Use of Online Food Delivery Services to Order Food Prepared Away-From-Home and Associated Sociodemographic Characteristics: A Cross-Sectional, Multi-Country Analysis

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Measures
2.3. Study Sample
2.4. Statistical Analysis
3. Results
3.1. Sociodemographic Characteristics
3.2. Meals Purchased Away-From-Home
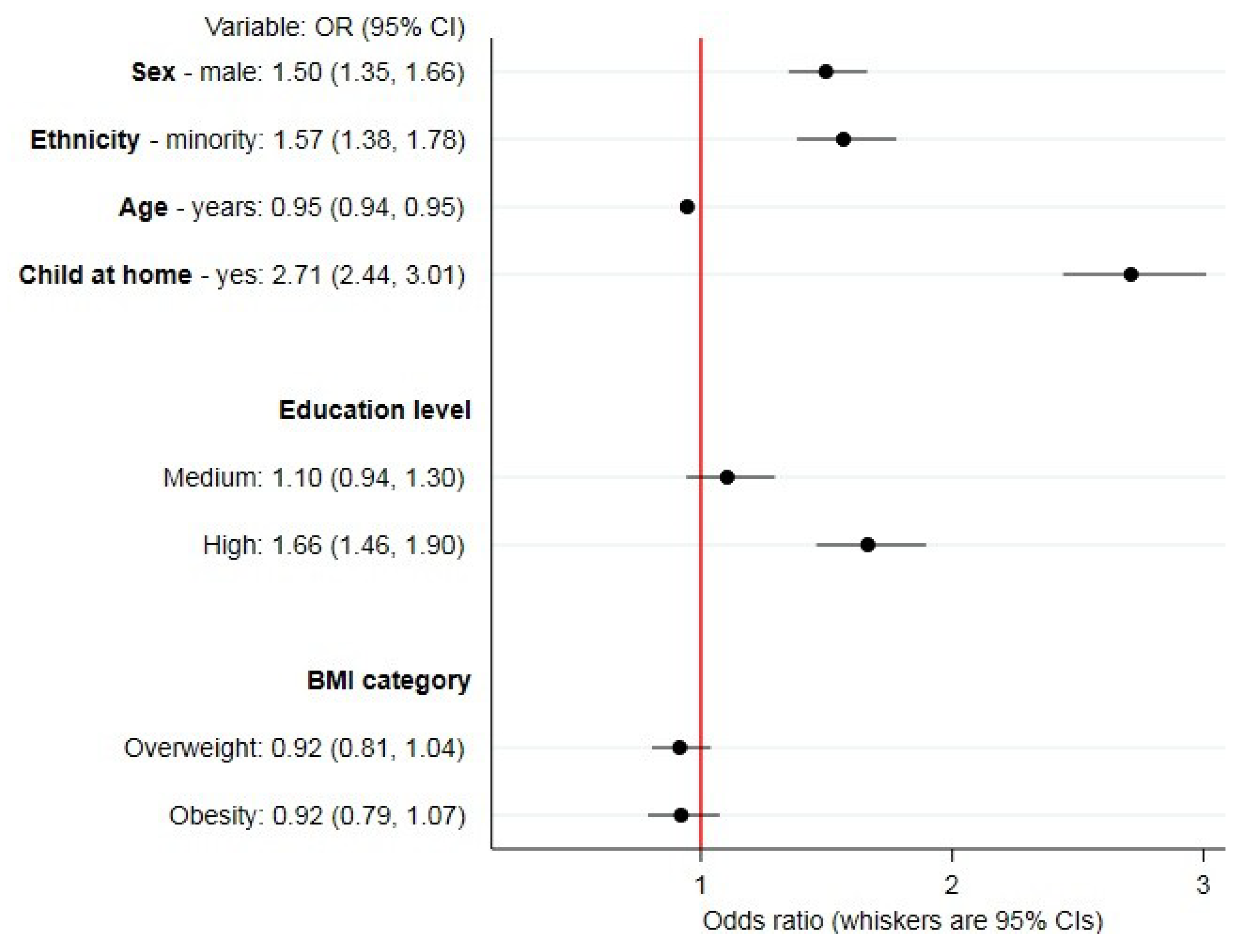
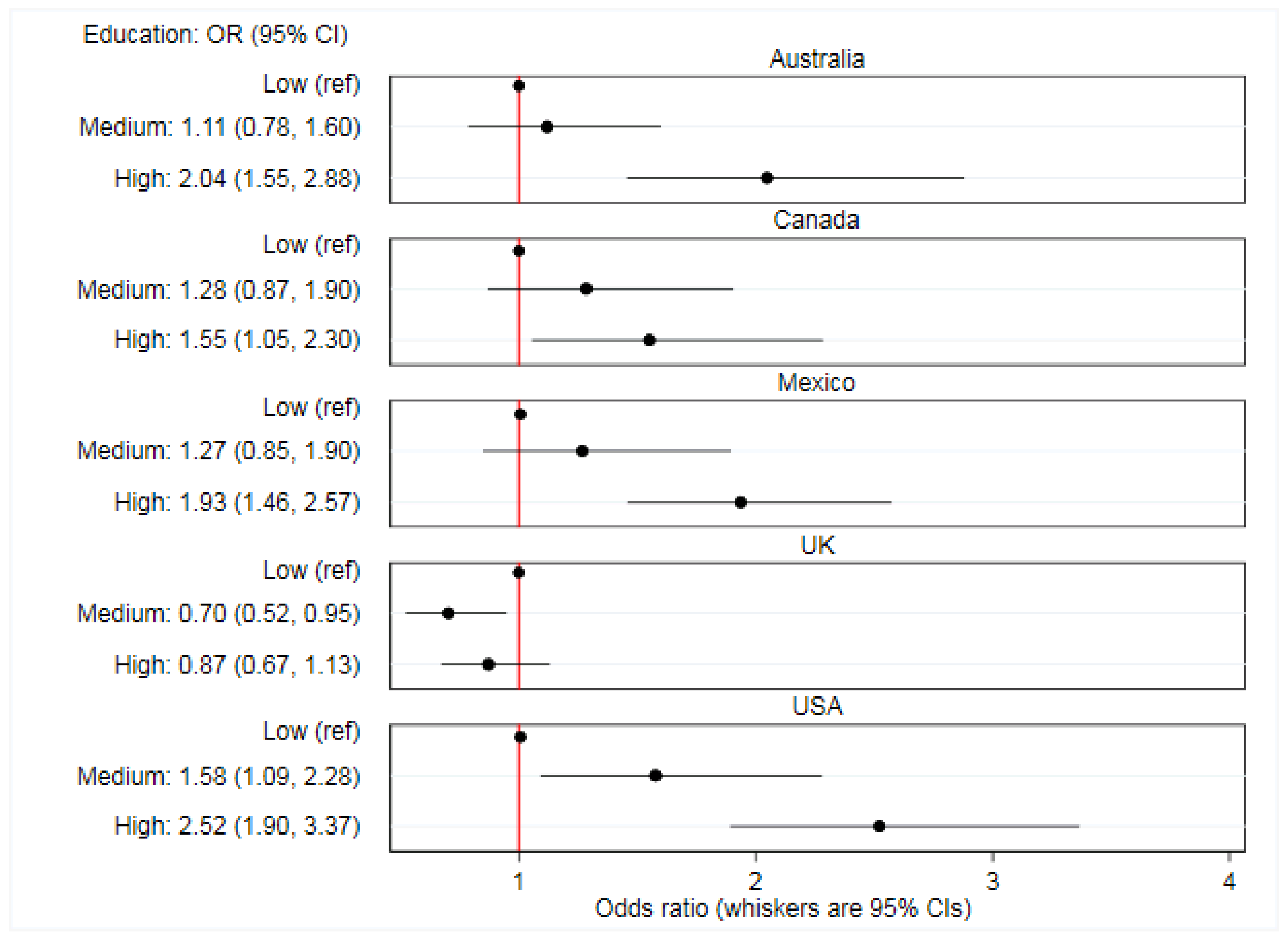
3.3. Sociodemographic Correlates of Online Food Delivery Service Use
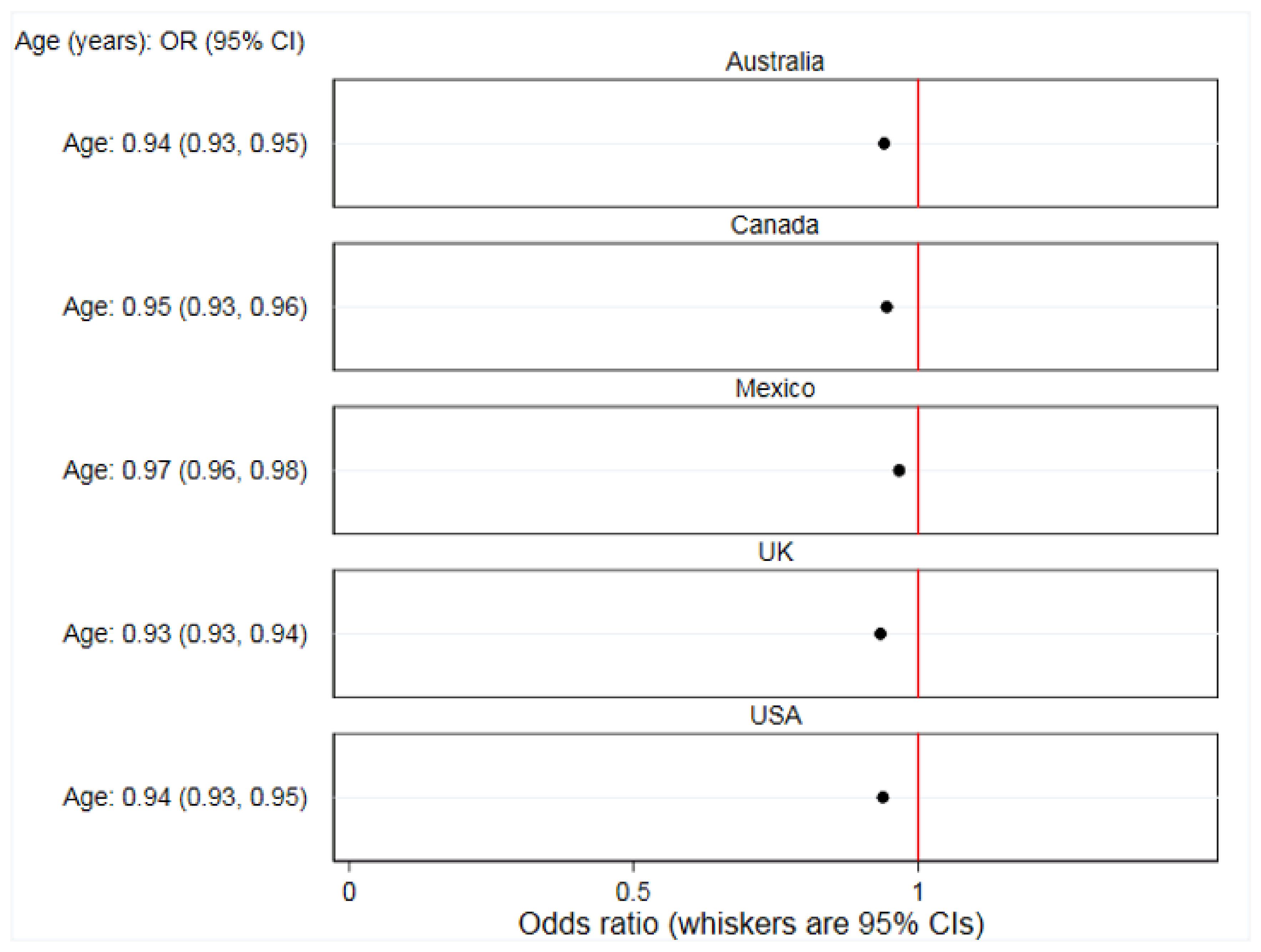
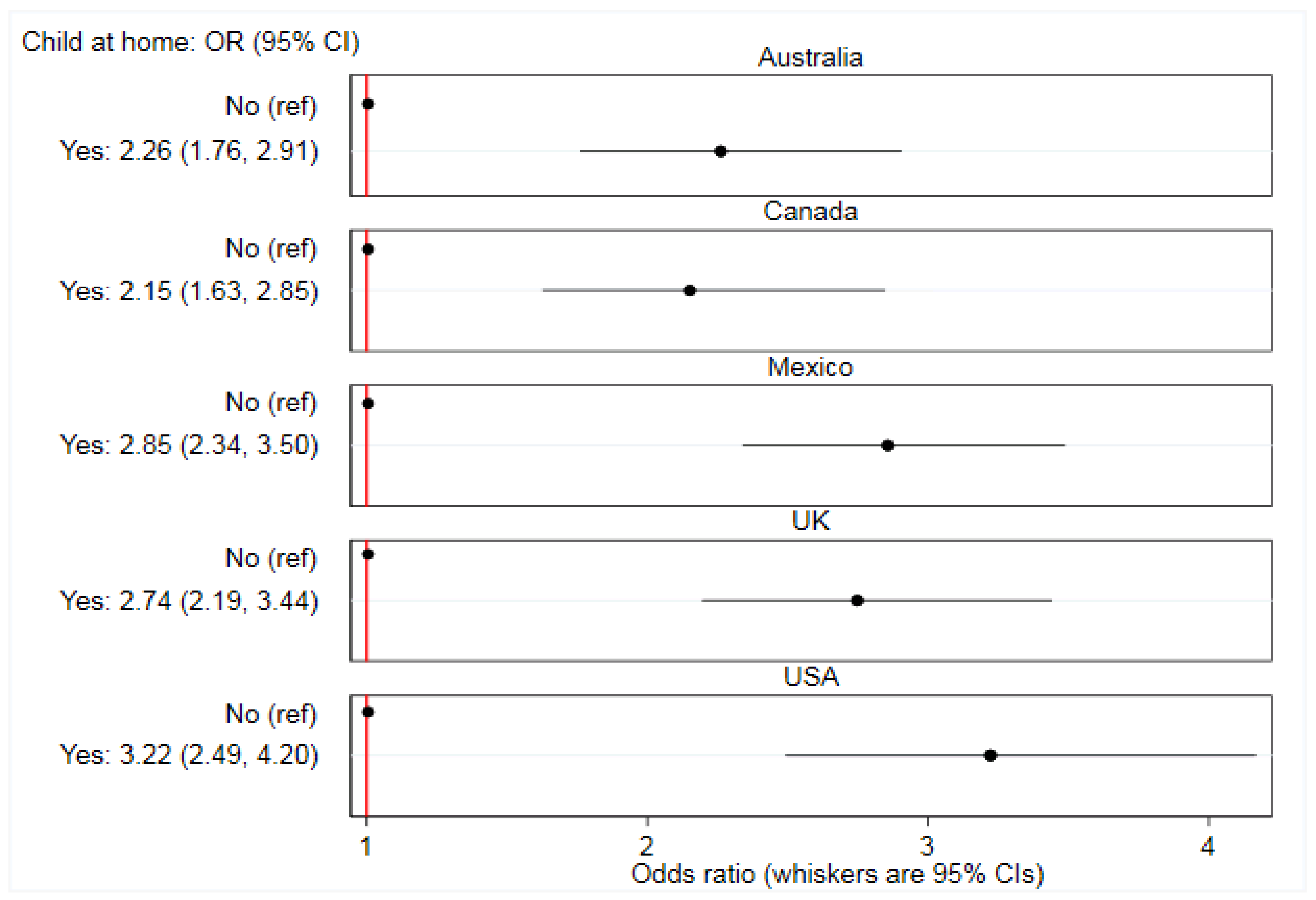
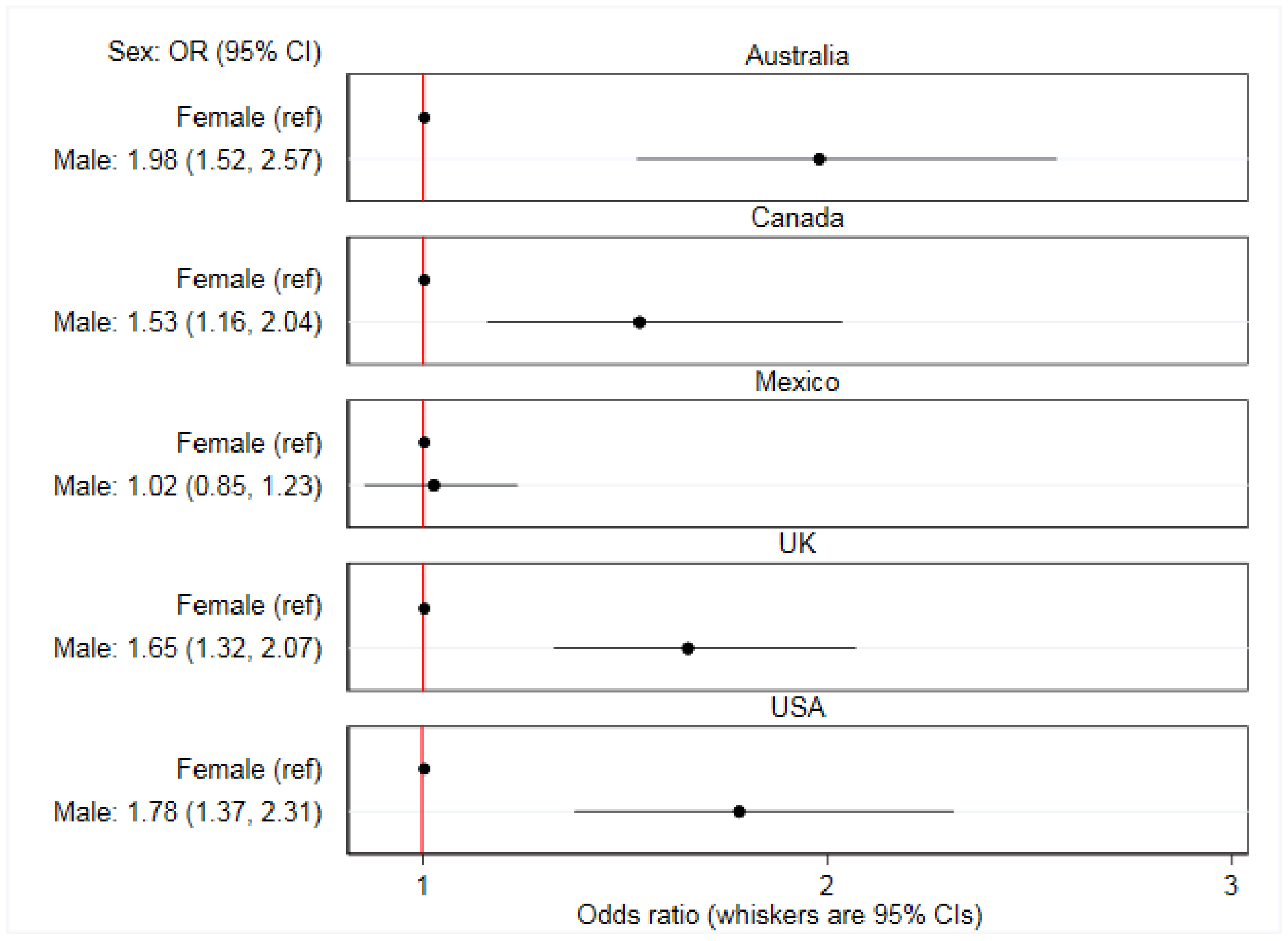
3.4. Between-Country Variation
4. Discussion
4.1. Summary of Findings
4.2. Interpretation of Findings and Further Research
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Jia, P.; Luo, M.; Li, Y.; Zheng, J.-S.; Xiao, Q.; Luo, J. Fast-food restaurant, unhealthy eating, and childhood obesity: A systematic review and meta-analysis. Obes. Rev. 2019, 1–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Health Observatory (GHO) data. Available online: https://www.who.int/gho/ncd/risk_factors/overweight_text/en/ (accessed on 29 March 2020).
- Imamura, F.; Micha, R.; Khatibzadeh, S.; Fahimi, S.; Shi, P.; Powles, J.; Mozaffarian, D. Dietary quality among men and women in 187 countries in 1990 and 2010: A systematic assessment. Lancet Glob. Health 2015, 3, 132–142. [Google Scholar] [CrossRef] [Green Version]
- Finegood, D.T.; Merth, T.D.N.; Rutter, H. Implications of the foresight obesity system map for solutions to childhood obesity. Obesity 2010, 18, S13–S16. [Google Scholar] [CrossRef] [PubMed]
- Rutter, H. The single most important intervention to tackle obesity. Int. J. Public Health 2012, 57, 657–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaworowska, A.; Blackham, T.; Stevenson, L.; Davies, I.G. Determination of salt content in hot takeaway meals in the United Kingdom. Appetite 2012, 59, 517–522. [Google Scholar] [CrossRef]
- Jaworowska, A.; Toni, M.B.; Rachel, L.; Catherine, T.; Matthew, A.; Leonard, S.; Ian, G.D. Nutritional composition of takeaway food in the UK. Nutr. Food Sci. 2014, 44, 414–430. [Google Scholar] [CrossRef]
- Lachat, C.; Nago, E.; Verstraeten, R.; Roberfroid, D.; Van Camp, J.; Kolsteren, P. Eating out of home and its association with dietary intake: A systematic review of the evidence. Obes Rev. 2012, 13, 329–346. [Google Scholar] [CrossRef]
- Scourboutakos, M.J.; L’Abbé, M.R. Restaurant menus: Calories, caloric density, and serving size. Am. J. Prev. Med. 2012, 43, 249–255. [Google Scholar] [CrossRef]
- Todd, J.E.; Mancino, L.; Lin, B.-H. The impact of food away from home on adult diet quality. Available online: https://www.ers.usda.gov/webdocs/publications/46352/8170_err90_1_.pdf (accessed on 29 March 2020).
- Popkin, B.M.; Adair, L.S.; Ng, S.W. Global nutrition transition and the pandemic of obesity in developing countries. Nutr. Rev. 2012, 70, 3–21. [Google Scholar] [CrossRef] [Green Version]
- Burgoine, T.; Mackenbach, D.J.; Lakerveld, J.; Forouhi, G.N.; Griffin, J.S.; Brage, S.; Wareham, J.N.; Monsivais, P. Interplay of socioeconomic status and supermarket distance is associated with excess obesity risk: A UK cross-sectional study. Int. J. Environ. Res. Public Health 2017, 14, 1290. [Google Scholar] [CrossRef] [Green Version]
- United States Department of Agriculture Economic Research Service. Food prices and spending. Available online: https://www.ers.usda.gov/data-products/ag-and-food-statistics-charting-the-essentials/food-prices-and-spending/ (accessed on 29 March 2020).
- Maimaiti, M.; Zhao, X.; Jia, M.; Ru, Y.; Zhu, S. How we eat determines what we become: Opportunities and challenges brought by food delivery industry in a changing world in China. Eur. J. Clin. Nutr. 2018, 72, 1282–1286. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.; Piecyk, M.; Piotrowska, M. An analysis of online shopping and home delivery in the UK. Available online: https://westminsterresearch.westminster.ac.uk/item/q16z5/analysis-of-online-shopping-and-home-delivery-in-the-uk (accessed on 14 February 2020).
- Yeo, V.C.S.; Goh, S.-K.; Rezaei, S. Consumer experiences, attitude and behavioral intention toward online food delivery (OFD) services. J. Retail. Consum. Serv. 2017, 35, 150–162. [Google Scholar] [CrossRef]
- Deliveroo. About Deliveroo. Available online: https://deliveroo.co.uk/about-us (accessed on 28 October 2019).
- Uber Eats. When and where is Uber Eats available? Available online: https://help.uber.com/ubereats/article/when-and-where-is-uber-eats-available-?nodeId=3f8de61e-09dd-4844-afb2-749c9ffc65a8 (accessed on 17 December 2019).
- Just Eat. 2019 Half Year Results. Available online: https://jeweb-11431-s3.s3.eu-west-2.amazonaws.com/application/files/3615/6455/1992/Just_Eat_plc_-_2019_Half_Year_Results_RNS.pdf (accessed on 23 September 2019).
- Grubhub. What is Grubhub? Available online: https://about.grubhub.com/about-us/what-is-grubhub/default.aspx (accessed on 6 April 2020).
- Statista. Online Food Delivery Report 2019. Available online: https://www.statista.com/study/40457/food-delivery/ (accessed on 21 February 2020).
- Robinson, E.; Jones, A.; Whitelock, V.; Mead, B.R.; Haynes, A. (Over)eating out at major UK restaurant chains: Observational study of energy content of main meals. BMJ 2018, 363, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suhartanto, D.; Helmi Ali, M.; Tan, K.H.; Sjahroeddin, F.; Kusdibyo, L. Loyalty toward online food delivery service: The role of e-service quality and food quality. J. Foodserv. Bus. Res. 2019, 22, 81–97. [Google Scholar] [CrossRef]
- Hammond, D.; White, C.M.; Rynard, V.L.; Vanderlee, L. International food policy study: Technical report 2018 survey (Wave 2). Available online: http://foodpolicystudy.com/methods/ (accessed on 1 October 2019).
- Kant, A.K.; Whitley, M.I.; Graubard, B.I. Away from home meals: Associations with biomarkers of chronic disease and dietary intake in American adults, NHANES 2005–2010. Int. J. Obes. 2015, 39, 820–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiggers, D.; Vanderlee, L.; White, C.M.; Reid, J.L.; Minaker, L.; Hammond, D. Food sources among young people in five major Canadian cities. Can. J. Public Health 2018, 109, 506–515. [Google Scholar] [CrossRef]
- Galobardes, B.; Morabia, A.; Bernstein, M.S. Diet and socioeconomic position: Does the use of different indicators matter? Int. J. Epidemiol. 2001, 30, 334–340. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Body mass index—BMI. Available online: http://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 20 May 2019).
- Pedersen, A.B.; Mikkelsen, E.M.; Cronin-Fenton, D.; Kristensen, N.R.; Pham, T.M.; Pedersen, L.; Petersen, I. Missing data and multiple imputation in clinical epidemiological research. Clin. Epidemiol. 2017, 9, 157–166. [Google Scholar] [CrossRef] [Green Version]
- Van de Mortel, T.F. Faking it: Social desirability response bias in self-report research. Aust. J. Adv. Nurs. 2008, 25, 40–48. [Google Scholar]
- Langkamp, D.L.; Lehman, A.; Lemeshow, S. Techniques for handling missing data in secondary analyses of large surveys. Acad. Pediatr. 2010, 10, 205–210. [Google Scholar] [CrossRef] [Green Version]
- Sperandei, S. Understanding logistic regression analysis. Biochem. Med. 2014, 24, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Greenland, S. Modeling and variable selection in epidemiologic analysis. Am. J. Public Health 1989, 79, 340–349. [Google Scholar] [CrossRef] [Green Version]
- Backman, P. Delivery the disruptor. Available online: https://www.peterbackmanfs.com/delivery-the-disruptor (accessed on 29 March 2020).
- Keeble, M.; Burgoine, T.; White, M.; Summerbell, C.; Cummins, S.; Adams, J. How does local government use the planning system to regulate hot food takeaway outlets? A census of current practice in England using document review. Health Place 2019, 57, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.A.; Kartashov, A.I.; Ebbeling, C.B.; Van Horn, L.; Slattery, M.L.; Jacobs, D.R., Jr.; Ludwig, D.S. Fast-food habits, weight gain, and insulin resistance (the CARDIA study): 15-year prospective analysis. Lancet 2005, 365, 36–42. [Google Scholar] [CrossRef]
- Statista. Food delivery and takeaway market in the United Kingdom (UK)—Statistics & Facts. Available online: https://www.statista.com/topics/4679/food-delivery-and-takeaway-market-in-the-united-kingdom-uk/ (accessed on 20 February 2020).
- Miura, K.; Giskes, K.; Turrell, G. Socio-economic differences in takeaway food consumption among adults. Public Health Nutr. 2011, 15, 218–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mills, S.; Adams, J.; Wrieden, W.; White, M.; Brown, H. Sociodemographic characteristics and frequency of consuming home-cooked meals and meals from out-of-home sources: Cross-sectional analysis of a population-based cohort study. Public Health Nutr. 2018, 21, 2255–2266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Virudachalam, S.; Long, J.; Harhay, M.; Polsky, D.; Feudtner, C. Prevalence and patterns of cooking dinner at home in the USA: National Health and nutrition examination survey (NHANES) 2007–2008. Public Health Nutr. 2014, 17, 1022–1030. [Google Scholar] [CrossRef] [Green Version]
- Taillie, L.S. Who’s cooking? Trends in US home food preparation by gender, education, and race/ethnicity from 2003 to 2016. Nutr. J. 2018, 17, 41–50. [Google Scholar] [CrossRef] [Green Version]
- Clifford Astbury, C.; Penney, T.L.; Adams, J. Comparison of individuals with low versus high consumption of home-prepared food in a group with universally high dietary quality: A cross-sectional analysis of the UK National Diet & Nutrition Survey (2008–2016). Int. J. Behav. Nutr. Phys. Act. 2019, 16, 9–24. [Google Scholar] [CrossRef] [Green Version]
- Kern, D.M.; Auchincloss, A.H.; Stehr, M.F.; Roux, A.V.D.; Moore, L.V.; Kanter, G.P.; Robinson, L.F. Neighborhood prices of healthier and unhealthier foods and associations with diet quality: Evidence from the multi-ethnic study of atherosclerosis. Int J. Environ. Res. Public Health 2017, 14, 1394. [Google Scholar] [CrossRef] [Green Version]
- Liese, A.D.; Ma, X.; Hutto, B.; Sharpe, P.A.; Bell, B.A.; Wilcox, S. Food shopping and acquisition behaviors in relation to BMI among residents of low-income communities in South Carolina. Int J. Environ. Res. Public Health 2017, 14, 1075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bates, S.; Reeve, B.; Trevena, H. A narrative review of online food delivery in Australia: Challenges and opportunities for public health nutrition policy. Public Health Nutr. 2020, 1–11, (epub ahead of print). [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Chan, A.H.S. A review of technology acceptance by older adults. Gerontechnology 2011, 10, 1–12. [Google Scholar] [CrossRef]
- Jabs, J.; Devine, C.M. Time scarcity and food choices: An overview. Appetite 2006, 47, 196–204. [Google Scholar] [CrossRef]
- Warin, M.; Jay, B.; Zivkovic, T. “Ready-made” assumptions: Situating convenience as care in the Australian obesity debate. Food Foodways 2019, 27, 273–295. [Google Scholar] [CrossRef]
- Turrell, G.; Giskes, K. Socioeconomic disadvantage and the purchase of takeaway food: A multilevel analysis. Appetite 2008, 51, 69–81. [Google Scholar] [CrossRef]
- Rydell, S.A.; Harnack, L.J.; Oakes, J.M.; Story, M.; Jeffery, R.W.; French, S.A. Why eat at fast-food restaurants: Reported reasons among frequent consumers. J. Am. Diet. Assoc. 2008, 108, 2066–2070. [Google Scholar] [CrossRef]
- Penney, T.L.; Jones, N.R.V.; Adams, J.; Maguire, E.R.; Burgoine, T.; Monsivais, P. Utilization of away-from-home food establishments, dietary approaches to stop hypertension dietary pattern, and obesity. Am. J. Prev. Med. 2017, 53, e155–e163. [Google Scholar] [CrossRef] [Green Version]
- Rivera, J.A.; Barquera, S.; Gonzalez-Cossio, T.; Olaiz, G.; Sepulveda, J. Nutrition transition in Mexico and in other Latin American countries. Nutr. Rev. 2004, 62, S149–S157. [Google Scholar] [CrossRef]
- Poelman, M.P.; Thornton, L.; Zenk, S.N. A cross-sectional comparison of meal delivery options in three international cities. Eur. J. Clin. Nutr. 2020, 1–9, (epub ahead of print). [Google Scholar] [CrossRef]
- PEW Research Center. Internet penetration rates are high in North America, Europe and parts of the Asia-Pacific 2018. Available online: https://www.pewresearch.org/global/2018/06/19/social-media-use-continues-to-rise-in-developing-countries-but-plateaus-across-developed-ones/pg_2018-06-19_global-tech_0-01/ (accessed on 24 January 2020).
- Krumpal, I. Determinants of social desirability bias in sensitive surveys: A literature review. Qual. Quant. 2013, 47, 2025–2047. [Google Scholar] [CrossRef]
- Cook, A.; Pryer, J.; Shetty, P. The problem of accuracy in dietary surveys. Analysis of the over 65 UK National Diet and Nutrition Survey. J. Epidemiol. Community Health 2000, 54, 611–616. [Google Scholar] [CrossRef] [PubMed]
- Galobardes, B.; Shaw, M.; Lawlor, D.A.; Lynch, J.W.; Davey Smith, G. Indicators of socioeconomic position (part 1). J. Epidemiol. Community Health 2006, 60, 7–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cummins, S.; Berger, N.; Cornelsen, L.; Eling, J.; Er, V.; Greener, R.; Kalbus, A.; Karapici, A.; Law, C.; Ndlovu, D.; et al. COVID-19: Impact on the urban food retail system, diet and health inequalities in the UK. Cities Health 2020, 1–11, (epub ahead of print). [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Australia (n = 3578) | Canada (n = 3698) | Mexico (n = 3515) | UK (n = 4694) | USA (n = 3893) | Total (n = 19,378) | p Value for Difference b | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Online food delivery service customers c | 498 | (13.9) | 327 | (8.8) | 895 | (25.5) | 747 | (15.9) | 461 | (11.9) | 2929 | (15.1) | p > 0.0001 |
| Variable | |||||||||||||
| Sex | p > 0.0001 | ||||||||||||
| Male | 305 | (61.1) | 196 | (60.0) | 433 | (48.3) | 422 | (56.4) | 273 | (59.2) | 1629 | (55.6) | |
| Ethnicity | p > 0.0001 | ||||||||||||
| Majority | 310 | (32.1) | 201 | (61.3) | 662 | (73.9) | 570 | (76.3) | 259 | (56.1) | 2001 | (68.3) | |
| Age (years) | |||||||||||||
| Median (IQR) | 31 | (25–40) | 33 | (26–41) | 34 | (27–42) | 32 | (25–41) | 33 | (26–38) | 33 | (26–41) | |
| Education | p > 0.0001 | ||||||||||||
| Low | 136 | (27.4) | 95 | (28.9) | 119 | (13.3) | 320 | (42.8) | 177 | (38.3) | 846 | (28.9) | |
| Medium | 133 | (26.6) | 110 | (33.7) | 90 | (10.1) | 171 | (22.9) | 35 | (7.6) | 538 | (18.4) | |
| High | 229 | (46.0) | 122 | (37.4) | 686 | (76.6) | 257 | (34.4) | 250 | (54.4) | 1545 | (52.7) | |
| BMI (kg/m2) | p > 0.0001 | ||||||||||||
| Not overweight (≤24.9) | 255 | (51.2) | 164 | (50.2) | 420 | (46.9) | 321 | (42.9) | 206 | (44.6) | 1366 | (46.6) | |
| Overweight (25.0–29.9) | 118 | (23.7) | 77 | (23.4) | 265 | (29.6) | 150 | (20.1) | 135 | (29.2) | 744 | (25.4) | |
| Obesity (≥30.0) | 52 | (10.3) | 60 | (18.2) | 145 | (16.1) | 106 | (14.2) | 77 | (16.7) | 439 | (15.0) | |
| Missing | 73 | (14.7) | 27 | (8.2) | 66 | (7.4) | 170 | (22.8) | 44 | (9.5) | 380 | (13.0) | |
| Child < 18 years in home | p > 0.0001 | ||||||||||||
| Yes | 226 | (45.4) | 131 | (40.0) | 639 | (71.4) | 364 | (48.7) | 240 | (51.9) | 1600 | (54.6) | |
| Australia (n = 3578) | Canada (n = 3698) | Mexico (n = 3515) | UK (n = 4694) | USA (n = 3893) | Total (n = 19378) | p Value for Difference a | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Online food delivery service customer’s b: n (%) | 498 | (13.9) | 327 | (8.8) | 895 | (25.5) | 747 | (15.9) | 461 | (11.9) | 2929 | (15.1) | |
| Online food delivery services c | p > 0.0001 | ||||||||||||
| Number of meals | 2.0 | (1.0–2.0) | 1.0 | (1.0–2.0) | 2.0 | (1.0–3.0) | 1.0 | (1.0–2.0) | 2.0 | (1.0–3.0) | 2.0 | (1.0–3.0) | |
| Proportion (%) | 40.0 | (50.0–57.1) | 40.0 | (25.0–66.7) | 33.3 | (23.1–50.0) | 50.0 | (33.3–100.0) | 33.3 | (25.0–50.0) | 35.7 | (25.0–50.0) | |
| Directly from food outlets for delivery c | p > 0.0001 | ||||||||||||
| Number of meals | 0.0 | (0.0–1.0) | 0.0 | (0.0–1.0) | 1.0 | (0.0–2.0) | 0.0 | (0.0–1.0) | 1.0 | (0.0–2.0) | 1.0 | (0.0–2.0) | |
| Proportion (%) | 0.0 | (0.0–28.6) | 0.0 | (0.0–28.6) | 25.0 | (0.0–40.0) | 0.0 | (0.0–25.0) | 20.0 | (0.0–33.3) | 16.7 | (0.0–33.3) | |
| Directly from food outlets in–person c | p > 0.0001 | ||||||||||||
| Number of meals | 2.0 | (0.0–3.0) | 1.0 | (0.0–3.0) | 2.0 | (1.0–4.0) | 1.0 | (0.0–2.0) | 2.0 | (1.0–4.0) | 2.0 | (0.0–3.0) | |
| Proportion (%) | 40.0 | (0.0–60.0) | 40.0 | (0.0–54.5) | 40.0 | (20.0–52.4) | 33.3 | (0.0–50.0) | 40.0 | (20.0–57.1) | 40.0 | (0.0–50.0) | |
| Non–online food delivery service customers d: n (%) | 2188 | (61.2) | 2420 | (65.4) | 2396 | (68.2) | 2439 | (52.0) | 2721 | (69.9) | 12163 | (62.8) | |
| Directly from food outlets for delivery c | p > 0.0001 | ||||||||||||
| Number of meals | 1.0 | (1.0–2.0) | 1.0 | (1.0–2.0) | 2.0 | (1.0–4.0) | 1.0 | (1.0–2.0) | 2.0 | (1.0–3.0) | 2.0 | (1.0–3.0) | |
| Proportion (%) | 66.7 | (50.0–100.0) | 100.0 | (40.0–100.0) | 75.0 | (50.0–100.0) | 100.0 | (50.0–100.0) | 100.0 | (40.0–100.0) | 83.3 | (50.0–100.0) | |
| Directly from food outlets in-person c | p > 0.0001 | ||||||||||||
| Number of meals | 2.0 | (1.0–3.0) | 2.0 | (1.0–3.0) | 3.0 | (2.0–4.0) | 2.0 | (1.0–3.0) | 2.0 | (1.0–4.0) | 2.0 | (1.0–3.0) | |
| Proportion (%) | 100.0 | (100.0–100.0) | 100.0 | (100.0–100.0) | 100.0 | (66.7–100.0) | 100.0 | (100.0–100.0) | 100.0 | (100.0–100.0) | 100.0 | (100.0–100.0) | |
| Country | OR b | 95% CI c | |
|---|---|---|---|
| Australia (reference) | - | - | |
| Canada | 0.65 | 0.54 | 0.78 |
| Mexico | 1.21 | 1.03 | 1.43 |
| UK | 1.39 | 1.18 | 1.64 |
| USA | 0.85 | 0.72 | 1.02 |
| Australia | 1.55 | 1.29 | 1.87 |
| Canada (reference) | - | - | |
| Mexico | 1.88 | 1.58 | 2.25 |
| UK | 2.15 | 1.79 | 2.57 |
| USA | 1.32 | 1.10 | 1.59 |
| Australia | 0.82 | 0.69 | 0.97 |
| Canada | 0.53 | 0.45 | 0.63 |
| Mexico (reference) | - | - | |
| UK | 1.14 | 0.98 | 1.33 |
| USA | 0.70 | 0.60 | 0.82 |
| Australia | 0.72 | 0.61 | 0.85 |
| Canada | 0.47 | 0.39 | 0.56 |
| Mexico | 0.88 | 0.75 | 1.02 |
| UK (reference) | - | - | |
| USA | 0.61 | 0.52 | 0.73 |
| Australia | 1.17 | 0.98 | 1.40 |
| Canada | 0.76 | 0.63 | 0.91 |
| Mexico | 1.43 | 1.22 | 1.67 |
| UK | 1.63 | 1.37 | 1.93 |
| USA (reference) | - | - | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keeble, M.; Adams, J.; Sacks, G.; Vanderlee, L.; White, C.M.; Hammond, D.; Burgoine, T. Use of Online Food Delivery Services to Order Food Prepared Away-From-Home and Associated Sociodemographic Characteristics: A Cross-Sectional, Multi-Country Analysis. Int. J. Environ. Res. Public Health 2020, 17, 5190. https://doi.org/10.3390/ijerph17145190
Keeble M, Adams J, Sacks G, Vanderlee L, White CM, Hammond D, Burgoine T. Use of Online Food Delivery Services to Order Food Prepared Away-From-Home and Associated Sociodemographic Characteristics: A Cross-Sectional, Multi-Country Analysis. International Journal of Environmental Research and Public Health. 2020; 17(14):5190. https://doi.org/10.3390/ijerph17145190
Chicago/Turabian StyleKeeble, Matthew, Jean Adams, Gary Sacks, Lana Vanderlee, Christine M. White, David Hammond, and Thomas Burgoine. 2020. "Use of Online Food Delivery Services to Order Food Prepared Away-From-Home and Associated Sociodemographic Characteristics: A Cross-Sectional, Multi-Country Analysis" International Journal of Environmental Research and Public Health 17, no. 14: 5190. https://doi.org/10.3390/ijerph17145190
APA StyleKeeble, M., Adams, J., Sacks, G., Vanderlee, L., White, C. M., Hammond, D., & Burgoine, T. (2020). Use of Online Food Delivery Services to Order Food Prepared Away-From-Home and Associated Sociodemographic Characteristics: A Cross-Sectional, Multi-Country Analysis. International Journal of Environmental Research and Public Health, 17(14), 5190. https://doi.org/10.3390/ijerph17145190