
A Contemporary Review of Thoracic Aortic Aneurysm: From Molecular Pathogenesis to Clinical Integration


Abstract

{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Normal Histology and Molecular Structure of the Aortic Wall
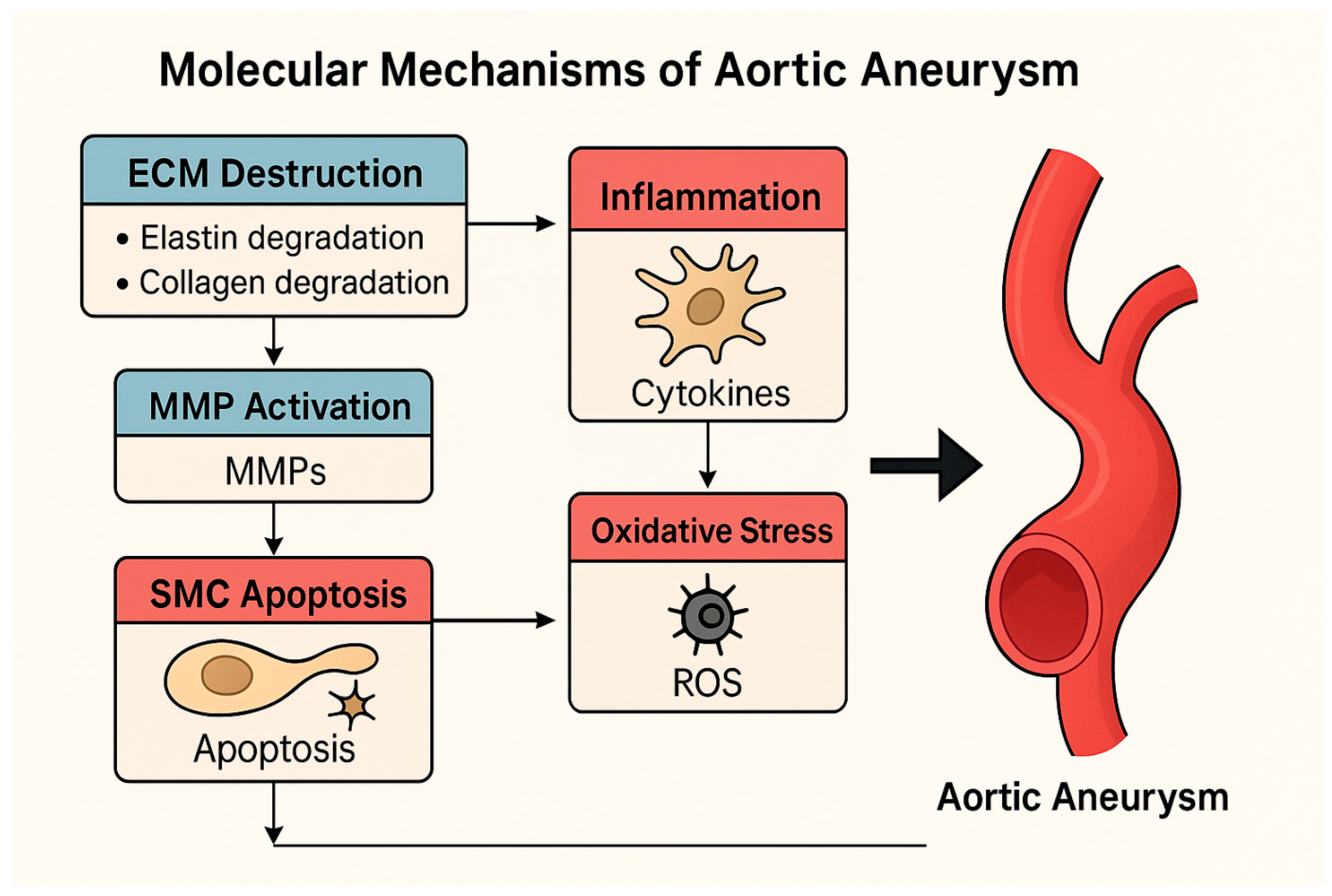
3. Pathogenesis and Molecular Mechanisms in Aortic Aneurysm
3.1. Matrix Metalloproteinases (MMPs) and ECM Degradation
3.2. Smooth Muscle Cell (SMC) Apoptosis and Phenotypic Change
3.3. Inflammation and the Role of the Immune System
3.4. The Role of Oxidative Stress
3.5. Disruption of the TGF-β Signaling Pathway
3.6. Genetic Contributions to Aneurysm Formation
4. Genetic and Epigenetic Factors
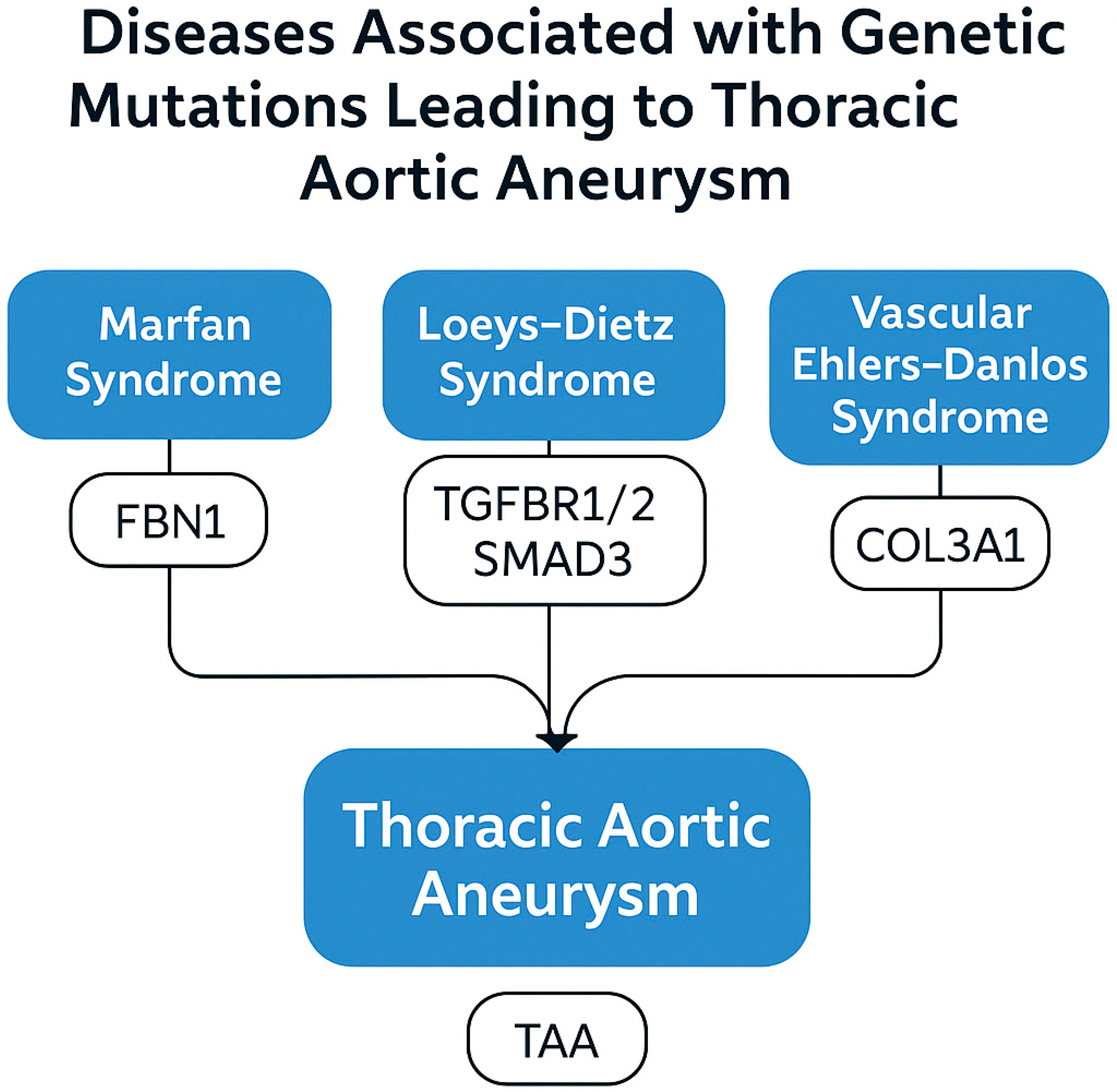
4.1. Hereditary Connective Tissue Diseases and Monogenic Mutations
- Marfan syndrome is caused by mutations in the FBN1 gene that result in a defect in the fibrillin-1 protein. This defect leads to disruption of elastic fiber organization and excessive activation of the TGF-β signaling pathway [42,43]. In addition to the well-established TGF-β pathway genes, variants in smooth muscle contractile apparatus genes such as ACTA2, MYH11, LOX, and PRKG1 have been linked to familial thoracic aortic aneurysms. ACTA2 mutations impair actin polymerization, weakening vessel wall tension and predisposing to dissection. LOX mutations reduce elastin crosslinking, compromising structural integrity.
- Ehlers–Danlos syndrome (vascular type) is caused by mutations in the COL3A1 gene that result in a defect in type III collagen synthesis. This condition severely weakens the mechanical strength of the aortic wall and increases the risk of spontaneous rupture [48].
4.2. Genetic Polymorphisms in Sporadic Aortic Aneurysms
- Genome-wide association studies (GWASs) have identified new risk loci associated with AAA. These studies have shown that genetic variations contribute to aneurysm formation [51].
4.3. Epigenetic Regulations
- DNA Methylation: Hypermethylation in promoter regions can suppress anti-inflammatory genes or genes involved in ECM production [53].
- Histone Modifications: Acetylation or methylation of histone proteins determines whether genes remain on or off by affecting chromatin structure. Increased histone acetylation has been detected in aneurysm tissues, particularly in the promoter regions of genes associated with the inflammatory response [56].
5. Animal Models and Translational Findings
5.1. Elastase-Induced Abdominal Aortic Aneurysm Model
5.2. Calcium Chloride (CaCl2) Model
5.3. Angiotensin II (Ang II)-Induced Aneurysm Model
5.4. Genetic Models
5.5. Translational Findings and Clinical Relevance
- MMP inhibitors (such as doxycycline) have slowed aneurysm development by suppressing MMP activity in experimental models but have had limited success in clinical trials [67].
- Therapeutic agents directed against microRNAs (such as miR-29 antagomirs) have shown positive results by preserving ECM homeostasis in animal models [54].
- Oxidative stress-reducing strategies (such as NADPH oxidase inhibitors) have reduced medial damage by reducing ROS levels [68].
- β-aminopropionitrile (BAPN), an irreversible inhibitor of lysyl oxidase, induces medial degeneration by preventing the crosslinking of collagen and elastin. Administered orally in mice, BAPN leads to weakening of the aortic wall and dissection, especially when combined with Ang II. This model simulates medial degeneration and is increasingly used to study the pathophysiology of thoracic aortic dissection.
6. Molecular Biomarkers and Future Diagnostic–Therapeutic Approaches
6.1. Potential Molecular Biomarkers
6.2. Molecular Targeted Treatment Approaches
6.3. Future Perspectives
6.4. Clinical Translation and Ongoing Trials
7. Discussion
8. Conclusions and Future Perspectives
9. Final Remarks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chaikof, E.L.; Dalman, R.L.; Eskandari, M.K.; Jackson, B.M.; Lee, W.A.; Mansour, M.A.; Starnes, B.W. The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. J. Vasc. Surg. 2018, 67, 2–77.e2. [Google Scholar] [CrossRef]
- Erbel, R.; Aboyans, V.; Boileau, C.; Di Bartolomeo, R.; Eggebrecht, H.; Vrints, C.J. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases. Eur. Heart J. 2014, 35, 2873–2926. [Google Scholar] [CrossRef]
- Golledge, J.; Thanigaimani, S.; Powell, J.T.; Tsao, P.S. Pathogenesis and management of abdominal aortic aneurysm. Eur. Heart J. 2023, 44, 2682–2697. [Google Scholar] [CrossRef]
- Wanhainen, A.; Verzini, F.; Van Herzeele, I.; Allaire, E.; Bown, M.; Cohnert, T. Editor’s Choice—European Society for Vascular Surgery (ESVS) 2019 Clinical Practice Guidelines on the Management of Abdominal Aorto-iliac Artery Aneurysms. Eur. J. Vasc. Endovasc. Surg. 2019, 57, 8–93. [Google Scholar] [CrossRef]
- Sakalihasan, N.; Michel, J.B.; Katsargyris, A.; Kuivaniemi, H.; Defraigne, J.O.; Nchimi, A.; Hultgren, R. Abdominal aortic aneurysms. Nat. Rev. Dis. Primers 2018, 4, 34. [Google Scholar] [CrossRef]
- Golledge, J.; Norman, P.E. Pathophysiology of abdominal aortic aneurysm relevant to improvements in patients’ management. Curr. Opin. Cardiol. 2009, 24, 532–538. [Google Scholar] [CrossRef]
- Thompson, R.W.; Geraghty, P.J.; Lee, J.K. Abdominal aortic aneurysms: Basic mechanisms and clinical implications. Curr. Probl. Surg. 2002, 39, 110–230. [Google Scholar] [CrossRef]
- Newby, A.C. Metalloproteinase expression in monocytes and macrophages and its relationship to atherosclerotic plaque instability. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 2108–2114. [Google Scholar] [CrossRef]
- Mills, A.C.; Sandhu, H.K.; Ikeno, Y.; Tanaka, A. Heritable thoracic aortic disease: A literature review on genetic aortopathies and current surgical management. Gen. Thorac. Cardiovasc. Surg. 2024, 72, 293–304. [Google Scholar] [CrossRef]
- Isselbacher, E.M.; Preventza, O.; Black, J.H.; Augoustides, J.G.; Beck, A.W.; Woo, Y.J. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease. J. Am. Coll. Cardiol. 2022, 80, e223–e393. [Google Scholar] [CrossRef]
- Kim, H.; Lee, J.H.; Chung, S.R.; Park, P.W.; Park, T.K.; Kang, I.S.; Sung, K. Impact of early diagnosis on surgical outcomes in patients with Loeys-Dietz syndrome. Front. Cardiovasc. Med. 2024, 11, 1429222. [Google Scholar] [CrossRef] [PubMed]
- Ganizada, B.H.; Veltrop, R.J.A.; Akbulut, A.C.; Koenen, R.R.; Accord, R.; Lorusso, R.; Schurgers, L.J. Unveiling cellular and molecular aspects of ascending thoracic aortic aneurysms and dissections. Basic. Res. Cardiol. 2024, 119, 371–395. [Google Scholar] [CrossRef]
- Golledge, J.; Tsao, P.S.; Dalman, R.L.; Norman, P.E. Circulating biomarkers in abdominal aortic aneurysm: Current status and prospects. Circulation 2008, 118, 2382–2389. [Google Scholar] [CrossRef] [PubMed]
- Ajoolabady, A.; Pratico, D.; Lin, L.; Mantzoros, C.S.; Bahijri, S.; Tuomilehto, J.; Ren, J. Inflammation in atherosclerosis: Pathophysiology and mechanisms. Cell Death Dis. 2024, 15, 817. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, S.A.; Mulvihill, J.J.; Barrett, H.E.; Kavanagh, E.G.; Walsh, M.T.; McGloughlin, T.M.; Doyle, B.J. Determining the influence of calcification on the failure properties of abdominal aortic aneurysm tissue. J. Mech. Behav. Biomed. Mater. 2015, 42, 154–167. [Google Scholar] [CrossRef]
- Wolinsky, H.; Glagov, S. A lamellar unit of aortic medial structure and function in mammals. Circ. Res. 1967, 20, 99–111. [Google Scholar] [CrossRef]
- Davis, F.M.; Rateri, D.L.; Daugherty, A. Abdominal aortic aneurysm: Novel mechanisms and therapies. Curr. Opin. Cardiol. 2015, 30, 566–573. [Google Scholar] [CrossRef]
- Gimbrone, M.A., Jr.; García-Cardeña, G. Endothelial cell dysfunction and the pathobiology of atherosclerosis. Circ. Res. 2016, 118, 620–636. [Google Scholar] [CrossRef]
- Sumpio, B.E.; Riley, J.T.; Dardik, A. Cells in focus: Endothelial cell. Int. J. Biochem. Cell Biol. 2002, 34, 1508–1512. [Google Scholar] [CrossRef]
- Deanfield, J.E.; Halcox, J.P.; Rabelink, T.J. Endothelial function and dysfunction: Testing and clinical relevance. Circulation 2007, 115, 1285–1295. [Google Scholar] [CrossRef]
- Wassef, M.; Baxter, B.T.; Chisholm, R.L.; Fillinger, M.F.; Heinecke, J.; Zarins, C.K. Pathogenesis of abdominal aortic aneurysms: A multidisciplinary research program supported by the NHLBI. J. Vasc. Surg. 2001, 34, 730–738. [Google Scholar] [CrossRef]
- Touat, Z.; Ollivier, V.; Dai, J.; Huisse, M.G.; Bezeaud, A.; Sebbag, U.; Michel, J.B. Renewal of mural thrombus releases plasma markers and is involved in AAA evolution. Am. J. Pathol. 2006, 168, 1022–1030. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.J.; Lee, M.R.; Park, J.G. Aortic aneurysms: Current pathogenesis and therapeutic targets. Exp. Mol. Med. 2023, 55, 2519–2530. [Google Scholar] [CrossRef] [PubMed]
- Daugherty, A.; Manning, M.W.; Cassis, L.A. Angiotensin II promotes atherosclerotic lesions and aneurysms in ApoE-deficient mice. J. Clin. Investig. 2000, 105, 1605–1612. [Google Scholar] [CrossRef]
- Michel, J.B.; Jondeau, G.; Milewicz, D.M. From genetics to response to injury: Vascular smooth muscle cells in aneurysms and dissections of the ascending aorta. Cardiovasc. Res. 2018, 114, 578–589. [Google Scholar] [CrossRef] [PubMed]
- Basalyga, D.M.; Simionescu, D.T.; Xiong, W.; Baxter, B.T.; Starcher, B.C.; Vyavahare, N.R. Elastin degradation and calcification in an abdominal aorta injury model: Role of matrix metalloproteinases. Circulation 2004, 110, 3480–3487. [Google Scholar] [CrossRef]
- Jones, J.A.; Stroud, R.E.; O’Quinn, E.C.; Black, L.E.; Barth, J.L.; Elefteriades, J.A.; Ikonomidis, J.S. Selective microRNA suppression in human thoracic aneurysms: Relationship of miR-29a to aortic size and proteolytic induction. Circulation 2011, 124, 1460–1469. [Google Scholar] [CrossRef]
- Thompson, R.W.; Parks, W.C. Role of matrix metalloproteinases in abdominal aortic aneurysms. Ann. New York Acad. Sci. 1996, 800, 157–174. [Google Scholar] [CrossRef]
- Lu, H.; Rateri, D.L.; Bruemmer, D.; Cassis, L.A.; Daugherty, A. Novel mechanisms of abdominal aortic aneurysms. Curr. Atheroscler. Rep. 2012, 14, 402–412. [Google Scholar] [CrossRef]
- Curci, J.A.; Liao, S.; Huffman, M.D.; Shapiro, S.D.; Thompson, R.W. Expression and localization of macrophage elastase (matrix metalloproteinase-12) in abdominal aortic aneurysms. J. Clin. Investig. 1998, 102, 1900–1910. [Google Scholar] [CrossRef]
- Longo, G.M.; Xiong, W.; Greiner, T.C.; Zhao, Y.; Fiotti, N.; Baxter, B.T. Matrix metalloproteinases 2 and 9 work in concert to produce aortic aneurysms. J. Clin. Investig. 2002, 110, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Rabkin, S.W. The Role Matrix Metalloproteinases in the Production of Aortic Aneurysm. Prog. Mol. Biol. Transl. Sci. 2017, 147, 239–265. [Google Scholar] [CrossRef] [PubMed]
- Song, T.; Zhao, S.; Luo, S.; Chen, C.; Liu, X.; Wu, X.; Ji, Y. SLC44A2 regulates vascular smooth muscle cell phenotypic switching and aortic aneurysm. J. Clin. Investig. 2024, 134, e173690. [Google Scholar] [CrossRef]
- Golledge, J. Abdominal aortic aneurysm: Update on pathogenesis and medical treatments. Nat. Rev. Cardiol. 2019, 16, 225–242. [Google Scholar] [CrossRef] [PubMed]
- Anidjar, S.; Salzmann, J.L.; Gentric, D.; Lagneau, P.; Camilleri, J.P.; Michel, J.B. Elastase-induced experimental aneurysms in rats. Circulation 1990, 82, 973–981. [Google Scholar] [CrossRef]
- Usui, F.; Shirasuna, K.; Kimura, H.; Tatsumi, K.; Kawashima, A.; Karasawa, T.; Takahashi, M. Inflammasome activation by mitochondrial oxidative stress in macrophages leads to the development of angiotensin II-induced aortic aneurysm. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 127–136. [Google Scholar] [CrossRef]
- Huang, J.; Liu, H.; Liu, Z.; Wang, Z.; Xu, H.; Li, Z.; Fu, Y. Inhibition of aortic CX3CR1+ macrophages mitigates thoracic aortic aneurysm progression in Marfan syndrome in mice. J. Clin. Investig. 2025, 135, e178198. [Google Scholar] [CrossRef]
- Sylvester, A.L.; Zhang, D.X.; Ran, S.; Zinkevich, N.S. Inhibiting NADPH Oxidases to Target Vascular and Other Pathologies: An Update on Recent Experimental and Clinical Studies. Biomolecules 2022, 12, 823. [Google Scholar] [CrossRef]
- Jie, H.; Zhang, J.; Wu, S.; Yu, L.; Li, S.; Dong, B.; Yan, F. Interplay between energy metabolism and NADPH oxidase-mediated pathophysiology in cardiovascular diseases. Front. Pharmacol. 2025, 15, 1503824. [Google Scholar] [CrossRef]
- Ailawadi, G.; Eliason, J.L.; Upchurch, G.R., Jr. Current concepts in the pathogenesis of abdominal aortic aneurysm. J. Vasc. Surg. 2003, 38, 584–588. [Google Scholar] [CrossRef]
- Habashi, J.P.; Judge, D.P.; Holm, T.M.; Cohn, R.D.; Loeys, B.L.; Cooper, T.K.; Dietz, H.C. Losartan, an AT1 antagonist, prevents aortic aneurysm in a mouse model of Marfan syndrome. Science 2006, 312, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Loeys, B.L.; Chen, J.; Neptune, E.R.; Judge, D.P.; Podowski, M.; Holm, T.; Dietz, H.C. A syndrome of altered cardiovascular, craniofacial, neurocognitive and skeletal development caused by mutations in TGFBR1 or TGFBR2. Nat. Genet. 2005, 37, 275–281. [Google Scholar] [CrossRef]
- Lindsay, M.E.; Dietz, H.C. Lessons on the pathogenesis of aneurysm from heritable conditions. Nature 2011, 473, 308–316. [Google Scholar] [CrossRef]
- Jones, J.A.; Spinale, F.G.; Ikonomidis, J.S. Transforming growth factor-beta signaling in thoracic aortic aneurysm development: A paradox in pathogenesis. J. Vasc. Res. 2009, 46, 119–137. [Google Scholar] [CrossRef] [PubMed]
- Milewicz, D.M.; Regalado, E.S. Use of genetics for personalized management of heritable thoracic aortic disease: How do we get there? J. Thorac. Cardiovasc. Surg. 2015, 149 (Suppl. S2), S3–S5. [Google Scholar] [CrossRef] [PubMed]
- MacCarrick, G.; Black, J.H.; Bowdin, S.; El-Hamamsy, I.; Frischmeyer-Guerrerio, P.A.; Guerrerio, A.L.; Dietz, H.C. Loeys-Dietz syndrome: A primer for diagnosis and management. Genet. Med. 2014, 16, 576–587. [Google Scholar] [CrossRef]
- Takeda, N.; Komuro, I. Genetic basis of hereditary thoracic aortic aneurysms and dissections. J. Cardiol. 2018, 71, 345–351. [Google Scholar] [CrossRef]
- Byers, P.H.; Belmont, J.; Black, J.; De Backer, J.; Frank, M.; Jeunemaitre, X.; Wheeldon, N. Diagnosis, natural history, and management in vascular Ehlers-Danlos syndrome. Am. J. Med. Genet. C Semin. Med. Genet. 2017, 175, 40–47. [Google Scholar] [CrossRef]
- Duellman, T.; Warren, C.L.; Peissig, P.; Wynn, M.; Yang, J. Matrix metalloproteinase-9 genotype as a potential genetic marker for abdominal aortic aneurysm. Circ. Cardiovasc. Genet. 2012, 5, 529–537. [Google Scholar] [CrossRef]
- Klarin, D.; Verma, S.S.; Judy, R.; Dikilitas, O.; Wolford, B.N.; Paranjpe, I.; Tsao, P.S. Genetic Architecture of Abdominal Aortic Aneurysm in the Million Veteran Program. Circulation 2020, 142, 1633–1646. [Google Scholar] [CrossRef]
- Bown, M.J.; Jones, G.T.; Harrison, S.C.; Wright, B.J.; Bumpstead, S.; Baas, A.F.; Samani, N.J. Abdominal aortic aneurysm is associated with a variant in low-density lipoprotein receptor-related protein 1. Am. J. Hum. Genet. 2011, 89, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Maegdefessel, L.; Spin, J.M.; Raaz, U.; Eken, S.M.; Toh, R.; Azuma, J.; Tsao, P.S. miR-24 limits aortic vascular inflammation and murine abdominal aneurysm development. Nat. Commun. 2014, 5, 5214. [Google Scholar] [CrossRef] [PubMed]
- Chu, S.; Shan, D.; He, L.; Yang, S.; Feng, Y.; Zhang, Y.; Yu, J. Anemoside B4 attenuates abdominal aortic aneurysm by limiting smooth muscle cell transdifferentiation and its mediated inflammation. Front. Immunol. 2024, 15, 1412022. [Google Scholar] [CrossRef]
- Maegdefessel, L.; Azuma, J.; Toh, R.; Merk, D.R.; Deng, A.; Chin, J.T.; Tsao, P.S. Inhibition of microRNA-29b reduces murine abdominal aortic aneurysm development. J. Clin. Investig. 2012, 122, 497–506. [Google Scholar] [CrossRef]
- Liu, X.; Cheng, Y.; Zhang, S.; Lin, Y.; Yang, J.; Zhang, C. A necessary role of miR-221 and miR-222 in vascular smooth muscle cell proliferation and neointimal hyperplasia. Circ. Res. 2009, 104, 476–487. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Zhang, H.; Huang, S.; Yin, L.; Wang, F.; Luo, P.; Huang, H. Epigenetic regulation in cardiovascular disease: Mechanisms and advances in clinical trials. Signal Transduct. Target. Ther. 2022, 7, 200. [Google Scholar] [CrossRef]
- Daugherty, A.; Cassis, L.A. Mouse models of abdominal aortic aneurysms. Arterioscler. Thromb. Vasc. Biol. 2004, 24, 429–434. [Google Scholar] [CrossRef]
- Yin, L.; Kent, E.W.; Wang, B. Progress in murine models of ruptured abdominal aortic aneurysm. Front. Cardiovasc. Med. 2022, 9, 950018. [Google Scholar] [CrossRef]
- Tian, K.; Malik, F.; Zhao, S. Animal models for abdominal aortic aneurysms: Where we are and where we need to go. Animal Model. Exp. Med. 2025, 8, 573–577. [Google Scholar] [CrossRef]
- Atkinson, G.; Bianco, R.; Di Gregoli, K.; Johnson, J.L. The contribution of matrix metalloproteinases and their inhibitors to the development, progression, and rupture of abdominal aortic aneurysms. Front. Cardiovasc. Med. 2023, 10, 1248561. [Google Scholar] [CrossRef]
- Freestone, T.; Turner, R.J.; Coady, A.; Higman, D.J.; Greenhalgh, R.M.; Powell, J.T. Inflammation and matrix metalloproteinases in the enlarging abdominal aortic aneurysm. Arterioscler. Thromb. Vasc. Biol. 1995, 15, 1145–1151. [Google Scholar] [CrossRef]
- Chiou, A.C.; Chiu, B.; Pearce, W.H. Murine aortic aneurysm produced by periarterial application of calcium chloride. J. Surg. Res. 2001, 99, 371–376. [Google Scholar] [CrossRef]
- Rateri, D.L.; Davis, F.M.; Balakrishnan, A.; Howatt, D.A.; Moorleghen, J.J.; O’Connor, W.N.; Daugherty, A. Angiotensin II induces region-specific medial disruption during development of ascending aortic aneurysms. Am. J. Pathol. 2014, 184, 2586–2595. [Google Scholar] [CrossRef]
- Lindsay, M.E.; Schepers, D.; Bolar, N.A.; Doyle, J.J.; Gallo, E.; Fert-Bober, J.; Loeys, B.L. Loss-of-function mutations in TGFB2 cause a syndromic presentation of thoracic aortic aneurysm. Nat. Genet. 2012, 44, 922–927. [Google Scholar] [CrossRef] [PubMed]
- Galis, Z.S.; Khatri, J.J. Matrix metalloproteinases in vascular remodeling and atherogenesis: The good, the bad, and the ugly. Circ. Res. 2002, 90, 251–262. [Google Scholar] [CrossRef] [PubMed]
- Golledge, J.; Norman, P.E. Atherosclerosis and abdominal aortic aneurysm: Cause, response, or common risk factors? Arterioscler. Thromb. Vasc. Biol. 2010, 30, 1075–1077. [Google Scholar] [CrossRef] [PubMed]
- Curci, J.A. Digging in the “soil” of the aorta to understand the growth of abdominal aortic aneurysms. J. Vasc. Surg. 2009, 49, 260–263. [Google Scholar] [CrossRef]
- Gavrila, D.; Li, W.G.; McCormick, M.L.; Thomas, M.; Daugherty, A.; Cassis, L.A.; Weintraub, N.L. Vitamin E inhibits abdominal aortic aneurysm formation in angiotensin II-infused apolipoprotein E–deficient mice. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 1671–1677. [Google Scholar] [CrossRef]
- Yuan, Z.; Lu, Y.; Wei, J.; Wu, J.; Yang, J.; Cai, Z. Abdominal Aortic Aneurysm: Roles of Inflammatory Cells. Front. Immunol. 2021, 11, 609161. [Google Scholar] [CrossRef]
- MA3RS Study Investigators. Aortic Wall Inflammation Predicts Abdominal Aortic Aneurysm Expansion, Rupture, and Need for Surgical Repair. Circulation 2017, 136, 787–797. [Google Scholar] [CrossRef]
- Takagi, H.; Manabe, H.; Kawai, N.; Goto, S.; Umemoto, T. Plasma fibrinogen and D-dimer concentrations are associated with the presence of abdominal aortic aneurysm: A systematic review and meta-analysis. Eur. J. Vasc. Endovasc. Surg. 2009, 38, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Raffetto, J.D.; Khalil, R.A. Matrix metalloproteinases and their inhibitors in vascular remodeling and vascular disease. Biochem. Pharmacol. 2008, 75, 346–359. [Google Scholar] [CrossRef]
- Shimizu, K.; Mitchell, R.N.; Libby, P. Inflammation and cellular immune responses in abdominal aortic aneurysms. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 987–994. [Google Scholar] [CrossRef]
- Golledge, J.; Muller, J.; Daugherty, A.; Norman, P. Abdominal aortic aneurysm: Pathogenesis and implications for management. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 2605–2613. [Google Scholar] [CrossRef]
- Lei, C.; Kan, H.; Xian, X.; Chen, W.; Xiang, W.; Song, X.; Zheng, Y. FAM3A reshapes VSMC fate specification in abdominal aortic aneurysm by regulating KLF4 ubiquitination. Nat. Commun. 2023, 14, 5360. [Google Scholar] [CrossRef]
- Khan, H.; Abu-Raisi, M.; Feasson, M.; Shaikh, F.; Saposnik, G.; Mamdani, M.; Qadura, M. Current Prognostic Biomarkers for Abdominal Aortic Aneurysm: A Comprehensive Scoping Review of the Literature. Biomolecules 2024, 14, 661. [Google Scholar] [CrossRef] [PubMed]
- Salata, K.; Syed, M.; Hussain, M.A.; de Mestral, C.; Greco, E.; Mamdani, M.; Al-Omran, M. Statins Reduce Abdominal Aortic Aneurysm Growth, Rupture, and Perioperative Mortality: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2018, 7, e008657. [Google Scholar] [CrossRef]
- Baxter, B.T.; Matsumura, J.; Curci, J.A.; McBride, R.; Larson, L.; Blackwelder, W. Effect of Doxycycline on Aneurysm Growth Among Patients with Small Infrarenal Abdominal Aortic Aneurysms: A Randomized Clinical Trial. JAMA 2020, 323, 2029–2038. [Google Scholar] [CrossRef] [PubMed]
- Pramana, K.A.A.P.; Pintaningrum, Y.; Rahmat, B. The effects of statin therapy on aneurysm size, growth rate, and matrix metalloproteinases-9 levels in patients with aortic aneurysm: A systematic review and meta-analysis. Egypt. Heart J. 2023, 75, 88. [Google Scholar] [CrossRef]
- Mangum, K.D.; Farber, M.A. Genetic and epigenetic regulation of abdominal aortic aneurysms. Clin. Genet. 2020, 97, 815–826. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ardahanlı, İ.; Aslan, R.; Özkan, H.İ.; Özel, F.; Özmen, M. A Contemporary Review of Thoracic Aortic Aneurysm: From Molecular Pathogenesis to Clinical Integration. J. Vasc. Dis. 2025, 4, 26. https://doi.org/10.3390/jvd4030026
Ardahanlı İ, Aslan R, Özkan Hİ, Özel F, Özmen M. A Contemporary Review of Thoracic Aortic Aneurysm: From Molecular Pathogenesis to Clinical Integration. Journal of Vascular Diseases. 2025; 4(3):26. https://doi.org/10.3390/jvd4030026
Chicago/Turabian StyleArdahanlı, İsa, Ramazan Aslan, Halil İbrahim Özkan, Faik Özel, and Murat Özmen. 2025. "A Contemporary Review of Thoracic Aortic Aneurysm: From Molecular Pathogenesis to Clinical Integration" Journal of Vascular Diseases 4, no. 3: 26. https://doi.org/10.3390/jvd4030026
APA StyleArdahanlı, İ., Aslan, R., Özkan, H. İ., Özel, F., & Özmen, M. (2025). A Contemporary Review of Thoracic Aortic Aneurysm: From Molecular Pathogenesis to Clinical Integration. Journal of Vascular Diseases, 4(3), 26. https://doi.org/10.3390/jvd4030026