Abstract
Background: Off-label nebulization of tranexamic acid (TXA) solution is common practice for the treatment of hemoptysis. However, data regarding nebulization protocols, resulting aerodynamic parameters of the generated aerosol, and corresponding biopharmaceutical parameters are missing. The aim of this in vitro study was to investigate the aerosol characteristics of nebulized sterile, aqueous TXA solution. Methods: TXA solution 100 mg/mL was nebulized for 2 min by a multi-dose vibrating mesh nebulizer using 15 L/min and 30 L/min air flow rates. The generated aerosol was analyzed by a Next Generation Cascade Impactor. For each air flow rate, the mean Fine Particle Dose (FPD), Fine Particle Fraction (FPF), the Mass Median Aerodynamic Diameter (MMAD), and Geometric Standard Deviation (GSD) were quantified. Results: Nebulization at 15 L/min air flow rate resulted in a MMAD of 6.68 ± 0.23 µm and GSD of 2.02 ± 0.16. The FPD < 5 µm was 16.56 ± 0.45 mg, the FPF < 5 µm 28.91 ± 3.40%. Nebulization at 30 L/min air flow rate revealed a MMAD of 5.18 ± 0.12 µm and GSD of 2.14 ± 0.10. The FPD < 5 µm was 16.30 ± 1.38 mg, the FPF < 5 µm 35.43 ± 0.59%. Conclusions: Nebulization of TXA 100 mg/mL solution by a specified vibrating mesh nebulizer generated an aerosol particle distribution and deposition pattern suitable for the treatment of hemoptysis with bronchial origin.
1. Introduction
Tranexamic acid (TXA) is widely used by intravenous administration for prophylaxis and treatment of bleeding caused by hyperfibrinolysis in various medical scenarios such as menstrual bleeding, gastrointestinal bleeding, urinary tract disorders, surgeries, childbirth, cardiovascular procedures, and as an antidote for bleeding during fibrinolytic therapy [1,2]. Tranexamic acid, which binds to the lysine-binding sites of plasminogen, thereby inhibiting plasmin formation and preserving fibrin’s matrix structure. TXA is generally well tolerated, with serious side effects being rare and dose-dependent [1,3].
Of note, it is worldwide common clinical practice to use TXA off-label via inhalation for the control of pulmonary bleeding and hemoptysis [3,4,5,6,7,8]. Mostly, 500 mg TXA doses are administered three times a day via nebulization [3,4]. Typical TXA concentrations used for nebulization are 100 mg/mL or 50 mg/mL diluted with 0.9% sodium chloride solution [3]. In general, TXA containing medicinal products licensed for intravenous injection (500 mg/5 mL or 1000 mg/10 mL) are used for pulmonary administration using conventional nebulizers [3]. In our medical center, it is common practice to nebulize 5 mL of TXA injection solution 100 mg/mL three to four times a day using a multi-dose vibrating mesh nebulizer for the treatment of hemoptysis. To date, studies on the aerodynamic parameters and corresponding bioavailability of TXA aerosols [9] are not published and TXA containing medicinal products licensed for nebulization are not available.
Nebulization facilitates the delivery of active substances directly to the lower respiratory tract. Successful inhalation therapy with nebulizers highly depends on the physical characteristics of the generated particles and the inspiratory flow patterns. The mass median aerodynamic diameter (MMAD) plays a crucial role in assessing aerosol dynamics and related lung deposition [10,11]. Particles larger than 10 µm are mainly deposited in the upper respiratory tract due to impaction, and particles smaller than 1 µm are frequently exhaled. Particles ≥ 5 µm, ≤10 µm tend to deposit predominantly in the upper parts of the lower airways, such as the bronchi, while particles ranging from 1 µm to 5 µm deposit in the lower lung alveoli [10,11]. The fine particle dose (FPD < 5 µm) and the fine particle fraction (FPF < 5 µm) specify the absolute and percentage rate of potential lung-deposited aerosol with particle sizes smaller than 5 µm in relation to the total dose delivered.
Aerosol characteristics vary with the nebulizer system used, e.g., jet or vibrating mesh nebulizer, and can be assessed in vitro via cascade impaction [11,12]. The suitability of a medicinal product for nebulization depends on the characteristics of the active substance (e.g., solubility, thermal stability) and the characteristics of the dosage form (e.g., viscosity). TXA (trans-4-(Aminomethyl) cyclohexanecarboxylic acid) (Figure 1) is a small (Mw 157.2 g/mol) synthetic lysine analog, highly water-soluble active substance [2,13] and TXA injection solutions are free from any excipients [14]. Storage of TXA injection solution at 50 °C over a seven day period does not cause significant chemical degradation [15].
Figure 1.
Chemical structural formula of TXA.
Although there is widespread use of TXA inhalation and evidence of its clinical benefits [3,4,5,6,7,8], qualitative and quantitative aerosol characteristics of nebulized TXA solutions are not investigated. The aim of our proof-of-concept study was to determine the aerodynamic characteristics of aqueous TXA 100 mg/mL solutions nebulized with a multi-dose vibrating mesh nebulizer using two different inspiratory air flow rates thereby simulating exemplary conditions of TXA inhalation. The TXA aerosol characteristics are determined by cascade impaction and calculation of the MMAD, geometric standard deviation (GSD), FPD and FPF. Based on the results, the suitability of TXA 100 mg/mL aqueous injection solution for nebulization and the appropriateness of the aerodynamic parameters and deposition pattern of the TXA aerosol to control pulmonary bleeding and hemoptysis will be assessed.
2. Materials and Methods
2.1. Materials
Tranexamic acid injection solution 100 mg/mL, 10 mL (100 mg Tranexamic acid dissolved in 1 mL aqua ad inj.), batch number: 20230807-02, unlicensed on stock product of the Pharmacy Department of the University Medical Center Mainz.
Glass fiber filter (MN 85/70, article number 403007, Macherey-Nagel, Düren, Germany).
Anhydrous acetic acid (100%, article number 6755.1, Carl Roth GmbH + Co. KG, Karlsruhe, Germany).
Perchloric acid (0.1 M, article number 1.09065.1000, Sigma-Aldrich, St. Louis, MI, USA).
Gentian violet solution 0.5% as titration indicator (0.5 g of gentian violet solved in 100 mL anhydrous acetic acid).
Water for injection Ph. Eur. 0169 [16].
2.2. Methods
The experiments were designed to simulate clinical practice of TXA 100 mg, 5 mL aerosolization by the Aerogen® Solo nebulizer (G-AS 3001, Aerogen Ltd., Galway, Ireland) at the University Medical Center Mainz. Characteristics of the generated aerosol were determined by cascade impaction following the Ph. Eur. monograph 2.9.18 “Preparations for Inhalation: Aerodynamic Assessment of Fine Particles; Equipment E” [17] and the Euro norm EN 13544-1: 2007 + A1 (August 2009) [18]. All experiments were conducted at room temperature (22 ± 0.5 °C) and at 60–65% relative humidity. The collection time of 2 min was chosen based on pre-test results to facilitate a sufficient and quantifiable deposition of TXA on all impactor stages. The experimental setup and TXA aerosol characteristics determined are summarized in Table 1.

Table 1.
Overview of the aerodynamic analysis parameters of TXA 100 mg/mL aerosol and analytical methods used.
2.2.1. Aerodynamic Assessment of TXA Aerosol by Cascade Impaction
Experiments were performed with the next generation cascade impactor (NGI, Copley S/N NGI-0271, Copley Scientific Limited, Nottingham, UK). Prior to each experiment, the cleaned NGI was stored in a refrigerated room for at least two hours (2–8 °C). Each experiment was performed in quadruplicate. A new Aerogen® Solo nebulizer was used for each test to ensure that the mesh was not clogged or functionally impaired.
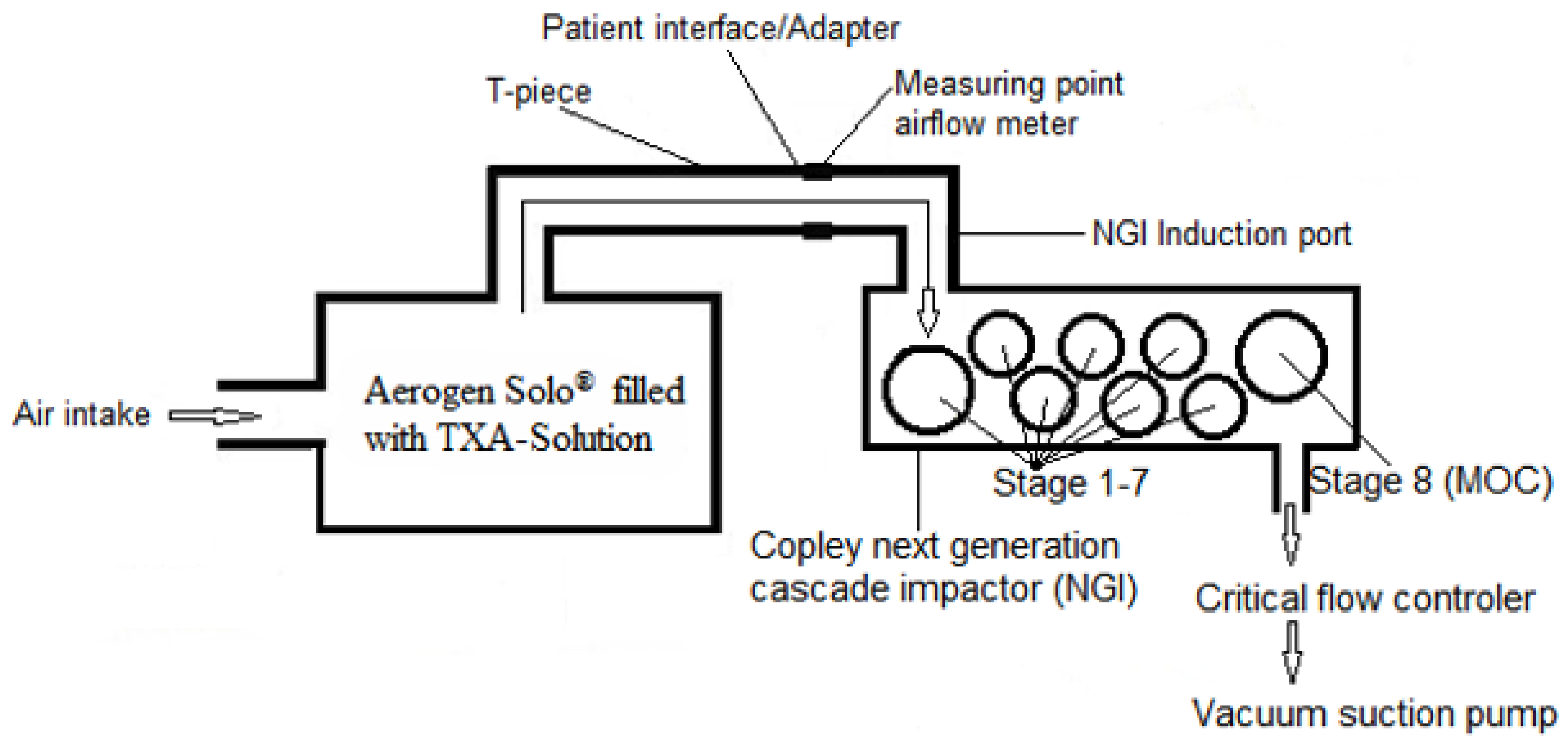
The NGI was connected to a vacuum pump (Copley Model HCP5, Copley Scientific Limited, Nottingham, UK) via a solenoid valve of a critical flow controller (Copley Model TPK, Copley Scientific Limited, Nottingham, UK). The NGI induction port was connected to the Aerogen® Solo nebulizer adult T-piece (Item number 10-356, Aerogen Ltd., Galway, Ireland) using a mouthpiece adapter (custom-cut bromobutyl stopper). The targeted continuous air flow of 15 L/min or 30 L/min was controlled with the Flow Meter DFM 2000 (Copley Scientific Limited, Nottingham, UK) connected to the Aerogen® Solo nebulizer adult T-piece. The test configuration is depicted in Figure 2. The reservoir of the Aerogen® Solo nebulizer was filled with 5 mL TXA 100 mg/mL injection solution. The vacuum pump and the critical flow controller were started first, followed by the nebulizer five seconds later. The TXA aerosol was collected during the nebulization time of 2 min in stage 1–7 of the NGI and a micro-orifice collector (MOC). To ensure full recovery of very fine particles an additional glass fiber filter (not shown in Figure 2) was placed downstream of the MOC. After 120 s, the nebulizer was switched off and after another five seconds the vacuum pump and the critical flow controller were also switched off. During the nebulization time, approximately 0.7 mL of TXA 100 mg/mL solution was nebulized.
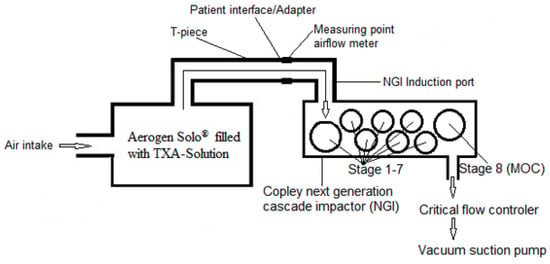
Figure 2.
Scheme of the aerodynamic assessment of TXA 100 mg/mL aerosol generated via the Aerogen® Solo nebulizer and sorted by the NGI cascade impactor.
2.2.2. Quantitative TXA Analysis by Anhydrous Titration
The mouthpiece adapter, the NGI induction port, the NGI stages 1–7, and the MOC together with the glass fiber filter were washed with approximately 5 mL of water for injection each. The resulting washing solution was individually collected in ten 250 mL Erlenmeyer flasks. In an additional flask, 5 mL of the pure water washing solution was prepared as a blank sample. The flasks were placed in a drying oven at 100 °C for about 3 h until completely dry.
The dry residue in each flask was solved in 20 mL anhydrous acetic acid, 0.1 mL of gentian violet solution (0.5%), added as indicator, and titrated with 0.1 M perchloric acid [19]. 1 mL perchloric acid 0.1 M corresponds to 15.72 mg TXA.
2.2.3. Data Processing
The mass of the TXA captured by the NGI at each step was calculated starting with the smallest diameter (MOC plus glass fiber filter) and in consideration of the air flow rate used (15 and 30 L/min). The cumulative mass was calculated for each of the seven stages as a function of the cutoff diameter for the respective impactor stage. The cutoff diameters are as follows: For 15 mL/min: 0.98 µm, 1.36 µm, 2.08 µm, 3.30 µm, 5.39 µm, 8.61 µm, 14.10 µm [20]. For 30 mL/min: 0.54 µm, 0.83 µm, 1.36 µm, 2.30 µm, 3.99 µm, 6.40 µm, 11.72 µm [17]. FPD, FPF, GSD were calculated according to the Ph. Eur. 2.9.18 [17]. MMAD was determined by plotting the cumulative fraction of TXA mass against the log 10 cutoff diameters. The MMAD represents the particle size at the intersection with the 50% cumulative fraction of TXA mass. Figures were prepared with Microsoft Excel Version 2016.
3. Results
Aerosolization of TXA 100 mg/mL injection solution was performed with the Aerogen® Solo nebulizer using the air flow rate 15 L/min and 30 mL/min. At both air flow rates, aerosolization of TXA 100 mg/mL revealed to generate an aerosol with MMAD, GSD, FPD, and FPF adequate for inhalation therapy. Detailed results of each experiment (n = 4) and mean values are given in Table 2 and Table 3, and Figure 3 regarding the air flow rate 15 L/min and 30 L/min, respectively. The air flow rate setting remained unchanged during the nebulization period of 2 min.
Table 2.
Aerosol characteristics of TXA 100 mg/mL, 0.6 mL nebulized at the air flow rate 15 L/min ± 5%; SD = Standard deviation.
Table 3.
Aerosol characteristics of TXA 100 mg/mL, 0.6 mL nebulized at the air flow rate 30 L/min ± 5%; SD = Standard deviation.
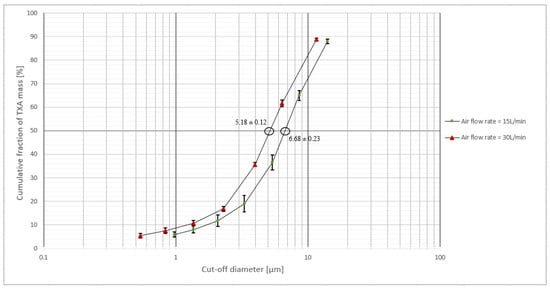
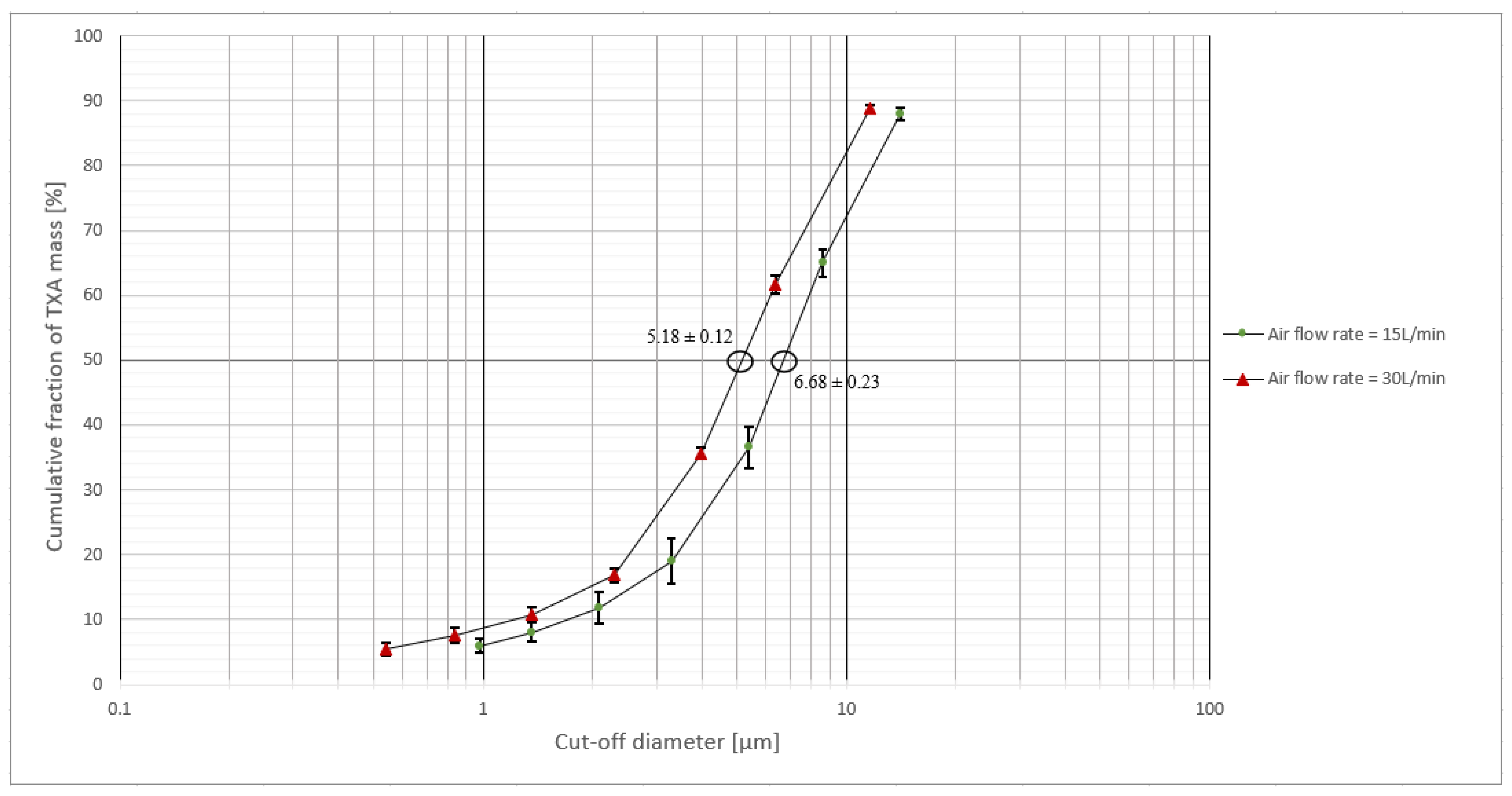
Figure 3.
Mean (n = 4) ± SD cumulative fraction of TXA mass plotted versus the log 10 cut-off diameter of the aerosol particles determined at the air flow rate 15 L/min and 30 L/min. The MMAD (indicated with circles) amounts to 5.18 ± 0.12 at the air flow rate 30 L/min and 6.68 ± 0.23 at the air flow rate 15 L/min.
The MMAD amounted to 6.68 µm at the flowrate 15 L/min and 5.18 µm at 30 L/min corresponding to deposition of the aerosol particles in the middle and upper regions of the lower respiratory tract. The FPF amounted to about 30%, independently from the air flow rate applied. The TXA-FPD amounted to about 16 mg and the GSD to approximately 2 at both air flow rates. Determination of the mass balance revealed TXA recovery rates of 91.83% ± 1.22% and 90.70% ± 3.93% at a flow rate of 15 L/min and 30 L/min, respectively.
4. Discussion
The study was designed to prove the appropriateness of TXA aerosols generated by nebulization to treat hemoptysis. Since data on the nebulization characteristics of TXA solution are not available, we simulated the TXA aerosolization protocol used in our hospital and determined the aerodynamic parameters and deposition pattern. The TXA concentration tested, amounted to 100 mg/mL, thereby corresponding to the concentration most often used in clinical practice [3]. Simulating our current clinical practice, the Aerogen® Solo device was utilized for nebulization. It belongs to a new generation of multi-dose vibrating mesh nebulizers and is a disposable device intended for use in a single patient. This type of nebulizer generates a negligible gas flow of its own and thereby avoiding the unfavorable increase in particle velocity in ventilated patients [12]. While other nebulization methods, e.g., with ultrasonic or jet nebulizers, may result in different aerosol characteristics, evaluating these was beyond the scope of our current study. For example, jet nebulizers are known to be significantly more sensitive to changes in airflow, which can impact aerosol generation and reproducibility. Heating the nebulizer solution can be a cause for concern with ultrasonic nebulizers, whereas vibrating mesh nebulizers cause a negligible increase in temperature. However, chemical stability of aqueous TXA solutions is proven and moderate temperature increases during nebulization do not adversely affect TXA stability and activity.
The aerodynamic assessment of fine particles of the TXA aerosol was performed by cascade impaction with an NGI utilizing the inspiratory air flow rates of 15 L/min and 30 L/min to carry the aerosol during the experiments. The air flow rate of 30 L/min was chosen according to the pharmacopeial specification (Ph. Eur. 2.9.18 [17]), which is the most relevant pharmaceutical regulation of aerosol performance testing in Europe. Of note, the flow rate is recommended for aerosol performance testing of pressurized metered-dose inhalers in combination with the NGI. The air flow rate of 15 L/min was used as specified in relevant national and international norms [18,20] and the applicable USP monograph [18,20,21,22], and because it is commonly used for testing air-jet nebulizers in combination with the NGI. In addition, it has become the established default for many in vitro studies, particularly in the context of spontaneously breathing patients. The use of both flow rates broadens the scope and comparability of our results.
The measured MMAD of 6.7 µm (15 L/min air flow rate) and 5.2 µm (30 L/min air flow rate) for the TXA aerosols were considerably larger than the MMAD specified for albuterol aerosols generated with the Aerogen® Solo following EN 13544-1 (2.90–3.23 µm, flow-rate 15 L/min) [23]. This discrepancy is most likely attributed to the much higher concentration of the TXA solution 100 mg/mL compared to albuterol 5 mg/mL and other typical inhalation solutions of small molecules.
There is a tendency to a lower MMAD and a higher FPF with increasing air flow rates, a fact that has already been observed in other experimental studies [24]. The higher air flow rate (simulating the inspiratory flow rate) leads to increased shear forces at the mesh, which results in the formation of smaller aerosol droplets. Consequently, this leads to a reduction in MMAD and an increase in FPF, which is exactly in line with our experimental findings comparing the 15 L/min and 30 L/min air flow rate. While vibrating mesh nebulizers are generally considered to produce aerosols independently of the air flow rate set, secondary effects such as flow-assisted droplet transport and evaporation can still influence the final particle size distribution in the NGI. In the USP <1601> is given that the CEN Standard indicates 15 L/min as preferred air flow rate “because this value represents a good approximation to the mid-inhalation flow rate achievable by a healthy adult breathing at 500 mL tidal volume” [22]. Generally, flow rates depend on the needs of the individual patient and on the device used for aerosol delivery. In clinical practice, inspiratory flow rates can increase up to 60 L/min and more, e.g., in mechanically ventilated patients. The setup of mechanical ventilation differs substantially from the analytical NGI-based measurement setup. In clinical practice, an individualized adjustment of the air flow rate is necessary, balancing device-specific characteristics (e.g., optimal operating range of the nebulizer), the physicochemical properties of the formulation, and patient-specific factors such as lung function [9]. Therefore, the experimental parameters chosen provide a meaningful and robust basis for further investigations.
In our TXA nebulization experiments, the FPF amounted to 29% (15 L/min) and 35% (30 L/min). When Haghi et al. investigated the characteristics resulting from inhalation of a spray-dried TXA with a dry powder inhaler, the MMAD was 3.3 ± 0.4 µm, the GSD 1.9 ± 0.1, and the FPF 47.0 ± 2.5% [25]. They categorized the particle size distribution as suitable for delivery of TXA to the lung [25]. Our reference to DPI data can only be seen as a rough benchmark. Although dry powder formulations offer advantages in particle control and portability, we used the standard injection solution, as it reflects current clinical practice, where nebulized liquid TXA (100 mg/mL) is routinely used for hemoptysis treatment in the absence of licensed formulations.
Overall, the aerodynamic assessment of the fine particle fraction revealed that the robust, low molecular TXA active substance is suitable for aerosolization. The particle size distribution of the nebulized TXA aerosols indicates optimal deposition in the upper parts of the lower respiratory tract, which coincides with the primary sites of origin for the majority of hemoptysis cases [26,27,28]. The targeted site of action can be reached without a very low MMAD and a very high FPD and FPF are not necessary because TXA does not need to reach the deepest areas of the lungs to be effective. The same assumption might be appropriate for pediatric patients, where otherwise a high fine particle fraction < 3 µm is targeted. These findings are in line with the clinical observation of an effective inhalation therapy with nebulized TXA in hemoptysis. To evaluate the relevance and to set a specification, clinical studies are necessary in order to investigate the pharmacokinetic/pharmacodynamic relationship of nebulized TXA and to determine an optimal TXA dose and concentration for the treatment of hemoptysis.
Limitations
Aerodynamic parameters were obtained by nebulizing TXA 100 mg/mL solution for two minutes by a specified mesh nebulization device typically used in clinical practice. Results cannot be extrapolated to other TXA concentrations and other experimental settings. Different types of nebulizers may produce aerosols with different aerodynamic characteristics [29]. For example, the aerosolization of sodium fluoride with different types of nebulizers resulted in threefold varying MMAD (6.8 µm vs. 2.1 µm) [9,30]. The European Respiratory Society (ERS) also states that when exchanging nebulizers, a variation in the inhaled drug doses of up to ten times must be expected [31]. In the context of mechanical ventilation, the precise positioning of the nebulizer within the ventilation apparatus is also crucial. Variations in the aerosol spectrum may arise depending on the placement of the nebulizer, leading to differences in volume flow, air temperature, and oxygen saturation [32,33].
Optimized aerosol performance was not the primary aim of this investigation. Using two different air flow rates, we observed that the higher air flow rate led to a reduced MMAD and a higher FPF. Thus, increased air flow rates may be a potential strategy to enhance the effectiveness of TXA inhalation. However, whether this would be clinically meaningful or feasible depends on the inhalation technique and individual patient conditions.
This proof-of-concept study focused on the aerodynamic parameters of TXA aerosols and the TXA content of the aerosol particles was determined by titration. This analytical method was chosen according to the pharmacopeia monograph. TXA is a small synthetic molecule that is neither proteinaceous nor formulated by encapsulation. The well-documented physicochemical stability of TXA solutions is neither influenced by heat or shear stress, and degradation during nebulization is not expected [15]. To investigate purity and degradation products of TXA aerosols, an elaborate HPLC analysis would be necessary. Experimental studies to measure the bioavailability of aerosolized TXA were beyond the scope of this proof-of-concept study.
Transfer of in vitro aerosol characteristics to clinical situations is limited by lung anatomy, patient breathing patterns, particle velocity, as well as electrostatic and hygroscopic properties of the aerosol. The TXA formulation tested does not contain sodium chloride or other electrolytes. The ionic properties of TXA itself impart a certain electrical conductivity to the solution, albeit lower than that of sodium chloride solutions. Consequently, we expect limited electrostatic effects during nebulization.
5. Conclusions
Nebulization of TXA 100 mg/mL solution by the Aerogen® Solo nebulizer revealed the aerodynamic characteristics of the resulting TXA aerosol appropriate for deposition in the middle and upper regions of the lower respiratory tract. According to the particulate deposition pattern, and thereby bioavailability, the TXA aerosols are appropriate to treat hemoptysis, which is predominantly located in the bronchial region. Further studies are necessary to investigate optimized doses and concentrations of TXA solutions in combination with appropriate inhalation devices in order to assure effectiveness and the safety of pulmonary TXA administration to treat hemoptysis.
Author Contributions
Conceptualization, I.K.; Formal analysis, G.S.; Investigation, G.S.; Supervision, I.K.; Visualization, G.S.; Writing—original draft, G.S.; Writing—review and editing, F.E., W.K. and I.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed at the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- McCormack, P.L. Tranexamic Acid. Drugs 2012, 72, 585–617. [Google Scholar] [CrossRef] [PubMed]
- Pfizer. Fachinformation Cyklokapron®-Injektionslösung Frankfurt, Germany. 2024. Available online: https://figi.pfizer.de/sites/default/files/FI-8797.pdf (accessed on 20 December 2024).
- Vitug, L.C.G.; Pempengco, M.S.A.; Santiaguel, J.M. Local Pulmonary Administration of Tranexamic Acid as Inhalational or Nebulized for the Control of Hemoptysis. Philipp. J. Chest Dis. 2022, 20, 61–69. [Google Scholar] [CrossRef]
- Wand, O.; Guber, E.; Guber, A.; Epstein Shochet, G.; Israeli-Shani, L.; Shitrit, D. Inhaled Tranexamic Acid for Hemoptysis Treatment: A Randomized Controlled Trial. Chest 2018, 154, 1379–1384. [Google Scholar] [CrossRef]
- Tsai, Y.-S.; Hsu, L.-W.; Wu, M.-S.; Chen, K.-H.; Kang, Y.-N. Effects of Tranexamic Acid on Hemoptysis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Clin. Drug Investig. 2020, 40, 789–797. [Google Scholar] [CrossRef]
- Gadre, A.; Stoller, J.K. Tranexamic Acid for Hemoptysis: A Review. Clin. Pulm. Med. 2017, 24, 69–74. [Google Scholar] [CrossRef]
- Gopinath, B.; Mishra, P.R.; Aggarwal, P.; Nayaka, R.; Naik, S.R.; Kappagantu, V.; Shrimal, P.; Ramaswami, A.; Bhoi, S.; Jamshed, N.; et al. Nebulized vs IV Tranexamic Acid for Hemoptysis: A Pilot Randomized Controlled Trial. Chest 2023, 163, 1176–1184. [Google Scholar] [CrossRef]
- Mahmud, S.; Alam, S.F.; Islam, T. Inhaled Tranexamic Acid: A Therapeutic Option For Hemoptysis. Clin. Pulm. Med. 2019, 26, 170–172. [Google Scholar] [CrossRef]
- Adorni, G.; Seifert, G.; Buttini, F.; Colombo, G.; Stecanella, L.A.; Krämer, I.; Rossi, A. Aerosolization performance of jet nebulizers and biopharmaceutical aspects. Pharmaceutics 2019, 11, 406. [Google Scholar] [CrossRef] [PubMed]
- Heyder, J.; Gebhart, J.; Rudolf, G.; Schiller, C.F.; Stahlhofen, W. Deposition of particles in the human respiratory tract in the size range 0.005–15 μm. J. Aerosol Sci. 1986, 17, 811–825. [Google Scholar] [CrossRef]
- Darquenne, C. Deposition Mechanisms. J. Aerosol Med. Pulm. Drug Deliv. 2020, 33, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.R.; Finlay, W.H. Nebulizers for drug delivery to the lungs. Expert Opin. Drug Deliv. 2015, 12, 889–900. [Google Scholar] [CrossRef]
- Ph. Eur. Monograph 0875 Tranexamic Acid. In European Pharmacopeia; EDQM Council of Europe: Straßbourg, France, 2023; Volume 11.0.
- U.S. Pharmacopeia National Formulary. USP-NF Monograph Tranexamic Acid Injection Electronic Version 2024. Available online: https://online.uspnf.com/uspnf/document/1_GUID-F8721089-4EFC-43A4-845A-781DAF48AEFE_8_en-US?source=Quick%20Search&highlight=tranexamic (accessed on 20 December 2024).
- Loner, C.; Estephan, M.; Davis, H.; Cushman, J.T.; Acquisto, N.M. Effect of fluctuating extreme temperatures on tranexamic acid. Prehosp. Disaster Med. 2019, 34, 340–342. [Google Scholar] [CrossRef]
- Ph. Eur. Monograph 0169 Water for injections. In European Pharmacopeia; EDQM Council of Europe: Straßbourg, France, 2023; Volume 11.0.
- Ph. Eur. Monograph 2.9.18. Preparations for inhalation: Aerodynamic Assessment of Fine Particles. In European Pharmacopeia; EDQM Council of Europe: Straßbourg, France, 2023; Volume 11.0.
- CEN: EN 13544-1:2007 + A1:2009; Respiratory Therapy Equipment: Nebulizing Systems and Their Components. British Standard Institute: London, UK, 2010.
- U.S. Pharmacopeia National Formulary. USP-NF Monograph Tranexamic Acid Electronic Version 2024. Available online: https://online.uspnf.com/uspnf/document/1_GUID-FEC38B38-8DD5-4B5D-B4CA-83865AC39C2B_6_en-US?source=Quick%20Search&highlight=tranexamic (accessed on 20 December 2024).
- Marple, V.A.; Olson, B.A.; Santhanakrishnan, K.; Roberts, D.L.; Mitchell, J.P.; Hudson-Curtis, B.L. Next Generation Pharmaceutical Impactor: A New Impactor for Pharmaceutical Inhaler Testing. Part III. Extension of Archival Calibration to 15 L/min. J. Aerosol Med. 2004, 17, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Arzneibuchkommentar zur, Ph. Eur. 5.2: 2.9.18. Zubereitungen zur Inhalation: Aerodynamische Beurteilung feiner Teilchen. In 2.Verzeichnis aller Texte der 11. Ausgabe; Deutscher Apotheker Verlag: Stuttgart, Germany, 2006; p. 25.
- U.S. Pharmacopeia National Formulary. USP-NF <1601> Products for Nebulization—Characterization Tests Electronic Version 2021. Available online: https://online.uspnf.com/uspnf/document/1_GUID-6A8052DE-3176-4AAA-8293-EE07D28F0CA4_3_en-US?source=Quick%20Search&highlight=1601 (accessed on 20 December 2024).
- Aerogen Ltd. USB Controller System Instruction Manual for Use with Aerogen® Solo and Aerogen® Pro Galway, Ireland 2021. Available online: https://inspiration-medical.de/PDFs/Aeroneb_USB_Manual.pdf (accessed on 20 December 2024).
- Kamin, W.E.; Genz, T.; Roeder, S.; Scheuch, G.; Trammer, T.; Juenemann, R.; Cloes, R.M. Mass output and particle size distribution of glucocorticosteroids emitted from different inhalation devices depending on various inspiratory parameters. J. Aerosol Med. 2002, 15, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Haghi, M.; van den Oetelaar, W.; Moir, L.M.; Zhu, B.; Phillips, G.; Crapper, J.; Young, P.M.; Traini, D. Inhalable tranexamic acid for haemoptysis treatment. Eur. J. Pharm. Biopharm. 2015, 93, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Jean-Baptiste, E. Clinical assessment and management of massive hemoptysis. Crit. Care Med. 2000, 28, 1642–1647. [Google Scholar] [CrossRef]
- Yoon, W.; Kim, J.K.; Kim, Y.H.; Chung, T.W.; Kang, H.K. Bronchial and nonbronchial systemic artery embolization for life-threatening hemoptysis: A comprehensive review. Radiographics 2002, 22, 1395–1409. [Google Scholar] [CrossRef]
- Ittrich, H.; Bockhorn, M.; Klose, H.; Simon, M. Diagnostik und Therapie der Hämoptysen. Dtsch. Ärzteblatt Int. 2017, 114, 371–381. [Google Scholar] [CrossRef]
- Hardy, J.; Newman, S.; Knoch, M. Lung deposition from four nebulizers. Respir. Med. 1993, 87, 461–465. [Google Scholar] [CrossRef]
- Seifert, G.; Krämer, I.; Rossi, A.; Kamin, W. Vergleichende Untersuchung von aktuell in Deutschland vermarkteten Druckluftverneblern und den damit erzeugten Aerosolen. Krankenhauspharmazie 2019, 40, 241–249. [Google Scholar]
- Boe, J.; Dennis, J.H.; O’Driscoll, B.R.; Bauer, T.T.; Carone, M.; Dautzenberg, B.; Diot, P.; Heslop, K.; Lannefors, L. European Respiratory Society Guidelines on the use of nebulizers. Eur. Respir. J. 2001, 18, 228–242. [Google Scholar] [CrossRef] [PubMed]
- Arzu, A.; Orcin Telli, A.; Robert, H.; Meryl, M.S.; Essam, A.A.; James, B.F. Influence of Nebulizer Type, Position, and Bias Flow on Aerosol Drug Delivery in Simulated Pediatric and Adult Lung Models During Mechanical Ventilation. Respir. Care 2010, 55, 845. Available online: http://rc.rcjournal.com/content/55/7/845.abstract (accessed on 10 January 2025).
- Hou, H.; Xu, D.; Dai, B.; Zhao, H.; Wang, W.; Kang, J.; Tan, W. Position of different nebulizer types for aerosol delivery in an adult model of mechanical ventilation. Front. Med. 2022, 9, 950569. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).