3.1. Functional Layout
- (1)
Observation results
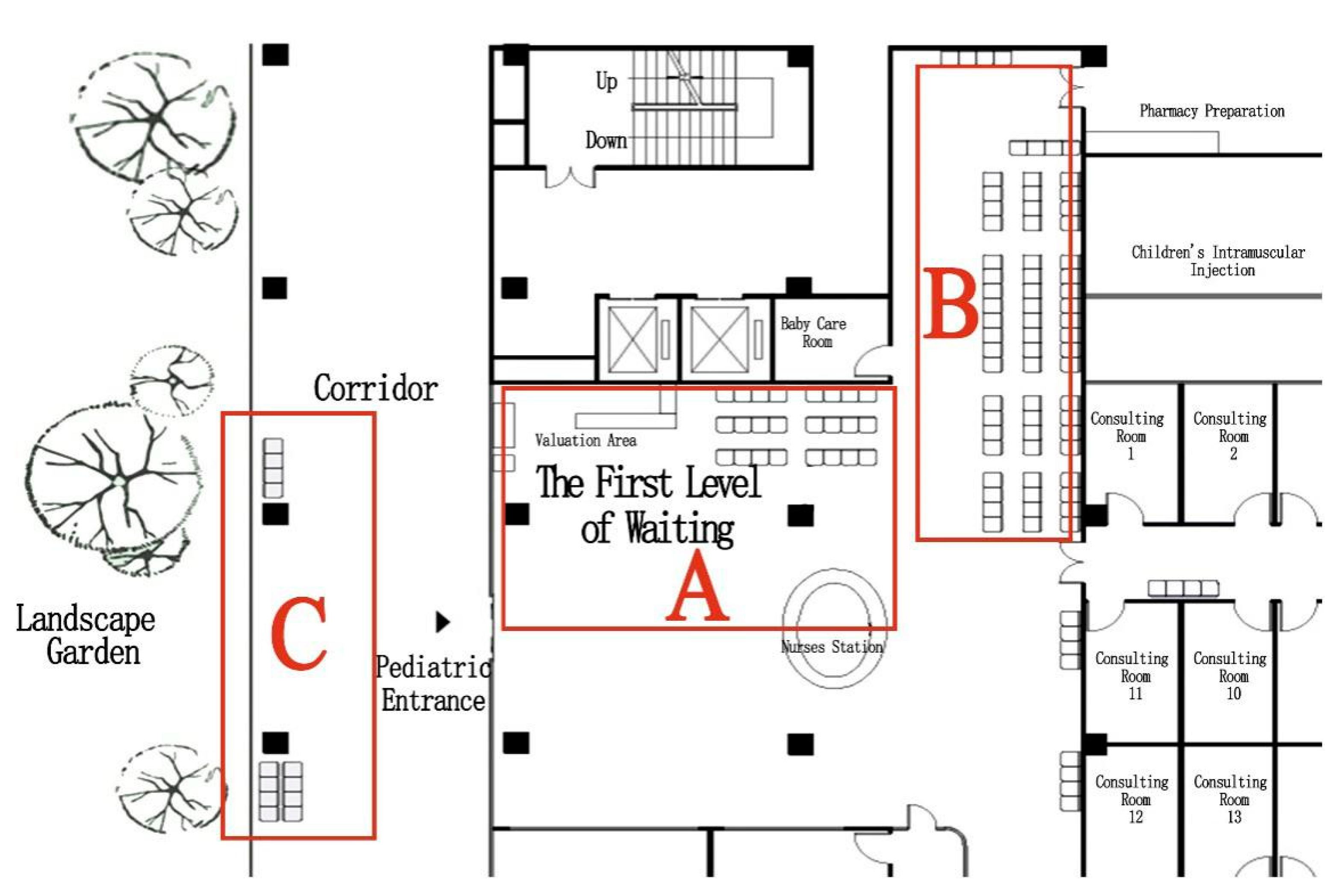
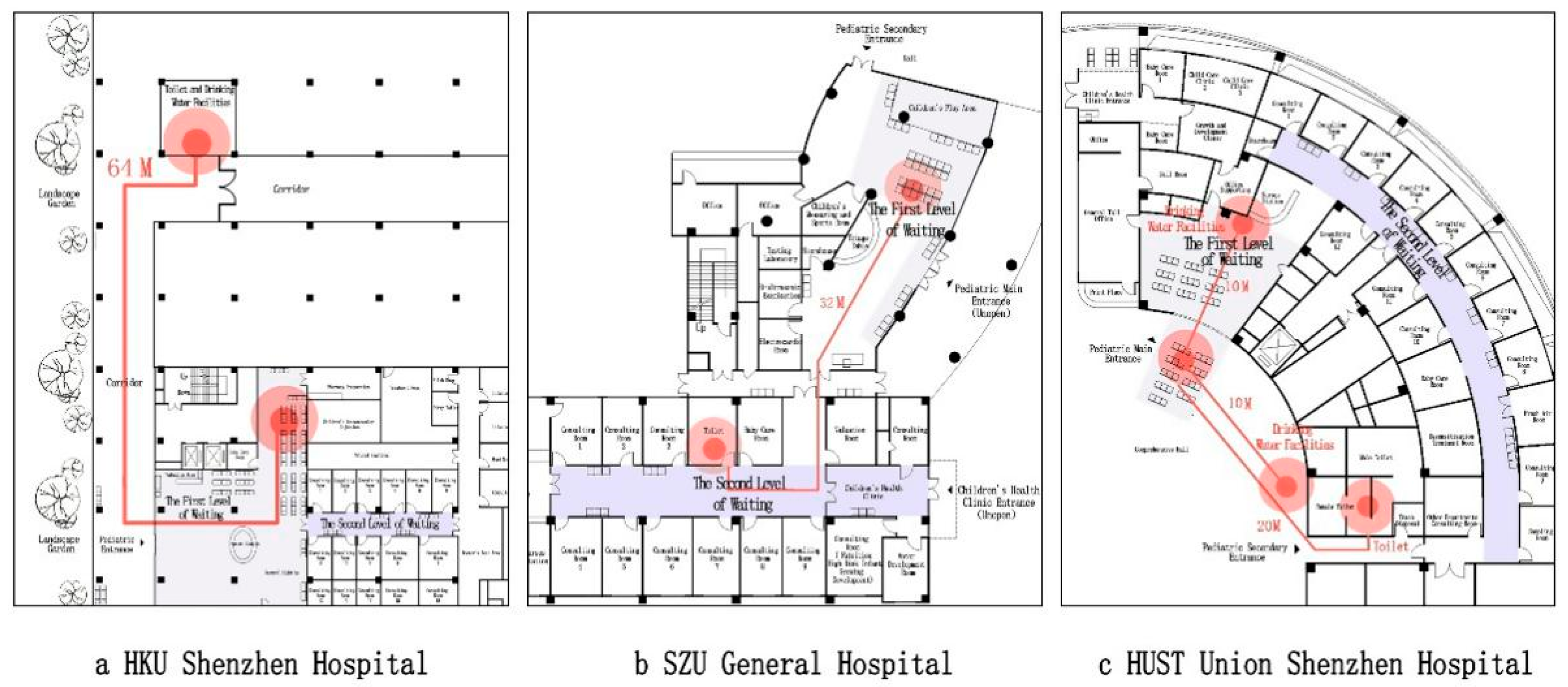
Layout of the waiting area: The survey at HKU Shenzhen Hospital (
Figure 2) revealed that the pediatric department has an outdoor landscaped garden, close to the semi-outdoor public corridor (point A in
Figure 2). Such a landscape has a soothing effect on patients while also maximizing natural lighting and ventilation. However, according to on-site observations, the seating is positioned away from the garden (point B in
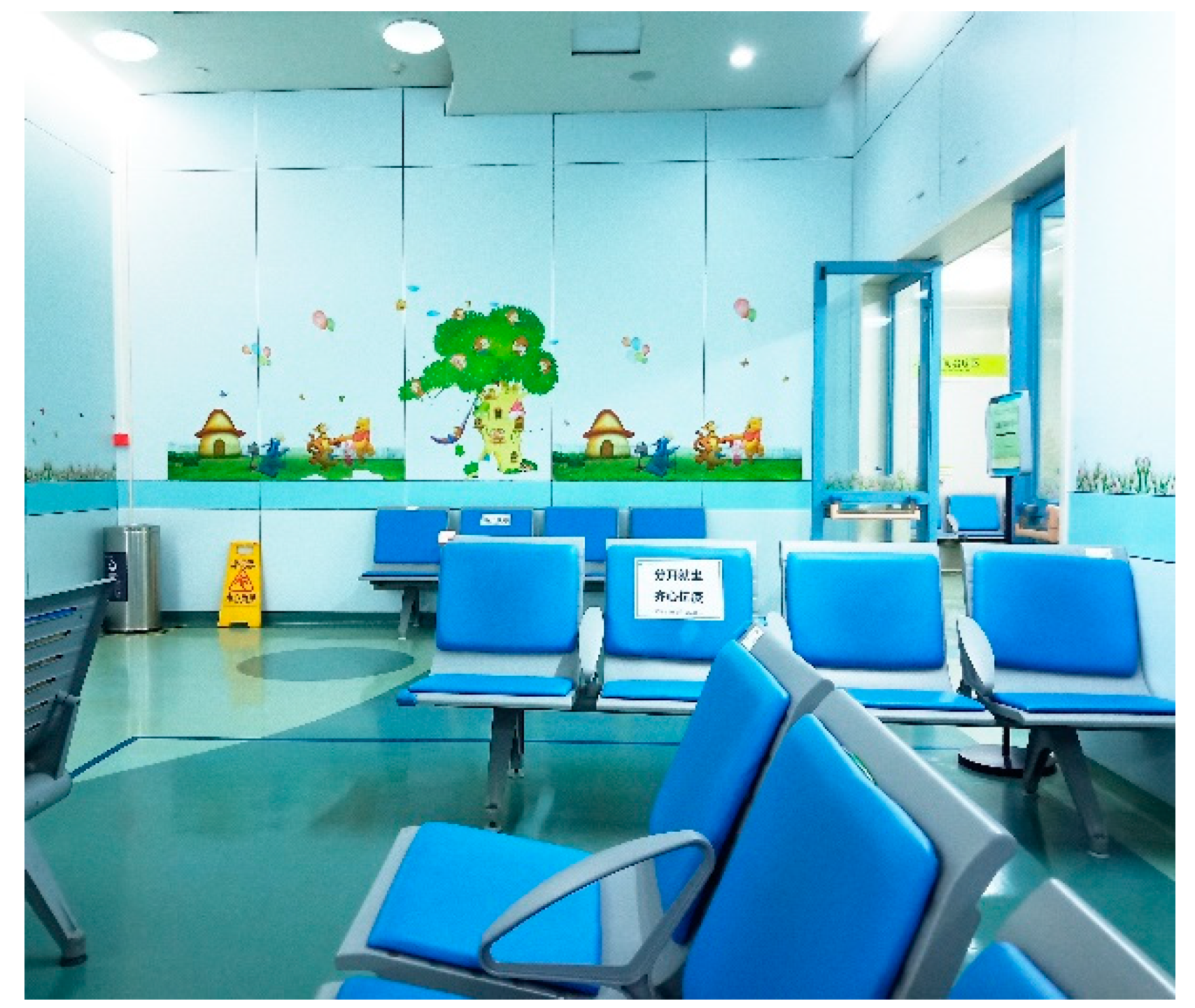
Figure 2) and the window facing the back of the seating was not open at the time of the study, so the overall environment in the waiting area was humid and heavy (
Figure 3). Therefore, some people preferred to wait for their diagnostic results in semi-outdoor space C (
Figure 4).
Inadequate divisions between waiting spaces: The survey in HUST revealed that four groups of families were required to gather at the entrance of the clinic. Unpredictable noise can be distracting for doctors, which may even trigger inaccurate diagnosis or medication advice (Ulrich et al., 2008). According to Hall’s theory of interpersonal communication distance, the social distance required by ordinary people is 1.22 m–3.66 m. The distance between waiting families in HUST was less than 1 m, intensifying the anxiety associated with receiving medical treatment. The solution offered by SZU General Hospital also failed to achieve the target effect due to mixed use of waiting spaces.
Waiting space occupied by strollers: All of the pediatric waiting areas were found to have problems with stroller obstruction. SZU General Hospital has the widest waiting corridor, at 3.5 m. However, when patients were seated on both sides, strollers still caused congestion in the corridor.
- (2)
Subjective preference results
Waiting area and corridor width: In the survey, 30.8% of the respondents preferred a waiting area larger than 80 square meters, which was larger than the existing waiting spaces in the three hospitals. Layout of waiting area: 45.1% of the respondents preferred a combined hallway waiting space; only 11.3% of the respondents chose an enclosed inner hallway, which was the least popular option. Size of mother and infant room: The expected area of the mother and infant room was 6–20 square meters. Size of children’s play area: 16.9% of the respondents felt that there was no need for a play area, mainly because they were worried about “insecurity” and “physical discomfort”. However, 30.8% of the respondents thought that the children’s play area should be 21–30 square meters and that diversified play facilities should be provided.
3.4. Environmental Details
- (1)
Observation results
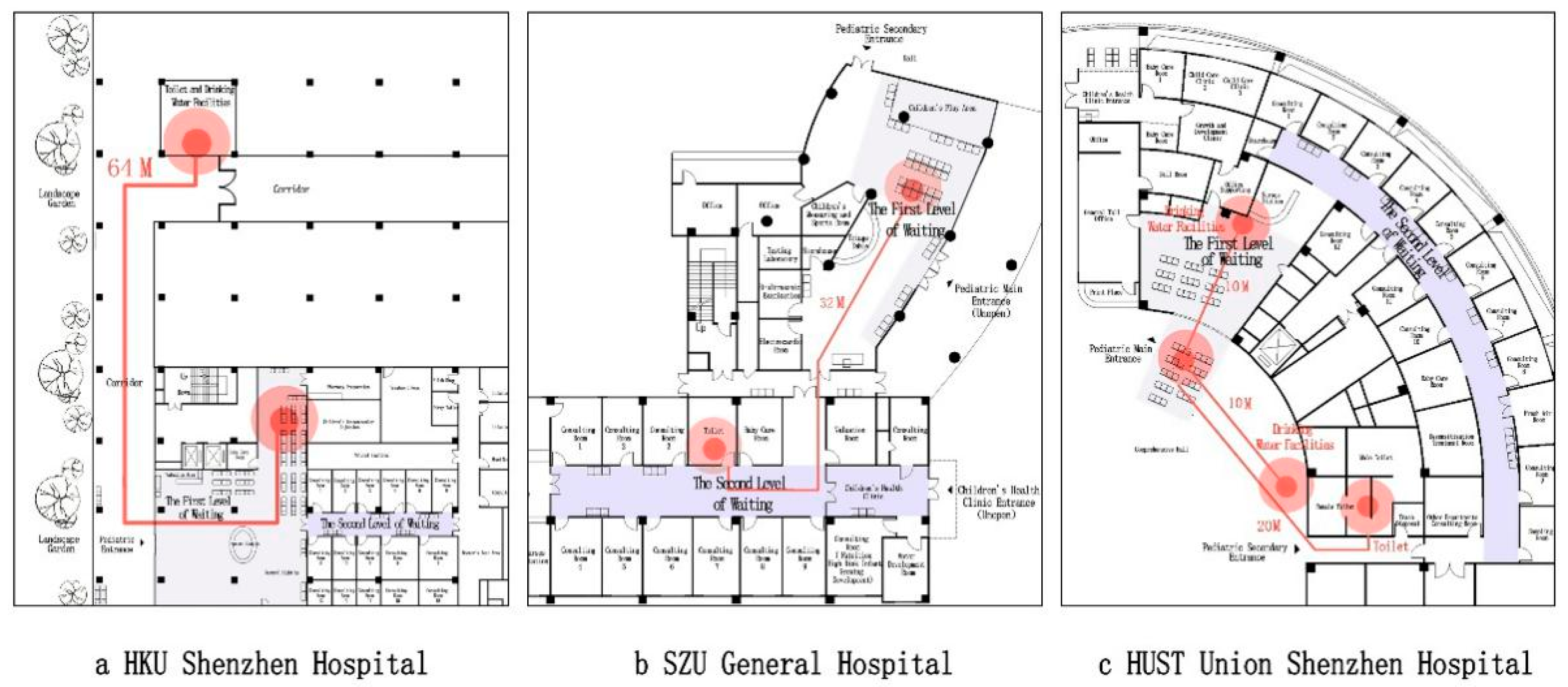
Lack of natural environment: At the HKU Shenzhen Hospital, the observation revealed a landscaped garden outside the waiting space, far away from the seating area. Distance from nature reduces its therapeutic effect. Some of the people waiting chose to wait near the garden, but this put them at risk of not hearing their names being called. In the HUST Union Shenzhen Hospital, the waiting space is enclosed by multiple walls and lacks natural scenery. The environment in the SZU General Hospital is the best, with large windows on the long side of the waiting space. There are no buildings outside the windows to block the line of sight. The view is wide and there is some natural scenery.
Inadequate child-friendly design: Some aspects of the design were found to fail to meet children’s usage requirements in the surveyed hospitals. The waiting areas have colorful cartoon decorations. Although the waiting area of the SZU General Hospital is equipped with child safe handrails, and its fire extinguisher facilities are equipped with anti-collision bars, the other two hospitals lack similar environmental considerations.
- (2)
Subjective preference results
View outside the window: 22.1% of the respondents believed that a pediatric waiting area must offer a view out of a window, and 38.5% of the respondents believed that such a view may be necessary. Number of indoor green plants: 43.6% of the respondents expected there to be 3–5 indoor green plants. Warm and cold colors: 67.2% of the respondents preferred warm colors such as red, yellow and orange. Anti-slip surface: 64.1% of the waiting patients thought that an anti-slip surface is necessary. Sound, light and ventilation: 57.9% of the respondents preferred a quiet environment, 65.1% preferred a brightly lit environment and 64.6% preferred natural ventilation.
3.5. Analysis
- (1)
Sample Validation and Reliability Analysis
A total of 240 questionnaire copies were distributed. HKU, SZU and HUST received 67, 74 and 68 valid questionnaires, with a recovery rate of 93%. To keep the same sample size, each hospital randomly selected 65 sample questionnaires by Excel for data analysis, and 195 questionnaires were selected for data analysis (
Table 3). Due to the limitations imposed by the children’s age on their cognitive abilities, the main questionnaires and interviews focused on the accompanying people/parents. Similar studies have focused on parents as the object of information collection (e.g., Cartland et al., 2018). In this study, children aged 3 and under accounted for 49.7% of the sample, children aged 4–6 accounted for 34.4% and preschool children were the main waiting population. The companions were mostly the children’s parents, of which fathers accounted for 41% and mothers accounted for 55.4%. The number of accompanying people ranged from 1 to 2, with an average of 1.6.
The Cronbach’s alpha coefficients for the total data and the grouped data of the three hospitals were 0.948, 0.960, 0.937 and 0.946, respectively. As these values are all greater than 0.8, the questionnaire results were assumed to reflect the subjective satisfaction status of the waiting population.
- (2)
Validity analysis and factor analysis
Kaiser–Meyer–Olkin (KMO) is a coefficient that reflects the validity of data, ranging from 0 to 1. A larger value indicates a higher correlation between variables, which is suitable for factor analysis. In general, the actual threshold is greater than 0.7. Validity analysis results showed that KMO was 0.914, greater than 0.7, indicating that the sample data were valid. Significance level was <0.001, indicating that the data is valid and suitable for factor analysis.
In the component matrix obtained by rotation, principal factors could generalize second-level indexes, and a correlation value that exceeds 0.5 is considered as a main factor. Thus, the 27 indicators are reduced to 6 main factors, which belong to 4 categories: (1). Functional layout: layout and area; (2) Flow organization; (3) Supporting facilities; and (4) Environmental details: physical environment and landscape environment.
Of the six main factors, the first factor related to supporting facilities. The second related to flow organization. The third and fourth factors can be summed up as functional layout and site area. The fifth factor related to light and dark, ventilation and acoustics, which can be summarized as the physical environment in the environmental details. The sixth factor was related to the landscape outside the window and the type(s) and quantity of indoor green plants. This factor can be summarized as landscape environment in the environmental details. Total analysis of variance revealed that the six factors had an explanatory ability of 69.762% (
Table 4). The selected factors showed a high level of representativeness and were able to explain users’ subjective satisfaction evaluation of the waiting space well.
- (3)
Regression analysis
In regression analysis, it is assumed that the independent variable has no significant effect on the dependent variable, ANOVA is used to analyze whether the hypothesis is valid and less than 0.01 would overturn the hypothesis.
Table 5 indicates that at least one of the six factors could have a significant impact on the satisfaction of waiting space.
Regression analysis of the six factors showed that the overall regression effect was strong. The linear regression equation showed that the significance of the six factors was 0.000 (less than 0.05), indicating that all six factors had a significant positive correlation with the dependent variable (
Table 6). The results indicate that supporting facilities and environmental details (physical environment) have the closest relationship with satisfaction with the waiting space.
In general, satisfaction with environmental details (physical environment), supporting facilities and waiting space led to a higher satisfaction rate than the other factors. Environmental details (landscape environment), functional layout and the humanization of functional requirements also had an impact on satisfaction evaluation.
- (4)
Satisfaction analysis
Spearman correlation analysis showed that all
p values were 0.000, indicating that each index was correlated with satisfaction. As shown in
Table 7, all 27 second-level indicators are positively correlated with satisfaction.
Analysis of the average values of the first-level indicators (functional layout, flow organization, supporting facilities, environmental details) revealed similar levels of satisfaction with the waiting space at the HKU Shenzhen Hospital and the SZU General Hospital. At these hospitals, users’ satisfaction with the functional layout and environmental details was high, and the difference between the numerical values was less than 0.22. At HUST Union Shenzhen Hospital, users were more satisfied with the flow organization and supporting facilities, with the largest gap between the four numerical values being 0.35; satisfaction with environmental details was only 3.55, which is lower than the values for the other first-level indicators.
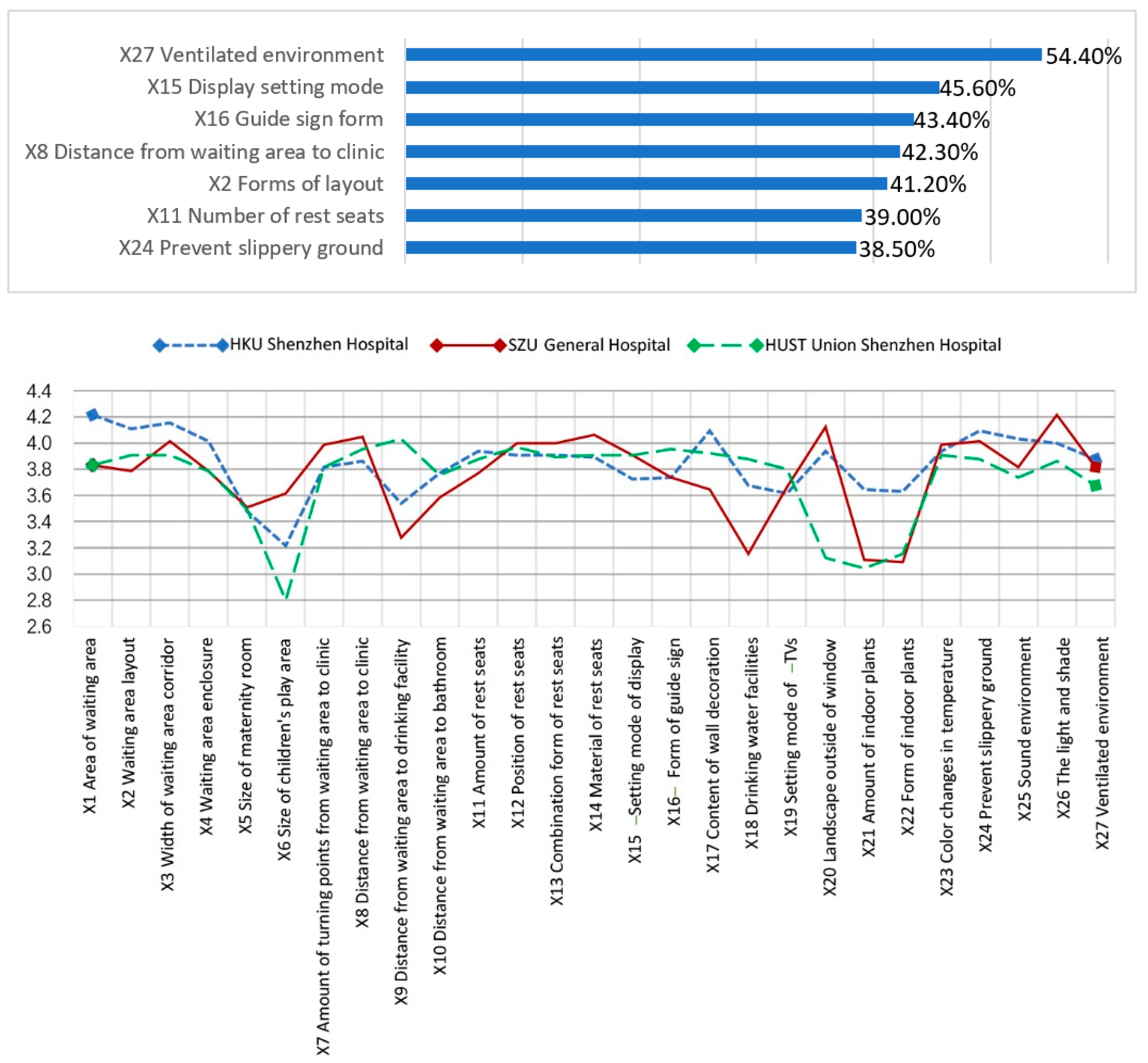
In the analysis of the average values of the secondary indicators (
Figure 7), satisfaction with indoor green plants (types and quantity) was low, indicating that the waiting areas fail to meet the human need for a view of nature. In addition, the size of children’s play areas should be increased.
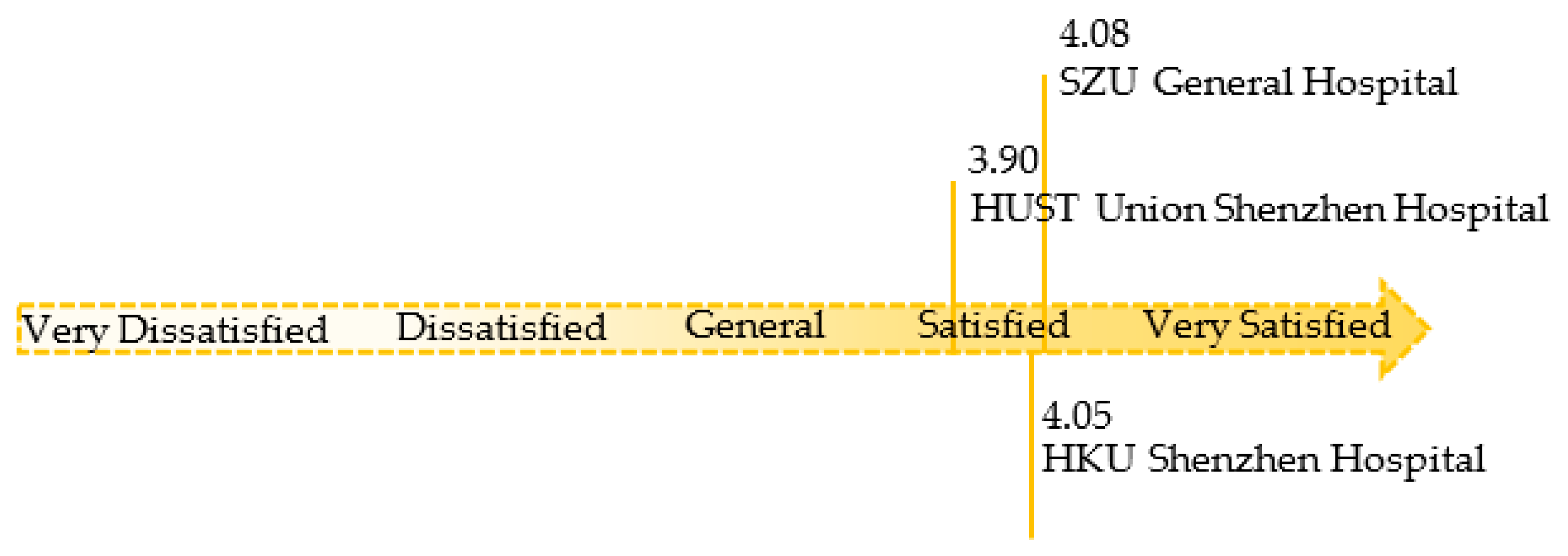
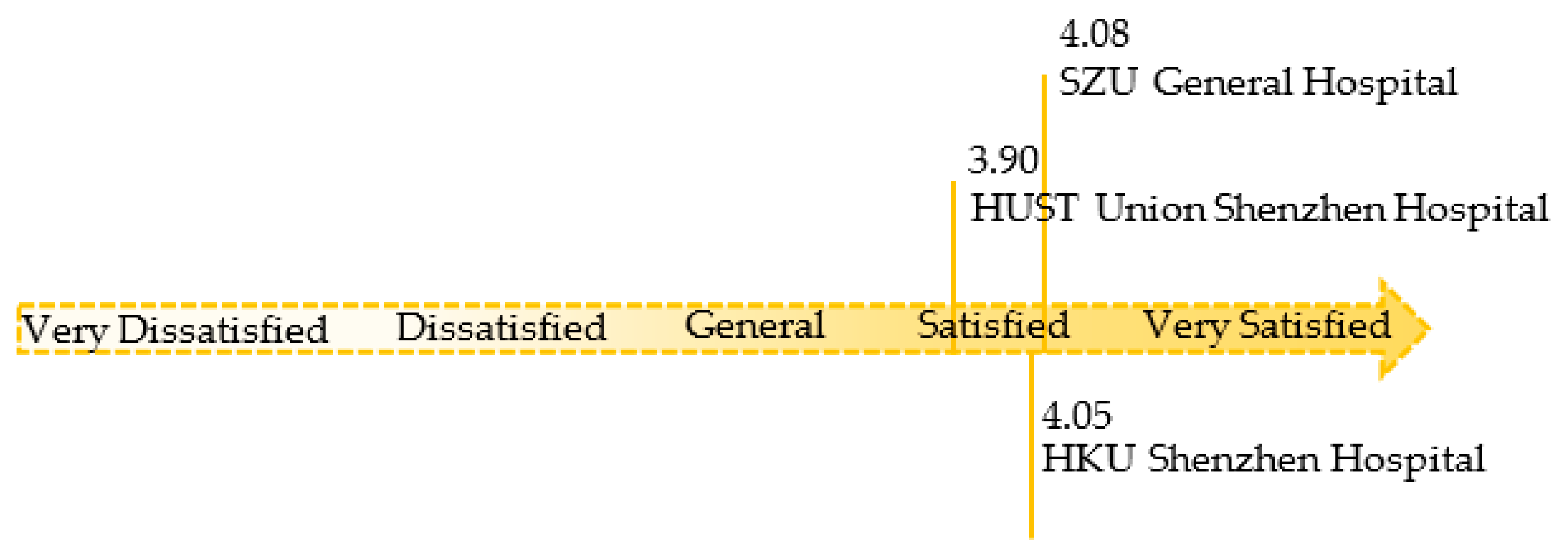
The overall satisfaction value for the three hospitals was between 3.90 and 4.08 (
Figure 8). The satisfaction ratings for SZU General Hospital and HKU Shenzhen Hospital were 4.08 and 4.05, respectively, higher than the satisfaction rate for HUST Union Shenzhen Hospital (3.9).
- (5)
Importance Analysis
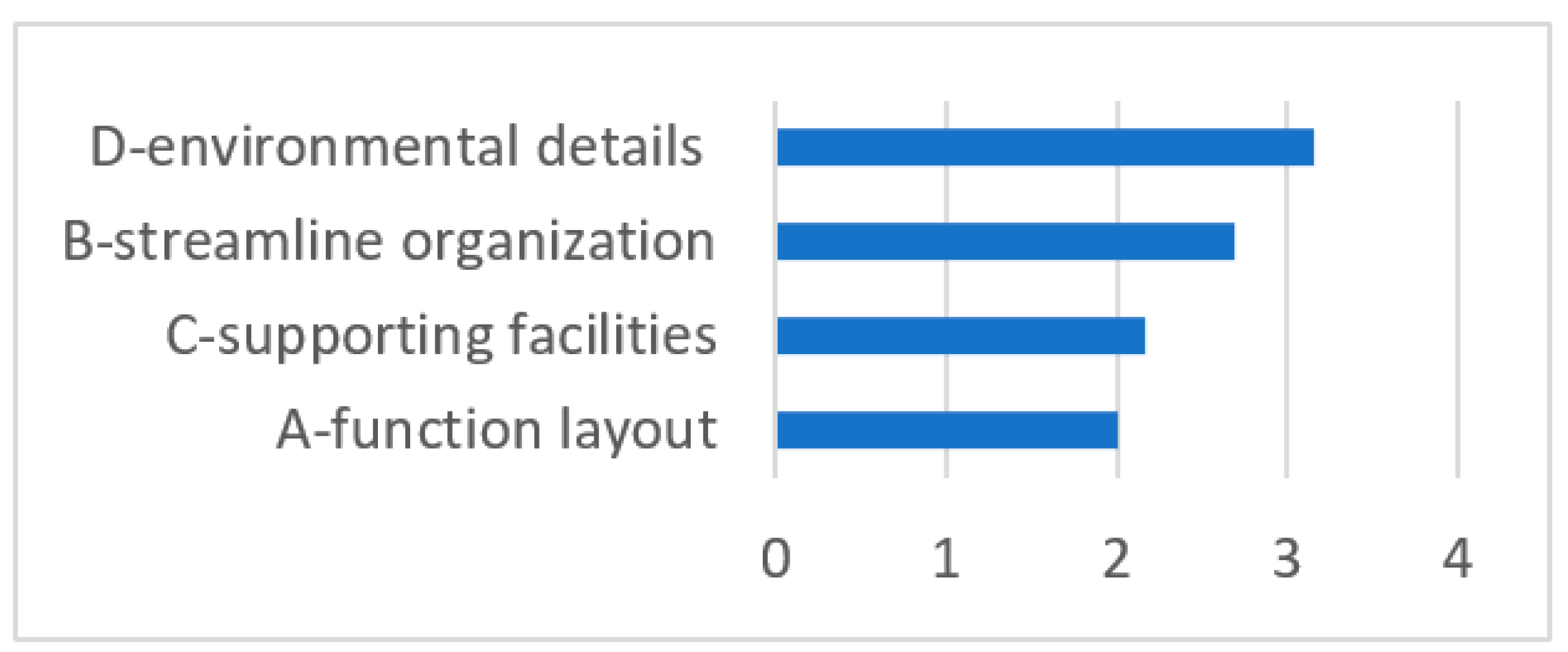
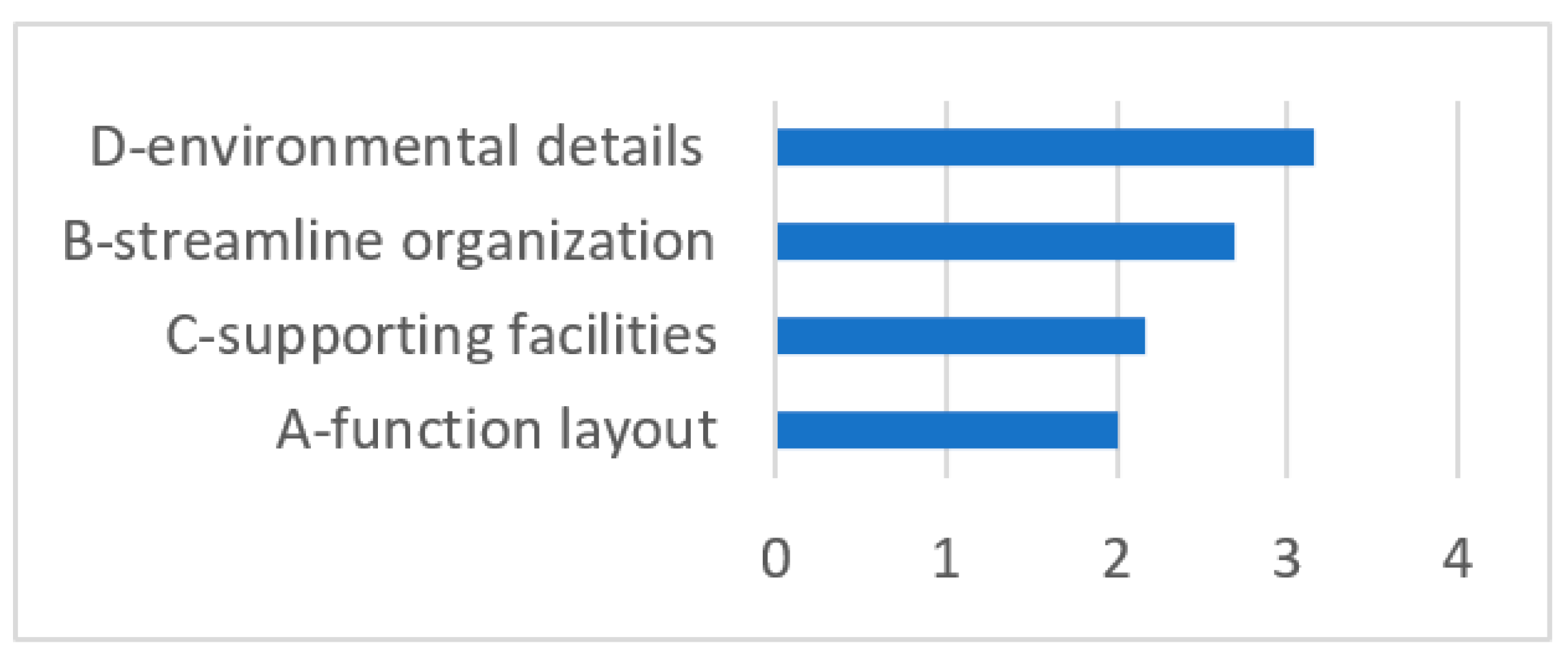
This study collected the subjective importance rankings of the questionnaire subjects for the four first-level indicators. The ranking by importance to the waiting population of the spatial elements was D—environmental details > B—flow organization > C—supporting facilities > A—functional layout (
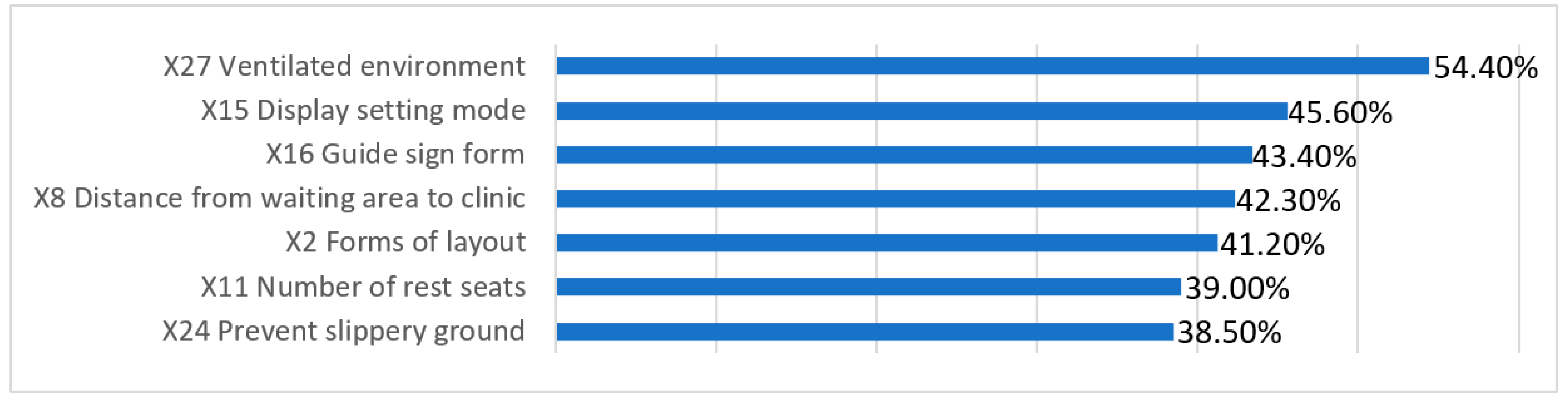
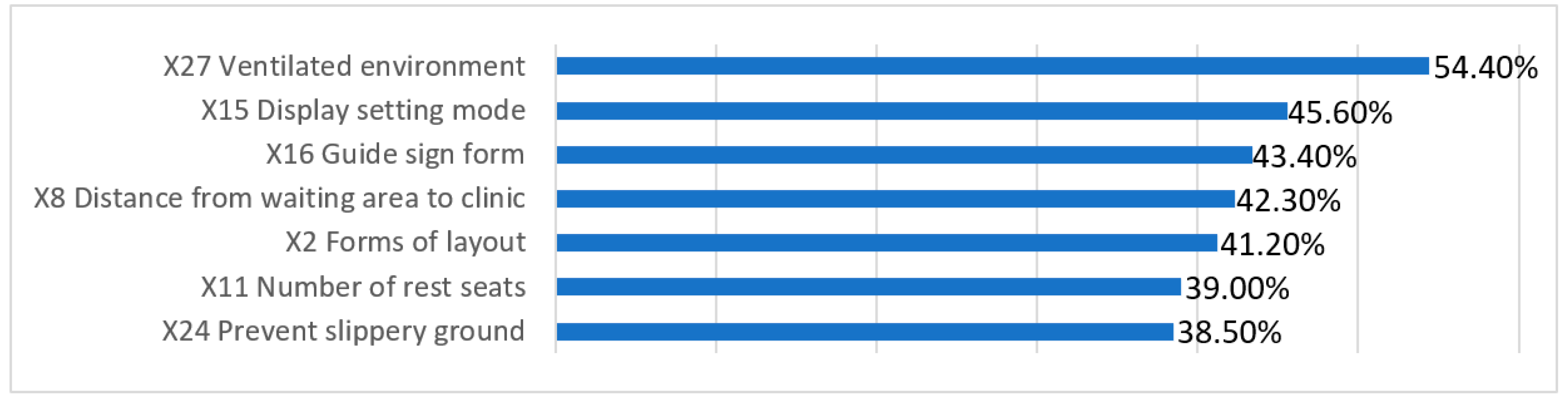
Figure 9). In general, environmental details were the most important, flow organization and supporting facilities were the second most important and the functional layout was the least important. From the ranking of the importance of secondary indicators, it can be seen that the respondents emphasized objective elements of the waiting space that meet basic waiting needs (
Figure 10), such as a well-ventilated environment, call number display screens and guide signs. Factors such as the layout of the waiting space and distance from the clinic were also key elements.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}


