
Cannulation Technique of Vascular Access in Haemodialysis and the Impact on the Arteriovenous Fistula Survival: Protocol of Systematic Review




{kind=link}
Abstract
:1. Introduction
2. Methods and Analysis
2.1. Objectives
2.2. Eligibility Criteria
2.3. Types of Participants/Population
2.4. Types of Study to Be Included
2.5. To Be Excluded
2.6. Search Methods for Identification of Studies
2.7. Other Sources
2.8. Comparator Control
2.9. Context
2.10. Primary Outcomes
2.11. Secondary Outcomes
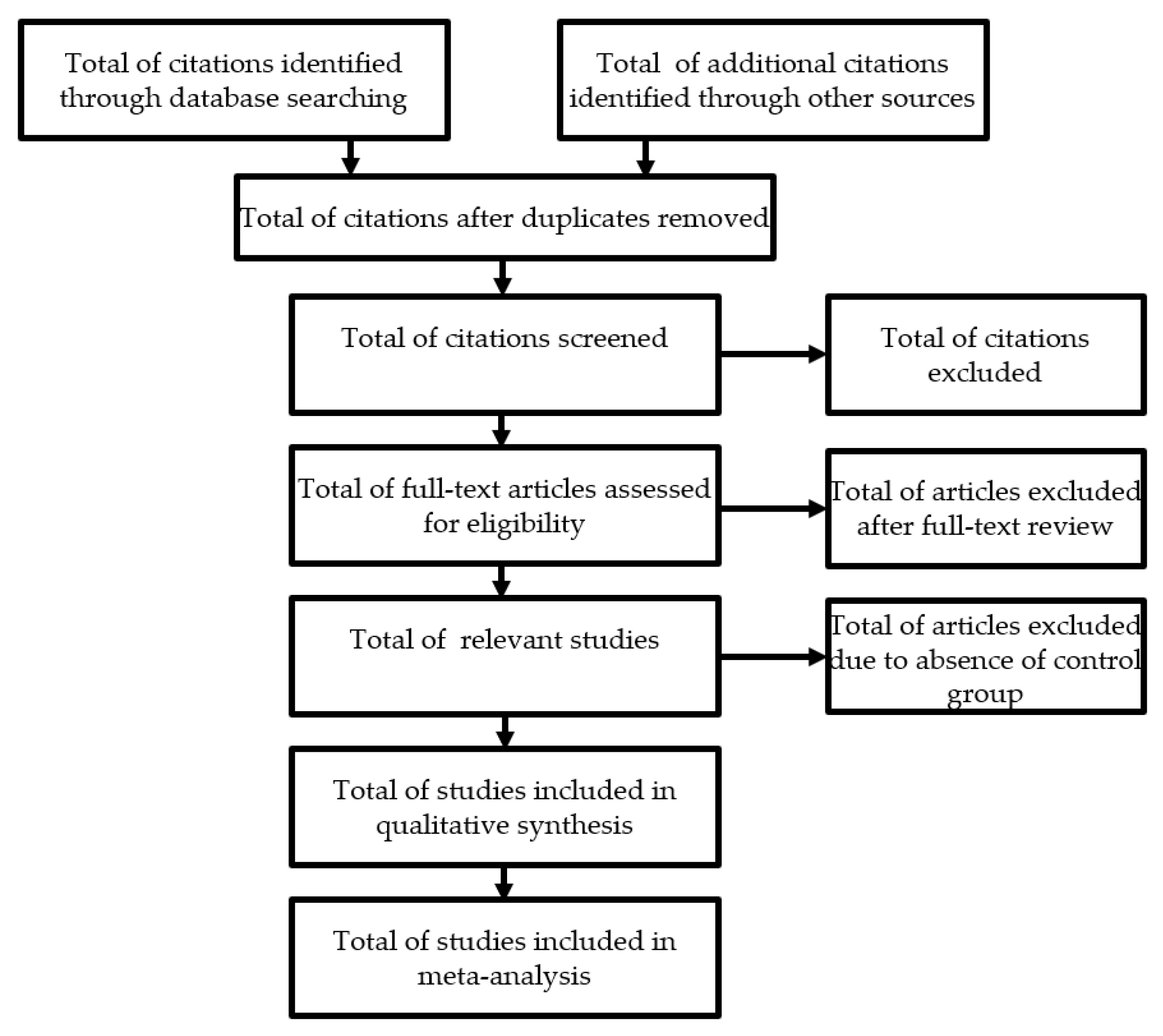
2.12. Data Extraction (Selection and Coding)
2.13. Risk of Bias Assessment
2.14. Strategy for Data Synthesis
2.15. Analysis of Subgroups or Subsets
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Lee, T. Novel paradigms for dialysis vascular access: Downstream vascular biology-is there a final common pathway? Clin. J. Am. Soc. Nephrol. 2013, 8, 2194–2201. [Google Scholar] [CrossRef] [Green Version]
- Nath, K.A. Dialysis Vascular Access Intervention and the Search for Biomarkers. J. Am. Soc. Nephrol. 2016, 27, 970–972. [Google Scholar] [CrossRef] [Green Version]
- Ethier, J.; Mendelssohn, D.C.; Elder, S.J.; Hasegawa, T.; Akizawa, T.; Akiba, T.; Canaud, B.J.; Pisoni, R.L. Vascular access use and outcomes: An international perspective from the dialysis outcomes and practice patterns study. Nephrol. Dial. Transpl. 2008, 23, 3219–3226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feldman, H.I.; Held, P.J.; Hutchinson, J.T.; Stoiber, E.; Hartigan, M.F.; Berlin, J.A. Hemodialysis vascular access morbidity in the United States. Kidney Int. 1993, 43, 1091–1096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roy-Chaudhury, P. Hemodialysis Vascular Access Dysfunction: A Cellular and Molecular Viewpoint. J. Am. Soc. Nephrol. 2006, 17, 1112–1127. [Google Scholar] [CrossRef] [PubMed]
- Dhingra, R.K.; Young, E.W.; Hulbert-Shearon, T.E.; Leavey, S.F.; Port, F.K. Type of vascular access and mortality in U.S. hemodialysis patients. Kidney Int. 2001, 60, 1443–1451. [Google Scholar] [CrossRef] [Green Version]
- McCann, M.; Einarsdottir, H.; Waeleghem, J.P.; Van Murphy, F.; Nurs, R.; Sedgwick, J. Vascular access management II: AVF/AVG cannulation techniques and complications. J. Ren. Care 2009, 35, 90–98. [Google Scholar] [CrossRef]
- Gallieni, M.; Hollenbeck, M.; Inston, N.; Kumwenda, M.; Powell, S.; Tordoir, J.; Shakarchi, J.A.; Berger, P.; Bolignano, D.; Cassidy, D.; et al. Clinical practice guideline on peri- and postoperative care of arteriovenous fistulas and grafts for haemodialysis in adults. Nephrol. Dial. Transpl. 2019, 34, II1–II42. [Google Scholar] [CrossRef]
- Ball, L.K. Improving arteriovenous fistula cannulation skills. Nephrol. Nurs. J. 2005, 32, 611–617. [Google Scholar]
- Dinwiddie, L.C.; Ball, L.; Brouwer, D.; Doss-Mcquitty, S.; Holland, J. What Nephrologists Need to Know about Vascular Access Cannulation. Semin. Dial. 2013, 26, 315–322. [Google Scholar] [CrossRef]
- Parisotto, M.T.; Schoder, V.U.; Miriunis, C.; Grassmann, A.H.; Scatizzi, L.P.; Kaufmann, P.; Stopper, A.; Marcelli, D. Cannulation technique influences arteriovenous fistula and graft survival. Kidney Int. 2014, 86, 790–797. [Google Scholar] [CrossRef] [Green Version]
- Sukthinthai, N.; Sittipraneet, A.; Tummanittayangkoon, B.; Vasuvattakul, S.; Chanchairujira, T. Buttonhole technique better than area puncture technique on hemostasis and pain associated with needle cannulation. J. Med. Assoc. Thai. 2012, 95 (Suppl. 2), 4–6. [Google Scholar]
- Gallieni, M.; Brenna, I.; Brunini, F.; Mezzina, N.; Pasho, S.; Fornasieri, A. Which cannulation technique for which patient. J. Vasc. Access 2014, 15 (Suppl. 7), 85–90. [Google Scholar] [CrossRef]
- Aitken, E.; McLellan, A.; Glen, J.; Serpell, M.; Mactier, R.; Clancy, M. Pain resulting from arteriovenous fistulae: Prevalence and impact. Clin. Nephrol. 2013, 80, 328–333. [Google Scholar] [CrossRef]
- da Silva, O.M.; Rigon, E.; Corradi Dalazen, J.V.; Bissoloti, A.; Rabelo-Silva, E.R. Pain during Arteriovenous Fistula Cannulation in Chronic Renal Patients on Hemodialysis. Open J. Nurs. 2016, 6, 1028–1037. [Google Scholar] [CrossRef] [Green Version]
- MacRae, J.M.; Ahmed, S.B.; Atkar, R.; Hemmelgarn, B.R. A randomized trial comparing buttonhole with rope ladder needling in conventional hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2012, 7, 1632–1638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Twardowski, Z.; Kubara, H. Different sites versus constant sites of needle insertion into arteriovenous fistulas for treatment by repeated dialysis. Dial. Transpl. 1979, 8, 978–980. [Google Scholar]
- Grudzinski, A.; Mendelssohn, D.; Pierratos, A.; Nesrallah, G. A systematic review of buttonhole cannulation practices and outcomes. Semin. Dial. 2013, 26, 465–475. [Google Scholar] [CrossRef]
- Collier, S.; Kandil, H.; Yewnetu, E.; Cross, J.; Caplin, B.; Davenport, A. Infection Rates Following Buttonhole Cannulation in Hemodialysis Patients. Ther. Apher. Dial. 2016, 20, 476–482. [Google Scholar] [CrossRef] [PubMed]
- Ren, C.; Han, X.; Huang, B.; Yuan, L.; Cao, Y.; Yang, X. Efficacy of buttonhole cannulation (BH) in hemodialysis patients with arteriovenous fistula: A meta-analysis. Int. J. Clin. Exp. Med. 2016, 9, 15363–15370. [Google Scholar]
- Van Loon, M.M.; Goovaerts, T.; Kessels, A.G.H.; Van Der Sande, F.M.; Tordoir, J.H.M. Buttonhole needling of haemodialysis arteriovenous fistulae results in less complications and interventions compared to the rope-ladder technique. Nephrol. Dial. Transpl. 2010, 25, 225–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chow, J.; Rayment, G.; Miguel, S.S.; Gilbert, M. A randomised controlled trial of buttonhole cannulation for the prevention of fistula access complications. J. Ren. Care. 2011, 37, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Wong, B.; Muneer, M.; Wiebe, N.; Storie, D.; Shurraw, S.; Pannu, N.; Klarenbach, S.; Grudzinski, A.; Nesrallah, G.; Pauly, R.P. Buttonhole versus rope-ladder cannulation of arteriovenous fistulas for hemodialysis: A systematic review. Am. J. Kidney Dis. 2014, 64, 918–936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muir, C.A.; Kotwal, S.S.; Hawley, C.M.; Polkinghorne, K.; Gallagher, M.P.; Snelling, P.; Jardine, M.J. Buttonhole cannulation and clinical outcomes in a home hemodialysis cohort and systematic review. Clin. J. Am. Soc. Nephrol. 2014, 9, 110–119. [Google Scholar] [CrossRef] [Green Version]
- Struthers, J.; Allan, A.; Peel, R.K.; Lambie, S.H. Buttonhole needling of ateriovenous fistulae: A randomized controlled trial. ASAIO J. 2010, 56, 319–322. [Google Scholar] [CrossRef] [PubMed]
- Toma, S.; Shinzato, T.; Fukui, H.; Nakai, S.; Miwa, M.; Takai, I.; Maeda, K. A timesaving method to create a fixed puncture route for the buttonhole technique. Nephrol. Dial. Transpl. 2003, 18, 2118–2121. [Google Scholar] [CrossRef] [Green Version]
- Vaux, E.; King, J.; Lloyd, S.; Moore, J.; Bailey, L.; Reading, I.; Naik, R. Effect of buttonhole cannulation with a polycarbonate peg on in-center hemodialysis fistula outcomes: A randomized controlled trial. Am. J. Kidney Dis. 2013, 62, 81–88. [Google Scholar] [CrossRef]
- Peralta, R.; Matos, J.F.; Carvalho, H. Safe Needling of Arteriovenous Fistulae in Patients on Hemodialysis: Literature Review and a New Approach. Nephrol. Nurs. J. 2021, 48, 169–177. [Google Scholar] [CrossRef]
- Peralta, R.; Fazendeiro Matos, J.; Pinto, B.; Gonçalves, P.; Sousa, R.; Felix, C.; Carvalho, H.; Vinhas, J.; Ponce, P. Multiple single cannulation technique of arteriovenous fistula: A randomized controlled trial. Hemodial. Int. 2021, 1–9. [Google Scholar] [CrossRef]
- Balaz, P.; Björck, M. True aneurysm in autologous hemodialysis fistulae: Definitions, classification and indications for treatment. J. Vasc. Access 2015, 16, 446–453. [Google Scholar] [CrossRef]
- Page, M.J.; Mckenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 58, 20–25. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. Revised Cochrane Risk-of-Bias Tool for Randomized Trials (RoB 2); Cochrane: London, UK, 2019; p. 366. Available online: https://methods.cochrane.org/risk-bias-2 (accessed on 23 January 2021).
- Sterne, J.A.C.; Higgins, J.P.T.; Elbers, R.G.; Reeves, B.C.; on behalf of the Development Group for ROBINS-I. Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I). 2016. Available online: http://www.riskofbias.info (accessed on 23 January 2021).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peralta, R.; Sousa, L.; Cristóvão, A.F. Cannulation Technique of Vascular Access in Haemodialysis and the Impact on the Arteriovenous Fistula Survival: Protocol of Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 12554. https://doi.org/10.3390/ijerph182312554
Peralta R, Sousa L, Cristóvão AF. Cannulation Technique of Vascular Access in Haemodialysis and the Impact on the Arteriovenous Fistula Survival: Protocol of Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(23):12554. https://doi.org/10.3390/ijerph182312554
Chicago/Turabian StylePeralta, Ricardo, Luís Sousa, and António Filipe Cristóvão. 2021. "Cannulation Technique of Vascular Access in Haemodialysis and the Impact on the Arteriovenous Fistula Survival: Protocol of Systematic Review" International Journal of Environmental Research and Public Health 18, no. 23: 12554. https://doi.org/10.3390/ijerph182312554