Abstract
Background: Patients presenting to the Emergency Department (ED) with amphetamine-type stimulant (ATS) use can exhibit a wide range of symptoms, ranging from mild agitation to life-threatening dysrhythmias. Early identification of patients at risk for more severe medical complications after ATS use is a key challenge in emergency care. Objective: To identify clinical and demographic predictors associated with a medical condition among patients presenting to the ED after ATS use. Methods: Retrospective cohort study of patients who presented to the ED with suspected ATS use at a large academic community hospital in Ontario from 1 September 2016 to 31 August 2017. Patients were screened using ICD-10 codes and included if they had a positive drug screen and clinical suspicion for ATS use. Our primary outcome was a composite of recognized complications of ATS toxicity. Predictor variables included age, sex, employment status, mental illness or substance use history, ED administration of benzodiazepines, antipsychotics, or physical restraints. Multivariable logistic regression was used to assess associations. Results: Of 1591 charts reviewed, 128 (8%) met the inclusion criteria. The median age was 29.5 years (interquartile range [IQR]: 23–36), and 50.8% were female. In adjusted analyses, benzodiazepine administration was significantly associated with a medical condition (Odds Ratio [OR] 3.33; 95% CI: 1.31–8.45; p = 0.011) as was employment status (OR 9.30; 95% CI: 1.00–86.03; p = 0.019). Conclusions: Benzodiazepine administration and unemployment were strong predictors of a medical condition among patients presenting to the ED after ATS use. These patients should undergo thorough physical examination and diagnostic testing to identify and manage potentially life-threatening conditions.
1. Introduction
Amphetamine-type stimulants (ATS), including methamphetamine and amphetamine, are among the most commonly misused stimulants worldwide [1]. In 2021, an estimated 36 million people globally reported stimulant use, representing approximately 0.7% of the global population [1]. As use has increased, so too has the burden on emergency health services. In Ontario, Canada, amphetamine-related emergency department (ED) visits increased 15-fold between 2003 and 2020 [2]. Similarly, a recent California-based study found that stimulant-related presentations rose from 2064 to 2586 per 100,000 ED visits between 2017 and 2021 [3].
In the ED, patients presenting after ATS use pose significant challenges to healthcare providers. Many arrive in a state of acute agitation or psychosis, often requiring physical or chemical restraint, which can hinder accurate history-taking and physical examination. As a result, ED providers may rely on clinical gestalt to determine whether further diagnostic workup, such as laboratory tests, electrocardiography (ECG) monitoring, or observation, is necessary. Although the majority of amphetamine-related ED presentations resolve with minimal intervention, a significant subset develops medical complications, owing to the sympathomimetic effects of ATS use. These can range from rhabdomyolysis due to severe agitation, hyperthermia and excessive muscle activity, to end-organ ischemia secondary to vasoconstriction and poor tissue perfusion—resulting in acute kidney injury (AKI) and myocardial ischemia—and, finally, to ventricular dysrhythmias driven by an increase in circulating catecholamines and cardiac potassium channel effects [4,5,6]. These conditions can be life-threatening, especially if unrecognized. Timely identification of such complications is often difficult, and currently, there is little evidence to provide risk stratification for this population.
Understanding whether clinical or demographic features predict the presence of a medical condition among those presenting after ATS use could assist ED providers in determining which patients warrant further investigation, yet it is poorly understood. Therefore, we performed a retrospective cohort study to identify predictors of a medical condition among patients presenting to the ED following ATS use.
2. Materials and Methods
2.1. Study Design and Participants
We performed a retrospective cohort study of patients who presented to the emergency department (ED) after ATS use at Sault Area Hospital (SAH), a large academic community hospital, between 1 September 2016 and 31 August 2017. The facility is a 289-bed hospital in Northern Ontario, serving a catchment area of 115,000 people and receives approximately 55,000 to 60,000 ED visits each year. The study received Research Ethics Board (REB) approval by the joint Sault Area Hospital/Group Health Centre REB (REB 2017-12-02).
Using Sault Area Hospital databases, a broad search strategy was undertaken to generate a cohort of patients with ED visits related to amphetamine-type stimulant (ATS) use. This was performed using the International Statistical Classification of Diseases, version 10 (ICD-10) codes identifying ATS use, used in previous studies, as well as codes where ATS use might conceivably be found (Supplementary Materials, Table S1) for overdoses, mental health diagnostic codes (e.g., anxiety disorders) and other substance use disorders (e.g., alcohol, cocaine, opiates) [7]. Patients were then included in the study if the primary reason for their emergency department visit was due to ATS use, determined by a combination of documented final diagnosis in the written chart, history of presenting illness describing current ATS use and urine drug screen positive for either amphetamine or methamphetamine if performed. Patients were excluded if they did not meet these criteria.
2.2. Outcome Measures
The primary outcome measure was a composite outcome of important complications of ATS use. These were selected a priori by the team based on clinical importance and review of the literature. The secondary outcome of this study was admission to the hospital at the conclusion of the emergency department visit.
2.3. Data Analysis
Patient characteristics were described using descriptive statistics: data were inspected and summarized graphically using means and standard deviations for continuous variables, and counts and proportions for categorical variables. This included patient age, sex and employment status; the patient’s history of primary substance use and intravenous drug use; history of a mental health disorder; the use of benzodiazepines (all administration routes), antipsychotics (all administration routes) and physical restraints in the emergency department; and whether the patient was readmitted within seven days of their initial emergency department visit.
Next, these variables were used as potential predictors in a logistic regression model of the primary outcome. Using guidelines proposed by Harrell et al. (1996), a predictive model was constructed for the primary outcome [8]. Univariate logistic regression was used to obtain unadjusted Odds Ratios and their associated 95% confidence intervals, as well as p-values. Each predictor from the univariable analysis was then included in a multivariable logistic regression model, and the c-index was calculated for the multivariable model. The c-index is defined as the area under the receiver operating characteristic curve and estimates the probability of concordance between predicted and observed responses (i.e., how well the model discriminates between patients with the outcome and patients without it) [9]. A c-index of 0.50 would indicate that a model has no more than a random chance of predicting an outcome correctly [9].
For the secondary outcome of hospital admission, a multivariable logistic regression model was constructed, and the same predictors as in the primary outcome analysis, along with medical complications included as additional predictors for this analysis. The c-index for this model was again calculated.
All analyses were performed using the JMP version 13.2.1 (Cary, NC, USA). All statistical analyses were conducted with a two-tailed alpha set to 0.05.
3. Results
Using the broad list of ICD-10 codes, 1591 potential patient visits were identified, and, ultimately, 128 (8%) patients met the inclusion criteria (Figure 1). The median age was 29.5 years (interquartile range [IQR]: 23–36), 50.8% were female and most (96%) were unemployed (Table 1). Further, many patients had a history of substance use (95.3%) as well as a history of mental illness (76.6%) (Table 1). The most commonly identified medical complication was tachydysrhythmia (26.3%), followed by cellulitis (12.3%) and elevated serum creatinine (12.3%) (Table 2). In adjusted analyses, benzodiazepine administration was significantly associated with a medical condition (Odds Ratio [OR] 3.33; 95% CI: 1.31–8.45; p = 0.011) as was employment status (OR 9.30; 95% CI: 1.00–86.03; p = 0.019) (Table 1). There were no differences in re-presentation to the emergency department within 7 days between individuals with a medical complication and those who did not have a medical complication.
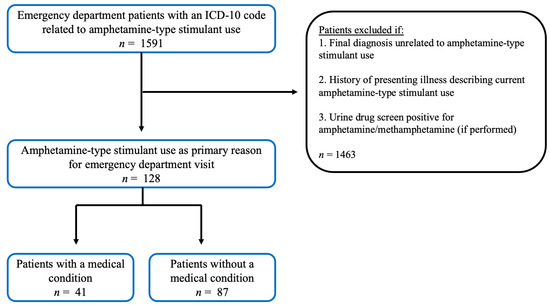
Figure 1.
Flow diagram illustrating patient inclusion criteria used to generate the cohort of patients with emergency department visits related to amphetamine-type stimulant use.

Table 1.
Univariable and multivariable results of the primary outcome: predictors of medical complications.
Table 2.
Medical complications with respective definition and frequency among those who developed a medical issue * (n = 41).
Results of multivariable analysis were similar to univariable analysis (Table 1), although employment status and benzodiazepine use in the emergency department were stronger predictors of medical complications after accounting for the other predictors in the multivariable logistic regression model. Overall, the model had fair predictive ability for medical complications, with a c-index of 0.75.
With respect to the secondary outcome of hospital admission, the presence of any medical complication was the only statistically significant predictor of admission after accounting for the other predictors in the multivariable logistic regression model (OR 3.16; 95% CI 1.02 to 9.74; p = 0.0452). Overall, this model had good predictive ability for hospital admission, with a c-index of 0.86.
4. Discussion
We found that patients presenting to the emergency department (ED) after amphetamine-type stimulant (ATS) use had more than a three-fold increase in the odds of having a medical condition when administered a benzodiazepine. Employment status was also associated with increased odds of a medical complication, and patients with a medical complication were more likely to be admitted. While previous studies have focused on the rising frequency of ATS-related ED visits and hospitalization across North America, or on predictors of mortality in non-ED populations, this is, to our knowledge, the first study to examine predictors of medical complications in this specific ED population [1,2,3,10].
In the absence of validated clinical decision pathways, ED clinicians often rely on gestalt to determine which patients require investigations or observation, which can lead to under- or over-investigation [11,12]. Our findings suggest that benzodiazepine administration may serve as a clinical “red flag” in patients presenting with ATS use, prompting a lower threshold for investigation. Although not previously studied in this context, it is plausible that patients requiring sedation represent cases of more severe intoxication, in keeping with the known dose–response relationship of ATS use [13]. Accordingly, patients who require benzodiazepines in the ED should undergo a workup for known complications of ATS use, including laboratory investigations, electrocardiography, serial assessments and consideration for extended observation.
Unexpectedly, we found that employment was associated with a higher odds of a medical condition. While counterintuitive, employment status often serves as a proxy for socioeconomic status, which may influence care-seeking behavior and provider decision-making [14]. Employed patients may appear more cooperative, leading to more thorough assessment and increased detection of complications. However, given the small number of employed patients in our cohort and the wide confidence interval, this finding should be interpreted cautiously and validated in larger studies. Unsurprisingly, patients with medical complications were significantly more likely to be admitted. This reinforces the importance of early detection, as disposition decisions hinge on the identification of an underlying medical issue. Our model had a high predictive ability of admission, with a c-index over 0.80, which compares favorably with other widely used ED decision tools such as CHADS-VASc (c-index 0.68) [15].
Similar patterns have been reported internationally. In an Australian ED cohort, methamphetamine-related presentations frequently required chemical sedation and were complicated by rhabdomyolysis and acute kidney injury complications, which were included as part of our composite outcome [16]. A Spanish series of ATS poisonings likewise described high rates of agitation, psychosis, tachycardia and hypertension, with many patients requiring sedation and a substantial proportion being admitted, although specific sedatives administered were not reported [17]. While no studies have directly examined predictors of medical complications among ED patients with ATS use, related research in broader overdose populations has identified predictors of cardiac toxicity, including QTC prolongation, metabolic acidosis and a history of cardiac disease [18]. Cardiac toxicity is a major concern in ATS overdose, and QTc prolongation was therefore included as one of the medical complications in our composite outcome, along with a number of other cardiac markers. However, because of our modest sample size and the use of a composite outcome, we were unable to assess the predictive value of individual components. Notably, no prior ATS studies have evaluated demographic predictors such as employment status. Future studies should focus on validating these findings using larger, multicenter datasets and on developing clinical decision tools to estimate the risk of adverse medical outcomes in this population. Additionally, exploring longitudinal outcomes such as 30-day morbidity or mortality would be important.
Limitations of our study include a lower-than-expected sample size, which limited event rates and constrained the number of potential predictor variables included in our model. Further, chart abstraction was not performed by a second reviewer and composite outcome measures were used, driven by less serious and more frequent components of that outcome. Finally, the single-center nature of our study limits generalizability. Nonetheless, our model still demonstrated fair predictive ability to identify patients with a medical condition after ATS use.
5. Conclusions
In conclusion, we identified benzodiazepine administration during ED visits for ATS use as a significant and novel predictor of medical complications. This readily observable clinical feature may help guide assessment and management decisions. Our findings provide a foundation for the development of future risk-stratification tools to enhance the safety and efficiency of emergency care for this growing and high-risk patient population.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/ecm2040057/s1, Table S1: Amphetamine-type stimulant (ATS) and related diagnostic codes.
Author Contributions
This manuscript was a collaborative effort involving all authors equally. Conceptualization, J.T.K., S.S. and L.A.F.; methodology, J.T.K., S.S. and L.A.F.; software, J.T.K., S.S. and L.A.F.; validation, J.T.K., S.S. and L.A.F.; formal analysis, J.T.K., S.S. and L.A.F.; investigation, J.T.K., S.S. and L.A.F.; resources, J.T.K., S.S. and L.A.F.; data curation, J.T.K., S.S. and L.A.F.; writing—original draft preparation, J.T.K., S.S. and L.A.F.; writing—review and editing, J.T.K., S.S. and L.A.F.; visualization, J.T.K., S.S. and L.A.F.; supervision, J.T.K., S.S. and L.A.F.; project administration, J.T.K., S.S. and L.A.F.; funding acquisition, J.T.K., S.S. and L.A.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded through a Micro Grant (<5000), awarded on behalf of the Sault Ste. Marie Academic Medical Association (SSMAMA).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the joint Sault Area Hospital and Group Health Centre Research Ethics Board (approval code: REB2017-12-02; approval date: 1 December 2017).
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study, as approved by the institutional REB.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
The authors would like to acknowledge and offer thanks to Clare Atzema for feedback on earlier versions of the manuscript.
Conflicts of Interest
The authors have no disclosures or conflicts of interest to declare. SSMAMA had no part in the study design, conducting the study or data analysis, and did not have any authority over these activities.
References
- United Nations Office on Drugs and Crime (UNODC). World Drug Report 2023. 2023. Available online: https://www.unodc.org/unodc/en/data-and-analysis/world-drug-report-2023.html (accessed on 20 September 2025).
- Crispo, J.A.G.; Liu, L.; Bach, P.; Ansell, D.R.; Sivapathasundaram, B.; Nguyen, F.; Kurdyak, P.; Seitz, D.P.; Conlon, M.; Cragg, J.J. Amphetamine-related emergency department visits in Ontario, Canada, 2003–2020. Can. J. Psychiatry 2023, 68, 838–849. [Google Scholar] [CrossRef] [PubMed]
- Han, B.H.; Brennan, J.J.; Kepner, W.E.; Chen, S.; Lin, S.; Carley, J.A.; Larson, J.; Castillo, E.M. Trends in stimulant-related emergency department visits among adults in California, 2017–2021. Am. J. Emerg. Med. 2025, 93, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Winkelman, T.N.A.; Admon, L.K.; Jennings, L.; Shippee, N.D.; Richardson, C.R.; Bart, G. Evaluation of amphetamine-related hospitalizations and associated clinical outcomes and costs in the United States. JAMA Netw. Open 2018, 1, e183758. [Google Scholar] [CrossRef] [PubMed]
- Vasan, S.; Murray, B.P.; Olango, G.J. Amphetamine Toxicity. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2025. Available online: https://www.ncbi.nlm.nih.gov/books/NBK470276/ (accessed on 20 September 2025).
- Dominic, P.; Ahmad, J.; Awwab, H.; Bhuiyan, S.; Kevil, C.G.; Goeders, N.E.; Murnane, K.S.; Patterson, J.C.; Sandau, K.E.; Olshansky, B.; et al. Stimulant drugs of abuse and cardiac arrhythmias. Circ. Arrhythm. Electrophysiol. 2022, 15, e010273. [Google Scholar] [CrossRef] [PubMed]
- Shearer, R.D.; Shippee, N.D.; Winkelman, T.N.A. Characterizing trends in methamphetamine-related health care use when there is no ICD code for “methamphetamine use disorder”. J. Subst. Abuse Treat. 2021, 127, 108369. [Google Scholar] [CrossRef] [PubMed]
- Harrell, F.E., Jr.; Lee, K.L.; Mark, D.B. Multivariable prognostic models: Issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat. Med. 1996, 15, 361–387. [Google Scholar] [CrossRef]
- Uno, H.; Cai, T.; Pencina, M.; D’Agostino, R.; Wei, L. On the C-statistics for evaluating overall adequacy of risk prediction procedures with censored survival data. Stat. Med. 2011, 30, 1105–1117. [Google Scholar] [CrossRef] [PubMed]
- Åhman, A.; Karlsson, A.; Berge, J.; Håkansson, A. Mortality, morbidity, and predictors of death among amphetamine-type stimulant users—A longitudinal, nationwide register study. Addict. Behav. Rep. 2024, 19, 100553. [Google Scholar] [CrossRef] [PubMed]
- Pandey, S.R.; Knack, S.K.S.; Driver, B.E.; Prekker, M.E.; Scott, N.; Ringstrom, S.J.; Maruggi, E.; Kaus, O.; Tordsen, W.; Puskarich, M.A.; et al. Factors and outcomes associated with under- and overdiagnosis of sepsis in the first hour of emergency department care. Acad. Emerg. Med. 2025, 32, 204–215. [Google Scholar] [CrossRef] [PubMed]
- Cervellin, G.; Borghi, L.; Lippi, G. Do clinicians decide relying primarily on Bayesian principles or on Gestalt perception? Some pearls and pitfalls of Gestalt perception in medicine. Intern. Emerg. Med. 2014, 9, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Logan, B.K. Methamphetamine and driving impairment. J. Forensic Sci. 1996, 41, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Clough, A.R.; Robertson, J.; Fitts, M.S.; Lawson, K.; Bird, K.; Hunter, E.; Gynther, B.; Obrecht, K. Impacts of Methamphetamine, Other Drugs and Alcohol in Rural and Remote Areas in Northern and North-East Queensland: An Environmental Scan; James Cook University: Cairns, QLD, Australia, 2015; Available online: http://www.healthinfonet.ecu.edu.au/uploads/resources/30834_30834.pdf (accessed on 20 September 2025).
- van den Ham, H.A.; Klungel, O.H.; Singer, D.E.; Leufkens, H.G.M.; van Staa, T.P. Comparative performance of ATRIA, CHADS2, and CHA2DS2-VASc risk scores predicting stroke in patients with atrial fibrillation: Results from a national primary care database. J. Am. Coll. Cardiol. 2015, 66, 1851–1859. [Google Scholar] [CrossRef] [PubMed]
- Isoardi, K.Z.; Ayles, S.F.; Harris, K.; Finch, C.J.; Page, C.B. Methamphetamine presentations to an emergency department: Management and complications. Emerg. Med. Australas. 2019, 31, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Roset Ferrer, C.; Gomila Muñiz, I.; Elorza Guerrero, M.A.; Puiguriguer Ferrando, J.; Leciñena Estean, M.Á.; Tuero León, G.; Sahuquillo Frias, L.; Ripoll Vera, T.; Socias Crespi, L.; Sanchis Cortes, P.; et al. Amphetamine and methamphetamine poisonings attended in hospital emergency departments: Clinical features and the usefulness of laboratory confirmation. Emergencias 2020, 32, 26–32. [Google Scholar] [PubMed]
- Manini, A.F.; Hoffman, R.S.; Stimmel, B.; Vlahov, D. Clinical risk factors for in-hospital adverse cardiovascular events after acute drug overdose. Acad. Emerg. Med. 2015, 22, 499–507. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).