
Effectiveness, Retrievability, and Safety of Celect vs. ALN Inferior Vena Cava Filters: A Randomized Prospective Multicenter Controlled Study

 , , , , , , and
, , , , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. IVCF Indication
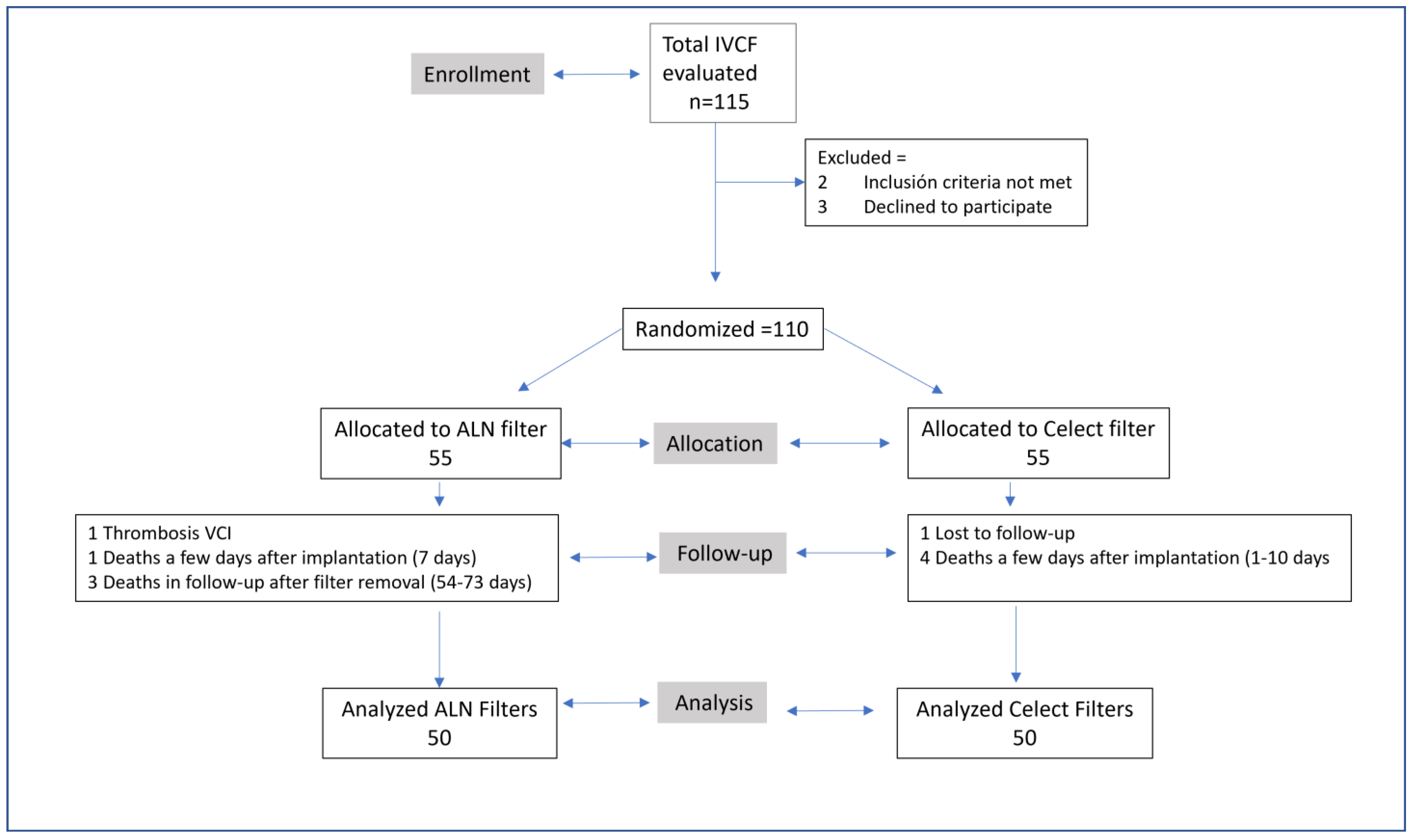
2.2. Study Design
2.3. Randomization and Blinding
2.4. Sample Size
2.5. Filter Placement
2.6. Filter Retrieval
2.7. Outcome Measures
2.8. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| IVC | Inferior vena cava |
| VTD | Venous thromboembolic disease |
| DVT | Deep vein thrombosis |
| PE | Pulmonary embolism |
| AC | Anticoagulants |
| IVCF | Inferior vena cava filter |
| SIR | Society of Interventional Radiology |
| SIDI | Ibero-American Society of Interventionism |
| SERVEI | Spanish Society of Vascular and Interventional Radiology |
References
- Monreal, M.; Mahé, I.; Bura-Riviere, A.; Prandoni, P.; Verhamme, P.; Brenner, B.; Wells, P.S.; Di Micco, P.; Bertoletti, L. Pulmonary embolism: Epidemiology and registries. Presse Med. 2015, 44, e377–e383. [Google Scholar] [CrossRef] [PubMed]
- Pattullo, C.S.; Barras, M.; Tai, B.; Mckean, M.; Donovan, P. New oral anticoagulants: Appropriateness of prescribing in real-world setting. Intern. Med. J. 2016, 46, 812–818. [Google Scholar] [CrossRef] [PubMed]
- Konstantinides, S.V.; Meyer, G. The 2019 ESC Guidelines on the Diagnosis and Management of Acute Pulmonary Embolism. Eur. Heart J. 2019, 40, 3453–3455. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, J.A.; Barnes, G.D.; Chaer, R.A.; Cuschieri, J.; Eberhardt, R.T.; Johnson, M.S.; Kuo, W.T.; Murin, S.; Patel, S.; Rajasekhar, A.; et al. Society of Interventional Radiology Clinical Practice Guideline for Inferior Vena Cava Filters in the Treatment of Patients with Venous Thromboembolic Disease: Developed in collaboration with the American College of Cardiology, American College of Chest Phy-sicians, American College of Surgeons Committee on Trauma, American Heart Association, Society for Vascular Surgery, and Society for Vascular Medicine. J. Vasc. Interv. Radiol. 2020, 31, 1529–1544. [Google Scholar]
- De Gregorio, M.A.; Guirola, J.A.; Sierre, S.; Urbano, J.; Ciampi-Dopazo, J.J.; Abadal, J.M.; Pulido, J.; Eyheremendy, E.; Lonjedo, E.; Guerrero, G.; et al. Ibero-American Society of Interventionism (SIDI) and the Spanish Society of Vascular and Interventional Radiology (SERVEI) Standard of Practice (SOP) for the Management of Inferior Vena Cava Filters in the Treatment of Acute Venous Thromboembolism. J. Clin. Med. 2021, 11, 77. [Google Scholar] [CrossRef]
- Lee, M.J.; Valenti, D.; De Gregorio, M.A.; Minocha, J.; Rimon, U.; Pellerin, O. The CIRSE Retrievable IVC Filter Registry: Retrieval Success Rates in Practice. Cardiovasc. Interv. Radiol. 2015, 38, 1502–1507. [Google Scholar] [CrossRef]
- Jia, Z.; Fuller, T.A.; McKinney, J.M.; Paz-Fumagalli, R.; Frey, G.T.; Sella, D.M.; Van Ha, T.; Wang, W. Utility of Re-trievable Inferior Vena Cava Filters: A Systematic Literature Review and Analysis of the Reasons for Nonretrieval of Filters with Temporary Indications. Cardiovasc. Interv. Radiol. 2018, 41, 675–682. [Google Scholar]
- Uberoi, R.; Tapping, C.R.; Chalmers, N.; Allgar, V. British Society of Interventional Radiology (BSIR) Inferior Vena Cava (IVC) Filter Registry. Cardiovasc. Interv. Radiol. 2013, 36, 1548–1561. [Google Scholar] [CrossRef]
- Bikdeli, B.; Jiménez, D.; Kirtane, A.J.; Bracken, M.B.; Spencer, F.A.; Monreal, M.; Krumholz, H.M. Systematic re-view of efficacy and safety of retrievable inferior vena caval filters. Thromb. Res. 2018, 165, 79–82. [Google Scholar] [CrossRef]
- Morales, J.P.; Li, X.; Irony, T.Z.; Ibrahim, N.G.; Moynahan, M.; Cavanaugh, K.J. Decision analysis of retrievable inferior vena cava filters in patients without pulmonary embolism. J. Vasc. Surg. Venous Lymphat. Disord. 2013, 1, 376–384. [Google Scholar] [CrossRef]
- United States Food and Drug Administration. Alerts and Notices (Medical Devices) Removing Retrieva-Ble Inferior Vena Cava Filters: Initial Communication. Available online: http://www.fda.gov/medicaldevices/safety/alertsandnotices/ucm221676.htm (accessed on 24 August 2022).
- Ryu, R.K.; Desai, K.; Karp, J.; Gupta, R.; Evans, A.E.; Rajeswaran, S.; Salem, R.; Lewandowski, R.J. A comparison of retrievability: Celect versus Option filter. J. Vasc. Interv. Radiol. 2015, 26, 865–869. [Google Scholar] [CrossRef] [PubMed]
- Han, K.; Kim, M.-D.; Kim, G.M.; Kwon, J.H.; Lee, J.; Won, J.Y.; Moon, S.; An, H. Comparison of Retrievability and Indwelling Complications of Celect and Denali Infrarenal Vena Cava Filters: A Randomized, Controlled Trial. Cardiovasc. Interv. Radiol. 2021, 44, 1536–1542. [Google Scholar] [CrossRef]
- De Gregorio, M.A.; Guirola, J.A.; Serrano, C.; Figueredo, A.; Kuo, W.T.; Quezada, C.A.; Jimenez, D. Success in Optional Vena Cava Filter Retrieval. An Analysis of 246 Patients. Arch. Bronconeumol. 2018, 54, 371–377. [Google Scholar] [CrossRef]
- De Gregorio, M.A.; Gamboa, P.; Bonilla, D.L.; Sanchez, M.; Higuera, M.T.; Medrano, J.; Mainar, A.; Lostalé, F.; Laborda, A. Retrieval of Gunther Tulip optional vena cava filters 30 days after implantation: A prospective clinical study. J. Vasc. Interv. Radiol. 2006, 17, 1781–1789. [Google Scholar] [CrossRef]
- Urbaniak, G.C.; Plous, S. Research Randomizer (Version 4.0). 2013. Available online: http://www.randomizer.org/ (accessed on 21 September 2021).
- De Gregorio, M.A.; Guirola, J.A.; Urbano, J.; Díaz-Lorenzo, I.; Muñoz, J.J.; Villacastin, E.; Lopez-Medina, A.; Fi-gueredo, A.L.; Guerrero, J.; Sierre, S.; et al. Spanish multicenter real—Life registry of retrievable vena cava filters (REFiVeC). CVIR Endovasc. 2020, 3, 26. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Pellerin, O.; Barral, F.G.; Lions, C.; Novelli, L.; Beregi, J.P.; Sapoval, M. Early and late retrieval of the ALN re-movable vena cava filter: Results from a multicenter study. Cardiovasc. Interv. Radiol. 2008, 31, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.E.; Van Allan, R.J.; Friedman, M.L.; Lipshutz, H.G. Complications and retrieval characteristics of Celect Platinum inferior vena cava filters. J. Vasc. Surg. Venous Lymphat. Disord. 2018, 6, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Kleedehn, M.; Moore, K.; Longo, K.; Woo, K.; Laeseke, P. An analysis of factors associated with increased fluoroscopy time or the need for complex techniques at IVC filter retrieval. Eur. Radiol. 2019, 29, 1931–1938. [Google Scholar] [CrossRef]
- Dinglasan, L.A.V.; Oh, J.C.; Schmitt, J.; Trerotola, S.O.; Shlansky-Goldberg, R.; Stavropoulos, S.W. Complicated Inferior Vena Cava Filter Retrievals: Associated Factors Identified at Preretrieval CT. Radiology 2013, 266, 347–354. [Google Scholar] [CrossRef]
- Kuyumcu, G.; Walker, T.G. Inferior vena cava filter retrievals, standard and novel techniques. Cardiovasc. Diagn. Ther. 2016, 6, 642–650. [Google Scholar] [CrossRef] [PubMed]
- Desai, K.R.; Lewandowski, R.J.; Salem, R.; Mouli, S.K.; Karp, J.K.; Laws, J.L.; Ryu, R.K. Retrieval of Inferior Vena Cava Filters With Prolonged Dwell Time: A Single-Center Experience in 648 Retrieval Procedures. JAMA Intern. Med. 2015, 175, 1572–1574. [Google Scholar] [CrossRef]
- Merritt, T.; Powell, C.; Hansmann, J. Safety and Effectiveness of Advanced Retrieval Techniques for Inferior Vena Cava Filters Compared with Standard Retrieval Techniques: A Systematic Review of the Literature and Meta-Analysis. J. Vasc. Interv. Radiol. 2022, 33, 564–571.e4. [Google Scholar] [CrossRef]
- Liu, J.; Jiang, P.; Tian, X.; Jia, W.; Huang, N.-L.; Zhan, H.; Chen, W. Clinical outcomes of retrievable inferior vena cava filters for venous thromboembolic diseases. J. Comp. Eff. Res. 2022, 11, 437–449. [Google Scholar] [CrossRef]
- Ramaswamy, R.S.; Jun, E.; van Beek, D.; Mani, N.; Salter, A.; Kim, S.K.; Akinwande, O. Denali, Tulip, and Option Inferior Vena Cava Filter Retrieval: A Single Center Experience. Cardiovasc. Interv. Radiol. 2018, 41, 572–577. [Google Scholar] [CrossRef]
- Kuo, W.T.; Doshi, A.A.; Ponting, J.M.; Rosenberg, J.K.; Liang, T.; Hofmann, L.V. Laser-Assisted Removal of Embedded Vena Cava Filters: A First-In-Human Escalation Trial in 500 Patients Refractory to High-Force Retrieval. J. Am. Heart Assoc. 2020, 9, e017916. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| VTD with contraindication to AC | Age < 18 years |
| Recurrent VDT or PE during AC | Uncontrollable coagulopathy |
| Prevention of PE in high-risk patients | Pre-existing IVCF |
| Preganancy |
| Suprarenal IVCF |
| Variable | Celect Filter (n = 50) | ALN (n = 50) | p Value |
|---|---|---|---|
| Age years (mean, sd, range) | 62.8 ± 12 range (29–85) | 63.7 ± 12 range (29–87) | 0.503 a |
| Sex (n, %) Male Female | 27 (52%) 23 (46%) | 32 (64%) 18 (36%) | 0.313 b |
| BMI (mean, sd, range) | 27.1 ± 4.6 range (21–39) | 28.2 ± 5 range (21.3–40) | 0.314 a |
| Indications (n, %) Contraindication for AC Prevention of high risk of PE Recurrence of PE despite correct AC | 18 (36%) 25 (50%) 7 (14%) | 23 (46%) 20 (40%) 7 (14%) | 0.317 c |
| IVC area (mm2, mean, sd, range) | 433.7 ± 190 range (265–878.2) | 377.9 ± 150 range (282–813) | 0.945 a |
| Deep venous thormbosis (n, %): IVC Iliac vein Femoral vein Popliteal and infra-poplietal vein | 2 (4%) 28 (56%) 35 (70%) 23 (46) | 1 (2%) 23 (46%) 29 (58%) 22 (44%) | 0.629 b 0.687 b 0.398 b 0.685 b |
| Filter immediately after release Centered filter Tilted filter Filter repositioning | 41 (82%) 9 (18%) 9 (18%) | 43 (86%) 7 (14%) 6 (12%) | 0.538 b 0.424 b |
| Venous pressure in IVC (mm Hg) Basal venous pressure (mean, sd, range) Valsalva venous pressure (mean, sd, range) | 12 ± 2.4 range (10–19) 44.4 ± 9.9 range (25–69) | 12 ± 2.1 range (8–18) 43.8 ± 11.9 range (12–84) | 0.827 a 0.613 a |
| Fluoroscopy time (mean, sd, range) | 9.9 ± 1.1 range (5–29) | 7.8 ± 4.3 range (3–15) | 0.380 a |
| Variables | Celect Filter | ALN | |
|---|---|---|---|
| indwelling time of vena cava filter (mean, SD, range) | 55.4 ± 131.9 range (26–996 d) | 34.0 ± 5.8 range (26–61 d) | 0.520 a |
| CT complications before removal | |||
| Tilt at retrieval | 21 (42.0%) | 12 (24.0%) | 0.056 b |
| Filter tip embedment | 12 (24.0%) | 4 (8.0%) | 0.029 b |
| Struts penetration | 7 (14.0%) | 4 (8.0%) | 0.338 b |
| Filter migration | 0 (0.0%) | 0 (0.0%) | - |
| Filter fracture | 0 (0.0%) | 0 (0.0%) | - |
| Intrafilter thrombous | 2 (4.0%) | 1 (2.0%) | 1.000 c |
| IVC Thrombosis | 1 (2.0%) | 0 (0.0%) | 1.000 c |
| Anticoagulation (treatment) | Yes = 47 (94.0%) No = 3 (6.0%) | Yes = 48 (96.0%) No = 2 (4.0%) | 1.000 c |
| Filter removal | |||
| Standard | 41 (82.0%) | 45 (90.0%) | 0.249 b |
| Complex | 9 (18.0%) | 5 (10.0%) | |
| Subjective ease of IVCF removal | |||
| Without difficulty | 33 (66.0%) | 43 (86.0%) | 0.047 d |
| Medium difficulty | 9 (18.0%) | 5 (10.0%) | |
| Quite difficulty | 5 (10.0%) | 2 (4.0%) | |
| Hard | 3 (6.0%) | 0 (0.0%) | |
| Impossible | 0 (0.0%) | 0 (0.0%) | |
| Fluoroscopy time minutes (mean, SD, range) | |||
| Standard | 6.9 ± 2.5 range (3.2–12.5) | 5.9 ± 4.1 range (2.2–26.4) | 0.006 a |
| Complex | 29.1 ± 12.0 range (15.0–51.0) | 17.5 ± 10.3 range (6.5–29.3) | 0.095 e |
| Removal IVCF (mean, SD, range) | |||
| Success | 50 (100%) | 50 (100%) | - |
| Failure | 0 (0.0%) | 0 (0.0%) | |
| Recurrent pulmonary embolism | 0 (0.0%) | 0 (0.0%) | - |
| Post- Thrombotic syndrome (mild-moderate) | |||
| 1 Month | 14 (28.0%) | 12 (24.0%) | 0.648 b |
| 12 Month | 18 (36.0%) | 19 (38.0%) | 0.836 b |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Gregorio, M.A.; Ciampi-Dopazo, J.J.; Urbano, J.; Bernal, R.; Serrano-Casorrán, C.; Bonastre, C.; Abadal, J.M.; Mendez, S.; Fredes, A.; Rodriguez, J.; et al. Effectiveness, Retrievability, and Safety of Celect vs. ALN Inferior Vena Cava Filters: A Randomized Prospective Multicenter Controlled Study. J. Vasc. Dis. 2023, 2, 177-187. https://doi.org/10.3390/jvd2010012
De Gregorio MA, Ciampi-Dopazo JJ, Urbano J, Bernal R, Serrano-Casorrán C, Bonastre C, Abadal JM, Mendez S, Fredes A, Rodriguez J, et al. Effectiveness, Retrievability, and Safety of Celect vs. ALN Inferior Vena Cava Filters: A Randomized Prospective Multicenter Controlled Study. Journal of Vascular Diseases. 2023; 2(1):177-187. https://doi.org/10.3390/jvd2010012
Chicago/Turabian StyleDe Gregorio, Miguel Angel, Juan Jose Ciampi-Dopazo, Jose Urbano, Roman Bernal, Carolina Serrano-Casorrán, Cristina Bonastre, Jose Maria Abadal, Santiago Mendez, Arturo Fredes, Jose Rodriguez, and et al. 2023. "Effectiveness, Retrievability, and Safety of Celect vs. ALN Inferior Vena Cava Filters: A Randomized Prospective Multicenter Controlled Study" Journal of Vascular Diseases 2, no. 1: 177-187. https://doi.org/10.3390/jvd2010012
APA StyleDe Gregorio, M. A., Ciampi-Dopazo, J. J., Urbano, J., Bernal, R., Serrano-Casorrán, C., Bonastre, C., Abadal, J. M., Mendez, S., Fredes, A., Rodriguez, J., Rodriguez, S., & Guirola, J. A. (2023). Effectiveness, Retrievability, and Safety of Celect vs. ALN Inferior Vena Cava Filters: A Randomized Prospective Multicenter Controlled Study. Journal of Vascular Diseases, 2(1), 177-187. https://doi.org/10.3390/jvd2010012