20,000 | 190 (36.7) | 36.2 | 37.9 | 35.2 | |
| >20,000 | 49 (9.5) | 17.4 | 6.2 | 6.3 | |
| Region of residence | 0.043 | ||||
| Central region | 200 (38.6) | 46.3 | 33.0 | 39.4 | |
| Western region | 196 (37.8) | 37.6 | 38.3 | 37.3 | |
| Eastern region | 44 (8.5) | 6.0 | 11.5 | 6.3 | |
| Southern region | 63 (12.2) | 6.7 | 15.4 | 12.7 | |
| Northern region | 15 (2.9) | 3.4 | 1.8 | 4.2 | |
| Prevalent chronic diseases | <0.001 | ||||
| No | 345 (66.6) | 55.0 | 66.1 | 79.6 | |
| Yes | 173 (33.4) | 45.0 | 33.9 | 20.4 | |
| Self-infection with COVID-19 | 0.207 | ||||
| No | 509 (98.3) | 97.3 | 99.6 | 97.9 | |
| Yes | 9 (1.7) | 2.7 | 0.4 | 2.1 | |
| Relative-infection with COVID-19 | 0.134 | ||||
| No | 324 (62.5) | 55.0 | 63.0 | 62.5 | |
| Yes | 194 (37.5) | 45.0 | 37.0 | 37.5 | |
| Predicted Marginal Mean | Coefficient (95% CI) a | Cohen’s d | |
|---|---|---|---|
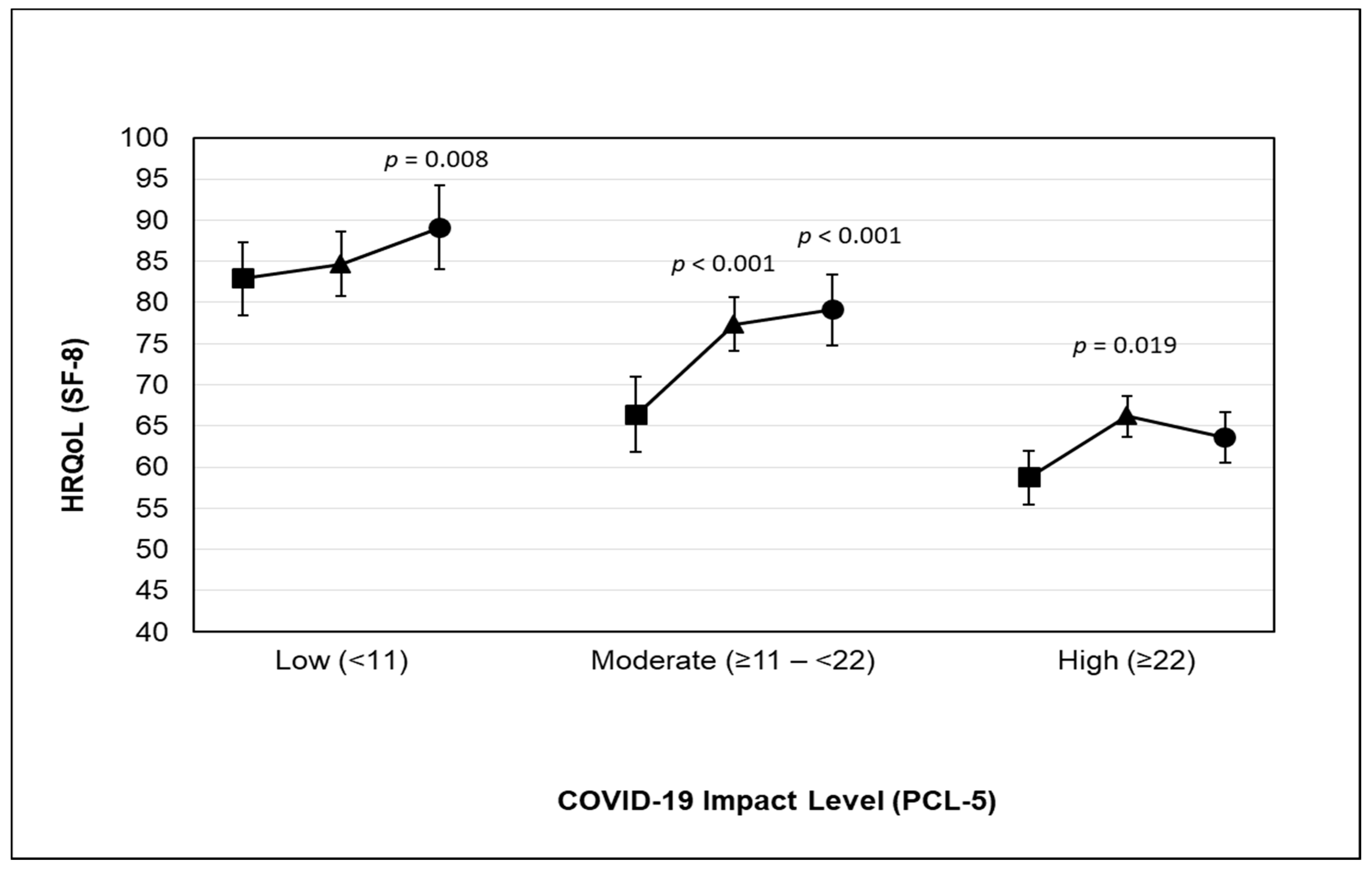
| HRQoL (SF-8) b | |||
| Low (n = 206) | 84.80 (1.00) | Referent | |
| Moderate (n = 151) | 74.60 (1.14) | −10.19 (−13.18, −7.21) | −0.55 |
| High (n = 161) | 64.40 (1.14) | −20.39 (−23.47, −17.32) | −1.03 |
| Trend p value | <0.001 | ||
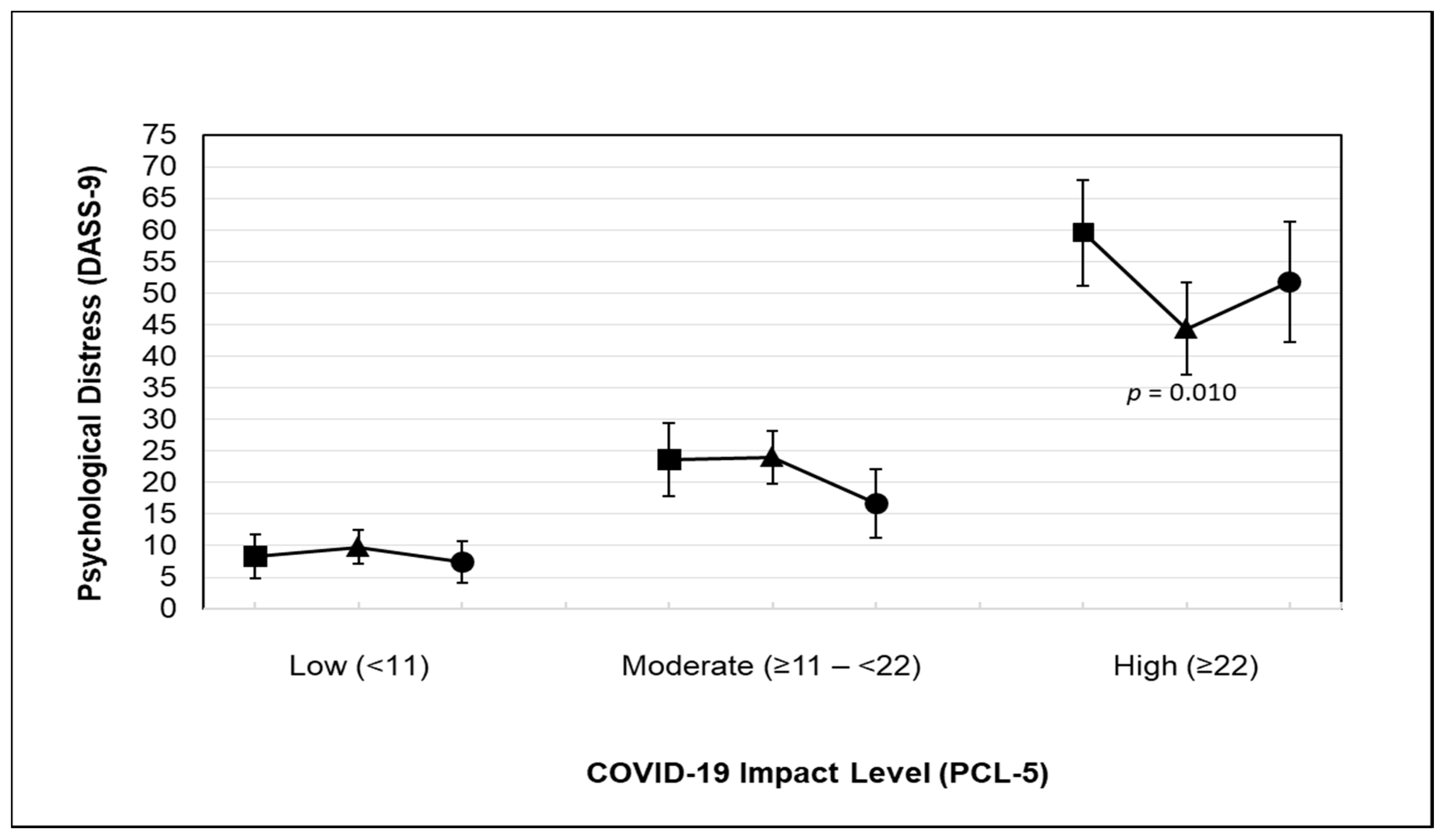
| Psychological Distress (DASS-9) b | |||
| Low (n = 206) | 9.85 (1.48) | Referent | |
| Moderate (n = 151) | 21.74 (1.69) | 11.89 (7.46, 16.32) | 0.43 |
| High (n = 161) | 49.63 (1.69) | 39.77 (35.21, 44.33) | 1.35 |
| Trend p value | <0.001 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alzahrani, H.; Alshehri, F.; Alsufiany, M.; Allam, H.H.; Almeheyawi, R.; Eid, M.M.; Sadarangani, K.P. Impact of the 2019 Coronavirus Disease Pandemic on Health-Related Quality of Life and Psychological Status: The Role of Physical Activity. Int. J. Environ. Res. Public Health 2021, 18, 3992. https://doi.org/10.3390/ijerph18083992
Alzahrani H, Alshehri F, Alsufiany M, Allam HH, Almeheyawi R, Eid MM, Sadarangani KP. Impact of the 2019 Coronavirus Disease Pandemic on Health-Related Quality of Life and Psychological Status: The Role of Physical Activity. International Journal of Environmental Research and Public Health. 2021; 18(8):3992. https://doi.org/10.3390/ijerph18083992
Chicago/Turabian StyleAlzahrani, Hosam, Fahad Alshehri, Muhsen Alsufiany, Hatem H. Allam, Rania Almeheyawi, Marwa M. Eid, and Kabir P. Sadarangani. 2021. "Impact of the 2019 Coronavirus Disease Pandemic on Health-Related Quality of Life and Psychological Status: The Role of Physical Activity" International Journal of Environmental Research and Public Health 18, no. 8: 3992. https://doi.org/10.3390/ijerph18083992
APA StyleAlzahrani, H., Alshehri, F., Alsufiany, M., Allam, H. H., Almeheyawi, R., Eid, M. M., & Sadarangani, K. P. (2021). Impact of the 2019 Coronavirus Disease Pandemic on Health-Related Quality of Life and Psychological Status: The Role of Physical Activity. International Journal of Environmental Research and Public Health, 18(8), 3992. https://doi.org/10.3390/ijerph18083992