
Performance of the InfraScanner for the Detection of Intracranial Bleeding in a Population of Traumatic Brain Injury Patients in Colombia

 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
- An instructional video explaining the operation of the device was shown to eligible patients or their legal representatives, and the objectives and procedures of the study were explained to obtain informed consent.
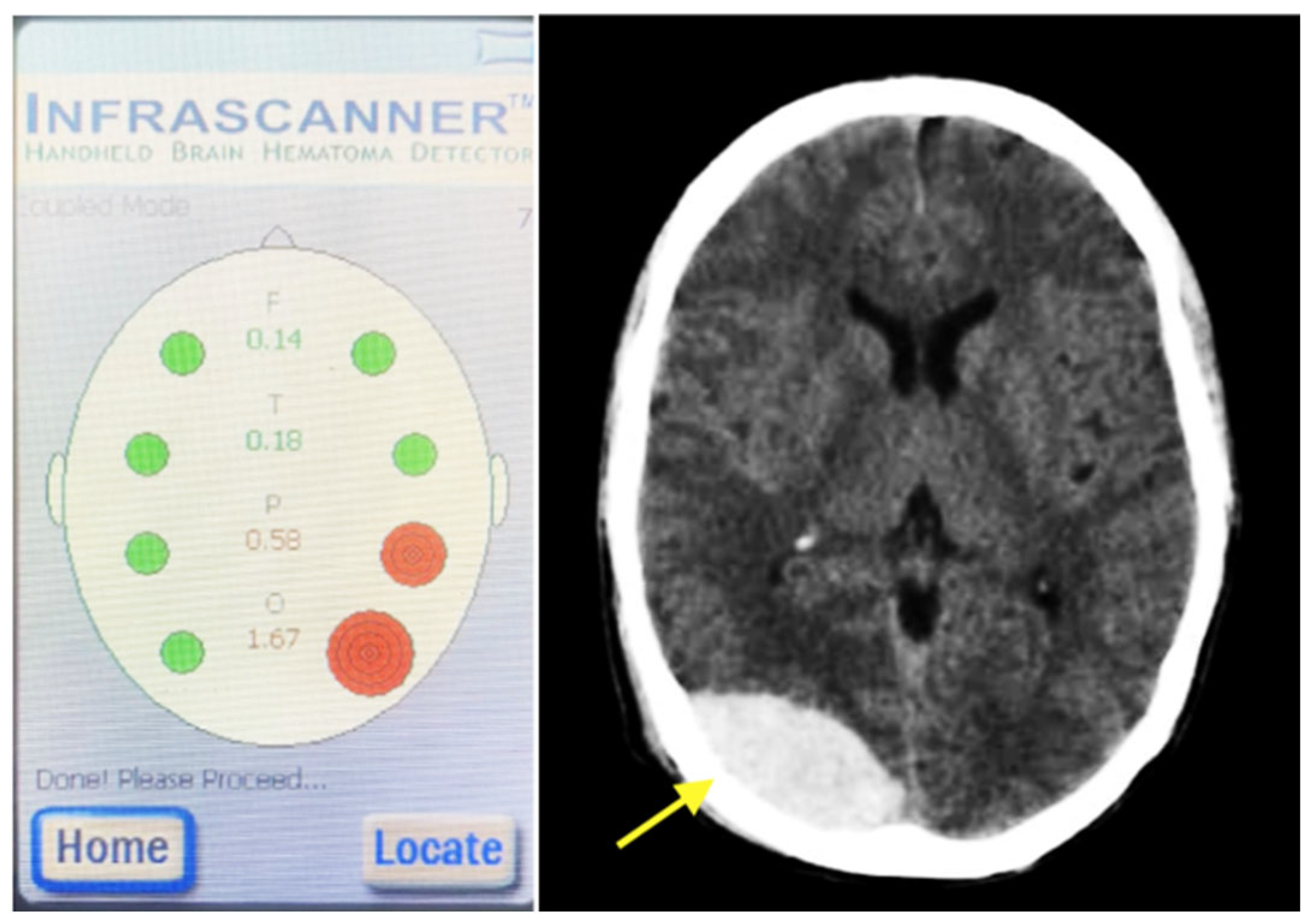
- NIRS measurements were performed in the emergency department according to the device’s user manual, and the resulting data were recorded (Figure 2).
- A non-contrast head CT scan was obtained for all participants and independently reviewed by a trauma neurosurgeon who was blinded to the NIRS results.
- All data were securely stored in a restricted-access database available only to the study investigators. The data collection instrument and measured variables are presented in Table 1.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dewan, M.C.; Rattani, A.; Gupta, S.; Baticulon, R.E.; Hung, Y.-C.; Punchak, M.; Agrawal, A.; Adeleye, A.O.; Shrime, M.G.; Rubiano, A.M.; et al. Estimating the global incidence of traumatic brain injury. J. Neurosurg. 2019, 130, 1080–1097. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Barber, R.M.; Bell, B.; Bertozzi-Villa, A.; Biryukov, S.; Bolliger, I.; Charlson, F.; Davis, A.; Degenhardt, L.; Dicker, D.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [Google Scholar] [CrossRef] [PubMed]
- Mowafi, H.; Ngaruiya, C.; O’Reilly, G.; Kobusingye, O.; Kapil, V.; Rubiano, A.M.; Ong, M.; Puyana, J.C.; Rahman, A.F.; Jooma, R.; et al. Emergency care surveillance and emergency care registries in low-income and middle-income countries: Conceptual challenges and future directions for research. BMJ Glob. Health 2019, 4 (Suppl. 6), e001442. [Google Scholar] [CrossRef] [PubMed]
- Norton, R.; Kobusingye, O. Injuries. N. Engl. J. Med. 2013, 368, 1723–1730. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.Y.; Lee, A.Y.W. Traumatic Brain Injuries: Pathophysiology and Potential Therapeutic Targets. Front. Cell. Neurosci. 2019, 13, 528. [Google Scholar] [CrossRef] [PubMed]
- Khan, Z.; Sharafat, S.; Ali, H.; Khan, A.; Noushad, A.; Farman, J.; Sajjad, M. Assessing the Impact of Pre-surgical Delay on Extradural Hematoma Outcomes. Cureus. 18 February 2025. Available online: https://www.cureus.com/articles/332714-assessing-the-impact-of-pre-surgical-delay-on-extradural-hematoma-outcomes (accessed on 2 July 2025).
- Merakis, M.; Lewis, D.P.; Weaver, N.; Balogh, Z.J. Time from injury to operative intervention in traumatic intracranial hematoma: A systematic literature review and meta-analysis. World J. Surg. 2024, 48, 2273–2282. [Google Scholar] [CrossRef] [PubMed]
- Leon-Carrion, J.; Dominguez-Roldan, J.M.; Leon-Dominguez, U.; Murillo-Cabezas, F. The Infrascanner, a handheld device for screening in situ for the presence of brain haematomas. Brain Inj. 2010, 24, 1193–1201. [Google Scholar] [CrossRef] [PubMed]
- Robertson, C.S.; Zager, E.L.; Narayan, R.K.; Handly, N.; Sharma, A.; Hanley, D.F.; Garza, H.; Maloney-Wilensky, E.; Plaum, J.M.; Koenig, C.H.; et al. Clinical Evaluation of a Portable Near-Infrared Device for Detection of Traumatic Intracranial Hematomas. J. Neurotrauma 2010, 27, 1597–1604. [Google Scholar] [CrossRef] [PubMed]
- Robertson, C.S.; Gopinath, S.; Chance, B. Use of Near Infrared Spectroscopy to Identify Traumatic Intracranial Hematomas. J. Biomed. Opt. 1997, 2, 31–42. [Google Scholar] [CrossRef] [PubMed]
- The World Bank. World Bank Country and Lending Groups. Report No.: World Bank Country and Lending Groups Country Classification. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-%20253%20and-lending-groups (accessed on 9 January 2025).
- Instituto Nacional de Medicina Legal y Ciencias Forenses. Forensis. 2018. Available online: https://www.medicinalegal.gov.co/documents/20143/386932/Forensis+2018.pdf (accessed on 9 January 2025).
- Xu, L.; Tao, X.; Liu, W.; Li, Y.; Ma, J.; Lu, T.; Han, B.; Liu, B.; Zhao, Y.; Li, J.; et al. Portable near-infrared rapid detection of intracranial hemorrhage in Chinese population. J. Clin. Neurosci. 2017, 40, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Kisat, M.; Zafar, S.N.; Latif, A.; Villegas, C.V.; Efron, D.T.; Stevens, K.A.; Haut, E.R.; Schneider, E.B.; Zafar, H.; Haider, A.H. Predictors of Positive Head CT Scan and Neurosurgical Procedures After Minor Head Trauma. J. Surg. Res. 2012, 173, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Ibañez, J.; Arikan, F.; Pedraza, S.; Sánchez, E.; Poca, M.A.; Rodriguez, D.; Rubio, E. Reliability of clinical guidelines in the detection of patients at risk following mild head injury: Results of a prospective study. J. Neurosurg. 2004, 100, 825–834. [Google Scholar] [CrossRef] [PubMed]
- Stiell, I.G.; Wells, G.A.; Vandemheen, K.; Clement, C.; Lesiuk, H.; Laupacis, A.; McKnight, R.D.; Verbeek, R.; Brison, R.; Cass, D.; et al. The Canadian CT Head Rule for patients with minor head injury. Lancet 2001, 357, 1391–1396. [Google Scholar] [CrossRef] [PubMed]
- Liang, C.-Y.; Yang, Y.; Shen, C.-S.; Wang, H.-J.; Liu, N.-M.; Wang, Z.-W.; Zhu, F.-L.; Xu, R.-X. Chinese Military Evaluation of a Portable Near-Infrared Detector of Traumatic Intracranial Hematomas. Mil. Med. 2018, 183, e318-23. [Google Scholar] [CrossRef] [PubMed]
- Kontojannis, V.; Hostettler, I.; Brogan, R.J.; Raza, M.; Harper-Payne, A.; Kareem, H.; Boutelle, M.; Wilson, M. Detection of intracranial hematomas in the emergency department using near infrared spectroscopy. Brain Inj. 2019, 33, 875–883. [Google Scholar] [CrossRef] [PubMed]
- Francis, S.V.; Ravindran, G.; Visvanathan, K.; Ganapathy, K. Screening for unilateral intracranial abnormalities using near infrared spectroscopy. A preliminary report. J. Clin. Neurosci. 2005, 12, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Kahraman, S.; Kayali, H.; Atabey, C.; Acar, F.; Gocmen, S. The Accuracy of Near-Infrared Spectroscopy in Detection of Subdural and Epidural Hematomas. J. Trauma 2006, 61, 1480–1483. [Google Scholar] [CrossRef] [PubMed]
- Chance, B.; Gopinath, S.P.; Robertson, C.S.; Grossman, R.G. Near-infrared spectroscopic localization of intracranial hematomas. J. Neurosurg. 1993, 79, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Hennes, H.-J.; Lott, C.; Windirsch, M.; Hanley, D.F.; Boor, S.; Brambrink, A.; Dick, W.; Benaron, D.A.; Chance, B.; Ferrari, M. Noninvasive detection of intracerebral hemorrhage using near-infrared spectroscopy (NIRS). Photon Propag. Tissues III 1997, 3194, 42–54. [Google Scholar]
- Kessel, B.; Jeroukhimov, I.; Ashkenazi, I.; Khashan, T.; Oren, M.; Haspel, J.; Medvedev, M.; Nesterenko, V.; Halevy, A.; Alfici, R. Early detection of life-threatening intracranial haemorrhage using a portable near-infrared spectroscopy device. Injury 2007, 38, 1065–1068. [Google Scholar] [CrossRef] [PubMed]
- Ghalenoui, H.; Saidi, H.; Azar, M.; Yahyavi, S.T.; Razavi, H.B.; Khalatbari, M. Near-Infrared Laser Spectroscopy as a Screening Tool for Detecting Hematoma in Patients with Head Trauma. Prehospital Disaster Med. 2008, 23, 558–561. [Google Scholar] [CrossRef] [PubMed]
- Coskun, F.; Sezer, E.A.; Karamercan, M.A.; Akinci, E.; Vural, K. An assessment on the use of infrascanner for the diagnosis of the brain hemotoma by using support vector machine. Sci. Res. Essays 2010, 5, 1911–1915. [Google Scholar]
- Akyol, P.Y.; Bayram, B.; Acerer, A.; Girgin, M.C.; Yılmaz, D.Ç.; Men, S.; Atilla, R. Comparison of near-infrared spectroscopy and head CT interpretations of the ED patients with minor head injury. Am. J. Emerg. Med. 2016, 34, 1364–1368. [Google Scholar] [CrossRef] [PubMed]
- Peters, J.; Van Wageningen, B.; Hoogerwerf, N.; Tan, E. Near-Infrared Spectroscopy: A Promising Prehospital Tool for Management of Traumatic Brain Injury. Prehospital Disaster Med. 2017, 32, 414–418. [Google Scholar] [CrossRef] [PubMed]
- Trehan, V.; Maheshwari, V.; Kulkarni, S.; Kapoor, S.; Gupta, A. Evaluation of near infrared spectroscopy as screening tool for detecting intracranial hematomas in patients with traumatic brain injury. Med. J. Armed Forces India 2018, 74, 139–142. [Google Scholar] [CrossRef] [PubMed]
- Yuksen, C.; Sricharoen, P.; Puengsamran, N.; Saksobhavivat, N.; Sittichanbuncha, Y.; Sawanyawisuth, K. Diagnostic properties of a portable near-infrared spectroscopy to detect intracranial hematoma in traumatic brain injury patients. Eur. J. Radiol. Open 2020, 7, 100246. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (n = 140) | |
|---|---|---|
| Age | n (%) | Population Mean (μ) |
| 18–39 years | 89 (63.57) | 28 |
| 40–59 years | 27 (19.28) | 49 |
| 60–79 years | 19 (13.57) | 67 |
| >80 years | 4 (3.85) | 84 |
| No data | 1 (0.71) | 1 |
| Gender | ||
| Female | 47 (33.57%) | |
| Male | 93 (66.42%) | |
| Hair type | ||
| Straight | 70 (50) | |
| Curly | 59 (42) | |
| Wavy | 5 (4) | |
| No hair | 6 (4) | |
| Hair color | ||
| Black | 93 (66) | |
| Blond | 15 (11) | |
| White | 18 (13) | |
| Brown | 7 (5) | |
| Other | 1(1) | |
| No hair | 6 (4) | |
| Length | ||
| Short | 78 (56) | |
| Medium | 32 (23) | |
| Long | 24 (17) | |
| No hair | 6 (4) | |
| GCS (patients with positive CT scan) | ||
| 14–15 (mild TBI) | 9 (60) | |
| 9–13 (moderate TBI) | 4 (26.6) | |
| ≤8 (severe TBI) | 2 (13.3) |
| Positive CT Scan | Negative CT Scan | Total | |
|---|---|---|---|
| Positive InfraScanner test | 9 | 27 | 36 |
| Negative InfraScanner test | 6 | 98 | 104 |
| Marginal totals | 15 | 125 | 140 |
| Variable | Value | CI 95% |
|---|---|---|
| Sensitivity | 60.00% | 35.20–84.8 |
| Specificity | 78.40% | 71.19–85.61 |
| PPV | 25.00% | 10.85–39.15 |
| NPV | 94.23% | 89.75–98.71 |
| LR+ | 2.73 | 1.63–4.73 |
| LR− | 0.51 | 0.27–0.95 |
| Prevalence | 0.1071 | - |
| Pre-test Prob. | 0.1071 | - |
| Odds pre-test | 0.1199 | - |
| Odds post-test (+) | 0.3273 | - |
| Post-test probability (+) | 0.2466 | 16–36% |
| Odds post-test (−) | 0.0611 | - |
| Post-test probability (−) | 0.0576 | 3–10% |
| InfraScanner Results | CT-Scan | GCS | ||||||
|---|---|---|---|---|---|---|---|---|
| Result | Location (Positive Side) | Subgaleal | Result | Type(s) of Intracranial Hemorrhage | Location | Volume of Bleeding | Depth of Bleeding | |
| Positive | Parietal (L) | No | Positive | tSAH | Temporal (R) | N/A | 1.4 | 8 |
| Temporal (L) | N/A | 2.3 | ||||||
| Positive | Frontal (R) and temporal (R) | Frontal (R) and temporal (R) | Positive | EDH | Temporal–Parietal–Occipital (R) | 9 | 1.6 | 15 |
| Parietal–Occipital (L) | 1.8 | 1.2 | ||||||
| Positive | Frontal (R) | Frontal (R) + frontal (R) fracture | Positive | IPH | Frontal–Temporal (R) | N/A | 1.5 | 15 |
| Positive | Temporal (L) | No | Positive | tSAH | Temporal (L) | N/A | 1.4 | 15 |
| Positive | Frontal (L) | Parietal (R) | Positive | Subdural | Temporal–parietal–Occipital (L) | 0.9 | 1.4 | 14 |
| Contusion | Temporal–Parietal(L) | N/A | 1.1 | |||||
| Positive | Parietal and occipital (L) | No | Positive | tSAH | Temporal (L) | N/A | 2.5 | 15 |
| Positive | Temporal and Parietal (R) | Temporal and parietal (R) + temporal–parietal fracture (R) | Positive | Subdural | Temporal–Parietal (R) | 0.6 | 0.8 | 15 |
| EDH | Temporal–Parietal (R) | 21 | 1 | |||||
| tSAH | Temporal–Parietal (R) | N/A | 0.8 | |||||
| Positive | Frontal (R) | No | Positive | Subdural | Parietal (R) | 0.3 | 1.2 | 12 |
| Contusion | Parietal (L) | N/A | 1.4 | |||||
| Positive | Frontal, parietal, occipital (L) | No | Positive | Subdural | Frontal–Temporal–Parietal–Occipital (L) | 2.13 | Front: 0.8; Occipital: 0.7; Parietal: 0.6 | 14 |
| Positive | Parietal (R) | Frontal (L) | Positive | tSAH | Frontal (R) | N/A | 1.09 | 15 |
| InfraScanner Results | CT-Scan | GCS | ||||||
|---|---|---|---|---|---|---|---|---|
| Result | Location (Positive Side) | Subgaleal | Result | Type(s) of Intracranial Hemorrhage | Location | Volume of Bleeding | Depth of Bleeding | |
| Negative | N/A | Temporal (L) | Positive | Subdural | Temporal (R) | 0.6 | 0.48 | 14 |
| Negative | N/A | No | Positive | Subdural | Frontal (R) | 0.1 | 1.9 | 12 |
| Positive | tSAH | Frontal (L) | N/A | 1.15 | ||||
| Negative | N/A | No | Positive | tSAH | Occipital (R) | N/A | 1.0 | 13 |
| Occipital (L) | N/A | 2.6 | ||||||
| Negative | N/A | No | Positive | IPH | Frontal–Parietal (R) | N/A | Front: 2.03; Parietal: 0.7 | 3 |
| Positive | Frontal–Parietal (L) | N/A | Front: 1.2; Parietal: 3.2 | |||||
| Negative | N/A | Occipital (R) | Positive | Contusion | Frontal (L) | N/A | 1.8 | 10 |
| tSAH | Temporal (L) | N/A | 2.6 | |||||
| Study Number | Author, Country, Year and Reference | Sample Size | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|
| 1 | Gopinath et al., USA, 1993 [21] | 56 | 100% | 100% | 100% | 100% |
| 2 | Hennes et al., Germany, 1997 [22] | 212 | 95.9% | 28.9% | 64.6% | 83.9% |
| 3 | Francis et al., India, 2005 [19] | 71 | 77.8% | 100% | 100% | 93% |
| 4 | Kahraman et al., Turkey, 2006 [20] | 60 | 86.7% | 100% | 100% | 88.2% |
| 5 | Kessel et al., Israel, 2007 [23] | 110 | 67.9% | 95.1% | 82.6% | 89.7% |
| 6 | Ghalenoui et al., Iran, 2008 [24] | 148 | 88.9% | 77.7% | 69.6% | 92.4% |
| 7 | Coskun et al., Turkey, 2010 [25] | 253 | 86.4% | 54.5% | 15.3% | 97.7% |
| 8 | Leon-Carrion et al., Spain, 2010 [8] | 35 | 89.5% | 81.3% | 85% | 86.7% |
| 9 | Robertson et al., USA and India, 2010 [9] | 319 | 88% | 90.7% | 63.7% | 97.6% |
| 10 | Akyol et al., Turkey, 2016 [26] | 151 | 85.7% | 66.6% | 11.1% | 98.9% |
| 11 | Xu et al., China, 2017 [13] | 85 | 95.6% | 92.5% | 93.5% | 94.9% |
| 12 | Peters et al., Netherlands, 2017 [27] | 60 | 92.9% | 72.7% | 81.3% | 88.9% |
| 13 | Trehan et al., India, 2018 [28] | 100 | 58.9% | 42.9% | 65.5% | 35.7% |
| 14 | Liang et al., China, 2018 [17] | 102 | 100% | 93.6% | 82.8% | 100% |
| 15 | Yuksen et al., Thailand, 2020 [29] | 47 | 100% | 44.4% | 35.5% | 100% |
| Variable | Options |
|---|---|
| Health center | South/North/East/Referral Center |
| Sex | Male/Female |
| TBI Type | Blunt/Penetrating |
| Time and date of the trauma | DD/MM/YY and time |
| Time and date of the NIRS measurement | DD/MM/YY and time |
| Positive NIRS | Yes/No |
| Hair type | Straight/Curly wavy/No hair |
| Hair color | Black/Blond/White/Brown/Other/No hair |
| Hair length | Short/Medium/Long/No hair |
| Subgaleal hematoma | Yes/No |
| Scalp laceration | Yes/No |
| Time and date of the CT scan | DD/MM/YY and time |
| Intracranial hematoma on the CT scan | Yes/No |
| Type of hematoma | Subdural < 1 cm/Subdural > 1 cm/Epidural < 30 cc/Epidural > 30 cc/Intraparenchymal hematoma/Subarachnoid hemorrhage |
| Location of the hemorrhage on the CT scan | Frontal/temporal/parietal/occipital |
| Laterality of the hemorrhage on the CT scan | Left/Right |
| Midline shift on the CT scan | Yes/No |
| Clinical conduct after ER | Discharge/Surgical management/Nonsurgical management |
| Hematoma volume | In cubic centimeters (mL) |
| Hematoma depth | In centimeters (cm) |
| Glasgow coma scale at time of initial presentation | 3–15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cardona-Collazos, S.; Olaya-Perea, S.; Fernández, L.; Griswold, D.; Villota, A.; Aristizabal, S.; Ginalis, E.; Sanchez, D.; Kolias, A.; Hutchinson, P.; et al. Performance of the InfraScanner for the Detection of Intracranial Bleeding in a Population of Traumatic Brain Injury Patients in Colombia. Emerg. Care Med. 2025, 2, 35. https://doi.org/10.3390/ecm2030035
Cardona-Collazos S, Olaya-Perea S, Fernández L, Griswold D, Villota A, Aristizabal S, Ginalis E, Sanchez D, Kolias A, Hutchinson P, et al. Performance of the InfraScanner for the Detection of Intracranial Bleeding in a Population of Traumatic Brain Injury Patients in Colombia. Emergency Care and Medicine. 2025; 2(3):35. https://doi.org/10.3390/ecm2030035
Chicago/Turabian StyleCardona-Collazos, Santiago, Sandra Olaya-Perea, Laura Fernández, Dylan Griswold, Alvaro Villota, Sarita Aristizabal, Elizabeth Ginalis, Diana Sanchez, Angelos Kolias, Peter Hutchinson, and et al. 2025. "Performance of the InfraScanner for the Detection of Intracranial Bleeding in a Population of Traumatic Brain Injury Patients in Colombia" Emergency Care and Medicine 2, no. 3: 35. https://doi.org/10.3390/ecm2030035
APA StyleCardona-Collazos, S., Olaya-Perea, S., Fernández, L., Griswold, D., Villota, A., Aristizabal, S., Ginalis, E., Sanchez, D., Kolias, A., Hutchinson, P., & Rubiano, A. M. (2025). Performance of the InfraScanner for the Detection of Intracranial Bleeding in a Population of Traumatic Brain Injury Patients in Colombia. Emergency Care and Medicine, 2(3), 35. https://doi.org/10.3390/ecm2030035