Abstract
Background: Glaucoma is the leading cause of irreversible blindness around the world and is characterized as a group of irreversible optic neuropathies with multiple risk factors such as age, race/ethnicity, sex, and intraocular pressure (IOP), amongst many others that play a role in disease etiology. However, IOP is the only modifiable risk factor, with higher IOP often causing increased damage to the optic nerve, resulting in the vast majority of medical and surgical treatments aiming to reduce IOP. There are a number of interventions available to treat glaucoma including micro-invasive glaucoma surgery (MIGS), whose usage has drastically increased due to its safety and efficacy. Studies also highlight the IOP-reducing effect of cataract surgery, which is the most common procedure performed globally. However, other, more targeted therapies and surgeries have been shown to have a more significant effect on IOP reduction. The objective of this study is to compare the IOP and medication reduction between cataract surgery (CS), MIGS, and MIGS and cataract surgery (MACS) clinical trials. Methods: This analysis consisted of publicly available data on CS, MIGS, and MACS clinical trials from 2005 to 2017 using ClinicalTrials.gov. Data reporting and synthesis adhered to PRISMA guidelines. MIGS interventions studied in this analysis include iStent®, CyPass® Micro-Stent, Ex-PRESS®, Hydrus®, PRESERFLO™ MicroShunt, and XEN® Gel Stent. The main variables of interest are the mean IOP and mean number of glaucoma medications used. The primary outcomes were the baseline, post-procedure, and reduction in IOP and glaucoma medication use. Cohorts were further subdivided by the follow-up period (6, 12, and 24 months), as well as their medicated or unmedicated status for pre-op IOP measurement. PROSPERO CRD42025102892. Results: A total of 21 trials were included in this review, comprising 3330 clinical trial participants: 7 CS trials (N = 570), 13 MIGS trials (N = 1577), and 9 MACS trials (N = 1183). All interventions studied resulted in a decrease in both the IOP and medication usage with varying degrees. At 12 months, the wash-out baseline IOP reduction (mmHg) was 6.9 (27.5%) for CS, 8.8 (34.0%) for MIGS, and 8.2 (32.6%) for MACS. The medication reduction was 0.8 (56.1%) following CS, 1.0 (39.5%) for MIGS, and 1.3 (86.4%) for MACS. At 24 months, the wash-out baseline IOP reduction was 6.3 (25.1%) for CS, 8.4 (33.1%) for MIGS, and 7.6 (30.1%) for MACS. At 24 months, the medication reduction was 0.9 (58.3%) for CS, 1.5 (79.8%) for MIGS, and 1.3 (86.1%) for MACS. Conclusions: The results indicate that CS, MIGS, and MACS all result in a decrease in the IOP and glaucoma medications; however, MIGS and MACS outperform CS in IOP and medication reduction. Adopting MIGS and MACS for patients with ocular hypertension or mild-to-moderate glaucoma will help improve patient outcomes through reducing the IOP and medication burden. Given that glaucoma affects certain populations to a greater degree, future research analyzing racial representation is critical in ensuring the appropriate applicability of clinical trial results toward diverse populations.
1. Introduction
Cataracts and glaucoma are both leading causes of visual impairment and blindness around the world [1]. In 2020, cataracts were the largest contributors to global blindness in adults aged 50 years and older with over 15 million cases, which is approximately 35% of the total cases for global blindness [2]. However, cataracts are usually curable through surgical intervention. The prevalence of cataracts increases with age, and while most scholars agree that this is a normal part of the aging process, others argue that the increase in prevalence with age is related to the cumulative exposure to risk factors such as UV radiation and cigarette smoke [3]. As part of the normal aging process, the crystalline lens inside the eye undergoes hardening and opacification. This opacification with the accumulation of yellow-brown pigment within the lens results in a decreased amount of light transmission to the retina, causing a subsequent reduction in visual acuity amongst many other symptoms [4]. Because of the global prevalence of cataracts, cataract surgery is one of the most common procedures performed worldwide and may also be considered among the most successful treatments in medicine [4,5]. In the surgery, the lens is broken up by a phacoemulsification device using ultrasound and aspirated out of the eye. After removal, an artificial intraocular lens is placed in the lens capsule, with a multitude of options and qualities that result in varying degrees of improved vision. Due to consistent advancements in cataract surgery, surgical time, cost, and outcomes have drastically improved, resulting in an increasing amount of people being able to receive the procedure [5].
Glaucoma is the leading cause of irreversible blindness worldwide and the second leading cause of blindness in America. In 2020, glaucoma was estimated to have impacted 76 million adults aged between 40 and 80 years of age, and it is projected to affect 111.8 million adults by 2040 [6]. Glaucoma is categorized into open angle and angle closure, depending on the anterior chamber angle anatomy. The global prevalence of primary open angle glaucoma (POAG) is 3.05%, with the highest rates of the disease being found in people of African ancestry, while the prevalence of primary angle closure glaucoma is 0.5%, with the highest rates in people of Asian ancestry [6]. Glaucoma is an optic neuropathy that is characterized by damage to the optic nerve, resulting in irreversible vision loss. The only modifiable risk factor for glaucoma is intraocular pressure (IOP), which is the main target for the various treatments that are available. Intraocular pressure is directly impacted by the level of aqueous humor outflow in the eye, with decreases in the aqueous outflow increasing both the intraocular pressure and the risk of developing glaucomatous neuropathy [7,8]. To date, the pathogenesis of glaucoma is not fully understood, but the levels of intraocular pressure are directly related to rate of retinal ganglion cell death.
There are numerous treatments available for glaucoma, ranging from pharmaceutical to surgical treatment. Since IOP is the only modifiable risk factor for glaucoma, all the treatments aim to control or reduce IOP in hopes of decreasing the risk for the progression of glaucoma. The first line of treatment for glaucoma is pharmacotherapy, although it has a number of challenges including patient noncompliance, difficulty with drop administration, ocular and systemic side effects, and a high cost, among others [9,10,11,12]. Various initial methods to treat patients stem from the consistent regimens of topical eye drops such as prostaglandin analogs or beta-blockers [7]. Other treatments include laser procedures to create alternative drainage pathways or to stimulate areas of the trabecular meshwork. These laser procedures include selective laser trabeculoplasty and laser peripheral iridotomy, amongst others [13]. Popular treatments such as trabeculectomies are also used to surgically create an alternative drainage pathway for the aqueous humor [14]. Other, more severe cases of glaucoma require glaucoma drainage devices, such as the Ahmed Glaucoma Valve, that can significantly reduce the intraocular pressure. However, these procedures come with increased long-term risks such as bleeding, infection, corneal swelling, and macular edema [15].
Over the last two decades, micro-invasive glaucoma surgery (MIGS) has significantly grown in popularity as a result of its safety and efficacy profile [16]. Specifically in the US, MIGS utilization has grown more than 400% from 2013 to 2018, resulting in many new clinical trials and devices being introduced to the field [17,18]. MIGS are characterized by their relatively atraumatic surgical approach, minimal disruption to ocular tissues, and rapid postoperative recovery compared to traditional glaucoma surgeries [19]. MIGS devices include Schlemm’s canal devices such as iStent or Hydrus, suprachoroidal devices such as CyPass and iStent Supra, and subconjunctival devices such as XEN-45 [20]. The majority of MIGS procedures are used to treat open angle glaucoma subtypes such as primary open angle glaucoma [16]. These surgeries are best suited for patients with mild-to-moderate glaucoma or ocular hypertension and those who have trouble with topical medications but are not eligible to receive more invasive, traditional glaucoma surgery [21,22]. In addition to decreasing the IOP, these low-risk surgeries can also decrease eye drop dependence and increase quality of life as a result. Due to their higher efficacy, lower surgical times, and faster recovery, MIGS are becoming a staple in modern glaucoma treatment.
Moreover, due to the convenience and micro-invasive nature of MIGS, these surgeries can be conducted alongside other, more-invasive, surgeries in order to limit the patient’s time in the operating room. Cataract surgery is a common procedure that is conducted alongside MIGS, allowing for lower costs for the patient in addition to reduced risk due to the patient spending less time under anesthesia [23]. As a result of the growing prevalence of MIGS, more clinical trials are also testing the effects of MIGS devices alongside other surgeries like cataract surgery. Cataract surgery alone can also result in reduced intraocular pressure, which can be enhanced when coupled with a MIGS device [16,24]. This decline in post-op intraocular pressure can occur in patients with or without glaucoma, although the degree to which the reduction is reported to occur is not consistent among the studies [24,25]. Because lens growth plays a pivotal mechanist role in primary angle closure glaucoma, lens extraction has been shown to control the IOP, widen the iridocorneal angle, deepen the anterior chamber, and reduce angle crowding in patients with narrow angles or angle closure glaucoma, in addition to correcting persistent pupillary block [26]. However, the pathophysiology of POAG is less mechanistically related to the lens; therefore, the relationship between cataract surgery and the IOP decrease is not as well established. Due to the growing global population and increased life expectancy, especially in first world countries, many people are developing cataracts in addition to glaucoma. Studies have found glaucoma to be one of the leading ocular comorbidities for cataracts [27]. Hence, it is crucial to understand the efficacy of each surgery individually and together to identify the most optimal treatment plan for patients, especially those with both glaucoma and cataracts. The primary objective of this study is to compare the IOP and medication reduction between MIGS, cataract surgery, and MIGS and cataract surgery (MACS). We also determined whether combined cataract surgery and MIGS provided better outcomes than cataract surgery or MIGS alone.
2. Methods
2.1. Study Search and Selection
This review adheres to the Preferred Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines and focuses on peer-reviewed evidence for the devices, implants, and procedures summarized in Table 1 [28].

Table 1.
Baseline characteristics of each trial.
The clinical trial data was sourced from ClinicalTrials.gov using appropriate keywords and filters such as glaucoma, cataract, glaucoma and cataract, studies with results, completed studies, and interventional studies. The search and data extraction was conducted in June 2024 using trials on MIGS, MIGS and cataract surgery combined or cataract surgery alone. The start years of the collected trial data spanned between 2003 and 2017. Only randomized controlled trials (RCTs) published in English were included. The protocol was registered with the international prospective register of systematic reviews (PROSPERO CRD42025102892) [50].
This review was deemed exempt from institutional review board approval and informed consent because it collected and synthesized non-identifiable data from previously published studies.
2.1.1. Inclusion Criteria
- MIGS clinical trials, cataract surgery clinical trials, or MIGS and cataract surgery clinical trials;
- Completed interventional studies;
- Publicly available studies with results;
- Institutional review board-approved studies;
- Outcome data including IOP and medication reduction.
2.1.2. Exclusion Criteria
- Follow-up shorter than 6 months;
- Glaucoma types other than POAG (e.g., NTG or ACG);
- Lack of data on medication usage or intraocular pressure (IOP);
- Studies still ongoing, open to accrual, or not published in English.
2.1.3. Interventions
This study adopts the definition of MIGS from Saheb and Ahmed’s 2012 review, which characterizes the class of surgical procedures defined by a favorable safety profile, preservation of ocular anatomy, ab interno approach, demonstrated efficacy, and ease of use [19].
MIGS procedures can be classified based on their mechanism of action and anatomical site, which includes the following:
- -
- Schlemm’s canal devices (e.g., iStent, Hydrus Microstent, trabectome, Kahook dual blade, and GATT);
- -
- Suprachoroidal space (e.g., CyPass);
- -
- Subconjunctival space (e.g., XEN Gel Stent, PRESERFLO MicroShunt);
- -
- Ciliary body (e.g., endocyclophotocoagulation) [21].
After screening the clinical trials, the following interventions were included:
- -
- Cataract surgery/phacoemulsification;
- -
- iStent®;
- -
- CyPass® Micro-Stent;
- -
- Ex-PRESS®;
- -
- Hydrus®;
- -
- PRESERFLO™ MicroShunt (F.K.A., InnFocus, MIDI Arrow);
- -
- XEN® Gel Stent.
Screening of trials was carried out by reviewing the exported trial information from ClinicalTrials.Gov. Each trial was then evaluated independently for eligibility by reviewing the “Conditions, Study Type, and Intervention”. The process was made according to the PRISMA flow diagram included in the Results section (Figure 1).
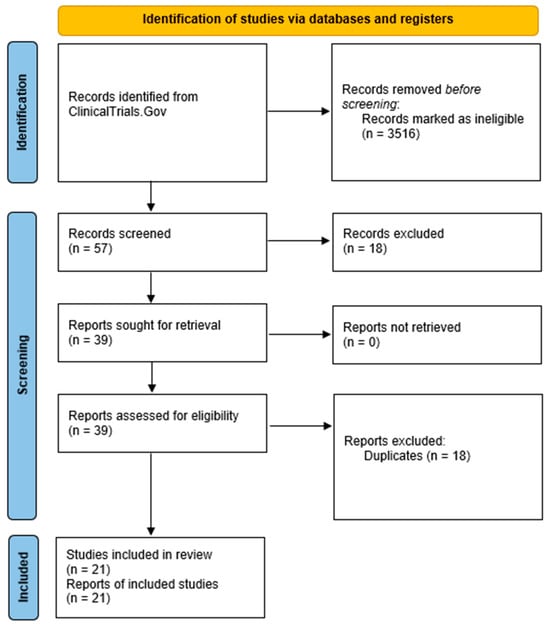
Figure 1.
PRISMA flow diagram demonstrating number of clinical trials included and excluded.
2.2. Data Synthesis and Analysis
Extracted data included (1) medical intervention, (2) number of participants, (3) year the study started, (4) year the study ended, (5) region in which the study was conducted, (6) financial sponsor, (7) participant sex/gender, (8) ethnicity (if indicated), (9) race (if indicated), (10) age (if indicated), (11) IOP baseline, (12) post-procedure IOP, (13) IOP reduction, (14) baseline medications, (15) post-procedure medications, (16) medication reduction, and (17) baseline IOP measurement method (medicated vs. unmedicated).
The geographic region of a study was defined using the United Nations classification, which includes Africa, Asia, Europe, Latin America and the Caribbean, North America, and Oceania [51]. We also added “multiregional” as a category to account for studies that encompassed more than 1 region. Sponsors for these trials were medical device companies, medical centers or universities, foundations, or government agencies. These were organized as such into (1) medical center or university, (2) medical device companies, or (3) collaborators, which included more than one sponsor type working together, as some sponsors of more than one category worked together on one trial. Details on the sponsors, interventions, trial type, and a detailed summary for each of the trials can be found in the Supplement, File S1, in Tables S1–S4.
Statistical analyses were conducted using Microsoft Excel v2508 (Microsoft Corporation, Redmond, WA, USA) and Python, v3.10.12. Trials were grouped according to the trial start year, the region in which the trial took place, the type of study sponsor, and IOP collection method when available. Descriptive statistics were obtained for all collected data. The weighted mean difference in IOP and number of glaucoma medications from baseline to endpoint was calculated for each follow-up period.
The primary outcomes of this analysis were the effect of MIGS compared to cataract surgery alone and MACS on reduction in IOP and medication usage 6, 12, and 24 months after surgery. The measure of effect was the mean change in IOP (mmHg) and mean change in the number of glaucoma medications. The number of glaucoma medications was defined as the total count of distinct topical or systemic medications used by participants in the clinical trials for the treatment of glaucoma. This includes, but is not limited to, alpha agonists, beta blockers, carbonic anhydrase inhibitors, and prostaglandin analogs. This metric does not account for dosing frequency or number of daily administrations.
3. Results
3.1. Study Selection
A total of 3573 records were exported and screened from ClinicalTrials.Gov using the search strategy described above. At the end of the process, 21 clinical trials were identified and included in the analysis, which comprised 3330 participants. Seven trials compared MACS with cataract surgery alone, one trial compared MACS with MACS, one trial compared MACS with MIGS alone, two trials compared MIGS with MIGS, three trials compared MIGS with Trabeculectomy, and seven trials studied MIGS alone. Figure 1 displays the PRISMA diagram for this review, which visually represents the process for how studies are identified, screened, and ultimately included.
3.2. Baseline Characteristics
Baseline characteristics of the included studies are reported in Table 1 below and include the trial type, primary author, start year, ClinicalTrial.gov NCT number, trial name, if available, sponsor, region, follow-up period, treatment group, and the control group. Please note that two of the included studies (NCTABC, NCTX) were not found on ClinicalTrial.gov, as they were referenced separately.
A summary of the baseline demographic and clinical characteristics of the study populations across the included trials is presented in Table 2.
Table 2.
Overall clinical trial demographics.
3.3. Outcomes Analysis
The tables below report the baseline (IOP-B), post-procedure (IOP-P), and reduction in IOP (IOP-R). All IOP measurements are recorded as mmHg. The tables also report the baseline (MED-B), post-procedure (MED-P), and reduction in glaucoma medications (MED-R). Values are aggregated by the IOP baseline measurement type (medicated and unmedicated) and clinical trial. The tables also include the trial type, intervention type, author, start year, NCT number, and IOP baseline measurement. Table 3, Table 4 and Table 5 below report the IOP and glaucoma medications for the clinical trials reporting a 6-, 12-, and 24-month follow-up, respectively.
Table 3.
Summary of IOP and glaucoma medication changes in clinical trials at 6 month follow-up. Cells are marked “NR” if the trial did not report those values.
Table 4.
Summary of IOP and glaucoma medication changes in clinical trials at 12 month follow-up. Cells are marked “NR” if the trial did not report those values.
Table 5.
Summary of IOP and glaucoma medication changes in clinical trials at 24 month follow-up. Cells are marked “NR” if the trial did not report those values.
3.3.1. 6 Month Outcomes
Figure 2 and Figure 3 visually illustrate the IOP and medication reduction between the baseline and post-procedure at six months, respectively. The CS unmedicated cohort had an IOP reduction of 16.9% (4.0 mmHg) and a 58.3% decrease in medication use. In the medicated baseline, the MIGS cohort saw a 31.7% IOP reduction (7.8 mmHg) and an 85.0% reduction in medication usage, while the unmedicated cohort saw an IOP reduction of 45.0% (11.3 mmHg). In the medicated baseline, MACS saw an IOP reduction of 20.5% (4.1 mmHg) and medication use by 70.8%. In the unmedicated baseline, it had a 35.5% IOP reduction (8.6 mmHg) and a 90.9% decrease in medication use. Table 6 summarizes the 6-month follow-up outcomes data.
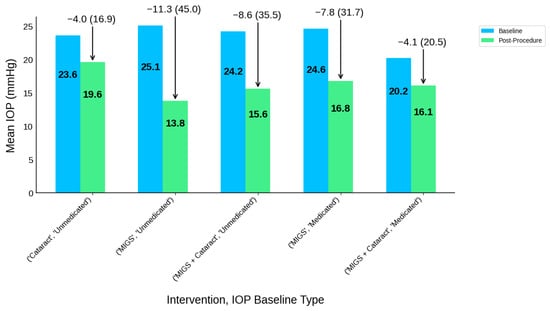
Figure 2.
IOP at baseline and post-procedure at 6-month follow-up.

Figure 3.
Glaucoma medication baseline and post-procedure at 6-month follow-up.
Table 6.
Summary of outcomes data at 6-month follow-up including IOP and glaucoma medication baseline, post-procedure, and reduction. Cells are marked “NR” if the trial did not report those values.
3.3.2. 12 Month Outcomes
Figure 4 and Figure 5 visually illustrate the IOP and medication reduction between the baseline and post-procedure at 12 months, respectively. In the medicated baseline, CS resulted in an IOP reduction of 0.4% (0.1 mmHg) and 58.8% decrease in medication use. In the unmedicated baseline, it saw a 27.5% (6.9 mmHg) and 56.1% reduction in IOP and medication usage, respectively. In the medicated baseline, MIGS led to a 24.5% IOP reduction (5.1 mmHg) and a 64.4% reduction in medication burden, while in unmedicated patients, MIGS saw a 34.0% IOP reduction (8.8 mmHg) and 39.5% reduction in medication burden. In the medicated cohort, MACS reduced the IOP by 18.4% (3.6 mmHg) and medication use by 72.3%, whereas in the unmedicated cohort, it led to a 32.6% IOP reduction (8.2 mmHg) and an 86.4% decrease in medication use. Table 7 summarizes the 12-month follow-up outcomes data.

Figure 4.
IOP baseline and post-procedure at 12-month follow-up.
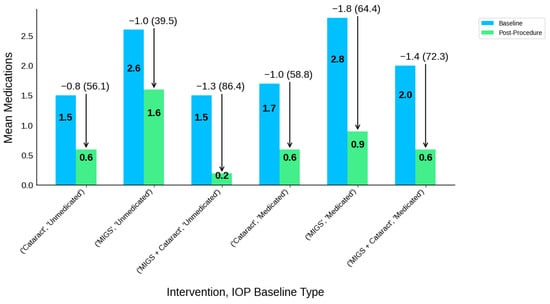
Figure 5.
Glaucoma medication baseline and post-procedure at 12-month follow-up.
Table 7.
Summary of outcomes data at 12-month follow-up including IOP and glaucoma medication baseline, post-procedure, and reduction.
3.3.3. 24 Month Outcomes
Figure 6 and Figure 7 visually illustrate the IOP and medication reduction between the baseline and post-procedure at 24 months, respectively. In the medicated baseline, CS resulted in an IOP reduction of 3.2% (0.6 mmHg) and 54.4% decrease in medication use, while the unmedicated baseline saw a 25.1% (6.3 mmHg) and 58.3% reduction in IOP and medication use, respectively. In the medicated cohort, MIGS led to a 25.9% IOP reduction (5.4 mmHg) and a 71.0% reduction in medication burden, while in the unmedicated cohort, MIGS achieved a 33.1% IOP reduction (8.4 mmHg) and 79.8% reduction in medication use. In the medicated cohort, MACS reduced the IOP by 15.4% (2.9 mmHg) and medication use by 73.1%. In the unmedicated baseline, it led to a 30.1% IOP reduction (7.6 mmHg) and an 86.1% decrease in medication use. Table 8 summarizes the 24-month follow-up outcomes data.

Figure 6.
IOP baseline and post-procedure at 24-month follow-up.

Figure 7.
Glaucoma medication baseline and post-procedure at 24-month follow-up.
Table 8.
Summary of outcomes data at 24-month follow-up including IOP and glaucoma medication baseline, post-procedure, and reduction.
4. Discussion
4.1. Outcomes
We have performed a review of 21 clinical trials, consisting of 3330 participants, that studied MIGS alone, cataract surgery alone, or MIGS combined with cataract surgery. Several different types of clinical trials were included such as MIGS combined vs. MIGS combined, MIGS combined vs. cataract surgery, MIGS combined vs. MIGS, MIGS vs. MIGS, MIGS vs. Trabeculectomy, and MIGS alone. These studies primarily investigated IOP and medication reductions at 6-, 12-, or 24-month follow-up. Trials utilized either a wash-out IOP baseline (unmedicated), non-wash-out baseline (medicated), or provided both values.
Stability of IOP Reduction and Glaucoma Medication Reduction
At six months, IOP and glaucoma medication reductions varied by intervention type. MIGS achieved the greatest IOP reduction and medication burden reduction in the medicated baseline cohort (31.7% and 85.0%, respectively), while MACS had the greatest decrease in medication burden in the unmedicated baseline cohort (90.9%). Cataract surgery alone resulted in a modest IOP reduction of 16.9% and a 58.3% decrease in medication use in the unmedicated baseline group; however, no results were published for patients with a medicated IOP baseline measurement. By 12 months, MIGS continued to provide a superior IOP reduction in both baseline cohorts. However, MACS saw a greater medication reduction and similar IOP reduction using wash-out IOP values. Similar findings were seen at 24 months: MIGS and MACS both had similar IOP reductions in using the wash-out IOP baseline values (33.1% and 30.1%), while the latter had a greater medication reduction in both baseline cohorts (73.1% vs. 71.0% for medicated; 86.1% vs. 79.8% for unmedicated). These findings suggest that both MIGS and MACS provide a stable and durable reduction in the IOP and glaucoma medication use over time.
4.2. Safety Profile of Cataract Surgery and MIGS
The excellent safety profile of MIGS devices is a leading cause for such a rapid growth in usage over the past decade, especially when compared to more traditional glaucoma surgeries like Trabeculectomy and tube shunts, which have higher rates of intraoperative and vision-threatening complications [52]. Due to their minimally invasive nature and high safety profile, MIGS devices are oftentimes also used in conjunction with more invasive procedures such as cataract surgery. When factoring whether a patient should receive MIGS only vs. MIGS and cataract surgery, the physician must understand the efficacy measures and also the general safety outcomes of the procedures and devices.
MIGS devices that enhance the aqueous outflow through the trabecular meshwork with an implant such as the iStent inject or Hydrus Microstent did have some reports of adverse reactions, which were generally transient [52]. Fea et al. found that possible complications of the iStent inject included IOP spikes and stent obstruction, which is also seen in Hydrus Microstent as well [52,53]. In the three-year findings of the HORIZON Trial, Ahmed et al. found peripheral anterior synechiae formation in those with Hydrus Microstents and cataract surgery but not in the cataract surgery alone group [54]. Additionally, hyphema was a common complication for MIGS methods that use tissue excision to bypass the trabecular meshwork such as trabectome, Ab Interno Canaloplasty, and KDB goniotomy [52]. Studies with the OMNI system also found anterior chamber (AC) inflammation and hyphema, which required subsequent AC wash-out [55]. Posterior capsular opacification and corneal edema were also found in 17% and 4.9% of patients, respectively, who underwent an operation with OMNI and cataract surgery [56]. Another study analyzing iStent and iStent inject alone and with cataract surgery found comparable safety profiles, with no significant adverse events between the combined MIGS and cataract and isolated MIGS [57]. Generally, adverse events such as posterior capsular opacification and corneal edema that can occur under cataract surgery alone can also be present when conducted with MIGS [58].
In their study about analyzing the postoperative outcomes of iStent Supra, which is a suprachoroidal MIGS, Myers and colleagues found that 15% of patients had a Best Corrected Visual Acuity (BCVA) loss of three lines or more [59]. A prospective study by Grover et al. with 65 patients that underwent surgery with an XEN gel implant, which is a MIGS that shunts the aqueous outflow into the subconjunctival space, found that 21.5% of patients experienced an IOP spike, 27.7% with a BCVA loss of two lines or more and 24.6% with transient hypotony [42]. Especially, due to the subconjunctival space needed for MIGS, requiring bleb formation, related complications such as needling, hypotony, and choroidal effusions can occur; other, more serious side effects due to blebs are endophthalmitis, which can result in severe vision loss [52]. Although MIGS does not achieve as much of an IOP reduction as traditional glaucoma surgeries, such as tube shunts, the minimal number of severe and long-term complications helps MIGS become a viable option for people with early-stage glaucoma, whether it be with cataract surgery or alone.
4.3. Availability and Ease of Implementation of MIGS in Countries with High Glaucoma Burden
With glaucoma being the leading cause of irreversible blindness around the world, the disease is prevalent in many regions around the world. However, certain regions such as Africa and Latin America have a high burden of glaucoma, specifically the primary open angle subtype, with estimated prevalences of 4.2% and 3.65%, respectively, in 2013 [6]. Developing countries in Africa and Latin America have the highest prevalences of glaucoma due to the decreased use of eye care and screening, along with genetic factors linked to these populations. Low- and middle-income countries usually rely on opportunistic screenings and prevention, which results in significant amounts of patients being screened with advanced stages of diseases [60,61]. On the other hand, MIGS has been proven to have a high efficacy in patients with ocular hypertension or mild-to-moderate glaucoma. Due to developing countries with a high glaucoma burden having a substantial amount of end-stage glaucoma patients, providers may elect to perform more invasive traditional glaucoma surgeries in hopes of having more of the IOP decreasing effect.
Developing countries also might not have abundant access to the latest forms of medical devices and technologies such as MIGS due to the cost and ease of implementation. MIGS devices are generally priced at a premium, which is evident by the target markets being countries with significant healthcare coverage and resources such as the United States, United Kingdom, and Canada [62]. Markets in developing countries with a high burden of glaucoma tend to rely on cheaper MIGS devices. Hence, it is critical for companies to try to shift business models toward reducing the prices in exchange for an increase in sales volume, resulting in substantially more people having better outcomes in addition to profit for the manufacturer [62]. Developed countries that oftentimes have a lower comparative glaucoma burden compared to countries in Africa or Latin America are also at the forefront of clinical trials and studies related to MIGS, emphasizing the need to include more countries that have a high glaucoma burden. The lack of inclusion of developing countries in MIGS advancements could account for the decreased usage and development of these devices in those regions [60,63].
Another constraint toward the increased accessibility of these devices and surgical methods is the additional specialized training that is required to perform MIGS. The specific surgical skill and knowledge of the mechanisms of action might cause already established glaucoma physicians that use traditional glaucoma surgeries to face a steep learning curve [64,65]. The implementation of these devices requires updates to established residency and fellowship programs in addition to additional funding to allow physicians in training to adequately train in MIGS cases. Additional challenges emerge when factoring in the lack of available faculty trained in these surgical techniques [66]. Yim et al. found that MIGS devices such as iStent, endocyclophotocoagulation (ECP), and trabectome were commonly taught in US ophthalmology residency programs. However, programs with less resources can implement more affordable MIGS options such as 23-gauge cystotome goniotomy [66]. Due to the novelty of MIGS devices in the field of glaucoma treatment, there have been constant advancements that have improved surgical techniques, safety, and efficacy. Moving forward, when considering which surgical techniques to use for patients who fit the treatment category of having ocular hypertension or mild-to-moderate glaucoma, the initial cost of MIGS devices could be overcome due to long-term savings through a lower reliance on medications and less requirements for postoperative management due to the devices’ safety profile. Additionally, existing glaucoma physicians and ophthalmologists should continue to participate in community and specialty conferences and discussions to be up to date on the latest and most effective treatments in order to provide the best outcomes for their patients.
4.4. Limitations
There are several limitations to our study. First, we excluded ongoing trials that were still open to accrual. Future analyses should explore the prevalence of minority representation in such trials.
Another methodological limitation involved variations in trial design. Only a subset of studies implemented a wash-out period before measuring the IOP, likely due to ethical considerations, complicating direct comparisons across trials. Follow-up durations also varied, with many trials limiting follow-up to 12 months or less due to the relative novelty of MIGS procedures. This study did not evaluate the safety outcomes or adverse events reported in trials. Future research should consider longer-term outcomes to assess the efficacy and safety of treatments.
Furthermore, we did not directly contact the study authors for raw data, which posed challenges in data extraction, as some trials did not publish their results explicitly. In such cases, we had to estimate data from charts or graphs from published results. Discrepancies were also observed between demographic and outcome data reported in ClinicalTrials.gov and corresponding journal publications, possibly due to data updates occurring before or after trial results were posted, suggesting a need for additional research or oversight into the trial data reporting process.
5. Conclusions
As glaucoma continues to grow as the world’s leading cause of irreversible blindness, new surgical procedures such as MIGS will continue to be created and applied in different settings and disease stages. MIGS has rapidly grown in popularity due to its minimally invasive nature resulting in excellent efficacy and safety profiles, which has also enabled physicians to combine this procedure with other, more invasive surgeries such as cataract surgery. The results indicate that CS, MIGS, and MACS all result in a decrease in IOP and glaucoma medications. However, MIGS and MACS outperform CS in IOP and medication reductions, with MIGS being an effective and safe addition to intraocular surgeries such as CS. Hence, when treating patients with ocular hypertension or mild-to-moderate glaucoma, MIGS alone or with cataract surgery can offer effective outcomes, especially with the excellent efficacy and safety profiles of MIGS devices compared to more traditional glaucoma surgeries. Glaucoma continues to affect certain populations to a greater degree, with regions such as Africa facing a severe disease burden. Hence, future research should analyze racial representation in clinical trials across the various disciplines of medicine to ensure the appropriate applicability of the respective results toward diverse populations and minorities.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/jcto3040020/s1, Table S1: Interventions Included. Table S2: Types of Sponsors. Table S3: Characteristics of Clinical Trials. Table S4: Clinical Trial Summary. File S1: Clinical Trial Detailed Information [29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49].
Author Contributions
Conceptualization, K.A. and D.P.; Methodology, K.A. and D.P.; Software, J.A. and A.V.; Validation, K.A., J.A., and A.V.; Formal Analysis, J.A. and A.V.; Investigation, J.A.; Resources, K.A. and A.V.; Data curation, J.A. and A.V.; Writing—original draft preparation, J.A.; Writing—review and editing, K.A., A.V., and D.P.; Visualization, A.V., Supervision, D.P.; Project administration, K.A.; Funding acquisition, K.A. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no specific funding for this work.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Flaxman, S.R.; Bourne, R.R.A.; Resnikoff, S.; Ackland, P.; Braithwaite, T.; Cicinelli, M.V.; Das, A.; Jonas, J.B.; Keeffe, J.; Kempen, J.H.; et al. Global causes of blindness and distance vision impairment 1990–2020: A systematic review and meta-analysis. Lancet Glob. Health 2017, 5, e1221–e1234. [Google Scholar] [CrossRef]
- Abdulhussein, D.; Abdul Hussein, M. WHO Vision 2020: Have We Done It? Ophthalmic Epidemiol. 2023, 30, 331–339. [Google Scholar] [CrossRef]
- Hashemi, H.; Pakzad, R.; Yekta, A.; Aghamirsalim, M.; Pakbin, M.; Ramin, S.; Khabazkhoob, M. Global and regional prevalence of age-related cataract: A comprehensive systematic review and meta-analysis. Eye 2020, 34, 1357–1370. [Google Scholar] [CrossRef]
- Allen, D.; Vasavada, A. Cataract and surgery for cataract. BMJ 2006, 333, 128–132. [Google Scholar] [CrossRef]
- Davis, G. The Evolution of Cataract Surgery. Mo. Med. 2016, 113, 58–62. [Google Scholar]
- Tham, Y.C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.Y. Global Prevalence of Glaucoma and Projections of Glaucoma Burden through 2040: A Systematic Review and Meta-Analysis. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef]
- Schuster, A.K.; Erb, C.; Hoffmann, E.M.; Dietlein, T.; Pfeiffer, N. The Diagnosis and Treatment of Glaucoma. Dtsch. Arztebl. Int. 2020, 117, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Sharaawy, T.; Bhartiya, S. Surgical management of glaucoma: Evolving paradigms. Indian J. Ophthalmol. 2011, 59 (Suppl. S1), S123–S130. [Google Scholar] [CrossRef] [PubMed]
- Zaharia, A.C.; Dumitrescu, O.M.; Radu, M.; Rogoz, R.E. Adherence to Therapy in Glaucoma Treatment—A Review. J. Pers. Med. 2022, 12, 514. [Google Scholar] [CrossRef] [PubMed]
- Lacey, J.; Cate, H.; Broadway, D.C. Barriers to adherence with glaucoma medications: A qualitative research study. Eye 2009, 23, 924–932. [Google Scholar] [CrossRef]
- Tsai, J.C.; McClure, C.A.; Ramos, S.E.; Schlundt, D.G.; Pichert, J.W. Compliance barriers in glaucoma: A systematic classification. J. Glaucoma 2003, 12, 393–398. [Google Scholar] [CrossRef]
- Newman-Casey, P.A.; Robin, A.L.; Blachley, T.; Farris, K.; Heisler, M.; Resnicow, K.; Lee, P.P. Most Common Barriers to Glaucoma Medication Adherence: A Cross-Sectional Survey. Ophthalmology 2015, 122, 1308–1316. [Google Scholar] [CrossRef]
- Chang, R.T.; Singh, K. Glaucoma Suspect: Diagnosis and Management. Asia-Pac. J. Ophthalmol. 2016, 5, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Binibrahim, I.H.; Bergström, A.K. The role of trabeculectomy in enhancing glaucoma patient’s quality of life. Oman J. Ophthalmol. 2017, 10, 150–154. [Google Scholar] [CrossRef]
- Gedde, S.J.; Herndon, L.W.; Brandt, J.D.; Budenz, D.L.; Feuer, W.J.; Schiffman, J.C. Postoperative Complications in the Tube Versus Trabeculectomy (TVT) Study During Five Years of Follow-up. Am. J. Ophthalmol. 2012, 153, 804–814.e1. [Google Scholar] [CrossRef]
- Birnbaum, F.A.; Neeson, C.; Solá-Del Valle, D. Microinvasive Glaucoma Surgery: An Evidence-Based Review. Semin. Ophthalmol. 2021, 36, 772–786. [Google Scholar] [CrossRef]
- Radcliffe, N. The case for standalone micro-invasive glaucoma surgery: Rethinking the role of surgery in the glaucoma treatment paradigm. Curr. Opin. Ophthalmol. 2023, 34, 138–145. [Google Scholar] [CrossRef]
- Yang, S.A.; Mitchell, W.; Hall, N.; Elze, T.; Lorch, A.C.; Miller, J.W.; Zebardast, N.; Pershing, S.; Hyman, L.; Haller, J.A.; et al. Trends and Usage Patterns of Minimally Invasive Glaucoma Surgery in the United States: IRIS® Registry Analysis 2013–2018. Ophthalmol. Glaucoma 2021, 4, 558–568. [Google Scholar] [CrossRef]
- Saheb, H.; Ahmed, I.I.K. Micro-invasive glaucoma surgery: Current perspectives and future directions. Curr. Opin. Ophthalmol. 2012, 23, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Otárola, F.; Pooley, F. Minimally invasive glaucoma surgery (MIGS) devices: Risks, benefits and suitability. Community Eye Health 2021, 34, 59–60. [Google Scholar] [PubMed]
- Gillmann, K.; Mansouri, K. Minimally Invasive Glaucoma Surgery: Where Is the Evidence? Asia Pac. J. Ophthalmol. 2020, 9, 203–214. [Google Scholar] [CrossRef]
- Cantor, L.; Lindfield, D.; Ghinelli, F.; Świder, A.W.; Torelli, F.; Steeds, C.; Jr, J.E.D.; Nguyen, D.Q. Systematic Literature Review of Clinical, Economic, and Humanistic Outcomes Following Minimally Invasive Glaucoma Surgery or Selective Laser Trabeculoplasty for the Treatment of Open-Angle Glaucoma with or Without Cataract Extraction. Clin. Ophthalmol. 2023, 17, 85–101. [Google Scholar] [CrossRef]
- Porter. Combined Cataract-Glaucoma Surgery and MIGS. American Academy of Ophthalmology. 25 May 2023. Available online: https://www.aao.org/eye-health/treatments/combined-cataract-glaucoma-surgery-facts (accessed on 15 January 2025).
- Berdahl, J.P. Cataract Surgery to Lower Intraocular Pressure. Middle East Afr. J. Ophthalmol. 2009, 16, 119–122. [Google Scholar] [CrossRef]
- Mansberger, S.L.; Gordon, M.O.; Jampel, H.; Bhorade, A.; Brandt, J.D.; Wilson, B.; Kass, M.A. Reduction in intraocular pressure after cataract extraction: The Ocular Hypertension Treatment Study. Ophthalmology 2012, 119, 1826–1831. [Google Scholar] [CrossRef] [PubMed]
- Tarongoy, P.; Ho, C.L.; Walton, D.S. Angle-closure Glaucoma: The Role of the Lens in the Pathogenesis, Prevention, and Treatment. Surv. Ophthalmol. 2009, 54, 211–225. [Google Scholar] [CrossRef] [PubMed]
- Pham, T.Q.; Wang, J.J.; Rochtchina, E.; Maloof, A.; Mitchell, P. Systemic and ocular comorbidity of cataract surgical patients in a western Sydney public hospital. Clin. Exp. Ophthalmol. 2004, 32, 383–387. [Google Scholar] [CrossRef]
- PRISMA Statement. PRISMA 2020 Checklist. Available online: https://www.prisma-statement.org/prisma-2020-checklist (accessed on 14 March 2025).
- Ivantis, Inc. A Prospective, Multicenter, Randomized Comparison of the Hydrus Microstent to the iStent for Lowering Intraocular Pressure in Glaucoma Patients Undergoing Cataract Surgery. clinicaltrials.gov. 2024. Available online: https://clinicaltrials.gov/study/NCT02024464 (accessed on 2 March 2025).
- Fan Gaskin, J.C.; Bigirimana, D.; Kong, G.Y.X.; McGuinness, M.B.; Atik, A.; Liu, L.; Brooks, A.M.; Ang, G.S. Prospective, Randomized Controlled Trial of Cataract Surgery vs Combined Cataract Surgery with Insertion of iStent Inject. Ophthalmol. Glaucoma 2024, 7, 326–334. [Google Scholar] [CrossRef]
- Fea, A.M. Phacoemulsification versus phacoemulsification with micro-bypass stent implantation in primary open-angle glaucoma. J. Cataract. Refract. Surg. 2010, 36, 407–412. [Google Scholar] [CrossRef]
- Fernández-Barrientos, Y.; García-Feijoó, J.; Martínez-De-La-Casa, J.M.; Pablo, L.E.; Fernández-Pérez, C.; Sánchez, J.G. Fluorophotometric Study of the Effect of the Glaukos Trabecular Microbypass Stent on Aqueous Humor Dynamics. Investig. Opthalmology Vis. Sci. 2010, 51, 3327–3332. [Google Scholar] [CrossRef]
- Pfeiffer, N.; Garcia-Feijoo, J.; Martinez-De-La-Casa, J.M.; Larrosa, J.M.; Fea, A.; Lemij, H.; Gandolfi, S.; Schwenn, O.; Lorenz, K.; Samuelson, T.W. A Randomized Trial of a Schlemm’s Canal Microstent with Phacoemulsification for Reducing Intraocular Pressure in Open-Angle Glaucoma. Ophthalmology 2015, 122, 1283–1293. [Google Scholar] [CrossRef] [PubMed]
- Samuelson, T.W.; Katz, L.J.; Wells, J.M.; Duh, Y.-J.; Giamporcaro, J.E.; US iStent Study Group. Randomized Evaluation of the Trabecular Micro-Bypass Stent with Phacoemulsification in Patients with Glaucoma and Cataract. Ophthalmology 2011, 118, 459–467. [Google Scholar] [CrossRef]
- Samuelson, T.W.; Chang, D.F.; Marquis, R.; Flowers, B.; Lim, K.S.; Ahmed, I.I.K.; Jampel, H.D.; Aung, T.; Crandall, A.S.; Singh, K.; et al. A Schlemm Canal Microstent for Intraocular Pressure Reduction in Primary Open-Angle Glaucoma and Cataract. Ophthalmology 2019, 126, 29–37. [Google Scholar] [CrossRef]
- Vold, S.; Ahmed, I.I.K.; Craven, E.R.; Mattox, C.; Stamper, R.; Packer, M.; Brown, R.H.; Ianchulev, T. Two-Year COMPASS Trial Results: Supraciliary Microstenting with Phacoemulsification in Patients with Open-Angle Glaucoma and Cataracts. Ophthalmology 2016, 123, 2103–2112. [Google Scholar] [CrossRef]
- For The Apex Study Group; Reitsamer, H.; Sng, C.; Vera, V.; Lenzhofer, M.; Barton, K.; Stalmans, I. Two-year results of a multicenter study of the ab interno gelatin implant in medically uncontrolled primary open-angle glaucoma. Graefe’s Arch. Clin. Exp. Ophthalmol. 2019, 257, 983–996. [Google Scholar] [CrossRef]
- Beckers, H.J.; Aptel, F.; Webers, C.A.; Bluwol, E.; Martínez-De-La-Casa, J.M.; García-Feijoó, J.; Lachkar, Y.; Méndez-Hernández, C.D.; Riss, I.; Shao, H.; et al. Safety and Effectiveness of the PRESERFLO® MicroShunt in Primary Open-Angle Glaucoma. Ophthalmol. Glaucoma 2022, 5, 195–209. [Google Scholar] [CrossRef]
- de Jong, L.A.M.S. The Ex-PRESS glaucoma shunt versus trabeculectomy in open-angle glaucoma: A prospective randomized study. Adv. Ther. 2009, 26, 336–345. [Google Scholar] [CrossRef]
- Denis, P.; Hirneiß, C.; Durr, G.M.; Reddy, K.P.; Kamarthy, A.; Calvo, E.; Hussain, Z.; Ahmed, I.K. Two-year outcomes of the MINIject drainage system for uncontrolled glaucoma from the STAR-I first-in-human trial. Br. J. Ophthalmol. 2020, 106, 65–70. [Google Scholar] [CrossRef]
- Garcìa-Feijoo, J.; Höh, H.; Uzunov, R.; Dickerson, J.E., Jr. Supraciliary Microstent in Refractory Open-Angle Glaucoma: Two-Year Outcomes from the DUETTE Trial. J. Ocul. Pharmacol. Ther. 2018, 34, 538–542. [Google Scholar] [CrossRef]
- Grover, D.S.; Flynn, W.J.; Bashford, K.P.; Lewis, R.A.; Duh, Y.-J.; Nangia, R.S.; Niksch, B. Performance and Safety of a New Ab Interno Gelatin Stent in Refractory Glaucoma at 12 Months. Arch. Ophthalmol. 2017, 183, 25–36. [Google Scholar] [CrossRef]
- Hoeh, H.; Vold, S.D.; Ahmed, I.K.; Anton, A.; Rau, M.; Singh, K.; Chang, D.F.; Shingleton, B.J.; Ianchulev, T. Initial Clinical Experience With the CyPass Micro-Stent. Eur. J. Gastroenterol. Hepatol. 2016, 25, 106–112. [Google Scholar] [CrossRef]
- Riss, I. A 2-Year, Single-Center Study to Assess the Safety and Effectiveness of the MicroShunt in Primary Open-Angle Glaucoma. Ophthalmic Res. 2022, 66, 206–217. [Google Scholar] [CrossRef]
- Ahmed, I.I.K.; Fea, A.; Au, L.; Ang, R.E.; Harasymowycz, P.; Jampel, H.D.; Samuelson, T.W.; Chang, D.F.; Rhee, D.J. A Prospective Randomized Trial Comparing Hydrus and iStent Microinvasive Glaucoma Surgery Implants for Standalone Treatment of Open-Angle Glaucoma. Ophthalmology 2020, 127, 52–61. [Google Scholar] [CrossRef]
- Transcend Medical, Inc. Randomized, Prospective Clinical Evaluation of the Safety and Effectiveness of Visco-Assisted CyPass® Implantation in Patients with Open Angle Glaucoma. clinicaltrials.gov. 2019. Available online: https://clinicaltrials.gov/study/NCT02448875 (accessed on 1 March 2025).
- Baker, N.D.; Barnebey, H.S.; Moster, M.R.; Stiles, M.C.; Vold, S.D.; Khatana, A.K.; Flowers, B.E.; Grover, D.S.; Strouthidis, N.G.; Panarelli, J.F. Ab-Externo MicroShunt versus Trabeculectomy in Primary Open-Angle Glaucoma. Ophthalmology 2021, 128, 1710–1721. [Google Scholar] [CrossRef]
- Netland, P.A.; Sarkisian, S.R., Jr.; Moster, M.R.; Ahmed, I.I.; Condon, G.; Salim, S.; Sherwood, M.B.; Siegfried, C.J. Randomized, prospective, comparative trial of EX-PRESS glaucoma filtration device versus trabeculectomy (XVT study). Am J Ophthalmol. 2014, 157, 433–440. [Google Scholar] [CrossRef]
- Wagschal, L.D.; Trope, G.E.; Jinapriya, D.; Jin, Y.P.; Buys, Y.M. Prospective Randomized Study Comparing Ex-PRESS to Trabeculectomy: 1-Year Results. J. Glaucoma 2015, 24, 624–629. [Google Scholar] [CrossRef]
- PROSPERO. Available online: https://www.crd.york.ac.uk/PROSPERO/view/CRD420251028923 (accessed on 15 April 2025).
- UNSD—Methodology. Standard Country or Area Codes for Statistical Use (M49). Available online: https://unstats.un.org/unsd/methodology/m49 (accessed on 8 April 2025).
- Rowson, A.C.; Hogarty, D.T.; Maher, D.; Liu, L. Minimally Invasive Glaucoma Surgery: Safety of Individual Devices. J. Clin. Med. 2022, 11, 6833. [Google Scholar] [CrossRef]
- Fea, A.M.; Belda, J.I.; Rękas, M.; Junemann, A.; Chang, L.; Pablo, L.; Voskanyan, L.; Katz, L.J. Prospective unmasked randomized evaluation of the iStent inject® versus two ocular hypotensive agents in patients with primary open-angle glaucoma. Clin. Ophthalmol. 2014, 8, 875–882. [Google Scholar] [CrossRef]
- Ahmed, I.I.K.; Rhee, D.J.; Jones, J.; Singh, I.P.; Radcliffe, N.; Gazzard, G.; Samuelson, T.W.; Ong, J.; Singh, K. Three-Year Findings of the HORIZON Trial: A Schlemm Canal Microstent for Pressure Reduction in Primary Open-Angle Glaucoma and Cataract. Ophthalmology 2021, 128, 857–865. [Google Scholar] [CrossRef]
- Toneatto, G.; Zeppieri, M.; Papa, V.; Rizzi, L.; Salati, C.; Gabai, A.; Brusini, P. 360° Ab-Interno Schlemm’s Canal Viscodilation with OMNI Viscosurgical Systems for Open-Angle Glaucoma-Midterm Results. J. Clin. Med. 2022, 11, 259. [Google Scholar] [CrossRef]
- Hirsch, L.; Cotliar, J.; Vold, S.; Selvadurai, D.; Campbell, A.G.; Ferreira, G.; Aminlari, A.; Cho, A.; Heersink, S.; Hochman, M.; et al. Canaloplasty and trabeculotomy ab interno with the OMNI system combined with cataract surgery in open-angle glaucoma: 12-month outcomes from the ROMEO study. J. Cataract. Refract. Surg. 2021, 47, 907–915. [Google Scholar] [CrossRef]
- Silveira Seixas, R.C.; Balbino, M.; Basile Neto, A.; de Alcantara Almeida Costa, A.; Jordão, M.L.d.S.; Russ, H.H.A. Mid-Term Evaluation of iStent Inject® Trabecular Micro-Bypass Stent Implantation with or without Phacoemulsification: A Retrospective Study. Clin. Ophthalmol. 2020, 14, 4403–4413. [Google Scholar] [CrossRef]
- Briceno-Lopez, C.; Burguera-Giménez, N.; García-Domene, M.C.; Díez-Ajenjo, M.A.; Peris-Martínez, C.; Luque, M.J. Corneal Edema after Cataract Surgery. J. Clin. Med. 2023, 12, 6751. [Google Scholar] [CrossRef]
- Myers, J.S.; Masood, I.; Hornbeak, D.M.; Belda, J.I.; Auffarth, G.; Jünemann, A.; Giamporcaro, J.E.; Martinez-De-La-Casa, J.M.; Ahmed, I.I.K.; Voskanyan, L.; et al. Prospective Evaluation of Two iStent® Trabecular Stents, One iStent Supra® Suprachoroidal Stent, and Postoperative Prostaglandin in Refractory Glaucoma: 4-year Outcomes. Adv. Ther. 2018, 35, 395–407. [Google Scholar] [CrossRef]
- Li, R.; Liu, H.; Zhang, K.; Lu, Z.; Wang, N. Global tendency and research trends of minimally invasive surgery for glaucoma from 1992 to 2023: A visual bibliometric analysis. Heliyon 2024, 10, e36591. [Google Scholar] [CrossRef]
- Liu, H.; Li, R.; Zhang, Y.; Zhang, K.; Yusufu, M.; Liu, Y.; Mou, D.; Chen, X.; Tian, J.; Li, H.; et al. Economic evaluation of combined population-based screening for multiple blindness-causing eye diseases in China: A cost-effectiveness analysis. Lancet Glob. Health 2023, 11, e456–e465. [Google Scholar] [CrossRef]
- Sng, C.C.A.; Tham, C.C.; Budenz, D.L.; Healey, P.R.; Wang, N. Globalization of MIGS. In Minimally Invasive Glaucoma Surgery; Sng, C.C.A., Barton, K., Eds.; Springer: Singapore, 2021; pp. 147–156. [Google Scholar] [CrossRef]
- Allison, K.; Patel, D.G.; Greene, L. Racial and Ethnic Disparities in Primary Open-Angle Glaucoma Clinical Trials: A Systematic Review and Meta-analysis. JAMA Netw Open. 2021, 4, e218348. [Google Scholar] [CrossRef]
- Dhawale, K.K.; Tidake, P. A Comprehensive Review of Recent Advances in Minimally Invasive Glaucoma Surgery: Current Trends and Future Directions. Cureus 2024, 16, e65236. [Google Scholar] [CrossRef]
- Cheema, A.A.; Cheema, H.R. The Evolution and Current Landscape of Minimally Invasive Glaucoma Surgeries: A Review. Cureus 2024, 16, e52183. [Google Scholar] [CrossRef]
- Yim, C.K.; Teng, C.C.; Warren, J.L.; Tsai, J.C.; Chadha, N. Microinvasive Glaucoma Surgical Training in United States Ophthalmology Residency Programs. Clin. Ophthalmol. 2020, 14, 1785–1789. [Google Scholar] [CrossRef]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).