Abstract
We conducted a two-sample Mendelian randomization (MR) study including only European men to test for a causal relationship between serum urate (SU), gout, and prostate cancer. Using genome-wide association (GWAS) data, we generated instrumental variables (IVs) associated with gout and urate. These included 20 single nucleotide polymorphisms (SNPs) associated with gout but not urate (non-hyperuricemia compartment of gout) and four SNPs from loci containing urate transporter genes for an IV representing urate levels. MR methods included the inverse-variance weighted (IVW) method, MR-Egger regression, and the weighted median method. The non-hyperuricemia compartment of gout IV showed a causal effect of gout on prostate cancer (weighted median: p = 0.01). In contrast, the SU IV showed no evidence of a causal effect of SU on prostate cancer (IVW: p = 0.83; weighted median: p = 0.97). MR-Egger showed no evidence of horizontal pleiotropy (gout: p = 0.33; urate: p = 0.80). Loci contributing most strongly to the non-hyperuricemia causal effect included three genes: IL1R1, IL1RN, and SLC30A5. There was no evidence of a causal relationship between prostate cancer and gout or SU. In conclusion, MR analysis in a European male population found evidence of a causal relationship between the non-hyperuricemia compartment of gout and prostate cancer. Implication of the IL1R1 and IL1RN genes directly implicates the gouty inflammation pathway in prostate cancer.
1. Introduction
Gout is an inflammatory disorder characterized by an elevation in SU that manifests as local and systemic inflammation secondary to monosodium urate (MSU) crystal deposition in joints and other tissues. If left untreated, gout frequently manifests as recurrent episodes of acute inflammation that are very painful and severely disabling, potentially increasing the risk of comorbidities including heart failure, myocardial infarction, chronic kidney disease stage ≥2 and diabetes [1,2,3]. Gout affects approximately 5.1% of adults in the US, with ~ a 3-fold increased prevalence in men, and men have elevated SU levels compared to women [4,5,6,7]. There is evidence that the prostate plays a role in urate homeostasis in men, with urate being present in human semen, and MSU crystals being found in 47.5% of non-malignant prostate sections [8,9,10]. Additionally, gout is associated with an increased risk of benign prostatic hyperplasia (BPH) and treatment with the urate-lowering drug allopurinol decreases the risk of BPH, suggesting that the presence of higher urate levels and gout may both contribute to prostatic enlargement [11,12]. BPH shares a number of features with prostate cancer, including hormone-dependent growth and metabolic disruption playing key roles in disease development, and a causal relationship between BPH and prostate cancer has recently been established [13,14].
Mendelian randomization (MR) is a genetic epidemiological approach to establish causality between two phenotypes by testing genetic variants (instrumental variables) associated with an increased risk of exposure to the outcome (17). One advantage of using MR is that genetic variants are fixed at conception, making the method resistant to the influence of confounding factors [15,16]. Previous studies using MR examined whether a causal relationship exists between urate and prostate cancer [17,18], though none have tested the association of gout with prostate cancer. Studies that have examined genetic links between SU and prostate cancer have had contradictory findings. In an East Asian cohort, increased urate levels were causally associated with prostate cancer, but no causal relationship was found in a European cohort [17,18]. However, these studies included females in the GWAS for development of the SU instrumental variable. Since females have lower SU levels [5], and prostate cancer only affects males, the results found from these studies may be biased.
Due to the genetic and epidemiological evidence of a potential relationship between gout, urate, prostatic inflammation, and prostate cancer, limitations of previous MR studies, and the fact that gout has not yet been examined as an exposure in prostate cancer MR, we aimed to identify whether there was a potential causal relationship between urate, gout-related inflammation, and prostate cancer. Unlike all previous MR studies in gout, we isolated the non-hyperuricemic (inflammatory) compartment of gout and tested this signal along with urate transport genes against prostate cancer risk.
2. Materials and Methods
2.1. Exposure Instrumental Variable and Outcome GWAS Summary Statistics for Two-Sample MR Study
Our study was designed to identify any potential causal effects of SU and of the non-hyperuricemia compartment of gout on prostate cancer risk. Since prostate cancer is a male-only condition, we identified male-only genome-wide association studies (GWAS) of SU and gout and used effect sizes from these studies in the MR analysis. We used previously published European ancestry male-only gout and SU GWAS [19]. The European, male-only gout GWAS contained 74,503 cases and ~850,000 controls, and defined gout according to self-reported diagnosis and/or use of urate-lowering medication, clinical diagnosis and/or the American College of Rheumatology gout classification criteria [20], dependent on the information available in each source cohort [19]. The SU GWAS contained a total of 145,625 men aged 40–69 with complete SU measurements from the UK Biobank (project number 12611). The prostate cancer GWAS was sourced from Wang et al. and contained 122,188 cases and 604,640 male controls of European ancestry [21].
2.2. Statistical Analysis
We selected gout instrumental variables (IVs) from the gout GWAS to represent the non-hyperuricemia compartment of gout. This was determined previously by Major et al. by conducting colocalization analysis between the lead variants for signals in gout and SU [19], where lead SNPs from signals with posterior probabilities for H1 or H3 ≥ 0.8 represented an association with gout but not urate, and therefore the non-hyperuricemia compartment of gout (such as promotion of gout inflammation and deposition of MSU crystals). The lead SNPs from these genetic signals were used for MR analysis as IVs [19]. SU IVs were selected as the lead SNPs from the SU GWAS at loci including genes involved in urate transport: SLC2A9, SLC2A11, PDZK1, SLC17A1. This was to minimize pleiotropy owing to the established function of the four proteins in directly influencing urate levels and without robust evidence for a role in other physiological processes. F-statistics were calculated for each SNP from both the gout and SU GWAS, as described previously [22]. A full list of all SNPs used for the non-hyperuricemia compartment of gout, all proxy variants selected, and a list of all SNPs used to represent urate transporter genes are available in Supplementary Table S1. Proxy variants were selected when an SNP in the IV was not present in the prostate cancer GWAS. Proxies were selected by identifying variants in high LD (r2 > 0.95) and selecting the top variant available in both the SU/gout and prostate cancer GWAS.
We also conducted the reverse MR, i.e., testing prostate cancer for causality of gout and SU. Due to the large number of significant risk variants in the source prostate cancer GWAS (451 risk variants were identified by Wang et al.) [21], we selected only the most significant SNPs (p < 1 × 10−80) to reduce the risk of pleiotropy. The IV was identified by first identifying loci with SNPs associated with prostate cancer at a level of p < 1 × 10−50. After these loci were identified, we selected only the top SNP from each locus, keeping only SNPs with p < 1 × 10−80. This resulted in a set of 18 SNPs (Supplementary Table S2).
For these IVs to be valid, they each should fulfill the assumptions necessary for MR: (1) all selected IVs are significantly associated with the exposure (F-Statistic > 10); (2) IVs are independent of confounders that could affect both the exposure and outcome; (3) IVs influence the outcome only through the exposure [15]. We did not evaluate assumption 2 because we did not identify any obvious conditions that may be potential confounders or mediators between gout/SU and prostate cancer. Assumption 3 was tested using MR-Egger, which accounts for potential horizontal pleiotropic effects between the exposure and outcomes [15].
Three main methods of MR were used: the inverse-variance weighted MR (IVW), MR-Egger regression, and the weighted median method. Additional sensitivity analyses included the penalization of IVW and the exclusion of outlier SNPs. All MR analyses used R 4.3.1 and the MendelianRandomization package [23]. For all MR analyses, we used the effect size for the outcome as the response variable and the effect size for the exposure as the predictor variable. This resulted in two main relationships being tested: (1) whether the non-hyperuricemia compartment of gout is causal for prostate cancer and (2) whether the SU is causal for prostate cancer. The reverse relationships were also tested: (1) whether prostate cancer is causal for gout; and (2) whether prostate cancer is causal for SU.
After MR analysis, we examined whether the SNPs driving the MR results acted as potential expression quantitative trait loci (eQTL) in the following tissues from the Genotype-Tissue Expression (GTEx) data (22): whole blood, prostate, cultured fibroblast cells, Epstein–Barr-virus (EBV)-transformed lymphocytes, and testes. The data for these analyses were obtained from dbGaP accession number phs000424.v10.p2, and European GTEx v8 eQTL data were used. Colocalization results were sourced from Major et al. [19].
3. Results
3.1. Gout to Prostate Cancer Mendelian Randomization
Using the weighted median method, we observed evidence that gout may be causal for prostate cancer (OR: 1.18; 95% CI: 1.03–1.35; p = 0.01; Table 1; Figure 1) although this was not supported using the IVW method (IVW: OR: 1.10; 95% CI: 0.92–1.31; p = 0.29; Table 1; Figure 1). MR-Egger showed no evidence of horizontal pleiotropy (intercept: −0.010; SE: 0.010; p = 0.33; Table 1). Sensitivity analysis using the penalized IVW method to handle potential outliers supported our hypothesis that gout is causal for prostate cancer (OR: 1.16; 95% CI: 1.03–1.31; p = 0.01; Supplementary Table S3). The results of all gout non-hyperuricemia compartment SNPs are available in Supplementary Figure S1. The gout-risk alleles of three SNPs, rs2560449, rs17767183, and rs9973741, drove this causal relationship, while the gout-risk allele of one SNP, rs2395180, was significantly protective of prostate cancer.

Table 1.
Mendelian Randomization results.
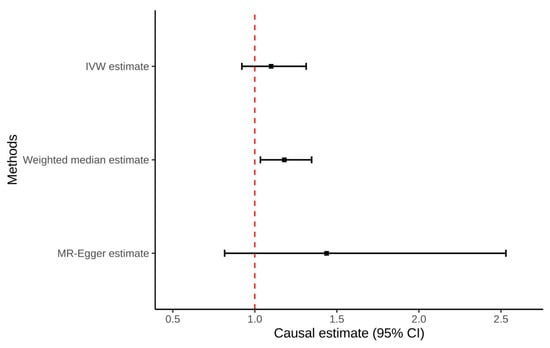
Figure 1.
Forest plot of all Mendelian Randomization tests for the non-hyperuricemia compartment of gout to prostate cancer.
LocusZoom plots were generated for each SNP that significantly contributed to the positive association between gout and prostate cancer, and each SNP was assigned to the closest gene: SLC30A5 (rs2560449; Supplementary Figure S2), IL1R1 (rs17767183; Supplementary Figure S3), IL1RN (rs9973741; Supplementary Figure S4). Even though rs9973741 is in very close proximity to both IL1RN and IL1F10, we only assigned it to IL1RN since IL1F10 is only expressed in skin tissue (GTEx). We noted that rs2395180 was located in the HLA locus, in close proximity to a number of genes (Supplementary Figure S5). Using the Major et al. data [19] we identified one potentially colocalizing eQTL from the SNPs and tissues of interest: rs9973741 with IL1RN expression in the testes (Supplementary Table S4; Supplementary Figure S6). The IL1RN eQTL signal overlaps only with gout, and not with prostate cancer (Supplementary Figure S6).
We conducted a secondary analysis excluding rs2395180 as a clear outlier with non-overlapping 95% confidence intervals (CIs) with other variants in the IV and being in a locus with erratic association with gout, perhaps driven by (uncorrected) population structure [24]. In this analysis, the IVW, weighted median, and penalized IVW methods all showed causal effects of gout on prostate cancer (Table 1; Figure 2).
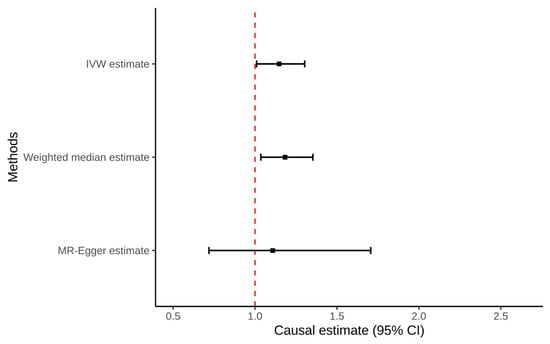
Figure 2.
Forest plot of all Mendelian Randomization tests for the non-hyperuricemia compartment of gout to prostate cancer, excluding outlier (rs2395180).
3.2. Serum Urate to Prostate Cancer Mendelian Randomization
Using the IVW method, there was no evidence that genetically predicted SU was causal for prostate cancer (OR: 1.00; 95% CI: 0.97–1.02; p = 0.83; Table 1; Figure 3). This lack of causal relationship was also seen in the weighted median analysis (OR: 1.00; 95% CI: 0.98–1.02; p = 0.97; Table 1; Figure 3). Additionally, MR-Egger showed no evidence for horizontal pleiotropy (Intercept: 0.004; SE: 0.017; p = 0.80; Table 1). No individual SNPs were significantly associated.
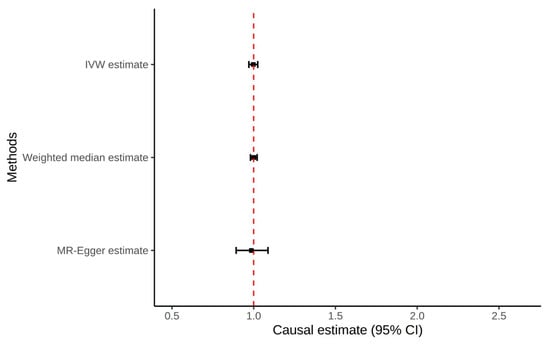
Figure 3.
Forest plot of all Mendelian Randomization tests for the urate transporter SNPs to prostate cancer.
3.3. Prostate Cancer to Serum Urate and Gout Mendelian Randomization
There was no evidence that genetically predicted prostate cancer was causal for gout using either the IVW (OR: 0.99; 95% CI: 0.96–1.02; p = 0.61; Table 1) or weighted median MR methods (OR: 0.99; 95% CI: 0.96–1.02; p = 0.53; Table 1). There was also no evidence that genetically predicted prostate cancer was causal for SU using either the IVW method (OR: 1.01; 95% CI: 0.93–1.09; p = 0.89; Table 1) or the weighted median method (OR: 1.02; 95% CI: 0.95–1.10; p = 0.53; Table 1). Additionally, MR-Egger showed no evidence for horizontal pleiotropy in either gout (Intercept: 0.005; SE: 0.007; p = 0.47; Table 1) or SU (Intercept: 0.001; SE: 0.020; p = 0.97; Table 1).
4. Discussion
Our study tested whether the non-hyperuricemia compartment of gout and SU are causal for prostate cancer in men of European ancestry. We assessed this using a two-sample MR analysis in men and found evidence supporting a causal relationship between gout inflammation (two of the three positively associated variants were in loci encoding genes central to IL-1β signaling) and prostate cancer. There was no evidence for a causal relationship of SU for prostate cancer, or on prostate cancer for gout or SU.
Our findings align with previous MR findings that SU is not causal of prostate cancer among European males [18], although there have been mixed findings from MR studies in East Asians and in observational studies, with observational studies showing differences in SU levels in those with prostate cancer vs. those without [17,25,26,27]. However, none of these studies assessed the reverse relationships or gout-causing inflammatory factors, and observational studies cannot infer causality.
To our knowledge, this is the first evidence that the non-hyperuricemia compartment of gout may be causal of prostate cancer. There have been observational studies of gout and prostate cancer, but the results have been conflicting. In one cohort study of Taiwanese patients with 8408 male gout patients and 25,010 age-matched and time-of-diagnosis-matched controls, gout patients were 3 times more likely to develop prostate cancer when compared to the non-gout population [28]. In another Taiwanese cohort study including 355,278 male patients, 25,943 of whom had gout, gout patients were 1.7 times more likely to develop prostate cancer than non-gout patients [29]. However, in a Korean health insurance data study of 179,930 age-matched gout patients and non-gout controls, men with prostate cancer had a lower incidence rate of gout when compared to age-matched non-gout controls [30]. In another study of hospital discharges in Sweden, there was no association between gout and the incidence of prostate cancer [31].
Our MR study identified three genes driving the relationship between the non-hyperuricemia compartment of gout and prostate cancer: IL1R1 (rs17767183), IL1RN (rs9973741), and SLC30A5 (rs2560449). IL1R1 [32], Il1RN [33], and SLC30A5 [34] have all been previously implicated in prostate cancer. The IL-1 pathway has been shown to play a role in both the development and progression of prostate cancer, though the exact mechanism is still unknown [32,33]. Additionally, depleted zinc concentration is associated with prostate cancer progression, and zinc transporter SLC30A5 has been shown to be downregulated in cancerous tissue [34]. Though we do not fully understand the mechanisms through which these SNPs may be causal of prostate cancer, it is notable that two of the top SNPs are both involved in the same inflammatory pathway (the IL1 pathway) with the protein encoded by IL1RN (IL1-RA) being an antagonist for IL1-R1, which is also a receptor for the key gout cytokine IL-1β. This biological linkage supports the hypothesis that prostatic inflammation, perhaps triggered by MSU crystals, is a risk factor for prostate cancer.
We hypothesize that the deposition and accumulation of MSU crystals in the prostate [10] may induce a pro-inflammatory state in prostatic tissue with shared pathways to those in gout inflammation. Men with gout would have increased proclivity to respond to MSU crystals deposited in the prostate. IL1R1 encodes an IL-1 receptor protein which binds IL-1α and IL-1β, and IL1RN encodes for an IL1 receptor antagonist (IL1-RA), which mediates IL-1α and IL-1β activity and inflammation. In eQTL analysis, rs9973741 (allele G, which is the risk allele for gout) associated with decreased expression of IL1RN in the prostate and decreased expression of both IL1RN and IL1R1 in whole blood, while increasing IL1RN expression in the testes. This indicates that the putative pathway may involve complex patterns of regulation of gene expression. Further validation of our findings may lead to new clinical treatments to mitigate the risk of prostate cancer, such as the use of urate lowering therapies to reduce prostatic inflammation. Notably, allopurinol has previously been used to reduce symptoms of non-bacterial prostatitis [35,36].
The exact mechanisms by which SLC30A5 may contribute to a causal relationship is less clear. SLC30A5 encodes for ZnT5 and transports zinc into membrane-bound organelles and out of the cell and is vital in maintaining zinc homeostasis [37]. A specific mechanism has not yet linked SLC30A5 and gout. However, chronic zinc deficiency is associated with increased production of pro-inflammatory cytokines [38], many of which are associated with gout, including IL-1 β, and IL-6. We hypothesize that a downregulation of the ZnT5 protein may exacerbate inflammatory responses in the body, potentially resulting in gout. ZnT5’s association with prostate cancer has been more clearly explored, has been shown to be downregulated in prostate cancer tissue, and this downregulation is an early event in prostate cancer progression [34,39].
To further establish the biological plausibility of causality of the inflammatory aspect of gout for prostate cancer, future MR studies should replicate our findings as further datasets become available. Additionally, in silico clinical trials of urate-lowering therapy in men followed by assessment of prostate cancer rates could be performed to further establish this relationship.
Our study has various strengths. We utilized a two-sample MR analysis, which allowed for finding causal genetic relationships. We used SNPs representing specific aspects of gout risk and SU level, rather than using all SNPs which are significantly associated with gout, which allowed us to test specific mechanistic hypotheses. We included only men in the various genetic datasets used in our study. We tested the causal associations using three methods, the IVW, weighted median, and MR-Egger methods, which robustly test for causal relationships and test for horizontal pleiotropy. However, our study also has limitations. We only included European men in our analysis, which means that these results may not be applicable to other populations. Major et al. [19] compartmentalized the gout IV as gout-specific (not significantly associated with urate), and we described it as representative of the non-hyperuricemia compartment of gout to encapsulate the combined process of MSU crystal deposition and inflammation, but there has been no specific genetic or experimental studies to test the biological validity of this stratification. Even though we conducted tests for horizontal pleiotropy, the MR-Egger test does not guarantee that no pleiotropy exists, and we did not conduct extensive checks for vertical pleiotropy. Owing to the lack of independent, male-only datasets not already included in the GWAS used in our analyses, we were unable to include replication in the study design, thus there is the possibility that our evidence for a causal association is false positive. Additionally, our study used genetic predictors of SU levels rather than of prostatic urate levels. The collective evidence supports that the prostate produces urate, but genetic predictors of serum urate levels may not reflect those of prostate urate level.
In conclusion, our MR analyses of a European male population provided evidence for a causal relationship between the non-hyperuricemia compartment of gout and prostate cancer, but not between SU and prostate cancer.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/gucdd3040020/s1, Figure S1: Forest plot of all non-hyperuricemia compartment of gout SNPs to prostate cancer; Figure S2: LocusZoom plot of rs2560449 in prostate cancer (A) and in gout (B) in men; Figure S3: LocusZoom plot of rs17767183 in prostate cancer (A) and in gout (B) in men; Figure S4: LocusZoom plot of rs9973741 in prostate cancer (A) and in gout (B) in men; Figure S5: LocusZoom plot of rs2395180 in prostate cancer (A) and in gout (B) in men; Figure S6: LocusZoom of the eQTL for the association of rs9973741 and IL1RN in testis tissue (A) and with gout (B) and prostate cancer (C); Figure S7: Forest plot of all urate transporter SNPs to prostate cancer; Table S1: Variants and proxies used for the non-inflammatory compartment of gout and urate transporter gene Mendelian randomization; Table S2: Variants used for the prostate cancer Mendelian randomization; Table S3: Additional tests run for the non-hyperuricemia compartment of gout Mendelian randomization; Table S4: Significant expression quantitative trait loci (eQTL) for the non-hyperuricemia compartment of gout from selected tissues.
Author Contributions
Conceptualization, S.C., T.R.M. and J.S.; methodology and analytics, S.C., R.T., N.S. and T.R.M.; writing—initial draft preparation, S.C.; writing—review and editing, all authors. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All new data generated are included in the manuscript and Supplementary Materials.
Conflicts of Interest
All authors except J.S. declare that they have no conflicts of interest relevant to this study. J.S. has received consultant fees from ROMTech, Atheneum, Clearview healthcare partners, American College of Rheumatology, Yale, Hulio, Horizon Pharmaceuticals/DINORA, ANI/Exeltis, USA Inc., Frictionless Solutions, Schipher, Crealta/Horizon, Medisys, Fidia, PK Med, Two labs Inc., Adept Field Solutions, Clinical Care options, Putnam associates, Focus forward, Navigant consulting, Spherix, MedIQ, Jupiter Life Science, UBM LLC, Trio Health, Medscape, WebMD, and Practice Point communications, the National Institutes of Health, and the American College of Rheumatology. JAS has received institutional research support from Zimmer Biomet Holdings. JAS received food and beverage payments from Intuitive Surgical Inc./Philips Electronics North America. JAS owns stock options in Atai life sciences, Kintara therapeutics, Intelligent Biosolutions, Acumen pharmaceutical, TPT Global Tech, Vaxart pharmaceuticals, Atyu biopharma, Adaptimmune Therapeutics, GeoVax Labs, Pieris Pharmaceuticals, Enzolytics Inc., Seres Therapeutics, Tonix Pharmaceuticals Holding Corp., Aebona Pharmaceuticals, and Charlotte’s Web Holdings, Inc. JAS previously owned stock options in Amarin, Viking and Moderna pharmaceuticals. JAS is on the speaker’s bureau of Simply Speaking.
References
- Dalbeth, N.; Gosling, A.L.; Gaffo, A.; Abhishek, A. Gout. Lancet 2021, 397, 1843–1855. [Google Scholar] [CrossRef] [PubMed]
- Colantonio, L.D.; Saag, K.G.; Singh, J.A.; Chen, L.; Reynolds, R.J.; Gaffo, A.; Plante, T.B.; Curtis, J.R.; Bridges, S.L., Jr.; Levitan, E.B.; et al. Gout is associated with an increased risk for incident heart failure among older adults: The REasons for Geographic and Racial Differences in Stroke (REGARDS) cohort study. Arthritis Res. Ther. 2020, 22, 86. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Pandya, B.J.; Choi, H.K. Comorbidities of gout and hyperuricemia in the US general population: NHANES 2007-2008. Am. J. Med. 2012, 125, 679–687.e1. [Google Scholar] [CrossRef]
- Yokose, C.; McCormick, N.; Lu, N.; Tanikella, S.; Lin, K.; Joshi, A.D.; Raffield, L.M.; Warner, E.; Merriman, T.; Hsu, J.; et al. Trends in Prevalence of Gout Among US Asian Adults, 2011-2018. JAMA Netw. Open 2023, 6, e239501. [Google Scholar] [CrossRef]
- Chen-Xu, M.; Yokose, C.; Rai, S.K.; Pillinger, M.H.; Choi, H.K. Contemporary prevalence of gout and hyperuricemia in the United States and decadal trends: The National Health and Nutrition Examination Survey, 2007-2016. Arthritis Rheumatol. 2019, 71, 991–999. [Google Scholar] [CrossRef]
- Halperin Kuhns, V.L.; Woodward, O.M. Sex differences in urate handling. Int. J. Mol. Sci. 2020, 21, 4269. [Google Scholar] [CrossRef]
- Liu-Bryan, R.; Guo, T.; Lee, J.; Terkeltaub, R. Atherogenic activation of human vascular smooth muscle cells by monosodium urate crystals. Gout Urate Cryst. Depos. Dis. 2023, 1, 192–207. [Google Scholar]
- Srivastava, A.; Chopra, S.K.; Dasgupta, P.R. Biochemical analysis of human seminal plasma. II. Protein, non-protein nitrogen, urea, uric acid and creatine. Andrologia 1984, 16, 265–268. [Google Scholar] [CrossRef]
- Zhang, H.Y.; Lu, J.C.; Zhang, R.S.; Xia, Y.X.; Huang, Y.F. Determination of uric acid in seminal plasma and correlation between seminal uric acid and semen parameters. Zhonghua Nan Ke Xue 2007, 13, 1016–1019. [Google Scholar]
- Park, J.J.; Roudier, M.P.; Soman, D.; Mokadam, N.A.; Simkin, P.A. Prevalence of birefringent crystals in cardiac and prostatic tissues, an observational study. BMJ Open 2014, 4, e005308. [Google Scholar] [CrossRef] [PubMed]
- Li, W.M.; Pasaribu, N.; Lee, S.S.; Tsai, W.C.; Li, C.Y.; Lin, G.T.; Chuang, H.Y.; Tung, Y.C.; Tu, H.P. Risk of incident benign prostatic hyperplasia in patients with gout: A retrospective cohort study. Prostate Cancer Prostatic Dis. 2018, 21, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Kukko, V.; Kaipia, A.; Talala, K.; Taari, K.; Tammela, T.L.J.; Auvinen, A.; Murtola, T.J. Allopurinol and risk of benign prostatic hyperplasia in a Finnish population-based cohort. Prostate Cancer Prostatic Dis. 2018, 21, 373–378. [Google Scholar] [CrossRef]
- Zhang, Y.; Ou, G.; Li, R.; Peng, L.; Shi, J. Causal relationship between benign prostatic hyperplasia and prostate cancer: A bidirectional Mendelian randomization analysis. Postgrad. Med. J. 2024, 101, 427–434. [Google Scholar] [CrossRef]
- Orsted, D.D.; Bojesen, S.E. The link between benign prostatic hyperplasia and prostate cancer. Nat. Rev. Urol. 2013, 10, 49–54. [Google Scholar] [CrossRef]
- De Leeuw, C.; Savage, J.; Bucur, I.G.; Heskes, T.; Posthuma, D. Understanding the assumptions underlying Mendelian randomization. Eur. J. Hum. Genet. 2022, 30, 653–660. [Google Scholar] [CrossRef]
- Davies, N.M.; Holmes, M.V.; Davey Smith, G. Reading Mendelian randomisation studies: A guide, glossary, and checklist for clinicians. BMJ 2018, 362, k601. [Google Scholar] [CrossRef]
- Deng, Y.; Huang, J.; Wong, M.C.S. Association between serum uric acid and prostate cancer risk in East Asian populations: A Mendelian randomization study. Eur. J. Nutr. 2023, 62, 1323–1329. [Google Scholar] [CrossRef]
- Jiang, M.; Ren, L.; Chen, S.; Li, G. Serum uric acid levels and risk of eight site-specific cancers: A Mendelian randomization study. Front. Genet. 2021, 12, 608311. [Google Scholar] [CrossRef] [PubMed]
- Major, T.J.; Takei, R.; Matsuo, H.; Leask, M.P.; Sumpter, N.A.; Topless, R.K.; Shirai, Y.; Wang, W.; Cadzow, M.J.; Phipps-Green, A.J.; et al. A genome-wide association analysis reveals new pathogenic pathways in gout. Nat. Genet. 2024, 56, 2392–2406. [Google Scholar] [CrossRef] [PubMed]
- Neogi, T.; Jansen, T.L.; Dalbeth, N.; Fransen, J.; Schumacher, H.R.; Berendsen, D.; Brown, M.; Choi, H.; Edwards, N.L.; Janssens, H.J.; et al. 2015 Gout Classification Criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheumatol. 2015, 67, 2557–2568. [Google Scholar] [CrossRef]
- Wang, A.; Shen, J.; Rodriguez, A.A.; Saunders, E.J.; Chen, F.; Janivara, R.; Darst, B.F.; Sheng, X.; Xu, Y.; Chou, A.J.; et al. Characterizing prostate cancer risk through multi-ancestry genome-wide discovery of 187 novel risk variants. Nat. Genet. 2023, 55, 2065–2074. [Google Scholar] [CrossRef]
- Bowden, J.; Del Greco, M.F.; Minelli, C.; Zhao, Q.; Lawlor, D.A.; Sheehan, N.A.; Thompson, J.; Davey Smith, G. Improving the accuracy of two-sample summary-data Mendelian randomization: Moving beyond the NOME assumption. Int. J. Epidemiol. 2019, 48, 728–742. [Google Scholar] [CrossRef] [PubMed]
- Burgess, S.; Yavorska, O. MendelianRandomization: Mendelian Randomization Package, R package version 0.10.0; R Core Team: Vienna, Austria, 2024. [Google Scholar]
- Lokki, M.L.; Paakkanen, R. The complexity and diversity of major histocompatibility complex challenge disease association studies. HLA 2019, 93, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.; Barber, J.R.; Tin, A.; De Marzo, A.M.; Kottgen, A.; Joshu, C.E.; Platz, E.A. Serum Urate, Genetic Variation, and Prostate Cancer Risk: Atherosclerosis Risk in Communities (ARIC) Study. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1259–1261. [Google Scholar] [CrossRef]
- Singh, S.; Jaiswal, S.; Faujdar, G.; Priyadarshi, S. Comparison of serum uric acid levels between localised prostate cancer patients and a control group. Urologia 2024, 91, 320–325. [Google Scholar] [CrossRef]
- Park, J.W.; Lee, J.H.; Cho, H.J.; Ha, Y.J.; Kang, E.H.; Shin, K.; Byun, S.S.; Lee, E.Y.; Song, Y.W.; Lee, Y.J. Influence of androgen deprivation therapy on serum urate levels in patients with prostate cancer: A retrospective observational study. PLoS ONE 2018, 13, e0209049. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.J.; Yen, J.H.; Chang, S.J. Gout patients have an increased risk of developing most cancers, especially urological cancers. Scand. J. Rheumatol. 2014, 43, 385–390. [Google Scholar] [CrossRef]
- Kuo, C.F.; Luo, S.F.; See, L.C.; Chou, I.J.; Fang, Y.F.; Yu, K.H. Increased risk of cancer among gout patients: A nationwide population study. Jt. Bone Spine 2012, 79, 375–378. [Google Scholar] [CrossRef]
- Oh, Y.J.; Lee, Y.J.; Lee, E.; Park, B.; Kwon, J.W.; Heo, J.; Moon, K.W. Cancer risk in Korean patients with gout. Korean J. Intern. Med. 2022, 37, 460–467. [Google Scholar] [CrossRef]
- Boffetta, P.; Nordenvall, C.; Nyren, O.; Ye, W. A prospective study of gout and cancer. Eur. J. Cancer Prev. 2009, 18, 127–132. [Google Scholar] [CrossRef]
- Dahl, H.C.; Kanchwala, M.; Thomas-Jardin, S.E.; Sandhu, A.; Kanumuri, P.; Nawas, A.F.; Xing, C.; Lin, C.; Frigo, D.E.; Delk, N.A. Chronic IL-1 exposure drives LNCaP cells to evolve androgen and AR independence. PLoS ONE 2020, 15, e0242970. [Google Scholar] [CrossRef]
- Fan, Y.C.; Lee, K.D.; Tsai, Y.C. Roles of interleukin-1 receptor antagonist in prostate cancer progression. Biomedicines 2020, 8, 602. [Google Scholar] [CrossRef]
- Singh, C.K.; Malas, K.M.; Tydrick, C.; Siddiqui, I.A.; Iczkowski, K.A.; Ahmad, N. Analysis of zinc-exporters expression in prostate cancer. Sci. Rep. 2016, 6, 36772. [Google Scholar] [CrossRef]
- McNaughton, C.O.; Wilt, T. Allopurinol for chronic prostatitis. Cochrane Database Syst. Rev. 2002, CD001041. [Google Scholar] [CrossRef]
- Persson, B.E.; Ronquist, G.; Ekblom, M. Ameliorative effect of allopurinol on nonbacterial prostatitis: A parallel double-blind controlled study. J. Urol. 1996, 155, 961–964. [Google Scholar] [CrossRef]
- Kambe, T.; Matsunaga, M.; Takeda, T.A. Understanding the contribution of zinc transporters in the function of the early secretory pathway. Int. J. Mol. Sci. 2017, 18, 2179. [Google Scholar] [CrossRef] [PubMed]
- Bonaventura, P.; Benedetti, G.; Albarede, F.; Miossec, P. Zinc and its role in immunity and inflammation. Autoimmun. Rev. 2015, 14, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Bafaro, E.; Liu, Y.; Xu, Y.; Dempski, R.E. The emerging role of zinc transporters in cellular homeostasis and cancer. Signal Transduct. Target. Ther. 2017, 2, 17029. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Gout, Hyperuricemia and Crystal Associated Disease Network. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).