
Prevalence of Erectile Dysfunction and Help-Seeking Behavior Among Patients Attending Primary Healthcare Centers for Non-Urological Complaints

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Study Population
2.3. Data Collection
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. Study Population
3.2. Prevalence of Erectile Dysfunction
3.3. Help-Seeking Behaviors and Treatment Outcomes
3.4. Associations with Sociodemographic and Lifestyle Factors
3.5. Knowledge and Awareness
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fisher, W.A.; Rosen, R.C.; Eardley, I.; Sand, M.; Goldstein, I. Sexual experience of female partners of men with erectile dysfunction: The female experience of men’s attitudes to life events and sexuality (FEMALES) study. J. Sex. Med. 2005, 2, 675–684, Erratum in J. Sex. Med. 2006, 3, 189. [Google Scholar] [CrossRef]
- Kessler, A.; Sollie, S.; Challacombe, B.; Briggs, K.; Van Hemelrijck, M. The global prevalence of erectile dysfunction: A review. BJU Int. 2019, 124, 587–599. [Google Scholar] [CrossRef]
- Hatzimouratidis, K.; Amar, E.; Eardley, I.; Giuliano, F.; Hatzichristou, D.; Montorsi, F.; Vardi, Y.; Wespes, E.; European Association of Urology. Guidelines on male sexual dysfunction: Erectile dysfunction and premature ejaculation. Eur. Urol. 2010, 57, 804–814. [Google Scholar] [CrossRef]
- Raheem, O.A.; Su, J.J.; Wilson, J.R.; Hsieh, T.C. The association of erectile dysfunction and cardiovascular disease: A systematic critical review. Am. J. Men’s Health 2017, 11, 552–563. [Google Scholar] [CrossRef]
- Hatzimouratidis, K. Sildenafil in the treatment of erectile dysfunction: An overview of the clinical evidence. Clin. Interv. Aging 2006, 1, 403–414. [Google Scholar] [CrossRef]
- Williams, P.; McBain, H.; Amirova, A.; Newman, S.; Mulligan, K. Men’s beliefs about treatment for erectile dysfunction—What influences treatment use? A systematic review. Int. J. Impot. Res. 2021, 33, 16–42. [Google Scholar] [CrossRef]
- Alenezi, T.M.; Ahamed, S.S.; Almutairi, H.R.; Aleisa, M.F.; Alasmari, M.M.; Bagaies, A.A.; Albinhar, T.H. Prevalence and the associated factors of erectile dysfunction among Saudi married males. Cureus 2022, 14, e30998. [Google Scholar] [CrossRef]
- Simopoulos, E.F.; Trinidad, A.C. Male erectile dysfunction: Integrating psychopharmacology and psychotherapy. Gen. Hosp. Psychiatry 2013, 35, 33–38. [Google Scholar] [CrossRef]
- Albarakati, M.; El-Tholoth, H.S.; Alzahrani, A.; Alghamdi, O.S.; Alquliti, A.; Alnuami, M.; Althobity, A.; Almardawi, A.; Bedaiwi, K. Predictors of phosphodiesterase Type 5 inhibitor treatment failure in patients diagnosed with erectile dysfunction. Cureus 2023, 15, e50515. [Google Scholar] [CrossRef]
- Kim, S.C.; Lee, Y.S.; Seo, K.K.; Jung, G.W.; Kim, T.H. Reasons and predictive factors for discontinuation of PDE-5 inhibitors despite successful intercourse in erectile dysfunction patients. Int. J. Impot. Res. 2014, 26, 87–93. [Google Scholar] [CrossRef]
- Bivalacqua, T.J.; Usta, M.F.; Champion, H.C.; Kadowitz, P.J.; Hellstrom, W.J. Endothelial dysfunction in erectile dysfunction: Role of the endothelium in erectile physiology and disease. J. Androl. 2003, 24 (Suppl. S6), S17–S37. [Google Scholar] [CrossRef]
- Al-Shaiji, T.F. Breaking the ice of erectile dysfunction taboo: A focus on clinician-patient communication. J. Patient Exp. 2022, 9, 1–5. [Google Scholar] [CrossRef]
- Sansone, A.; Guida, E.; Dolci, S.; Frangione, V.; Asso, A.; Bellia, G.; Jannini, E.A. Future perspectives for PDE5 inhibitors bridging the gap between cardiovascular health and psychological status. Basic Clin. Androl. 2025, 35, 3. [Google Scholar] [CrossRef]
- Azadzoi, K.M.; Yang, J.; Siroky, M.B. Neural regulation of sexual function in men. World J. Clin. Urol. 2013, 2, 32–41. [Google Scholar] [CrossRef]
- Rizk, P.J.; Kohn, T.P.; Pastuszak, A.W.; Khera, M. Testosterone therapy improves erectile function and libido in hypogonadal men. Curr. Opin. Urol. 2017, 27, 511–515. [Google Scholar] [CrossRef]
- Allen, M.S.; Wood, A.M.; Sheffield, D. The psychology of erectile dysfunction. Curr. Dir. Psychol. Sci. 2023, 32, 487–493. [Google Scholar] [CrossRef]
- Çayan, S.; Kendirci, M.; Yaman, Ö.; Aşçı, R.; Orhan, İ.; Usta, M.F.; Ekmekçioğlu, O.; Kadıoğlu, A. Prevalence of erectile dysfunction in men over 40 years of age in Turkey: Results from the Turkish Society of Andrology Male Sexual Health Study Group. Turk. J. Urol. 2017, 43, 122–129. [Google Scholar] [CrossRef]
- Ferrini, M.G.; Gonzalez-Cadavid, N.F.; Rajfer, J. Aging related erectile dysfunction-potential mechanism to halt or delay its onset. Transl. Androl. Urol. 2017, 6, 20–27. [Google Scholar] [CrossRef]
- Pellegrino, F.; Sjoberg, D.D.; Tin, A.L.; Benfante, N.E.; Briganti, A.; Montorsi, F.; Eastham, J.A.; Mulhall, J.P.; Vickers, A.J. Relationship Between Age, Comorbidity, and the Prevalence of Erectile Dysfunction. Eur. Urol. Focus 2023, 9, 162–167. [Google Scholar] [CrossRef]
- Ghalayini, I.F.; Al-Ghazo, M.A.; Al-Azab, R.; Bani-Hani, I.; Matani, Y.S.; Barham, A.E.; Harfeil, M.N.; Haddad, Y. Erectile dysfunction in a Mediterranean country: Results of an epidemiological survey of a representative sample of men. Int. J. Impot. Res. 2010, 22, 196–203. [Google Scholar] [CrossRef]
- Bogari, M.; Alzahrani, B.A.; Aghashami, A.S.; Alsubeay, A.M.S.; Hassan, F.; Ahmed, M.E.; Almuqati, M.M. Male Sexual Dysfunction-Related Medical Comorbidities in a Tertiary Care Center, Western Region, Saudi Arabia. Cureus 2023, 15, e41732. [Google Scholar] [CrossRef]
- El Bizri, L.; Jarrar, L.G.; Ali, W.K.A.; Omar, A.H. The role of community pharmacists in increasing access and use of self-care interventions for sexual and reproductive health in the Eastern Mediterranean Region: Examples from Egypt, Jordan, Lebanon and Somalia. Health Res. Policy Syst. 2021, 19 (Suppl. S1), 49. [Google Scholar] [CrossRef]
- Moreira, E.D.; Glasser, D.B.; Nicolosi, A.; Duarte, F.G.; Gingell, C.; GSSAB Investigators’ Group. Sexual problems and help-seeking behaviour in adults in the United Kingdom and continental Europe. BJU Int. 2008, 101, 1005–1011. [Google Scholar] [CrossRef]
- Buvat, J.; Glasser, D.; Neves, R.C.; Duarte, F.G.; Gingell, C.; Moreira, E.D., Jr.; Global Study of Sexual Attitudes and Behaviours (GSSAB) Investigators’ Group. Sexual problems and associated help-seeking behavior patterns: Results of a population-based survey in France. Int. J. Urol. 2009, 16, 632–638. [Google Scholar] [CrossRef]
- Zhang, K.; Yu, W.; He, Z.J.; Jin, J. Help-seeking behavior for erectile dysfunction: A clinic-based survey in China. Asian J. Androl. 2014, 16, 131–135. [Google Scholar] [CrossRef]
- Zarski, A.C.; Velten, J.; Knauer, J.; Berking, M.; Ebert, D.D. Internet- and mobile-based psychological interventions for sexual dysfunctions: A systematic review and meta-analysis. NPJ Digit. Med. 2022, 5, 139. [Google Scholar] [CrossRef]
- Alzahrani, M.A.; Khan, M.A.; Hakami, B.O.; Alahmadi, A.; Alzahrani, M.; Alsaleh, F.; Almurayyi, M.; Safar, O.; Ahmad, M.S. Is Arabic Information on YouTube About Erectile Dysfunction Based on Scientific Evidence? Res. Rep. Urol. 2023, 15, 261–272. [Google Scholar] [CrossRef]
- Saffati, G.; Seyan, Z.; Rendon, D.O.; Almuhaideb, M.; Hinojosa-Gonzalez, D.E.; Kronstedt, S.; Khera, M. Erectile dysfunction as a holistic indicator of well-being: A narrative review. Sex. Med. Rev. 2025, 13, 11–19. [Google Scholar] [CrossRef]
- El Ansari, W.; El-Ansari, K.; Arafa, M. Breaking the silence—Systematic review of the socio-cultural underpinnings of men’s sexual and reproductive health in Middle East and North Africa (MENA): A handful of taboos? Arab. J. Urol. 2024, 23, 16–32. [Google Scholar] [CrossRef]
- Alluhaibi, B.A.; Awadalla, A.W. Attitudes and stigma toward seeking psychological help among Saudi Adults. BMC Psychol. 2022, 10, 216. [Google Scholar] [CrossRef]
- Almigbal, T.H.; Schattner, P. The willingness of Saudi men with type 2 diabetes to discuss erectile dysfunction with their physicians and the factors that influence this. PLoS ONE 2018, 13, e0201105. [Google Scholar] [CrossRef] [PubMed]
- Brotto, L.A.; Atallah, S.; Carvalho, J.; Gordon, E.; Pascoal, P.M.; Reda, M.; Stephenson, K.R.; Tavares, I.M. Psychological and interpersonal dimensions of sexual function and dysfunction: Recommendations from the fifth international consultation on sexual medicine (ICSM 2024). Sex. Med. Rev. 2024, 13, 118–143. [Google Scholar] [CrossRef] [PubMed]
- Atallah, S.; Haydar, A.; Jabbour, T.; Kfoury, P.; Sader, G. The effectiveness of psychological interventions alone, or in combination with phosphodiesterase-5 inhibitors, for the treatment of erectile dysfunction: A systematic review. Arab. J. Urol. 2021, 19, 310–322. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Parameter | n | Percentage (%) | |
|---|---|---|---|
| Age group (Mean ± SD = 39 ± 8.5) | ≤34 | 109 | 28.4 |
| 35–45 | 105 | 27.3 | |
| 45–55 | 90 | 23.4 | |
| >55 | 80 | 20.8 | |
| Number of children (Mean ± SD = 3 ± 2) | 0 | 29 | 7.6 |
| 1 | 50 | 13.0 | |
| 2 | 92 | 24.0 | |
| 3 | 82 | 21.4 | |
| 4 | 69 | 18.0 | |
| >4 | 62 | 16.1 | |
| Number of wives | 1 | 287 | 74.7 |
| 2 | 74 | 19.3 | |
| 3 | 20 | 5.2 | |
| 4 | 3 | 0.8 | |
| Education level | No formal education | 18 | 4.7 |
| Primary | 22 | 5.7 | |
| Intermediate | 59 | 15.4 | |
| Secondary | 129 | 33.6 | |
| University | 156 | 40.6 | |
| Chronic diseases | Hypertension | 74 | 19.3 |
| Diabetes mellitus | 119 | 31.0 | |
| Hypercholesterolemia | 54 | 14.1 | |
| Cardiovascular disease (e.g., stroke, angina) | 23 | 6.0 | |
| Kidney failure | 5 | 1.3 | |
| Mental illness | 4 | 1.0 | |
| Neurological disorders | 3 | 0.7 | |
| None | 108 | 28.2 | |
| Weight (kg) (Mean ± SD = 86.2 ± 15.7) | ≤70 | 74 | 19.3 |
| 71–85 | 123 | 32.0 | |
| 86–100 | 97 | 25.3 | |
| >100 | 90 | 23.4 | |
| Height (cm) (Mean ± SD = 164.3 ± 8.9) | ≤155 | 73 | 19.0 |
| 156–165 | 146 | 38.0 | |
| 166–175 | 107 | 27.9 | |
| >175 | 58 | 15.1 | |
| Exercise frequency (per week) | None | 139 | 36.2 |
| Once | 102 | 26.6 | |
| 2–3 times | 78 | 20.3 | |
| 4–5 times | 38 | 9.9 | |
| ≥6 times | 27 | 7.0 | |
| Smoking status | Cigarette smoker | 89 | 23.2 |
| Hookah smoker | 148 | 38.5 | |
| Electronic cigarette user | 61 | 15.9 | |
| Non-smoker | 86 | 22.4 | |
| Parameter | n | Percentage (%) | |
|---|---|---|---|
| Frequency of achieving an erection during sexual activity | No sexual activity | 4 | 1.0 |
| Almost always or always | 116 | 30.2 | |
| Very often (much more than half the time) | 129 | 33.6 | |
| Sometimes (about half the time) | 88 | 22.9 | |
| Infrequently (much less than half the time) | 39 | 10.2 | |
| Almost never or never | 8 | 2.1 | |
| Frequency of having an erection strong enough for vaginal penetration | No sexual arousal | 5 | 1.3 |
| Almost always or always | 124 | 32.3 | |
| Very often (much more than half the time) | 110 | 28.6 | |
| Sometimes (about half the time) | 98 | 25.5 | |
| Rarely (much less than half the time) | 35 | 9.1 | |
| Almost never or never | 12 | 3.1 | |
| Frequency of successful penetration during intercourse | I have never attempted intercourse | 4 | 1.0 |
| Almost always or always | 118 | 30.7 | |
| Often (much more than half the time) | 118 | 30.7 | |
| Sometimes (about half the time) | 93 | 24.2 | |
| Rarely (much less than half the time) | 42 | 10.9 | |
| Almost never or never | 9 | 2.3 | |
| Frequency of maintaining an erection after penetration | I have never attempted intercourse | 4 | 1.0 |
| Almost always or always | 124 | 32.3 | |
| Often (much more than half the time) | 108 | 28.1 | |
| Sometimes (about half the time) | 94 | 24.5 | |
| Rarely (much less than half the time) | 40 | 10.4 | |
| Almost never or never | 14 | 3.6 | |
| Difficulty in maintaining an erection to complete intercourse | I have never attempted intercourse | 4 | 1.0 |
| Very difficult | 2 | 0.5 | |
| Difficult | 54 | 14.1 | |
| Somewhat difficult | 120 | 31.3 | |
| Mild difficulty | 127 | 33.1 | |
| No difficulty | 77 | 20.1 | |
| Confidence in achieving and maintaining an erection | Very high | 45 | 11.7 |
| High | 126 | 32.8 | |
| Medium | 115 | 29.9 | |
| Low | 82 | 21.4 | |
| Very low | 16 | 4.2 | |
| Parameter | n | Percentage (%) | |
|---|---|---|---|
| Sources of information about ED (Multiple responses allowed) (n = 176) # | Friends | 36 | 20.4 |
| Wife | 54 | 30.7 | |
| Doctor | 54 | 30.7 | |
| Pharmacist | 28 | 15.9 | |
| Social media | 42 | 23.9 | |
| Perceived need for ED treatment | Yes | 190 | 49.5 |
| No | 194 | 50.5 | |
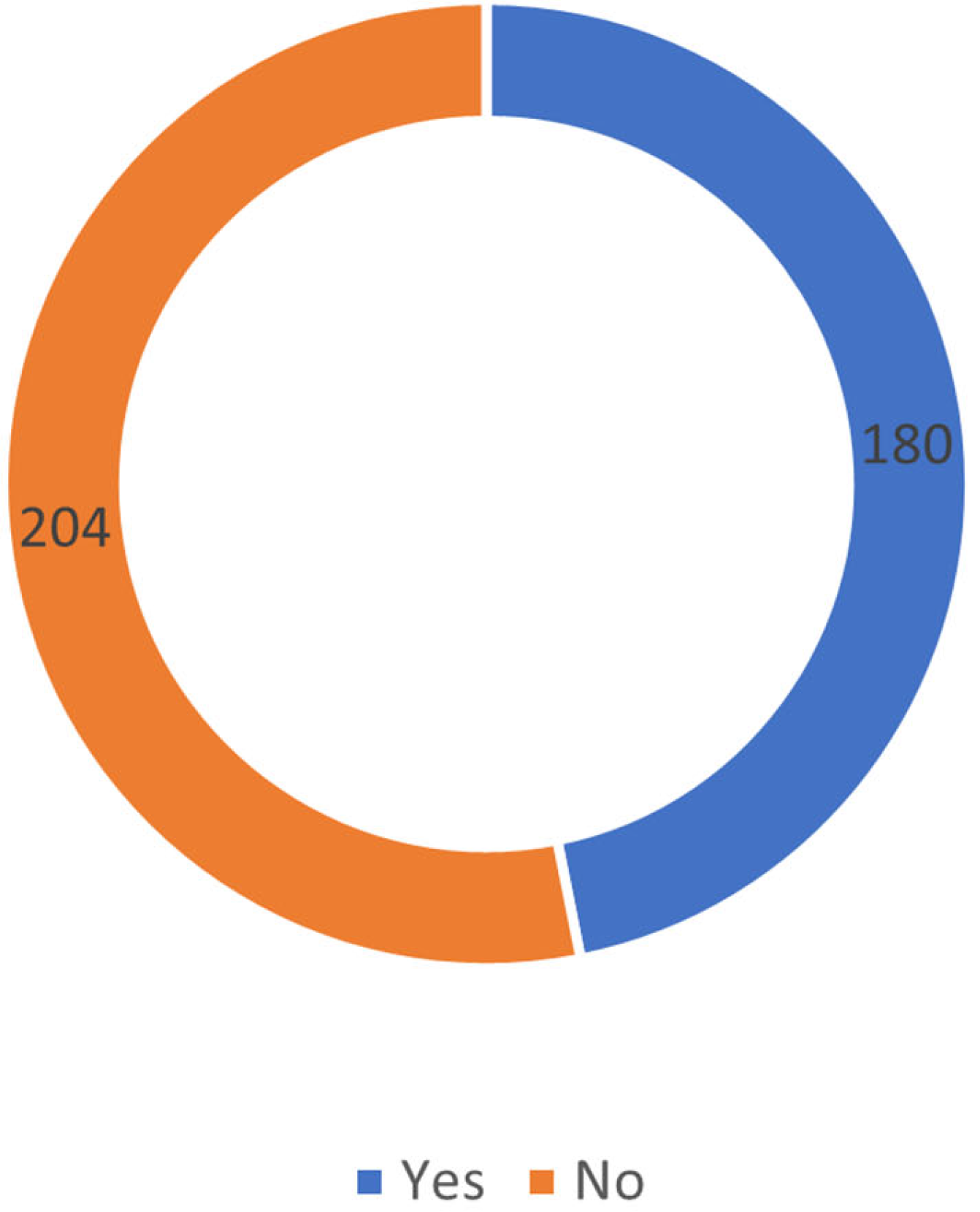
| Consultation at male clinics for ED | Yes | 180 | 46.9 |
| No | 204 | 53.1 | |
| Reasons for not seeking medical consultation (Multiple responses allowed) (n = 235) | ED is not a serious condition | 30 | 12.8 |
| Reluctant to discuss ED due to social embarrassment | 70 | 29.8 | |
| Not interested in sexual intercourse | 100 | 26.0 | |
| Concerned about the harmful effects of medications | 61 | 26.0 | |
| Satisfied with self-medication | 73 | 31.0 | |
| Medications are available without a prescription | 40 | 17.0 | |
| Use of medication for ED | Yes | 181 | 47.1 |
| No | 203 | 52.9 | |
| Preferred treatment modality (Multiple responses allowed) (n = 187) | Medical treatment | 70 | 37.4 |
| Alternative treatments | 64 | 34.3 | |
| Self-treatment | 53 | 28.3 | |
| Sources of treatment information (n = 186) (Multiple responses allowed) * | Friends | 32 | 17.2 |
| Wife | 39 | 21.0 | |
| Doctor | 52 | 28.0 | |
| Pharmacist | 45 | 24.2 | |
| Social media | 29 | 15.6 | |
| Perceived effectiveness of ED treatment (n = 191) | No improvement | 29 | 15.2 |
| Slight improvement | 46 | 24.1 | |
| Uncertain | 57 | 29.8 | |
| Moderate improvement | 35 | 18.3 | |
| Significant improvement | 24 | 12.5 | |
| Perceptions of sexual enhancers (Viagra, Snafi) | Safe | 114 | 29.7 |
| Unsafe | 158 | 41.1 | |
| Uncertain | 112 | 29.2 | |
| Reasons for considering sexual enhancers unsafe (Multiple responses allowed) (n = 268) * | Risk of addiction or dependence | 69 | 25.7 |
| Serious side effects | 79 | 29.5 | |
| Potential cardiovascular risks | 74 | 27.6 | |
| Uncertain | 69 | 25.7 | |
| Parameters | Have You Ever Taken Medication for Erectile Dysfunction? | Total (N = 384) | p Value * | ||
|---|---|---|---|---|---|
| Yes | No | ||||
| Age group (years) | ≤34 | 42 | 67 | 109 | 0.019 |
| 23.2% | 33.0% | 28.4% | |||
| 34–45 | 45 | 60 | 105 | ||
| 24.9% | 29.6% | 27.3% | |||
| 45 to 55 | 46 | 44 | 90 | ||
| 25.4% | 21.7% | 23.4% | |||
| >55 | 48 | 32 | 80 | ||
| 26.5% | 15.8% | 20.8% | |||
| Number of children | 0 | 10 | 19 | 29 | 0.081 |
| 5.5% | 9.4% | 7.6% | |||
| 1 | 21 | 29 | 50 | ||
| 11.6% | 14.3% | 13.0% | |||
| 2 | 40 | 52 | 92 | ||
| 22.1% | 25.6% | 24.0% | |||
| 3 | 36 | 46 | 82 | ||
| 19.9% | 22.7% | 21.4% | |||
| 4 | 43 | 26 | 69 | ||
| 23.8% | 12.8% | 18.0% | |||
| >4 | 31 | 31 | 62 | ||
| 17.1% | 15.3% | 16.1% | |||
| Number of wives | 1 | 129 | 158 | 287 | 0.282 |
| 71.3% | 77.8% | 74.7% | |||
| 2 | 37 | 37 | 74 | ||
| 20.4% | 18.2% | 19.3% | |||
| 3 | 13 | 7 | 20 | ||
| 7.2% | 3.4% | 5.2% | |||
| 4 | 2 | 1 | 3 | ||
| 1.1% | 0.5% | 0.8% | |||
| Educational level | No formal education | 10 | 8 | 18 | 0.127 |
| 5.5% | 3.9% | 4.7% | |||
| Primary | 13 | 9 | 22 | ||
| 7.2% | 4.4% | 5.7% | |||
| Intermediate | 33 | 26 | 59 | ||
| 18.2% | 12.8% | 15.4% | |||
| Secondary | 63 | 66 | 129 | ||
| 34.8% | 32.5% | 33.6% | |||
| University | 62 | 94 | 156 | ||
| 34.3% | 46.3% | 40.6% | |||
| Diabetes or hypertension | No | 84 | 110 | 194 | 0.128 |
| 46.4% | 54.2% | 50.5% | |||
| Yes | 97 | 93 | 190 | ||
| 53.6% | 45.8% | 49.5% | |||
| Smoking status | Cigarette smoker | 39 | 50 | 89 | 0.865 |
| 21.5% | 24.6% | 23.2% | |||
| Hookah smoker | 70 | 78 | 148 | ||
| 38.7% | 38.4% | 38.5% | |||
| Electronic cigarette user | 31 | 30 | 61 | ||
| 17.1% | 14.8% | 15.9% | |||
| Non-smoker | 41 | 45 | 86 | ||
| 22.7% | 22.2% | 22.4% | |||
| Parameters | Have You Consulted Male Clinics Regarding Erectile Dysfunction? | Total (N = 384) | p Value * | ||
|---|---|---|---|---|---|
| Yes | No | ||||
| Age | ≤34 | 54 | 55 | 109 | 0.235 |
| 30.0% | 27.0% | 28.4% | |||
| 34–45 | 44 | 61 | 105 | ||
| 24.4% | 29.9% | 27.3% | |||
| 45–55 | 38 | 52 | 90 | ||
| 21.1% | 25.5% | 23.4% | |||
| >55 | 44 | 36 | 80 | ||
| 24.4% | 17.6% | 20.8% | |||
| Number of children | 0 | 13 | 16 | 29 | 0.394 |
| 7.2% | 7.8% | 7.6% | |||
| 1 | 23 | 27 | 50 | ||
| 12.8% | 13.2% | 13.0% | |||
| 2 | 35 | 57 | 92 | ||
| 19.4% | 27.9% | 24.0% | |||
| 3 | 41 | 41 | 82 | ||
| 22.8% | 20.1% | 21.4% | |||
| 4 | 38 | 31 | 69 | ||
| 21.1% | 15.2% | 18.0% | |||
| >4 | 30 | 32 | 62 | ||
| 16.7% | 15.7% | 16.1% | |||
| Number of wives | 1 | 135 | 152 | 287 | 0.198 |
| 75.0% | 74.5% | 74.7% | |||
| 2 | 31 | 43 | 74 | ||
| 17.2% | 21.1% | 19.3% | |||
| 3 | 11 | 9 | 20 | ||
| 6.1% | 4.4% | 5.2% | |||
| 4 | 3 | 0 | 3 | ||
| 1.7% | 0.0% | 0.8% | |||
| Educational level | Uneducated | 13 | 5 | 18 | 0.270 |
| 7.2% | 2.5% | 4.7% | |||
| Primary | 11 | 11 | 22 | ||
| 6.1% | 5.4% | 5.7% | |||
| Intermediate | 26 | 33 | 59 | ||
| 14.4% | 16.2% | 15.4% | |||
| Secondary | 60 | 69 | 129 | ||
| 33.3% | 33.8% | 33.6% | |||
| University | 70 | 86 | 156 | ||
| 38.9% | 42.2% | 40.6% | |||
| Diabetes or hypertension | No | 86 | 108 | 194 | 0.313 |
| 47.8% | 52.9% | 50.5% | |||
| Yes | 94 | 96 | 190 | ||
| 52.2% | 47.1% | 49.5% | |||
| Smoking status | Cigarette smoker | 38 | 51 | 89 | 0.554 |
| 21.1% | 25.0% | 23.2% | |||
| Hookah smoker | 76 | 72 | 148 | ||
| 42.2% | 35.3% | 38.5% | |||
| Electronic cigarette user | 28 | 33 | 61 | ||
| 15.6% | 16.2% | 15.9% | |||
| Non-smoker | 38 | 48 | 86 | ||
| 21.1% | 23.5% | 22.4% | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alnazari, M.; Abdullah, S.; Aljohani, A.K.; Rajih, E.S.; Alghamdi, G.S.; Sebaa, F.S.; Alraddadi, A.A.; Khan, W.; Moalwi, A. Prevalence of Erectile Dysfunction and Help-Seeking Behavior Among Patients Attending Primary Healthcare Centers for Non-Urological Complaints. Healthcare 2025, 13, 1088. https://doi.org/10.3390/healthcare13091088
Alnazari M, Abdullah S, Aljohani AK, Rajih ES, Alghamdi GS, Sebaa FS, Alraddadi AA, Khan W, Moalwi A. Prevalence of Erectile Dysfunction and Help-Seeking Behavior Among Patients Attending Primary Healthcare Centers for Non-Urological Complaints. Healthcare. 2025; 13(9):1088. https://doi.org/10.3390/healthcare13091088
Chicago/Turabian StyleAlnazari, Mansour, Sulaiman Abdullah, Abdullah K. Aljohani, Emad S. Rajih, Ghadi S. Alghamdi, Faris S. Sebaa, Ali A. Alraddadi, Wesam Khan, and Adel Moalwi. 2025. "Prevalence of Erectile Dysfunction and Help-Seeking Behavior Among Patients Attending Primary Healthcare Centers for Non-Urological Complaints" Healthcare 13, no. 9: 1088. https://doi.org/10.3390/healthcare13091088
APA StyleAlnazari, M., Abdullah, S., Aljohani, A. K., Rajih, E. S., Alghamdi, G. S., Sebaa, F. S., Alraddadi, A. A., Khan, W., & Moalwi, A. (2025). Prevalence of Erectile Dysfunction and Help-Seeking Behavior Among Patients Attending Primary Healthcare Centers for Non-Urological Complaints. Healthcare, 13(9), 1088. https://doi.org/10.3390/healthcare13091088