
Exploring the Holistic Needs of People Living with Cancer in Care Homes: An Integrative Review

 , , , , , , , , and
, , , , , , , , and 
Abstract
:1. Introduction
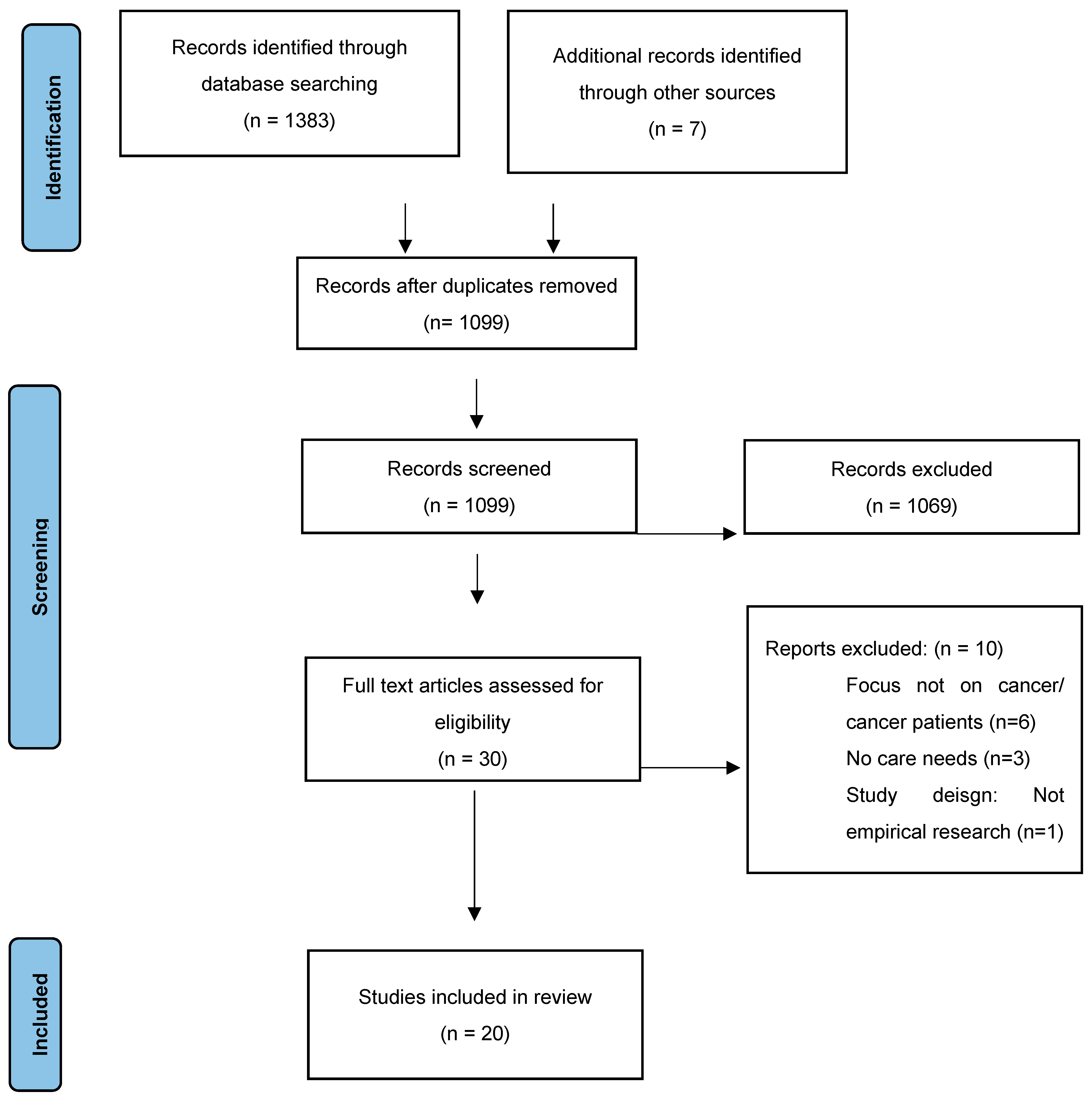
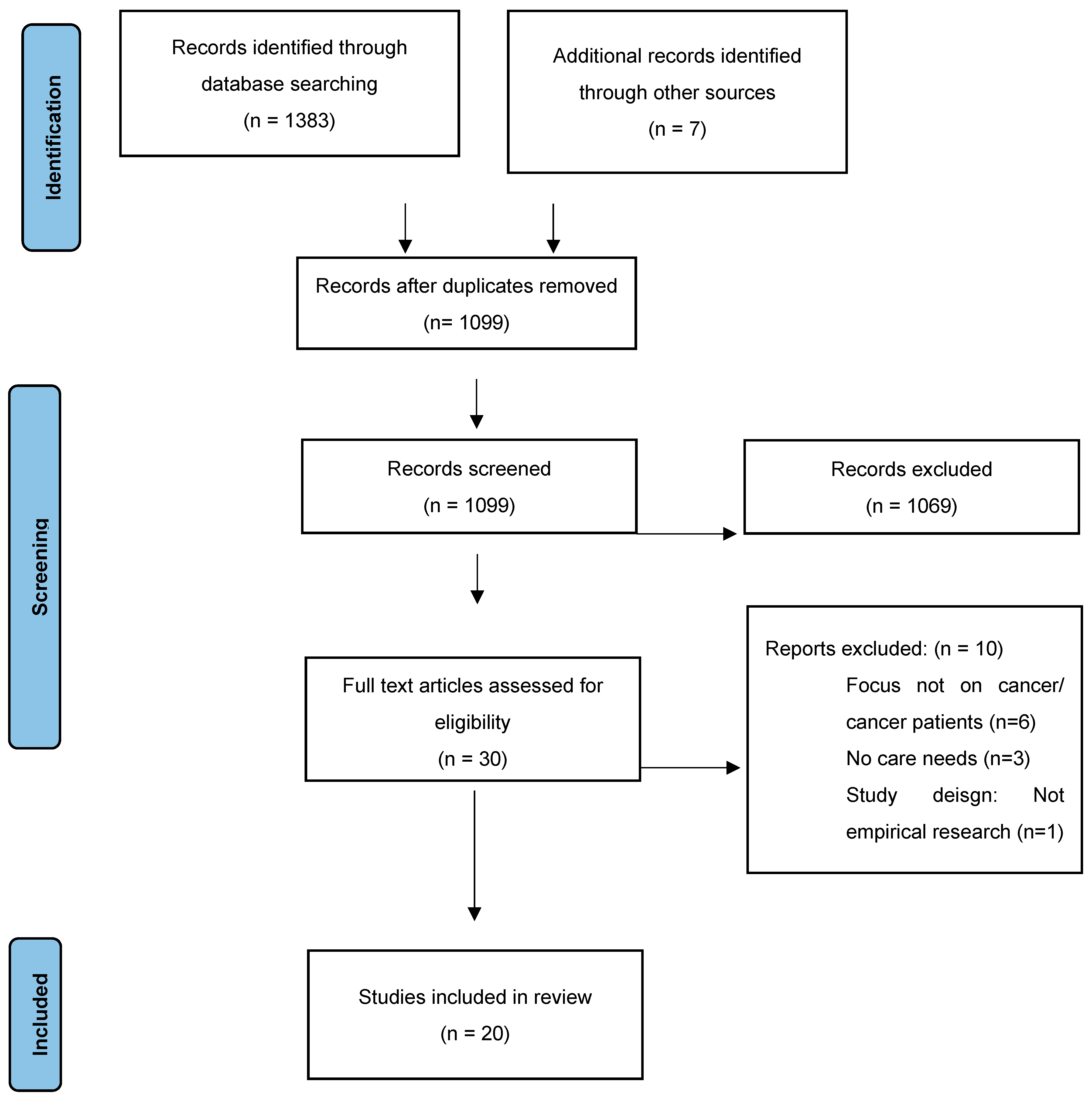
2. Materials and Methods
2.1. Search Method
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Quality Appraisal
2.4. Data Analysis
3. Results
3.1. Characteristics of Included Studies
3.2. Methodological Rigor
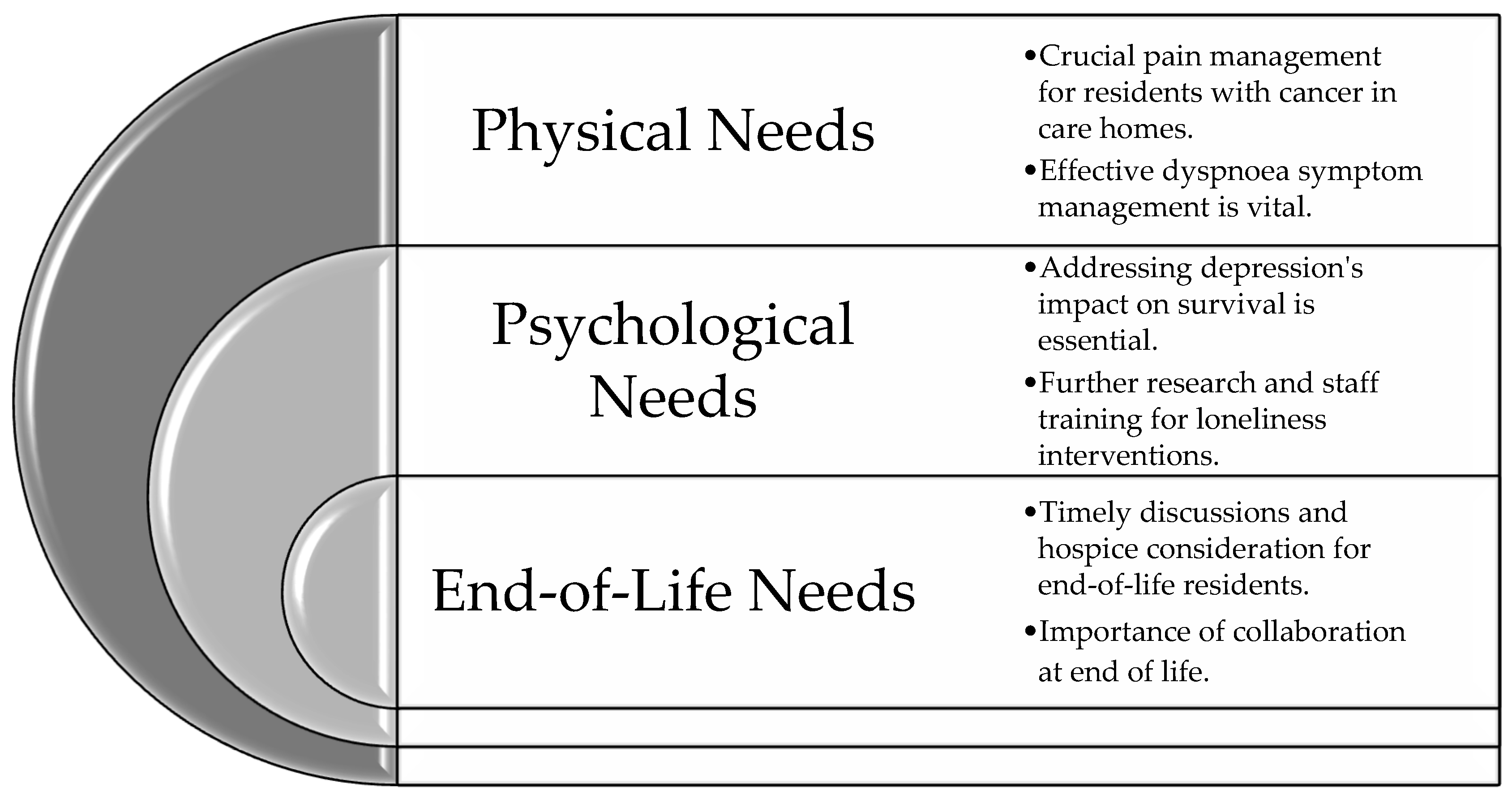
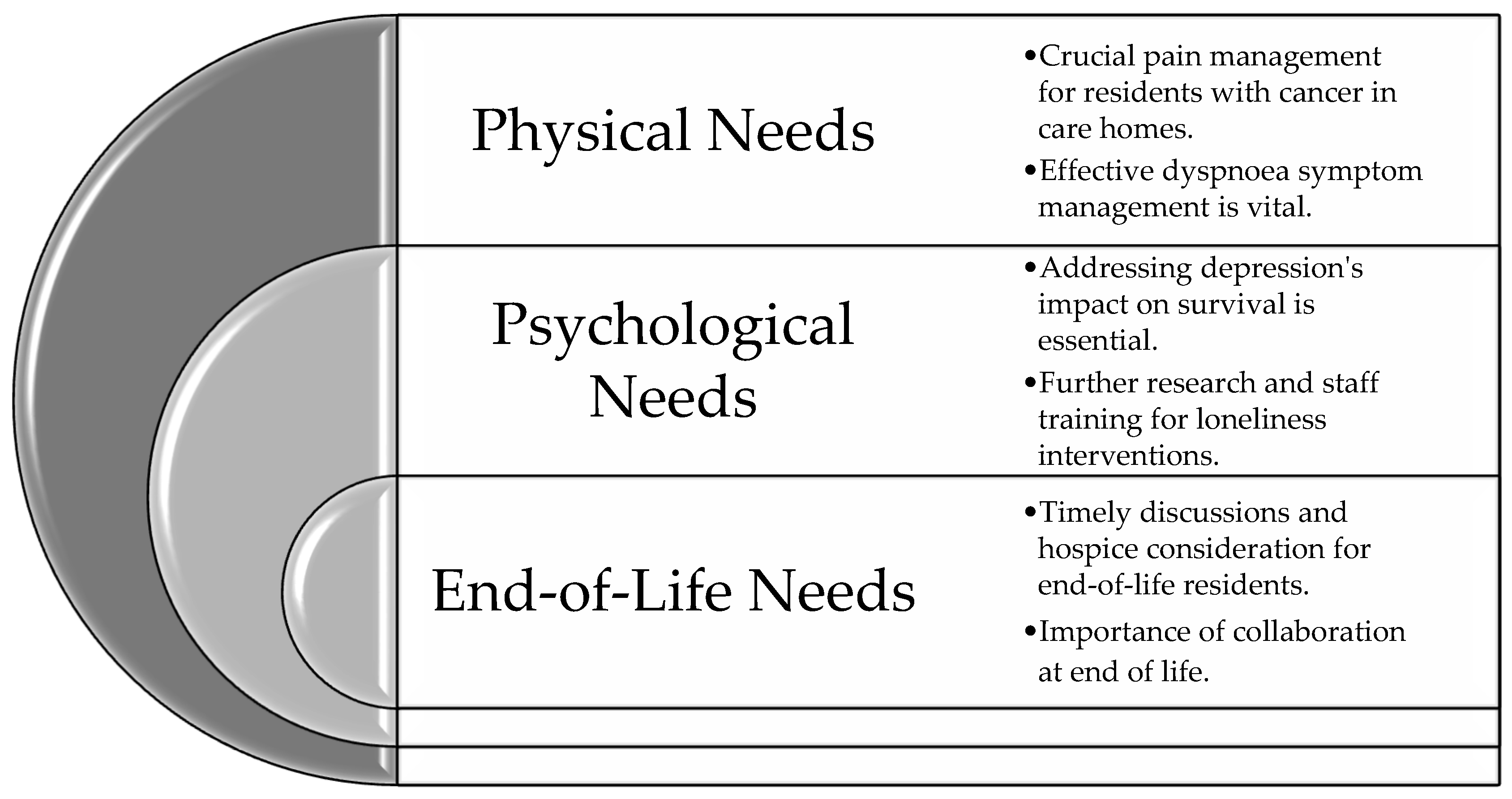
3.3. Synthesis of Evidence
3.3.1. Theme 1: Physical Needs
3.3.2. Theme 2: Psychological Needs
3.3.3. Theme 3: End-of-Life Needs
4. Discussion
4.1. Implications for Practice
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). WHO Cancer; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- Cooper, G.M. The Development and Causes of Cancer. In The Cell: A Molecular Approach, 2nd ed.; Sinauer Associates: Sunderland, MA, USA, 2000. Available online: https://www.ncbi.nlm.nih.gov/books/NBK9963/ (accessed on 1 December 2023).
- National Cancer Institute (NCI). Age and Cancer Risk. 2021. Available online: https://www.cancer.gov/about-cancer/causes-prevention/risk/age#:~:text=Age%20and%20Cancer%20Risk,-Advancing%20age%20is&text=The%20incidence%20rates%20for%20cancer,groups%2060%20years%20and%20older (accessed on 24 April 2023).
- Cancer Research UK. Age and Cancer. 2021. Available online: https://www.cancerresearchuk.org/about-cancer/causes-of-cancer/age-and-cancer (accessed on 24 April 2023).
- Department of Health and Social Care. The Health and Social Care Act 2008 (Regulated Activities) Regulations 2014; Department of Health and Social Care: London, UK, 2014. [Google Scholar]
- Rand, S.; Smith, N.; Jones, K.; Dargan, A.; Hogan, H. Measuring safety in older adult care homes: A scoping review of the international literature. BMJ Open 2021, 11, e043206. [Google Scholar] [CrossRef] [PubMed]
- Department of Health United Kingdom. Care Standards Act 2000; Department of Health United Kingdom: London, UK, 2000. [Google Scholar]
- Spilsbury, K.; Hanratty, B.; McCaughan, D. Supporting Nursing in Care Homes; University of York: York, UK, 2015. [Google Scholar]
- Villani, E.R.; Fusco, D.; Franza, L.; Onder, G.; Bernabei, R.; Colloca, G.F. Characteristics of patients with cancer in European long-term care facilities. Aging Clin. Exp. Res. 2022, 34, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Kittelson, S.M.; Elie, M.C.; Pennypacker, L. Palliative Care Symptom Management. Crit. Care Nurs. Clin. N. Am. 2015, 27, 315–339. [Google Scholar] [CrossRef]
- Vermylen, J.H.; Szmuilowicz, E.; Kalhan, R. Palliative care in COPD: An unmet area for quality improvement. Int. J. Chronic Obstr. Pulm. Dis. 2015, 10, 1543–1551. [Google Scholar] [CrossRef] [PubMed]
- Crooms, R.C.; Gelfman, L.P. Palliative Care and End-of-Life Considerations for the Frail Patient. Anesth. Analg. 2020, 130, 1504–1515. [Google Scholar] [CrossRef] [PubMed]
- Antonione, R.; Fieramosca, M.; Moroni, M.; Nodari, S.; Valle, A. Overview and symptom management in heart failure patients eligible for palliative care. G. Ital. Cardiol. 2020, 21, 629–638. [Google Scholar]
- Senderovich, H.; Jimenez Lopez, B. Integration of palliative care in Parkinson’s disease management. Curr. Med. Res. Opin. 2021, 37, 1745–1759. [Google Scholar] [CrossRef]
- Ng, Z.X.; Ong, M.S.; Jegadeesan, T.; Deng, S.; Yap, C.T. Breast Cancer: Exploring the Facts and Holistic Needs during and beyond Treatment. Healthcare 2017, 5, 26. [Google Scholar] [CrossRef]
- Whittemore, R.; Knafl, K. The integrative review: Updated methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef]
- Joanna Briggs Institute (JBI). Critical Appraisal Tools. 2022. Available online: https://jbi.global/critical-appraisal-tools (accessed on 1 December 2023).
- Popay, J.; Roberts, H.; Sowden, A.; Petticrew, M.; Arai, L.; Rodgers, M.; Britten, N.; Roen, K.; Duffy, S. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews: A Product from the ESRC Methods Programme. 2006. Available online: https://www.lancaster.ac.uk/media/lancaster-university/content-assets/documents/fhm/dhr/chir/NSsynthesisguidanceVersion1-April2006.pdf (accessed on 1 December 2023).
- Boyd, M.; Frey, R.; Balmer, D.; Robinson, J.; McLeod, H.; Foster, S.; Slark, J.; Gott, M. End of life care for long-term care residents with dementia, chronic illness and cancer: Prospective staff survey. BMC Geriatr. 2019, 19, 137. [Google Scholar] [CrossRef]
- Drageset, J.; Eide, G.E.; Harrington, C.; Ranhoff, A.H. Acute hospital admission for nursing home residents without cognitive impairment with a diagnosis of cancer. Eur. J. Cancer Care 2015, 24, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Drageset, J.; Eide, G.E.; Ranhoff, A.H. Anxiety and Depression and Mortality among Cognitively Intact Nursing Home Residents with and without a Cancer Diagnosis. Cancer Nurs. 2013, 36, E68–E74. [Google Scholar] [CrossRef]
- Drageset, J.; Eide, G.E.; Kirkevold, M.; Ranhoff, A.H. Emotional loneliness is associated with mortality among mentally intact nursing home residents with and without cancer: A five-year follow-up study. J. Clin. Nurs. 2013, 22, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Drageset, J.; Eide, G.E.; Dysvik, E.; Furnes, B.; Hauge, S. Loneliness, loss, and social support among cognitively intact older people with cancer, living in nursing homes—A mixed-methods study. Clin. Interv. Aging 2015, 10, 1529–1536. [Google Scholar] [CrossRef] [PubMed]
- Drageset, J.; Eide, G.E.; Hauge, S. Symptoms of depression, sadness and sense of coherence (coping) among cognitively intact older people with cancer living in nursing homes—A mixed-methods study. PeerJ 2016, 4, e2096. [Google Scholar] [CrossRef] [PubMed]
- Drageset, J.; Eide, G.E.; Corbett, A. Health-related quality of life among cognitively intact nursing home residents with and without cancer—A 6-year longitudinal study. Patient Relat. Outcome Meas. 2017, 8, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Drageset, J.; Eide, G.E. Loneliness Among Cognitively Intact Residents of Nursing Homes with and without Cancer: A 6-Year Longitudinal Study. SAGE Open Nurs. 2020, 6, 2377960820907778. [Google Scholar] [CrossRef]
- Dubé, C.E.; Mack, D.S.; Hunnicutt, J.N.; Lapane, K.L. Cognitive Impairment and Pain among Nursing Home Residents with Cancer. J. Pain Symptom Manag. 2018, 55, 1509–1518. [Google Scholar] [CrossRef]
- Hunnicutt, J.N.; Tjia, J.; Lapane, K.L. Hospice Use and Pain Management in Elderly Nursing Home Residents with Cancer. J. Pain Symptom Manag. 2017, 53, 561–570. [Google Scholar] [CrossRef]
- Lage, D.E.; DuMontier, C.; Lee, Y.; Nipp, R.D.; Mitchell, S.L.; Temel, J.S.; El-Jawahri, A.; Berry, S.D. Potentially burdensome end-of-life transitions among nursing home residents with poor-prognosis cancer. Cancer 2020, 126, 1322–1329. [Google Scholar] [CrossRef]
- Monroe, T.B.; Carter, M.A.; Feldt, K.S.; Dietrich, M.S.; Cowan, R.L. Pain and hospice care in nursing home residents with dementia and terminal cancer. Geriatr. Gerontol. Int. 2013, 13, 1018–1025. [Google Scholar] [CrossRef] [PubMed]
- Pimentel, C.B.; Briesacher, B.A.; Gurwitz, J.H.; Rosen, A.B.; Pimentel, M.T.; Lapane, K.L. Pain Management in Nursing Home Residents with Cancer. J. Am. Geriatr. Soc. 2015, 63, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Bainbridge, D.; Hsien, S.; Sussman, J.; Pond, G. Factors associated with acute care use among nursing home residents dying of cancer: A population-based study. Int. J. Palliat. Nurs. 2015, 21, 349356. [Google Scholar] [CrossRef] [PubMed]
- Mack, D.S.; Hunnicutt, J.N.; Jesdale, B.M.; Lapane, K.L. Non-Hispanic Black-White disparities in pain and pain management among newly admitted nursing home residents with cancer. J. Pain Res. 2018, 11, 753–761. [Google Scholar] [CrossRef] [PubMed]
- Blytt, K.M.; Selbæk, G.; Drageset, J.; Natvig, G.K.; Husebo, B.S. Comorbid Dementia and Cancer in Residents of Nursing Homes: Secondary Analyses of a Cross-Sectional Study. Cancer Nurs. 2018, 41, E13–E20. [Google Scholar] [CrossRef] [PubMed]
- Monroe, T.; Carter, M.; Feldt, K.; Tolley, B.; Cowan, R.L. Assessing advanced cancer pain in older adults with dementia at the end-of-life. J. Adv. Nurs. 2012, 68, 2070–2078. [Google Scholar] [CrossRef] [PubMed]
- Finlayson, E.; Zhao, S.; Boscardin, W.J.; Fries, B.E.; Landefeld, C.S.; Dudley, R.A. Functional Status after Colon Cancer Surgery in Elderly Nursing Home Residents. J. Am. Geriatr. Soc. 2012, 60, 967–973. [Google Scholar] [CrossRef]
- Drageset, J.; Eide, G.E.; Ranhoff, A.H. Cancer in nursing homes: Characteristics and health-related quality of life among cognitively intact residents with and without cancer. Cancer Nurs. 2012, 35, 295–301. [Google Scholar] [CrossRef]
- Parast, L.; Tolpadi, A.A.; Teno, J.M.; Elliott, M.N.; Price, R.A. Hospice Care Experiences Among Cancer Patients and Their Caregivers. J. Gen. Intern. Med. 2021, 36, 961–969. [Google Scholar] [CrossRef]
- Barnett-Page, E.; Thomas, J. Methods for the synthesis of qualitative research: A critical review. BMC Med. Res. Methodol. 2009, 9, 59. [Google Scholar] [CrossRef]
- Anekar, A.A.; Cascella, M. WHO Analgesic Ladder; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Brazier, J.E.; Harper, R.; Jones, N.M.; O’Cathain, A.; Thomas, K.J.; Usherwood, T.; Westlake, L. Validating the SF-36 health survey questionnaire: New outcome measure for primary care. BMJ 1992, 305, 160–164. [Google Scholar] [CrossRef]
- Stevenson, K.M.; Brown, R.L.; Dahl, J.L.; Ward, S.E.; Brown, M.S. The Discomfort Behavior Scale: A measure of discomfort in the cognitively impaired based on the Minimum Data Set 2.0. Res. Nurs. Health 2006, 29, 576–587. [Google Scholar] [CrossRef]
- Morris, D.; Galicia-Castillo, M. Dying With Dyspnea in the Hospital. Am. J. Hosp. Palliat. Care 2017, 34, 132–134. [Google Scholar] [CrossRef]
- Gannon, J.A.; Guinan, E.M.; Doyle, S.L.; Beddy, P.; Reynolds, J.V.; Hussey, J. Reduced fitness and physical functioning are long-term sequelae after curative treatment for esophageal cancer: A matched control study. Dis. Esophagus 2017, 30, 1–7. [Google Scholar] [CrossRef]
- Sand, L.; Strang, P.; Milberg, A. Dying cancer patients’ experiences of powerlessness and helplessness. Support. Care Cancer 2008, 16, 853–862. [Google Scholar] [CrossRef]
- Harnett, T. The Trivial Matters: Everyday Power in Swedish Elder Care. Ph.D. Thesis, Intellect Infolog, Kållered, Sweden, 2010. [Google Scholar]
- Kok, R.M.; Reynolds, C.F., 3rd. Management of Depression in Older Adults: A Review. JAMA 2017, 317, 2114–2122. [Google Scholar] [CrossRef]
- Pitman, A.; Suleman, S.; Hyde, N.; Hodgkiss, A. Depression and anxiety in patients with cancer. BMJ 2018, 361, k1415. [Google Scholar] [CrossRef]
- Creighton, A.S.; Davison, T.E.; Kissane, D.W. The prevalence of anxiety among older adults in nursing homes and other residential aged care facilities: A systematic review. Int. J. Geriatr. Psychiatry 2016, 31, 555–566. [Google Scholar] [CrossRef]
- Schofield, P. Loneliness in care homes, is it a phenomenon? And what can we do to improve the situation? Evid. Based Nurs. 2021, 24, 127. [Google Scholar] [CrossRef]
- Gardiner, C.; Laud, P.; Heaton, T.; Gott, M. What is the prevalence of loneliness amongst older people living in residential and nursing care homes? A systematic review and meta-analysis. Age Ageing 2020, 49, 748–757. [Google Scholar] [CrossRef]
- Gardiner, C.; Geldenhuys, G.; Gott, M. Interventions to reduce social isolation and loneliness among older people: An integrative review. Health Soc. Care Community 2018, 26, 147–157. [Google Scholar] [CrossRef]
- Bethell, J.; Aelick, K.; Babineau, J.; Bretzlaff, M.; Edwards, C.; Gibson, J.L.; Hewitt Colborne, D.; Iaboni, A.; Lender, D.; Schon, D.; et al. Social Connection in Long-Term Care Homes: A Scoping Review of Published Research on the Mental Health Impacts and Potential Strategies During COVID-19. J. Am. Med. Dir. Assoc. 2021, 22, 228–237.e25. [Google Scholar] [CrossRef]
- Carreno, D.F.; Eisenbeck, N. Existential Insights in Cancer: Meaning in Life Adaptability. Medicina 2022, 58, 461. [Google Scholar] [CrossRef]
- Vos, J. Meaning and existential givens in the lives of cancer patients: A philosophical perspective on psycho-oncology. Palliat. Support. Care 2015, 13, 885–900. [Google Scholar] [CrossRef]
- Regier, N.G.; Parisi, J.M.; Perrin, N.; Gitlin, L.N. Engagement in Favorite Activity and Implications for Cognition, Mental Health, and Function in Persons Living With and Without Dementia. J. Appl. Gerontol. 2022, 41, 441–449. [Google Scholar] [CrossRef]
- Smit, D.; de Lange, J.; Willemse, B.; Pot, A.M. Predictors of activity involvement in dementia care homes: A cross-sectional study. BMC Geriatr. 2017, 17, 175. [Google Scholar] [CrossRef]
- Hunt, R.W.; D’Onise, K.; Nguyen, A.T.; Venugopal, K. Where Patients With Cancer Die: A Population-Based Study, 1990 to 2012. J. Palliat. Care 2019, 34, 224–231. [Google Scholar] [CrossRef]
- Mitchell, G.; Agnelli, J.; McGreevy, J.; Diamond, M.; Roble, H.; McShane, E.; Strain, J. Palliative and end of life care for people living with dementia in care homes: Part 1. Nurs. Stand. 2016, 30, 54–63. [Google Scholar] [CrossRef]
- Verbeek, H.; Mitchell, G. Changing the long-term care spectrum. BMC Geriatr. 2022, 22, 303. [Google Scholar] [CrossRef]
- Mitchell, G.; Strain, J. The role of the named nurse in long-term settings. Nurs. Older People 2015, 27, 26–29. [Google Scholar] [CrossRef]
- Hatamipour, K.; Rassouli, M.; Yaghmaie, F.; Zendedel, K.; Majd, H.A. Spiritual needs of cancer patients: A qualitative study. Indian J. Palliat. Care 2015, 21, 61–67. [Google Scholar]
- Forouzi, M.A.; Tirgari, B.; Safarizadeh, M.H.; Jahani, Y. Spiritual Needs and Quality of Life of Patients with Cancer. Indian J. Palliat. Care 2017, 23, 437–444. [Google Scholar]
- Cheng, Q.; Xu, X.; Liu, X.; Mao, T.; Chen, Y. Spiritual needs and their associated factors among cancer patients in China: A cross-sectional study. Support. Care Cancer 2018, 26, 3405–3412. [Google Scholar] [CrossRef]
- Vitorino, L.M.; Lucchetti, G.; Santos, A.E.O.; Lucchetti, A.L.G.; Ferreira, E.B.; Adami, N.P.; Vianna, L.A.C. Spiritual Religious Coping is Associated with Quality of Life in Institutionalized Older Adults. J. Relig. Health 2016, 55, 549–559. [Google Scholar] [CrossRef]
- Mitchell, G.; Cousins, C.; Burrows, R.; Cousins, G. A review of safe-staffing models and their applicability to care homes. J. Nurs. Manag. 2017, 25, 157–162. [Google Scholar] [CrossRef]
- Mitchell, G.; Porter, S.; Manias, E. Enabling sustained communication with patients for safe and effective management of oral chemotherapy: A longitudinal ethnography. J. Adv. Nurs. 2021, 77, 899–909. [Google Scholar] [CrossRef]
- Cousins, C.; Burrows, R.; Cousins, G.; Dunlop, E.; Mitchell, G. An overview of the challenges facing care homes in the UK. Nurs. Older People 2016, 28, 18–21. [Google Scholar] [CrossRef]
- Harding, A.; Preston, N.; Doherty, J.; Cousins, E.; Varey, S.; McCann, A.; Dening, K.H.; Finucane, A.; Carter, G.; Mitchell, G.; et al. Developing and evaluating online COVID-centric advance care planning training and information resources for nursing staff and family members in nursing homes: The necessary discussions study protocol. BMC Geriatr. 2021, 21, 456. [Google Scholar] [CrossRef]
- Shallcross, L.; Burke, D.; Abbott, O.; Donaldson, A.; Hallatt, G.; Hayward, A.; Hopkins, S.; Krutikov, M.; Sharp, K.; Wardman, L.; et al. Factors associated with SARS-CoV-2 infection and outbreaks in long-term care facilities in England: A national cross-sectional survey. Lancet Healthy Longev. 2021, 2, e129–e142. [Google Scholar] [CrossRef]
- Zhang, N.J.; Unruh, L.; Wan, T.T. Gaps in nurse staffng and nursing home resident needs. Nurs. Econ. 2013, 31, 289–297. [Google Scholar]
- NHS. Enhanced Health in Care Homes; NHS: Leeds, UK, 2020. [Google Scholar]
- Firn, J.; Preston, N.; Walshe, C. What are the views of hospital-based generalist palliative care professionals on what facilitates or hinders collaboration with in-patient specialist palliative care teams? A systematically constructed narrative synthesis. Palliat. Med. 2016, 30, 240–256. [Google Scholar] [CrossRef]
- James, I.; Blomberg, K.; Kihlgren, A. A meaningful daily life in nursing homes—A place of shelter and a space of freedom: A participatory appreciative action reflection study. BMC Nurs. 2014, 13, 19. [Google Scholar] [CrossRef]
- Cousins, E.; Preston, N.; Doherty, J.; Varey, S.; Harding, A.; McCann, A.; Harrison Dening, K.; Finucane, A.; Carter, G.; Mitchell, G.; et al. Implementing and evaluating online advance care planning training in UK nursing homes during COVID-19: Findings from the Necessary Discussions multi-site case study project. BMC Geriatr. 2022, 22, 419. [Google Scholar] [CrossRef]
- Gonella, S.; Mitchell, G.; Bavelaar, L.; Conti, A.; Vanalli, M.; Basso, I.; Cornally, N. Interventions to support family caregivers of people with advanced dementia at the end of life in nursing homes: A mixed-methods systematic review. Palliat. Med. 2022, 36, 268–291. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Authors, Country | Aim of Research | Research Design | Outcome of Critical Appraisal (JBI, 2020) | Sample and Setting | Main Findings |
|---|---|---|---|---|---|
| Bainbridge et al., 2015 Canada [32] | To examine the contribution of covariates to having an emergency department (ED) visit in the last 6 months of life or to dying in hospital. | Cohort study | Strong | Long-term care facility residents (n = 1196) Long-term care facility | A total of 61% visited the emergency department in the last 6 months of life (average of 2.3 visits per person) and 20% died in the hospital. Cancer type, income, gender, time in long-term care, and rural location did not predict acute care outcomes. However, comorbidities, younger age, and region of residence were significant predictors of emergency department visits and/or hospital deaths. |
| Blytt et al., 2018 Norway [35] | To identify the prevalence of cancer and differences regarding neuropsychiatric symptoms (NPSs) and medication among nursing home (NH) patients with and without dementia and cancer. | Cross-sectional study | Strong | Nursing home residents (n = 1825) with and without dementia with cancer from 64 nursing homes in Norway. Nursing homes | Patients with comorbid dementia and cancer received significantly more analgesics than patients without cancer but with dementia. Patients with comorbid dementia and cancer also had significantly more NPS, including sleep disturbances and agitation, compared to patients without dementia but with cancer. |
| Boyd et al., 2019 New Zealand [19] | To describe the end-of-life experience of those living in LTC facilities in New Zealand. | Cross-sectional study | Moderate | Residents in 61 long-term care facilities (n = 286) who had died from cancer (17%), dementia (49%), both cancer and dementia (4%), or another chronic illness (30%). Long-term care facility | Palliative care principles should be integrated with geriatric care to provide high-quality end-of-life care in LTC facilities. It is essential that those working in LTC facilities recognize palliative care philosophy, and specialist palliative care providers work collaboratively with gerontologists to ensure high-quality end-of-life care for people with complex geriatric syndromes. |
| Drageset et al., 2020 Norway [26] | To examine loneliness among nursing home residents over 6 years and whether sociodemographic factors, sense of coherence, social support, or depression symptoms might influence loneliness. | Cross-sectional study | Strong | Nursing home residents (n = 122) living with cancer aged 65 years or older. Nursing homes | This study has three important findings. First, loneliness did not change over time during the 6 years of follow-up. Second, symptoms of depression and the sense of coherence seem to be important components of loneliness. Third, social support dimensions and having a diagnosis of cancer were not associated with loneliness. |
| Drageset et al., 2012 Norway [37] | To study the sociodemographic characteristics and HRQOL among NH residents with and without a cancer diagnosis, adjusting for comorbidity. | Cross-sectional study | Strong | Nursing home residents (n = 60) living with cancer aged 65 years or older. Nursing homes | NH residents with cancer reported worse HRQOL compared to those without cancer, including more pain and worse general health. However, after adjusting for comorbidities, the difference in general health was no longer statistically significant. Cognitively intact residents with cancer reported less role limitation related to emotional problems. |
| Drageset et al., 2013 Norway [22] | To investigate loneliness and mortality among cognitively intact NH residents with cancer vs. those without cancer. | Cross-sectional study | Moderate | Nursing home residents (n = 227) with cognition intact, with cancer (n = 60), and without cancer (n = 167) from 30 nursing homes. Nursing homes | Age, education, comorbidity, and emotional loneliness (attachment) were associated with mortality in nursing home residents, but survival did not differ significantly between residents with and without cancer. |
| Drageset et al., 2013 Norway [21] | To investigate whether anxiety and/or depression: 1. Are associated with survival and 2. Have different effects on survival; for residents with and without cancer. | Cross-sectional study | Moderate | Nursing home residents (n = 227) with cognition intact, with cancer (n = 60), and without cance4r (n = 167) from 30 nursing homes. Nursing homes | Depression and comorbidity predicted 5-year mortality for NH residents. Cancer diagnosis did not have a significant impact on survival time, but anxiety symptoms predicted shorter survival for residents with cancer. Caregivers should closely observe residents with cancer for anxiety symptoms and depression and comorbidity should be monitored regardless of cancer diagnosis. |
| Drageset et al., 2015 Norway [23] | To investigate loneliness and social support among cognitively intact nursing home residents with cancer. | Mixed-methods study | Strong | Nursing home residents (n = 60) living with cancer aged 65 years or older. Nursing homes | Loneliness is associated with reassurance of worth. It is experienced as inner pain, loss, and feeling small. To alleviate loneliness, one should be engaged in activities, be in contact with others, and occupy oneself. |
| Drageset et al., 2015 Norway [20] | To investigate the holistic needs of cancer patients living in care homes without a cognitive impairment during an acute hospital admission. | Cross-sectional study | Strong | Nursing home residents (n = 60) living with cancer aged 65 years or older. Nursing homes | Residents with cancer had more admissions (25/60) than those without (53/167). Social integration was correlated with admission (p = 0.04) regardless of cancer diagnosis. |
| Drageset et al., 2016 Norway [24] | To investigate the sense of coherence (SOC) and depression among cognitively intact NH residents with cancer and their experience with depression and coping. | Mixed-methods study | Moderate | Nursing home residents (n = 60) living with cancer aged 65 years or older. Nursing homes | This study found that the General Depression Scale (GDS) was significantly correlated with SOC, with a stronger SOC associated with less symptoms of depression. The experience of sadness was identified as a dominant theme in coping with symptoms of depression. Over half of nursing home residents reported symptoms of depression, highlighting the need to pay attention to their experience of depression and SOC to improve their situation. |
| Drageset et al., 2017 Norway [25] | The study aimed to examine HRQOL over time during a 6-year period among residents of NHs who are not cognitively impaired and to examine whether sense of coherence and a diagnosis of cancer influence HRQOL. | Cross-sectional study | Strong | Nursing home residents (n = 227) with cognition intact. Nursing homes | During a 6-year follow-up, physical functioning and role limitation-physical sub-scores declined, and having cancer at baseline was negatively associated with general health. Sense of coherence at baseline was positively correlated with all sub-scores of a 36-Item Short Form Survey (SF-36). Sense of coherence was found to be an important component of HRQOL, and having cancer was linked to a decline in general health. |
| Dubé et al., 2018 USA [27] | To evaluate whether the documentation and management of pain varies by level of cognitive impairment among nursing home residents with cancer. | Cross-sectional study | Strong | Nursing home residents (n = 367, 462) with cancer. Nursing homes | For those with staff-assessed pain, pain prevalence was 55.5% with no/mild cognitive impairment and 50.5% in those severely impaired. Pain was common in those able to self-report. Greater cognitive impairment was associated with reduced prevalence of any pain. Pharmacologic pain management was less prevalent in those with severe cognitive impairment. |
| Finlayson et al., 2012 USA [36] | To compare outcomes of nursing home residents undergoing colectomy with benchmark mortality and functional decline in the general nursing home population. | Cohort study | Strong | Nursing home residents (n = 6822) who underwent surgery for colon cancer who were 65 years or older. Nursing homes | Nursing home residents who underwent colectomy experienced a 3.9-point worsening in Minimum Data Set (MDS)-ADL score on average after 1 year, with mortality and sustained functional decline rates of 53% and 24%, respectively. Older age, readmission after surgical hospitalization, and surgical complications were associated with functional decline at 1 year. The study suggests that initiatives aimed at improving surgical outcomes are needed in this vulnerable population. |
| Hunnicutt et al., 2017 USA [28] | To estimate the extent to which receipt of hospice in nursing homes (NHs) increases the receipt of pain management for residents with cancer at the end of life. | Cohort study | Strong | Medicare beneficiaries with cancer (n = 78,160) who were nursing home residents in the last 90 days of life. Nursing homes | In hospice residents, pain prevalence was higher compared to non-hospice residents, but untreated pain was uncommon. Hospice use was associated with receiving scheduled analgesics and medication “as needed”, and this association was similar in residents with staff-assessed pain. Therefore, hospice is linked with increased pain management in those with documented pain. |
| Lage et al., 2020 USA [29] | To examine factors associated with potentially burdensome end-of-life (EOL) transitions between care settings among older adults with advanced cancer in nursing homes (NHs). | Cohort study | Strong | Deceased older nursing home residents with cancer (n = 34,670). Nursing Hhomes | A study of 34,670 subjects showed that 53.8% had moderate to severe cognitive impairment and full dependence on activities of daily living (ADLs). A total of 56.3% of patients used hospice in the 90 days before death, while 36% had potentially burdensome end-of-life transitions, which was higher in patients who did not receive hospice care. Factors associated with higher risk of burdensome EOL transitions were full dependence on ADLs, congestive heart failure, and chronic obstructive pulmonary disease. Patients with do-not-resuscitate directives and impaired cognition had lower odds of burdensome EOL transitions. |
| Mack et al., 2018 USA [33] | To evaluate racial disparities in pain management among residents with cancer in nursing homes at time of admission | Cross-sectional study | Strong | Newly admitted nursing home residents with cancer (n = 342,920) Nursing homes | Among nursing home residents with cancer, 60% reported pain, with non-Hispanic Blacks less likely to have both self-reported pain and staff-reported pain documentation compared with Non-Hispanic Whites. Although most residents received some pharmacologic pain management, Blacks were less likely to receive any compared with Whites, consistent with differences in receipt of non-pharmacologic treatments. |
| Monroe et al., 2012 USA [35] | To assess pain in nursing home residents with mild to very severe Alzheimer’s disease (AD) who died from cancer. | Cross-sectional study | Strong | Nursing home residents (n = 48) with mild to severe dementia Nursing homes | The severity of Alzheimer’s disease was negatively related to pain behaviours, with a significant difference between moderate and very severe Alzheimer’s. There was no significant correlation between opioid analgesics and pain behavior, but individuals with severe Alzheimer’s disease received fewer opioids. |
| Monroe et al., 2013 USA [30] | The aim of the current pilot study was to examine the association between hospice enrolment, dementia severity, and pain among nursing home residents who died from advanced cancer. | Cross-sectional study | Strong | Nursing home residents (n = 55) with dementia who died from cancer, 54.5% female. Mean age 86.4 ± 7.8. Nursing homes | About 45% of nursing home residents were in hospice at the end of life, and they were more likely to receive an opioid but less likely to have severe cognitive impairment. Hospice enrolment was linked to an increased chance of receiving an opioid, but lower cognitive functioning decreased the likelihood of receiving an opioid. However, it is noteworthy that 40% of nursing home residents with dementia who died from cancer did not receive any opioid during this time. |
| Parast et al., 2021 USA [38] | To compare the quality of hospice care provided in various venues while looking at the experiences of decedents with a primary cancer diagnosis and their family caregivers. | Cross-sectional study | Moderate | Caregiver respondents (n = 217,596) whose family member had a primary cancer diagnosis and died in 2017–2018 while receiving hospice care from 2890 hospices. Long-term care facilities | The study found that quality measures for care in nursing homes and assisted living facilities varied significantly, with scores ranging from 74.9 for receiving hospice care training to 89.5 for treating family members with respect. Caregivers of deceased patients consistently reported lower quality of care, with scores varying significantly across settings. The overall score for obtaining treatment for symptoms was 75.1, with scores ranging from 60.6 to 84.5 for individual items within the measure. |
| Pimentel et al., 2015 USA [31] | To assess improvements in pain management of NH residents with cancer since the implementation of pain management quality indicators. | Cross-Sectional Study | Strong | Nursing home residents (n = 8094) with cancer. Nursing Homes | The study found that over 65% of nursing home residents with cancer had some level of pain, with 28.3% experiencing daily pain and 37.3% experiencing pain less than daily. Of those with pain, 13.5% had severe pain and 61.3% had moderate pain. Women, residents admitted from acute care or who were bedfast, and those with compromised activities of daily living, depressed mood, indwelling catheter, or terminal prognosis were more likely to have pain. However, over 17% of residents with daily pain received no analgesics, including 11.7% with daily severe pain and 16.9% with daily moderate pain. The treatment was negatively associated with age > 85 years, cognitive impairment, presence of a feeding tube, and restraints. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Craig, S.; Cao, Y.; McMahon, J.; Anderson, T.; Stark, P.; Brown Wilson, C.; Creighton, L.; Gonella, S.; Bavelaar, L.; Vlčková, K.; et al. Exploring the Holistic Needs of People Living with Cancer in Care Homes: An Integrative Review. Healthcare 2023, 11, 3166. https://doi.org/10.3390/healthcare11243166
Craig S, Cao Y, McMahon J, Anderson T, Stark P, Brown Wilson C, Creighton L, Gonella S, Bavelaar L, Vlčková K, et al. Exploring the Holistic Needs of People Living with Cancer in Care Homes: An Integrative Review. Healthcare. 2023; 11(24):3166. https://doi.org/10.3390/healthcare11243166
Chicago/Turabian StyleCraig, Stephanie, Yanting Cao, James McMahon, Tara Anderson, Patrick Stark, Christine Brown Wilson, Laura Creighton, Silvia Gonella, Laura Bavelaar, Karolina Vlčková, and et al. 2023. "Exploring the Holistic Needs of People Living with Cancer in Care Homes: An Integrative Review" Healthcare 11, no. 24: 3166. https://doi.org/10.3390/healthcare11243166